
Modulation of Neuroendocrine and Immunological Biomarkers Following Rehabilitation in Sarcopenic Patients

 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients Enrolled in the Study
2.2. Plasma Sample Collection
2.3. ELISA
2.4. Statistical Analysis
3. Results
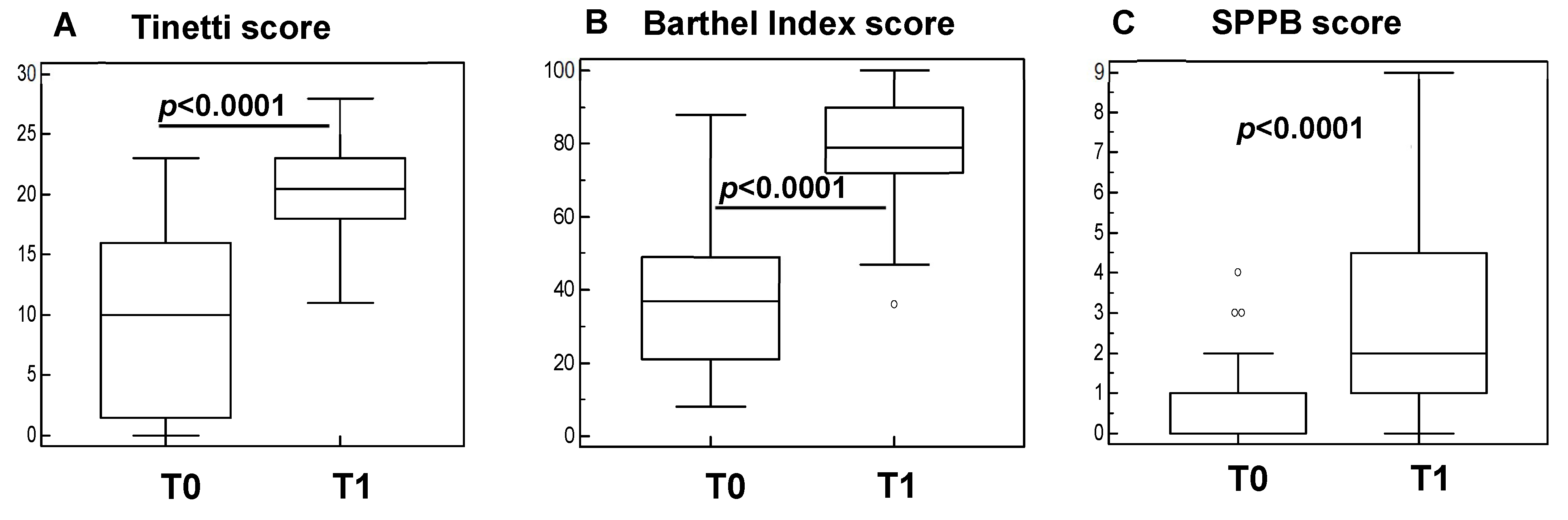
3.1. Rehabilitation Significantly Improves Clinical Parameters in Sarcopenic Subjects
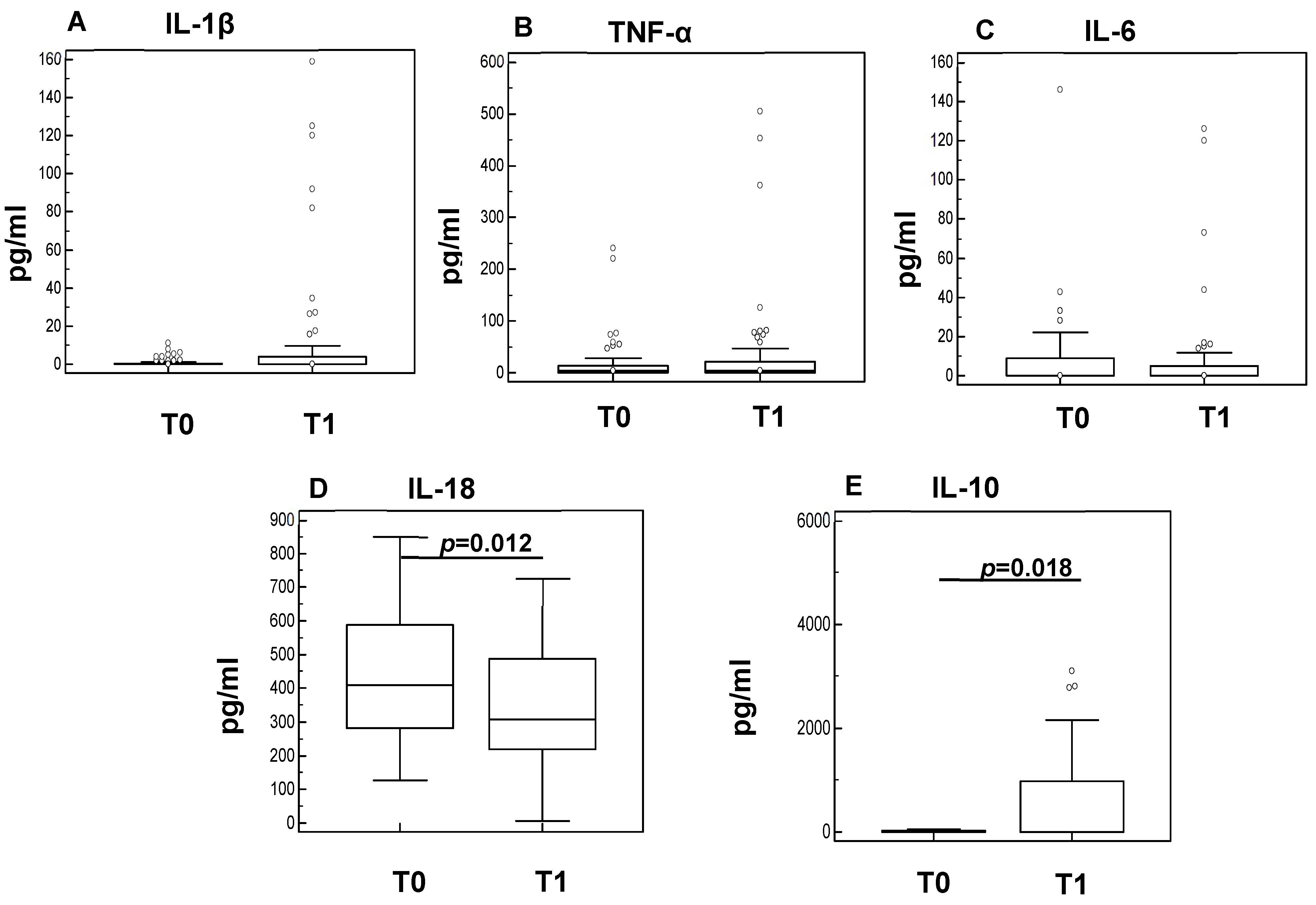
3.2. Rehabilitation Has an Anti-Inflammatory Effect in Sarcopenic Subjects
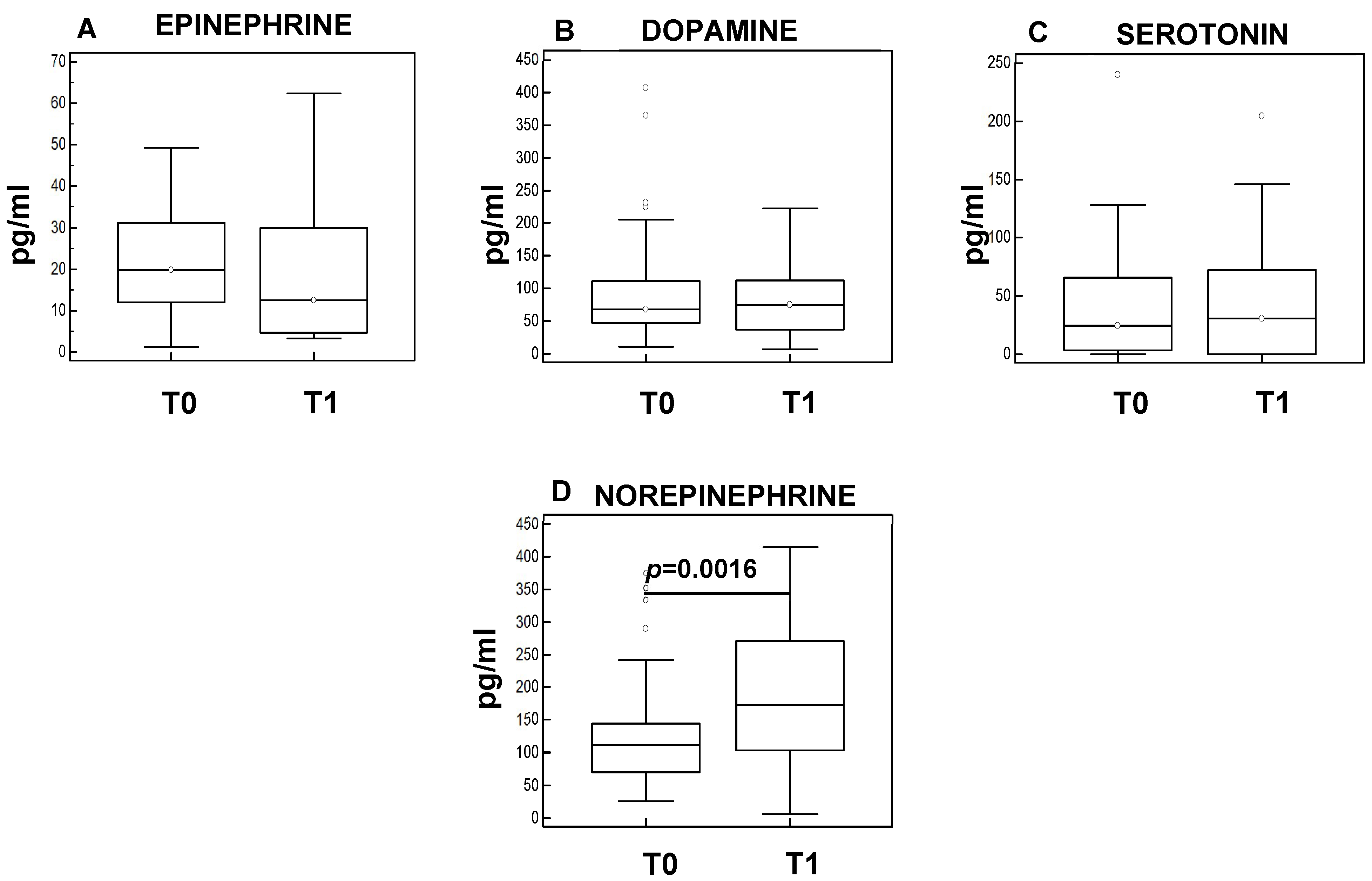
3.3. Rehabilitation Results in Neuromodulation in Sarcopenic Subjects
3.4. Correlation of Clinical Functional Scales and Biological Parameters
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Cruz-Jentoft, A.J.; Sayer, A.A. Sarcopenia. Lancet 2019, 393, 2636–2646. [Google Scholar] [CrossRef]
- Vellas, B.; Fielding, R.A.; Bens, C.; Bernabei, R.; Cawthon, P.M.; Cederholm, T.; Cruz-Jentoft, A.J.; Del Signore, S.; Donahue, S.; Morley, J.; et al. Implications of ICD-10 for Sarcopenia Clinical Practice and Clinical Trials: Report by the International Conference on Frailty and Sarcopenia Research Task Force. J. Frailty Aging 2018, 7, 2–9. [Google Scholar] [CrossRef]
- Tournadre, A.; Vial, G.; Capel, F.; Soubrier, M.; Boirie, Y. Sarcopenia. Jt. Bone Spine 2019, 86, 309–314. [Google Scholar] [CrossRef] [PubMed]
- Fuggle, N.; Shaw, S.; Dennison, E.; Cooper, C. Sarcopenia. Best Pract. Res. Clin. Rheumatol. 2017, 31, 218–242. [Google Scholar] [CrossRef] [Green Version]
- Bauer, J.; Morley, J.E.; Schols, A.M.W.J.; Ferrucci, L.; Cruz-Jentoft, A.J.; Dent, E.; Baracos, V.E.; Crawford, J.A.; Doehner, W.; Heymsfield, S.B.; et al. Sarcopenia: A Time for Action. An SCWD Position Paper. J. Cachexia Sarcopenia Muscle 2019, 10, 956–961. [Google Scholar] [CrossRef]
- Hodo, T.W.; de Aquino, M.T.P.; Shimamoto, A.; Shanker, A. Critical Neurotransmitters in the Neuroimmune Network. Front. Immunol. 2020, 11, 1869. [Google Scholar] [CrossRef]
- Pongratz, G.; Straub, R.H. The sympathetic nervous response in inflammation. Arthritis Res. Ther. 2014, 16, 504. [Google Scholar] [CrossRef] [Green Version]
- Cruz-Jentoft, A.J.; Baeyens, J.P.; Bauer, J.M.; Boirie, Y.; Cederholm, T.; Landi, F.; Martin, F.C.; Michel, J.P.; Rolland, Y.; Schneider, S.M.; et al. Sarcopenia: European consensus on definition and diagnosis: Report of the European Working Group on Sarcopenia in Older People. Age Ageing 2010, 39, 412–423. [Google Scholar] [CrossRef] [Green Version]
- Meng, S.J.; Yu, L.J. Oxidative stress, molecular inflammation and sarcopenia. Int. J. Mol. Sci. 2010, 1, 1509–1526. [Google Scholar] [CrossRef] [Green Version]
- Sakuma, K.; Yamaguchi, A. Novel intriguing strategies attenuating to sarcopenia. J. Aging Res. 2012, 2012, 251217. [Google Scholar] [CrossRef]
- Cupps, T.R.; Fauci, A.S. Corticosteroid-mediated immunoregulation in man. Immunol. Rev. 1982, 65, 133–155. [Google Scholar] [CrossRef] [PubMed]
- Bergmann, M.; Gornikiewicz, A.; Sautner, T.; Waldmann, E.; Weber, T.; Mittlböck, M.; Roth, E.; Függer, R. Attenuation of catecholamine-induced immunosuppression in whole blood from patients with sepsis. Shock 1999, 12, 421–427. [Google Scholar] [CrossRef] [PubMed]
- Cruz-Jentoft, A.J.; Bahat, G.; Bauer, J.; Boirie, Y.; Bruyère, O.; Cederholm, T.; Cooper, C.; Landi, F.; Rolland, Y.; Sayer, A.A.; et al. Writing Group for the European Working Group on Sarcopenia in Older People 2 (EWGSOP2), and the Extended Group for EWGSOP2. Sarcopenia: Revised European consensus on definition and diagnosis. Age Ageing 2019, 48, 16–31. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Guralnik, J.M.; Simonsick, E.M.; Ferrucci, L.; Glynn, R.J.; Berkman, L.F.; Blazer, D.G.; Scherr, P.A.; Wallace, R.B. A short physical performance battery assessing lower extremity function: Association with self-reported disability and prediction of mortality and nursing home admission. J. Gerontol. 1994, 49, M85–M94. [Google Scholar] [CrossRef]
- Mahoney, F.I.; Barthel, D.W. Functional evaluation: The Barthel index. Md. State Med. J. 1965, 14, 61–65. [Google Scholar]
- Tinetti, M.; Richman, D.; Powell, L. Falls efficacy as a measure of fear of falling. J. Gerontol. 1990, 45, P239. [Google Scholar] [CrossRef]
- Ulus, Y.; Durmus, D.; Akyol, Y.; Terzi, Y.; Bilgici, A.; Kuru, O. Reliability and validity of the Turkish version of the Falls Efficacy Scale International (FES-I) in community-dwelling older persons. Arch. Gerontol. Geriatr. 2012, 54, 429–433. [Google Scholar] [CrossRef]
- Rosenberg, I.H. Sarcopenia: Origins and clinical relevance. J. Nutr. 1997, 127 (Suppl. 5), 990S–991S. [Google Scholar] [CrossRef] [Green Version]
- Cruz-Jentoft, A.J.; Romero-Yuste, S.; Chamizo Carmona, E.; Nolla, J.M. Sarcopenia, immune-mediated rheumatic diseases, and nutritional interventions. Aging Clin. Exp. Res. 2021, 33, 2929–2939. [Google Scholar] [CrossRef]
- Budui, S.L.; Rossi, A.P.; Zamboni, M. The pathogenetic bases of sarcopenia. Clin. Cases Miner. Bone Metab. 2015, 12, 22–26. [Google Scholar] [CrossRef]
- Schaap, L.A.; Pluijm, S.M.; Deeg, D.J.; Harris, T.B.; Kritchevsky, S.B.; Newman, A.B.; Colbert, L.H.; Pahor, M.; Rubin, S.M.; Tylavsky, F.A.; et al. Higher inflammatory marker levels in older persons: Associations with 5-year change in muscle mass and muscle strength. J. Gerontol. A Biol. Sci. Med. Sci. 2009, 64, 1183–1189. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Geffken, D.F.; Cushman, M.; Burke, G.L.; Polak, J.F.; Sakkinen, P.A.; Tracy, R.P. Association between physical activity and markers of inflammation in a healthy elderly population. Am. J. Epidemiol. 2001, 153, 242–250. [Google Scholar] [CrossRef] [PubMed]
- Mathur, N.; Pedersen, B.K. Exercise as a mean to control low-grade systemic inflammation. Mediat. Inflamm. 2008, 2008, 109502. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Smart, N.A.; Larsen, A.I.; Le Maitre, J.P.; Ferraz, A.S. Effect of exercise training on interleukin-6, tumour necrosis factor alpha and functional capacity in heart failure. Cardiol. Res. Pract. 2011, 2011, 532620. [Google Scholar] [CrossRef] [Green Version]
- Flynn, M.G.; McFarlin, B.K.; Markofski, M.M. The Anti-Inflammatory Actions of Exercise Training. Am. J. Lifestyle Med. 2007, 1, 220–235. [Google Scholar] [CrossRef] [Green Version]
- Trøseid, M.; Lappegård, K.T.; Mollnes, T.E.; Arnesen, H.; Seljeflot, I. The effect of exercise on serum levels of interleukin-18 and components of the metabolic syndrome. Metab. Syndr. Relat. Disord. 2009, 7, 579–584. [Google Scholar] [CrossRef]
- Petersen, A.M.; Pedersen, B.K. The anti-inflammatory effect of exercise. J. Appl. Physiol. 2005, 98, 1154–1162. [Google Scholar] [CrossRef] [Green Version]
- Mota, B.C.; Pereira, L.; Souza, M.A.; Silva, L.F.; Magni, D.V.; Ferreira, A.P.; Oliveira, M.S.; Furian, A.F.; Mazzardo-Martins, L.; Silva, M.D.; et al. Exercise pre-conditioning reduces brain inflammation and protects against toxicity induced by traumatic brain injury: Behavioral and neurochemical approach. Neurotox. Res. 2012, 21, 175–184. [Google Scholar] [CrossRef]
- Steensberg, A. The role of IL-6 in exercise-induced immune changes and metabolism. Exerc. Immunol. Rev. 2003, 9, 40–47. [Google Scholar]
- Steensberg, A.; Fischer, C.P.; Keller, C.; Moller, K.; Pedersen, B.K. IL-6 enhances plasma IL-1ra, IL-10, and cortisol in humans. Am. J. Physiol. Endocrinol. Metab. 2003, 285, E433–E437. [Google Scholar] [CrossRef]
- Dimitrov, S.; Hulteng, E.; Hong, S. Inflammation and exercise: Inhibition of monocytic intracellular TNF production by acute exercise via β2-adrenergic activation. Brain Behav. Immun. 2017, 61, 60–68. [Google Scholar] [CrossRef] [PubMed]
- Sharma, D.; Farrar, J.D. Adrenergic regulation of immune cell function and inflammation. Semin. Immunopathol. 2020, 42, 709–717. [Google Scholar] [CrossRef] [PubMed]
- Stolk, R.F.; van der Pasch, E.; Naumann, F.; Schouwstra, J.; Bressers, S.; van Herwaarden, A.E.; Gerretsen, J.; Schambergen, R.; Ruth, M.M.; van der Hoeven, J.G.; et al. Norepinephrine Dysregulates the Immune Response and Compromises Host Defense during Sepsis. Am. J. Respir. Crit. Care Med. 2020, 202, 830–842. [Google Scholar] [CrossRef] [PubMed]
- Lorton, D.; Bellinger, D.L. Molecular mechanisms underlying β-adrenergic receptor-mediated cross-talk between sympathetic neurons and immune cells. Int. J. Mol. Sci. 2015, 16, 5635–5665. [Google Scholar] [CrossRef] [PubMed] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Sarcopenic Subjects (N = 60) | |
|---|---|
| Gender (M:F) | 11:49 |
| Age (years) | 74.5 (71–79) |
| MMSE | 27.5 ± 0.3 |
| Handgrip strength (right) | 18.4 ± 6.6 |
| Handgrip strength (left) | 16.6 ± 6.6 |
| SPPB | 1 (0–1) |
| Sarcopenic Patients | NE | IL-10 | IL-18 | Barthel Index | SPPB Walking | SPPB Balance | SPPB Sit to Stand | SPPB Total | Tinetti | |
|---|---|---|---|---|---|---|---|---|---|---|
| NE | Rsp p value | 0.136 0.180 | −0.3 0.015 | 0.51 <0.0001 | 0.3 0.01 | 0.34 0.007 | 0.4 0.0001 | 0.38 0.0002 | 0.53 <0.0001 | |
| IL-10 | Rsp p value | 0.136 0.180 | −0.139 0.155 | 0.089 0.399 | 0.047 0.655 | 0.151 0.150 | 0.137 0.193 | 0.140 0.184 | 0.130 0.218 | |
| IL-18 | Rsp p value | −0.244 0.015 | −0.139 0.155 | −0.237 0.022 | −0.060 0.568 | −0.021 0.844 | −0.116 0.271 | −0.071 0.499 | −0.143 0.173 | |
| Barthel Index | Rsp p value | 0.51 <0.0001 | 0.089 0.399 | −0.237 0.022 | 0.503 <0.0001 | 0.494 <0.0001 | 0.404 0.0001 | 0.547 <0.0001 | 0.807 <0.0001 | |
| SPPB walking | Rsp p value | 0.3 0.01 | 0.047 0.655 | −0.060 0.568 | 0.503 <0.0001 | 0.574 <0.0001 | 0.474 <0.0001 | 0.763 <0.0001 | 0.572 <0.0001 | |
| SPPB balance | Rsp p value | 0.34 0.007 | 0.151 0.150 | −0.021 0.844 | 0.494 <0.0001 | 0.574 <0.0001 | 0.675 <0.0001 | 0.919 <0.0001 | 0.416 <0.0001 | |
| SPPB sit to stand | Rsp p value | 0.4 0.0001 | 0.137 0.193 | −0.116 0.271 | 0.404 0.0001 | 0.474 <0.0001 | 0.675 <0.0001 | 0.848 <0.0001 | 0.403 0.0001 | |
| SPPB Total | Rsp p value | 0.38 0.0002 | 0.140 0.184 | −0.071 0.499 | 0.547 <0.0001 | 0.763 <0.0001 | 0.919 <0.0001 | 0.848 <0.0001 | 0.528 <0.0001 | |
| Tinetti | Rsp p value | 0.53 <0.0001 | 0.130 0.218 | −0.143 0.173 | 0.807 <0.0001 | 0.572 <0.0001 | 0.416 <0.0001 | 0.403 0.0001 | 0.528 <0.0001 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Piancone, F.; La Rosa, F.; Marventano, I.; Hernis, A.; Miglioli, R.; Trecate, F.; Saresella, M.; Clerici, M. Modulation of Neuroendocrine and Immunological Biomarkers Following Rehabilitation in Sarcopenic Patients. Cells 2022, 11, 2477. https://doi.org/10.3390/cells11162477
Piancone F, La Rosa F, Marventano I, Hernis A, Miglioli R, Trecate F, Saresella M, Clerici M. Modulation of Neuroendocrine and Immunological Biomarkers Following Rehabilitation in Sarcopenic Patients. Cells. 2022; 11(16):2477. https://doi.org/10.3390/cells11162477
Chicago/Turabian StylePiancone, Federica, Francesca La Rosa, Ivana Marventano, Ambra Hernis, Rossella Miglioli, Fabio Trecate, Marina Saresella, and Mario Clerici. 2022. "Modulation of Neuroendocrine and Immunological Biomarkers Following Rehabilitation in Sarcopenic Patients" Cells 11, no. 16: 2477. https://doi.org/10.3390/cells11162477