
Current and Novel Therapeutic Approaches for Treatment of Diabetic Macular Edema

 , , and
, , and
Abstract
:1. Introduction
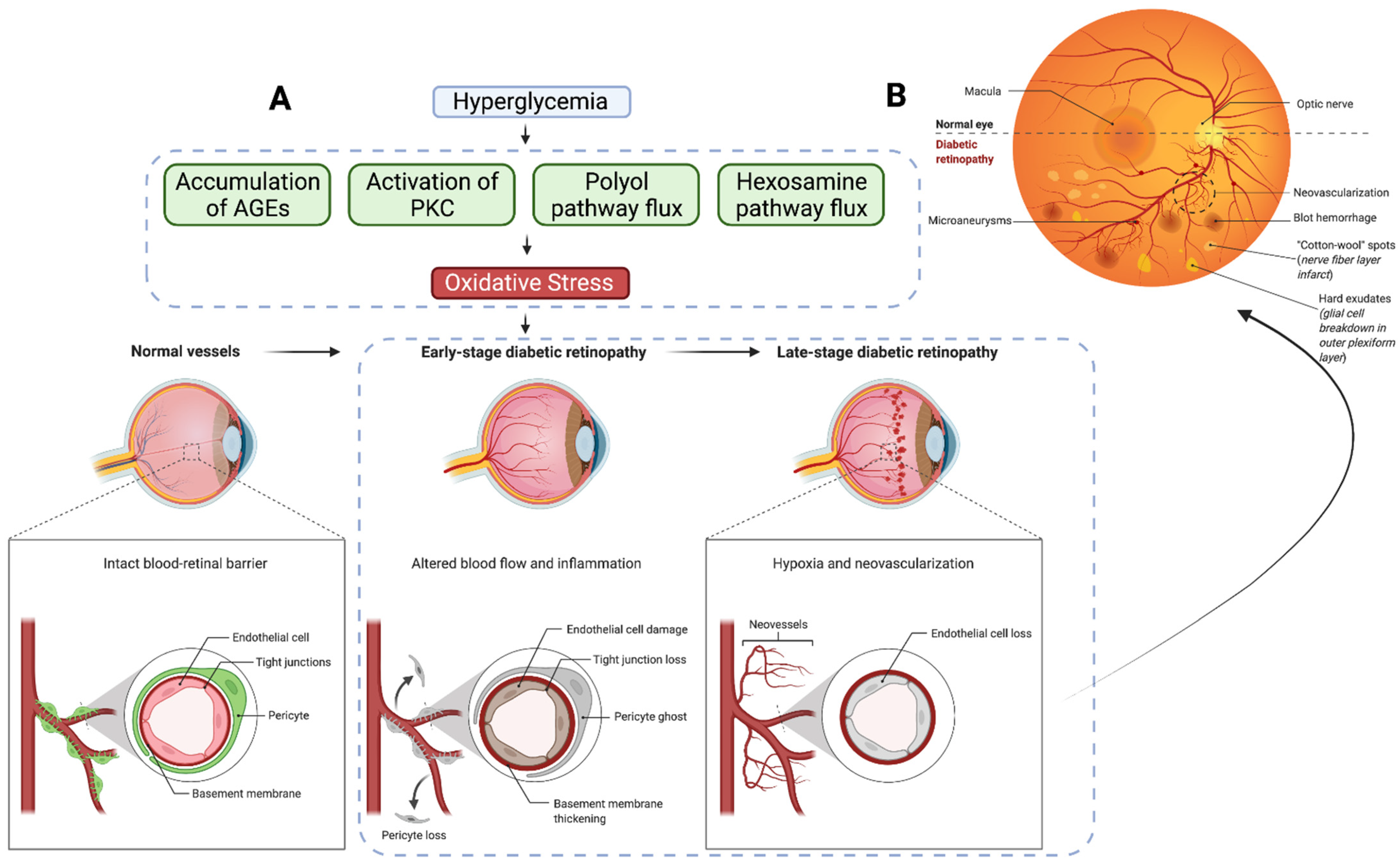
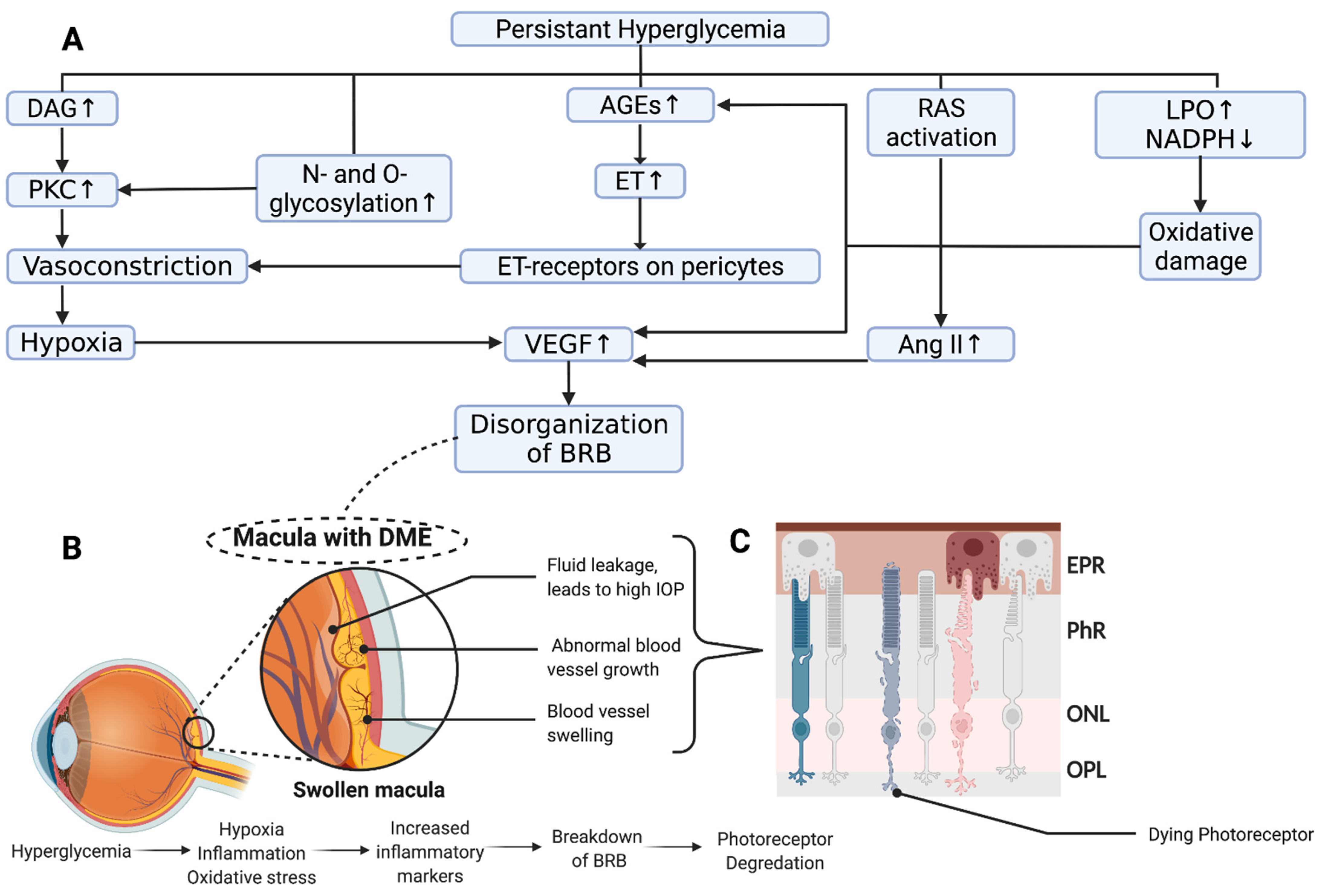
2. Overview of the Pathogenesis of Diabetic Macular Edema
3. Current Therapeutics
3.1. Primary Glycemic Control
3.2. Laser Photocoagulation
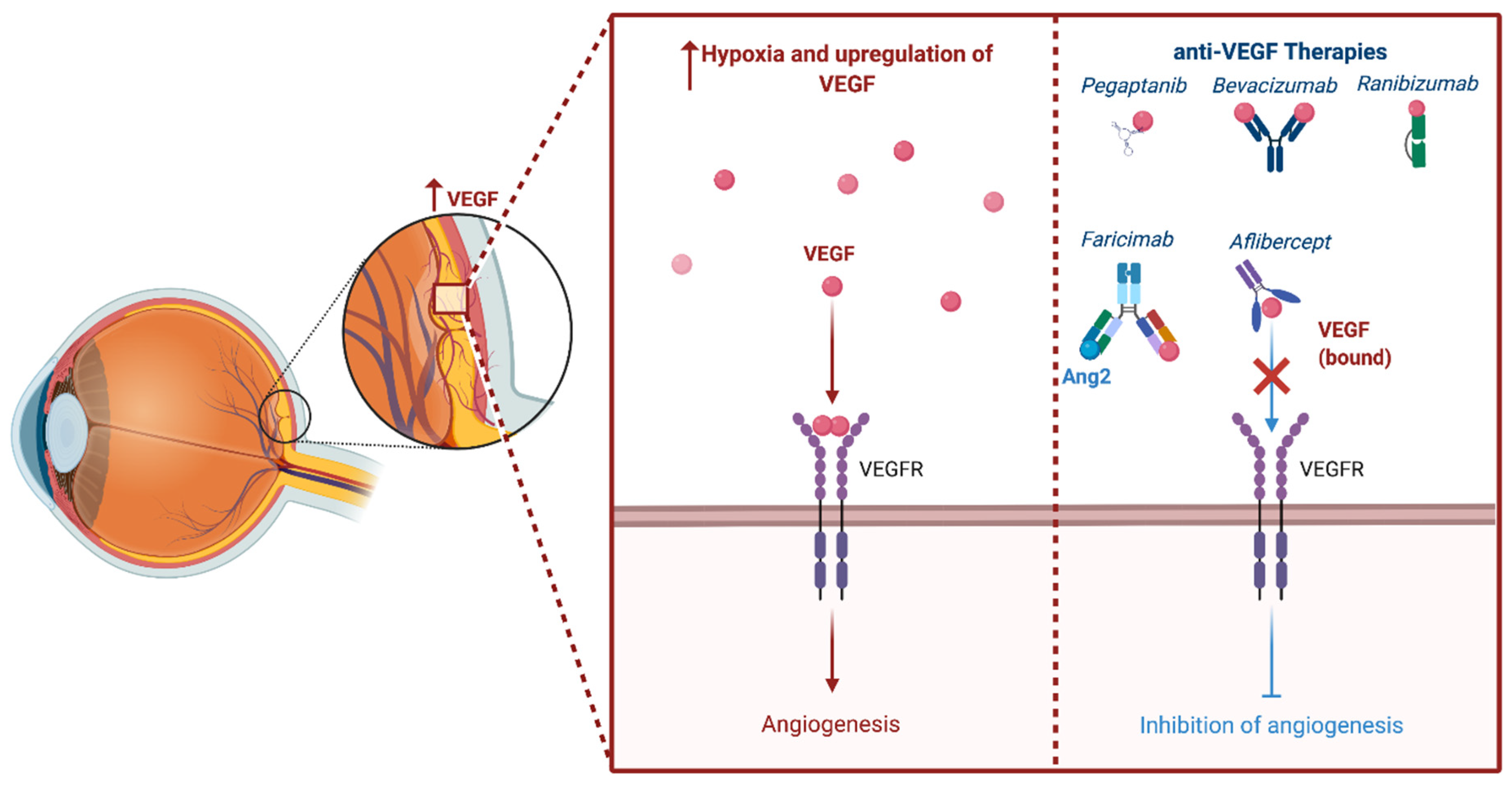
3.3. Anti-Vascular Endothelial Growth Factor


3.4. Anti-VEGF Biosimilars
3.5. Intravitreal Corticosteroids
3.6. Combinatorial Therapy
3.7. Pars Plana Vitrectomy
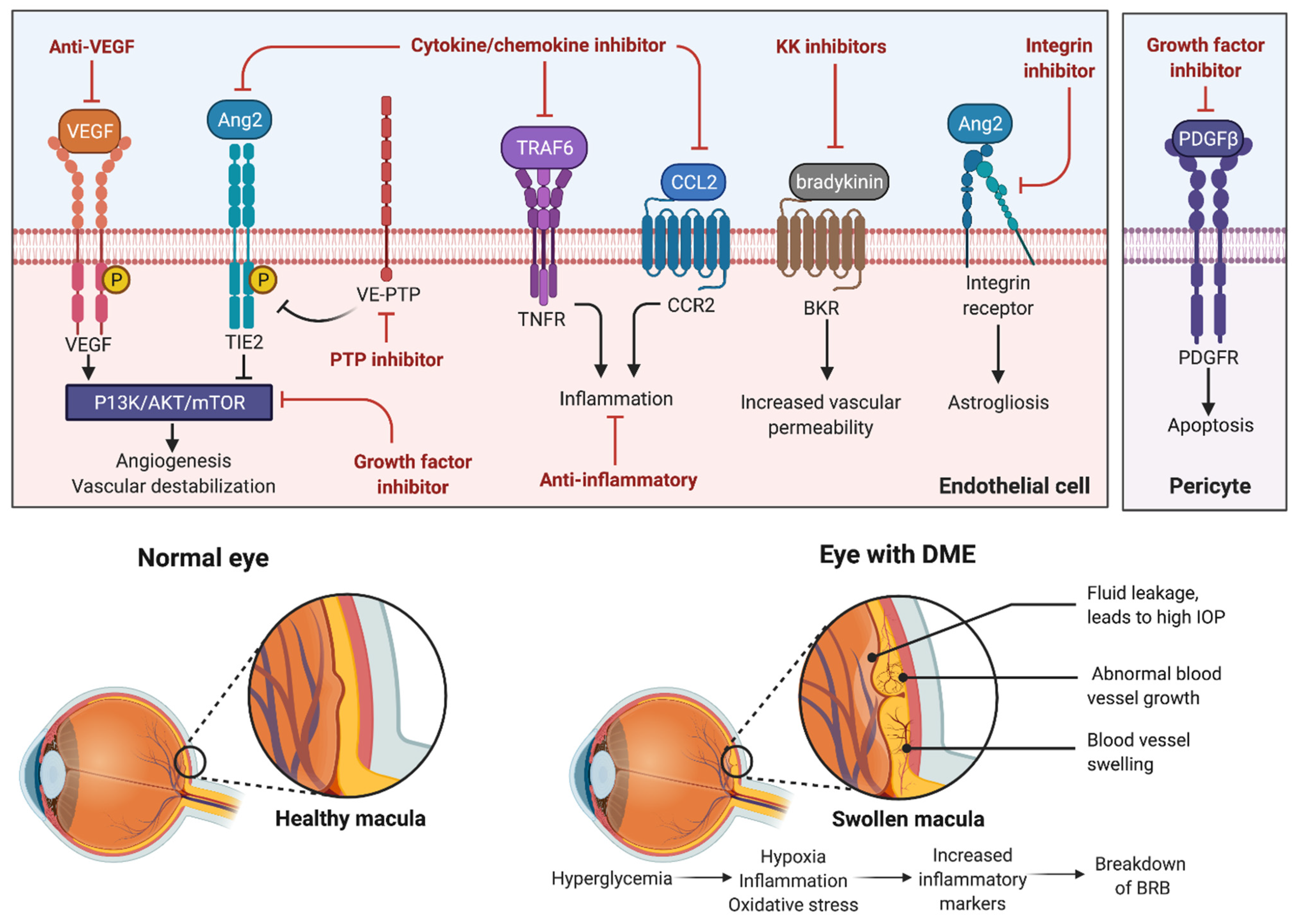
4. Novel Therapeutics
4.1. Cytokine Inhibitors
4.2. Adhesion Molecule Inhibitors
4.3. Kallikrein–Kinin (KK) System Inhibitors
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kumar, V.; Abbas, A.K.; Aster, J.C.; Perkins, J.A. Robbins Basic Pathology, 10th ed.; Elsevier: Philadelphia, PA, USA, 2018; p. xiv. 935p. [Google Scholar]
- GBD 2019 Blindness and Vision Impairment Collaborators on behalf of the Vision Loss Expert Group of the Global Burden of Disease Study. Causes of blindness and vision impairment in 2020 and trends over 30 years, and prevalence of avoidable blindness in relation to VISION 2020: The Right to Sight: An analysis for the Global Burden of Disease Study. Lancet Glob. Health 2021, 9, e144–e160. [Google Scholar] [CrossRef]
- Liu, R.; Ma, B.; Gao, Y.; Ma, B.; Liu, Y.; Qi, H. Tear Inflammatory Cytokines Analysis and Clinical Correlations in Diabetes and Nondiabetes With Dry Eye. Am. J. Ophthalmol. 2019, 200, 10–15. [Google Scholar] [CrossRef] [PubMed]
- Wiemer, N.G.; Dubbelman, M.; Kostense, P.J.; Ringens, P.J.; Polak, B.C. The influence of chronic diabetes mellitus on the thickness and the shape of the anterior and posterior surface of the cornea. Cornea 2007, 26, 1165–1170. [Google Scholar] [CrossRef] [PubMed]
- Spaide, R.F. Measurable Aspects of the Retinal Neurovascular Unit in Diabetes, Glaucoma, and Controls. Am. J. Ophthalmol. 2019, 207, 395–409. [Google Scholar] [CrossRef]
- Lu, W.L.; Shen, P.C.; Lee, C.H.; Su, Y.T.; Chen, L.M. High Risk of Early Cataracts in Young Type 1 Diabetes Group: A Nationwide Cohort Study. Int. J. Endocrinol. 2020, 2020, 8160256. [Google Scholar] [CrossRef]
- Giuliari, G.P.; Sadaka, A.; Chang, P.Y.; Cortez, R.T. Diabetic papillopathy: Current and new treatment options. Curr. Diabetes Rev. 2011, 7, 171–175. [Google Scholar] [CrossRef]
- Annabi, A.; Lasjaunias, P.; Lapresle, J. Paralysis of the 3d cranial nerves in diabetes and common oculomotor vascularization. J. Neurol. Sci. 1979, 41, 359–367. [Google Scholar] [CrossRef]
- Afroze, S.N.; Korlepara, R.; Rao, G.V.; Madala, J. Mucormycosis in a Diabetic Patient: A Case Report with an Insight into Its Pathophysiology. Contemp. Clin. Dent. 2017, 8, 662–666. [Google Scholar] [CrossRef]
- Ixcamey, M.; Palma, C. Diabetic macular edema. Dis. Mon. 2021, 67, 101138. [Google Scholar] [CrossRef]
- Holekamp, N.M. Overview of diabetic macular edema. Am. J. Manag. Care 2016, 22, s284–s291. [Google Scholar]
- Takamura, Y.; Ohkoshi, K.; Murata, T. New Strategies for Treatment of Diabetic Macular Edema. J. Ophthalmol. 2018, 2018, 4292154. [Google Scholar] [CrossRef] [Green Version]
- Haritoglou, C.; Maier, M.; Neubauer, A.S.; Augustin, A.J. Current concepts of pharmacotherapy of diabetic macular edema. Expert Opin. Pharmacother. 2020, 21, 467–475. [Google Scholar] [CrossRef] [PubMed]
- Klein, B.E. Overview of epidemiologic studies of diabetic retinopathy. Ophthalmic Epidemiol. 2007, 14, 179–183. [Google Scholar] [CrossRef]
- Miller, K.; Fortun, J.A. Diabetic Macular Edema: Current Understanding, Pharmacologic Treatment Options, and Developing Therapies. Asia-Pac. J. Ophthalmol. 2018, 7, 28–35. [Google Scholar] [CrossRef]
- Moldogazieva, N.T.; Mokhosoev, I.M.; Mel’nikova, T.I.; Porozov, Y.B.; Terentiev, A.A. Oxidative Stress and Advanced Lipoxidation and Glycation End Products (ALEs and AGEs) in Aging and Age-Related Diseases. Oxid. Med. Cell. Longev. 2019, 2019, 3085756. [Google Scholar] [CrossRef] [Green Version]
- Srivastava, S.P.; Shi, S.; Koya, D.; Kanasaki, K. Lipid mediators in diabetic nephropathy. Fibrogenesis Tissue Repair 2014, 7, 12. [Google Scholar] [CrossRef] [Green Version]
- Xu, H.; Czerwinski, P.; Hortmann, M.; Sohn, H.Y.; Forstermann, U.; Li, H. Protein kinase C alpha promotes angiogenic activity of human endothelial cells via induction of vascular endothelial growth factor. Cardiovasc. Res. 2008, 78, 349–355. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Williams, B.; Gallacher, B.; Patel, H.; Orme, C. Glucose-induced protein kinase C activation regulates vascular permeability factor mRNA expression and peptide production by human vascular smooth muscle cells in vitro. Diabetes 1997, 46, 1497–1503. [Google Scholar] [CrossRef] [PubMed]
- Campochiaro, P.A.; Akhlaq, A. Sustained suppression of VEGF for treatment of retinal/choroidal vascular diseases. Prog. Retin. Eye Res. 2021, 83, 100921. [Google Scholar] [CrossRef] [PubMed]
- Qaum, T.; Xu, Q.; Joussen, A.M.; Clemens, M.W.; Qin, W.; Miyamoto, K.; Hassessian, H.; Wiegand, S.J.; Rudge, J.; Yancopoulos, G.D.; et al. VEGF-initiated blood-retinal barrier breakdown in early diabetes. Investig. Ophthalmol. Vis. Sci. 2001, 42, 2408–2413. [Google Scholar]
- Bosquet, F.; Grimaldi, A. Role of the polyol pathway in the occurrence of degenerative complications of diabetes. Presse. Med. 1986, 15, 879–883. [Google Scholar] [PubMed]
- Hussain, N.; Adrian, T.E. Diabetic Neuropathy: Update on Pathophysiological Mechanism and the Possible Involvement of Glutamate Pathways. Curr. Diabetes Rev. 2017, 13, 488–497. [Google Scholar] [CrossRef]
- Shosha, E.; Fouda, A.Y.; Narayanan, S.P.; Caldwell, R.W.; Caldwell, R.B. Is the Arginase Pathway a Novel Therapeutic Avenue for Diabetic Retinopathy? J. Clin. Med. 2020, 9, 425. [Google Scholar] [CrossRef] [Green Version]
- Shosha, E.; Fouda, A.Y.; Lemtalsi, T.; Haigh, S.; Fulton, D.; Ibrahim, A.; Al-Shabrawey, M.; Caldwell, R.W.; Caldwell, R.B. Endothelial arginase 2 mediates retinal ischemia/reperfusion injury by inducing mitochondrial dysfunction. Mol. Metab. 2021, 53, 101273. [Google Scholar] [CrossRef] [PubMed]
- Atawia, R.T.; Bunch, K.L.; Fouda, A.Y.; Lemtalsi, T.; Eldahshan, W.; Xu, Z.; Saul, A.; Elmasry, K.; Al-Shabrawey, M.; Caldwell, R.B.; et al. Role of Arginase 2 in Murine Retinopathy Associated with Western Diet-Induced Obesity. J. Clin. Med. 2020, 9, 317. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alcazar, O.; Hernandez, L.F.; Nakayasu, E.S.; Nicora, C.D.; Ansong, C.; Muehlbauer, M.J.; Bain, J.R.; Myer, C.J.; Bhattacharya, S.K.; Buchwald, P.; et al. Parallel Multi-Omics in High-Risk Subjects for the Identification of Integrated Biomarker Signatures of Type 1 Diabetes. Biomolecules 2021, 11, 383. [Google Scholar] [CrossRef]
- Pannicke, T.; Iandiev, I.; Wurm, A.; Uckermann, O.; vom Hagen, F.; Reichenbach, A.; Wiedemann, P.; Hammes, H.P.; Bringmann, A. Diabetes alters osmotic swelling characteristics and membrane conductance of glial cells in rat retina. Diabetes 2006, 55, 633–639. [Google Scholar] [CrossRef] [Green Version]
- Bhagat, N.; Grigorian, R.A.; Tutela, A.; Zarbin, M.A. Diabetic macular edema: Pathogenesis and treatment. Surv. Ophthalmol. 2009, 54, 1–32. [Google Scholar] [CrossRef]
- Wat, N.; Wong, R.L.; Wong, I.Y. Associations between diabetic retinopathy and systemic risk factors. Hong Kong Med. J. 2016, 22, 589–599. [Google Scholar] [CrossRef] [Green Version]
- Diabetes Control and Complications Trial Research Group. The relationship of glycemic exposure (HbA1c) to the risk of development and progression of retinopathy in the diabetes control and complications trial. Diabetes 1995, 44, 968–983. [Google Scholar] [CrossRef]
- Nathan, D.M.; Group, D.E.R. The diabetes control and complications trial/epidemiology of diabetes interventions and complications study at 30 years: Overview. Diabetes Care 2014, 37, 9–16. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Diabetes Control and Complications Trial/Epidemiology of Diabetes Interventions and Complications Research Group. Retinopathy and nephropathy in patients with type 1 diabetes four years after a trial of intensive therapy. N. Engl. J. Med. 2000, 342, 381–389. [Google Scholar] [CrossRef] [Green Version]
- Diabetes Control and Complications Trial Research Group. Early worsening of diabetic retinopathy in the Diabetes Control and Complications Trial. Arch. Ophthalmol. 1998, 116, 874–886. [Google Scholar] [CrossRef] [PubMed]
- UK Prospective Diabetes Study (UKPDS) Group. Intensive blood-glucose control with sulphonylureas or insulin compared with conventional treatment and risk of complications in patients with type 2 diabetes (UKPDS 33). Lancet 1998, 352, 837–853. [Google Scholar] [CrossRef]
- Chatziralli, I.P. The Role of Glycemic Control and Variability in Diabetic Retinopathy. Diabetes Ther. 2018, 9, 431–434. [Google Scholar] [CrossRef] [Green Version]
- Pradeepa, R.; Anitha, B.; Mohan, V.; Ganesan, A.; Rema, M. Risk factors for diabetic retinopathy in a South Indian Type 2 diabetic population--the Chennai Urban Rural Epidemiology Study (CURES) Eye Study 4. Diabet. Med. 2008, 25, 536–542. [Google Scholar] [CrossRef]
- Group, A.S.; Group, A.E.S.; Chew, E.Y.; Ambrosius, W.T.; Davis, M.D.; Danis, R.P.; Gangaputra, S.; Greven, C.M.; Hubbard, L.; Esser, B.A.; et al. Effects of medical therapies on retinopathy progression in type 2 diabetes. N. Engl. J. Med. 2010, 363, 233–244. [Google Scholar] [CrossRef] [Green Version]
- Chew, E.Y.; Davis, M.D.; Danis, R.P.; Lovato, J.F.; Perdue, L.H.; Greven, C.; Genuth, S.; Goff, D.C.; Leiter, L.A.; Ismail-Beigi, F.; et al. The effects of medical management on the progression of diabetic retinopathy in persons with type 2 diabetes: The Action to Control Cardiovascular Risk in Diabetes (ACCORD) Eye Study. Ophthalmology 2014, 121, 2443–2451. [Google Scholar] [CrossRef] [Green Version]
- Hammes, H.P.; Welp, R.; Kempe, H.P.; Wagner, C.; Siegel, E.; Holl, R.W.; Mellitus, D.P.V.I.-G.B.C.N.D. Risk Factors for Retinopathy and DME in Type 2 Diabetes-Results from the German/Austrian DPV Database. PLoS ONE 2015, 10, e0132492. [Google Scholar] [CrossRef]
- Eleiwa, K.T.; Bayoumy, A.; Elhusseiny, M.A.; Gamil, K.; Sharawy, A. Longitudinal analysis of subfoveal choroidal thickness after panretinal laser photocoagulation in diabetic retinopathy using swept-source optical coherence tomography. Rom. J. Ophthalmol. 2020, 64, 285–291. [Google Scholar] [CrossRef]
- Photocoagulation for Diabetic Macular Edema. Early Treatment Diabetic Retinopathy Study report number 1. Early Treatment Diabetic Retinopathy Study research group. Arch. Ophthalmol. 1985, 103, 1796–1806. [Google Scholar] [CrossRef]
- Distefano, L.N.; Garcia-Arumi, J.; Martinez-Castillo, V.; Boixadera, A. Combination of Anti-VEGF and Laser Photocoagulation for Diabetic Macular Edema: A Review. J. Ophthalmol. 2017, 2017, 2407037. [Google Scholar] [CrossRef]
- Popa, D.; Gavris, M.; Horge, I.; Marian, N. Mechanisms of laser photocoagulation in diabetic retinopathy. Oftalmologia 2006, 50, 6–11. [Google Scholar]
- Midena, E.; Micera, A.; Frizziero, L.; Pilotto, E.; Esposito, G.; Bini, S. Sub-threshold micropulse laser treatment reduces inflammatory biomarkers in aqueous humour of diabetic patients with macular edema. Sci. Rep. 2019, 9, 10034. [Google Scholar] [CrossRef] [Green Version]
- Apple, D.J.; Goldberg, M.F.; Wyhinny, G. Histopathology and ultrastructure of the argon laser lesion in human retinal and choroidal vasculatures. Am. J. Ophthalmol. 1973, 75, 595–609. [Google Scholar] [CrossRef]
- Baker, C.W.; Glassman, A.R.; Beaulieu, W.T.; Antoszyk, A.N.; Browning, D.J.; Chalam, K.V.; Grover, S.; Jampol, L.M.; Jhaveri, C.D.; Melia, M.; et al. Effect of Initial Management With Aflibercept vs Laser Photocoagulation vs Observation on Vision Loss Among Patients With Diabetic Macular Edema Involving the Center of the Macula and Good Visual Acuity: A Randomized Clinical Trial. JAMA 2019, 321, 1880–1894. [Google Scholar] [CrossRef] [Green Version]
- Park, Y.G.; Kim, E.Y.; Roh, Y.J. Laser-based strategies to treat diabetic macular edema: History and new promising therapies. J. Ophthalmol. 2014, 2014, 769213. [Google Scholar] [CrossRef] [Green Version]
- Bandello, F.; Polito, A.; Del Borrello, M.; Zemella, N.; Isola, M. “Light” versus “classic” laser treatment for clinically significant diabetic macular oedema. Br. J. Ophthalmol. 2005, 89, 864–870. [Google Scholar] [CrossRef] [Green Version]
- Hirabayashi, K.; Kakihara, S.; Tanaka, M.; Shindo, T.; Murata, T. Investigation of the therapeutic mechanism of subthreshold micropulse laser irradiation in retina. Graefe’s Arch. Clin. Exp. Ophthalmol. 2020, 258, 1039–1047. [Google Scholar] [CrossRef]
- Lavinsky, D.; Cardillo, J.A.; Melo, L.A.S.; Dare, A.; Farah, M.E.; Belfort, R. Randomized Clinical Trial Evaluating mETDRS versus Normal or High-Density Micropulse Photocoagulation for Diabetic Macular Edema. Investig. Ophthalmol. Vis. Sci. 2011, 52, 4314–4323. [Google Scholar] [CrossRef]
- Luttrull, J.K.; Sinclair, S.H. Safety of transfoveal subthreshold diode micropulse laser for fovea-involving diabetic macular edema in eyes with good visual acuity. Retina 2014, 34, 2010–2020. [Google Scholar] [CrossRef] [Green Version]
- Valera-Cornejo, D.A.; García-Roa, M.; Quiroz-Mendoza, J.; Arias-Gómez, A.; Ramírez-Neria, P.; Villalpando-Gómez, Y.; Romero-Morales, V.; García-Franco, R. Micropulse laser in patients with refractory and treatment-naïve center–involved diabetic macular edema: Short terms visual and anatomic outcomes. Ther. Adv. Ophthalmol. 2021, 13, 251584142097911. [Google Scholar] [CrossRef]
- Park, Y.G.; Kim, J.R.; Kang, S.; Seifert, E.; Theisen-Kunde, D.; Brinkmann, R.; Roh, Y.-J. Safety and efficacy of selective retina therapy (SRT) for the treatment of diabetic macular edema in Korean patients. Graefe’s Arch. Clin. Exp. Ophthalmol. 2016, 254, 1703–1713. [Google Scholar] [CrossRef]
- Tode, J.; Richert, E.; Koinzer, S.; Klettner, A.; Von Der Burchard, C.; Brinkmann, R.; Lucius, R.; Roider, J. Selective Retina Therapy Reduces Bruch’s Membrane Thickness and Retinal Pigment Epithelium Pathology in Age-Related Macular Degeneration Mouse Models. Transl. Vis. Sci. Technol. 2019, 8, 11. [Google Scholar] [CrossRef] [Green Version]
- Roider, J.; Liew, S.H.M.; Klatt, C.; Elsner, H.; Poerksen, E.; Hillenkamp, J.; Brinkmann, R.; Birngruber, R. Selective retina therapy (SRT) for clinically significant diabetic macular edema. Graefe’s Arch. Clin. Exp. Ophthalmol. 2010, 248, 1263–1272. [Google Scholar] [CrossRef]
- Everett, L.A.; Paulus, Y.M. Laser Therapy in the Treatment of Diabetic Retinopathy and Diabetic Macular Edema. Curr. Diabetes Rep. 2021, 21, 35. [Google Scholar] [CrossRef]
- Inan, S.; Polat, O.; Yıgıt, S.; Inan, U.U. PASCAL laser platform produces less pain responses compared to conventional laser system during the panretinal photocoagulation: A randomized clinical trial. Afr. Health Sci. 2018, 18, 1010–1017. [Google Scholar] [CrossRef]
- Paulus, Y.M.; Kaur, K.; Egbert, P.R.; Blumenkranz, M.S.; Moshfeghi, D.M. Human histopathology of PASCAL laser burns. Eye 2013, 27, 995–996. [Google Scholar] [CrossRef] [Green Version]
- Jung, J.J.; Gallego-Pinazo1, R.; Lleó-Pérez, A.; Huz, J.I.; Barbazetto, I.A. NAVILAS Laser System Focal Laser Treatment for Diabetic Macular Edema—One Year Results of a Case Series. Open Ophthalmol. J. 2013, 7, 48–53. [Google Scholar] [CrossRef] [Green Version]
- Kozak, I.; Oster, S.F.; Cortes, M.A.; Dowell, D.; Hartmann, K.; Kim, J.S.; Freeman, W.R. Clinical evaluation and treatment accuracy in diabetic macular edema using navigated laser photocoagulator NAVILAS. Ophthalmology 2011, 118, 1119–1124. [Google Scholar] [CrossRef]
- Ogata, N.; Tombran-Tink, J.; Jo, N.; Mrazek, D.; Matsumura, M. Upregulation of pigment epithelium-derived factor after laser photocoagulation. Am. J. Ophthalmol. 2001, 132, 427–429. [Google Scholar] [CrossRef]
- Geudens, I.; Gerhardt, H. Coordinating cell behaviour during blood vessel formation. Development 2011, 138, 4569–4583. [Google Scholar] [CrossRef] [Green Version]
- Furino, C.; Boscia, F.; Reibaldi, M.; Alessio, G. Intravitreal Therapy for Diabetic Macular Edema: An Update. J. Ophthalmol. 2021, 2021, 6654168. [Google Scholar] [CrossRef]
- Massin, P.; Bandello, F.; Garweg, J.G.; Hansen, L.L.; Harding, S.P.; Larsen, M.; Mitchell, P.; Sharp, D.; Wolf-Schnurrbusch, U.E.; Gekkieva, M.; et al. Safety and efficacy of ranibizumab in diabetic macular edema (RESOLVE Study): A 12-month, randomized, controlled, double-masked, multicenter phase II study. Diabetes Care 2010, 33, 2399–2405. [Google Scholar] [CrossRef] [Green Version]
- Mitchell, P.; Bandello, F.; Schmidt-Erfurth, U.; Lang, G.E.; Massin, P.; Schlingemann, R.O.; Sutter, F.; Simader, C.; Burian, G.; Gerstner, O.; et al. The RESTORE study: Ranibizumab monotherapy or combined with laser versus laser monotherapy for diabetic macular edema. Ophthalmology 2011, 118, 615–625. [Google Scholar] [CrossRef] [Green Version]
- Nguyen, Q.D.; Brown, D.M.; Marcus, D.M.; Boyer, D.S.; Patel, S.; Feiner, L.; Gibson, A.; Sy, J.; Rundle, A.C.; Hopkins, J.J.; et al. Ranibizumab for diabetic macular edema: Results from 2 phase III randomized trials: RISE and RIDE. Ophthalmology 2012, 119, 789–801. [Google Scholar] [CrossRef]
- Brown, D.M.; Schmidt-Erfurth, U.; Do, D.V.; Holz, F.G.; Boyer, D.S.; Midena, E.; Heier, J.S.; Terasaki, H.; Kaiser, P.K.; Marcus, D.M.; et al. Intravitreal Aflibercept for Diabetic Macular Edema: 100-Week Results From the VISTA and VIVID Studies. Ophthalmology 2015, 122, 2044–2052. [Google Scholar] [CrossRef]
- Boyer, D.S.; Yoon, Y.H.; Belfort, R., Jr.; Bandello, F.; Maturi, R.K.; Augustin, A.J.; Li, X.Y.; Cui, H.; Hashad, Y.; Whitcup, S.M.; et al. Three-year, randomized, sham-controlled trial of dexamethasone intravitreal implant in patients with diabetic macular edema. Ophthalmology 2014, 121, 1904–1914. [Google Scholar] [CrossRef]
- Haritoglou, C.; Neubauer, A.S.; Kernt, M. Fluocinolone acetonide and its potential in the treatment of chronic diabetic macular edema. Clin. Ophthalmol. 2013, 7, 503–509. [Google Scholar] [CrossRef] [Green Version]
- Lien, S.; Lowman, H.B. Therapeutic Anti-VEGF Antibodies; Handbook of Experimental Pharmacology; Springer: Berlin/Heidelberg, Germany, 2008; pp. 131–150. [Google Scholar] [CrossRef]
- Cunningham, E.T.; Adamis, A.P.; Altaweel, M.; Aiello, L.P.; Bressler, N.M.; D’Amico, D.J.; Goldbaum, M.; Guyer, D.R.; Katz, B.; Patel, M.; et al. A phase II randomized double-masked trial of pegaptanib, an anti-vascular endothelial growth factor aptamer, for diabetic macular edema. Ophthalmology 2005, 112, 1747–1757. [Google Scholar] [CrossRef]
- Ishibashi, T.; Yuzawa, M.; Yoshimura, N.; Ohji, M.; Ishida, S.; Isogawa, N.; Esaka, E. Japan phase 3 study of pegaptanib sodium in patients with diabetic macular edema. Nippon Ganka Gakkai Zasshi 2014, 118, 773–782. [Google Scholar] [PubMed]
- Querques, G.; Bux, A.V.; Martinelli, D.; Iaculli, C.; Noci, N.D. Intravitreal pegaptanib sodium (Macugen) for diabetic macular oedema. Acta Ophthalmol. 2009, 87, 623–630. [Google Scholar] [CrossRef] [PubMed]
- Rinaldi, M.; Chiosi, F.; dell’Omo, R.; Romano, M.R.; Parmeggiani, F.; Semeraro, F.; Mastropasqua, R.; Costagliola, C. Intravitreal pegaptanib sodium (Macugen®) for treatment of diabetic macular oedema: A morphologic and functional study. Br. J. Clin. Pharmacol. 2012, 74, 940–946. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sivaprasad, S.; Browning, R.C.; Starita, C. An open-label, one-year, noncomparative study to evaluate the safety and tolerability of intravitreal pegaptanib sodium in patients with diabetic macular edema. Clin. Ophthalmol. 2014, 8, 1565–1571. [Google Scholar] [CrossRef] [Green Version]
- Kiire, C.A.; Morjaria, R.; Rudenko, A.; Fantato, A.; Smith, L.; Smith, A.; Chong, V. Intravitreal pegaptanib for the treatment of ischemic diabetic macular edema. Clin. Ophthalmol. 2015, 9, 2305–2311. [Google Scholar] [CrossRef] [Green Version]
- Wu, F.T.; Stefanini, M.O.; Mac Gabhann, F.; Kontos, C.D.; Annex, B.H.; Popel, A.S. A systems biology perspective on sVEGFR1: Its biological function, pathogenic role and therapeutic use. J. Cell. Mol. Med. 2010, 14, 528–552. [Google Scholar] [CrossRef]
- Failla, C.M.; Carbo, M.; Morea, V. Positive and Negative Regulation of Angiogenesis by Soluble Vascular Endothelial Growth Factor Receptor-1. Int. J. Mol. Sci. 2018, 19, 1306. [Google Scholar] [CrossRef] [Green Version]
- Michaelides, M.; Kaines, A.; Hamilton, R.D.; Fraser-Bell, S.; Rajendram, R.; Quhill, F.; Boos, C.J.; Xing, W.; Egan, C.; Peto, T.; et al. A prospective randomized trial of intravitreal bevacizumab or laser therapy in the management of diabetic macular edema (BOLT study) 12-month data: Report 2. Ophthalmology 2010, 117, 1078–1086.e1072. [Google Scholar] [CrossRef]
- Rajendram, R.; Fraser-Bell, S.; Kaines, A.; Michaelides, M.; Hamilton, R.D.; Esposti, S.D.; Peto, T.; Egan, C.; Bunce, C.; Leslie, R.D.; et al. A 2-year prospective randomized controlled trial of intravitreal bevacizumab or laser therapy (BOLT) in the management of diabetic macular edema: 24-month data: Report 3. Arch Ophthalmol. 2012, 130, 972–979. [Google Scholar] [CrossRef]
- Schmidt-Erfurth, U.; Garcia-Arumi, J.; Bandello, F.; Berg, K.; Chakravarthy, U.; Gerendas, B.S.; Jonas, J.; Larsen, M.; Tadayoni, R.; Loewenstein, A. Guidelines for the Management of Diabetic Macular Edema by the European Society of Retina Specialists (EURETINA). Ophthalmologica 2017, 237, 185–222. [Google Scholar] [CrossRef]
- Ranpura, V.; Hapani, S.; Chuang, J.; Wu, S. Risk of cardiac ischemia and arterial thromboembolic events with the angiogenesis inhibitor bevacizumab in cancer patients: A meta-analysis of randomized controlled trials. Acta Oncol. 2010, 49, 287–297. [Google Scholar] [CrossRef] [PubMed]
- Bakri, S.J.; Larson, T.A.; Edwards, A.O. Intraocular inflammation following intravitreal injection of bevacizumab. Graefe’s Arch. Clin. Exp. Ophthalmol. 2008, 246, 779–781. [Google Scholar] [CrossRef] [PubMed]
- Klettner, A.; Roider, J. Comparison of bevacizumab, ranibizumab, and pegaptanib in vitro: Efficiency and possible additional pathways. Investig. Ophthalmol. Vis. Sci. 2008, 49, 4523–4527. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brown, D.M.; Nguyen, Q.D.; Marcus, D.M.; Boyer, D.S.; Patel, S.; Feiner, L.; Schlottmann, P.G.; Rundle, A.C.; Zhang, J.; Rubio, R.G.; et al. Long-term outcomes of ranibizumab therapy for diabetic macular edema: The 36-month results from two phase III trials: RISE and RIDE. Ophthalmology 2013, 120, 2013–2022. [Google Scholar] [CrossRef] [Green Version]
- Pearce, I.; Banerjee, S.; Burton, B.J.; Chakravarthy, U.; Downey, L.; Gale, R.P.; Gibson, J.; Pagliarini, S.; Patel, J.; Sivaprasad, S.; et al. Ranibizumab 0.5 mg for Diabetic Macular Edema with Bimonthly Monitoring after a Phase of Initial Treatment: 18-Month, Multicenter, Phase IIIB RELIGHT Study. Ophthalmology 2015, 122, 1811–1819. [Google Scholar] [CrossRef]
- Bressler, S.B.; Almukhtar, T.; Bhorade, A.; Bressler, N.M.; Glassman, A.R.; Huang, S.S.; Jampol, L.M.; Kim, J.E.; Melia, M.; Investigators, D.R.C.R.N. Repeated intravitreous ranibizumab injections for diabetic macular edema and the risk of sustained elevation of intraocular pressure or the need for ocular hypotensive treatment. JAMA Ophthalmol. 2015, 133, 589–597. [Google Scholar] [CrossRef]
- Levin, A.M.; Chaya, C.J.; Kahook, M.Y.; Wirostko, B.M. Intraocular Pressure Elevation Following Intravitreal Anti-VEGF Injections: Short- and Long-term Considerations. J. Glaucoma 2021, 30, 1019–1026. [Google Scholar] [CrossRef]
- Korobelnik, J.F.; Do, D.V.; Schmidt-Erfurth, U.; Boyer, D.S.; Holz, F.G.; Heier, J.S.; Midena, E.; Kaiser, P.K.; Terasaki, H.; Marcus, D.M.; et al. Intravitreal aflibercept for diabetic macular edema. Ophthalmology 2014, 121, 2247–2254. [Google Scholar] [CrossRef]
- Wells, J.A.; Glassman, A.R.; Ayala, A.R.; Jampol, L.M.; Aiello, L.P.; Antoszyk, A.N.; Arnold-Bush, B.; Baker, C.W.; Bressler, N.M.; Browning, D.J.; et al. Aflibercept, bevacizumab, or ranibizumab for diabetic macular edema. N. Engl. J. Med. 2015, 372, 1193–1203. [Google Scholar] [CrossRef] [Green Version]
- Wells, J.A.; Glassman, A.R.; Ayala, A.R.; Jampol, L.M.; Bressler, N.M.; Bressler, S.B.; Brucker, A.J.; Ferris, F.L.; Hampton, G.R.; Jhaveri, C.; et al. Aflibercept, Bevacizumab, or Ranibizumab for Diabetic Macular Edema: Two-Year Results from a Comparative Effectiveness Randomized Clinical Trial. Ophthalmology 2016, 123, 1351–1359. [Google Scholar] [CrossRef] [Green Version]
- Chakraborty, D.; Sheth, J.U.; Boral, S.; Sinha, T.K. Off-label intravitreal brolucizumab for recalcitrant diabetic macular edema: A real-world case series. Am. J. Ophthalmol. Case Rep. 2021, 24, 101197. [Google Scholar] [CrossRef] [PubMed]
- Garweg, J.G. A Randomized, Double-Masked, Multicenter, Phase III Study Assessing the Efficacy and Safety of Brolucizumab versus Aflibercept in Patients with Visual Impairment due to Diabetic Macular Edema (KITE). Klin Monbl Augenheilkd 2020, 237, 450–453. [Google Scholar] [CrossRef] [PubMed]
- Brown, D.M.; Wolf, S.; Garweg, J.; Bandello, F.; Emanuelli, A.; Barranco, J.J.E.; Figueira, J.; Gupta, V.; Ngah, N.F.; Liew, G.; et al. Brolucizumab for the treatment of visual impairment due to diabetic macular edema: 52-week results from the KITE and KESTREL studies. Investig. Ophthalmol. Vis. Sci. 2021, 62, 1045. [Google Scholar]
- Brown, D.M.; Emanuelli, A.; Bandello, F.; Barranco, J.J.E.; Figueira, J.; Souied, E.; Wolf, S.; Gupta, V.; Ngah, N.F.; Liew, G.; et al. KESTREL and KITE: 52-week results from two Phase III pivotal trials of brolucizumab for diabetic macular edema. Am. J. Ophthalmol. 2022, 238, 157–172. [Google Scholar] [CrossRef]
- Mones, J.; Srivastava, S.K.; Jaffe, G.J.; Tadayoni, R.; Albini, T.A.; Kaiser, P.K.; Holz, F.G.; Korobelnik, J.F.; Kim, I.K.; Pruente, C.; et al. Risk of Inflammation, Retinal Vasculitis, and Retinal Occlusion-Related Events with Brolucizumab: Post Hoc Review of HAWK and HARRIER. Ophthalmology 2021, 128, 1050–1059. [Google Scholar] [CrossRef]
- Sharma, A.; Kumar, N.; Parachuri, N.; Sahyoun, J.Y.; Kuppermann, B.D.; Bandello, F. Brolucizumab horizontal line termination of 4 weekly trials horizontal line rebalancing the immunogenicity risk. Expert Opin. Biol. Ther. 2022, 22, 441–443. [Google Scholar] [CrossRef]
- Fayzullin, A.; Bakulina, A.; Mikaelyan, K.; Shekhter, A.; Guller, A. Implantable Drug Delivery Systems and Foreign Body Reaction: Traversing the Current Clinical Landscape. Bioengineering 2021, 8, 205. [Google Scholar] [CrossRef]
- Urias, E.A.; Urias, G.A.; Monickaraj, F.; McGuire, P.; Das, A. Novel therapeutic targets in diabetic macular edema: Beyond VEGF. Vis. Res. 2017, 139, 221–227. [Google Scholar] [CrossRef]
- Reibaldi, M.; Fallico, M.; Avitabile, T.; Marolo, P.; Parisi, G.; Cennamo, G.; Furino, C.; Lucenteforte, E.; Virgili, G. Frequency of intravitreal anti-vascular endothelial growth factor injections and risk of death: A systematic review with meta-analysis. Ophthalmol. Retin. 2021, 6, 369–376. [Google Scholar] [CrossRef]
- Sharma, A.; Hafeez Faridi, M.; Kumar, N.; Parachuri, N.; Sharma, R.; Kuppermann, B.D.; Bandello, F.; Loewenstein, A.; Regillo, C.D. Immunogenicity and efficacy after switching from original Ranibizumab to a Ranibizumab biosimilar: Real-world data. Eye 2020, 34, 1008–1009. [Google Scholar] [CrossRef]
- Kapur, M.; Nirula, S.; Naik, M.P. Future of anti-VEGF: Biosimilars and biobetters. Int. J. Retin. Vitr. 2022, 8, 2. [Google Scholar] [CrossRef]
- Sharma, S.; Khan, M.A.; Chaturvedi, A.; Group, R.-E.S.I. Real-Life Clinical Effectiveness of Razumab(R) (the World’s First Biosimilar of Ranibizumab) in Retinal Vein Occlusion: A Subgroup Analysis of the Pooled Retrospective RE-ENACT Study. Ophthalmologica 2019, 241, 24–31. [Google Scholar] [CrossRef]
- Verma, L.; Thulasidas, M.; Purohit, A.; Gupta, A.; Narula, R.; Talwar, D. Clinical efficacy and safety of Razumab(R) (CESAR) study: Our experience with the world’s first biosimilar Ranibizumab. Indian J. Ophthalmol. 2021, 69, 347–351. [Google Scholar] [CrossRef]
- Narayanan, R.; Hariprasad, S.M.; Sheth, J. Biosimilars for the Treatment of Retinal Diseases. Ophthalmic Surg. Lasers Imaging Retin. 2021, 52, 242–246. [Google Scholar] [CrossRef]
- Sharma, A.; Arunaprakash, J.; Das, A.; Nayaka, A.; Kumar, N.; Parachuri, N.; Kuppermann, B.D. Ranizurel safety evaluation in real-world -(RaSER) study. Am. J. Ophthalmol. Case Rep. 2022, 25, 101358. [Google Scholar] [CrossRef]
- Joussen, A.M.; Poulaki, V.; Le, M.L.; Koizumi, K.; Esser, C.; Janicki, H.; Schraermeyer, U.; Kociok, N.; Fauser, S.; Kirchhof, B.; et al. A central role for inflammation in the pathogenesis of diabetic retinopathy. FASEB J. 2004, 18, 1450–1452. [Google Scholar] [CrossRef]
- van der Wijk, A.E.; Hughes, J.M.; Klaassen, I.; Van Noorden, C.J.F.; Schlingemann, R.O. Is leukostasis a crucial step or epiphenomenon in the pathogenesis of diabetic retinopathy? J. Leukoc. Biol. 2017, 102, 993–1001. [Google Scholar] [CrossRef] [Green Version]
- Tamura, H.; Miyamoto, K.; Kiryu, J.; Miyahara, S.; Katsuta, H.; Hirose, F.; Musashi, K.; Yoshimura, N. Intravitreal injection of corticosteroid attenuates leukostasis and vascular leakage in experimental diabetic retina. Investig. Ophthalmol. Vis. Sci. 2005, 46, 1440–1444. [Google Scholar] [CrossRef]
- Tian, J.Y.; Dong, X.G.; Chen, N.; Xu, H.F.; Yuan, G.Q. Dexamethasone intensify the tight junctions in rat retinal vascular endothelial cells in vitro. Zhonghua Yan Ke Za Zhi 2007, 43, 646–650. [Google Scholar]
- Jonas, J.B.; Sofker, A. Intraocular injection of crystalline cortisone as adjunctive treatment of diabetic macular edema. Am. J. Ophthalmol. 2001, 132, 425–427. [Google Scholar] [CrossRef]
- Ciardella, A.P.; Klancnik, J.; Schiff, W.; Barile, G.; Langton, K.; Chang, S. Intravitreal triamcinolone for the treatment of refractory diabetic macular oedema with hard exudates: An optical coherence tomography study. Br. J. Ophthalmol. 2004, 88, 1131–1136. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lam, D.S.; Chan, C.K.; Tang, E.W.; Li, K.K.; Fan, D.S.; Chan, W.M. Intravitreal triamcinolone for diabetic macular oedema in Chinese patients: Six-month prospective longitudinal pilot study. Clin. Exp. Ophthalmol. 2004, 32, 569–572. [Google Scholar] [CrossRef]
- Massin, P.; Audren, F.; Haouchine, B.; Erginay, A.; Bergmann, J.F.; Benosman, R.; Caulin, C.; Gaudric, A. Intravitreal triamcinolone acetonide for diabetic diffuse macular edema: Preliminary results of a prospective controlled trial. Ophthalmology 2004, 111, 218–224. [Google Scholar] [CrossRef] [PubMed]
- Micelli Ferrari, T.; Sborgia, L.; Furino, C.; Cardascia, N.; Ferreri, P.; Besozzi, G.; Sborgia, C. Intravitreal triamcinolone acetonide: Valuation of retinal thickness changes measured by optical coherence tomography in diffuse diabetic macular edema. Eur. J. Ophthalmol. 2004, 14, 321–324. [Google Scholar] [CrossRef] [PubMed]
- Sutter, F.K.; Simpson, J.M.; Gillies, M.C. Intravitreal triamcinolone for diabetic macular edema that persists after laser treatment: Three-month efficacy and safety results of a prospective, randomized, double-masked, placebo-controlled clinical trial. Ophthalmology 2004, 111, 2044–2049. [Google Scholar] [CrossRef]
- Chieh, J.J.; Roth, D.B.; Liu, M.; Belmont, J.; Nelson, M.; Regillo, C.; Martidis, A. Intravitreal triamcinolone acetonide for diabetic macular edema. Retina 2005, 25, 828–834. [Google Scholar] [CrossRef]
- Er, H.; Yilmaz, H. Intravitreal cortisone injection for refractory diffuse diabetic macular edema. Ophthalmologica 2005, 219, 394–400. [Google Scholar] [CrossRef]
- Audren, F.; Erginay, A.; Haouchine, B.; Benosman, R.; Conrath, J.; Bergmann, J.F.; Gaudric, A.; Massin, P. Intravitreal triamcinolone acetonide for diffuse diabetic macular oedema: 6-month results of a prospective controlled trial. Acta Ophthalmol. Scand. 2006, 84, 624–630. [Google Scholar] [CrossRef]
- Dehghan, M.H.; Ahmadieh, H.; Ramezani, A.; Entezari, M.; Anisian, A. A randomized, placebo-controlled clinical trial of intravitreal triamcinolone for refractory diabetic macular edema. Int. Ophthalmol. 2008, 28, 7–17. [Google Scholar] [CrossRef]
- Diabetic Retinopathy Clinical Research, N.; Beck, R.W.; Edwards, A.R.; Aiello, L.P.; Bressler, N.M.; Ferris, F.; Glassman, A.R.; Hartnett, E.; Ip, M.S.; Kim, J.E.; et al. Three-year follow-up of a randomized trial comparing focal/grid photocoagulation and intravitreal triamcinolone for diabetic macular edema. Arch. Ophthalmol. 2009, 127, 245–251. [Google Scholar] [CrossRef] [Green Version]
- Diabetic Retinopathy Clinical Research, N.; Elman, M.J.; Aiello, L.P.; Beck, R.W.; Bressler, N.M.; Bressler, S.B.; Edwards, A.R.; Ferris, F.L., 3rd; Friedman, S.M.; Glassman, A.R.; et al. Randomized trial evaluating ranibizumab plus prompt or deferred laser or triamcinolone plus prompt laser for diabetic macular edema. Ophthalmology 2010, 117, 1064–1077.E1035. [Google Scholar] [CrossRef] [Green Version]
- Diabetic Retinopathy Clinical Research, N.; Chew, E.; Strauber, S.; Beck, R.; Aiello, L.P.; Antoszyk, A.; Bressler, N.; Browning, D.; Danis, R.; Fan, J.; et al. Randomized trial of peribulbar triamcinolone acetonide with and without focal photocoagulation for mild diabetic macular edema: A pilot study. Ophthalmology 2007, 114, 1190–1196. [Google Scholar] [CrossRef] [Green Version]
- Wykoff, C.C.; Khurana, R.N.; Lampen, S.I.R.; Noronha, G.; Brown, D.M.; Ou, W.C.; Sadda, S.R.; Group, H.S. Suprachoroidal Triamcinolone Acetonide for Diabetic Macular Edema: The HULK Trial. Ophthalmol. Retin. 2018, 2, 874–877. [Google Scholar] [CrossRef] [PubMed]
- Chawan-Saad, J.; Wu, M.; Wu, A.; Wu, L. Corticosteroids for Diabetic Macular Edema. Taiwan J. Ophthalmol. 2019, 9, 233–242. [Google Scholar] [CrossRef] [PubMed]
- Cunha-Vaz, J.; Ashton, P.; Iezzi, R.; Campochiaro, P.; Dugel, P.U.; Holz, F.G.; Weber, M.; Danis, R.P.; Kuppermann, B.D.; Bailey, C.; et al. Sustained delivery fluocinolone acetonide vitreous implants: Long-term benefit in patients with chronic diabetic macular edema. Ophthalmology 2014, 121, 1892–1903. [Google Scholar] [CrossRef] [Green Version]
- Barteselli, G.; Kozak, I.; El-Emam, S.; Chhablani, J.; Cortes, M.A.; Freeman, W.R. 12-month results of the standardised combination therapy for diabetic macular oedema: Intravitreal bevacizumab and navigated retinal photocoagulation. Br. J. Ophthalmol. 2014, 98, 1036–1041. [Google Scholar] [CrossRef] [Green Version]
- Do, D.V.; Nguyen, Q.D.; Khwaja, A.A.; Channa, R.; Sepah, Y.J.; Sophie, R.; Hafiz, G.; Campochiaro, P.A.; Group, R.-S. Ranibizumab for edema of the macula in diabetes study: 3-year outcomes and the need for prolonged frequent treatment. JAMA Ophthalmol. 2013, 131, 139–145. [Google Scholar] [CrossRef]
- Luttrull, J.K.; Sramek, C.; Palanker, D.; Spink, C.J.; Musch, D.C. Long-term safety, high-resolution imaging, and tissue temperature modeling of subvisible diode micropulse photocoagulation for retinovascular macular edema. Retina 2012, 32, 375–386. [Google Scholar] [CrossRef]
- Inagaki, K.; Hamada, M.; Ohkoshi, K. Minimally invasive laser treatment combined with intravitreal injection of anti-vascular endothelial growth factor for diabetic macular oedema. Sci. Rep. 2019, 9, 7585. [Google Scholar] [CrossRef]
- Thinda, S.; Patel, A.P.; Hunter, A.A.; Moshiri, A.; Morse, L.S. Combination therapy with subthreshold diode laser micropulse photocoagulation and intravitreal anti-vascular endothelial growth factor injections for diabetic macular edema. Investig. Ophthalmol. Vis. Sci. 2014, 55, 6363. [Google Scholar]
- Kang, S.W.; Sa, H.S.; Cho, H.Y.; Kim, J.I. Macular grid photocoagulation after intravitreal triamcinolone acetonide for diffuse diabetic macular edema. Arch. Ophthalmol. 2006, 124, 653–658. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lam, D.S.; Chan, C.K.; Mohamed, S.; Lai, T.Y.; Lee, V.Y.; Liu, D.T.; Li, K.K.; Li, P.S.; Shanmugam, M.P. Intravitreal triamcinolone plus sequential grid laser versus triamcinolone or laser alone for treating diabetic macular edema: Six-month outcomes. Ophthalmology 2007, 114, 2162–2167. [Google Scholar] [CrossRef] [PubMed]
- Gillies, M.C.; McAllister, I.L.; Zhu, M.; Wong, W.; Louis, D.; Arnold, J.J.; Wong, T.Y. Intravitreal triamcinolone prior to laser treatment of diabetic macular edema: 24-month results of a randomized controlled trial. Ophthalmology 2011, 118, 866–872. [Google Scholar] [CrossRef] [PubMed]
- Callanan, D.G.; Gupta, S.; Boyer, D.S.; Ciulla, T.A.; Singer, M.A.; Kuppermann, B.D.; Liu, C.C.; Li, X.Y.; Hollander, D.A.; Schiffman, R.M.; et al. Dexamethasone intravitreal implant in combination with laser photocoagulation for the treatment of diffuse diabetic macular edema. Ophthalmology 2013, 120, 1843–1851. [Google Scholar] [CrossRef]
- Maturi, R.K.; Bleau, L.; Saunders, J.; Mubasher, M.; Stewart, M.W. A 12-Month, Single-Masked, Randomized Controlled Study of Eyes with Persistent Diabetic Macular Edema after Multiple Anti-Vegf Injections to Assess the Efficacy of the Dexamethasone-Delayed Delivery System as an Adjunct to Bevacizumab Compared with Continued Bevacizumab Monotherapy. Retina 2015, 35, 1604–1614. [Google Scholar] [CrossRef]
- Singer, M.A.; Sheth, V.; Mansour, S.E.; Coughlin, B.; Gonzalez, V.H. Three-Year Safety and Efficacy of the 0.19-mg Fluocinolone Acetonide Intravitreal Implant for Diabetic Macular Edema: The PALADIN Study. Ophthalmology 2022, 129, 605–613. [Google Scholar] [CrossRef]
- Nasrallah, F.P.; Jalkh, A.E.; Van Coppenolle, F.; Kado, M.; Trempe, C.L.; McMeel, J.W.; Schepens, C.L. The role of the vitreous in diabetic macular edema. Ophthalmology 1988, 95, 1335–1339. [Google Scholar] [CrossRef]
- Flikier, S.; Wu, A.; Wu, L. Revisiting pars plana vitrectomy in the primary treatment of diabetic macular edema in the era of pharmacological treatment. Taiwan J. Ophthalmol. 2019, 9, 224–232. [Google Scholar] [CrossRef]
- Stitt, A.W.; Moore, J.E.; Sharkey, J.A.; Murphy, G.; Simpson, D.A.; Bucala, R.; Vlassara, H.; Archer, D.B. Advanced glycation end products in vitreous: Structural and functional implications for diabetic vitreopathy. Investig. Ophthalmol. Vis. Sci. 1998, 39, 2517–2523. [Google Scholar]
- Kang, Y.K.; Park, H.S.; Park, D.H.; Shin, J.P. Incidence and treatment outcomes of secondary epiretinal membrane following intravitreal injection for diabetic macular edema. Sci. Rep. 2020, 10, 528. [Google Scholar] [CrossRef]
- Barbazetto, I.A.; Liang, J.; Chang, S.; Zheng, L.; Spector, A.; Dillon, J.P. Oxygen tension in the rabbit lens and vitreous before and after vitrectomy. Exp. Eye Res. 2004, 78, 917–924. [Google Scholar] [CrossRef] [PubMed]
- Diabetic Retinopathy Clinical Research Network Writing Committee; Haller, J.A.; Qin, H.; Apte, R.S.; Beck, R.R.; Bressler, N.M.; Browning, D.J.; Danis, R.P.; Glassman, A.R.; Googe, J.M.; et al. Vitrectomy outcomes in eyes with diabetic macular edema and vitreomacular traction. Ophthalmology 2010, 117, 1087–1093.E1083. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thomas, D.; Bunce, C.; Moorman, C.; Laidlaw, D.A. A randomised controlled feasibility trial of vitrectomy versus laser for diabetic macular oedema. Br. J. Ophthalmol. 2005, 89, 81–86. [Google Scholar] [CrossRef]
- Simunovic, M.P.; Hunyor, A.P.; Ho, I.V. Vitrectomy for diabetic macular edema: A systematic review and meta-analysis. Can. J. Ophthalmol. 2014, 49, 188–195. [Google Scholar] [CrossRef] [PubMed]
- Rush, R.B.; Rush, S.W. Pars Plana Vitrectomy with Internal Limiting Membrane Peeling for Treatment-Naïve Diabetic Macular Edema: A Prospective, Uncontrolled Pilot Study. Clin. Ophthalmol. 2021, 15, 2619–2624. [Google Scholar] [CrossRef] [PubMed]
- Erie, J.C.; Raecker, M.E.; Baratz, K.H.; Schleck, C.D.; Robertson, D.M. Risk of retinal detachment after cataract extraction, 1980-2004: A population-based study. Trans. Am. Ophthalmol. Soc. 2006, 104, 167–175. [Google Scholar]
- Mason, M.; Lashkari, K.; Ugarte, S.; Christie, L.-A.; Rodrigues, G.; Lopez, F.J. Profile of vascular permeability factors in aqueous humor of diabetic macular edema. Investig. Ophthalmol. Vis. Sci. 2021, 62, 1068. [Google Scholar]
- Watanabe, D.; Suzuma, K.; Suzuma, I.; Ohashi, H.; Ojima, T.; Kurimoto, M.; Murakami, T.; Kimura, T.; Takagi, H. Vitreous levels of angiopoietin 2 and vascular endothelial growth factor in patients with proliferative diabetic retinopathy. Am. J. Ophthalmol. 2005, 139, 476–481. [Google Scholar] [CrossRef]
- Khan, M.; Aziz, A.A.; Shafi, N.A.; Abbas, T.; Khanani, A.M. Targeting Angiopoietin in Retinal Vascular Diseases: A Literature Review and Summary of Clinical Trials Involving Faricimab. Cells 2020, 9, 1869. [Google Scholar] [CrossRef]
- Sharma, A.; Kumar, N.; Kuppermann, B.D.; Bandello, F.; Loewenstein, A. Understanding biosimilars and its regulatory aspects across the globe: An ophthalmology perspective. Br. J. Ophthalmol. 2020, 104, 2–7. [Google Scholar] [CrossRef]
- Sahni, J.; Patel, S.S.; Dugel, P.U.; Khanani, A.M.; Jhaveri, C.D.; Wykoff, C.C.; Hershberger, V.S.; Pauly-Evers, M.; Sadikhov, S.; Szczesny, P.; et al. Simultaneous Inhibition of Angiopoietin-2 and Vascular Endothelial Growth Factor-A with Faricimab in Diabetic Macular Edema: BOULEVARD Phase 2 Randomized Trial. Ophthalmology 2019, 126, 1155–1170. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Eter, N.; Singh, R.P.; Abreu, F.; Asik, K.; Basu, K.; Baumal, C.; Chang, A.; Csaky, K.G.; Haskova, Z.; Lin, H.; et al. YOSEMITE and RHINE: Phase 3 Randomized Clinical Trials of Faricimab for Diabetic Macular Edema: Study Design and Rationale. Ophthalmol. Sci. 2022, 2, 100111. [Google Scholar] [CrossRef]
- Wykoff, C.C.; Abreu, F.; Adamis, A.P.; Basu, K.; Eichenbaum, D.A.; Haskova, Z.; Lin, H.; Loewenstein, A.; Mohan, S.; Pearce, I.A.; et al. Efficacy, durability, and safety of intravitreal faricimab with extended dosing up to every 16 weeks in patients with diabetic macular oedema (YOSEMITE and RHINE): Two randomised, double-masked, phase 3 trials. Lancet 2022, 399, 741–755. [Google Scholar] [CrossRef]
- Shaw, L.T.; Mackin, A.; Shah, R.; Jain, S.; Jain, P.; Nayak, R.; Hariprasad, S.M. Risuteganib-a novel integrin inhibitor for the treatment of non-exudative (dry) age-related macular degeneration and diabetic macular edema. Expert Opin. Investig. Drugs 2020, 29, 547–554. [Google Scholar] [CrossRef] [PubMed]
- Hu, T.T.; Vanhove, M.; Porcu, M.; Van Hove, I.; Van Bergen, T.; Jonckx, B.; Barbeaux, P.; Vermassen, E.; Feyen, J.H.M. The potent small molecule integrin antagonist THR-687 is a promising next-generation therapy for retinal vascular disorders. Exp. Eye Res. 2019, 180, 43–52. [Google Scholar] [CrossRef]
- Khanani, A.M.; Patel, S.S.; Gonzalez, V.H.; Moon, S.J.; Jaffe, G.J.; Wells, J.A.; Kozma, P.; Dugel, P.U.; Maturi, R.K. Phase 1 Study of THR-687, a Novel, Highly Potent Integrin Antagonist for the Treatment of Diabetic Macular Edema. Ophthalmol. Sci. 2021, 1, 100040. [Google Scholar] [CrossRef]
- Iwaki, T.; Castellino, F.J. Plasma levels of bradykinin are suppressed in factor XII-deficient mice. Thromb. Haemost. 2006, 95, 1003–1010. [Google Scholar] [CrossRef]
- Ma, J.X.; Song, Q.; Hatcher, H.C.; Crouch, R.K.; Chao, L.; Chao, J. Expression and cellular localization of the kallikrein-kinin system in human ocular tissues. Exp. Eye Res. 1996, 63, 19–26. [Google Scholar] [CrossRef] [PubMed]
- Phipps, J.A.; Clermont, A.C.; Sinha, S.; Chilcote, T.J.; Bursell, S.E.; Feener, E.P. Plasma kallikrein mediates angiotensin II type 1 receptor-stimulated retinal vascular permeability. Hypertension 2009, 53, 175–181. [Google Scholar] [CrossRef] [Green Version]
- Kita, T.; Clermont, A.C.; Murugesan, N.; Zhou, Q.; Fujisawa, K.; Ishibashi, T.; Aiello, L.P.; Feener, E.P. Plasma Kallikrein-Kinin System as a VEGF-Independent Mediator of Diabetic Macular Edema. Diabetes 2015, 64, 3588–3599. [Google Scholar] [CrossRef] [Green Version]
- Clermont, A.; Chilcote, T.J.; Kita, T.; Liu, J.; Riva, P.; Sinha, S.; Feener, E.P. Plasma kallikrein mediates retinal vascular dysfunction and induces retinal thickening in diabetic rats. Diabetes 2011, 60, 1590–1598. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Clermont, A.; Murugesan, N.; Zhou, Q.; Kita, T.; Robson, P.A.; Rushbrooke, L.J.; Evans, D.M.; Aiello, L.P.; Feener, E.P. Plasma Kallikrein Mediates Vascular Endothelial Growth Factor-Induced Retinal Dysfunction and Thickening. Investig. Ophthalmol. Vis. Sci. 2016, 57, 2390–2399. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sun, J.K.; Maturi, R.K.; Boyer, D.S.; Wells, J.A.; Gonzalez, V.H.; Tansley, R.; Hernandez, H.; Maetzel, A.; Feener, E.P.; Aiello, L.P. One-Time Intravitreal Injection of KVD001, a Plasma Kallikrein Inhibitor, in Patients with Central-Involved Diabetic Macular Edema and Reduced Vision: An Open-Label Phase 1B Study. Ophthalmol. Retin. 2019, 3, 1107–1109. [Google Scholar] [CrossRef] [PubMed]
- Bhatwadekar, A.D.; Kansara, V.S.; Ciulla, T.A. Investigational plasma kallikrein inhibitors for the treatment of diabetic macular edema: An expert assessment. Expert Opin. Investig. Drugs 2020, 29, 237–244. [Google Scholar] [CrossRef] [PubMed]
- Dugel, P.U.; Khanani, A.M.; Berger, B.B.; Patel, S.; Fineman, M.; Jaffe, G.J.; Kozma-Wiebe, P.; Heier, J. Phase 1 Dose-Escalation Study of Plasma Kallikrein Inhibitor THR-149 for the Treatment of Diabetic Macular Edema. Transl. Vis. Sci. Technol. 2021, 10, 28. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| BCVA (ETDRS Letters) | CRT (µm) | |||||||
|---|---|---|---|---|---|---|---|---|
| Study [Ref.] | Regimen | No. of Patients | Study Design | Group | Baseline | Change | Baseline | Change |
| RESOLVE [65] | Rani 0.3 mg | Control: 49 | Phase II, double-masked, randomized, sham- controlled, multicenter | Rani | 60.2 (9.9) | 7.8 (7.7) | 455.4 (114.2) | −194.2 (135.1) |
| Rani 0.5 mg | Total: 151 | Sham | 61.1 (9.0) | −0.1 (9.8) | 448.9 (102.8) | −48.4 (153.4) | ||
| RESTORE [66] | Rani 0.5 mg | Control: 111 | Phase III, double-masked, randomized, laser- controlled, multicenter | Rani + sham | N.A. | 6.1 (6.3) | N.A. | −118.7 (115.1) |
| Rani 0.5 mg + laser | Total: 345 | Rani + laser | N.A. | 5.9 (7.9) | N.A. | −128.3 (114.3) | ||
| Laser + sham | N.A. | 0.8 (8.6) | N.A. | −61.3 (132.3) | ||||
| RISE [67] | Rani 0.3 mg | Control: 127 | Phase III, randomized, sham-controlled, multicenter | Rani 0.3 mg | 54.7 (12.6) | 12.5 | 474.5 (174.8) | −250.6 |
| Rani 0.5 mg | Total: 377 | Rani 0.5 mg | 56.9 (11.6) | 11.9 | 463.8 (144.0) | −253.1 | ||
| Sham | 57.2 (11.1) | 2.6 | 467.3 (152.0) | −133.4 | ||||
| RIDE [67] | Rani 0.3 mg | Phase III, randomized, sham-controlled, multicenter | Rani 0.3 mg | 57.5 (11.6) | 10.9 | 482.6 (149.3) | −259.8 | |
| Rani 0.5 mg | Rani 0.5 mg | 56.9 (11.8) | 12.0 | 463.8 (175.5) | −270.7 | |||
| Sham | 57.3 (11.2) | 2.3 | 447.4 (154.4) | −125.8 | ||||
| VISTA [68] | Laser | Laser: 154 | Phase III, double-masked, randomized, active- controlled, multicenter | Aflib. 2q4 | 58.9 (10.8) | 11.5 | 485 (157) | −191.4 |
| Aflib. 2q4 | Aflib: 307 | Aflib. 2q8 | 59.4 (10.9) | 11.7 | 479 (154) | −191.1 | ||
| Aflib. 2q8 | Laser | 59.7 (10.9) | 6.3 | 483 (153) | −83.9 | |||
| VIVID [68] | Laser | Laser: 133 | Phase III, double-masked, randomized, active- controlled, multicenter | Aflib. 2q4 | 60.8 (10.7) | 11.8 | 502 (144) | −211.8 |
| Aflib. 2q4 | Aflib: 271 | Aflib. 2q8 | 58.8 (11.2) | 10.6 | 518 (147) | −195.8 | ||
| Aflib. 2q8 | Laser | 60.8 (10.6) | 5.5 | 540 (152) | −85.7 | |||
| MEAD [69] | DEX 0.7 mg | Control: 350 | Phase III, masked, randomized, sham-controlled, multicenter | DEX 0.35 mg | 56.1 (9.9) | 18.4% a | 463.0 (157.1) | −107.9 (135.8) |
| DEX 0.35 mg | Total: 1048 | DEX 0.7 mg | 55.5 (9.7) | 22.2% a | 466.8 (159.5) | −111.6 (134.1) | ||
| Sham | 56.9 (8.7) | 12.0% a | 460.9 (132.6) | −41.9 (116.0) | ||||
| FAME [70] | IFSR 0.2 µg/day | Control: 185 | Double-masked, randomized, sham- controlled, parallel-group, multicenter | IFSR 0.2 µg | 53.3 (12.7) | p = 0.019 | 460.8 (160.0) | p ≤ 0.003 |
| IFSR 0.5 µg/day | Total: 953 | IFSR 0.5 µg | 52.9 (12.2) | p = 0.015 | 460.8 (160.0) | p ≤ 0.003 | ||
| Sham | 54.7 (11.3) | N.A. | 460.8 (160.0) | N.A. | ||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chauhan, M.Z.; Rather, P.A.; Samarah, S.M.; Elhusseiny, A.M.; Sallam, A.B. Current and Novel Therapeutic Approaches for Treatment of Diabetic Macular Edema. Cells 2022, 11, 1950. https://doi.org/10.3390/cells11121950
Chauhan MZ, Rather PA, Samarah SM, Elhusseiny AM, Sallam AB. Current and Novel Therapeutic Approaches for Treatment of Diabetic Macular Edema. Cells. 2022; 11(12):1950. https://doi.org/10.3390/cells11121950
Chicago/Turabian StyleChauhan, Muhammad Z., Peyton A. Rather, Sajida M. Samarah, Abdelrahman M. Elhusseiny, and Ahmed B. Sallam. 2022. "Current and Novel Therapeutic Approaches for Treatment of Diabetic Macular Edema" Cells 11, no. 12: 1950. https://doi.org/10.3390/cells11121950