
Neutrophil Maturation, Reactivity and Granularity Research Parameters to Characterize and Differentiate Convalescent Patients from Active SARS-CoV-2 Infection

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Participants
2.2. Morphological and New Sysmex Parameters Connected with Neutrophils
2.3. Statistical Analysis
3. Results
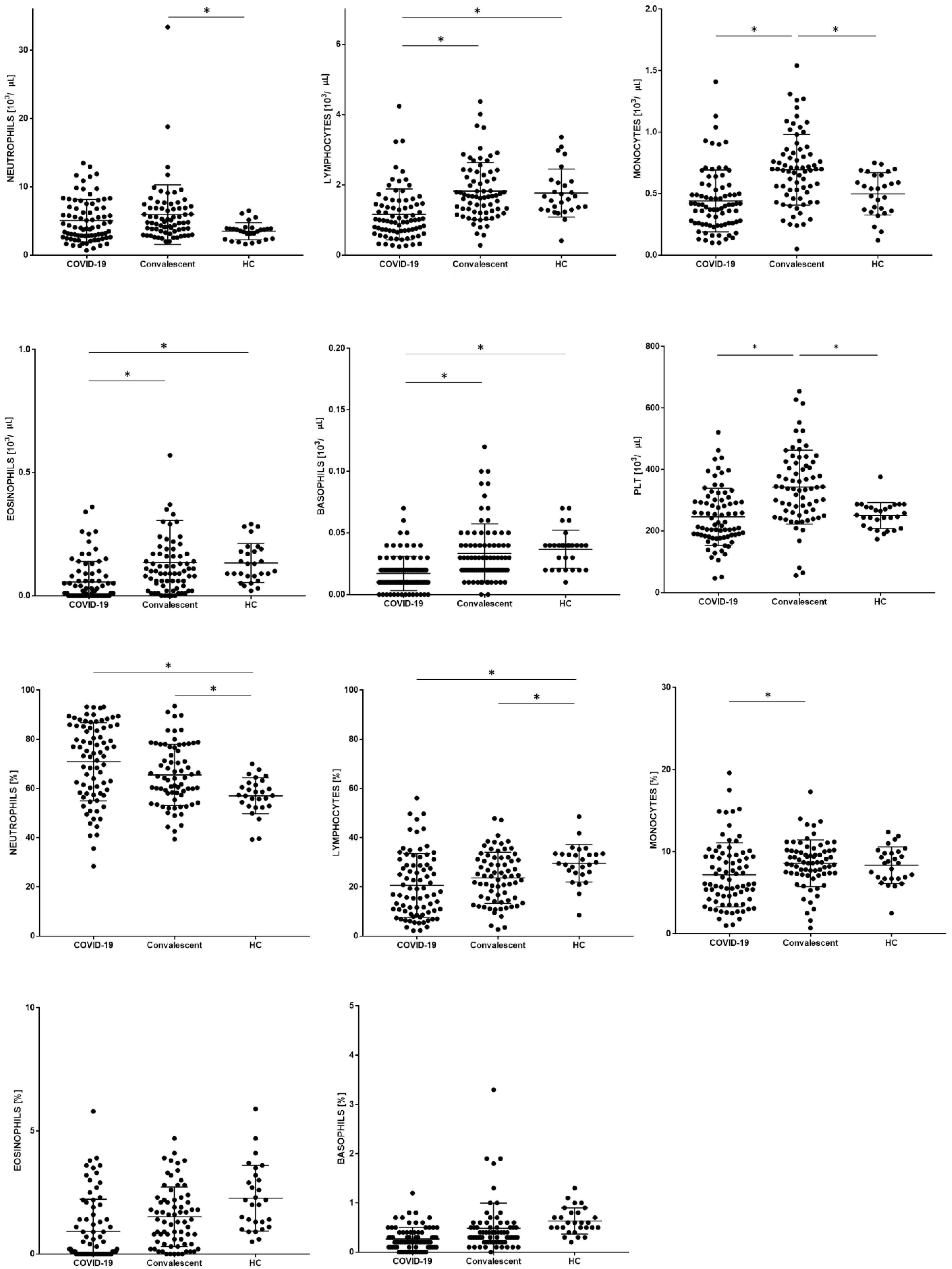
3.1. Patients Characteristic with Basic Leukocytes Subpopulation
3.2. New Neutrophil Parameters
3.3. Morphological and New Sysmex Parameters Depending on the Severity of COVID-19
4. Discussion
4.1. Role of Neutrophils in SARS-CoV-2 Infection
4.2. NEUT-RI
4.3. NEUT-GI
4.4. NE-FSC
4.5. NE-WX, NE-WY, NE-WZ
4.6. Combining Morphological Parameters with New Neutrophil Parameters
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A

References
- Baloch, S.; Baloch, M.A.; Zheng, T.; Pei, X. The Coronavirus Disease 2019 (COVID-19) Pandemic. Tohoku J. Exp. Med. 2020, 250, 271–278. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Peng, M. Outbreak of COVID-19: An emerging global pandemic threat. Biomed. Pharmacother. 2020, 129, 110499. [Google Scholar] [CrossRef] [PubMed]
- Pereyra, D.; Heber, S.; Jilma, B.; Zoufaly, A.; Assinger, A. Routine haematological parameters in COVID-19 prognosis. Lancet Haematol. 2020, 7, e709. [Google Scholar] [CrossRef]
- Taj, S.; Kashif, A.; Arzinda Fatima, S.; Imran, S.; Lone, A.; Ahmed, Q. Role of hematological parameters in the stratification of COVID-19 disease severity. Ann. Med. Surg. 2021, 62, 68–72. [Google Scholar] [CrossRef]
- Rutkowska, E.; Kwiecien, I.; Kulik, K.; Chelstowska, B.; Klos, K.; Rzepecki, P.; Chcialowski, A. Usefulness of the New Hematological Parameter: Reactive Lymphocytes RE-LYMP with Flow Cytometry Markers of Inflammation in COVID-19. Cells 2021, 10, 82. [Google Scholar] [CrossRef]
- Rutkowska, E.; Kwiecien, I.; Zabicka, M.; Maliborski, A.; Raniszewska, A.; Klos, K.; Urbanska, W.; Klajnowicz, I.; Rzepecki, P.; Chcialowski, A. Cytokines and Leukocytes Subpopulations Profile in SARS-CoV-2 Patients Depending on the CT Score Severity. Viruses 2021, 13, 880. [Google Scholar] [CrossRef]
- Rezaei, M.; Marjani, M.; Mahmoudi, S.; Mortaz, E.; Mansouri, D. Dynamic Changes of Lymphocyte Subsets in the Course of COVID-19. Int. Arch. Allergy Immunol. 2021, 182, 254–262. [Google Scholar] [CrossRef]
- Kwiecien, I.; Rutkowska, E.; Klos, K.; Wiesik-Szewczyk, E.; Jahnz-Rozyk, K.; Rzepecki, P.; Chcialowski, A. Maturation of T and B Lymphocytes in the Assessment of the Immune Status in COVID-19 Patients. Cells 2020, 9, 2615. [Google Scholar] [CrossRef]
- Zheng, M.; Gao, Y.; Wang, G.; Song, G.; Liu, S.; Sun, D.; Xu, Y.; Tian, Z. Functional exhaustion of antiviral lymphocytes in COVID-19 patients. Cell. Mol. Immunol. 2020, 17, 533–535. [Google Scholar] [CrossRef] [Green Version]
- Huang, I.; Pranata, R. Lymphopenia in severe coronavirus disease-2019 (COVID-19): Systematic review and meta-analysis. J. Intensive Care 2020, 8, 36. [Google Scholar] [CrossRef]
- Izcovich, A.; Ragusa, M.A.; Tortosa, F.; Lavena Marzio, M.A.; Agnoletti, C.; Bengolea, A.; Ceirano, A.; Espinosa, F.; Saavedra, E.; Sanguine, V.; et al. Prognostic factors for severity and mortality in patients infected with COVID-19: A systematic review. PLoS ONE 2020, 15, e0241955. [Google Scholar] [CrossRef]
- Barnes, B.J.; Adrover, J.M.; Baxter-Stoltzfus, A.; Borczuk, A.; Cools-Lartigue, J.; Crawford, J.M.; Dassler-Plenker, J.; Guerci, P.; Huynh, C.; Knight, J.S.; et al. Targeting potential drivers of COVID-19: Neutrophil extracellular traps. J. Exp. Med. 2020, 217, e20200652. [Google Scholar] [CrossRef]
- Tomar, B.; Anders, H.J.; Desai, J.; Mulay, S.R. Neutrophils and Neutrophil Extracellular Traps Drive Necroinflammation in COVID-19. Cells 2020, 9, 1383. [Google Scholar] [CrossRef]
- Liew, P.X.; Kubes, P. The Neutrophil’s Role During Health and Disease. Physiol. Rev. 2019, 99, 1223–1248. [Google Scholar] [CrossRef] [PubMed]
- Simadibrata, D.M.; Calvin, J.; Wijaya, A.D.; Ibrahim, N.A.A. Neutrophil-to-lymphocyte ratio on admission to predict the severity and mortality of COVID-19 patients: A meta-analysis. Am. J. Emerg. Med. 2021, 42, 60–69. [Google Scholar] [CrossRef] [PubMed]
- Henry, B.; Cheruiyot, I.; Vikse, J.; Mutua, V.; Kipkorir, V.; Benoit, J.; Plebani, M.; Bragazzi, N.; Lippi, G. Lymphopenia and neutrophilia at admission predicts severity and mortality in patients with COVID-19: A meta-analysis. Acta Bio-Med. Atenei Parm. 2020, 91, e2020008. [Google Scholar] [CrossRef]
- Wang, J.; Li, Q.; Yin, Y.; Zhang, Y.; Cao, Y.; Lin, X.; Huang, L.; Hoffmann, D.; Lu, M.; Qiu, Y. Excessive Neutrophils and Neutrophil Extracellular Traps in COVID-19. Front. Immunol. 2020, 11, 2063. [Google Scholar] [CrossRef] [PubMed]
- Parackova, Z.; Zentsova, I.; Bloomfield, M.; Vrabcova, P.; Smetanova, J.; Klocperk, A.; Meseznikov, G.; Casas Mendez, L.F.; Vymazal, T.; Sediva, A. Disharmonic Inflammatory Signatures in COVID-19: Augmented Neutrophils’ but Impaired Monocytes’ and Dendritic Cells’ Responsiveness. Cells 2020, 9, 2206. [Google Scholar] [CrossRef]
- Mohamed, M.M.A.; El-Shimy, I.A.; Hadi, M.A. Neutrophil Elastase Inhibitors: A potential prophylactic treatment option for SARS-CoV-2-induced respiratory complications? Crit. Care 2020, 24, 311. [Google Scholar] [CrossRef] [PubMed]
- Radermecker, C.; Detrembleur, N.; Guiot, J.; Cavalier, E.; Henket, M.; d’Emal, C.; Vanwinge, C.; Cataldo, D.; Oury, C.; Delvenne, P.; et al. Neutrophil extracellular traps infiltrate the lung airway, interstitial, and vascular compartments in severe COVID-19. J. Exp. Med. 2020, 217, e20201012. [Google Scholar] [CrossRef]
- Thierry, A.R.; Roch, B. Neutrophil Extracellular Traps and By-Products Play a Key Role in COVID-19: Pathogenesis, Risk Factors, and Therapy. J. Clin. Med. 2020, 9, 2942. [Google Scholar] [CrossRef] [PubMed]
- Henriot, I.; Launay, E.; Boubaya, M.; Cremet, L.; Illiaquer, M.; Caillon, H.; Desjonqueres, A.; Gillet, B.; Bene, M.C.; Eveillard, M. New parameters on the hematology analyzer XN-10 (SysmexTM) allow to distinguish childhood bacterial and viral infections. Int. J. Lab. Hematol. 2017, 39, 14–20. [Google Scholar] [CrossRef]
- Sysmex, E.G. Novel Haematological Parameters for Rapidly Monitoring the Immune System Response; Sysmex Europe GmbH: Norderstedt, Germany, 2017; Volume 27, pp. 1–5. [Google Scholar]
- Martens, R.J.H.; van Adrichem, A.J.; Mattheij, N.J.A.; Brouwer, C.G.; van Twist, D.J.L.; Broerse, J.; Magro-Checa, C.; van Dongen, C.M.P.; Mostard, R.L.M.; Ramiro, S.; et al. Hemocytometric characteristics of COVID-19 patients with and without cytokine Storm syndrome on the Sysmex XN-10 hematology analyzer. Clin. Chem. Lab. Med. 2020, 59, 783–793. [Google Scholar] [CrossRef]
- Dennison, D.; Al Khabori, M.; Al Mamari, S.; Aurelio, A.; Al Hinai, H.; Al Maamari, K.; Alshekaili, J.; Al Khadouri, G. Circulating activated neutrophils in COVID-19: An independent predictor for mechanical ventilation and death. Int. J. Infect. Dis. IJID Off. Publ. Int. Soc. Infect. Dis. 2021, 106, 155–159. [Google Scholar] [CrossRef]
- Flisiak, R.; Horban, A.; Jaroszewicz, J.; Kozielewicz, D.; Mastalerz-Migas, A.; Owczuk, R.; Parczewski, M.; Pawlowska, M.; Piekarska, A.; Simon, K.; et al. Management of SARS-CoV-2 infection: Recommendations of the Polish Association of Epidemiologists and Infectiologists as of 26 April 2021. Pol. Arch. Intern. Med. 2021, 131, 487–496. [Google Scholar] [CrossRef] [PubMed]
- Zeeshan-Haider, R.; Urrechaga, E.; Uddin-Ujjan, I.; Sultan-Shamsi, T. Neutrophil Scattering Data Driven Pre-Microscopic Flagging of Acute Leukemic Cases. Rev. Investig. Clin. Organo Hosp. Enferm. Nutr. 2020, 72, 37–45. [Google Scholar] [CrossRef] [Green Version]
- Maenhout, T.M.; Marcelis, L. Immature granulocyte count in peripheral blood by the Sysmex haematology XN series compared to microscopic differentiation. J. Clin. Pathol. 2014, 67, 648–650. [Google Scholar] [CrossRef]
- Ustyantseva, M.; Khokhlova, O.I.; Agadzhanyan, V. Innovative Technologies in the evaluation of the neutrophil functional activity in sepsis. Sysmex J. Int. 2019, 29, 8–13. [Google Scholar]
- Cornet, E.; Boubaya, M.; Troussard, X. Contribution of the new XN-1000 parameters NEUT-RI and NEUT-WY for managing patients with immature granulocytes. Int. J. Lab. Hematol. 2015, 37, e123–e126. [Google Scholar] [CrossRef]
- Rosales, C.; Demaurex, N.; Lowell, C.A.; Uribe-Querol, E. Neutrophils: Their Role in Innate and Adaptive Immunity. J. Immunol. Res. 2016, 2016, 1469780. [Google Scholar] [CrossRef]
- Roberts, R.E.; Hallett, M.B. Neutrophil Cell Shape Change: Mechanism and Signalling during Cell Spreading and Phagocytosis. Int. J. Mol. Sci. 2019, 20, 1383. [Google Scholar] [CrossRef] [Green Version]
- Vorobjeva, N.V.; Pinegin, B.V. Neutrophil extracellular traps: Mechanisms of formation and role in health and disease. Biochem. Biokhimiia 2014, 79, 1286–1296. [Google Scholar] [CrossRef] [PubMed]
- Borges, L.; Pithon-Curi, T.C.; Curi, R.; Hatanaka, E. COVID-19 and Neutrophils: The Relationship between Hyperinflammation and Neutrophil Extracellular Traps. Mediat. Inflamm. 2020, 2020, 8829674. [Google Scholar] [CrossRef] [PubMed]
- Zuo, Y.; Yalavarthi, S.; Shi, H.; Gockman, K.; Zuo, M.; Madison, J.A.; Blair, C.; Weber, A.; Barnes, B.J.; Egeblad, M.; et al. Neutrophil extracellular traps in COVID-19. JCI Insight 2020, 5, e138999. [Google Scholar] [CrossRef] [Green Version]
- Xie, X.; Shi, Q.; Wu, P.; Zhang, X.; Kambara, H.; Su, J.; Yu, H.; Park, S.Y.; Guo, R.; Ren, Q.; et al. Single-cell transcriptome profiling reveals neutrophil heterogeneity in homeostasis and infection. Nat. Immunol. 2020, 21, 1119–1133. [Google Scholar] [CrossRef] [PubMed]
- Evrard, M.; Kwok, I.W.H.; Chong, S.Z.; Teng, K.W.W.; Becht, E.; Chen, J.; Sieow, J.L.; Penny, H.L.; Ching, G.C.; Devi, S.; et al. Developmental Analysis of Bone Marrow Neutrophils Reveals Populations Specialized in Expansion, Trafficking, and Effector Functions. Immunity 2018, 48, 364–379.e368. [Google Scholar] [CrossRef] [Green Version]
- Adrover, J.M.; Aroca-Crevillen, A.; Crainiciuc, G.; Ostos, F.; Rojas-Vega, Y.; Rubio-Ponce, A.; Cilloniz, C.; Bonzon-Kulichenko, E.; Calvo, E.; Rico, D.; et al. Programmed ‘disarming’ of the neutrophil proteome reduces the magnitude of inflammation. Nat. Immunol. 2020, 21, 135–144. [Google Scholar] [CrossRef]
- Silvin, A.; Chapuis, N.; Dunsmore, G.; Goubet, A.G.; Dubuisson, A.; Derosa, L.; Almire, C.; Henon, C.; Kosmider, O.; Droin, N.; et al. Elevated Calprotectin and Abnormal Myeloid Cell Subsets Discriminate Severe from Mild COVID-19. Cell 2020, 182, 1401–1418.e1418. [Google Scholar] [CrossRef] [PubMed]
- Katahira, Y.; Higuchi, H.; Matsushita, H.; Yahata, T.; Yamamoto, Y.; Koike, R.; Ando, K.; Sato, K.; Imadome, K.I.; Kotani, A. Increased Granulopoiesis in the Bone Marrow following Epstein-Barr Virus Infection. Sci. Rep. 2019, 9, 13445. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mayadas, T.N.; Cullere, X.; Lowell, C.A. The multifaceted functions of neutrophils. Annu. Rev. Pathol. 2014, 9, 181–218. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Colom, B.; Bodkin, J.V.; Beyrau, M.; Woodfin, A.; Ody, C.; Rourke, C.; Chavakis, T.; Brohi, K.; Imhof, B.A.; Nourshargh, S. Leukotriene B4-Neutrophil Elastase Axis Drives Neutrophil Reverse Transendothelial Cell Migration In Vivo. Immunity 2015, 42, 1075–1086. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Giamarellos-Bourboulis, E.J.; Netea, M.G.; Rovina, N.; Akinosoglou, K.; Antoniadou, A.; Antonakos, N.; Damoraki, G.; Gkavogianni, T.; Adami, M.E.; Katsaounou, P.; et al. Complex Immune Dysregulation in COVID-19 Patients with Severe Respiratory Failure. Cell Host Microbe 2020, 27, 992–1000.e1003. [Google Scholar] [CrossRef] [PubMed]
- Meizlish, M.L.; Pine, A.B.; Bishai, J.D.; Goshua, G.; Nadelmann, E.R.; Simonov, M.; Chang, C.H.; Zhang, H.; Shallow, M.; Bahel, P.; et al. A neutrophil activation signature predicts critical illness and mortality in COVID-19. medRxiv Prepr. Serv. Health Sci. 2020, 5, 1164–1177. [Google Scholar] [CrossRef]
- Aschenbrenner, A.C.; Mouktaroudi, M.; Kramer, B.; Oestreich, M.; Antonakos, N.; Nuesch-Germano, M.; Gkizeli, K.; Bonaguro, L.; Reusch, N.; Bassler, K.; et al. Disease severity-specific neutrophil signatures in blood transcriptomes stratify COVID-19 patients. Genome Med. 2021, 13, 7. [Google Scholar] [CrossRef] [PubMed]
- Chua, R.L.; Lukassen, S.; Trump, S.; Hennig, B.P.; Wendisch, D.; Pott, F.; Debnath, O.; Thurmann, L.; Kurth, F.; Volker, M.T.; et al. COVID-19 severity correlates with airway epithelium-immune cell interactions identified by single-cell analysis. Nat. Biotechnol. 2020, 38, 970–979. [Google Scholar] [CrossRef] [PubMed]
- Liao, M.; Liu, Y.; Yuan, J.; Wen, Y.; Xu, G.; Zhao, J.; Cheng, L.; Li, J.; Wang, X.; Wang, F.; et al. Single-cell landscape of bronchoalveolar immune cells in patients with COVID-19. Nat. Med. 2020, 26, 842–844. [Google Scholar] [CrossRef]
- Wu, J.; Li, J.; Zhu, G.; Zhang, Y.; Bi, Z.; Yu, Y.; Huang, B.; Fu, S.; Tan, Y.; Sun, J.; et al. Clinical Features of Maintenance Hemodialysis Patients with 2019 Novel Coronavirus-Infected Pneumonia in Wuhan, China. Clin. J. Am. Soc. Nephrol. 2020, 15, 1139–1145. [Google Scholar] [CrossRef]
- Guan, W.J.; Ni, Z.Y.; Hu, Y.; Liang, W.H.; Ou, C.Q.; He, J.X.; Liu, L.; Shan, H.; Lei, C.L.; Hui, D.S.C.; et al. Clinical Characteristics of Coronavirus Disease 2019 in China. N. Engl. J. Med. 2020, 382, 1708–1720. [Google Scholar] [CrossRef]
- Schulte-Schrepping, J.; Reusch, N.; Paclik, D.; Bassler, K.; Schlickeiser, S.; Zhang, B.; Kramer, B.; Krammer, T.; Brumhard, S.; Bonaguro, L.; et al. Severe COVID-19 Is Marked by a Dysregulated Myeloid Cell Compartment. Cell 2020, 182, 1419–1440.e1423. [Google Scholar] [CrossRef]
- Zini, G.; Bellesi, S.; Ramundo, F.; d’Onofrio, G. Morphological anomalies of circulating blood cells in COVID-19. Am. J. Hematol. 2020, 95, 870–872. [Google Scholar] [CrossRef] [Green Version]
- Middleton, E.A.; He, X.Y.; Denorme, F.; Campbell, R.A.; Ng, D.; Salvatore, S.P.; Mostyka, M.; Baxter-Stoltzfus, A.; Borczuk, A.C.; Loda, M.; et al. Neutrophil extracellular traps contribute to immunothrombosis in COVID-19 acute respiratory distress syndrome. Blood 2020, 136, 1169–1179. [Google Scholar] [CrossRef] [PubMed]
- Buoro, S.; Seghezzi, M.; Vavassori, M.; Dominoni, P.; Apassiti Esposito, S.; Manenti, B.; Mecca, T.; Marchesi, G.; Castellucci, E.; Azzara, G.; et al. Clinical significance of cell population data (CPD) on Sysmex XN-9000 in septic patients with our without liver impairment. Ann. Transl. Med. 2016, 4, 418. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shekhar, R.; Pai, S.; Srinivasan, V.K.; Srinivas, V.; Adhikary, R.; Bhavana, M.V. Alterations in leucocyte cell population data in bacteraemia: A study from a tertiary care hospital in India. Int. J. Lab. Hematol. 2021, 43, e1–e4. [Google Scholar] [CrossRef]
- Lee, A.J.; Kim, S.G. Mean cell volumes of neutrophils and monocytes are promising markers of sepsis in elderly patients. Blood Res. 2013, 48, 193–197. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Witter, A.R.; Okunnu, B.M.; Berg, R.E. The Essential Role of Neutrophils during Infection with the Intracellular Bacterial Pathogen Listeria monocytogenes. J. Immunol. 2016, 197, 1557–1565. [Google Scholar] [CrossRef] [Green Version]
- Urrechaga, E. Reviewing the value of leukocytes cell population data (CPD) in the management of sepsis. Ann. Transl. Med. 2020, 8, 953. [Google Scholar] [CrossRef]
- Luo, Y.; Lin, J.; Chen, H.; Zhang, J.; Peng, S.; Kuang, M. Utility of neut-X, neut-Y and neut-Z parameters for rapidly assessing sepsis in tumor patients. Clin. Chim. Acta 2013, 422, 5–9. [Google Scholar] [CrossRef]
- Furundarena, J.R.; Araiz, M.; Uranga, M.; Sainz, M.R.; Agirre, A.; Trassorras, M.; Uresandi, N.; Montes, M.C.; Argoitia, N. The utility of the Sysmex XE-2100 analyzer’s NEUT-X and NEUT-Y parameters for detecting neutrophil dysplasia in myelodysplastic syndromes. Int. J. Lab. Hematol. 2010, 32, 360–366. [Google Scholar] [CrossRef]
- Haschke-Becher, E.; Vockenhuber, M.; Niedetzky, P.; Totzke, U.; Gabriel, C. A new high-throughput screening method for the detection of chronic lymphatic leukemia and myelodysplastic syndrome. Clin. Chem. Lab. Med. 2008, 46, 85–88. [Google Scholar] [CrossRef]
- Charafeddine, K.M.; Youssef, A.M.; Mahfouz, R.A.; Sarieddine, D.S.; Daher, R.T. Comparison of neutrophil volume distribution width to C-reactive protein and procalcitonin as a proposed new marker of acute infection. Scand. J. Infect. Dis. 2011, 43, 777–784. [Google Scholar] [CrossRef]
- Jung, Y.J.; Kim, J.H.; Park, Y.J.; Kahng, J.; Lee, H.; Lee, K.Y.; Kim, M.Y.; Han, K.; Lee, W. Evaluation of cell population data on the UniCel DxH 800 Coulter Cellular Analysis system as a screening for viral infection in children. Int. J. Lab. Hematol. 2012, 34, 283–289. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
| Parameters | Parameters Description |
|---|---|
| IG (Immature Granulocytes) | The IG fraction includes promyelocytes, myelocytes and metamyelocytes (blasts and band cells are not included). |
| NEUT-RI (Neutrophil Reactivity Intensity) | Represents the mean value of fluorescence intensity and increases in proportion to the content of nucleic acids in the cell. It reflects metabolic activity of neutrophils |
| NEUT-GI (Neutrophil Granularity Intensity) | Dependent on neutrophil complexity. Increases in the presence of cytoplasmic granulation or vacuoles. |
| NE-WX | Reflects the width of dispersion of neutrophils population, respect to neutrophil side-scatter (NE-SSC). |
| NE-WY | Represents the fluorescence distribution width of neutrophil population, respect to neutrophil fluorescence intensity (NE-SFL). |
| NE-WZ | Reflects the distribution width of neutrophils population, respect to neutrophil forward scatter (NE-FSC).Proportional to the width of dispersion of neutrophil cell size. |
| NE-FSC | Neutrophil forward scatter mean intensity. Reflects neutrophil cell size. |
| Patients n = 79 | |
|---|---|
| Sex: f/m (n) | 30/49 |
| Age (mean ± SD years) | 58.0 ± 15.0 |
| Women (mean ± SD years) | 57.9 ± 14.8 |
| Men (mean ± SD years) | 58.4 ± 14.4 |
| Clinical symptoms (n, %) | |
| 69, 87.3 |
| 52, 65.8 |
| 49, 62.0 |
| 18, 22.7 |
| Diseases comorbidities (n, %) | |
| 14, 17.7 |
| 30, 38.0 |
| 11, 13.9 |
| 13, 16.5 |
| 7, 8.8 |
| Saturation (mean ± SD years) | 91.8 ± 6.1 |
| Chest X-ray changes (n, %) | 62, 78.5 |
| Oxygen supplementation (n, %) | 64, 81.0 |
| Invasive ventilation (n, %) | 7, 8.7 |
| Sysmex Parameters Median [(Q1–Q3)] | A. COVID-19 n = 79 | B. Convalescent Patients n = 71 | C. HC n = 20 | * p < 0.05 A-B-C ANOVA Kruskal- Wallis | * p < 0.05 in Groups Post-Hoc |
|---|---|---|---|---|---|
| 6.51 (4.35–8.73) | 7.56 (5.86–9.90) | 5.95 (4.78–6.53) | * p = 0.0002 | A–B, B–C |
| 4.02 (2.64–7.04) | 4.81 (3.52–6.91) | 3.63 (2.36–3.90) | * p = 0.0018 | B–C |
| 1.00 (0.70–1.47) | 1.69 (1.26–2.37) | 1.63 (1.29–2.08) | * p = 0.0038 | A–B, A–C |
| 0.41 (0.26–0.55) | 0.70 (0.49–0.83) | 0.54 (0.36–0.65) | * p < 0.0001 | A–B, B–C |
| 0.01 (0.00–0.08) | 0.10 (0.04–0.17) | 0.12 (0.08–0.19) | * p < 0.0001 | A–B, A–C |
| 0.01 (0.01–0.02) | 0.03 (0.02–0.04) | 0.04 (0.02–0.04) | * p < 0.0001 | A–B, A–C |
| 227 (184–300) | 338 (260–421) | 249 (213–278) | * p < 0.0001 | A–B, B–C |
| 74.3 (58.0–85.3) | 64.2 (57.3–76.9) | 57.2 (52.8–61.8) | * p < 0.0001 | A–C, B–C |
| 18.1 (9.7–29.0) | 24.3 (14.5–31.8) | 29.7 (25.8–33.4) | * p = 0.0004 | A–C, B–C |
| 6.1 (4.2–9.5) | 8.7 (7.3–10.1) | 8.6 (6.7–9.9) | * p = 0.0048 | A–B |
| 0.1 (0.0–1.4) | 1.4 (0.4–2.3) | 2.1 (1.2–3.1) | * p < 0.0001 | A–B, A–C |
| 0.2 (0.1–0.4) | 0.3 (0.2–0.5) | 0.6 (0.5–0.8) | * p < 0.0001 | A–B, A–C, B–C |
| Sysmex Parameters [Median (Q1–Q3)] | A. COVID-19 n = 79 | B. Convalescent Patients n = 71 | C. HC n = 20 | * p < 0.05 A-B-C ANOVA Kruskal- Wallis | * p < 0.05 in Group Post-Hoc |
|---|---|---|---|---|---|
| 0.03 (0.02–0.07) | 0.08 (0.03–0.18) | 0.02 (0.01–0.02) | * p < 0.0001 | A–B, A–C, B–C |
| 0.6 (0.3–1.1) | 0.9 (0.4–1.8) | 0.3 (0.2–0.3) | * p < 0.0001 | A–C, B–C |
| 46.1 (44.1–48.4) | 43.7 (42.5–45.4) | 48.3 (46.5–49.3) | * p < 0.0001 | A–B. A–C, B–C |
| 151.6 (146.8–156.1) | 153.1 (150.1–156.3) | 153.3 (150.8–154.4) | p = 0.1689 | − |
| 87.2 (84.4–90.2) | 87.4 (84.6–90.6) | 94.6 (92.0–96.2) | * p < 0.0001 | A–C, B–C |
| 322 (304–346) | 335 (320–354) | 302 (295–308) | * p < 0.0001 | A–C, B–C |
| 609 (584–642) | 616 (594–642) | 584 (559–602) | * p = 0.0001 | A–C, B–C |
| 588 (559–610) | 582 (561–629) | 541 (530–565) | * p < 0.0001 | A–C, B–C |
| Sysmex Parameters [Median (Q1–Q3)] | Oxygen Supplementation n = 64 | Without Oxygen Supplementation n = 15 | * p < 0.05 The Mann–Whitney U Test |
|---|---|---|---|
| 4.85 (2.89–7.94) | 2.87 (2.18–3.97) | * p = 0.0076 |
| 0.94 (0.65–1.45) | 1.27 (0.97–1.99) | p = 0.0796 |
| 0.41 (0.26–0.55) | 0.36 (0.25–0.53) | p = 0.6891 |
| 0.01 (0.00–0.06) | 0.04 (0.00–0.09) | p = 0.2179 |
| 0.02 (0.01–0.02) | 0.01 (0.01–0.02) | p = 0.2813 |
| 242 (187–295) | 202 (182–325) | p = 0.5804 |
| 77.0 (60.8–85.9) | 61.0 (47.6–74.3) | * p = 0.0059 |
| 16.2 (8.7–27.5) | 30.1 (22.7–35.7) | * p = 0.0050 |
| 6.0 (3.9–9.4) | 7.6 (5.7–10.3) | p = 0.2132 |
| 0.1 (0.0–1.4) | 1.0 (0.0–2.9) | p = 0.1135 |
| 0.2 (0.1–0.4) | 0.2 (0.2–0.4) | p = 0.9040 |
| 0.04 (0.02–0.08) | 0.02 (0.01–0.02) | * p = 0.0204 |
| 0.60 (0.40–1.20) | 0.45 (0.20–0.60) | p = 0.0611 |
| 46.8 (44.3–48.4) | 45.0 44.1–47.9) | p = 0.5804 |
| 151.6 (146.4–156.1) | 151.8 (149.3–155.2) | p = 0.5764 |
| 46.8 (44.3–48.4) | 45.0 (44.1–47.9) | p = 0.0533 |
| 325 (303–349) | 317 (309–337) | p = 0.8349 |
| 613 (587–649) | 588 (566–624) | p = 0.0511 |
| 592 (570–614) | 553 (535–578) | p = 0.0601 |
| Sysmex Parameters [Median (Q1–Q3)] | Respiratory Failure n = 18 | Without Respiratory Failure n = 61 | * p < 0.05 The Mann–Whitney U Test |
|---|---|---|---|
| 5.58 (2.64–8.20) | 3.90 (2.79–6.81) | p = 0.4266 |
| 0.79 (0.61–1.22) | 1.02 (0.70–1.57) | p = 0.1603 |
| 0.41 (0.27–0.49) | 0.40 (0.25–0.55) | p = 0.9216 |
| 0.00 (0.00–0.09) | 0.01 (0.00–0.06) | p = 0.4828 |
| 0.02 (0.01–0.02) | 0.01 (0.01–0.02) | p = 0.6141 |
| 209 (187–295) | 229 (182–300) | p = 0.7943 |
| 78.2 (62.5–85.9) | 72.9 (57.4–85.2) | p = 0.3439 |
| 16.1 (8.5–25.7) | 20.8 (10.4–31.2) | p = 0.3206 |
| 6.7 (3.3–9.5) | 6.1 (4.6–9.4) | p = 0.8757 |
| 0.0 (0.0–2.0) | 0.2 (0.0–1.4) | p = 0.2024 |
| 0.2 (0.1–0.4) | 0.2 (0.1–0.4) | p = 0.6305 |
| 0.04 (0.02–0.07) | 0.03 (0.02–0.08) | p = 0.9508 |
| 0.5 (0.4–1.0) | 0.6 (0.3–1.1) | p = 0.9213 |
| 47.4 (45.5–51.2) | 45.8 (43.8–48.0) | * p = 0.0377 |
| 153.2 (147.7–157.4) | 151.2 (146.4–155.2) | p = 0.2936 |
| 86.6 (83.2–89.9) | 87.3 (84.6–90.4) | p = 0.5099 |
| 344 (303–350) | 317 (305–339) | p = 0.4251 |
| 625 (605–715) | 602 (577–633) | p = 0.0519 |
| 604 (681–622) | 579 (556–604) | p = 0.0597 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kwiecień, I.; Rutkowska, E.; Kulik, K.; Kłos, K.; Plewka, K.; Raniszewska, A.; Rzepecki, P.; Chciałowski, A. Neutrophil Maturation, Reactivity and Granularity Research Parameters to Characterize and Differentiate Convalescent Patients from Active SARS-CoV-2 Infection. Cells 2021, 10, 2332. https://doi.org/10.3390/cells10092332
Kwiecień I, Rutkowska E, Kulik K, Kłos K, Plewka K, Raniszewska A, Rzepecki P, Chciałowski A. Neutrophil Maturation, Reactivity and Granularity Research Parameters to Characterize and Differentiate Convalescent Patients from Active SARS-CoV-2 Infection. Cells. 2021; 10(9):2332. https://doi.org/10.3390/cells10092332
Chicago/Turabian StyleKwiecień, Iwona, Elżbieta Rutkowska, Katarzyna Kulik, Krzysztof Kłos, Katarzyna Plewka, Agata Raniszewska, Piotr Rzepecki, and Andrzej Chciałowski. 2021. "Neutrophil Maturation, Reactivity and Granularity Research Parameters to Characterize and Differentiate Convalescent Patients from Active SARS-CoV-2 Infection" Cells 10, no. 9: 2332. https://doi.org/10.3390/cells10092332