
Repurposing of High-Dose Erythropoietin as a Potential Drug Attenuates Sepsis in Preconditioning Renal Injury

 , , , ,
, , , , 
Abstract
:1. Introduction
2. Materials and Methods
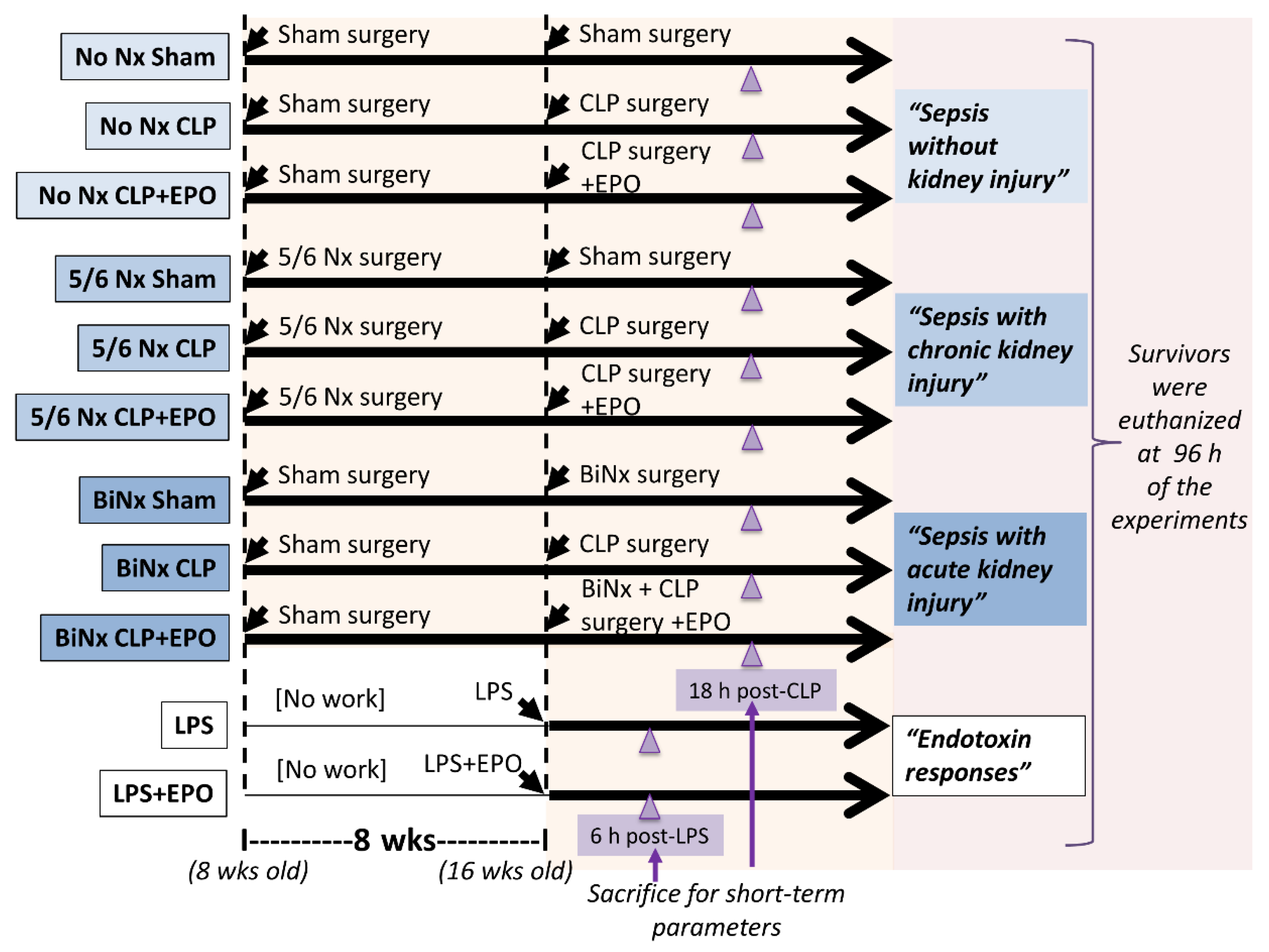
2.1. Animal Study and Animal Models
2.2. Analysis of Blood and Mouse Organs
2.3. Experiments on a Macrophage Cell Line
2.4. Experiments on a Hepatocyte Cell Line
2.5. General Description of the Human Study
2.6. Statistical Analysis
3. Results
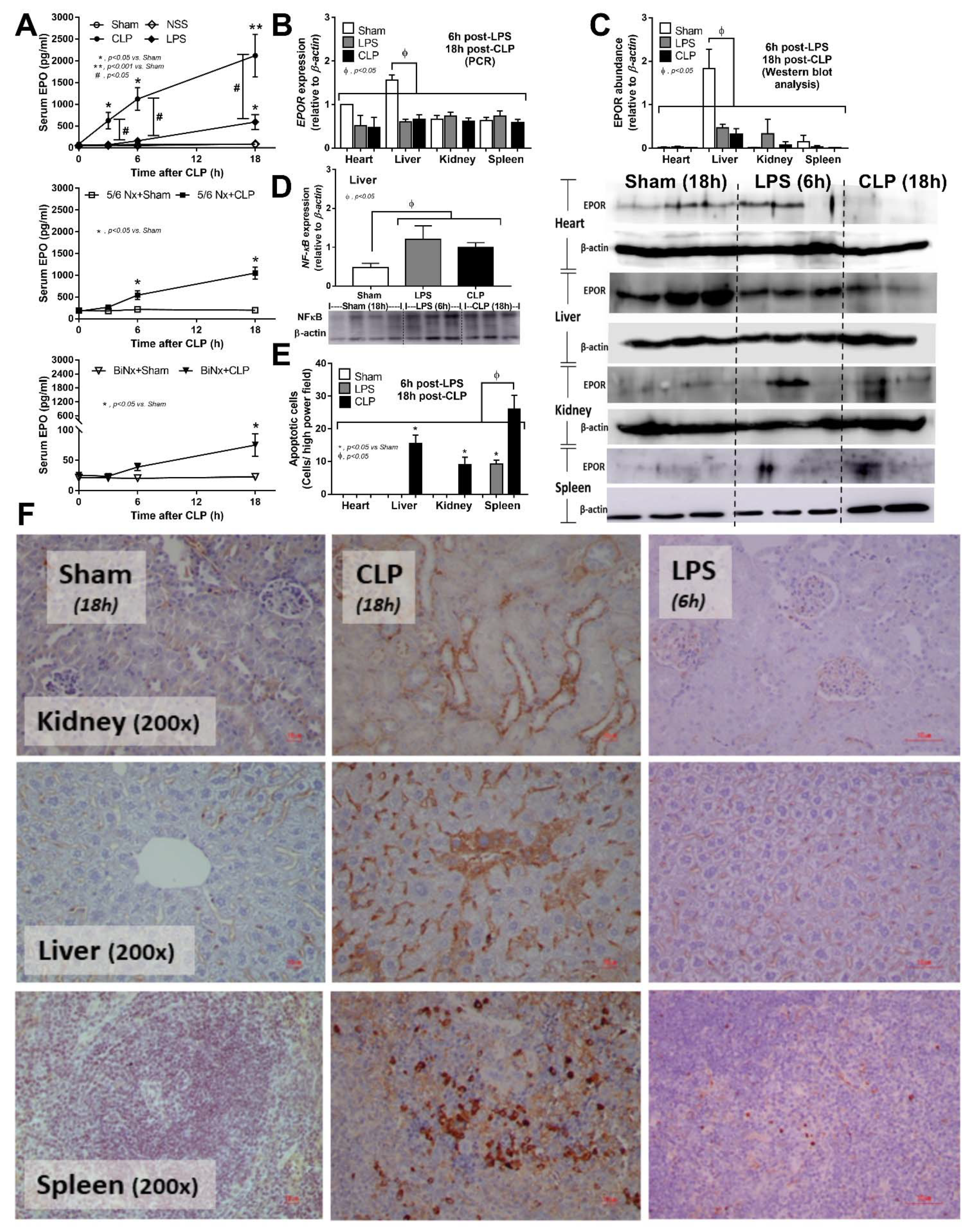
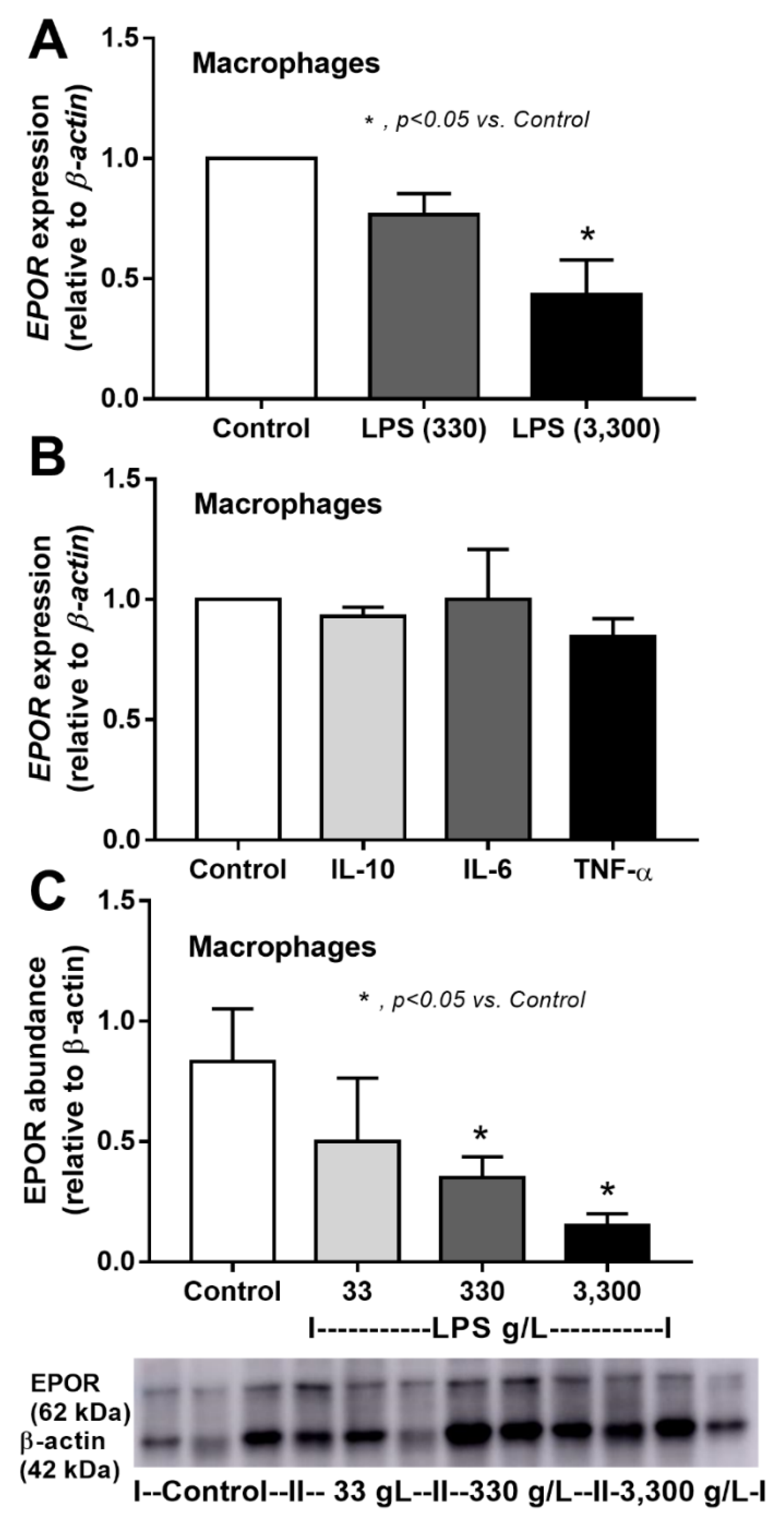
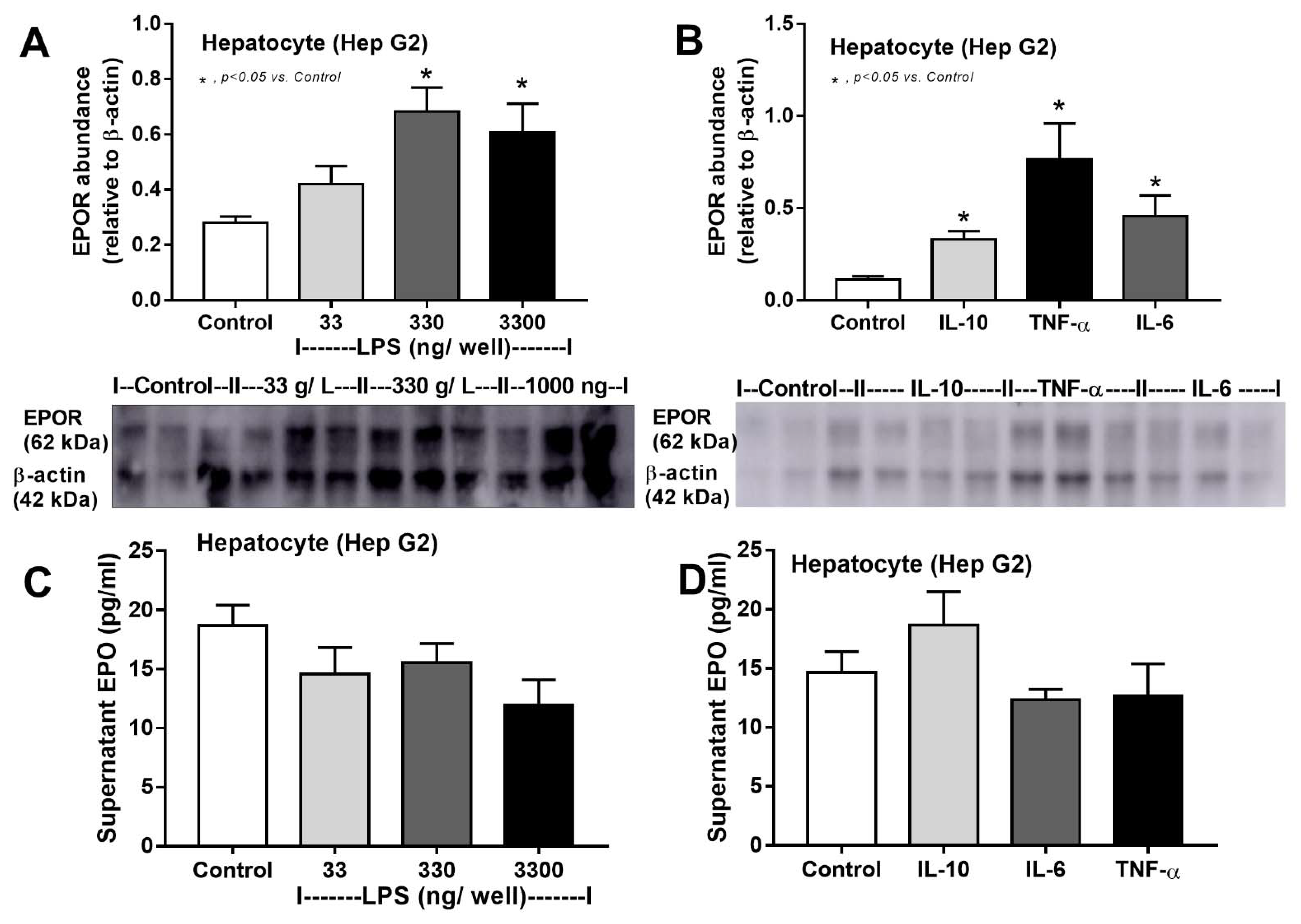
3.1. Sepsis Enhanced Endogenous EPO Production with or without Renal Injury Model, and Reduced EPO Receptor in the Liver
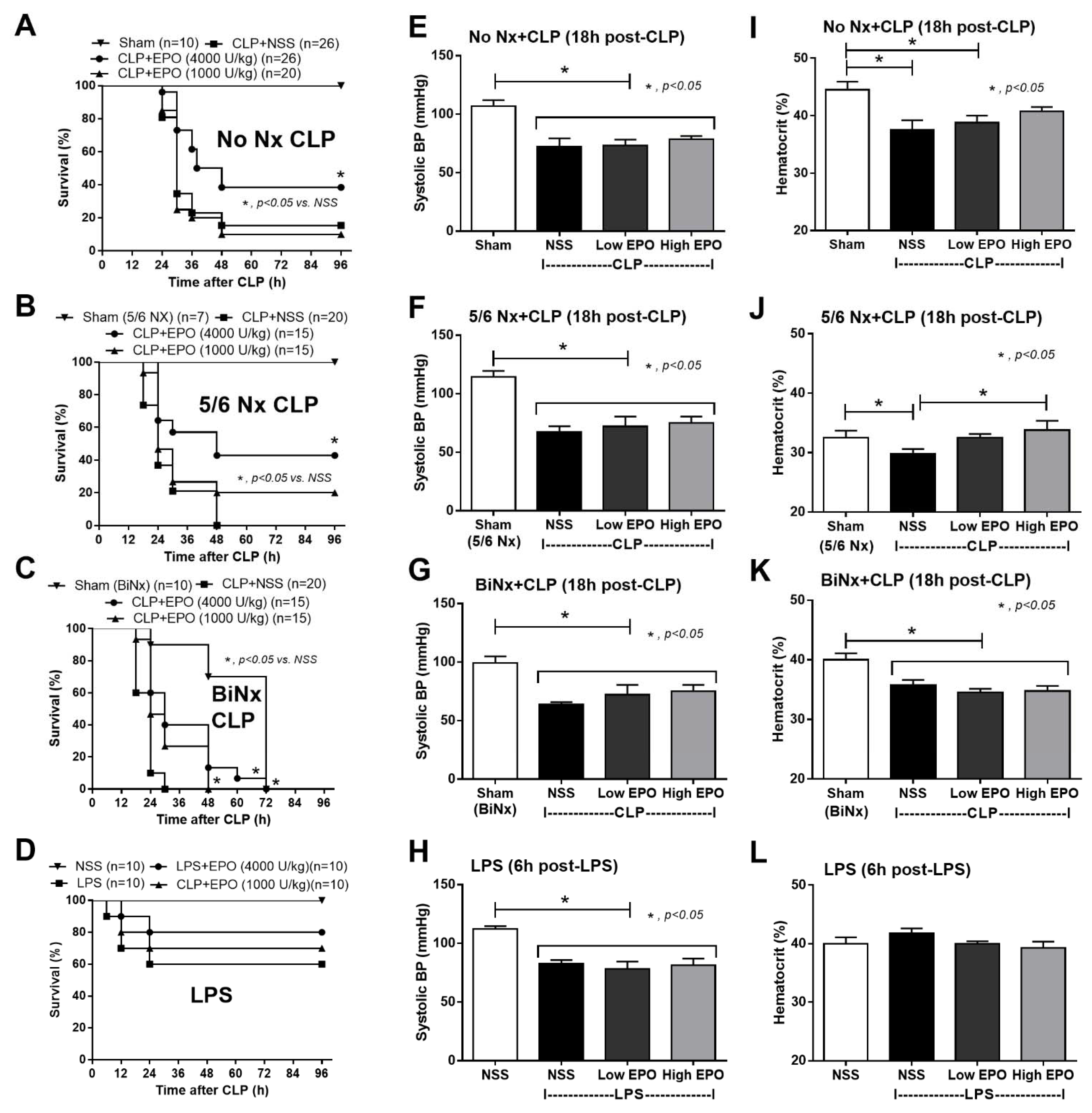
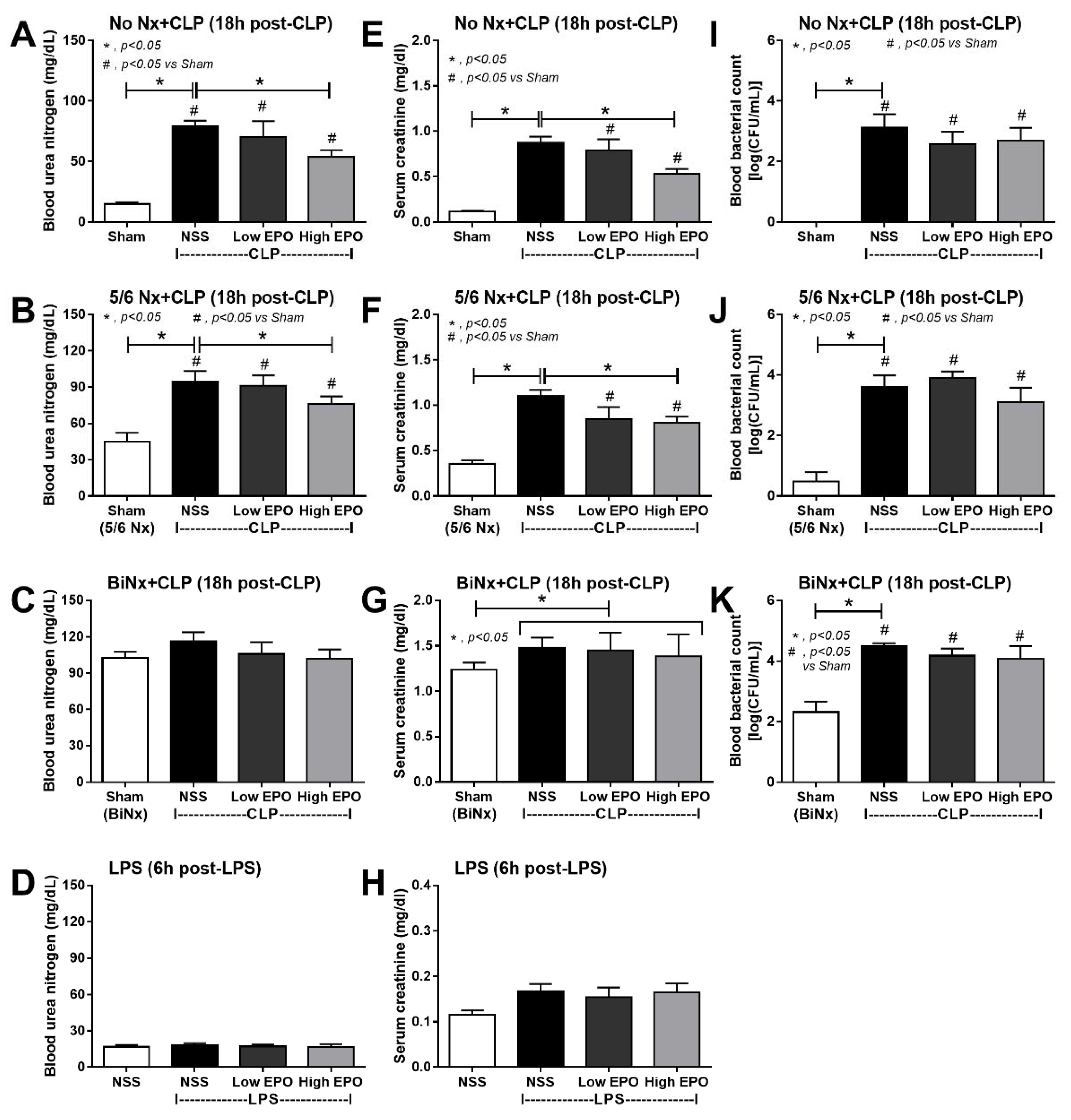
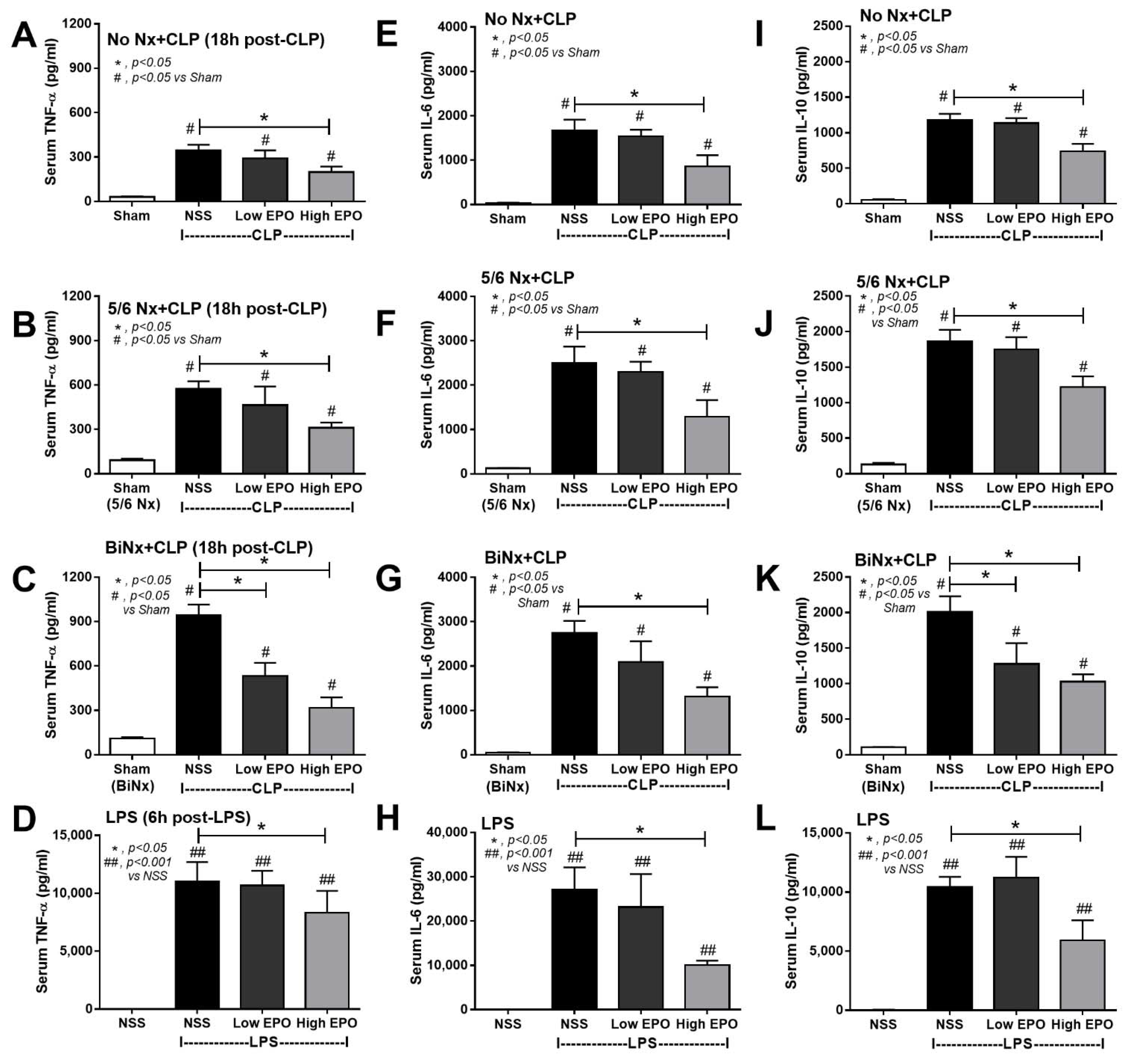
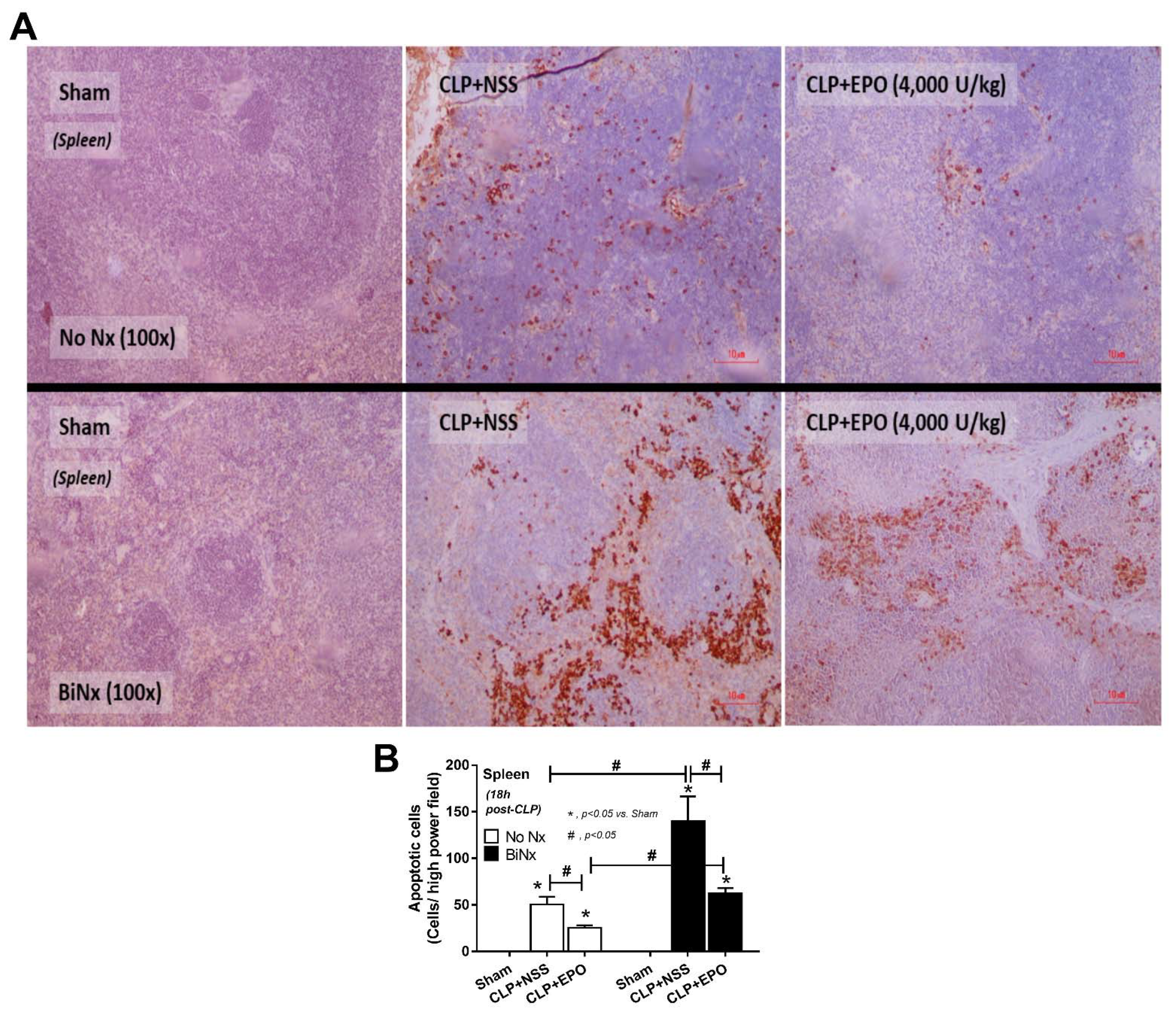
3.2. Mortality, Pre-Conditioning Renal Injury and Inflammation in Sepsis Were Attenuated by High-Dose EPO
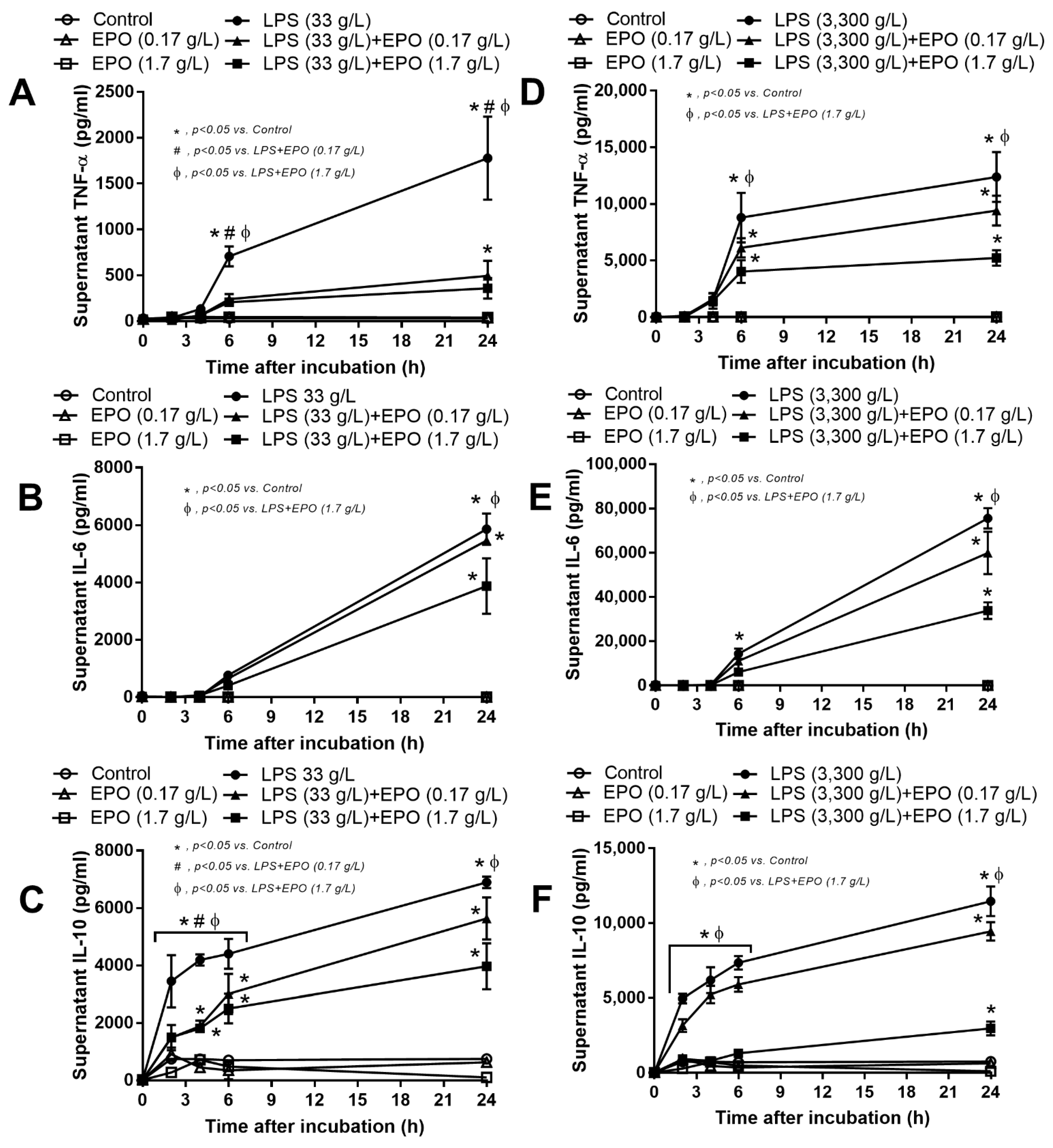
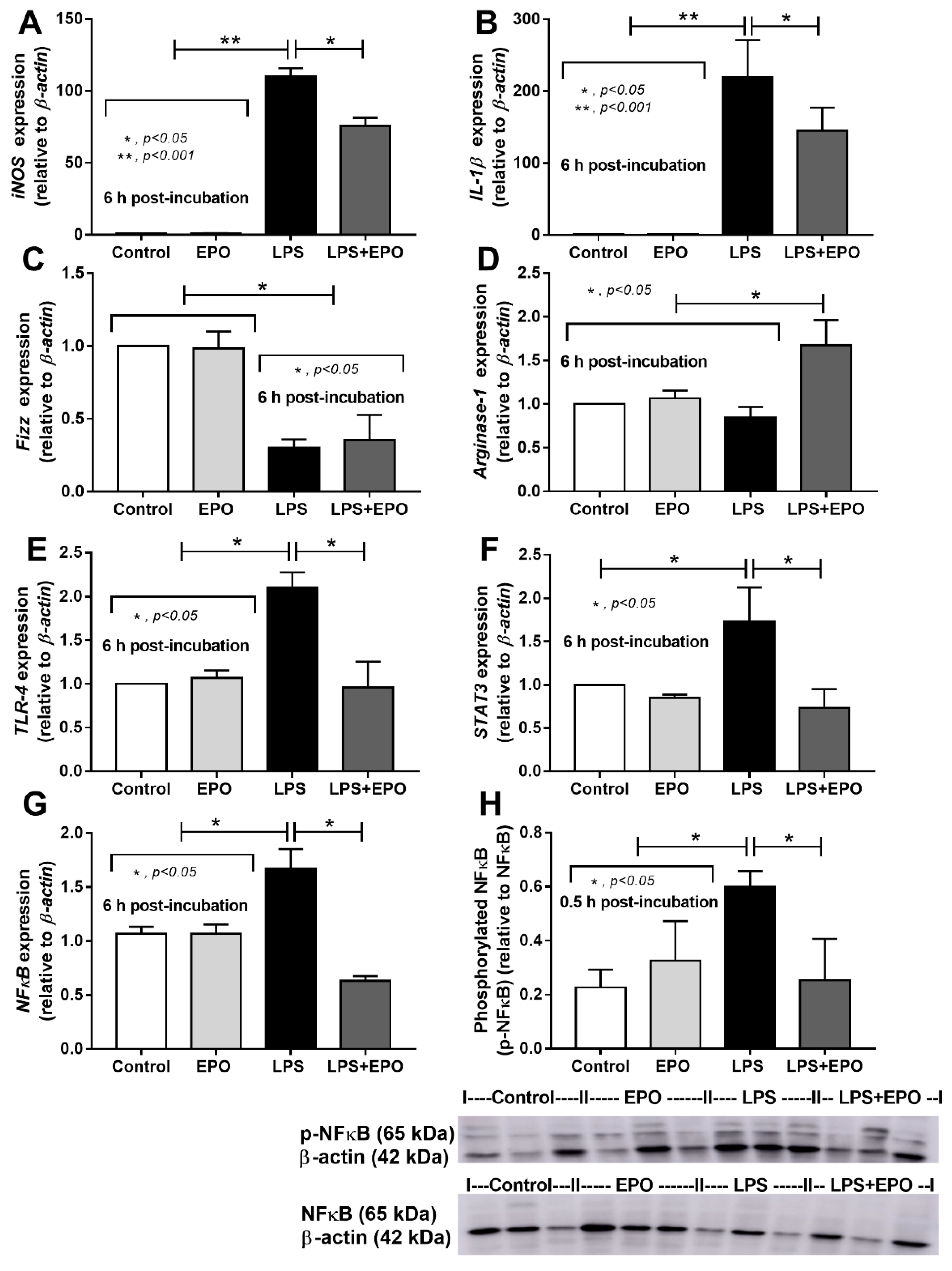
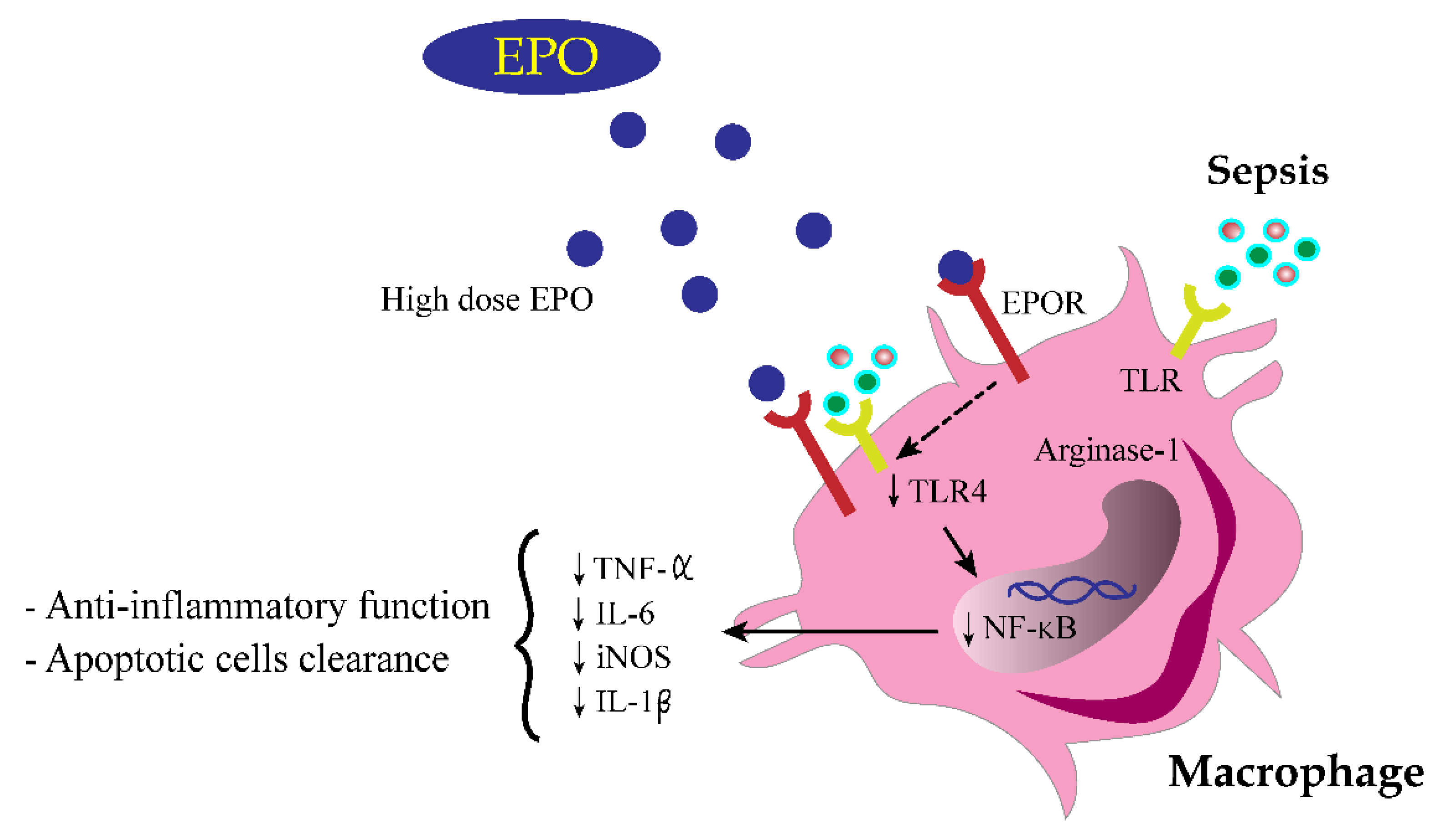
3.3. EPO Attenuated Inflammatory Responses in LPS-Activated Macrophages
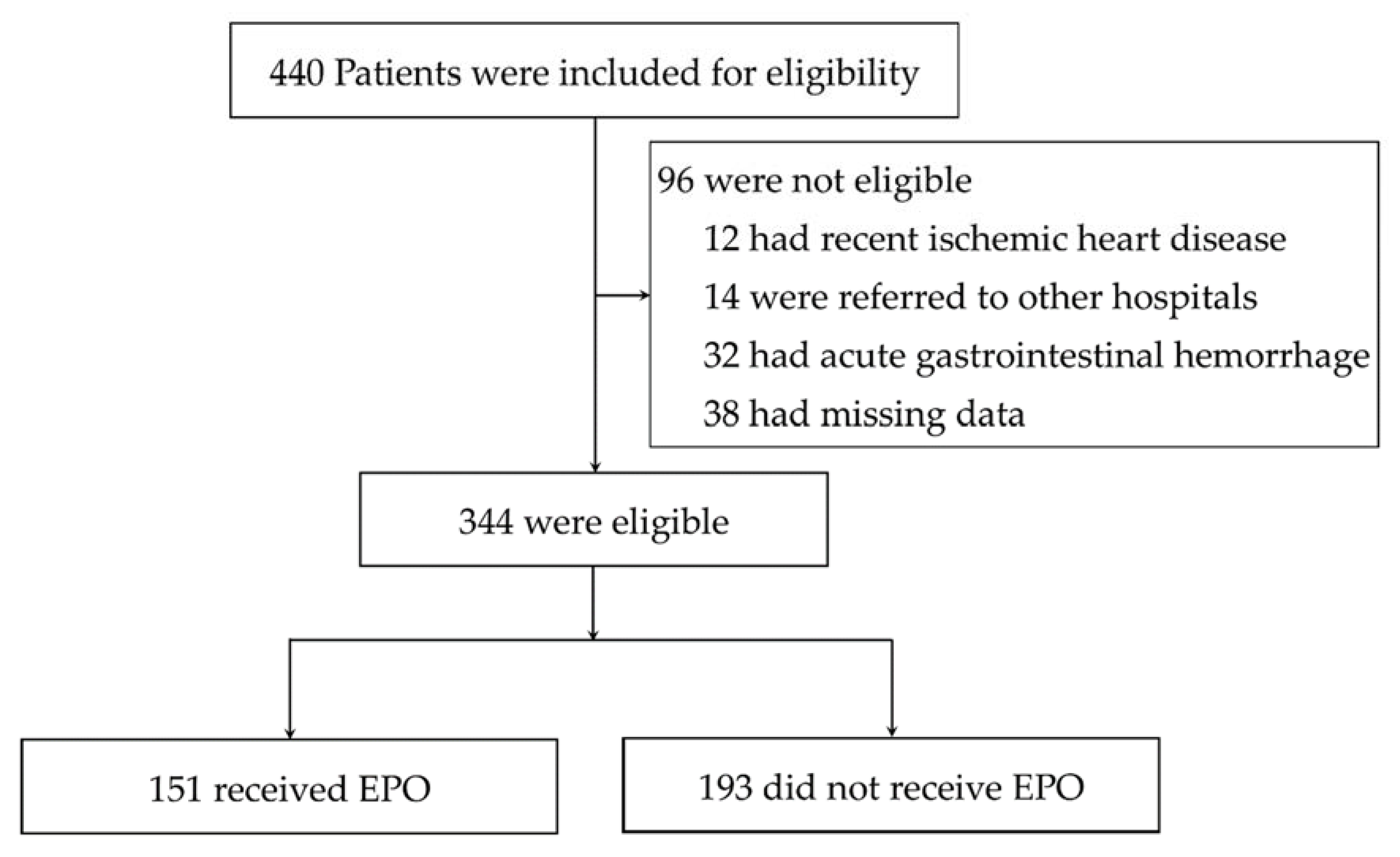
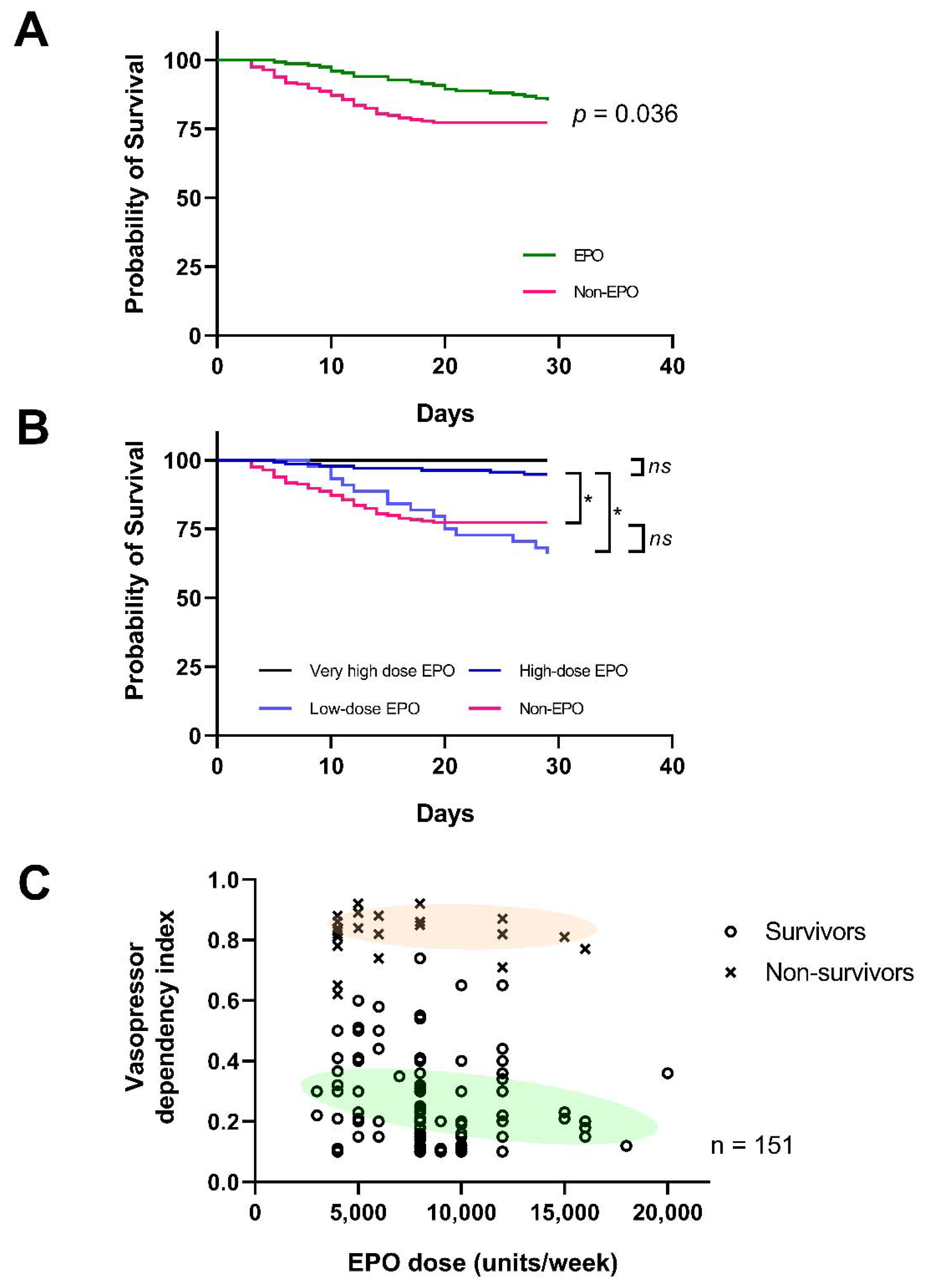
3.4. Mortality Rate Was Lower in Patients with EPO Administration, but Thrombotic Vascular Adverse Events Was Not Significantly Increased
4. Discussion
4.1. The Increased EPO Production in Response to the Reduced EPOR during Sepsis, an Immunomodulation of EPO
4.2. High-Dose EPO Administration in Mice and in Patients, an Adjuvant Therapy for Sepsis
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Singer, M.; Deutschman, C.S.; Seymour, C.C.; Shankar-Hari, M.; Annane, D.; Bauer, M.; Bellomo, R.; Bernard, G.R.; Chiche, J.-D.; Coopersmith, C.C.; et al. The Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3). JAMA 2016, 315, 801–810. [Google Scholar] [CrossRef]
- Bagshaw, S.M.; Uchino, S.; Bellomo, R.; Morimatsu, H.; Morgera, S.; Schetz, M.; Tan, I.; Bouman, C.; Macedo, E.; Gibney, N.; et al. Septic Acute Kidney Injury in Critically Ill Patients: Clinical Characteristics and Outcomes. Clin. J. Am. Soc. Nephrol. 2007, 2, 431–439. [Google Scholar] [CrossRef] [Green Version]
- Maiden, M.J.; Otto, S.; Brealey, J.K.; Finnis, M.E.; Chapman, M.J.; Kuchel, T.R.; Nash, C.H.; Edwards, J.; Bellomo, R. Structure and Function of the Kidney in Septic Shock. A Prospective Controlled Experimental Study. Am. J. Respir. Crit. Care Med. 2016, 194, 692–700. [Google Scholar] [CrossRef] [PubMed]
- See, E.J.; Jayasinghe, K.; Glassford, N.; Bailey, M.; Johnson, D.W.; Polkinghorne, K.R.; Toussaint, N.D.; Bellomo, R. Long-term risk of adverse outcomes after acute kidney injury: A systematic review and meta-analysis of cohort studies using consensus definitions of exposure. Kidney Int. 2019, 95, 160–172. [Google Scholar] [CrossRef] [PubMed]
- Doi, K. Role of kidney injury in sepsis. J. Intensive Care 2016, 4, 17. [Google Scholar] [CrossRef] [Green Version]
- Doi, K.; Leelahavanichkul, A.; Hu, X.; Sidransky, K.L.; Zhou, H.; Qin, Y.; Eisner, C.; Schnermann, J.; Yuen, P.S.; Star, R.A. Pre-existing renal disease promotes sepsis-induced acute kidney injury and worsens outcome. Kidney Int. 2008, 74, 1017–1025. [Google Scholar] [CrossRef] [Green Version]
- Leelahavanichkul, A.; Huang, Y.; Hu, X.; Zhou, H.; Tsuji, T.; Chen, R.; Kopp, J.B.; Schnermann, J.; Yuen, P.S.; Star, R.A. Chronic kidney disease worsens sepsis and sepsis-induced acute kidney injury by releasing High Mobility Group Box Protein-1. Kidney Int. 2011, 80, 1198–1211. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Neyra, J.A.; Mescia, F.; Li, X.; Adams-Huet, B.; Yessayan, L.; Yee, J.; Toto, R.D.; Moe, O.W.; Neyra, J.A.; Mescia, F.; et al. Impact of Acute Kidney Injury and CKD on Adverse Outcomes in Critically Ill Septic Patients. Kidney Int. Rep. 2018, 3, 1344–1353. [Google Scholar] [CrossRef] [Green Version]
- Rogiers, P.; Zhang, H.; Leeman, M.; Nagler, J.; Neels, H.; Melot, C.; Vincent, J.-L. Erythropoietin response is blunted in critically ill patients. Intensive Care Med. 1997, 23, 159–162. [Google Scholar] [CrossRef]
- Abel, J.; Spannbrucker, N.; Fandrey, J.; Jelkmann, W. Serum erythropoietin levels in patients with sepsis and septic shock. Eur. J. Haematol. 1996, 57, 359–363. [Google Scholar] [CrossRef]
- Stoyanoff, T.R.; Todaro, J.S.; Aguirre, M.V.; Zimmermann, M.C.; Brandan, N.C. Amelioration of lipopolysaccharide-induced acute kidney injury by erythropoietin: Involvement of mitochondria-regulated apoptosis. Toxicology 2014, 318, 13–21. [Google Scholar] [CrossRef]
- Coldewey, S.M.; Khan, A.I.; Kapoor, A.; Collino, M.; Rogazzo, M.; Brines, M.; Cerami, A.; Hall, P.; Sheaff, M.; Kieswich, J.E.; et al. Erythropoietin attenuates acute kidney dysfunction in murine experimental sepsis by activation of the β-common receptor. Kidney Int. 2013, 84, 482–490. [Google Scholar] [CrossRef] [Green Version]
- Aoshiba, K.; Onizawa, S.; Tsuji, T.; Nagai, A. Therapeutic effects of erythropoietin in murine models of endotoxin shock. Crit. Care Med. 2009, 37, 889–898. [Google Scholar] [CrossRef] [PubMed]
- Sølling, C.; Christensen, A.T.; Krag, S.; Wogensen, L.; Tønnesen, E.K.; Nygaard, U.; Frøkiær, J.; Krog, J. Erythropoietin does not attenuate renal dysfunction or inflammation in a porcine model of endotoxemia. Acta Anaesthesiol. Scand. 2011, 55, 411–421. [Google Scholar] [CrossRef] [PubMed]
- Chousterman, B.G.; Arnaud, M. Is There a Role for Hematopoietic Growth Factors During Sepsis? Front. Immunol. 2018, 9, 1015. [Google Scholar] [CrossRef] [PubMed]
- Lisowska-Myjak, B. Uremic Toxins and Their Effects on Multiple Organ Systems. Nephron Clin. Pract. 2014, 128, 303–311. [Google Scholar] [CrossRef]
- Vu, C.T.B.; Thammahong, A.; Yagita, H.; Azuma, M.; Hirankarn, N.; Ritprajak, P.; Leelahavanichkul, A. Blockade of PD-1 Attenuated Postsepsis Aspergillosis Via the Activation of IFN-γ and The Dampening of IL-10. Shock 2020, 53, 514–524. [Google Scholar] [CrossRef] [PubMed]
- Ondee, T.; Gillen, J.; Visitchanakun, P.; Somparn, P.; Issara-Amphorn, J.; Phi, C.D.; Chancharoenthana, W.; Gurusamy, D.; Nita-Lazar, A.; Leelahavanichkul, A. Lipocalin-2 (Lcn-2) Attenuates Polymicrobial Sepsis with LPS Preconditioning (LPS Tolerance) in FcGRIIb Deficient Lupus Mice. Cells 2019, 8, 1064. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Leelahavanichkul, A.; Somparn, P.; Issara-Amphorn, J.; Eiam-Ong, S.; Avihingsanon, Y.; Hirankarn, N.; Srisawat, N. Serum Neutrophil Gelatinase Associated Lipocalin (NGAL) Outperforms Serum Creatinine in Detecting Sepsis-Induced Acute Kidney Injury, Experiments on Bilateral Nephrectomy and Bilateral Ureter Obstruction Mouse Models. Shock 2016, 45, 570–576. [Google Scholar] [CrossRef]
- Leelahavanichkul, A.; Yan, Q.; Hu, X.; Eisner, C.; Huang, Y.; Chen, R.; Mizel, D.; Zhou, H.; Wright, E.C.; Kopp, J.; et al. Angiotensin II overcomes strain-dependent resistance of rapid CKD progression in a new remnant kidney mouse model. Kidney Int. 2010, 78, 1136–1153. [Google Scholar] [CrossRef] [Green Version]
- Heitrich, M.; García, D.M.D.L.; Stoyanoff, T.R.; Rodríguez, J.P.; Todaro, J.S.; Aguirre, M.V. Erythropoietin attenuates renal and pulmonary injury in polymicrobial induced-sepsis through EPO-R, VEGF and VEGF-R2 modulation. Biomed. Pharmacother. 2016, 82, 606–613. [Google Scholar] [CrossRef] [PubMed]
- Seujange, Y.; Leelahavanichkul, A.; Yisarakun, W.; Khawsuk, W.; Meepool, A.; Phamonleatmongkol, P.; Saechau, W.; Onlamul, W.; Tantiwarattanatikul, P.; Oonsook, W.; et al. Hibiscus SabdariffaLinnaeus Aqueous Extracts Attenuate the Progression of Renal Injury in 5/6 Nephrectomy Rats. Ren. Fail. 2012, 35, 118–125. [Google Scholar] [CrossRef] [Green Version]
- Rhodes, A.; Evans, L.E.; Alhazzani, W.; Levy, M.M.; Antonelli, M.; Ferrer, R.; Kumar, A.; Sevransky, J.E.; Sprung, C.L.; Nunnally, M.E.; et al. Surviving Sepsis Campaign. Crit. Care Med. 2017, 45, 486–552. [Google Scholar] [CrossRef]
- Cruz, D.N.; Antonelli, M.; Fumagalli, R.; Foltran, F.; Brienza, N.; Donati, A.; Malcangi, V.; Petrini, F.; Volta, G.; Pallavicini, F.M.B.; et al. Early Use of Polymyxin B Hemoperfusion in Abdominal Septic Shock: The EUPHAS randomized controlled trial. JAMA 2009, 301, 2445–2452. [Google Scholar] [CrossRef] [Green Version]
- Dellanna, F.; Winkler, R.E.; Bozkurt, F.; Schettler, V.; Graf, S.; Bockreiss, N.; Fliser, D.; on behalf of the MIRACEL Study Group. Dosing strategies for conversion of haemodialysis patients from short-acting erythropoiesis stimulating agents to once-monthly C.E.R.A.: Experience from the MIRACEL study. Int. J. Clin. Pract. 2011, 65, 64–72. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chancharoenthana, W.; Wattanatorn, S.; Vadcharavivad, S.; Eiam-Ong, S.; Leelahavanichkul, A. Agreement and Precision Analyses of Various Estimated Glomerular Filtration Rate Formulae in Cancer Patients. Sci. Rep. 2019, 9, 19356. [Google Scholar] [CrossRef] [Green Version]
- Birgegård, G.; Hallgren, R.; Caro, J. Serum erythropoietin in rheumatoid arthritis and other inflammatory arthritides: Relationship to anaemia and the effect of anti-inflammatory treatment. Br. J. Haematol. 1987, 65, 479–483. [Google Scholar] [CrossRef] [PubMed]
- Rodrigues, C.E.; Sanches, T.R.; Volpini, R.A.; Shimizu, M.H.; Semedo-Kuriki, P.; Camara, N.O.; Seguro, A.C.; Andrade, L. Effects of Continuous Erythropoietin Receptor Activator in Sepsis-Induced Acute Kidney Injury and Multi-Organ Dysfunction. PLoS ONE 2012, 7, e29893. [Google Scholar] [CrossRef] [Green Version]
- Morisaki, H.; Sibbald, W.; Martin, C.; Doig, G.; Inman, K. Hyperdynamic sepsis depresses circulatory compensation to normovolemic anemia in conscious rats. J. Appl. Physiol. 1996, 80, 656–664. [Google Scholar] [CrossRef]
- Pereira, R.S.; Bertoncheli, C.M.; Adefegha, S.A.; Castilhos, L.G.; Silveira, K.L.; Rezer, J.F.P.; Doleski, P.H.; Abdalla, F.H.; Santos, K.F.; Leal, C.A.; et al. Sepsis induced by cecal ligation and perforation (CLP) alters nucleotidase activities in platelets of rats. Microb. Pathog. 2017, 111, 345–351. [Google Scholar] [CrossRef]
- Yang, Q.-Y.; Ouyang, J.; Yang, J. Sepsis as an important risk factor for gastrointestinal bleeding in acute coronary syndrome patients: Two case reports. Medicine 2018, 97, e12273. [Google Scholar] [CrossRef] [PubMed]
- Pinto, J.; Ribeiro, S.; Pontes, H.; Thowfeequ, S.; Tosh, D.; Carvalho, F.; Porto, G. Erythropoietin mediates hepcidin expression in hepatocytes through EPOR signaling and regulation of C/EBPα. Blood 2008, 111, 5727–5733. [Google Scholar] [CrossRef]
- Arcasoy, M.O. The non-haematopoietic biological effects of erythropoietin. Br. J. Haematol. 2008, 141, 14–31. [Google Scholar] [CrossRef] [PubMed]
- Brines, M.; Grasso, G.; Fiordaliso, F.; Sfacteria, A.; Ghezzi, P.; Fratelli, M.; Latini, R.; Xie, Q.-W.; Smart, J.; Su-Rick, C.-J.; et al. Erythropoietin mediates tissue protection through an erythropoietin and common beta-subunit heteroreceptor. Proc. Natl. Acad. Sci. USA 2004, 101, 14907–14912. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yan, J.; Li, S.; Li, S. The Role of the Liver in Sepsis. Int. Rev. Immunol. 2014, 33, 498–510. [Google Scholar] [CrossRef] [Green Version]
- Peng, B.; Kong, G.; Yang, C.; Ming, Y. Erythropoietin and its derivatives: From tissue protection to immune regulation. Cell Death Dis. 2020, 11, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Issara-Amphorn, J.; Chancharoenthana, W.; Visitchanakun, P.; Leelahavanichkul, A. Syk Inhibitor Attenuates Polymicrobial Sepsis in FcgRIIb-Deficient Lupus Mouse Model, the Impact of Lupus Characteristics in Sepsis. J. Innate Immun. 2020, 12, 461–479. [Google Scholar] [CrossRef] [PubMed]
- Yu, Y.; Shiou, S.-R.; Guo, Y.; Lü, L.; Westerhoff, M.; Sun, J.; Petrof, E.O.; Claud, E.C. Erythropoietin Protects Epithelial Cells from Excessive Autophagy and Apoptosis in Experimental Neonatal Necrotizing Enterocolitis. PLoS ONE 2013, 8, e69620. [Google Scholar] [CrossRef] [Green Version]
- Kwak, J.; Kim, J.H.; Jang, H.N.; Jung, M.H.; Cho, H.S.; Chang, S.-H.; Kim, H.-J. Erythropoietin Ameliorates Ischemia/Reperfusion-Induced Acute Kidney Injury via Inflammasome Suppression in Mice. Int. J. Mol. Sci. 2020, 21, 3453. [Google Scholar] [CrossRef] [PubMed]
- Katavetin, P.; Tungsanga, K.; Eiam-Ong, S.; Nangaku, M. Antioxidative effects of erythropoietin. Kidney Int. 2007, 72, S10–S15. [Google Scholar] [CrossRef] [Green Version]
- Miao, S.; Wang, S.-M.; Cheng, X.; Li, Y.-F.; Zhang, Q.-S.; Li, G.; He, S.-Q.; Chen, X.-P.; Wu, P. Erythropoietin promoted the proliferation of hepatocellular carcinoma through hypoxia induced translocation of its specific receptor. Cancer Cell Int. 2017, 17, 1–14. [Google Scholar] [CrossRef] [Green Version]
- Köroğlu, T.F.; Yilmaz, O.; Gökmen, N.; Tugyan, K.; Baskin, H.; Eğrilmez, M.Y.; Yılmaz, O.; Tuğyan, K.; Baskın, H. Erythropoietin prevents lymphoid apoptosis but has no effect on survival in experimental sepsis. Pediatr. Res. 2013, 74, 148–153. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, X.; Dong, S.; Qin, Y.; Bian, X. Protective effect of erythropoietin against myocardial injury in rats with sepsis and its underlying mechanisms. Mol. Med. Rep. 2015, 11, 3317–3329. [Google Scholar] [CrossRef] [Green Version]
- Ates, I.; Doğan, N.; Aksoy, M.; Halıcı, Z.; Gundogdu, C.; Keles, M.S.; Halici, Z. The protective effects of IgM-enriched immunoglobulin and erythropoietin on the lung and small intestine tissues of rats with induced sepsis: Biochemical and histopathological evaluation. Pharm. Biol. 2014, 53, 78–84. [Google Scholar] [CrossRef] [PubMed]
- Knotek, M.; Rogachev, B.; Wang, W.; Ecder, T.; Melnikov, V.; Gengaro, P.E.; Esson, M.; Edelstein, C.L.; Dinarello, C.A.; Schrier, R.W. Endotoxemic renal failure in mice: Role of tumor necrosis factor independent of inducible nitric oxide synthase. Kidney Int. 2001, 59, 2243–2249. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tiwari, M.M.; Brock, R.W.; Megyesi, J.K.; Kaushal, G.P.; Mayeux, P.R. Disruption of renal peritubular blood flow in lipopolysaccharide-induced renal failure: Role of nitric oxide and caspases. Am. J. Physiol. Renal Physiol. 2005, 289, F1324–F1332. [Google Scholar] [CrossRef] [Green Version]
- Liu, S.F.; Malik, A.B. NF-κB activation as a pathological mechanism of septic shock and inflammation. Am. J. Physiol. Lung Cell. Mol. Physiol. 2006, 290, L622–L645. [Google Scholar] [CrossRef]
- Leelahavanichkul, A.; Yasuda, H.; Doi, K.; Hu, X.; Zhou, H.; Yuen, P.S.T.; Star, R.A. Methyl-2-acetamidoacrylate, an ethyl pyruvate analog, decreases sepsis-induced acute kidney injury in mice. Am. J. Physiol. Renal Physiol. 2008, 295, F1825–F1835. [Google Scholar] [CrossRef]
- Höcherl, K.; Schmidt, C.; Kurt, B.; Bucher, M. Inhibition of NF-κB ameliorates sepsis-induced downregulation of aquaporin-2/V2receptor expression and acute renal failure in vivo. Am. J. Physiol. Renal Physiol. 2010, 298, F196–F204. [Google Scholar] [CrossRef] [Green Version]
- de Souza, A.C.C.P.; Volpini, R.A.; Shimizu, M.H.M.; Sanches, T.R.C.; Camara, N.; Semedo-Kuriki, P.; Rodrigues, C.; Seguro, A.C.; Andrade, L. Erythropoietin prevents sepsis-related acute kidney injury in rats by inhibiting NF-κB and upregulating endothelial nitric oxide synthase. Am. J. Physiol. Renal Physiol. 2012, 302, F1045–F1054. [Google Scholar] [CrossRef] [Green Version]
- Wang, S.; Zhang, C.; Li, J.; Niyazi, S.; Zheng, L.; Xu, M.; Rong, R.; Yang, C.; Zhu, T. Erythropoietin protects against rhabdomyolysis-induced acute kidney injury by modulating macrophage polarization. Cell Death Dis. 2017, 8, e2725. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sakisaka, S.; Watanabe, M.; Tateishi, H.; Harada, M.; Shakado, S.; Mimura, Y.; Gondo, K.; Yoshitake, M.; Noguchi, K.; Hino, T.; et al. Erythropoietin production in hepatocellular carcinoma cells associated with polycythemia: Immunohistochemical evidence. Hepatology 1993, 18, 1357–1362. [Google Scholar] [CrossRef] [PubMed]
- Shi, M.; Flores, B.; Li, P.; Gillings, N.; McMillan, K.L.; Ye, J.; Huang, L.J.-S.; Sidhu, S.S.; Zhong, Y.-P.; Grompe, M.T.; et al. Effects of erythropoietin receptor activity on angiogenesis, tubular injury, and fibrosis in acute kidney injury: A “U-shaped” relationship. Am. J. Physiol. Renal Physiol. 2018, 314, F501–F516. [Google Scholar] [CrossRef] [PubMed]
- Nissenson, A.R.; Dylan, M.L.; Griffiths, R.I.; Yu, H.-T.; Dubois, R.W. Septicemia in Patients with ESRD Is Associated with Decreased Hematocrit and Increased Use of Erythropoietin. Clin. J. Am. Soc. Nephrol. 2006, 1, 505–510. [Google Scholar] [CrossRef]
- Walden, A.P.; Young, J.D.; Sharples, E. Bench to bedside: A role for erythropoietin in sepsis. Crit. Care 2010, 14, 227. [Google Scholar] [CrossRef] [Green Version]
- Corwin, H.L.; Gettinger, A.; Pearl, R.G.; Fink, M.P.; Levy, M.M.; Shapiro, M.J.; Corwin, M.; Colton, T.; for the EPO Critical Care Trials Group. Efficacy of Recombinant Human Erythropoietin in Critically Ill Patients: A randomized controlled trial. JAMA 2002, 288, 2827–2835. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Corwin, H.L.; Gettinger, A.; Fabian, T.C.; May, A.; Pearl, R.G.; Heard, S.O.; An, R.; Bowers, P.J.; Burton, P.; Klausner, M.A.; et al. Efficacy and Safety of Epoetin Alfa in Critically Ill Patients. N. Engl. J. Med. 2007, 357, 965–976. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tamion, F.; Le Cam-Duchez, V.; Menard, J.F.; Girault, C.; Coquerel, A.; Bonmarchand, G. Serum Erythropoietin Levels in Septic Shock. Anaesth. Intensive Care 2005, 33, 578–584. [Google Scholar] [CrossRef]
- Ehrenreich, H.; Weissenborn, K.; Begemann, M.; Busch, M.; Vieta, E.; Miskowiak, K.W. Erythropoietin as candidate for supportive treatment of severe COVID-19. Mol. Med. 2020, 26, 58. [Google Scholar] [CrossRef]














{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Primers | ||
|---|---|---|
| Inducible nitric oxide synthase (iNOS) | Forward | 5′-CCCTTCCGAAGTTTCTGGCAGCAGC-3′ |
| Reverse | 5′-GGCTGTCAGAGCCTCGTGGCTTTG-3′ | |
| Interleukin-1β (IL-1β) | Forward | 5′-GAAATGCCACCTTTTGACAGTG-3′ |
| Reverse | 5′-TGGATGCTCTCATCAGGACAG-3′ | |
| Arginase-1 (Arg-1) | Forward | 5′-CAGAAGAATG GAAGAGTCAG-3′ |
| Reverse | 5′-CAGATATGCA GGGA GTCACC-3′ | |
| Resistin-like molecule alpha (Fizz-1) | Forward | 5′-GCCAGGTCCTGGAACCTTTC-3′ |
| Reverse | 5′-GGAGCAGGGAGATGCAGATGAG-3′ | |
| Nuclear factor kappa B RelA (NF-κB) | Forward | 5′-CTTCCTCAGCCATGGTACCTCT-3′ |
| Reverse | 5′-CAAGTCTTCATCAGCATCAAACTG-3′ | |
| Toll-like receptor-4 (TLR-4) | Forward | 5′-GGCAGCAGGTGGAATTGTAT-3′ |
| Reverse | 5′-AGGCCCCAGAGTTTTGTTCT-3′ | |
| Erythropoietin receptor (EPOR) | Forward | 5′-GTCCTCATCTCGCTGTTGCT-3′ |
| Reverse | 5′-CAGGCCAGATCTTCTGCTG-3′ | |
| Signal transducer and activator of transcription 3 (Stat3) | Forward | 5′-CTTGTCTACCTCTACCCCGACAT-3′ |
| Reverse | 3′-GATCCATGTCAAACGTGAGCG-5′ | |
| Beta-actin (β-actin) | Forward | 5′-CGGTTCCGATGCCCTGAGGCTCTT-3′ |
| Reverse | 5′-CGTCACACTTCATGATGGAATTGA-3′ |
| Characteristic 1 | EPO Group (n = 151) | Non-EPO Group (n = 193) | p-Value |
|---|---|---|---|
| Age—yr | 65.9 ± 13.8 | 57.1 ± 8.5 | <0.0001 |
| Sex—no. (%) | |||
| Female | 102 (67.5) | 115 (59.6) | 0.14 |
| Sepsis—no. (%) | 106 (70.2) | 129 (66.8) | 0.56 |
| Septic shock—no. (%) | 45 (29.8) | 64 (33.2) | 0.56 |
| APACHE II score | 21.9 ± 8.9 | 22.3 ± 8.1 | 0.66 |
| Lactate level (mmol/L) | 4.1 ± 2.0 | 3.9 ± 2.3 | 0.85 |
| Vasopressor dependency index (VDI) | 0.26 ± 0.2 | 0.30 ± 0.2 | 0.07 |
| Specific diagnosis of sepsis on admission—no. (%) | |||
| Respiratory disease | 42 (27.8) | 72 (37.3) | 0.07 |
| Genitourinary disease | 94 (62.3) | 118 (61.1) | 0.91 |
| Hepatobiliary and intestinal disease | 15 (9.9) | 3 (1.6) | 0.0009 |
| Medical history—no. (%) | |||
| ≥1 coexisting condition | 151 (100) | 114 (59.1) | <0.0001 |
| Autoimmune disease | 7 (4.6) | 0 (0) | 0.003 |
| Cardiac disease | 84 (55.6) | 70 (36.3) | 0.0005 |
| Cerebrovascular disease | 26 (17.2) | 15 (7.8) | 0.01 |
| Chronic pulmonary disease | 11 (7.3) | 29 (15.0) | 0.03 |
| Chronic kidney disease | 151 (100) | 64 (33.2) | <0.0001 |
| Diabetes mellitus | 139 (92.1) | 75 (38.9) | <0.0001 |
| Hyperlipidemia | 107 (70.9) | 82 (42.5) | <0.0001 |
| Hypertension | 151 (100) | 176 (91.2) | <0.0001 |
| Liver disease | 8 (5.3) | 14 (7.3) | 0.51 |
| Solid organ tumor (cured) | 4 (2.6) | 7 (3.6) | 0.76 |
| Laboratory values | |||
| Hemoglobin—g/dL | 9.4 ± 1.1 | 11.3 ± 1.2 | <0.0001 |
| Reticulocytes—% | 2.0 ± 0.4 | 1.8 ± 0.6 | 0.0005 |
| Iron—µg/dL | 23.8 ± 20.5 | 26.9 ± 18.4 | 0.14 |
| Ferritin—ng/mL | 530.8 ± 256.2 | 569.1 ± 196.5 | 0.12 |
| Transferrin saturation—% | 16.7 ± 11.3 | 19.7 ± 18.2 | 0.08 |
| Creatinine—mg/dL | 3.6 ± 2.1 | 1.8 ± 1.3 | <0.0001 |
| eGFR (mL/min/1.73 m2) | 26.4 ± 22.2 | 38.9 ± 26.7 | <0.0001 |
| EPO dose prior to ICU admission | |||
| <8000 units/week | 48 (31.8) | — | |
| 8000–16,000 units/week | 101 (66.9) | — | |
| >16,000 units/week | 2 (1.3) | — | |
| Duration of therapy—months, median (IQR) | 39.7 (28.7–45.1) | — | |
| Short-acting EPO—no. (%) | 151 (100) | — | |
| Darbepoetin-α—no. (%) | — | — | |
| CERA—no. (%) | — | — | |
| Subcutaneous route—no. (%) | 125 (82.8) | — | |
| Intravenous route—no. (%) | 26 (17.2) | — | |
| Renal replacement therapy 2 | |||
| Intermittent hemodialysis—no. (%) | 34 (22.5) | 46 (23.8) | 0.77 |
| Sustained low-efficiency dialysis—no. (%) | 18 (11.9) | 16 (8.3) | 0.27 |
| Continuous renal replacement therapy—no. (%) | 7 (4.6) | 11 (5.7) | 0.65 |
| Thrombotic vascular events—no. (%) | 2 (1.3) | 5 (2.6) | 0.40 |
| Characteristics | Low-Dose EPO Group (n = 48) | High-Dose EPO Group (n = 101) | p-Value |
|---|---|---|---|
| Age—yr | 63.4 ± 8.8 | 66.3 ± 10.2 | 0.26 |
| Female gender—no. (%), | 24 (50) | 77 (76.2) | 0.001 |
| Sepsis—no. (%) | 34 (70.8) | 72 (71.3) | 0.95 |
| Septic shock—no. (%) | 14 (29.2) | 31 (30.7) | 0.85 |
| APACHE II score | 20.5 ± 4.2 | 22.6 ± 5.1 | 0.14 |
| Lactate level (mmol/L) | 3.7 ± 2.4 | 4.3 ± 2.3 | 0.71 |
| Vasopressor dependency index (VDI) | 0.25 ± 0.2 | 0.30 ± 0.2 | 0.99 |
| Specific diagnosis of sepsis on admission—no. (%) | |||
| Respiratory disease | 10 (20.8) | 32 (31.7) | 0.17 |
| Genitourinary disease | 33 (68.8) | 61 (60.3) | 0.32 |
| Medical history—no. (%) | |||
| ≥1 coexisting condition | 48 (100) | 101 (100) | - |
| Cardiac disease | 25 (52.1) | 57 (56.4) | 0.62 |
| Cerebrovascular disease | 10 (20.8) | 15 (14.9) | 0.01 |
| Chronic kidney disease | 48 (100) | 101 (100) | - |
| Diabetes mellitus | 43 (89.6) | 94 (93.1) | 0.46 |
| Hypertension | 48 (100) | 101 (100) | - |
| Liver disease | 2 (4.2) | 6 (5.9) | 0.67 |
| Solid organ tumor (cured) | 3 (6.3) | 1 (1.0) | 0.06 |
| Laboratory values | |||
| Hemoglobin—g/dL | 9.4 ± 0.6 | 9.5 ± 0.5 | 0.13 |
| Reticulocytes—% | 1.7 ± 0.2 | 1.9 ± 0.2 | 0.99 |
| Iron—µg/dL | 22.1 ± 10.4 | 24.8 ± 11.4 | 0.49 |
| Transferrin saturation—% | 15.4 ± 10.7 | 18.3 ± 12.2 | 0.32 |
| Creatinine—mg/dL | 3.5 ± 1.2 | 3.8 ± 1.0 | 0.13 |
| eGFR (mL/min/1.73 m2) | 30.5 ± 11.4 | 25.7 ± 13.5 | 0.20 |
| Route of EPO administration | |||
| Subcutaneous route—no. (%) | 37 (77.1) | 86 (85.1) | 0.23 |
| Intravenous route—no. (%) | 11 (22.9) | 15 (14.9) | 0.23 |
| Renal replacement therapy 1 | |||
| Intermittent hemodialysis—no. (%) | 15 (31.3) | 19 (18.8) | 0.09 |
| Sustained low-efficiency dialysis—no. (%) | 8 (16.7) | 10 (9.9) | 0.24 |
| Continuous renal replacement therapy—no. (%) | 3 (6.3) | 4 (4.0) | 0.54 |
| Thrombotic vascular events—no. (%) | 1 (2.1) | 1 (1.0) | 0.59 |
| Variable | EPO Group (n = 151) | Non-EPO Group (n = 193) | Odds Ratio (95% CI) | p-Value |
|---|---|---|---|---|
| Patients receiving a transfusion—no. (%) | 64 (42.4) | 50 (25.9) | 2.104 (1.333–3.320) | 0.0018 |
| Units transfused per patient | 4.1 ± 3.8 | 3.6 ± 3.1 | 0.18 | |
| Changes in hemoglobin concentration from baseline to day 29 | 3.6 ± 2.2 | 4.8 ± 1.6 | <0.0001 | |
| Vasopressor dependency index | ||||
| Day 1 (n = 45/151 vs. 64/193) | 0.37 ± 0.2 | 0.42 ± 0.2 | 0.20 | |
| Day 2 (n = 41/151 vs. 62/193) | 0.21 ± 0.2 | 0.28 ± 0.2 | 0.09 | |
| Day 3 (n = 40/151 vs. 60/193) | 0.18 ± 0.2 | 0.26 ± 0.2 | 0.04 | |
| Day 4 (n = 40/151 vs. 60/193) | 0.20 ± 0.2 | 0.32 ± 0.2 | 0.02 | |
| Day 5 (n = 40/151 vs. 60/193) | 0.20 ± 0.1 | 0.25 ± 0.1 | 0.02 | |
| Causes of death | ||||
| Septic shock with multiple organ failure—no. (%) | 12 (7.9) | 31 (16.1) | 0.02 | |
| Secondary acute coronary syndrome—no. (%) | 3 (2.0) | 1 (0.5) | 0.20 | |
| Severe gastrointestinal bleeding—no. (%) | 7 (4.6) | 12 (6.2) | 0.52 |
| Variables | HR (95% CI) EPO Group (n = 151) | HR (95% CI) Non-EPO Group (n = 193) |
|---|---|---|
| Gender (male) | 1.13 (1.02–1.18) | 1.00 (0.97–1.02) |
| Age (65–69 vs. <65 years) | 1.79 (1.45–1.89) | 1.75 (1.52–1.84) |
| Age (70–79 vs. <65 years) | 2.17 (2.02–2.28) | 1.88 (1.80–1.95) |
| Diabetes mellitus (yes vs. no) | 1.17 (1.10–1.20) | 1.10 (1.06–1.15) |
| Hypertension (yes vs. no) | 1.02 (0.97–1.05) | 0.96 (0.90–1.02) |
| Previous cardiac disease (yes vs. no) | 1.00 (0.96–1.04) | 0.70 (0.66–0.72) |
| Previous cerebrovascular accident (yes vs. no) | 0.99 (0.94–1.03) | 0.62 (0.60–0.65) |
| Renal function (eGFR 15–29 vs. >60 mL/min/1.73 m2) | 1.62 (1.34–1.70) | 2.01 (1.94–2.11) |
| Renal function (eGFR < 15 vs. >60 mL/min/1.73 m2) | 1.18 (1.14–1.22) | — |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chancharoenthana, W.; Udompronpitak, K.; Manochantr, Y.; Kantagowit, P.; Kaewkanha, P.; Issara-Amphorn, J.; Leelahavanichkul, A. Repurposing of High-Dose Erythropoietin as a Potential Drug Attenuates Sepsis in Preconditioning Renal Injury. Cells 2021, 10, 3133. https://doi.org/10.3390/cells10113133
Chancharoenthana W, Udompronpitak K, Manochantr Y, Kantagowit P, Kaewkanha P, Issara-Amphorn J, Leelahavanichkul A. Repurposing of High-Dose Erythropoietin as a Potential Drug Attenuates Sepsis in Preconditioning Renal Injury. Cells. 2021; 10(11):3133. https://doi.org/10.3390/cells10113133
Chicago/Turabian StyleChancharoenthana, Wiwat, Kanyarat Udompronpitak, Yolradee Manochantr, Piyawat Kantagowit, Ponthakorn Kaewkanha, Jiraporn Issara-Amphorn, and Asada Leelahavanichkul. 2021. "Repurposing of High-Dose Erythropoietin as a Potential Drug Attenuates Sepsis in Preconditioning Renal Injury" Cells 10, no. 11: 3133. https://doi.org/10.3390/cells10113133