
Relationship between the Plasma Proteome and Changes in Inflammatory Markers after Bariatric Surgery

 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Identification of Proteins
2.2. Determination of Glycosylated Haemoglobin (HbA1c), Glucose, Insulin and Inflammatory Markers
2.3. Ethics
2.4. Statistical Analysis
3. Results
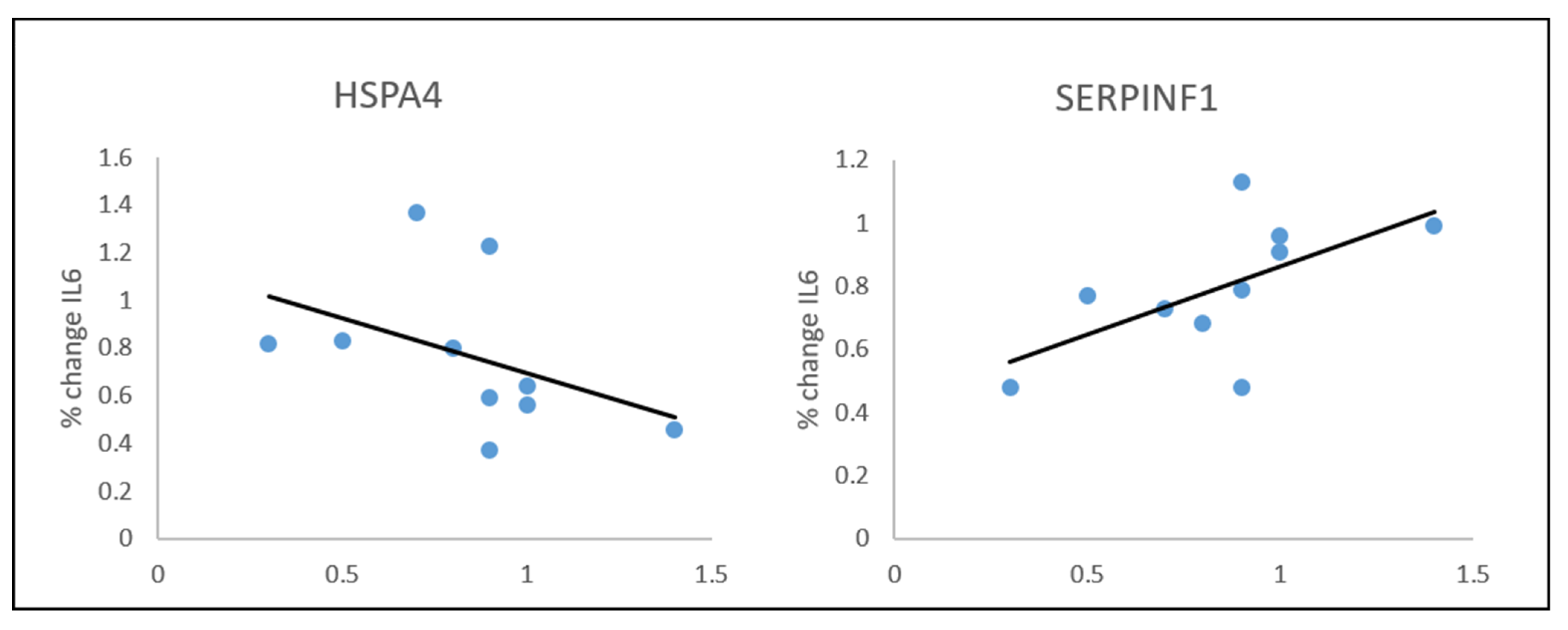
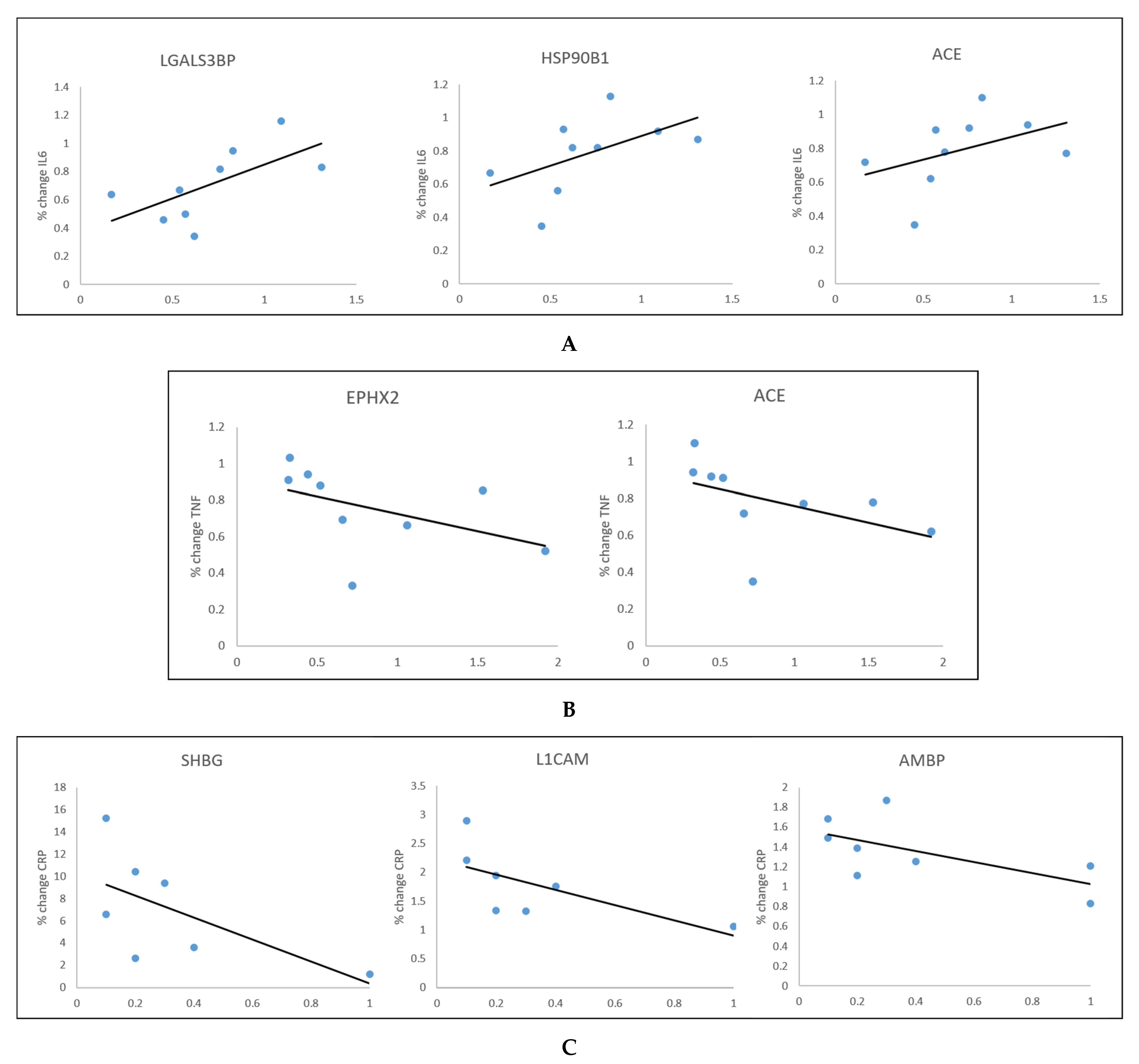
Changes in Inflammatory Markers vs. the Proteome
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Jastreboff, A.M.; Kotz, C.M.; Kahan, S.; Kelly, A.S.; Heymsfield, S.B. Obesity as a Disease: The Obesity Society 2018 Position Statement. Obesity 2019, 27, 7–9. [Google Scholar] [CrossRef] [Green Version]
- Bray, G.A.; Frühbeck, G.; Ryan, D.H.; Wilding, J.P.H. Management of obesity. Lancet 2016, 387, 1947–1956. [Google Scholar] [CrossRef] [Green Version]
- Heymsfield, S.B.; Wadden, T.A. Mechanisms, Pathophysiology, and Management of Obesity. N. Engl. J. Med. 2017, 376, 254–266. [Google Scholar] [CrossRef] [PubMed]
- Lin, C.; Cai, X.; Yang, W.; Lv, F.; Nie, L.; Ji, L. The Body Weight Alteration and Incidence of Neoplasm in Patients with Type 2 Diabetes: A Meta-Analysis of Randomized Controlled Trials. Front. Endocrinol. 2020, 11, 1001. [Google Scholar] [CrossRef]
- Ogrodnik, M.; Zhu, Y.; Langhi, L.G.P.; Tchkonia, T.; Krüger, P.; Fielder, E.; Victorelli, S.; Ruswhandi, R.A.; Giorgadze, N.; Pirtskhalava, T.; et al. Obesity-Induced Cellular Senescence Drives Anxiety and Impairs Neurogenesis. Cell Metab. 2019, 29, 1061–1077, e8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Flegal, K.M.; Graubard, B.I.; Williamson, D.F.; Gail, M.H. Cause-specific excess deaths associated with underweight, overweight, and obesity. JAMA 2007, 298, 2028–2037. [Google Scholar] [CrossRef] [Green Version]
- Apovian, C.M. Obesity: Definition, Comorbidities, Causes, and Burden. Am. J. Manag. Care 2016, 22, s176–s185. [Google Scholar]
- Ferrante, A.W., Jr. Obesity-induced inflammation: A metabolic dialogue in the language of inflammation. J. Intern. Med. 2007, 262, 408–414. [Google Scholar] [CrossRef]
- Galic, S.; Oakhill, J.S.; Steinberg, G.R. Adipose tissue as an endocrine organ. Mol. Cell. Endocrinol. 2010, 316, 129–139. [Google Scholar] [CrossRef]
- Hotamisligil, G.S. Inflammation and metabolic disorders. Nature 2006, 444, 860–867. [Google Scholar] [CrossRef]
- Dandona, P.; Aljada, A.; Bandyopadhyay, A. Inflammation: The link between insulin resistance, obesity and diabetes. Trends Immunol. 2004, 25, 4–7. [Google Scholar] [CrossRef]
- Schauer, P.R.; Burguera, B.; Ikramuddin, S.; Cottam, D.; Gourash, W.; Hamad, G.; Eid, G.M.; Mattar, S.; Ramanathan, R.; Barinas-Mitchel, E.; et al. Effect of laparoscopic Roux-en Y gastric bypass on type 2 diabetes mellitus. Ann. Surg. 2003, 238, 467–485. [Google Scholar] [CrossRef]
- Ammori, B.J.; Skarulis, M.C.; Soran, H.; Syed, A.A.; Eledrisi, M.; Malik, R.A. Medical and surgical management of obesity and diabetes: What’s new? Diabet. Med. 2020, 37, 203–210. [Google Scholar] [CrossRef] [Green Version]
- Iqbal, Z.; Adam, S.; Ho, J.H.; Syed, A.A.; Ammori, B.J.; Malik, R.A.; Soran, H. Metabolic and cardiovascular outcomes of bariatric surgery. Curr. Opin. Lipidol. 2020, 31, 246–256. [Google Scholar] [CrossRef]
- Aebersold, R.; Mann, M. Mass-spectrometric exploration of proteome structure and function. Nature 2016, 537, 347–355. [Google Scholar] [CrossRef]
- Tanner, S.D.; Baranov, V.I.; Ornatsky, O.I.; Bandura, D.R.; George, T.C. An introduction to mass cytometry: Fundamentals and applications. Cancer Immunol. Immunother. 2013, 62, 955–965. [Google Scholar] [CrossRef] [PubMed]
- Iqbal, Z.; Fachim, H.; Hamarashid, D.; Syed, A.A.; Gibson, J.M.; Donn, R.; Soran, H.; Heald, A.H. 1217-P: The Effects of Bariatric Surgery on the Proteome in People Achieving Remission of Type 2 Diabetes (T2DM) after Bariatric Surgery. J. Clin. Med. 2021, 10, 3659. [Google Scholar] [CrossRef] [PubMed]
- Gillet, L.C.; Navarro, P.; Tate, S.; Röst, H.; Selevsek, N.; Reiter, L.; Bonner, R.; Aebersold, R. Targeted data extraction of the MS/MS spectra generated by data-independent acquisition: A new concept for consistent and accurate proteome analysis. Mol. Cell. Proteom. 2012, 11. [Google Scholar] [CrossRef] [Green Version]
- Brethauer, S.A.; Kim, J.; el Chaar, M.; Papasavas, P.; Eisenberg, D.; Rogers, A.; Ballem, N.; Kligman, M.; Kothari, S. Standardized outcomes reporting in metabolic and bariatric surgery. Surg. Obes. Relat. Dis. 2015, 11, 489–506. [Google Scholar] [CrossRef] [PubMed]
- Matthews, D.R.; Hosker, J.P.; Rudenski, A.S.; Naylor, B.A.; Treacher, D.F.; Turner, R.C. Homeostasis model assessment: Insulin resistance and beta-cell function from fasting plasma glucose and insulin concentrations in man. Diabetologia 1985, 28, 412–419. [Google Scholar] [CrossRef] [Green Version]
- Rao, S.R. Inflammatory markers and bariatric surgery: A meta-analysis. Inflamm. Res. 2012, 61, 789–807. [Google Scholar] [CrossRef] [PubMed]
- Van Eden, W.; Van der Zee, R.; Prakken, B. Heat-shock proteins induce T-cell regulation of chronic inflammation. Nat. Rev. Immunol. 2005, 5, 318–330. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nakhjavani, M.; Morteza, A.; Khajeali, L.; Esteghamati, A.; Khalilzadeh, O.; Asgarani, F.; Outeiro, T.F. Increased serum HSP70 levels are associated with the duration of diabetes. Cell Stress Chaperones 2010, 15, 959–964. [Google Scholar] [CrossRef] [Green Version]
- Stygar, D.; Skrzep-Poloczek, B.; Romuk, E.; Chełmecka, E.; Poloczek, J.; Sawczyn, T.; Maciarz, J.; Kukla, M.; Karcz, K.W.; Jochem, J. The influence of high-fat, high-sugar diet and bariatric surgery on HSP70 and HSP90 plasma and liver concentrations in diet-induced obese rats. Cell Stress Chaperones 2019, 24, 427–439. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Crowe, S.; Wu, L.E.; Economou, C.; Turpin, S.M.; Matzaris, M.; Hoehn, K.L.; Hevener, A.L.; James, D.E.; Duh, E.J.; Watt, M.J. Pigment epithelium-derived factor contributes to insulin resistance in obesity. Cell Metab. 2009, 10, 40–47. [Google Scholar] [CrossRef] [Green Version]
- Böhm, A.; Ordelheide, A.M.; Machann, J.; Heni, M.; Ketterer, C.; Machicao, F.; Schick, F.; Stefan, N.; Fritsche, A.; Häring, H.U.; et al. Common Genetic Variation in the SERPINF1 Locus Determines Overall Adiposity, Obesity-Related Insulin Resistance, and Circulating Leptin Levels. PLoS ONE 2012, 7, e34035. [Google Scholar] [CrossRef]
- Geyer, P.E.; Wewer Albrechtsen, N.J.; Tyanova, S.; Grassl, N.; Iepsen, E.W.; Lundgren, J.; Madsbad, S.; Holst, J.J.; Torekov, S.S.; Mann, M. Proteomics reveals the effects of sustained weight loss on the human plasma proteome. Mol. Syst. Biol. 2016, 12, 901. [Google Scholar] [CrossRef]
- Wang, J.J.; Zhang, S.X.; Mott, R.; Chen, Y.; Knapp, R.R.; Cao, W.; Ma, J.X. Anti-inflammatory effects of pigment epithelium-derived factor in diabetic nephropathy. Am. J. Physiol. Ren. Physiol. 2008, 294, F1166–F1173. [Google Scholar] [CrossRef] [Green Version]
- Newlaczyl, A.U.; Yu, L.G. Galectin-3--a jack-of-all-trades in cancer. Cancer Lett. 2011, 313, 123–128. [Google Scholar] [CrossRef]
- Filer, A.; Bik, M.; Parsonage, G.N.; Fitton, J.; Trebilcock, E.; Howlett, K.; Cook, M.; Raza, K.; Simmons, D.L.; Thomas, A.M.; et al. Galectin 3 induces a distinctive pattern of cytokine and chemokine production in rheumatoid synovial fibroblasts via selective signaling pathways. Arthritis Rheum. 2009, 60, 1604–1614. [Google Scholar] [CrossRef] [Green Version]
- Hu, W.-M.; Yang, Y.-Z.; Zhang, T.-Z.; Qin, C.-F.; Li, X.-N. LGALS3 Is a Poor Prognostic Factor in Diffusely Infiltrating Gliomas and Is Closely Correlated With CD163+ Tumor-Associated Macrophages. Front. Med. 2020, 7, 182. [Google Scholar] [CrossRef]
- Han, L.; Wu, Z.; Zhao, Q. Revealing the molecular mechanism of colorectal cancer by establishing LGALS3-related protein-protein interaction network and identifying signaling pathways. Int. J. Mol. Med. 2014, 33, 581–588. [Google Scholar] [CrossRef]
- Salah, A.; Yoshifuji, H.; Ito, S.; Kitagori, K.; Kiso, K.; Yamada, N.; Nakajima, T.; Haga, H.; Tsuruyama, T.; Miyagawa-Hayashino, A. High Expression of Galectin-3 in Patients with IgG4-Related Disease: A Proteomic Approach. Pathol. Res. Int. 2017, 2017, 9312142. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Melin, E.O.; Dereke, J.; Hillman, M. Female sex, high soluble CD163, and low HDL-cholesterol were associated with high galectin-3 binding protein in type 1 diabetes. Biol. Sex Differ. 2019, 10, 51. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.; Das, S.; Zhuo, G.; Cai, H. Elevated serum levels of galectin-3 binding protein are associated with insulin resistance in non-diabetic women after menopause. Taiwan. J. Obstet. Gynecol. 2020, 59, 877–881. [Google Scholar] [CrossRef] [PubMed]
- Dai, W.; Wang, K.; Zheng, X.; Chen, X.; Zhang, W.; Zhang, Y.; Hou, J.; Liu, L. High fat plus high cholesterol diet lead to hepatic steatosis in zebrafish larvae: A novel model for screening anti-hepatic steatosis drugs. Nutr. Metab. 2015, 12, 42. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sims-Robinson, C.; Zhao, S.; Hur, J.; Feldman, E.L. Central nervous system endoplasmic reticulum stress in a murine model of type 2 diabetes. Diabetologia 2012, 55, 2276–2284. [Google Scholar] [CrossRef] [Green Version]
- Alam, Q.; Zubair Alam, M.; Hussain Wali Sait, K.; Anfinan, N.; Wahab Noorwali, A.; Amjad Kamal, M.; Sajjad Ahmad Khan, M.; Haque, A. Translational Shift of HSP90 as a Novel Therapeutic Target from Cancer to Neurodegenerative Disorders: An Emerging Trend in the Cure of Alzheimer’s and Parkinson’s Diseases. Curr. Drug Metab. 2017, 18, 868–876. [Google Scholar] [CrossRef] [PubMed]
- He, G.L.; Luo, Z.; Shen, T.T.; Yang, J.; Li, P.; Luo, X.; Yang, X.S. Inhibition of HSP90β by ganetespib blocks the microglial signalling of evoked pro-inflammatory responses to heat shock. Int. J. Biochem. Cell Biol. 2019, 106, 35–45. [Google Scholar] [CrossRef] [PubMed]
- Valente, V.; Izzo, R.; Manzi, M.V.; De Luca, M.R.; Barbato, E.; Morisco, C. Modulation of insulin resistance by renin angiotensin system inhibitors: Implications for cardiovascular prevention. Monaldi Arch. Chest Dis. 2021, 91. [Google Scholar] [CrossRef]
- Heald, A.H.; Anderson, S.G.; Ivison, F.; Riste, L.; Laing, I.; Cruickshank, J.K.; Gibson, J.M. Low sex hormone binding globulin is a potential marker for the metabolic syndrome in different ethnic groups. Exp. Clin. Endocrinol. Diabetes 2005, 113, 522–528. [Google Scholar] [CrossRef]
- Heald, A.H.; Laing, I.; Anderson, S.; Livingston, M. Low sex hormone binding globulin: A potential predictor of future glucose dysregulation in women. Cardiovasc. Endocrinol. Metab. 2021, 10, 191–192. [Google Scholar] [CrossRef]
- Tian, Z.; Zhang, Y.C.; Wang, Y.; Chang, X.H.; Zhu, H.L.; Zhao, Y. Effects of bariatric surgery on patients with obesity and polycystic ovary syndrome: A meta-analysis. Surg. Obes. Relat. Dis. 2021, 17, 1399–1408. [Google Scholar] [CrossRef] [PubMed]
- Khadir, A.; Kavalakatt, S.; Madhu, D.; Cherian, P.; Al-Mulla, F.; Abubaker, J.; Tiss, A. Soluble Epoxide Hydrolase 2 Expression Is Elevated in Obese Humans and Decreased by Physical Activity. Int. J. Mol. Sci. 2020, 21, 2056. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Patterson, S.A.; Deep, G.; Brinkley, T.E. Detection of the receptor for advanced glycation endproducts in neuronally-derived exosomes in plasma. Biochem. Biophys. Res. Commun. 2018, 500, 892–896. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Baseline (mean ± SEM) | 6 Months Post-MBS (mean ± SEM) | 12 Months Post-MBS (mean ± SEM) | p Value (Baseline × 6 Months) | p Value (Baseline × 12 Months) | |
|---|---|---|---|---|---|
| BMI | 54.9 ± 3.26 | 41.8 ± 2.20 | 38.6 ± 1.60 | <0.0001 * | <0.0001 * |
| HbA1c | 56.0 ± 4.46 | 40.0 ± 1.70 | 36.44 ± 1.01 | 0.002 * | 0.004 * |
| IL6 | 6.29 ± 1.19 | 4.8 ± 0.96 | 4.57 ± 1.10 | 0.160 | 0.029 * |
| TNFα | 5.98 ± 0.70 | 5.27 ± 1.20 | 4.59 ± 0.67 | 0.689 | 0.245 |
| CRP | 9.07 ± 2.45 | 7.14 ± 1.71 | 5.11 ± 1.88 | 0.226 | 0.180 |
| HOMA-IR | 0.56 ± 0.17 | 0.48 ± 0.19 | 0.36 ± 0.08 | 0.741 | 0.380 |
| HOMA-B | 331.86 ± 83.69 | 413.85 ± 104.60 | 376.43 ± 72.88 | 0.443 | 0.734 |
| Protein (Gene Symbol) | Fold Change ± SEM at 6 Months | Fold Change ± SEM at 12 Months |
|---|---|---|
| Heat shock protein 4 (HSPA4) | 0.7648 ± 0.10156 | N/S |
| Serpin family F member 1 (SERPINF1) | 0.7906 ± 0.06724 | N/S |
| Galectin 3 binding protein (LGALS3BP) | N/S | 0.7074 ± 0.08600 |
| Heat shock protein 90 Beta family member 1 (HSP90B1) | N/S | 0.7858 ± 0.07666 |
| Angiotensin-converting enzyme (ACE) | N/S | 0.7888 ± 0.07232 |
| Epoxide hydrolase 2 (EPHX2) | N/S | 0.7587 ± 0.07564 |
| Sex hormone-binding globulin (SHBG) | N/S | 6.1816 ± 1.83129 |
| L1 cell adhesion molecule (L1CAM) | N/S | 1.6862 ± 0.22992 |
| Alpha-1-microglobulin/Bikunin precursor (AMBP) | N/S | 1.3137 ± 0.11014 * |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fachim, H.A.; Iqbal, Z.; Gibson, J.M.; Baricevic-Jones, I.; Campbell, A.E.; Geary, B.; Syed, A.A.; Whetton, A.; Soran, H.; Donn, R.P.; et al. Relationship between the Plasma Proteome and Changes in Inflammatory Markers after Bariatric Surgery. Cells 2021, 10, 2798. https://doi.org/10.3390/cells10102798
Fachim HA, Iqbal Z, Gibson JM, Baricevic-Jones I, Campbell AE, Geary B, Syed AA, Whetton A, Soran H, Donn RP, et al. Relationship between the Plasma Proteome and Changes in Inflammatory Markers after Bariatric Surgery. Cells. 2021; 10(10):2798. https://doi.org/10.3390/cells10102798
Chicago/Turabian StyleFachim, Helene A., Zohaib Iqbal, J. Martin Gibson, Ivona Baricevic-Jones, Amy E. Campbell, Bethany Geary, Akheel A. Syed, Antony Whetton, Handrean Soran, Rachelle P. Donn, and et al. 2021. "Relationship between the Plasma Proteome and Changes in Inflammatory Markers after Bariatric Surgery" Cells 10, no. 10: 2798. https://doi.org/10.3390/cells10102798