
Dual-Level Augmentation Radiomics Analysis for Multisequence MRI Meningioma Grading

Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Data Acquirement
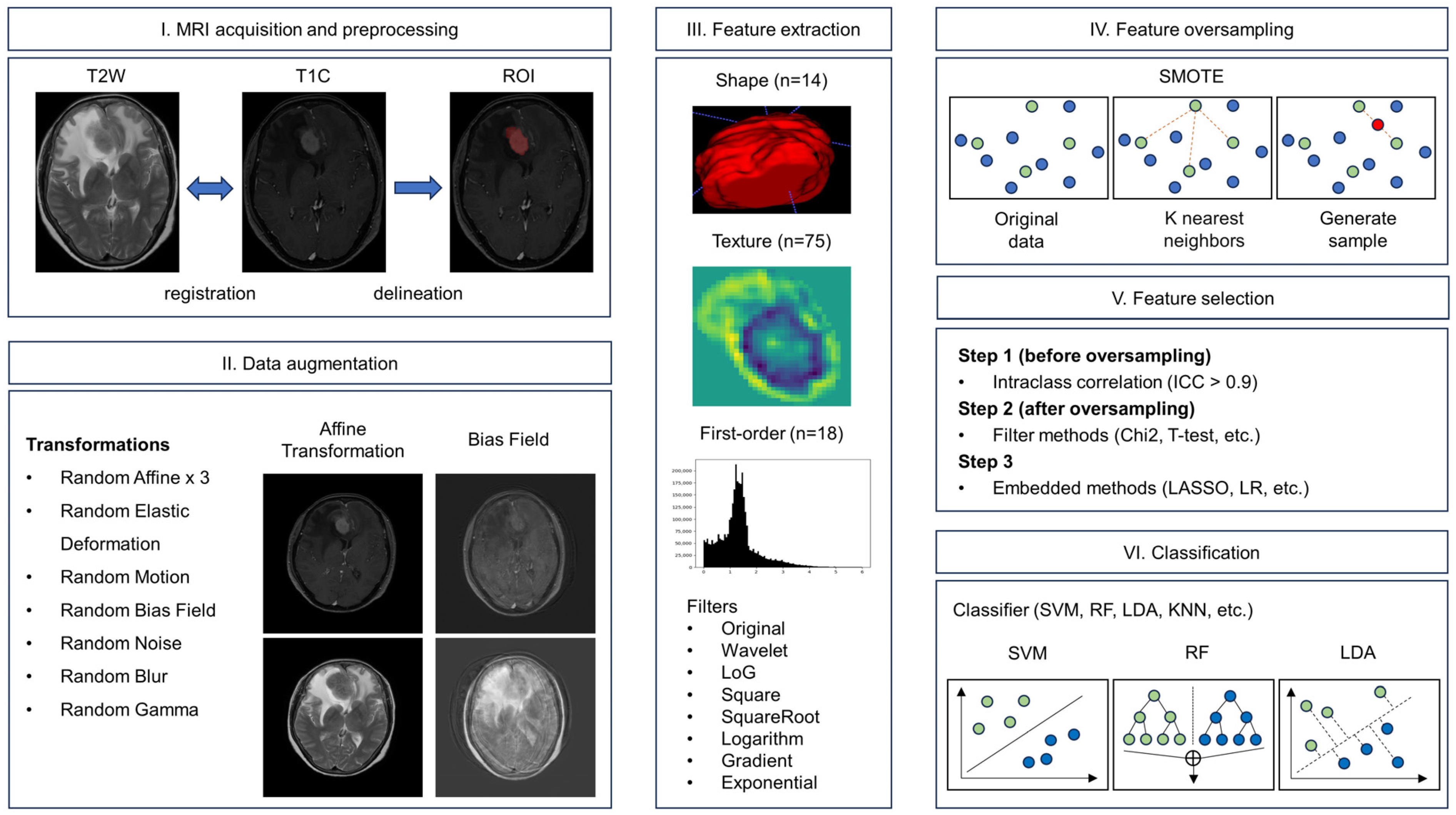
2.2. Imaging Registration and Label Delineation
2.3. Image-Level Augmentation
2.4. Radiomics Features Extraction
2.5. Feature-Level Augmentation
2.6. Feature Selection Methods
2.7. Classification Methods
2.8. Comparison of Augmentation Methods
2.9. Statistical Analysis
3. Results
3.1. Clinical Characteristics of the Patients
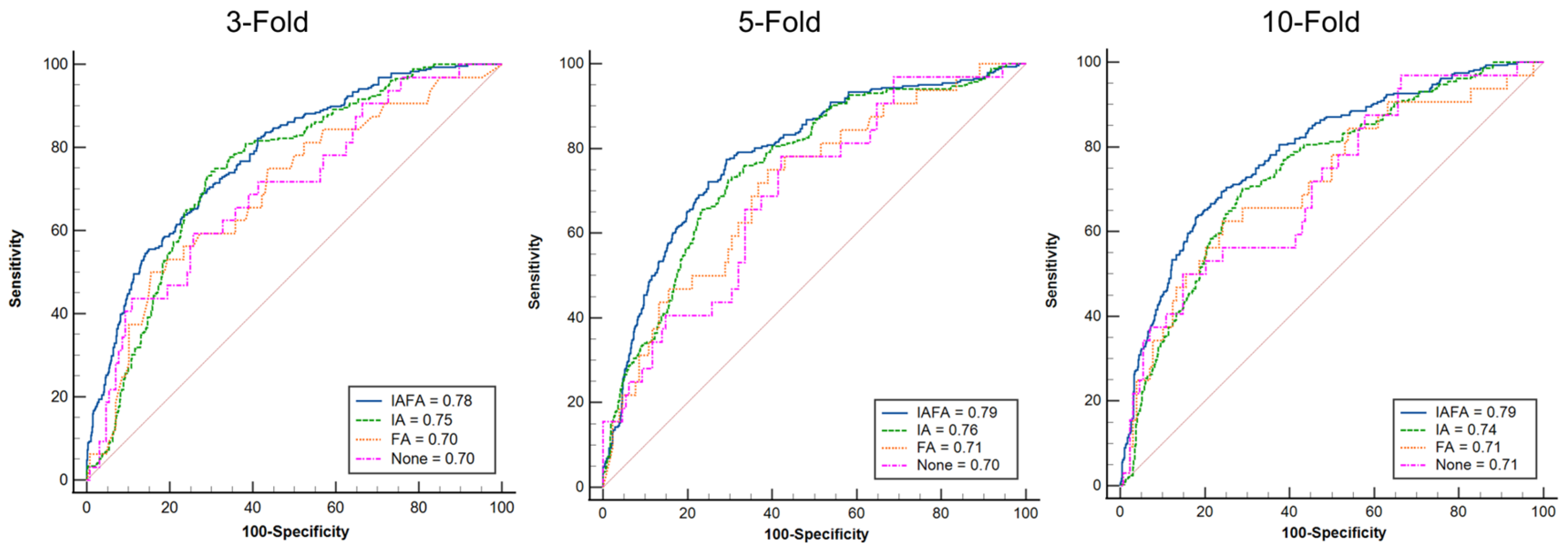
3.2. Comparison of the Best Performance of the Four Paired Settings
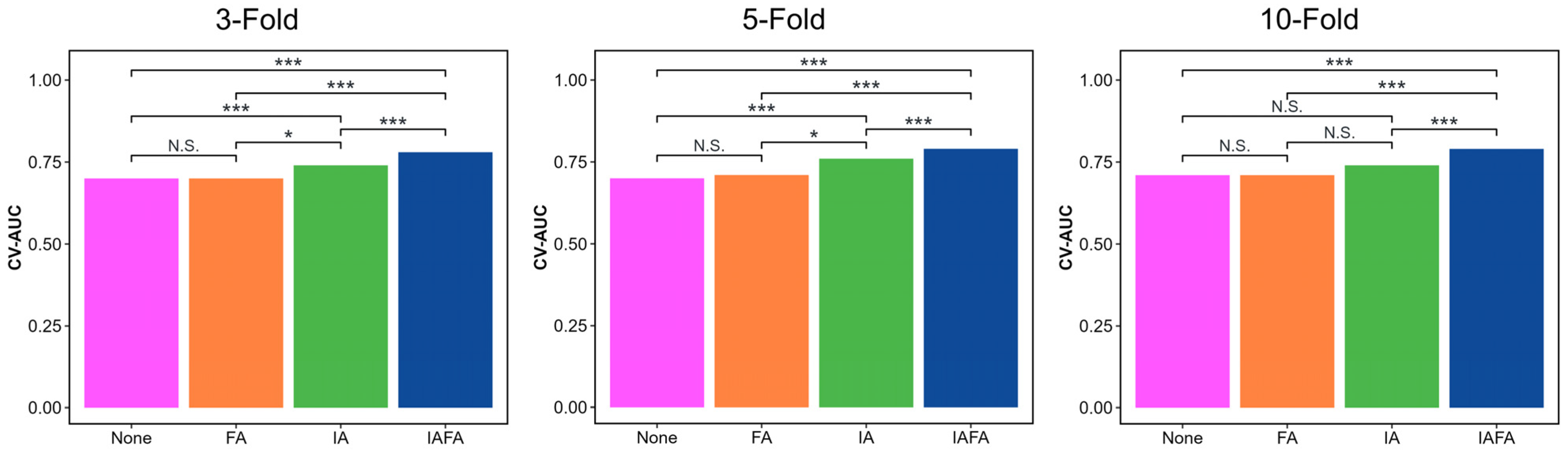
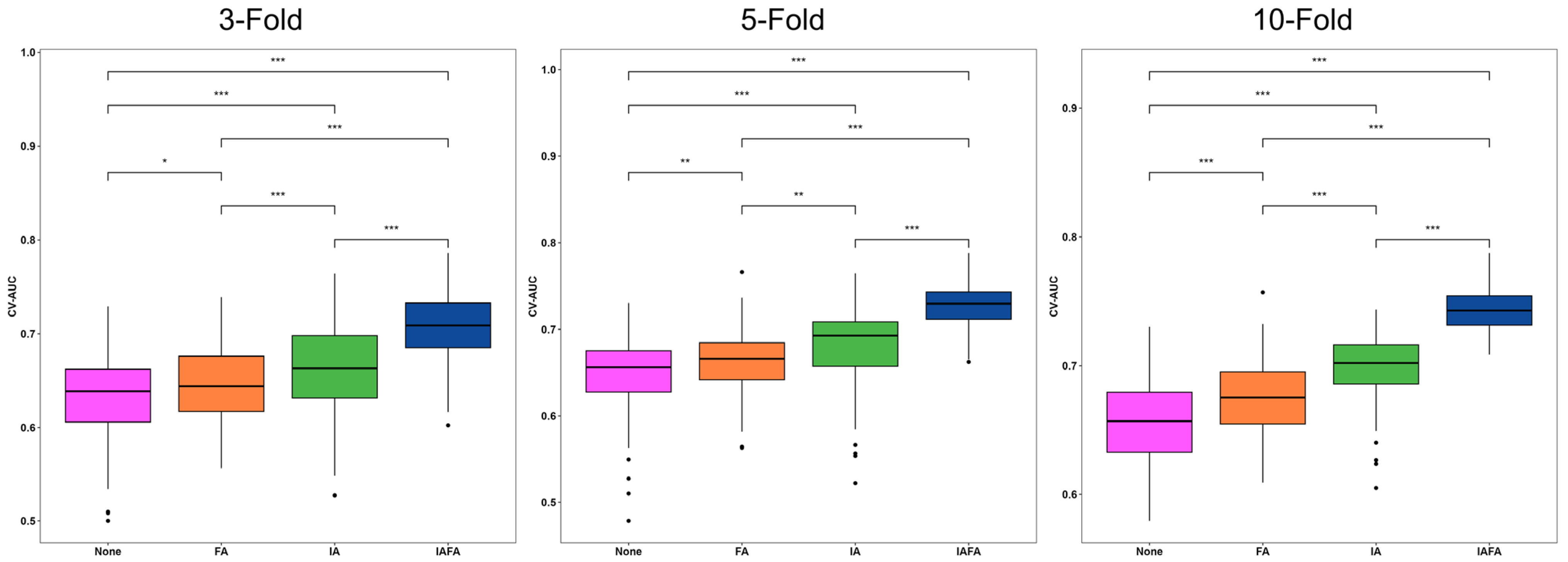
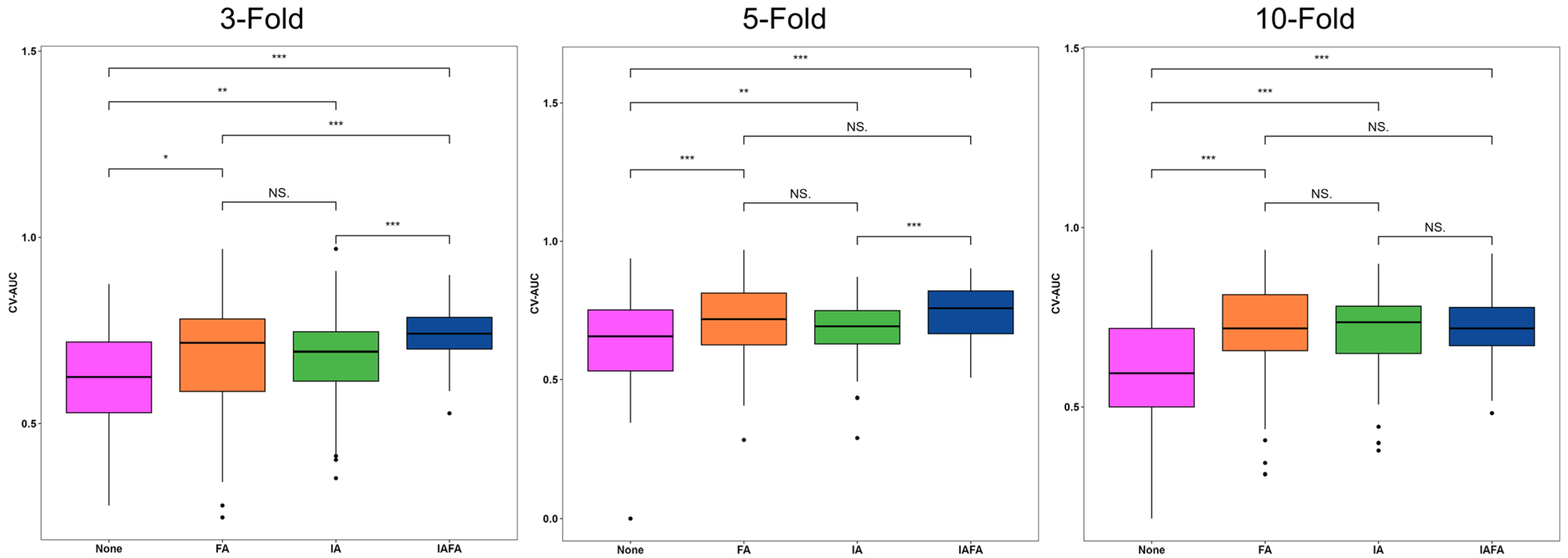
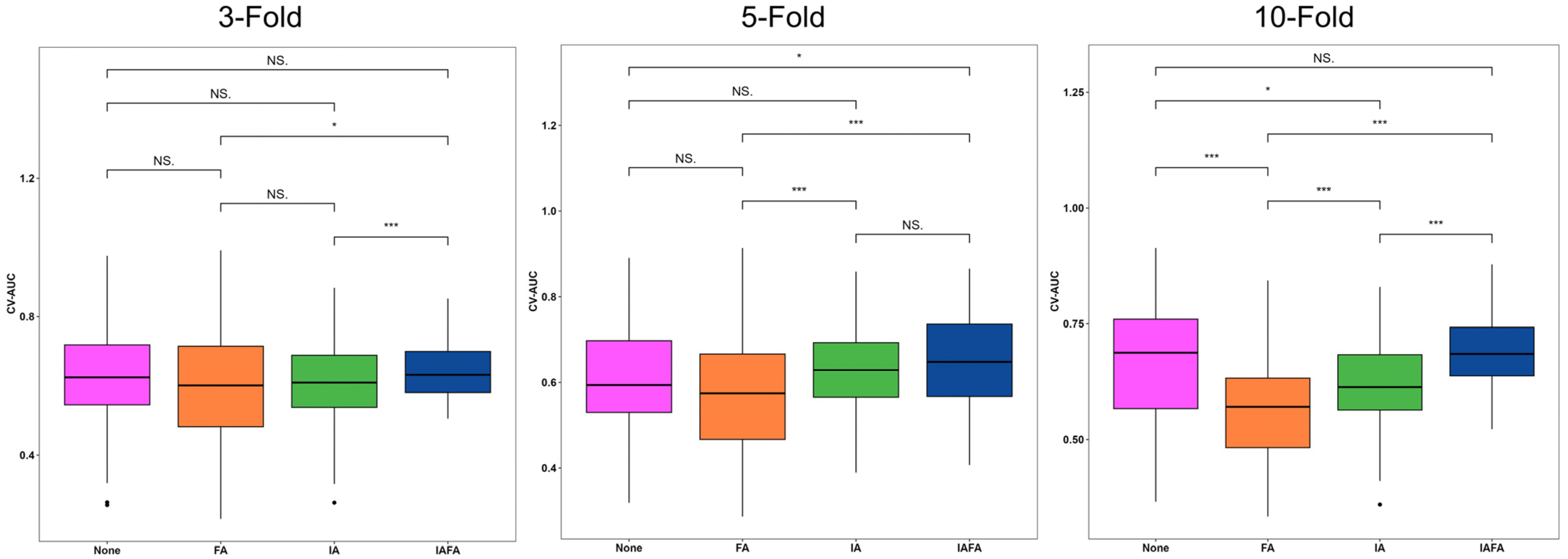
3.3. Comparison of the Distribution of the Performance Results of the Four Paired Settings
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ostrom, Q.T.; Cioffi, G.; Gittleman, H.; Patil, N.; Waite, K.; Kruchko, C.; Barnholtz-Sloan, J.S. CBTRUS statistical report: Primary brain and other central nervous system tumors diagnosed in the United States in 2012–2016. Neuro-Oncology 2019, 21, v1–v100. [Google Scholar] [CrossRef]
- Moliterno, J.; Cope, W.P.; Vartanian, E.D.; Reiner, A.S.; Kellen, R.; Ogilvie, S.Q.; Huse, J.T.; Gutin, P.H. Survival in patients treated for anaplastic meningioma. J. Neurosurg. 2015, 123, 23–30. [Google Scholar] [CrossRef] [PubMed]
- Goldbrunner, R.; Stavrinou, P.; Jenkinson, M.D.; Sahm, F.; Mawrin, C.; Weber, D.C.; Preusser, M.; Minniti, G.; Lund-Johansen, M.; Lefranc, F. EANO guideline on the diagnosis and management of meningiomas. Neuro-Oncology 2021, 23, 1821–1834. [Google Scholar] [CrossRef]
- Kshettry, V.R.; Ostrom, Q.T.; Kruchko, C.; Al-Mefty, O.; Barnett, G.H.; Barnholtz-Sloan, J.S. Descriptive epidemiology of World Health Organization grades II and III intracranial meningiomas in the United States. Neuro-Oncology 2015, 17, 1166–1173. [Google Scholar] [CrossRef]
- Ugga, L.; Spadarella, G.; Pinto, L.; Cuocolo, R.; Brunetti, A. Meningioma radiomics: At the nexus of imaging, pathology and biomolecular characterization. Cancers 2022, 14, 2605. [Google Scholar] [CrossRef] [PubMed]
- Louis, D.N.; Perry, A.; Reifenberger, G.; Von Deimling, A.; Figarella-Branger, D.; Cavenee, W.K.; Ohgaki, H.; Wiestler, O.D.; Kleihues, P.; Ellison, D.W. The 2016 World Health Organization classification of tumors of the central nervous system: A summary. Acta Neuropathol. 2016, 131, 803–820. [Google Scholar] [CrossRef] [PubMed]
- Kanazawa, T.; Minami, Y.; Jinzaki, M.; Toda, M.; Yoshida, K.; Sasaki, H. Preoperative prediction of solitary fibrous tumor/hemangiopericytoma and angiomatous meningioma using magnetic resonance imaging texture analysis. World Neurosurg. 2018, 120, e1208–e1216. [Google Scholar] [CrossRef]
- Koçak, B.; Durmaz E, Ş.; Ateş, E.; Kılıçkesmez, Ö. Radiomics with artificial intelligence: A practical guide for beginners. Diagn. Interv. Radiol. 2019, 25, 485. [Google Scholar] [CrossRef] [PubMed]
- Le, V.H.; Kha, Q.H.; Minh, T.N.T.; Nguyen, V.H.; Le, V.L.; Le, N.Q.K. Development and validation of ct-based radiomics signature for overall survival prediction in multi-organ cancer. J. Digit. Imaging 2023, 36, 911–922. [Google Scholar] [CrossRef]
- Aerts, H.J.; Velazquez, E.R.; Leijenaar, R.T.; Parmar, C.; Grossmann, P.; Carvalho, S.; Bussink, J.; Monshouwer, R.; Haibe-Kains, B.; Rietveld, D. Decoding tumour phenotype by noninvasive imaging using a quantitative radiomics approach. Nat. Commun. 2014, 5, 4006. [Google Scholar] [CrossRef]
- Chen, C.; Guo, X.; Wang, J.; Guo, W.; Ma, X.; Xu, J. The diagnostic value of radiomics-based machine learning in predicting the grade of meningiomas using conventional magnetic resonance imaging: A preliminary study. Front. Oncol. 2019, 9, 1338. [Google Scholar] [CrossRef] [PubMed]
- Park, Y.W.; Oh, J.; You, S.C.; Han, K.; Ahn, S.S.; Choi, Y.S.; Chang, J.H.; Kim, S.H.; Lee, S.-K. Radiomics and machine learning may accurately predict the grade and histological subtype in meningiomas using conventional and diffusion tensor imaging. Eur. Radiol. 2019, 29, 4068–4076. [Google Scholar] [CrossRef]
- Chu, H.; Lin, X.; He, J.; Pang, P.; Fan, B.; Lei, P.; Guo, D.; Ye, C. Value of MRI radiomics based on enhanced T1WI images in prediction of meningiomas grade. Acad. Radiol. 2021, 28, 687–693. [Google Scholar] [CrossRef]
- Arafat, M.Y.; Hoque, S.; Farid, D.M. Cluster-based under-sampling with random forest for multi-class imbalanced classification. In Proceedings of the 2017 11th International Conference on Software, Knowledge, Information Management and Applications (SKIMA), Malabe, Sri Lanka, 6–8 December 2017; pp. 1–6. [Google Scholar]
- Arafat, M.Y.; Hoque, S.; Xu, S.; Farid, D.M. An under-sampling method with support vectors in multi-class imbalanced data classification. Proceedings of 2019 the 13th International Conference on Software, Knowledge, Information Management and Applications (SKIMA), Island of Ulkulhas, Maldives, 26–28 August 2019; pp. 1–6. [Google Scholar]
- Chawla, N.V.; Bowyer, K.W.; Hall, L.O.; Kegelmeyer, W.P. SMOTE: Synthetic minority over-sampling technique. J. Artif. Intell. Res. 2002, 16, 321–357. [Google Scholar] [CrossRef]
- Mishra, A.K.; Roy, P.; Bandyopadhyay, S.; Das, S.K. Breast ultrasound tumour classification: A Machine Learning—Radiomics based approach. Expert Syst. 2021, 38, e12713. [Google Scholar] [CrossRef]
- Wang, G.; Wong, K.W.; Lu, J. AUC-based extreme learning machines for supervised and semi-supervised imbalanced classification. IEEE Trans. Syst. Man Cybern. Syst. 2020, 51, 7919–7930. [Google Scholar] [CrossRef]
- Kocak, B.; Durmaz, E.S.; Ates, E.; Ulusan, M.B. Radiogenomics in clear cell renal cell carcinoma: Machine learning–based high-dimensional quantitative CT texture analysis in predicting PBRM1 mutation status. Am. J. Roentgenol. 2019, 212, W55–W63. [Google Scholar] [CrossRef]
- Tsuchiya, M.; Masui, T.; Terauchi, K.; Yamada, T.; Katyayama, M.; Ichikawa, S.; Noda, Y.; Goshima, S. MRI-based radiomics analysis for differentiating phyllodes tumors of the breast from fibroadenomas. Eur. Radiol. 2022, 32, 4090–4100. [Google Scholar] [CrossRef]
- Götz, M.; Maier-Hein, K.H. Optimal statistical incorporation of independent feature stability information into radiomics studies. Sci. Rep. 2020, 10, 737. [Google Scholar] [CrossRef]
- Priya, S.; Aggarwal, T.; Ward, C.; Bathla, G.; Jacob, M.; Gerke, A.; Hoffman, E.A.; Nagpal, P. Radiomics side experiments and DAFIT approach in identifying pulmonary hypertension using Cardiac MRI derived radiomics based machine learning models. Sci. Rep. 2021, 11, 12686. [Google Scholar] [CrossRef]
- Makowski, M.R.; Bressem, K.K.; Franz, L.; Kader, A.; Niehues, S.M.; Keller, S.; Rueckert, D.; Adams, L.C. De novo radiomics approach using image augmentation and features from T1 mapping to predict Gleason scores in prostate cancer. Investig. Radiol. 2021, 56, 661–668. [Google Scholar] [CrossRef] [PubMed]
- Association, W.M. World Medical Association Declaration of Helsinki: Ethical principles for medical research involving human subjects. Jama 2013, 310, 2191–2194. [Google Scholar]
- Osborn, A.; Louis, D.; Poussaint, T.; Linscott, L.; Salzman, K. The 2021 world health organization classification of tumors of the central nervous system: What neuroradiologists need to know. Am. J. Neuroradiol. 2022, 43, 928–937. [Google Scholar] [CrossRef] [PubMed]
- Yushkevich, P.A.; Piven, J.; Hazlett, H.C.; Smith, R.G.; Ho, S.; Gee, J.C.; Gerig, G. User-guided 3D active contour segmentation of anatomical structures: Significantly improved efficiency and reliability. Neuroimage 2006, 31, 1116–1128. [Google Scholar] [CrossRef]
- Khan, A.R.; Khan, S.; Harouni, M.; Abbasi, R.; Iqbal, S.; Mehmood, Z. Brain tumor segmentation using K-means clustering and deep learning with synthetic data augmentation for classification. Microsc. Res. Tech. 2021, 84, 1389–1399. [Google Scholar] [CrossRef]
- Naseer, A.; Yasir, T.; Azhar, A.; Shakeel, T.; Zafar, K. Computer-aided brain tumor diagnosis: Performance evaluation of deep learner CNN using augmented brain MRI. Int. J. Biomed. Imaging 2021, 2021, 5513500. [Google Scholar] [CrossRef]
- Safdar, M.F.; Alkobaisi, S.S.; Zahra, F.T. A comparative analysis of data augmentation approaches for magnetic resonance imaging (MRI) scan images of brain tumor. Acta Inform. Medica 2020, 28, 29. [Google Scholar] [CrossRef]
- Pérez-García, F.; Sparks, R.; Ourselin, S. TorchIO: A Python library for efficient loading, preprocessing, augmentation and patch-based sampling of medical images in deep learning. Comput. Methods Programs Biomed. 2021, 208, 106236. [Google Scholar] [CrossRef]
- Van Griethuysen, J.J.; Fedorov, A.; Parmar, C.; Hosny, A.; Aucoin, N.; Narayan, V.; Beets-Tan, R.G.; Fillion-Robin, J.-C.; Pieper, S.; Aerts, H.J. Computational radiomics system to decode the radiographic phenotype. Cancer Res. 2017, 77, e104–e107. [Google Scholar] [CrossRef]
- Lemaître, G.; Nogueira, F.; Aridas, C.K. Imbalanced-learn: A python toolbox to tackle the curse of imbalanced datasets in machine learning. J. Mach. Learn. Res. 2017, 18, 559–563. [Google Scholar]
- Morin, O.; Chen, W.C.; Nassiri, F.; Susko, M.; Magill, S.T.; Vasudevan, H.N.; Wu, A.; Vallières, M.; Gennatas, E.D.; Valdes, G. Integrated models incorporating radiologic and radiomic features predict meningioma grade, local failure, and overall survival. Neuro-Oncol. Adv. 2019, 1, vdz011. [Google Scholar] [CrossRef] [PubMed]
- Speckter, H.; Radulovic, M.; Trivodaliev, K.; Vranes, V.; Joaquin, J.; Hernandez, W.; Mota, A.; Bido, J.; Hernandez, G.; Rivera, D. MRI radiomics in the prediction of the volumetric response in meningiomas after gamma knife radiosurgery. J. Neuro-Oncol. 2022, 159, 281–291. [Google Scholar] [CrossRef] [PubMed]
- Wang, C.; You, L.; Zhang, X.; Zhu, Y.; Zheng, L.; Huang, W.; Guo, D.; Dong, Y. A radiomics-based study for differentiating parasellar cavernous hemangiomas from meningiomas. Sci. Rep. 2022, 12, 15509. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Chen, J.-H.; Chen, T.-Y.; Lim, S.-W.; Wu, T.-C.; Kuo, Y.-T.; Ko, C.-C.; Su, M.-Y. Radiomics approach for prediction of recurrence in skull base meningiomas. Neuroradiology 2019, 61, 1355–1364. [Google Scholar] [CrossRef]
- Pedregosa, F.; Varoquaux, G.; Gramfort, A.; Michel, V.; Thirion, B.; Grisel, O.; Blondel, M.; Prettenhofer, P.; Weiss, R.; Dubourg, V. Scikit-learn: Machine learning in Python. J. Mach. Learn. Res. 2011, 12, 2825–2830. [Google Scholar]
- Chen, T.; Guestrin, C. Xgboost: A scalable tree boosting system. In Proceedings of the 22nd Acm Sigkdd International Conference on Knowledge Discovery and Data Mining, San Francisco, CA, USA, 13–17 August 2016; pp. 785–794. [Google Scholar]
- Urbanowicz, R.J.; Olson, R.S.; Schmitt, P.; Meeker, M.; Moore, J.H. Benchmarking relief-based feature selection methods for bioinformatics data mining. J. Biomed. Inform. 2018, 85, 168–188. [Google Scholar] [CrossRef]
- Ding, C.; Peng, H. Minimum redundancy feature selection from microarray gene expression data. J. Bioinform. Comput. Biol. 2005, 3, 185–205. [Google Scholar] [CrossRef]
- Van Rossum, G.; Drake, F.L. Python Reference Manual; Centrum voor Wiskunde en Informatica Amsterdam: Amsterdam, The Netherlands, 1995. [Google Scholar]
- DeLong, E.R.; DeLong, D.M.; Clarke-Pearson, D.L. Comparing the areas under two or more correlated receiver operating characteristic curves: A nonparametric approach. Biometrics 1988, 44, 837–845. [Google Scholar] [CrossRef]
- Schoonjans, F.; Zalata, A.; Depuydt, C.; Comhaire, F. MedCalc: A new computer program for medical statistics. Comput. Methods Programs Biomed. 1995, 48, 257–262. [Google Scholar] [CrossRef]
- Coroller, T.P.; Bi, W.L.; Huynh, E.; Abedalthagafi, M.; Aizer, A.A.; Greenwald, N.F.; Parmar, C.; Narayan, V.; Wu, W.W.; Miranda de Moura, S. Radiographic prediction of meningioma grade by semantic and radiomic features. PLoS ONE 2017, 12, e0187908. [Google Scholar] [CrossRef]
- Duan, C.; Li, N.; Li, Y.; Liu, F.; Wang, J.; Liu, X.; Xu, W. Comparison of different radiomic models based on enhanced T1-weighted images to predict the meningioma grade. Clin. Radiol. 2022, 77, e302–e307. [Google Scholar] [CrossRef] [PubMed]
- Duan, C.; Zhou, X.; Wang, J.; Li, N.; Liu, F.; Gao, S.; Liu, X.; Xu, W. A radiomics nomogram for predicting the meningioma grade based on enhanced T 1WI images. Br. J. Radiol. 2022, 95, 20220141. [Google Scholar] [CrossRef] [PubMed]
- Guo, Z.; Tian, Z.; Shi, F.; Xu, P.; Zhang, J.; Ling, C.; Zeng, Q. Radiomic features of the edema region may contribute to grading meningiomas with peritumoral edema. J. Magn. Reson. Imaging 2022, 58, 301–310. [Google Scholar] [CrossRef] [PubMed]
- Hamerla, G.; Meyer, H.-J.; Schob, S.; Ginat, D.T.; Altman, A.; Lim, T.; Gihr, G.A.; Horvath-Rizea, D.; Hoffmann, K.-T.; Surov, A. Comparison of machine learning classifiers for differentiation of grade 1 from higher gradings in meningioma: A multicenter radiomics study. Magn. Reson. Imaging 2019, 63, 244–249. [Google Scholar] [CrossRef]
- Han, Y.; Wang, T.; Wu, P.; Zhang, H.; Chen, H.; Yang, C. Meningiomas: Preoperative predictive histopathological grading based on radiomics of MRI. Magn. Reson. Imaging 2021, 77, 36–43. [Google Scholar] [CrossRef]
- Hu, J.; Zhao, Y.; Li, M.; Liu, J.; Wang, F.; Weng, Q.; Wang, X.; Cao, D. Machine learning-based radiomics analysis in predicting the meningioma grade using multiparametric MRI. Eur. J. Radiol. 2020, 131, 109251. [Google Scholar] [CrossRef]
- Laukamp, K.R.; Shakirin, G.; Baeßler, B.; Thiele, F.; Zopfs, D.; Hokamp, N.G.; Timmer, M.; Kabbasch, C.; Perkuhn, M.; Borggrefe, J. Accuracy of radiomics-based feature analysis on multiparametric magnetic resonance images for noninvasive meningioma grading. World Neurosurg. 2019, 132, e366–e390. [Google Scholar] [CrossRef]
- Lu, Y.; Liu, L.; Luan, S.; Xiong, J.; Geng, D.; Yin, B. The diagnostic value of texture analysis in predicting WHO grades of meningiomas based on ADC maps: An attempt using decision tree and decision forest. Eur. Radiol. 2019, 29, 1318–1328. [Google Scholar] [CrossRef]
- Duan, C.; Li, N.; Liu, X.; Cui, J.; Wang, G.; Xu, W. Performance comparison of 2D and 3D MRI radiomics features in meningioma grade prediction: A preliminary study. Front. Oncol. 2023, 13, 1157379. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Scanner | Philips Medical Systems | GE Medical System | ||||||
|---|---|---|---|---|---|---|---|---|
| Ingenia 1.5 T (n = 77) | Achieva 1.5 T (n = 9) | Achieva 3 T (n = 22) | SIGNA 3 T (n = 52) | |||||
| Parameters | T2W | T1C | T2W | T1C | T2W | T1C | T2W | T1C |
| Image Matrix | 672 × 672 | 320 × 320 or 480 × 480 | 512 × 512 | 288 × 288 | 1024 × 1024 | 224 × 224 or 256 × 256 or 288 × 288 | 512 × 512 | 512 × 512 |
| Slice no. | 25–30 | 180–320 | 23–25 | 180 | 25–29 | 170–191 | 25–35 | 276–392 |
| Spacing (mm) | (0.34, 0.34, 5.50) | (0.72, 0.72, 0.90) or (0.48, 0.48, 0.50) | (0.45, 0.45, 6.00) | (0.83, 0.83, 0.90) | (0.22, 0.22, 5.50 | (0.89, 0.89, 0.90) or (0.80, 0.80, 0.90) | 0.45, 0.45, 0.55 | 0.45, 0.45, 0.50 |
| Slice Thickness (mm) | 5 | 1–2 | 5 | 1.8 | 5 | 1.8 | 5 | 1 |
| TR (ms) | 5000–7000 | 25 or 33 | 4500–5000 | 25 | 2000–3100 | 25 | 3900–5100 | 6.10–6.20 or 11.70 |
| TE (ms) | 100 | 6–6.50 or 9.21 | 100 | 4.00–4.20 | 80 | 2.20–2.50 | 73–80 | 1.80–1.90 |
| Acquisition Matrix | 384 × 299 or 384 × 254 or 384 × 227) | 256 × 256 | 372 × 279 | 268 × 268 | 512 × 390 or 420 × 335 | 224 × 222 or 256 × 256 | 460 × 460 or 416 × 416 | 256 × 256 |
| Flip Angle (°) | 90 | 30 | 90 | 30 | 90 | 30 | 142 | 12 |
| Low-Grade | High-Grade | p-Value | ||
|---|---|---|---|---|
| WHO Grade I | WHO Grade II | WHO Grade III | ||
| Number (n) | 129 | 29 | 2 | - |
| Age (mean ± standard deviation, SD) | 62.33 ± 10.35 | 64.00 ± 13.60 | 73.00 ± 6.36 | 0.11 |
| Gender (n, %) | 0.11 | |||
| Male | 43, 72.88 | 14, 23.73 | 2, 3.39 | |
| Female | 86, 85.15 | 15, 14.85 | 0, 0 | |
| Brain invasion | 0 | 13 | 1 | - |
| The Proposed IAFA Method | |||
|---|---|---|---|
| Data Size | 160 Cases (129 Low Grade, 31 High Grade) | ||
| Folds | 3 | 5 | 10 |
| Best trial in 100 repetitions | |||
| Best combination | CHSQ, LASSO, and LR | CHSQ, LASSO, and LR | CHSQ, LASSO, and LR |
| Selected feature number | 7–9 | 4–9 | 7–10 |
| Mean AUC | 0.75 | 0.79 | 0.80 |
| Naïve train–test split AUC, range (train–test split) | 0.68–0.88 (2:1) | 0.66–0.94 (4:1) | 0.62–0.99 (9:1) |
| CV-AUC | 0.78 | 0.79 | 0.79 |
| CV-Sensitivity | 0.72 | 0.76 | 0.63 |
| CV-Specificity | 0.69 | 0.71 | 0.82 |
| 100 repetitions | |||
| CV-AUC, mean (95% CI) | 0.71 (0.70–0.72) | 0.73 (0.72–0.74) | 0.74 (0.74–0.75) |
| CV-AUC, range | 0.62–0.78 | 0.66–0.79 | 0.68–0.79 |
| Best Paired CV-AUC | ||||
|---|---|---|---|---|
| Setting | None | FA | IA | IAFA |
| 3-Fold | 0.70 | 0.70 | 0.74 | 0.78 |
| 5-Fold | 0.69 | 0.71 | 0.76 | 0.79 |
| 10-Fold | 0.71 | 0.71 | 0.74 | 0.79 |
| Mean (Standard Deviation, SD) | p-Value | |||||
|---|---|---|---|---|---|---|
| None | FA | IA | IAFA | |||
| 3-Fold | CV-AUC | 0.64 (0.04) | 0.65 (0.04) | 0.66 (0.05) | 0.71 (0.03) | <0.01 |
| CV-Sensitivity | 0.62 (0.14) | 0.67 (0.15) | 0.68 (0.11) | 0.74 (0.08) | <0.01 | |
| CV-Specificity | 0.63 (0.14) | 0.60 (0.16) | 0.60 (0.12) | 0.65 (0.09) | 0.18 | |
| 5-Fold | CV-AUC | 0.65 (0.05) | 0.66 (0.04) | 0.68 (0.05) | 0.73 (0.03) | <0.01 |
| CV-Sensitivity | 0.64 (0.17) | 0.72 (0.13) | 0.69 (0.10) | 0.75 (0.09) | <0.01 | |
| CV-Specificity | 0.61 (0.13) | 0.57 (0.14) | 0.63 (0.10) | 0.65 (0.10) | 0.23 | |
| 10-Fold | CV-AUC | 0.66 (0.04) | 0.68 (0.03) | 0.70 (0.03) | 0.74 (0.02) | <0.01 |
| CV-Sensitivity | 0.61 (0.14) | 0.71 (0.13) | 0.71 (0.10) | 0.72 (0.09) | <0.01 | |
| CV-Specificity | 0.66 (0.13) | 0.56 (0.11) | 0.62 (0.10) | 0.69 (0.08) | 0.82 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cai, Z.; Wong, L.M.; Wong, Y.H.; Lee, H.L.; Li, K.Y.; So, T.Y. Dual-Level Augmentation Radiomics Analysis for Multisequence MRI Meningioma Grading. Cancers 2023, 15, 5459. https://doi.org/10.3390/cancers15225459
Cai Z, Wong LM, Wong YH, Lee HL, Li KY, So TY. Dual-Level Augmentation Radiomics Analysis for Multisequence MRI Meningioma Grading. Cancers. 2023; 15(22):5459. https://doi.org/10.3390/cancers15225459
Chicago/Turabian StyleCai, Zongyou, Lun M. Wong, Ye Heng Wong, Hok Lam Lee, Kam Yau Li, and Tiffany Y. So. 2023. "Dual-Level Augmentation Radiomics Analysis for Multisequence MRI Meningioma Grading" Cancers 15, no. 22: 5459. https://doi.org/10.3390/cancers15225459