
Impact of Region-of-Interest Size on the Diagnostic Performance of Shear Wave Elastography in Differentiating Thyroid Nodules
 , and
, and
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. SWE Evaluation and Measurement
2.3. Statistical Analysis
3. Results
3.1. Patients
3.2. Comparison of SWE Elasticity Metrics in the Malignant Nodules, Benign Nodules, and Normal Subjects Groups
3.3. Comparison of SWE Elasticity Metrics in Three ROIs in the Malignant Nodules, Benign Nodules, and Normal Subjects Groups
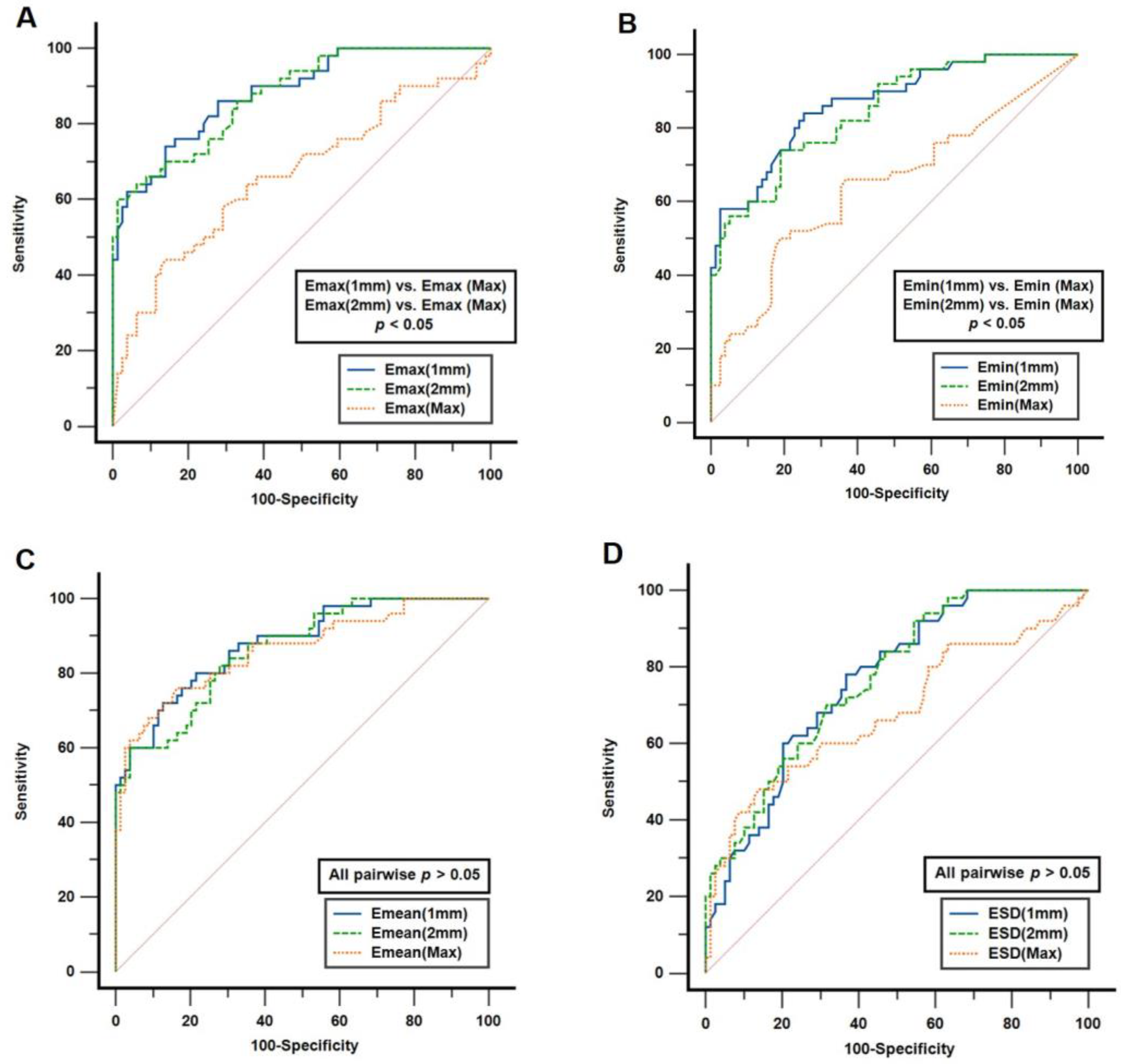
3.4. Assessment of the Diagnostic Performance of SWE Elasticity Metrics in Distinguishing between Malignant and Benign Nodules
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bercoff, J.; Tanter, M.; Fink, M. Supersonic shear imaging: A new technique for soft tissue elasticity mapping. IEEE Trans. Ultrason. Ferroelectr. Freq. Control 2004, 51, 396–409. [Google Scholar] [CrossRef] [PubMed]
- Tanter, M.; Bercoff, J.; Athanasiou, A.; Deffieux, T.; Gennisson, J.-L.; Montaldo, G.; Muller, M.; Tardivon, A.; Fink, M. Quantitative Assessment of Breast Lesion Viscoelasticity: Initial Clinical Results Using Supersonic Shear Imaging. Ultrasound Med. Biol. 2008, 34, 1373–1386. [Google Scholar] [CrossRef] [PubMed]
- Sebag, F.; Vaillant-Lombard, J.; Berbis, J.; Griset, V.; Henry, J.F.; Petit, P.; Oliver, C. Shear Wave Elastography: A New Ultrasound Imaging Mode for the Differential Diagnosis of Benign and Malignant Thyroid Nodules. J. Clin. Endocrinol. Metab. 2010, 95, 5281–5288. [Google Scholar] [CrossRef] [PubMed]
- Bhatia, K.S.S.; Tong, C.S.L.; Cho, C.C.M.; Yuen, E.H.Y.; Lee, Y.Y.P.; Ahuja, A.T. Shear wave elastography of thyroid nodules in routine clinical practice: Preliminary observations and utility for detecting malignancy. Eur. Radiol. 2012, 22, 2397–2406. [Google Scholar] [CrossRef] [PubMed]
- Veyrieres, J.B.; Albarel, F.; Lombard, J.V.; Berbis, J.; Sebag, F.; Oliver, C.; Petit, P. A threshold value in Shear Wave elastography to rule out malignant thyroid nodules: A reality? Eur. J. Radiol. 2012, 81, 3965–3972. [Google Scholar] [CrossRef]
- Park, A.Y.; Son, E.J.; Han, K.; Youk, J.H.; Kim, J.-A.; Park, C.S. Shear wave elastography of thyroid nodules for the prediction of malignancy in a large scale study. Eur. J. Radiol. 2015, 84, 407–412. [Google Scholar] [CrossRef]
- Brandenstein, M.; Wiesinger, I.; Künzel, J.; Hornung, M.; Stroszczynski, C.; Jung, E.-M. Multiparametric Sonographic Imaging of Thyroid Lesions: Chances of B-Mode, Elastography and CEUS in Relation to Preoperative Histopathology. Cancers 2022, 14, 4745. [Google Scholar] [CrossRef]
- Chambara, N.; Lo, X.; Chow, T.C.; Lai, C.M.; Liu, S.Y.; Ying, M. Combined Shear Wave Elastography and EU TIRADS in Differentiating Malignant and Benign Thyroid Nodules. Cancers 2022, 14, 5521. [Google Scholar] [CrossRef]
- Xue, J.-p.; Kang, X.-y.; Miao, J.-w.; Zhang, Y.-x.; Li, H.-z.; Yao, F.-c.; Kang, C.-s. Analysis of the Influence of Thyroid Nodule Characteristics on the Results of Shear Wave Elastography. Front. Endocrinol. 2022, 13, 858565. [Google Scholar] [CrossRef]
- Moon, J.H.; Hwang, J.-Y.; Park, J.S.; Koh, S.H.; Park, S.-Y. Impact of region of interest (ROI) size on the diagnostic performance of shear wave elastography in differentiating solid breast lesions. Acta Radiol. 2017, 59, 657–663. [Google Scholar] [CrossRef]
- Youk, J.H.; Son, E.J.; Han, K.; Gweon, H.M.; Kim, J.-A. Performance of shear-wave elastography for breast masses using different region-of-interest (ROI) settings. Acta Radiol. 2017, 59, 789–797. [Google Scholar] [CrossRef]
- Bulum, A.; Ivanac, G.; Divjak, E.; Biondić Špoljar, I.; Džoić Dominković, M.; Bojanić, K.; Lucijanić, M.; Brkljačić, B. Elastic Modulus and Elasticity Ratio of Malignant Breast Lesions with Shear Wave Ultrasound Elastography: Variations with Different Region of Interest and Lesion Size. Diagnostics 2021, 11, 1015. [Google Scholar] [CrossRef]
- Sun, Y.-M.; Dong, H.; Du, Z.-Y.; Yang, Z.-L.; Zhao, C.; Chong, J.; Li, P. The effect of regions-of-interest and elasticity modulus selection on differentiating benign and malignant cervical lymph nodes with shear wave elastography. Clinics 2020, 75, e1691. [Google Scholar] [CrossRef] [PubMed]
- Lahtinen, O.; Pulkkinen, M.; Sironen, R.; Vanninen, R.; Rautiainen, S. 2D-shear wave elastography in the evaluation of suspicious superficial inguinal lymph nodes: Reproducibility and region of interest selection. PLoS ONE 2022, 17, e0265802. [Google Scholar] [CrossRef]
- Filho, R.H.C.; Pereira, F.L.; Iared, W. Diagnostic Accuracy Evaluation of Two-Dimensional Shear Wave Elastography in the Differentiation Between Benign and Malignant Thyroid Nodules. J. Ultrasound Med. 2020, 39, 1729–1741. [Google Scholar] [CrossRef] [PubMed]
- Suh, C.H.; Choi, Y.J.; Baek, J.H.; Lee, J.H. The diagnostic performance of shear wave elastography for malignant cervical lymph nodes: A systematic review and meta-analysis. Eur. Radiol. 2017, 27, 222–230. [Google Scholar] [CrossRef] [PubMed]
- Yeon, E.K.; Sohn, Y.-M.; Seo, M.; Kim, E.-J.; Eun, Y.-G.; Park, W.S.; Yun, S.J. Diagnostic performance of a combination of shear wave elastography and B-mode ultrasonography in differentiating benign from malignant thyroid nodules. Clin. Exp. Otorhinolaryngol. 2020, 13, 186–193. [Google Scholar]
- Kim, H.J.; Kwak, M.K.; Choi, I.H.; Jin, S.Y.; Park, H.K.; Byun, D.W.; Suh, K.; Yoo, M.H. Utility of shear wave elastography to detect papillary thyroid carcinoma in thyroid nodules: Efficacy of the standard deviation elasticity. Korean J. Intern. Med. 2019, 34, 850–857. [Google Scholar] [CrossRef]
- Han, R.J.; Du, J.; Li, F.H.; Zong, H.R.; Wang, J.D.; Shen, Y.L.; Zhou, Q.Y. Comparisons and Combined Application of Two-Dimensional and Three-Dimensional Real-time Shear Wave Elastography in Diagnosis of Thyroid Nodules. J. Cancer 2019, 10, 1975–1984. [Google Scholar] [CrossRef]
- Chung, S.R.; Ahn, H.S.; Choi, Y.J.; Lee, J.Y.; Yoo, R.-E.; Lee, Y.J.; Kim, J.Y.; Sung, J.Y.; Kim, J.-h.; Baek, J.H. Diagnostic Performance of the Modified Korean Thyroid Imaging Reporting and Data System for Thyroid Malignancy: A Multicenter Validation Study. Korean J. Radiol. 2021, 22, 1579–1586. [Google Scholar] [CrossRef]
- Foncea, C.G.; Popescu, A.; Lupusoru, R.; Fofiu, R.; Sirli, R.; Danila, M.; Sporea, I. Comparative study between pSWE and 2D-SWE techniques integrated in the same ultrasound machine, with Transient Elastography as the reference method. Med. Ultrason. 2020, 22, 13–19. [Google Scholar] [CrossRef] [PubMed]
- Kang, H.-J.; Lee, J.Y.; Lee, K.B.; Joo, I.; Suh, K.-S.; Lee, H.-K.; Han, J.K. Addition of Reliability Measurement Index to Point Shear Wave Elastography: Prospective Validation via Diagnostic Performance and Reproducibility. Ultrasound Med. Biol. 2019, 45, 1594–1602. [Google Scholar] [CrossRef] [PubMed]
- Mulabecirovic, A.; Mjelle, A.B.; Gilja, O.H.; Vesterhus, M.; Havre, R.F. Repeatability of shear wave elastography in liver fibrosis phantoms—Evaluation of five different systems. PLoS ONE 2018, 13, e0189671. [Google Scholar] [CrossRef]
- Kiwan, C.; Donggeon, K.; Zaegyoo, H.; Hyoung-Ki, L. A reliability index of shear wave speed measurement for shear wave elastography. In Proceedings of the 2015 IEEE International Ultrasonics Symposium (IUS), Taipei, Taiwan, 21–24 October 2015; pp. 1–4. [Google Scholar]
- Öztürk, V.S.; Ertekin, E. Diagnostic performance of shear wave elastography and diffusion-weighted magneticresonance imaging in cervical lymph nodes: A comparative study. Turk. J. Med. Sci. 2021, 51, 2931–2942. [Google Scholar] [CrossRef]
- Oruk, Y.E.; Çildağ, M.B.; Karaman, C.Z.; Çildağ, S. Effectiveness of ultrasonography and shear wave sonoelastography in Sjögren syndrome with salivary gland involvement. Ultrasonography 2021, 40, 584–593. [Google Scholar] [CrossRef]
- Duan, S.B.; Yu, J.; Li, X.; Han, Z.Y.; Zhai, H.Y.; Liang, P. Diagnostic value of two-dimensional shear wave elastography in papillary thyroid microcarcinoma. OncoTargets Ther. 2016, 9, 1311–1317. [Google Scholar] [CrossRef]
- Prasad, S.B.; Lin, A.K.; Guppy-Coles, K.B.; Stanton, T.; Krishnasamy, R.; Whalley, G.A.; Thomas, L.; Atherton, J.J. Diastolic Dysfunction Assessed Using Contemporary Guidelines and Prognosis Following Myocardial Infarction. J. Am. Soc. Echocardiogr. 2018, 31, 1127–1136. [Google Scholar] [CrossRef]
- Koo, T.K.; Li, M.Y. A Guideline of Selecting and Reporting Intraclass Correlation Coefficients for Reliability Research. J. Chiropr. Med. 2016, 15, 155–163. [Google Scholar] [CrossRef]
- Dobruch-Sobczak, K.; Zalewska, E.B.; Gumińska, A.; Słapa, R.Z.; Mlosek, K.; Wareluk, P.; Jakubowski, W.; Dedecjus, M. Diagnostic Performance of Shear Wave Elastography Parameters Alone and in Combination with Conventional B-Mode Ultrasound Parameters for the Characterization of Thyroid Nodules: A Prospective, Dual-Center Study. Ultrasound Med. Biol. 2016, 42, 2803–2811. [Google Scholar] [CrossRef]
- He, Y.-P.; Xu, H.-X.; Wang, D.; Li, X.-L.; Ren, W.-W.; Zhao, C.-K.; Bo, X.-W.; Liu, B.-J.; Yue, W.-W. First experience of comparisons between two different shear wave speed imaging systems in differentiating malignant from benign thyroid nodules. Clin. Hemorheol. Microcirc. 2017, 65, 349–361. [Google Scholar] [CrossRef]
- Tan, S.; Sun, P.-F.; Xue, H.; Fu, S.; Zhang, Z.-P.; Mei, F.; Miao, L.-Y.; Wang, X.-H. Evaluation of thyroid micro-carcinoma using shear wave elastography: Initial experience with qualitative and quantitative analysis. Eur. J. Radiol. 2021, 137, 109571. [Google Scholar] [CrossRef]
- Yoo, H.W.; Kim, S.G.; Jang, J.Y.; Yoo, J.J.; Jeong, S.W.; Kim, Y.S.; Kim, B.S. Two-dimensional shear wave elastography for assessing liver fibrosis in patients with chronic liver disease: A prospective cohort study. Korean J. Intern. Med. 2022, 37, 285–293. [Google Scholar] [CrossRef]
- Foncea, C.; Popescu, A.; Lupusoru, R.; Cotrau, R.; Bende, F.; Moga, T.; Sirli, R.; Sporea, I. PErformance of a 2D-SWE Method for the Diagnosis of Liver Fibrosis Using Transient Elastography as Reference Method. Ultrasound Med. Biol. 2022, 48, S31. [Google Scholar] [CrossRef]
- Yoo, J.; Lee, J.M.; Joo, I.; Yoon, J.H. Assessment of liver fibrosis using 2-dimensional shear wave elastography: A prospective study of intra- and inter-observer repeatability and comparison with point shear wave elastography. Ultrasonography 2020, 39, 52–59. [Google Scholar] [CrossRef] [PubMed]
- Haugen, B.R.; Alexander, E.K.; Bible, K.C.; Doherty, G.M.; Mandel, S.J.; Nikiforov, Y.E.; Pacini, F.; Randolph, G.W.; Sawka, A.M.; Schlumberger, M.; et al. 2015 American Thyroid Association Management Guidelines for Adult Patients with Thyroid Nodules and Differentiated Thyroid Cancer: The American Thyroid Association Guidelines Task Force on Thyroid Nodules and Differentiated Thyroid Cancer. Thyroid Off. J. Am. Thyroid Assoc. 2016, 26, 1–133. [Google Scholar] [CrossRef]
- Kleiman, D.A.; Beninato, T.; Soni, A.; Shou, Y.; Zarnegar, R.; Fahey, T.J. Does Bethesda Category Predict Aggressive Features in Malignant Thyroid Nodules? Ann. Surg. Oncol. 2013, 20, 3484–3490. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Malignant (n = 50) | Benign (n = 79) | Normal Subjects (n = 78) | p | |
|---|---|---|---|---|
| Sex (F:M) | 38:12 | 63:16 | 57:21 | 0.62 C |
| Age (y/o) | 46.6 ± 10.5 | 48.3 ± 11.4 | 44.5 ± 11.9 | 0.19 A |
| 44.0 | 47.0 | 44.5 | ||
| (29–67) | (18–82) | (18–81) | ||
| Max. dia. (mm) | 12.9 ± 9.1 | 25.6 ± 12.5 | - | <0.05 M |
| 9.4 | 24.7 | |||
| (5.8–49.6) | (6.5–50.2) | |||
| Volume (mL) | 1.9 ± 6.1 | 6.7 ± 8.1 | - | <0.05 M |
| 0.30 | 3.6 | |||
| (0.06–41.7) | (0.06–35.1) |
| SWE Indices | Malignant (M) (n = 50) | ICC (95% CI) | Benign (B) (n = 79) | ICC (95% CI) | Normal Subjects (N) (n = 78) | p |
|---|---|---|---|---|---|---|
| Emax(Max) | 112.90 ± 43.69 105.20 (17.9–179.3) | 1.00 (0.99–1.00) | 89.26 ± 31.41 86.80 (28.20–179.3) | 0.98 (0.95–0.99) | 65.20 ± 31.18 61.40 (22.60–173.6) | <0.001 A (all pairwise p < 0.05) * |
| Emax(1mm) | 88.49 ± 37.50 87.80 (26.37–167.77) | 0.92 (0.81–0.97) | 37.72 ± 20.38 33.67 (5.40–91.73) | 0.96 (0.90–0.98) | 31.83 ± 13.98 29.03 (13.17–73.17) | <0.001 K (M vs. B; M vs. N) * |
| Emax(2mm) | 95.42 ± 36.72 94.17 (34.70–167.77) | 0.96 (0.90–0.98) | 45.15 ± 21.50 41.43 (11.07–94.83) | 0.95 (0.87–0.98) | 38.04 ± 16.85 33.88 (14.80–83.30) | <0.001 K (all pairwise p < 0.05) * |
| p | 0.007 A (Max vs. 1 mm; Max vs. 2 mm) * | <0.001 A (Max vs. 1 mm; Max vs. 2 mm) * | <0.001 K (all pairwise p < 0.05) * | |||
| Emin(Max) | 20.40 ± 19.03 18.70 (0.70–81.9) | 0.97 (0.92–0.99) | 11.11 ± 11.18 7.10 (0.70–48) | 0.97 (0.92–0.99) | 12.77 ± 5.39 12.20 (0.70–26.8) | 0.002 K (B vs. M; B vs. N) * |
| Emin(1mm) | 69.85 ± 34.99 68.68 (15.50–146.33) | 0.88 (0.73–0.95) | 27.92 ± 15.62 24.53 (3.97–72.47) | 0.97 (0.91–0.99) | 24.34 ± 10.21 22.30 (9.67–56.93) | <0.001 K (M vs. B; M vs. N) * |
| Emin(2mm) | 57.01 ± 29.0 57.65 (13.87–124.73) | 0.90 (0.77–0.96) | 24.80 ± 14.13 20.93 (5.63–63.30) | 0.95 (0.88–0.98) | 21.88 ± 8.55 20.50 (7.53–45.87) | <0.001 K (M vs. B; M vs. N) * |
| p | <0.001 K (Max vs. 1 mm; Max vs. 2 mm) * | <0.001 K (Max vs. 1 mm; Max vs. 2 mm) * | <0.001 K (Max vs. 1 mm; Max vs. 2 mm) * | |||
| Emean(Max) | 67.19 ± 24.38 71.70 (22.90–118) | 0.97 (0.93–0.99) | 34.25 ± 15.04 32.40 (10.90–77.1) | 0.99 (0.97–1.00) | 28.48 ± 11.40 27.15 (11.80–59.3) | <0.001 K (all pairwise p < 0.05) * |
| Emean(1mm) | 79.62 ± 36.66 77.68 (20.17–162.07) | 0.89 (0.74–0.95) | 32.67 ± 17.90 28.30 (4.57–77.90) | 0.96 (0.89–0.98) | 27.92 ± 11.89 25.15 (10.90–64.40) | <0.001 K (M vs. B; M vs. N) * |
| Emean(2mm) | 76.75 ± 33.74 74.90 (23.47–143.43) | 0.95 (0.88–0.98) | 33.65 ± 17.63 30.70 (8.33–80.83) | 0.95 (0.89–0.9891) | 28.95 ± 12.01 26.00 (10.97–59.13) | <0.001 K (M vs. B; M vs. N) * |
| p | 0.240 K | 0.566K | 0.838K | |||
| ESD(Max) | 23.62 ± 14.61 19.80 (4.40–60.4) | 0.99 (0.97–1.00) | 14.75 ± 7.58 13.50 (3.60–51.5) | 1.00 (0.99–1.00) | 10.31 ± 6.62 9.30 (2.20–27.9) | <0.001 K (all pairwise p < 0.05) * |
| ESD(1mm) | 4.79 ± 2.72 4.33 (1.33–13.37) | 0.86 (0.69–0.94) | 2.60 ± 1.95 2.13 (0.23–8.43) | 0.89 (0.75–0.96) | 1.90 ± 1.29 1.47 (0.40–5.27) | <0.001 K (all pairwise p < 0.05) * |
| ESD(2mm) | 9.52 ± 5.72 7.87 (3.07–29.33) | 0.65 (0.30–0.85) | 5.02 ± 2.92 4.87 (0.63–14.03) | 0.84 (0.63–0.93) | 4.07 ± 2.70 3.18 (0.67–12.37) | <0.001 K (all pairwise p < 0.05) * |
| p | <0.001 K (all pairwise p < 0.05) * | <0.001 K (all pairwise p < 0.05) * | <0.001 K (all pairwise p < 0.05) * |
| SWE Indices | AUC (95% CI) | Optimal Cutoff (kPa) | Sensitivity (%) (95% CI) | Specificity (%) (95% CI) |
|---|---|---|---|---|
| Emax(Max) | 0.664 (0.575–0.745) | >117.9 | 44.0 (30.0–58.7) | 86.1 (76.5–92.8) |
| Emax(1mm) | 0.883 (0.814–0.933) | >61.4 | 74.0 (59.7–85.4) | 86.1 (76.5–92.8) |
| Emax(2mm) | 0.877 (0.807–0.928) | >88.0 | 60.0 (45.2–73.6) | 98.7 (93.1–100.0) |
| Emin(Max) | 0.646 (0.557–0.728) | >18.4 | 50.0 (35.5–64.5) | 81.0 (70.6–89.0) |
| Emin(1mm) | 0.867 (0.797–0.921) | >37.0 | 84.0 (70.9–92.8) | 74.7 (63.6–83.8) |
| Emin(2mm) | 0.846 (0.772–0.903) | >37.4 | 74.0 (59.7–85.4) | 81.0 (70.6–89.0) |
| Emean(Max) | 0.863 (0.791–0.917) | >50.6 | 76.0 (61.8–86.9) | 83.5 (73.5–90.9) |
| Emean(1mm) | 0.879 (0.810–0.930) | >54.8 | 72.0 (57.5–83.8) | 87.3 (78.0–93.8) |
| Emean(2mm) | 0.863 (0.791–0.917) | >64.2 | 60.0 (45.2–73.6) | 96.2 (89.3–99.2) |
| ESD(Max) | 0.682 (0.594–0.761) | >20.9 | 48.0 (33.7–62.6) | 86.1 (76.5–92.8) |
| ESD(1mm) | 0.764 (0.681–0.834) | >2.6 | 78.0 (64.0–88.5) | 63.3 (51.7–73.9) |
| ESD(2mm) | 0.769 (0.687–0.839) | >6.2 | 70.0 (55.4–82.1) | 68.4 (56.9–78.4) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cheng, K.-L.; Lai, P.-H.; Su, C.-L.; Baek, J.H.; Lee, H.-L. Impact of Region-of-Interest Size on the Diagnostic Performance of Shear Wave Elastography in Differentiating Thyroid Nodules. Cancers 2023, 15, 5214. https://doi.org/10.3390/cancers15215214
Cheng K-L, Lai P-H, Su C-L, Baek JH, Lee H-L. Impact of Region-of-Interest Size on the Diagnostic Performance of Shear Wave Elastography in Differentiating Thyroid Nodules. Cancers. 2023; 15(21):5214. https://doi.org/10.3390/cancers15215214
Chicago/Turabian StyleCheng, Kai-Lun, Pin-Hsien Lai, Chun-Lang Su, Jung Hwan Baek, and Hsiang-Lin Lee. 2023. "Impact of Region-of-Interest Size on the Diagnostic Performance of Shear Wave Elastography in Differentiating Thyroid Nodules" Cancers 15, no. 21: 5214. https://doi.org/10.3390/cancers15215214