
Patients with Advanced Pancreatic Cancer Treated with Mistletoe and Hyperthermia in Addition to Palliative Chemotherapy: A Retrospective Single-Center Analysis
 ,
,
Abstract
:Simple Summary
Abstract
1. Introduction
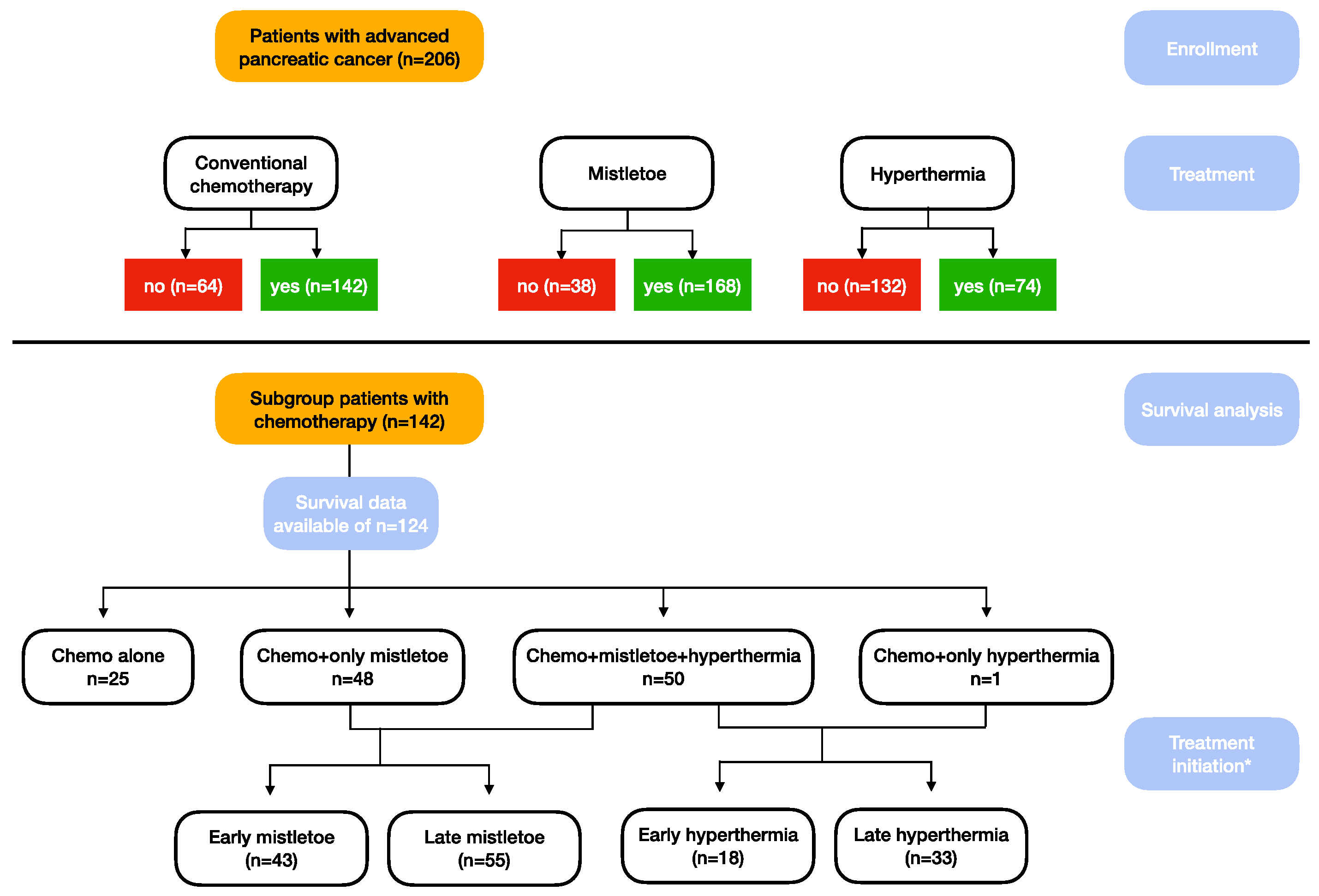
2. Materials and Methods
2.1. Baseline Characteristics
2.2. Mistletoe Therapy and Hyperthermia
2.3. Statistical Analysis
3. Results
3.1. Baseline Characteristics of Patients Receiving Chemotherapy with or without Mistletoe or Hyperthermia (n = 142)
3.2. Treatment Regimens
3.3. Integrative Therapies
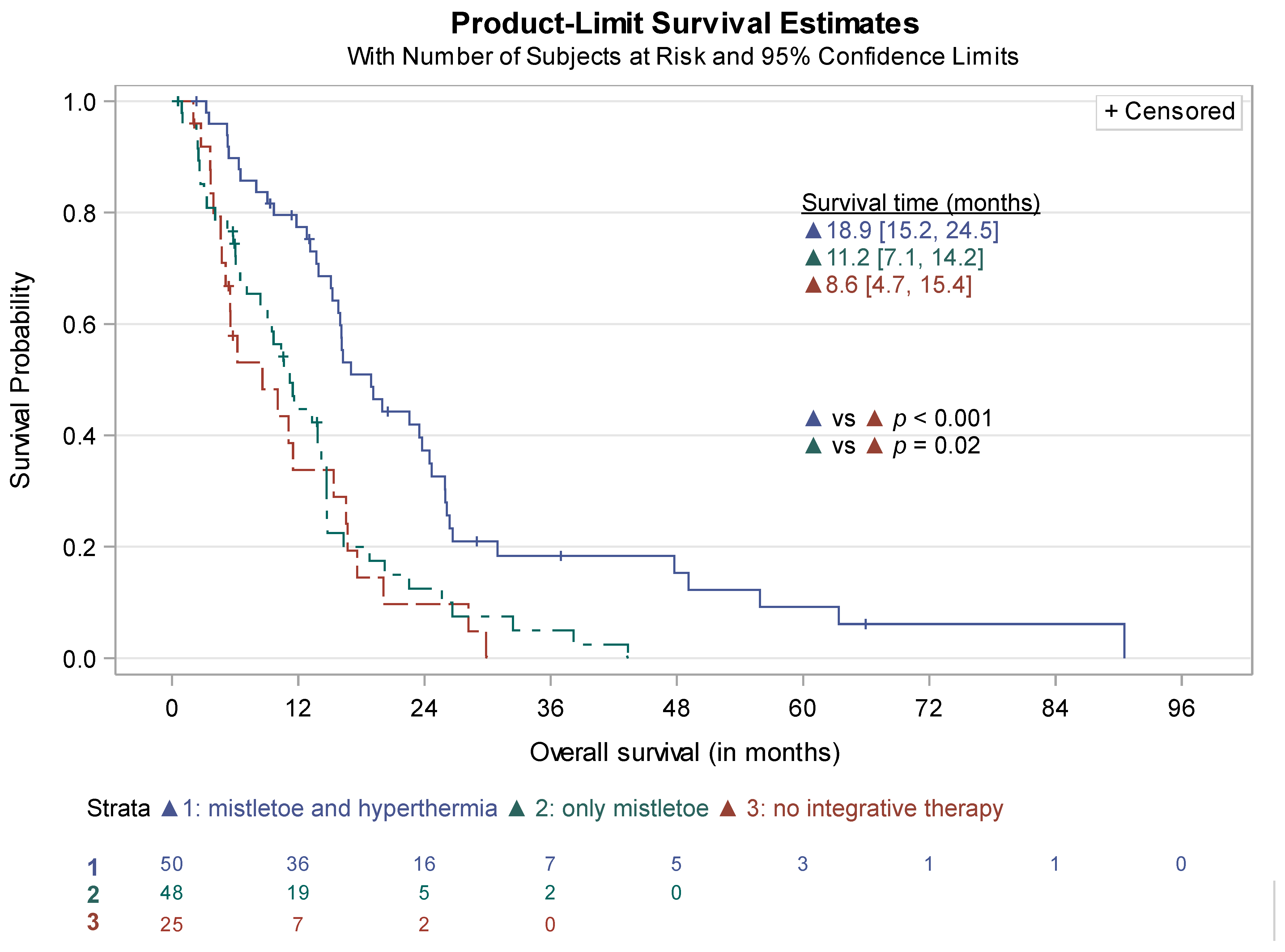
3.4. Survival Analysis
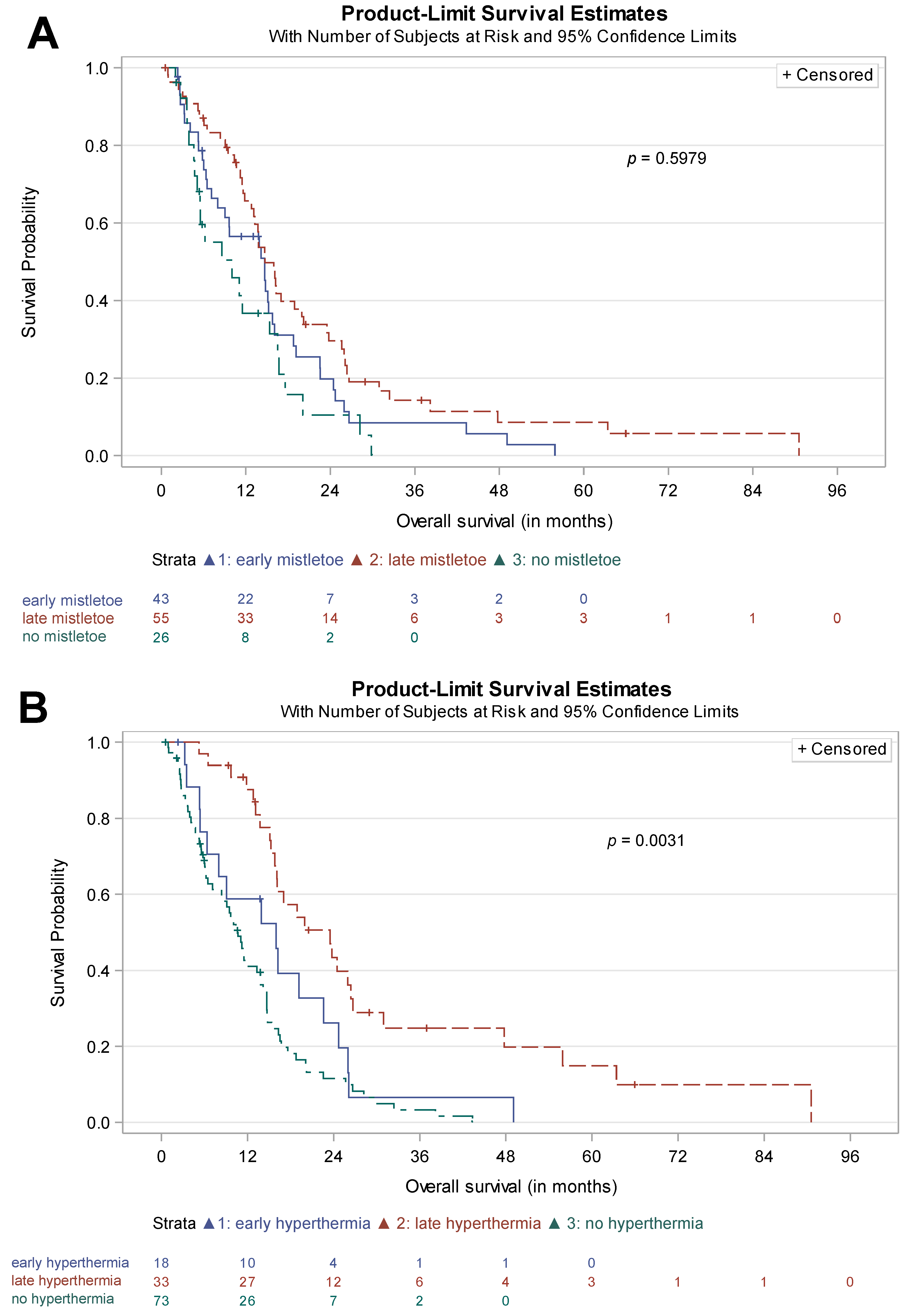
3.5. Time of Treatment Initiation
4. Discussion
Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Cai, J.; Chen, H.; Lu, M.; Zhang, Y.; Lu, B.; You, L.; Zhang, T.; Dai, M.; Zhao, Y. Advances in the Epidemiology of Pancreatic Cancer: Trends, Risk Factors, Screening, and Prognosis. Cancer Lett. 2021, 520, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Seufferlein, T.; Mayerle, J.; Böck, S.; Brunner, T.; Ettrich, T.J.; Grenacher, L.; Gress, T.M.; Hackert, T.; Heinemann, V.; Kestler, A.; et al. S3-Leitlinie zum exokrinen Pankreaskarzinom—Langversion 2.0—Dezember 2021—AWMF-Registernummer: 032/010OL. Z. Gastroenterol. 2022, 60, e812–e909. [Google Scholar] [CrossRef]
- Petrelli, F.; Comito, T.; Ghidini, A.; Torri, V.; Scorsetti, M.; Barni, S. Stereotactic Body Radiation Therapy for Locally Advanced Pancreatic Cancer: A Systematic Review and Pooled Analysis of 19 Trials. Int. J. Radiat. Oncol. Biol. Phys. 2017, 97, 313–322. [Google Scholar] [CrossRef] [PubMed]
- Potters, L.; Kavanagh, B.; Galvin, J.M.; Hevezi, J.M.; Janjan, N.A.; Larson, D.A.; Mehta, M.P.; Ryu, S.; Steinberg, M.; Timmerman, R.; et al. American Society for Therapeutic Radiology and Oncology (ASTRO) and American College of Radiology (ACR) Practice Guideline for the Performance of Stereotactic Body Radiation Therapy. Int. J. Radiat. Oncol. Biol. Phys. 2010, 76, 326–332. [Google Scholar] [CrossRef]
- Buwenge, M.; Macchia, G.; Arcelli, A.; Frakulli, R.; Fuccio, L.; Guerri, S.; Grassi, E.; Cammelli, S.; Cellini, F.; Morganti, A.G. Stereotactic Radiotherapy of Pancreatic Cancer: A Systematic Review on Pain Relief. J. Pain Res. 2018, 11, 2169–2178. [Google Scholar] [CrossRef] [PubMed]
- Bauer, M.R.; Bright, E.E.; MacDonald, J.J.; Cleary, E.H.; Hines, O.J.; Stanton, A.L. Quality of Life in Patients with Pancreatic Cancer and Their Caregivers: A Systematic Review. Pancreas 2018, 47, 368. [Google Scholar] [CrossRef]
- Carrato, A.; Falcone, A.; Ducreux, M.; Valle, J.W.; Parnaby, A.; Djazouli, K.; Alnwick-Allu, K.; Hutchings, A.; Palaska, C.; Parthenaki, I. A Systematic Review of the Burden of Pancreatic Cancer in Europe: Real-World Impact on Survival, Quality of Life and Costs. J. Gastrointest. Cancer 2015, 46, 201–211. [Google Scholar] [CrossRef] [PubMed]
- Liu, W.; Narayanan, S.; Cohen, L.; Lopez, G. Integrative Medicine in Pancreatic Cancer. In Pancreatic Cancer: A Multidisciplinary Approach; Bhutani, M.S., Katz, M.H.G., Maitra, A., Herman, J.M., Wolff, R.A., Eds.; Springer International Publishing: Cham, Switzerland, 2022; pp. 375–389. ISBN 978-3-031-05724-3. [Google Scholar]
- Leitlinienprogramm Onkologie (Deutsche Krebsgesellschaft, Deutsche Krebshilfe, AWMF): Komplementärmedizin in der Behandlung von onkologischen PatientInnen, Langversion 1.0, 2021, AWMF Registernummer: 032/055OL. Available online: https:///www.leitlinienprogramm-onkologie.de/leitlinien/komplementaermedizin (accessed on 5 August 2023).
- Lopez, G.; Lee, R.; Garcia, M.K.; Chaoul, A.; Cohen, L. Integrative Oncology. In Advances in Cancer Survivorship Management; Foxhall, L.E., Rodriguez, M.A., Eds.; MD Anderson Cancer Care Series; Springer: New York, NY, USA, 2015; pp. 433–448. ISBN 978-1-4939-0986-5. [Google Scholar]
- Boeck, S.; Bruns, C.J.; Sargent, M.; Schäfer, C.; Seufferlein, T.; Jauch, K.-W.; Heinemann, V. Current Oncological Treatment of Patients with Pancreatic Cancer in Germany: Results from a National Survey on Behalf of the Arbeitsgemeinschaft Internistische Onkologie and the Chirurgische Arbeitsgemeinschaft Onkologie of the Germany Cancer Society. OCL 2009, 77, 40–48. [Google Scholar] [CrossRef]
- Védie, A.-L.; Neuzillet, C. Pancreatic Cancer: Best Supportive Care. Presse Médicale 2019, 48, e175–e185. [Google Scholar] [CrossRef]
- Ostermann, T.; Appelbaum, S.; Poier, D.; Boehm, K.; Raak, C.; Büssing, A. A Systematic Review and Meta-Analysis on the Survival of Cancer Patients Treated with a Fermented Viscum Album L. Extract (Iscador): An Update of Findings. CMR 2020, 27, 260–271. [Google Scholar] [CrossRef]
- Loef, M.; Walach, H. Quality of Life in Cancer Patients Treated with Mistletoe: A Systematic Review and Meta-Analysis. BMC Complement. Med. Ther. 2020, 20, 227. [Google Scholar] [CrossRef] [PubMed]
- Freuding, M.; Keinki, C.; Micke, O.; Buentzel, J.; Huebner, J. Mistletoe in Oncological Treatment: A Systematic Review. J. Cancer Res. Clin. Oncol. 2019, 145, 695–707. [Google Scholar] [CrossRef] [PubMed]
- Kienle, G.S.; Kiene, H. Review Article: Influence of Viscum Album L (European Mistletoe) Extracts on Quality of Life in Cancer Patients: A Systematic Review of Controlled Clinical Studies. Integr. Cancer Ther. 2010, 9, 142–157. [Google Scholar] [CrossRef] [PubMed]
- Wider, B.; Rostock, M.; Huntley, A.; van Ackeren, G.; Horneber, M. Mistletoe Extracts for Cancer Treatment. Cochrane Database Syst. Rev. 2022, 2022, CD014782. [Google Scholar] [CrossRef]
- Horneber, M.; van Ackeren, G.; Linde, K.; Rostock, M. Mistletoe Therapy in Oncology. Cochrane Database Syst. Rev. 2008, 2008, CD003297. [Google Scholar] [CrossRef] [PubMed]
- Büssing, A.; Raak, C.; Ostermann, T. Quality of Life and Related Dimensions in Cancer Patients Treated with Mistletoe Extract (Iscador): A Meta-Analysis. Evid.-Based Complement. Altern. Med. 2011, 2012, e219402. [Google Scholar] [CrossRef]
- Sulyok, I.; Fleischmann, E.; Stift, A.; Roth, G.; Lebherz-Eichinger, D.; Kasper, D.; Spittler, A.; Kimberger, O. Effect of Preoperative Fever-Range Whole-Body Hyperthermia on Immunological Markers in Patients Undergoing Colorectal Cancer Surgery†. Br. J. Anaesth. 2012, 109, 754–761. [Google Scholar] [CrossRef]
- Bull, J.M.C.; Scott, G.L.; Strebel, F.R.; Nagle, V.L.; Oliver, D.; Redwine, M.; Rowe, R.W.; Ahn, C.W.; Koch, S.M. Fever-Range Whole-Body Thermal Therapy Combined with Cisplatin, Gemcitabine, and Daily Interferon-α: A Description of a Phase I-II Protocol. Int. J. Hyperth. 2008, 24, 649–662. [Google Scholar] [CrossRef]
- Issels, R.D.; Lindner, L.H.; Verweij, J.; Wessalowski, R.; Reichardt, P.; Wust, P.; Ghadjar, P.; Hohenberger, P.; Angele, M.; Salat, C.; et al. Effect of Neoadjuvant Chemotherapy Plus Regional Hyperthermia on Long-Term Outcomes Among Patients with Localized High-Risk Soft Tissue Sarcoma: The EORTC 62961-ESHO 95 Randomized Clinical Trial. JAMA Oncol. 2018, 4, 483–492. [Google Scholar] [CrossRef]
- Anderson, K.G.; Stromnes, I.M.; Greenberg, P.D. Obstacles Posed by the Tumor Microenvironment to T Cell Activity: A Case for Synergistic Therapies. Cancer Cell 2017, 31, 311–325. [Google Scholar] [CrossRef]
- Liu, Q.; Liao, Q.; Zhao, Y. Chemotherapy and Tumor Microenvironment of Pancreatic Cancer. Cancer Cell Int. 2017, 17, 68. [Google Scholar] [CrossRef] [PubMed]
- Chand, S.; O’Hayer, K.; Blanco, F.F.; Winter, J.M.; Brody, J.R. The Landscape of Pancreatic Cancer Therapeutic Resistance Mechanisms. Int. J. Biol. Sci. 2016, 12, 273–282. [Google Scholar] [CrossRef]
- Mahmood, J.; Shukla, H.D.; Soman, S.; Samanta, S.; Singh, P.; Kamlapurkar, S.; Saeed, A.; Amin, N.P.; Vujaskovic, Z. Immunotherapy, Radiotherapy, and Hyperthermia: A Combined Therapeutic Approach in Pancreatic Cancer Treatment. Cancers 2018, 10, 469. [Google Scholar] [CrossRef] [PubMed]
- Mahmood, J.; Alexander, A.A.; Samanta, S.; Kamlapurkar, S.; Singh, P.; Saeed, A.; Carrier, F.; Cao, X.; Shukla, H.D.; Vujaskovic, Z. A Combination of Radiotherapy, Hyperthermia, and Immunotherapy Inhibits Pancreatic Tumor Growth and Prolongs the Survival of Mice. Cancers 2020, 12, 1015. [Google Scholar] [CrossRef] [PubMed]
- Vaupel, P. (Ed.) Water-Filtered Infrared A (wIRA) Irradiation: From Research to Clinical Settings; Springer Nature: Berlin/Heidelberg, Germany, 2022. [Google Scholar]
- Liebl, C.M.; Kutschan, S.; Dörfler, J.; Käsmann, L.; Hübner, J. Systematic Review about Complementary Medical Hyperthermia in Oncology. Clin. Exp. Med. 2022, 22, 519–565. [Google Scholar] [CrossRef]
- Fiorentini, G.; Sarti, D.; Gadaleta, C.D.; Ballerini, M.; Fiorentini, C.; Garfagno, T.; Ranieri, G.; Guadagni, S. A Narrative Review of Regional Hyperthermia: Updates From 2010 to 2019. Integr. Cancer Ther. 2020, 19, 1534735420932648. [Google Scholar] [CrossRef]
- Kok, H.P.; Cressman, E.N.K.; Ceelen, W.; Brace, C.L.; Ivkov, R.; Grüll, H.; ter Haar, G.; Wust, P.; Crezee, J. Heating Technology for Malignant Tumors: A Review. Int. J. Hyperth. 2020, 37, 711–741. [Google Scholar] [CrossRef]
- Datta, N.R.; Ordóñez, S.G.; Gaipl, U.S.; Paulides, M.M.; Crezee, H.; Gellermann, J.; Marder, D.; Puric, E.; Bodis, S. Local Hyperthermia Combined with Radiotherapy And-/or Chemotherapy: Recent Advances and Promises for the Future. Cancer Treat. Rev. 2015, 41, 742–753. [Google Scholar] [CrossRef]
- Skitzki, J.J.; Repasky, E.A.; Evans, S.S. Hyperthermia as an Immunotherapy Strategy for Cancer. Curr. Opin. Investig. Drugs 2009, 10, 550–558. [Google Scholar]
- Horowitz, M.; Robinson, S.D.M. Heat Shock Proteins and the Heat Shock Response during Hyperthermia and Its Modulation by Altered Physiological Conditions. In Progress in Brain Research; Sharma, H.S., Ed.; Neurobiology of Hyperthermia; Elsevier: Amsterdam, The Netherlands, 2007; Volume 162, pp. 433–446. [Google Scholar]
- Binder, R.J.; Srivastava, P.K. Peptides Chaperoned by Heat-Shock Proteins Are a Necessary and Sufficient Source of Antigen in the Cross-Priming of CD8+ T Cells. Nat. Immunol. 2005, 6, 593–599. [Google Scholar] [CrossRef]
- Wode, K.; Hök Nordberg, J.; Kienle, G.S.; Elander, N.O.; Bernhardson, B.-M.; Sunde, B.; Sharp, L.; Henriksson, R.; Fransson, P. Efficacy of Mistletoe Extract as a Complement to Standard Treatment in Advanced Pancreatic Cancer: Study Protocol for a Multicentre, Parallel Group, Double-Blind, Randomised, Placebo-Controlled Clinical Trial (MISTRAL). Trials 2020, 21, 783. [Google Scholar] [CrossRef] [PubMed]
- Lagendijk, J.J.W.; Van Rhoon, G.C.; Hornsleth, S.N.; Wust, P.; De Leeuw, A.C.C.; Schneider, C.J.; Van Ddk, J.D.P.; Van Der Zee, J.; Heek-Romanowski, R.V.; Rahman, S.A.; et al. Esho Quality Assurance Guidelines for Regional Hyperthermia. Int. J. Hyperth. 1998, 14, 125–133. [Google Scholar] [CrossRef] [PubMed]
- Wehner, H.; Wey, S.; Meyer, A. Whole-Body Hyperthermia Guideline; Deutsche Gesellschaft Für Hyperthermie e.V: Wilhelmshaven, Germany, 2018. [Google Scholar]
- Tröger, W.; Galun, D.; Reif, M.; Schumann, A.; Stankovic, N.; Milicevic, M. Quality of Life of Patients with Advanced Pancreatic Cancer During Treatment with Mistletoe. Dtsch. Arztebl. Int. 2014, 111, 493–502. [Google Scholar] [CrossRef]
- Tröger, W.; Galun, D.; Reif, M.; Schumann, A.; Stanković, N.; Milićević, M. Viscum album [L.] Extract Therapy in Patients with Locally Advanced or Metastatic Pancreatic Cancer: A Randomised Clinical Trial on Overall Survival. Eur. J. Cancer 2013, 49, 3788–3797. [Google Scholar] [CrossRef]
- Issels, R.D.; Boeck, S.; Pelzer, U.; Mansmann, U.; Ghadjar, P.; Lindner, L.H.; Albertsmeier, M.; Angele, M.K.; Schmidt, M.; Xu, Y.; et al. Regional Hyperthermia with Cisplatin Added to Gemcitabine versus Gemcitabine in Patients with Resected Pancreatic Ductal Adenocarcinoma: The HEAT Randomised Clinical Trial. Eur. J. Cancer 2023, 181, 155–165. [Google Scholar] [CrossRef] [PubMed]
- Wainberg, Z.A.; Melisi, D.; Macarulla, T.; Cid, R.P.; Chandana, S.R.; Fouchardière, C.D.L.; Dean, A.; Kiss, I.; Lee, W.J.; Goetze, T.O.; et al. NALIRIFOX versus Nab-Paclitaxel and Gemcitabine in Treatment-Naive Patients with Metastatic Pancreatic Ductal Adenocarcinoma (NAPOLI 3): A Randomised, Open-Label, Phase 3 Trial. Lancet 2023. Online ahead of print. [Google Scholar] [CrossRef]
- Conroy, T.; Desseigne, F.; Ychou, M.; Bouché, O.; Guimbaud, R.; Bécouarn, Y.; Adenis, A.; Raoul, J.-L.; Gourgou-Bourgade, S.; de la Fouchardière, C.; et al. FOLFIRINOX versus Gemcitabine for Metastatic Pancreatic Cancer. N. Engl. J. Med. 2011, 364, 1817–1825. [Google Scholar] [CrossRef]
- Von Hoff, D.D.; Ervin, T.; Arena, F.P.; Chiorean, E.G.; Infante, J.; Moore, M.; Seay, T.; Tjulandin, S.A.; Ma, W.W.; Saleh, M.N.; et al. Increased Survival in Pancreatic Cancer with Nab-Paclitaxel plus Gemcitabine. N. Engl. J. Med. 2013, 369, 1691–1703. [Google Scholar] [CrossRef]
- Klein-Brill, A.; Amar-Farkash, S.; Lawrence, G.; Collisson, E.A.; Aran, D. Comparison of FOLFIRINOX vs Gemcitabine Plus Nab-Paclitaxel as First-Line Chemotherapy for Metastatic Pancreatic Ductal Adenocarcinoma. JAMA Netw. Open 2022, 5, e2216199. [Google Scholar] [CrossRef]
- Hegewisch-Becker, S.; Aldaoud, A.; Wolf, T.; Krammer-Steiner, B.; Linde, H.; Scheiner-Sparna, R.; Hamm, D.; Jänicke, M.; Marschner, N.; TPK-Group (Tumour Registry Pancreatic Cancer). Results from the Prospective German TPK Clinical Cohort Study: Treatment Algorithms and Survival of 1174 Patients with Locally Advanced, Inoperable, or Metastatic Pancreatic Ductal Adenocarcinoma. Int. J. Cancer 2019, 144, 981–990. [Google Scholar] [CrossRef]
- Matthes, H.; Friedel, W.E.; Bock, P.R.; Zanker, K.S. Molecular Mistletoe Therapy: Friend or Foe in Established Anti-Tumor Protocols? A Multicenter, Controlled, Retrospective Pharmaco-Epidemiological Study in Pancreas Cancer. Curr. Mol. Med. 2010, 10, 430–439. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Patients Receiving Chemotherapy (n = 142) | ||
|---|---|---|
| Sex male, n (%) | 77 (54.2) | |
| Age at diagnosis, median (Q1;Q3) | 66.7 (59.6;73.0) | |
| Surgical treatment, n (%) | 42 (29.6) | |
| Tumor localization, n (%) | ||
| Pancreas head | 76 (53.5) | |
| Pancreas body | 31 (21.8) | |
| Pancreas tail | 39 (27.5) | |
| Unknown | 14 (9.9) | |
| Local recurrence, n (%) | 35 (24.7) | |
| Liver metastases, n (%) | 84 (59.2) | |
| Peritoneal metastases, n (%) | 56 (39.4) | |
| Lymph node metastases, n (%) | 46 (32.4) | |
| Lung metastases, n (%) | 41 (28.9) | |
| Others, n (%) | 34 (23.9) | |
| Adjuvant therapy, n (%) | 32 (22.5) | |
| Treatment Regimens | Patients Receiving Chemotherapy (n = 142) | |
|---|---|---|
| First line treatment, n (%) | 142 (100) | |
| Duration of therapy (days), median (Q1;Q3) | 90.0 (53.0;153.0) | |
| Discontinued, n (%) | 140 (98.6) | |
| Gemcitabine, n (%) | 43 (30.3) | |
| Gemcitabine/nab-Paclitaxel, n (%) | 48 (33.8) | |
| FOLFIRINOX, n (%) | 51 (35.9) | |
| Second line treatment, n (%) | 70 (49.3) | |
| Duration of therapy (days), median (Q1;Q3) | 61.0 (31.0;96.0) | |
| Discontinued, n (%) | 69 (48.6) | |
| Gemcitabine, n (%) | 33 (23.2) | |
| Gemcitabine/nab-Paclitaxel, n (%) | 27 (19.0) | |
| FOLFIRINOX, n (%) | 10 (7.0) | |
| Third line treatment, n (%) | 17 (12.0) | |
| Duration of therapy (days), median (Q1;Q3) | 89.5 (45.5;106.0) | |
| Discontinued, n (%) | 17 (12.0) | |
| Integrative Therapies | Patients Receiving Chemotherapy (n = 142) | ||
|---|---|---|---|
| (A) Mistletoe therapy, n (%) | 117 (82.4) | ||
| Treatment initiation after first diagnosis (months), median (Q1;Q3) | 4.0 (1.5;12.3) | ||
| Treatment initiation after diagnosis of metastatic spread (months), median (Q1;Q3) | 1.9 (0.5;6.1) | ||
| Duration of therapy (days), median (Q1;Q3) | 41.0 (8.0;213.0) | ||
| (B) Hyperthermia therapy, n (%) | 74 (52.1) | ||
| Treatment initiation after first diagnosis (months), median (Q1;Q3) | 8.9 (3.9;13.8) | ||
| Treatment initiation after diagnosis of metastatic spread (months), median (Q1;Q3) | 5.7 (2.2;10.9) | ||
| Duration of therapy (days), median (Q1;Q3) | 57.0 (1.0;208.0) | ||
| Number of treatment sessions, median (Q1;Q3) | 4.0 (1.0;6.5) | ||
| Whole body hyperthermia, n (%) | 60 (81.1) | ||
| Local hyperthermia, n (%) | 26 (35.1) | ||
| Pancreas/epigastrium, n (%) | 22 (84.6) | ||
| Lung, n (%) | 1 (3.8) | ||
| Others, n (%) | 8 (30.8) | ||
| Median Survival (Months) | 95% CI | ||
|---|---|---|---|
| Conroy et al. (2011) [43], multicenter, randomized, phase 2–3 trial comparing FOLFIRINOX to gemcitabine monotherapy | 11.1 | 9.0 to 13.1 | |
| Von Hoff et al. (2013) [44], multicenter, open-label, randomized, phase 3 study comparing gemcitabine/nab-paclitaxel to gemcitabine monotherapy | 8.5 | 7.9 to 9.5 | |
| Hegewisch-Becker et al. (2019) [46], prospective clinical cohort study using different regimens (German TPK) | 9.2 | 8.5 to 10.0 | |
| Klein-Brill et al. (2022) [45], retrospective cohort study | 9.3 | 8.7 to 9.8 | |
| Wainberg et al. (2023) [42], multicenter, open-label, randomized, phase 3 study comparing NALIRIFOX to gemcitabine/nab-paclitaxel | 11.1 | 10.0 to 12.1 | |
| Current data | |||
| Chemotherapy alone | 8.6 | 4.7 to 15.4 | |
| Chemotherapy + only mistletoe | 11.2 | 7.1 to 14.2 | |
| Chemotherapy + combination mistletoe/hyperthermia | 18.9 | 15.2 to 24.5 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hohneck, A.L.; Sadikaj, L.; Heinemann, L.; Schroeder, M.; Riess, H.; Gerhards, A.; Burkholder, I.; Heckel-Reusser, S.; Gottfried, J.; Hofheinz, R.-D. Patients with Advanced Pancreatic Cancer Treated with Mistletoe and Hyperthermia in Addition to Palliative Chemotherapy: A Retrospective Single-Center Analysis. Cancers 2023, 15, 4929. https://doi.org/10.3390/cancers15204929
Hohneck AL, Sadikaj L, Heinemann L, Schroeder M, Riess H, Gerhards A, Burkholder I, Heckel-Reusser S, Gottfried J, Hofheinz R-D. Patients with Advanced Pancreatic Cancer Treated with Mistletoe and Hyperthermia in Addition to Palliative Chemotherapy: A Retrospective Single-Center Analysis. Cancers. 2023; 15(20):4929. https://doi.org/10.3390/cancers15204929
Chicago/Turabian StyleHohneck, Anna Lena, Largsi Sadikaj, Lara Heinemann, Maik Schroeder, Hartmut Riess, Annette Gerhards, Iris Burkholder, Stefan Heckel-Reusser, Julia Gottfried, and Ralf-Dieter Hofheinz. 2023. "Patients with Advanced Pancreatic Cancer Treated with Mistletoe and Hyperthermia in Addition to Palliative Chemotherapy: A Retrospective Single-Center Analysis" Cancers 15, no. 20: 4929. https://doi.org/10.3390/cancers15204929