
Cost–Utility and Budget Impact Analyses of Oral Chemotherapy for Stage III Colorectal Cancer: Real-World Evidence after Policy Implementation in Thailand
 , , , ,
, , , ,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Methods
2.1. Overall Description
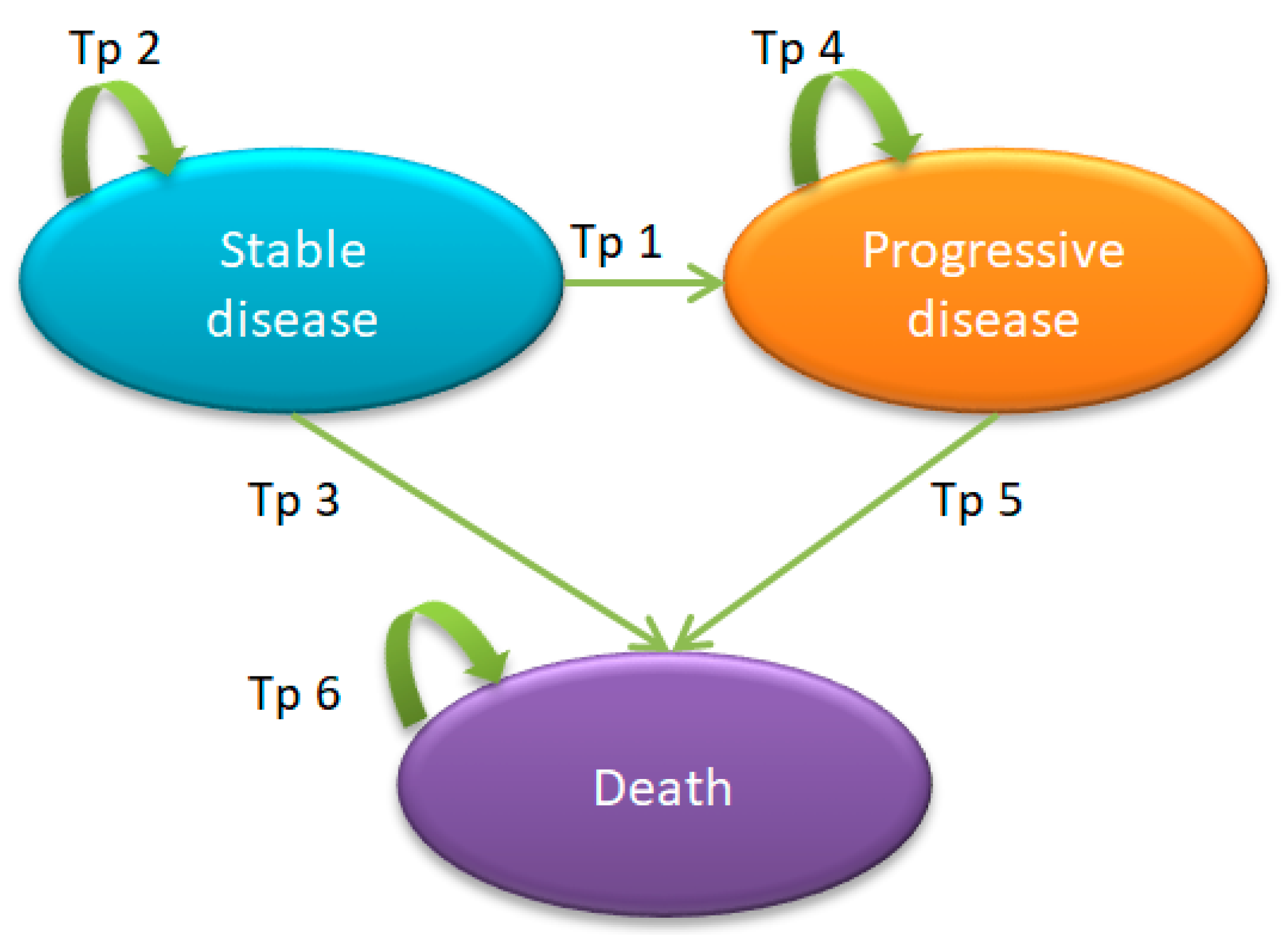
2.2. Economic Model
2.3. Model Input Parameters
2.3.1. Treatment Options and Effectiveness
2.3.2. Probability Data
2.3.3. Cost Data
2.3.4. Utility Data
2.4. Cost–Utility Analysis
2.4.1. Base Case Analysis
2.4.2. Sensitivity Analyses
2.4.3. Budget Impact Analysis
3. Results
3.1. Base Case Analysis
3.2. Sensitivity Analyses
3.2.1. One-Way Sensitivity Analyses
- the lower-limit values of the utility of stable disease when off treatment;
- the upper-limit value of the transition probability of CAPOX from stable disease to progressive disease;
- the lower-limit values of the transition probability of 5-FU/LV from stable disease to progressive disease, with respect to the descending order of sensitivity.
3.2.2. Probabilistic Sensitivity Analyses
3.3. Budget Impact Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ferlay, J.; Soerjomataram, I.; Dikshit, R.; Eser, S.; Mathers, C.; Rebelo, M.; Parkin, D.M.; Forman, D.; Bray, F. Cancer incidence and mortality worldwide: Sources, methods and major patterns in GLOBOCAN 2012. Int. J. Cancer 2015, 136, E359–E386. [Google Scholar] [CrossRef] [PubMed]
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA A Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef] [PubMed]
- Ministry of Public Health, National Cancer Institute Thailand. Cancer in Thailand, Volume VIII, 2010–2012; National Cancer Institute Thailand: Bangkok, Thailand, 2015.
- Bockelman, C.; Engelmann, B.E.; Kaprio, T.; Hansen, T.F.; Glimelius, B. Risk of recurrence in patients with colon cancer stage II and III: A systematic review and meta-analysis of recent literature. Acta Oncol. 2015, 54, 5–16. [Google Scholar] [CrossRef] [PubMed]
- National Cancer Institute Thailand. Guideline on Screening, Diagnosis, and Treatment of Colorectal Cancer; National Cancer Institute Thailand: Bangkok, Thailand, 2015.
- Pandor, A.; Eggington, S.; Paisley, S.; Tappenden, P.; Sutcliffe, P. The clinical and cost-effectiveness of oxaliplatin and capecitabine for the adjuvant treatment of colon cancer: Systematic review and economic evaluation. Health Technol. Assess. 2006, 10, iii–iv, xi–xiv, 1–185. [Google Scholar] [CrossRef] [PubMed]
- Landre, T.; Uzzan, B.; Nicolas, P.; Aparicio, T.; Zelek, L.; Mary, F.; Taleb, C.; Des Guetz, G. Doublet chemotherapy vs. single-agent therapy with 5FU in elderly patients with metastatic colorectal cancer. a meta-analysis. Int. J. Color. Dis. 2015, 30, 1305–1310. [Google Scholar] [CrossRef]
- Folprecht, G.; Seymour, M.T.; Saltz, L.; Douillard, J.Y.; Hecker, H.; Stephens, R.J.; Maughan, T.S.; Van Cutsem, E.; Rougier, P.; Mitry, E.; et al. Irinotecan/fluorouracil combination in first-line therapy of older and younger patients with metastatic colorectal cancer: Combined analysis of 2691 patients in randomized controlled trials. J. Clin. Oncol. 2008, 26, 1443–1451. [Google Scholar] [CrossRef]
- Krol, M.; Koopman, M.; Uyl-de Groot, C.; Punt, C.J. A systematic review of economic analyses of pharmaceutical therapies for advanced colorectal cancer. Expert Opin. Pharmacother. 2007, 8, 1313–1328. [Google Scholar] [CrossRef]
- Jansman, F.G.A.; Postma, M.J.; van Hartskamp, D.; Willemse, P.H.B.; Brouwers, J.R.B.J. Cost-benefit analysis of capecitabine versus 5-fluorouracil/leucovorin in the treatment of colorectal cancer in the Netherlands. Clin. Ther. 2004, 26, 579–589. [Google Scholar] [CrossRef]
- Cassidy, J.; Douillard, J.Y.; Twelves, C.; McKendrick, J.J.; Scheithauer, W.; Bustová, I.; Johnston, P.G.; Lesniewski-Kmak, K.; Jelic, S.; Fountzilas, G.; et al. Pharmacoeconomic analysis of adjuvant oral capecitabine vs. intravenous 5-FU/LV in Dukes’ C colon cancer: The X-ACT trial. Br. J. Cancer 2006, 94, 1122. [Google Scholar] [CrossRef]
- Eggington, S.; Tappenden, P.; Pandor, A.; Paisley, S.; Saunders, M.; Seymour, M.; Sutcliffe, P.; Chilcott, J. Cost-effectiveness of oxaliplatin and capecitabine in the adjuvant treatment of stage III colon cancer. Br. J. Cancer 2006, 95, 1195. [Google Scholar] [CrossRef]
- Aballéa, S.; Chancellor, J.V.M.; Raikou, M.; Drummond, M.F.; Weinstein, M.C.; Jourdan, S.; Bridgewater, J. Cost-effectiveness analysis of oxaliplatin compared with 5-fluorouracil/leucovorin in adjuvant treatment of stage III colon cancer in the US. Cancer 2007, 109, 1082–1089. [Google Scholar] [CrossRef] [PubMed]
- Douillard, J.Y.; Tilleul, P.; Ychou, M.; Dufour, P.; Perrocheau, G.; Seitz, J.F.; Maes, P.; Lafuma, A.; Husseini, F. Cost Consequences of Adjuvant Capecitabine, Mayo Clinic and de Gramont Regimens for Stage III Colon Cancer in the French Setting. Oncology 2007, 72, 248–254. [Google Scholar] [CrossRef] [PubMed]
- Attard, C.L.; Maroun, J.A.; Alloul, K.; Grima, D.T.; Bernard, L.M. Cost-effectiveness of oxaliplatin in the adjuvant treatment of colon cancer in Canada. Curr. Oncol. 2010, 17, 17–24. [Google Scholar] [CrossRef] [PubMed]
- Lerdkiattikorn, P.; Chaikledkaew, U.; Lausoontornsiri, W.; Chindavijak, S.; Khuhaprema, T.; Tantai, N.; Teerawattananon, Y. Cost-utility analysis of adjuvant chemotherapy in patients with stage III colon cancer in Thailand. Expert Rev. Pharmacoecon. Outcomes Res. 2015, 15, 687–700. [Google Scholar] [CrossRef]
- Chindaprasirt, J.; Sookprasert, A.; Wirasorn, K.; Limpawattana, P.; Sutra, S.; Thavornpitak, Y. Cost of colorectal cancer care in hospitalized patients of Thailand. J. Med. Assoc. Thail. 2012, 95 (Suppl. 7), S196–S200. [Google Scholar]
- Arnold, M.; Sierra, M.S.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global patterns and trends in colorectal cancer incidence and mortality. Gut 2017, 66, 683. [Google Scholar] [CrossRef]
- Thai Working Group on Health Technology Assessment Guidelines in Thailand. Thai Health Technology Accessment Guideline, 2nd ed.; Usa, C., Teerawattananon, Y., Eds.; Chulalongkorn University Book Center: Bangkok, Thailand, 2013. [Google Scholar]
- Teerawattananon, Y.; Tritasavit, N.; Suchonwanich, N.; Kingkaew, P. The use of economic evaluation for guiding the pharmaceutical reimbursement list in Thailand. Z. Evid. Fortbild. Qual. Gesundheitswesen 2014, 108, 397–404. [Google Scholar] [CrossRef]
- The Bureau of Registration Administration (BORA), Department of Provincial Administration. Official Statistics Registration Systems. 2018. Available online: http://stat.dopa.go.th (accessed on 1 August 2019).
- Ministry of Public Health. Drug and Medical Supply Information Center. Available online: http://dmsic.moph.go.th/dmsic/index.php?p=1&type=3&s=3&id=drug_normal (accessed on 12 January 2022).
- Riewpaiboon, A. Standard Cost Lists for Health Technology Assessment. Available online: http://costingmenu.hitap.net/ (accessed on 28 February 2019).
- World Health Organization. Life Tables by Country: Thailand. 2019. Available online: https://www.who.int/data/gho/data/indicators/indicator-details/GHO/gho-ghe-life-tables-nmx-age-specific-death-rate-between-ages-x-and-x-plus-n (accessed on 19 July 2022).
- Bank of Thailand. Historical Foreign Exchange Rates. 2022. Available online: https://www.bot.or.th (accessed on 15 July 2022).
- Bureau of Trade and Economic Indices, Ministry of Commerce. Consumer Price index (CPI) of Thailand, Economic and Trade Indices Database (ETID). 2021. Available online: http://www.price.moc.go.th (accessed on 15 July 2022).
- Katanyoo, K.; Chitapanarux, I.; Tungkasamit, T.; Chakrabandhu, S.; Chongthanakorn, M.; Jiratrachu, R.; Kridakara, A.; Townamchai, K.; Muangwong, P.; Tovanabutra, C.; et al. Cost-utility analysis of 5-fluorouracil and capecitabine for adjuvant treatment in locally advanced rectal cancer. J. Gastrointest. Oncol. 2018, 9, 425–434. [Google Scholar] [CrossRef]
- Benson, A.B.; Venook, A.P.; Al-Hawary, M.M.; Cederquist, L.; Chen, Y.J.; Ciombor, K.K.; Cohen, S.; Cooper, H.S.; Deming, D.; Engstrom, P.F.; et al. NCCN guidelines insights: Colon cancer, version 2.2018. J. Natl. Compr. Cancer Netw. 2018, 16, 359–369. [Google Scholar] [CrossRef]
- Twelves, C.J. Xeloda in Adjuvant Colon Cancer Therapy (X-ACT) trial: Overview of efficacy, safety, and cost-effectiveness. Clin. Color. Cancer 2006, 6, 278–287. [Google Scholar] [CrossRef]
- Shankaran, V. Cost Considerations in the Evaluation and Treatment of Colorectal Cancer. Curr. Treat. Options Oncol. 2015, 16, 41. [Google Scholar] [CrossRef]
- Shiroiwa, T.; Fukuda, T.; Shimozuma, K.; Ohashi, Y.; Tsutani, K. Cost-effectiveness analysis of capecitabine compared with bolus 5-fluorouracil/l-leucovorin for the adjuvant treatment of colon cancer in Japan. Pharmacoeconomics 2009, 27, 597–608. [Google Scholar] [CrossRef] [PubMed]
- Lin, J.K.; Tan, E.C.; Yang, M.C. Comparing the effectiveness of capecitabine versus 5-fluorouracil/leucovorin therapy for elderly Taiwanese stage III colorectal cancer patients based on quality-of-life measures (QLQ-C30 and QLQ-CR38) and a new cost assessment tool. Health Qual. Life Outcomes 2015, 13, 61. [Google Scholar] [CrossRef]
- Pumpalova, Y.; Rogers, A.M.; Tan, S.X.; Herbst, C.L.; Ruff, P.; Neugut, A.I.; Hur, C. Modeling the Cost-Effectiveness of Adjuvant Chemotherapy for Stage III Colon Cancer in South African Public Hospitals. JCO Glob. Oncol. 2021, 7, 1730–1741. [Google Scholar] [CrossRef] [PubMed]
- Ginghina, O.; Hudita, A.; Zaharia, C.; Tsatsakis, A.; Mezhuev, Y.; Costache, M.; Galateanu, B. Current Landscape in Organic Nanosized Materials Advances for Improved Management of Colorectal Cancer Patients. Materials 2021, 14, 2440. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Chemotherapy | Dosage Regimen | Reference |
|---|---|---|
| 5-FU/LV |
| [5] |
| Capecitabine |
| [5] |
| FOLFOX |
| [5] |
| CAPOX |
| [5] |
| FOLFIRI |
| [5] |
| Input Parameters | Distribution | Base Case Values (Standard Error) | Reference |
|---|---|---|---|
| Time horizon | lifetime | [19] | |
| Cycle length (year) | 1 | ||
| Annual discount rate (range) | 3% (0–6%) | [19] | |
| Age-specific incidence rate of stage III CRC per 100,000 population | 39.72 | [4] | |
| %Eligible case | 80% | Primary data | |
| Population growth rate | 0.3% | [21] | |
| Patient body weight (kg) | 60 | Primary data | |
| Patient body surface area (m2) | 1.7 | Mosteller’s formula | |
| Annual transition probabilities | |||
| 5-FU/LV | |||
| SD to PD | Beta | 0.175 (0.012) | [16] |
| SD to death year 1 | 0.053 | Primary data | |
| SD to death year 2 | 0.152 | Primary data | |
| SD to death year 3 | 0.199 | Primary data | |
| SD to death year 4 | 0.108 | Primary data | |
| SD to death subsequent years | 0.121 | Primary data | |
| Capecitabine | |||
| SD to PD | Beta | 0.149 (0.010) | [16] |
| SD to death year 1 | 0.057 | Primary data | |
| SD to death year 2 | 0.073 | Primary data | |
| SD to death year 3 | 0.108 | Primary data | |
| SD to death year 4 | 0.105 | Primary data | |
| SD to death subsequent years | 0.072 | Primary data | |
| FOLFOX | |||
| SD to PD | Beta | 0.133 (0.009) | [16] |
| SD to death year 1 | 0.000 | Primary data | |
| SD to death year 2 | 0.082 | Primary data | |
| SD to death year 3 | 0.060 | Primary data | |
| SD to death year 4 | 0.063 | Primary data | |
| SD to death subsequent years | 0.068 | Primary data | |
| PD to death year 1 | 0.208 | Primary data | |
| PD to death year 2 | 0.351 | Primary data | |
| PD to death year 3 | 0.514 | Primary data | |
| PD to death subsequent years | 0.222 | Primary data | |
| CAPOX | |||
| SD to PD | Beta | 0.140 (0.010) | [16] |
| SD to death year 1 | 0.012 | Primary data | |
| SD to death year 2 | 0.037 | Primary data | |
| SD to death year 3 | 0.071 | Primary data | |
| SD to death year 4 | 0.069 | Primary data | |
| SD to death subsequent years | 0.030 | Primary data | |
| PD to death year 1 | 0.176 | Primary data | |
| PD to death year 2 | 0.435 | Primary data | |
| PD to death year 3 | 0.318 | Primary data | |
| PD to death subsequent years | 0.267 | Primary data | |
| FOLFIRI | |||
| PD to death year 1 | 0.474 | Primary data | |
| PD to death year 2 | 0.574 | Primary data | |
| PD to death year 3 | 0.462 | Primary data | |
| PD to death subsequent years | 0.500 | Primary data | |
| Costs (2021; USD) | |||
| Direct medical costs | |||
| Cost of chemotherapy (2021; USD per dosage unit) | |||
| 5-FU (1000 mg/vial) | Gamma | 4 | [22] |
| LV (300 mg/vial) | Gamma | 9 | [22] |
| Capecitabine (500 mg/tab) | Gamma | 2 | [22] |
| Oxaliplatin (100 mg/vial) | Gamma | 39 | [22] |
| Irinotecan (100 mg/vial) | Gamma | 43 | [22] |
| Cost of chemotherapy administration (2021; USD per visit) | |||
| OPD IV bolus | Gamma | 14 | [23] |
| OPD IV infusion | Gamma | 32 | Primary data |
| IPD IV infusion | Gamma | 122 | [23] |
| Other healthcare costs (2021; USD per year) | |||
| SD year 1 (OPD regimen) | Gamma | 2041 | Primary data |
| SD year 1 (IPD regimen) | Gamma | 7321 | Primary data |
| SD year 2 | Gamma | 2041 | Primary data |
| SD year 3 and subsequent years | Gamma | 1875 | Primary data |
| PD year 1 (OPD regimen) | Gamma | 3789 | Primary data |
| PD year 1 (IPD regimen) | Gamma | 8445 | Primary data |
| PD year 2 | Gamma | 3789 | Primary data |
| PD year 3 and subsequent years | Gamma | 3136 | Primary data |
| Direct non-medical costs (2021; USD per visit) | |||
| Food | Gamma | 2 (0.4) | [23] |
| Transportation | Gamma | 5 (0.2) | [23] |
| Hospital visits rate | |||
| 5-FU/LV (per course) | 30 | [5] | |
| Capecitabine * (per course) | 6 | Assumption | |
| FOLFOX (per course) | 12 | [5] | |
| CAPOX (per course) | 8 | [5] | |
| FOLFIRI (per course) | 12 | [5] | |
| SD, latter half of year 1 (off treatment) | 6 | Primary data | |
| SD, year 2 | 13 | Primary data | |
| SD, year 3 and subsequent years | 12 | Primary data | |
| PD, latter half of year 1 (off treatment) | 9 | Primary data | |
| PD, year 2 | 20 | Primary data | |
| PD, year 3 and subsequent years | 18 | Primary data | |
| Utilities | |||
| SD, on IV CMT | Beta | 0.600 (0.063) | [16] |
| SD, on oral CMT | Beta | 0.651 (0.047) | [16] |
| SD, off treatment | Beta | 0.850 (0.100) | [16] |
| PD, on IV CMT | Beta | 0.560 (0.101) | [16] |
| PD, off treatment | Beta | 0.624 (0.043) | [16] |
| Treatment Options | Total Cost (USD) | LYs | QALYs | Incremental Cost (USD) | Incremental QALYs | ICERs (USD/QALY Gained) | Interpretation |
|---|---|---|---|---|---|---|---|
| 5-FU/LV→FOLFIRI | 15,422 | 4.52 | 2.14 | −1671 | −0.40 | 4214 | dominated by 5-FU/LV→CAPOX |
| 5-FU/LV→FOLFOX | 17,092 | 5.31 | 2.54 | - | - | - | base case |
| 5-FU/LV→CAPOX | 14,321 | 5.35 | 2.56 | −2771 | 0.02 | - | cost saving compared to base case |
| Capecitabine→FOLFIRI | 17,719 | 5.57 | 2.82 | 627 | 0.29 | 2176 | dominated by capecitabine→CAPOX |
| Capecitabine→FOLFOX | 19,477 | 6.42 | 3.24 | 2385 | 0.71 | 3377 | dominated by capecitabine→CAPOX |
| Capecitabine→CAPOX | 16,532 | 6.46 | 3.27 | −561 | 0.73 | - | cost saving compared to base case |
| FOLFOX→FOLFIRI | 26,259 | 6.39 | 3.37 | 9166 | 0.83 | 10,986 | dominated by CAPOX→FOLFIRI |
| CAPOX→FOLFIRI | 21,644 | 6.87 | 3.60 | 4552 | 1.07 | 4258 | cost effective compared to base case |
| Regimen | Year | Total over 5 Years (USD) | Per Year (USD) | ||||
|---|---|---|---|---|---|---|---|
| 1 | 2 | 3 | 4 | 5 | |||
| 5-FU/LV→FOLFOX * | 1,172,438 | 1,564,064 | 1,882,169 | 2,140,896 | 2,351,667 | 9,111,234 | 1,822,247 |
| 5-FU/LV→CAPOX | 1,172,438 | 1,716,961 | 2,159,003 | 2,518,277 | 2,810,706 | 10,377,386, | 2,075,477 |
| 5-FU/LV→FOLFIRI | 1,172,438 | 1,869,648 | 2,435,455 | 2,895,138 | 3,269,112 | 11,641,790 | 2,328,358 |
| Capecitabine→FOLFOX | 2,030,097 | 2,361,654 | 2,641,650 | 2,878,404 | 3,078,891 | 12,990,697 | 2,598,139 |
| Capecitabine→CAPOX | 2,030,097 | 2,489,890 | 2,877,811 | 3,205,456 | 3,482,551 | 14,085,805 | 2,817,161 |
| Capecitabine→FOLFIRI | 2,030,097 | 2,617,949 | 3,113,646 | 3,532,058 | 3,885,653, | 15,179,402 | 3,035,881 |
| FOLFOX→FOLFIRI | 5,805,720 | 6,337,576 | 6,797,503 | 7,195,766 | 7,541,166 | 33,677,731 | 6,735,546 |
| CAPOX→FOLFIRI | 4,049,712 | 4,605,604 | 5,081,072 | 5,488,246 | 5,837,427 | 25,062,061 | 5,012,412 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Phisalprapa, P.; Kositamongkol, C.; Korphaisarn, K.; Akewanlop, C.; Srimuninnimit, V.; Supakankunti, S.; Apiraksattayakul, N.; Chaiyakunapruk, N. Cost–Utility and Budget Impact Analyses of Oral Chemotherapy for Stage III Colorectal Cancer: Real-World Evidence after Policy Implementation in Thailand. Cancers 2023, 15, 4930. https://doi.org/10.3390/cancers15204930
Phisalprapa P, Kositamongkol C, Korphaisarn K, Akewanlop C, Srimuninnimit V, Supakankunti S, Apiraksattayakul N, Chaiyakunapruk N. Cost–Utility and Budget Impact Analyses of Oral Chemotherapy for Stage III Colorectal Cancer: Real-World Evidence after Policy Implementation in Thailand. Cancers. 2023; 15(20):4930. https://doi.org/10.3390/cancers15204930
Chicago/Turabian StylePhisalprapa, Pochamana, Chayanis Kositamongkol, Krittiya Korphaisarn, Charuwan Akewanlop, Vichien Srimuninnimit, Siripen Supakankunti, Natnasak Apiraksattayakul, and Nathorn Chaiyakunapruk. 2023. "Cost–Utility and Budget Impact Analyses of Oral Chemotherapy for Stage III Colorectal Cancer: Real-World Evidence after Policy Implementation in Thailand" Cancers 15, no. 20: 4930. https://doi.org/10.3390/cancers15204930