
Pathology of Combined Hepatocellular Carcinoma-Cholangiocarcinoma: An Update

Abstract
:Simple Summary
Abstract
1. Introduction
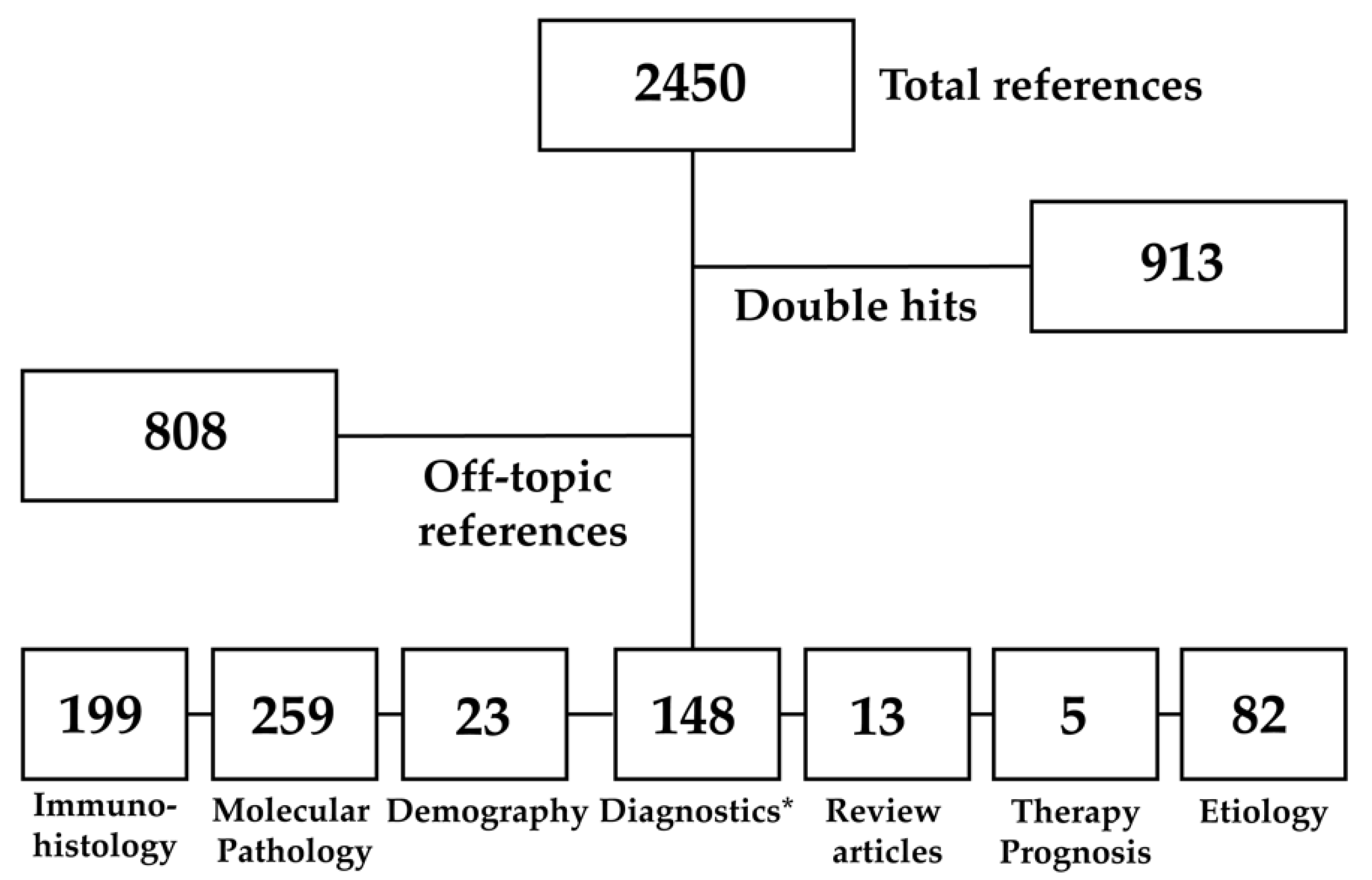
2. Materials and Methods
3. Results
3.1. Epidemiology
3.2. Risk Factors and Prognostic Factors
3.3. Basic Clinical Aspects
3.4. Histopathological Features
3.4.1. A Historical Perspective
3.4.2. The WHO Classification
3.5. Immunohistochemical Landscape
3.5.1. General Considerations
3.5.2. Immunohistochemical Expression Patterns of Conventional Differentiation Markers
3.5.3. Immunhistochemical Expression Patterns of Stem Cell and Progenitor Cell Markers
3.5.4. Other Investigated Markers

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Tumor | Immunohistochemical Stains | References |
|---|---|---|
| Most commonly used biomarkers | ||
| Hepatocellular cells | Hepatocyte Paraffin 1 (Hep Par 1) | [104,114,126,127,128,129,137,138,139,153,163] |
| Arginase 1 | [111,130] | |
| Cholangiocellular cells | Cytokeratin 7 | [44,118,126,127,128,137,138,139,140,141,163] |
| Cytokeratin 8 | [126,164,165] | |
| Cytokeratin 19 | [44,104,114,118,127,129,138,139,140,141,142,163,166] | |
| Further studied biomarkers | ||
| Hepatocellular cells | Albumin | [164] |
| Alpha-1-antichymotrypsin | [164] | |
| Alpha-1-antitrypsin | [59,164] | |
| alpha-Fetoprotein | [59,104,113,118,126,127,132,133,138,144,163] | |
| Alpha-human chorionic gonadotropin | [132,164] | |
| Asialoglycoproteinreceptor | [164] | |
| Biliary glycoprotein | [164] | |
| ß-microglobulin | [164] | |
| CA IX | [151] | |
| Carcinoembryonic antigen (CEA) polyclonal | [59,104,113,118,126,131,132,133] | |
| Cathepsin B | [164,167,168,169,170] | |
| CD44 | [140] | |
| C-reactive protein (CRP) | [152,164] | |
| Cytokeratin 18 | [126,164,165] | |
| Cytokeratin 20 | [114,118,126] | |
| Cytokeratin AE1/AE3 | [113,118,126] | |
| Cytokeratin CAM 5.2 | [113,118,126] | |
| Delta-like 1 homolog (DLK1) | [144] | |
| Epithelial membrane antigen (EMA) | [113,118,126,127,138] | |
| EpCAM | [126,127,138,140,143,144,171] | |
| Erythropoiesis-associated antigen (ERY-1) | [133,164] | |
| Factor XIIIa | [114,153,164,172] | |
| Ferritin | [164] | |
| Fibrinogen | [59,164] | |
| Metallothionein | [154,155,156,164] | |
| P21 | [164] | |
| P53 | [126,164] | |
| Proliferating cell nuclear antigen (PCNA) | [164,171] | |
| Prothymosin | [164,173] | |
| Retinoblastoma | [129,164] | |
| Thrombospondin | [164] | |
| Transferrin receptor | [164] | |
| Ubiquitin | [164] | |
| Vimentin | [115,132,161,164] | |
| Yes-associated protein 1 (YAP1) | [162,174,175,176] | |
| Intermediate cells | Alpha-Fetoprotein (AFP) | [59,104,113,118,126,127,132,133,138,144,163] |
| Arginase 1 (ARG1) | [111,130] | |
| Carcinoembryonic antigen (CEA) polyclonal | [59,104,113,118,126,131,132,133] | |
| CD133 | [140,143,144] | |
| CK34ßE12 | [126,150] | |
| c-KIT | [104,105,138,139,150] | |
| Cytokeratin 7 | [44,118,126,127,128,137,138,139,140,141,163] | |
| Cytokeratin 8 | [126,164,165] | |
| Cytokeratin 18 | [126,164,165] | |
| Cytokeratin 19 | [44,104,114,118,127,129,138,139,140,141,142,163,166] | |
| Delta-like 1 homolog (DLK1) | [144] | |
| EpCAM | [126,127,138,140,143,144,171] | |
| Hepatocyte Paraffin 1 (HepPar 1) | [104,114,126,127,128,129,137,138,139,153,163] | |
| LIF | [105] | |
| Nestin | [141,149,177] | |
| Neural cell adhesion molecule (NCAM)/CD56 | [126,127,138,141,143,144] | |
| OCT4 | [105] | |
| P63 | [150] | |
| Polyductin | [160] | |
| Prominin-1 | [105] | |
| Yes-associated protein 1 (YAP1) | [162,174,175,176] | |
| Cholangiocellular cells | ARID1A | [178] |
| CA IX | [151] | |
| Carcinoembryonic antigen (CEA) polyclonal | [59,104,113,118,126,131,132,133] | |
| c-KIT | [104,105,138,139,150] | |
| Cytokeratin 7 | [44,118,126,127,128,137,138,139,140,141,163] | |
| Cytokeratin 19 | [44,104,114,118,127,129,138,139,140,141,142,163,166] | |
| Cytokeratin AE1/AE3 | [113,118,126] | |
| Cytokeratin CAM 5.2 | [113,118,126] | |
| Delta-like 1 homolog (DLK1) | [144] | |
| Epithelial membrane antigen (EMA) | [113,118,126,127,138] | |
| EpCAM | [126,127,138,140,143,144,171] | |
| MUC1 | [126,137,157,159,179] | |
| MUC2 | [126,159,179] | |
| MUC3 | [159,179] | |
| MUC5/6 | [159] | |
| MUC5AC | [126,158] | |
| MUC6 | [126,158] | |
| MUC7 | [158] | |
| Neural cell adhesion molecule (NCAM)/CD56 | [126,127,138,141,143,144] | |
| Polyductin | [160] | |
| Tumor-associated glyocoprotein 72 (TAG-72) | [180] | |
| Yes-associated protein 1 (YAP1) | [162,174,175,176] |
3.6. Ultrastructural Features
3.7. Molecular Pathological Foundations
4. Discussion
5. Future Directions
6. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef]
- Ferlay, J.; Ervik, M.; Lam, F.; Colombet, M.; Mery, L.; Piñeros, M.; Znaor, A.; Soerjomataram, I.; Bray, F. Global Cancer Observatory: Cancer Today; International Agency for Research on Cancer: Lyon, France, 2020; Available online: https://gco.iarc.fr/today (accessed on 30 October 2022).
- Yang, J.D.; Hainaut, P.; Gores, G.J.; Amadou, A.; Plymoth, A.; Roberts, L.R. A global view of hepatocellular carcinoma: Trends, risk, prevention and management. Nat. Rev. Gastroenterol. Hepatol. 2019, 16, 589–604. [Google Scholar] [CrossRef] [PubMed]
- Marrero, J.A.; Kulik, L.M.; Sirlin, C.B.; Zhu, A.X.; Finn, R.S.; Abecassis, M.M.; Roberts, L.R.; Heimbach, J.K. Diagnosis, Staging, and Management of Hepatocellular Carcinoma: 2018 Practice Guidance by the American Association for the Study of Liver Diseases. Hepatology 2018, 68, 723–750. [Google Scholar] [CrossRef] [Green Version]
- Mungamuri, S.K.; Sinha, S.N.; Javvadi, Y. Understanding the Alterations in Lipid Metabolism in NAFLD Progression: Current Trends and Future Directions. Crit. Rev. Oncog. 2021, 26, 35–49. [Google Scholar] [CrossRef] [PubMed]
- Ito, Y.; Kojiro, M.; Nakashima, T.; Mori, T. Pathomorphologic characteristics of 102 cases of thorotrast-related hepatocellular carcinoma, cholangiocarcinoma, and hepatic angiosarcoma. Cancer 1988, 62, 1153–1162. [Google Scholar] [CrossRef] [PubMed]
- Johnson, F.L.; Lerner, K.G.; Siegel, M.; Feagler, J.R.; Majerus, P.W.; Hartmann, J.R.; Thomas, E.D. Association of androgenic-anabolic steroid therapy with development of hepatocellular carcinoma. Lancet 1972, 2, 1273–1276. [Google Scholar] [CrossRef]
- Pryor, A.C.; Cohen, R.J.; Goldman, R.L. Hepatocellular carcinoma in a woman on long-term oral contraceptives. Cancer 1977, 40, 884–888. [Google Scholar] [CrossRef]
- Christopherson, W.M.; Mays, E.T.; Barrows, G. Hepatocellular carcinoma in young women on oral contraceptives. Lancet 1978, 2, 38–39. [Google Scholar] [CrossRef]
- Menzies-Gow, N. Hepatocellular carcinoma associated with oral contraceptives. Br. J. Surg. 1978, 65, 316–317. [Google Scholar] [CrossRef]
- Dourdourekas, D.; Villa, F.; Szanto, P.B.; Steigmann, F. Hepatocellular carcinoma: Relation to alcohol, HB-antigen and alpha-fetoprotein. Am. J. Gastroenterol. 1975, 63, 307–311. [Google Scholar]
- Trichopoulos, D.; Day, N.E.; Kaklamani, E.; Tzonou, A.; Munoz, N.; Zavitsanos, X.; Koumantaki, Y.; Trichopoulou, A. Hepatitis B virus, tobacco smoking and ethanol consumption in the etiology of hepatocellular carcinoma. Int. J. Cancer 1987, 39, 45–49. [Google Scholar] [CrossRef] [PubMed]
- Yu, M.C.; Mack, T.; Hanisch, R.; Peters, R.L.; Henderson, B.E.; Pike, M.C. Hepatitis, alcohol consumption, cigarette smoking, and hepatocellular carcinoma in Los Angeles. Cancer Res. 1983, 43, 6077–6079. [Google Scholar] [PubMed]
- Trichopoulos, D.; MacMahon, B.; Sparros, L.; Merikas, G. Smoking and hepatitis B-negative primary hepatocellular carcinoma. J. Natl. Cancer Inst. 1980, 65, 111–114. [Google Scholar] [PubMed]
- Baiges, A.; Turon, F.; Simon-Talero, M.; Tasayco, S.; Bueno, J.; Zekrini, K.; Plessier, A.; Franchi-Abella, S.; Guerin, F.; Mukund, A.; et al. Congenital Extrahepatic Portosystemic Shunts (Abernethy Malformation): An International Observational Study. Hepatology 2020, 71, 658–669. [Google Scholar] [CrossRef]
- Khanna, R.; Verma, S.K. Pediatric hepatocellular carcinoma. World J. Gastroenterol. 2018, 24, 3980–3999. [Google Scholar] [CrossRef]
- Donath, H.; Woelke, S.; Theis, M.; Hess, U.; Knop, V.; Herrmann, E.; Krauskopf, D.; Kieslich, M.; Schubert, R.; Zielen, S. Progressive Liver Disease in Patients With Ataxia Telangiectasia. Front. Pediatr. 2019, 7, 458. [Google Scholar] [CrossRef] [Green Version]
- Knisely, A.S.; Strautnieks, S.S.; Meier, Y.; Stieger, B.; Byrne, J.A.; Portmann, B.C.; Bull, L.N.; Pawlikowska, L.; Bilezikci, B.; Ozcay, F.; et al. Hepatocellular carcinoma in ten children under five years of age with bile salt export pump deficiency. Hepatology 2006, 44, 478–486. [Google Scholar] [CrossRef]
- Sempoux, C.; Balabaud, C.; Bioulac-Sage, P. Malignant transformation of hepatocellular adenoma. Hepat. Oncol. 2014, 1, 421–431. [Google Scholar] [CrossRef]
- Massarweh, N.N.; El-Serag, H.B. Epidemiology of Hepatocellular Carcinoma and Intrahepatic Cholangiocarcinoma. Cancer Control 2017, 24, 1073274817729245. [Google Scholar] [CrossRef]
- Su, C.H.; Shyr, Y.M.; Lui, W.Y.; P’Eng, F.K. Hepatolithiasis associated with cholangiocarcinoma. Br. J. Surg. 1997, 84, 969–973. [Google Scholar] [CrossRef]
- Chijiiwa, K.; Yamashita, H.; Yoshida, J.; Kuroki, S.; Tanaka, M. Current management and long-term prognosis of hepatolithiasis. Arch. Surg. 1995, 130, 194–197. [Google Scholar] [CrossRef] [PubMed]
- Welzel, T.M.; Graubard, B.I.; El-Serag, H.B.; Shaib, Y.H.; Hsing, A.W.; Davila, J.A.; McGlynn, K.A. Risk factors for intrahepatic and extrahepatic cholangiocarcinoma in the United States: A population-based case-control study. Clin. Gastroenterol. Hepatol. 2007, 5, 1221–1228. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kobayashi, M.; Furuta, K.; Kitamura, H.; Oguchi, K.; Arai, M.; Koike, S.; Nakazawa, K. A case of primary biliary cirrhosis that complicated with combined hepatocellular and cholangiocellular carcinoma. Clin. J. Gastroenterol. 2011, 4, 236–241. [Google Scholar] [CrossRef]
- Donato, F.; Gelatti, U.; Tagger, A.; Favret, M.; Ribero, M.L.; Callea, F.; Martelli, C.; Savio, A.; Trevisi, P.; Nardi, G. Intrahepatic cholangiocarcinoma and hepatitis C and B virus infection, alcohol intake, and hepatolithiasis: A case-control study in Italy. Cancer Causes Control 2001, 12, 959–964. [Google Scholar] [CrossRef]
- Shaib, Y.H.; El-Serag, H.B.; Nooka, A.K.; Thomas, M.; Brown, T.D.; Patt, Y.Z.; Hassan, M.M. Risk factors for intrahepatic and extrahepatic cholangiocarcinoma: A hospital-based case-control study. Am. J. Gastroenterol. 2007, 102, 1016–1021. [Google Scholar] [CrossRef]
- Watanapa, P.; Watanapa, W.B. Liver fluke-associated cholangiocarcinoma. Br. J. Surg. 2002, 89, 962–970. [Google Scholar] [CrossRef] [PubMed]
- Melum, E.; Karlsen, T.H.; Schrumpf, E.; Bergquist, A.; Thorsby, E.; Boberg, K.M.; Lie, B.A. Cholangiocarcinoma in primary sclerosing cholangitis is associated with NKG2D polymorphisms. Hepatology 2008, 47, 90–96. [Google Scholar] [CrossRef]
- Claessen, M.M.; Vleggaar, F.P.; Tytgat, K.M.; Siersema, P.D.; van Buuren, H.R. High lifetime risk of cancer in primary sclerosing cholangitis. J. Hepatol. 2009, 50, 158–164. [Google Scholar] [CrossRef]
- Chapman, M.H.; Webster, G.J.; Bannoo, S.; Johnson, G.J.; Wittmann, J.; Pereira, S.P. Cholangiocarcinoma and dominant strictures in patients with primary sclerosing cholangitis: A 25-year single-centre experience. Eur. J. Gastroenterol. Hepatol. 2012, 24, 1051–1058. [Google Scholar] [CrossRef]
- Bergquist, A.; Glaumann, H.; Persson, B.; Broome, U. Risk factors and clinical presentation of hepatobiliary carcinoma in patients with primary sclerosing cholangitis: A case-control study. Hepatology 1998, 27, 311–316. [Google Scholar] [CrossRef]
- Lipsett, P.A.; Pitt, H.A.; Colombani, P.M.; Boitnott, J.K.; Cameron, J.L. Choledochal cyst disease. A changing pattern of presentation. Ann. Surg. 1994, 220, 644–652. [Google Scholar] [CrossRef] [PubMed]
- Khan, S.A.; Thomas, H.C.; Davidson, B.R.; Taylor-Robinson, S.D. Cholangiocarcinoma. Lancet 2005, 366, 1303–1314. [Google Scholar] [CrossRef]
- Coulouarn, C.; Cavard, C.; Rubbia-Brandt, L.; Audebourg, A.; Dumont, F.; Jacques, S.; Just, P.A.; Clement, B.; Gilgenkrantz, H.; Perret, C.; et al. Combined hepatocellular-cholangiocarcinomas exhibit progenitor features and activation of Wnt and TGFbeta signaling pathways. Carcinogenesis 2012, 33, 1791–1796. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moeini, A.; Sia, D.; Zhang, Z.; Camprecios, G.; Stueck, A.; Dong, H.; Montal, R.; Torrens, L.; Martinez-Quetglas, I.; Fiel, M.I.; et al. Mixed hepatocellular cholangiocarcinoma tumors: Cholangiolocellular carcinoma is a distinct molecular entity. J. Hepatol. 2017, 66, 952–961. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Theise, N.D.; Yao, J.L.; Harada, K.; Hytiroglou, P.; Portmann, B.; Thung, S.N.; Tsui, W.; Ohta, H.; Nakanuma, Y. Hepatic ’stem cell’ malignancies in adults: Four cases. Histopathology 2003, 43, 263–271. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Garancini, M.; Goffredo, P.; Pagni, F.; Romano, F.; Roman, S.; Sosa, J.A.; Giardini, V. Combined hepatocellular-cholangiocarcinoma: A population-level analysis of an uncommon primary liver tumor. Liver Transpl. 2014, 20, 952–959. [Google Scholar] [CrossRef]
- Aoki, K.; Takayasu, K.; Kawano, T.; Muramatsu, Y.; Moriyama, N.; Wakao, F.; Yamamoto, J.; Shimada, K.; Takayama, T.; Kosuge, T.; et al. Combined hepatocellular carcinoma and cholangiocarcinoma: Clinical features and computed tomographic findings. Hepatology 1993, 18, 1090–1095. [Google Scholar] [CrossRef]
- Jarnagin, W.R.; Weber, S.; Tickoo, S.K.; Koea, J.B.; Obiekwe, S.; Fong, Y.; DeMatteo, R.P.; Blumgart, L.H.; Klimstra, D. Combined hepatocellular and cholangiocarcinoma: Demographic, clinical, and prognostic factors. Cancer 2002, 94, 2040–2046. [Google Scholar] [CrossRef]
- Lee, C.C.; Wu, C.Y.; Chen, J.T.; Chen, G.H. Comparing combined hepatocellular-cholangiocarcinoma and cholangiocarcinoma: A clinicopathological study. Hepatogastroenterology 2002, 49, 1487–1490. [Google Scholar]
- Ramai, D.; Ofosu, A.; Lai, J.K.; Reddy, M.; Adler, D.G. Combined Hepatocellular Cholangiocarcinoma: A Population-Based Retrospective Study. Am. J. Gastroenterol. 2019, 114, 1496–1501. [Google Scholar] [CrossRef]
- Wachtel, M.S.; Zhang, Y.; Xu, T.; Chiriva-Internati, M.; Frezza, E.E. Combined hepatocellular cholangiocarcinomas; analysis of a large database. Clin. Med. Pathol. 2008, 1, 43–47. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liver Cancer Study Group of Japan. Primary liver cancer in Japan. Clinicopathologic features and results of surgical treatment. Ann. Surg. 1990, 211, 277–287. [Google Scholar]
- Maeda, T.; Adachi, E.; Kajiyama, K.; Sugimachi, K.; Tsuneyoshi, M. Combined hepatocellular and cholangiocarcinoma: Proposed criteria according to cytokeratin expression and analysis of clinicopathologic features. Hum. Pathol. 1995, 26, 956–964. [Google Scholar] [CrossRef] [PubMed]
- Yano, Y.; Yamamoto, J.; Kosuge, T.; Sakamoto, Y.; Yamasaki, S.; Shimada, K.; Ojima, H.; Sakamoto, M.; Takayama, T.; Makuuchi, M. Combined hepatocellular and cholangiocarcinoma: A clinicopathologic study of 26 resected cases. Jpn. J. Clin. Oncol. 2003, 33, 283–287. [Google Scholar] [CrossRef]
- Yin, X.; Zhang, B.H.; Qiu, S.J.; Ren, Z.G.; Zhou, J.; Chen, X.H.; Zhou, Y.; Fan, J. Combined hepatocellular carcinoma and cholangiocarcinoma: Clinical features, treatment modalities, and prognosis. Ann. Surg. Oncol. 2012, 19, 2869–2876. [Google Scholar] [CrossRef]
- Lee, S.D.; Park, S.J.; Han, S.S.; Kim, S.H.; Kim, Y.K.; Lee, S.A.; Ko, Y.H.; Hong, E.K. Clinicopathological features and prognosis of combined hepatocellular carcinoma and cholangiocarcinoma after surgery. Hepatobiliary Pancreat. Dis. Int. 2014, 13, 594–601. [Google Scholar] [CrossRef]
- Ide, R.; Oshita, A.; Nishisaka, T.; Nakahara, H.; Aimitsu, S.; Itamoto, T. Primary biliary cholangitis metachronously complicated with combined hepatocellular carcinoma-cholangiocellular carcinoma and hepatocellular carcinoma. World J. Hepatol. 2017, 9, 1378–1384. [Google Scholar] [CrossRef] [Green Version]
- Portolani, N.; Baiocchi, G.L.; Coniglio, A.; Piardi, T.; Grazioli, L.; Benetti, A.; Ferrari Bravo, A.; Giulini, S.M. Intrahepatic cholangiocarcinoma and combined hepatocellular-cholangiocarcinoma: A Western experience. Ann. Surg. Oncol. 2008, 15, 1880–1890. [Google Scholar] [CrossRef]
- Yang, Z.; Shi, G. Survival outcomes of combined hepatocellular-cholangiocarcinoma compared with intrahepatic cholangiocarcinoma: A SEER population-based cohort study. Cancer Med. 2022, 11, 692–704. [Google Scholar] [CrossRef]
- Zhou, Y.W.; Li, Q.F.; Chen, Y.Y.; Wang, K.; Pu, D.; Chen, X.R.; Li, C.H.; Jiang, L.; Wang, Y.; Li, Q.; et al. Clinicopathologic features, treatment, survival, and prognostic factors of combined hepatocellular and cholangiocarcinoma: A nomogram development based on SEER database and validation in multicenter study. Eur. J. Surg. Oncol. 2022, 48, 1559–1566. [Google Scholar] [CrossRef]
- Gera, S.; Ettel, M.; Acosta-Gonzalez, G.; Xu, R. Clinical features, histology, and histogenesis of combined hepatocellular-cholangiocarcinoma. World J. Hepatol. 2017, 9, 300–309. [Google Scholar] [CrossRef] [PubMed]
- Kassahun, W.T.; Hauss, J. Management of combined hepatocellular and cholangiocarcinoma. Int. J. Clin. Pract. 2008, 62, 1271–1278. [Google Scholar] [CrossRef] [PubMed]
- Bismuth, H.; Nakache, R.; Diamond, T. Management strategies in resection for hilar cholangiocarcinoma. Ann. Surg. 1992, 215, 31–38. [Google Scholar] [CrossRef] [PubMed]
- Krasinskas, A.; Pawlik, T.M.; Mino-Kenudson, M.; Vauthey, J.-N. Distal bile duct. In AJCC Cancer Staging Manual; AJCC: Chicago, IL, USA, 2017; p. 317. [Google Scholar]
- Nagorney, D.M.; Pawlik, T.M.; Chun, Y.S. Perihilar bile ducts. In AJCC Cancer Staging Manual; AJCC: Chicago, IL, USA, 2017; p. 311. [Google Scholar]
- Aloia, T.; Pawlik, T.M.; Taouli, B. Intrahepatic bile ducts. In AJCC Cancer Staging Manual; AJCC: Chicago, IL, USA, 2017; p. 295. [Google Scholar]
- DeOliveira, M.L.; Cunningham, S.C.; Cameron, J.L.; Kamangar, F.; Winter, J.M.; Lillemoe, K.D.; Choti, M.A.; Yeo, C.J.; Schulick, R.D. Cholangiocarcinoma: Thirty-one-year experience with 564 patients at a single institution. Ann. Surg. 2007, 245, 755–762. [Google Scholar] [CrossRef] [PubMed]
- Goodman, Z.D.; Ishak, K.G.; Langloss, J.M.; Sesterhenn, I.A.; Rabin, L. Combined hepatocellular-cholangiocarcinoma. A histologic and immunohistochemical study. Cancer 1985, 55, 124–135. [Google Scholar] [CrossRef]
- Groeschl, R.T.; Turaga, K.K.; Gamblin, T.C. Transplantation versus resection for patients with combined hepatocellular carcinoma-cholangiocarcinoma. J. Surg. Oncol. 2013, 107, 608–612. [Google Scholar] [CrossRef] [PubMed]
- Kim, K.H.; Lee, S.G.; Park, E.H.; Hwang, S.; Ahn, C.S.; Moon, D.B.; Ha, T.Y.; Song, G.W.; Jung, D.H.; Kim, K.M.; et al. Surgical treatments and prognoses of patients with combined hepatocellular carcinoma and cholangiocarcinoma. Ann. Surg. Oncol. 2009, 16, 623–629. [Google Scholar] [CrossRef]
- Koh, K.C.; Lee, H.; Choi, M.S.; Lee, J.H.; Paik, S.W.; Yoo, B.C.; Rhee, J.C.; Cho, J.W.; Park, C.K.; Kim, H.J. Clinicopathologic features and prognosis of combined hepatocellular cholangiocarcinoma. Am. J. Surg. 2005, 189, 120–125. [Google Scholar] [CrossRef]
- Lee, J.H.; Chung, G.E.; Yu, S.J.; Hwang, S.Y.; Kim, J.S.; Kim, H.Y.; Yoon, J.H.; Lee, H.S.; Yi, N.J.; Suh, K.S.; et al. Long-term prognosis of combined hepatocellular and cholangiocarcinoma after curative resection comparison with hepatocellular carcinoma and cholangiocarcinoma. J. Clin. Gastroenterol. 2011, 45, 69–75. [Google Scholar] [CrossRef]
- Lee, W.S.; Lee, K.W.; Heo, J.S.; Kim, S.J.; Choi, S.H.; Kim, Y.I.; Joh, J.W. Comparison of combined hepatocellular and cholangiocarcinoma with hepatocellular carcinoma and intrahepatic cholangiocarcinoma. Surg. Today 2006, 36, 892–897. [Google Scholar] [CrossRef]
- Nakamura, S.; Suzuki, S.; Sakaguchi, T.; Serizawa, A.; Konno, H.; Baba, S.; Baba, S.; Muro, H. Surgical treatment of patients with mixed hepatocellular carcinoma and cholangiocarcinoma. Cancer 1996, 78, 1671–1676. [Google Scholar] [CrossRef]
- Panjala, C.; Senecal, D.L.; Bridges, M.D.; Kim, G.P.; Nakhleh, R.E.; Nguyen, J.H.; Harnois, D.M. The diagnostic conundrum and liver transplantation outcome for combined hepatocellular-cholangiocarcinoma. Am. J. Transpl. 2010, 10, 1263–1267. [Google Scholar] [CrossRef] [PubMed]
- Sapisochin, G.; Fidelman, N.; Roberts, J.P.; Yao, F.Y. Mixed hepatocellular cholangiocarcinoma and intrahepatic cholangiocarcinoma in patients undergoing transplantation for hepatocellular carcinoma. Liver Transpl. 2011, 17, 934–942. [Google Scholar] [CrossRef] [PubMed]
- Song, S.; Moon, H.H.; Lee, S.; Kim, T.S.; Shin, M.; Kim, J.M.; Park, J.B.; Kwon, C.H.; Kim, S.J.; Lee, S.K.; et al. Comparison between resection and transplantation in combined hepatocellular and cholangiocarcinoma. Transpl. Proc. 2013, 45, 3041–3046. [Google Scholar] [CrossRef]
- Zuo, H.Q.; Yan, L.N.; Zeng, Y.; Yang, J.Y.; Luo, H.Z.; Liu, J.W.; Zhou, L.X. Clinicopathological characteristics of 15 patients with combined hepatocellular carcinoma and cholangiocarcinoma. Hepatobiliary Pancreat. Dis. Int. 2007, 6, 161–165. [Google Scholar]
- Jung, D.H.; Hwang, S.; Song, G.W.; Ahn, C.S.; Moon, D.B.; Kim, K.H.; Ha, T.Y.; Park, G.C.; Hong, S.M.; Kim, W.J.; et al. Longterm prognosis of combined hepatocellular carcinoma-cholangiocarcinoma following liver transplantation and resection. Liver Transpl. 2017, 23, 330–341. [Google Scholar] [CrossRef] [Green Version]
- Ma, K.W.; Chok, K.S.H. Importance of surgical margin in the outcomes of hepatocholangiocarcinoma. World J. Hepatol. 2017, 9, 635–641. [Google Scholar] [CrossRef]
- Vilchez, V.; Shah, M.B.; Daily, M.F.; Pena, L.; Tzeng, C.W.; Davenport, D.; Hosein, P.J.; Gedaly, R.; Maynard, E. Long-term outcome of patients undergoing liver transplantation for mixed hepatocellular carcinoma and cholangiocarcinoma: An analysis of the UNOS database. HPB 2016, 18, 29–34. [Google Scholar] [CrossRef] [Green Version]
- Wu, D.; Shen, Z.Y.; Zhang, Y.M.; Wang, J.; Zheng, H.; Deng, Y.L.; Pan, C. Effect of liver transplantation in combined hepatocellular and cholangiocellular carcinoma: A case series. BMC Cancer 2015, 15, 232. [Google Scholar] [CrossRef] [Green Version]
- Yoon, Y.I.; Hwang, S.; Lee, Y.J.; Kim, K.H.; Ahn, C.S.; Moon, D.B.; Ha, T.Y.; Song, G.W.; Jung, D.H.; Lee, J.W.; et al. Postresection Outcomes of Combined Hepatocellular Carcinoma-Cholangiocarcinoma, Hepatocellular Carcinoma and Intrahepatic Cholangiocarcinoma. J. Gastrointest. Surg. 2016, 20, 411–420. [Google Scholar] [CrossRef]
- Chan, A.C.; Lo, C.M.; Ng, I.O.; Fan, S.T. Liver transplantation for combined hepatocellular cholangiocarcinoma. Asian J. Surg. 2007, 30, 143–146. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fowler, K.; Saad, N.E.; Brunt, E.; Doyle, M.B.; Amin, M.; Vachharajani, N.; Tan, B.; Chapman, W.C. Biphenotypic Primary Liver Carcinomas: Assessing Outcomes of Hepatic Directed Therapy. Ann. Surg. Oncol. 2015, 22, 4130–4137. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.H.; Yoon, H.K.; Ko, G.Y.; Gwon, D.I.; Jang, C.S.; Song, H.Y.; Shin, J.H.; Sung, K.B. Nonresectable combined hepatocellular carcinoma and cholangiocarcinoma: Analysis of the response and prognostic factors after transcatheter arterial chemoembolization. Radiology 2010, 255, 270–277. [Google Scholar] [CrossRef] [PubMed]
- Na, S.K.; Choi, G.H.; Lee, H.C.; Shin, Y.M.; An, J.; Lee, D.; Shim, J.H.; Kim, K.M.; Lim, Y.S.; Chung, Y.H.; et al. The effectiveness of transarterial chemoembolization in recurrent hepatocellular-cholangiocarcinoma after resection. PLoS ONE 2018, 13, e0198138. [Google Scholar] [CrossRef]
- Salimon, M.; Prieux-Klotz, C.; Tougeron, D.; Hautefeuille, V.; Caulet, M.; Gournay, J.; Matysiak-Budnik, T.; Bennouna, J.; Tiako Meyo, M.; Lecomte, T.; et al. Gemcitabine plus platinum-based chemotherapy for first-line treatment of hepatocholangiocarcinoma: An AGEO French multicentre retrospective study. Br. J. Cancer 2018, 118, 325–330. [Google Scholar] [CrossRef] [Green Version]
- Chi, M.; Mikhitarian, K.; Shi, C.; Goff, L.W. Management of combined hepatocellular-cholangiocarcinoma: A case report and literature review. Gastrointest. Cancer Res. 2012, 5, 199–202. [Google Scholar]
- Kobayashi, S.; Terashima, T.; Shiba, S.; Yoshida, Y.; Yamada, I.; Iwadou, S.; Horiguchi, S.; Takahashi, H.; Suzuki, E.; Moriguchi, M.; et al. Multicenter retrospective analysis of systemic chemotherapy for unresectable combined hepatocellular and cholangiocarcinoma. Cancer Sci. 2018, 109, 2549–2557. [Google Scholar] [CrossRef]
- Rogers, J.E.; Bolonesi, R.M.; Rashid, A.; Elsayes, K.M.; Elbanan, M.G.; Law, L.; Kaseb, A.; Shroff, R.T. Systemic therapy for unresectable, mixed hepatocellular-cholangiocarcinoma: Treatment of a rare malignancy. J. Gastrointest. Oncol. 2017, 8, 347–351. [Google Scholar] [CrossRef] [Green Version]
- Trikalinos, N.A.; Zhou, A.; Doyle, M.B.M.; Fowler, K.J.; Morton, A.; Vachharajani, N.; Amin, M.; Keller, J.W.; Chapman, W.C.; Brunt, E.M.; et al. Systemic Therapy for Combined Hepatocellular-Cholangiocarcinoma: A Single-Institution Experience. J. Natl. Compr. Canc. Netw. 2018, 16, 1193–1199. [Google Scholar] [CrossRef]
- Spolverato, G.; Bagante, F.; Weiss, M.; Alexandrescu, S.; Marques, H.P.; Aldrighetti, L.; Maithel, S.K.; Pulitano, C.; Bauer, T.W.; Shen, F.; et al. Comparative performances of the 7th and the 8th editions of the American Joint Committee on Cancer staging systems for intrahepatic cholangiocarcinoma. J. Surg. Oncol. 2017, 115, 696–703. [Google Scholar] [CrossRef]
- Yap, A.Q.; Chen, C.L.; Yong, C.C.; Kuo, F.Y.; Wang, S.H.; Lin, C.C.; Liu, Y.W.; Lin, T.L.; Li, W.F.; Millan, C.A.; et al. Clinicopathological factors impact the survival outcome following the resection of combined hepatocellular carcinoma and cholangiocarcinoma. Surg. Oncol. 2013, 22, 55–60. [Google Scholar] [CrossRef] [PubMed]
- L’Esperance, E.S. Atypical Hemorrhagic Malignant Hepatoma. A Histological Study. J. Med. Res. 1915, 32, 225–250. [Google Scholar]
- Ewing, J. Neoplastic Diseases; Saunders Co.: Philadelphia, PA, USA; London, UK, 1940; Volume 4, p. 740. [Google Scholar]
- Koster, H. Primary duplex liver carcinoma. Am. J. Surg. 1932, 17, 237–241. [Google Scholar] [CrossRef]
- Bonne, C. Cancer and human races. Am. J. Cancer 1937, 435–454. [Google Scholar] [CrossRef] [Green Version]
- Gustafsen, E.G. An analysis of sixty-two cases of primary carcinoma of the liver based on 24,400 necropsies at Bellevue Hospital. Ann. Int. Med. 1937, 5, 889–900. [Google Scholar]
- Warvi, W.N. Primary neoplasms of the liver. Arch. Path. 1944, 37, 367–382. [Google Scholar]
- Goldzieher, M.A. Über multiple Carcinome, ein Beitrag zur Frage der Histogenese des Lebercarcinoms. Virchows Arch. Pathol. Anat. Physiol. Klin. Med. 1928, 267, 326–338. [Google Scholar] [CrossRef]
- Wells, H.G. Primary carcinoma of the liver. Am. J. M. Sci. 1903, 126, 403–417. [Google Scholar] [CrossRef]
- Winternitz, M.C. Primary carcinoma of the liver. Johns Hopkins Hosp. Rep. 1916, 126, 143–184. [Google Scholar]
- Goldzieher, M.; Von Bokay, Z. Der primäre Leberkrebs. Virchows Arch. Pathol. Anat. Physiol. Klin. Med. 1911, 203, 75–131. [Google Scholar] [CrossRef]
- Edmondson, H.A.; Steiner, P.E. Primary carcinoma of the liver: A study of 100 cases among 48,900 necropsies. Cancer 1954, 7, 462–503. [Google Scholar] [CrossRef] [PubMed]
- Popper, H.; Schaffner, F. Liver: Structure and Function; McGraw-Hill: New York, NY, USA, 1957; Volume 599. [Google Scholar]
- Edmondson, H.A. Tumors of the Liver and Intrahepatic Bile Ducts: Atlas of Tumor Pathology; Armed Forces Institute of Pathology: Washington, DC, USA, 1958; Volume 7. [Google Scholar]
- Allen, R.A.; Lisa, J.R. Combined liver cell and bile duct carcinoma. Am. J. Pathol. 1949, 25, 647–655. [Google Scholar] [PubMed]
- Steiner, P.E.; Higginson, J. Cholangiolocellular carcinoma of the liver. Cancer 1959, 12, 753–759. [Google Scholar] [CrossRef] [PubMed]
- Gibson, J. Histological Typing of Tumours of the Liver, Biliary Tract and Pancreas; World Health Organization: Geneva, Switzerland, 1978. [Google Scholar]
- Falkowski, O.; An, H.J.; Ianus, I.A.; Chiriboga, L.; Yee, H.; West, A.B.; Theise, N.D. Regeneration of hepatocyte ‘buds’ in cirrhosis from intrabiliary stem cells. J. Hepatol. 2003, 39, 357–364. [Google Scholar] [CrossRef]
- Fujii, T.; Zen, Y.; Harada, K.; Niwa, H.; Masuda, S.; Kaizaki, Y.; Watanabe, K.; Kawashima, A.; Nakanuma, Y. Participation of liver cancer stem/progenitor cells in tumorigenesis of scirrhous hepatocellular carcinoma--human and cell culture study. Hum. Pathol. 2008, 39, 1185–1196. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.; Park, C.; Han, K.H.; Choi, J.; Kim, Y.B.; Kim, J.K.; Park, Y.N. Primary liver carcinoma of intermediate (hepatocyte-cholangiocyte) phenotype. J. Hepatol. 2004, 40, 298–304. [Google Scholar] [CrossRef]
- Komuta, M.; Spee, B.; Vander Borght, S.; De Vos, R.; Verslype, C.; Aerts, R.; Yano, H.; Suzuki, T.; Matsuda, M.; Fujii, H.; et al. Clinicopathological study on cholangiolocellular carcinoma suggesting hepatic progenitor cell origin. Hepatology 2008, 47, 1544–1556. [Google Scholar] [CrossRef] [Green Version]
- Kuwahara, R.; Kofman, A.V.; Landis, C.S.; Swenson, E.S.; Barendswaard, E.; Theise, N.D. The hepatic stem cell niche: Identification by label-retaining cell assay. Hepatology 2008, 47, 1994–2002. [Google Scholar] [CrossRef] [Green Version]
- Theise, N.D.; Saxena, R.; Portmann, B.C.; Thung, S.N.; Yee, H.; Chiriboga, L.; Kumar, A.; Crawford, J.M. The canals of Hering and hepatic stem cells in humans. Hepatology 1999, 30, 1425–1433. [Google Scholar] [CrossRef]
- Shiota, K.; Taguchi, J.; Nakashima, O.; Nakashima, M.; Kojiro, M. Clinicopathologic study on cholangiolocellular carcinoma. Oncol. Rep. 2001, 8, 263–268. [Google Scholar] [CrossRef]
- Brunt, E.; Aishima, S.; Clavien, P.A.; Fowler, K.; Goodman, Z.; Gores, G.; Gouw, A.; Kagen, A.; Klimstra, D.; Komuta, M.; et al. cHCC-CCA: Consensus terminology for primary liver carcinomas with both hepatocytic and cholangiocytic differentation. Hepatology 2018, 68, 113–126. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sasaki, M.; Sato, H.; Kakuda, Y.; Sato, Y.; Choi, J.H.; Nakanuma, Y. Clinicopathological significance of ‘subtypes with stem-cell feature’ in combined hepatocellular-cholangiocarcinoma. Liver Int. 2015, 35, 1024–1035. [Google Scholar] [CrossRef] [PubMed]
- Yan, B.C.; Gong, C.; Song, J.; Krausz, T.; Tretiakova, M.; Hyjek, E.; Al-Ahmadie, H.; Alves, V.; Xiao, S.Y.; Anders, R.A.; et al. Arginase-1: A new immunohistochemical marker of hepatocytes and hepatocellular neoplasms. Am. J. Surg. Pathol. 2010, 34, 1147–1154. [Google Scholar] [CrossRef]
- Borscheri, N.; Roessner, A.; Rocken, C. Canalicular immunostaining of neprilysin (CD10) as a diagnostic marker for hepatocellular carcinomas. Am. J. Surg. Pathol. 2001, 25, 1297–1303. [Google Scholar] [CrossRef]
- Haratake, J.; Hashimoto, H. An immunohistochemical analysis of 13 cases with combined hepatocellular and cholangiocellular carcinoma. Liver 1995, 15, 9–15. [Google Scholar] [CrossRef] [PubMed]
- Leong, A.S.; Sormunen, R.T.; Tsui, W.M.; Liew, C.T. Hep Par 1 and selected antibodies in the immunohistological distinction of hepatocellular carcinoma from cholangiocarcinoma, combined tumours and metastatic carcinoma. Histopathology 1998, 33, 318–324. [Google Scholar] [CrossRef] [PubMed]
- Papotti, M.; Sambataro, D.; Marchesa, P.; Negro, F. A combined hepatocellular/cholangiocellular carcinoma with sarcomatoid features. Liver 1997, 17, 47–52. [Google Scholar] [CrossRef]
- Thung, S.N.; Gerber, M.A.; Sarno, E.; Popper, H. Distribution of five antigens in hepatocellular carcinoma. Lab. Investig. 1979, 41, 101–105. [Google Scholar]
- Xiao, S.Y.; Wang, H.L.; Hart, J.; Fleming, D.; Beard, M.R. cDNA arrays and immunohistochemistry identification of CD10/CALLA expression in hepatocellular carcinoma. Am. J. Pathol. 2001, 159, 1415–1421. [Google Scholar] [CrossRef] [Green Version]
- Tickoo, S.K.; Zee, S.Y.; Obiekwe, S.; Xiao, H.; Koea, J.; Robiou, C.; Blumgart, L.H.; Jarnagin, W.; Ladanyi, M.; Klimstra, D.S. Combined hepatocellular-cholangiocarcinoma: A histopathologic, immunohistochemical, and in situ hybridization study. Am. J. Surg. Pathol. 2002, 26, 989–997. [Google Scholar] [CrossRef]
- Martin de las Mulas, J.; Gomez-Villamandos, J.C.; Perez, J.; Mozos, E.; Estrado, M.; Mendez, A. Immunohistochemical evaluation of canine primary liver carcinomas: Distribution of alpha-fetoprotein, carcinoembryonic antigen, keratins and vimentin. Res. Vet. Sci. 1995, 59, 124–127. [Google Scholar] [CrossRef] [PubMed]
- Kwaspen, F.H.; Smedts, F.M.; Broos, A.; Bulten, H.; Debie, W.M.; Ramaekers, F.C. Reproducible and highly sensitive detection of the broad spectrum epithelial marker keratin 19 in routine cancer diagnosis. Histopathology 1997, 31, 503–516. [Google Scholar] [CrossRef] [Green Version]
- Ding, S.J.; Li, Y.; Tan, Y.X.; Jiang, M.R.; Tian, B.; Liu, Y.K.; Shao, X.X.; Ye, S.L.; Wu, J.R.; Zeng, R.; et al. From proteomic analysis to clinical significance: Overexpression of cytokeratin 19 correlates with hepatocellular carcinoma metastasis. Mol. Cell Proteom. 2004, 3, 73–81. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Uenishi, T.; Kubo, S.; Yamamoto, T.; Shuto, T.; Ogawa, M.; Tanaka, H.; Tanaka, S.; Kaneda, K.; Hirohashi, K. Cytokeratin 19 expression in hepatocellular carcinoma predicts early postoperative recurrence. Cancer Sci. 2003, 94, 851–857. [Google Scholar] [CrossRef]
- Ferrone, C.R.; Ting, D.T.; Shahid, M.; Konstantinidis, I.T.; Sabbatino, F.; Goyal, L.; Rice-Stitt, T.; Mubeen, A.; Arora, K.; Bardeesey, N.; et al. The Ability to Diagnose Intrahepatic Cholangiocarcinoma Definitively Using Novel Branched DNA-Enhanced Albumin RNA In Situ Hybridization Technology. Ann. Surg. Oncol. 2016, 23, 290–296. [Google Scholar] [CrossRef]
- Krings, G.; Ramachandran, R.; Jain, D.; Wu, T.T.; Yeh, M.M.; Torbenson, M.; Kakar, S. Immunohistochemical pitfalls and the importance of glypican 3 and arginase in the diagnosis of scirrhous hepatocellular carcinoma. Mod. Pathol. 2013, 26, 782–791. [Google Scholar] [CrossRef] [Green Version]
- Radwan, N.A.; Ahmed, N.S. The diagnostic value of arginase-1 immunostaining in differentiating hepatocellular carcinoma from metastatic carcinoma and cholangiocarcinoma as compared to HepPar-1. Diagn. Pathol. 2012, 7, 149. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Terada, T. Combined hepatocellular-cholangiocarcinoma with stem cell features, ductal plate malformation subtype: A case report and proposal of a new subtype. Int. J. Clin. Exp. Pathol. 2013, 6, 737–748. [Google Scholar]
- Xu, J.; Zhang, C.; Qiao, A.; Xi, Y. Combined hepatocellular-cholangiocarcinoma (cholangiolocellular type) with stem-cell features: A clinicopathologic analysis of 26 cases. Zhonghua Bing Li Xue Za Zhi 2016, 45, 175–179. [Google Scholar] [CrossRef]
- Zhao, Q.; Yu, W.L.; Lu, X.Y.; Dong, H.; Gu, Y.J.; Sheng, X.; Cong, W.M.; Wu, M.C. Combined hepatocellular and cholangiocarcinoma originating from the same clone: A pathomolecular evidence-based study. Chin. J. Cancer 2016, 35, 82. [Google Scholar] [CrossRef] [Green Version]
- Pozharisskii, K.M.; Granov, D.A.; Ten, V.P.; Kubaibergenova, A.G.; Leenman, E.E.; Rasskazov, A.I. The significance of immunohistochemistry in the investigation of liver neoplasms: Differential diagnosis, prognostic markers. Vopr. Onkol. 2008, 54, 417–433. [Google Scholar] [PubMed]
- Akiba, J.; Nakashima, O.; Hattori, S.; Naito, Y.; Kusano, H.; Kondo, R.; Nakayama, M.; Tanikawa, K.; Todoroki, K.; Umeno, Y.; et al. The expression of arginase-1, keratin (K) 8 and K18 in combined hepatocellular-cholangiocarcinoma, subtypes with stem-cell features, intermediate-cell type. J. Clin. Pathol. 2016, 69, 846–851. [Google Scholar] [CrossRef] [PubMed]
- Balaton, A.J.; Nehama-Sibony, M.; Gotheil, C.; Callard, P.; Baviera, E.E. Distinction between hepatocellular carcinoma, cholangiocarcinoma, and metastatic carcinoma based on immunohistochemical staining for carcinoembryonic antigen and for cytokeratin 19 on paraffin sections. J. Pathol. 1988, 156, 305–310. [Google Scholar] [CrossRef]
- Brumm, C.; Schulze, C.; Charels, K.; Morohoshi, T.; Kloppel, G. The significance of alpha-fetoprotein and other tumour markers in differential immunocytochemistry of primary liver tumours. Histopathology 1989, 14, 503–513. [Google Scholar] [CrossRef]
- Ganjei, P.; Nadji, M.; Albores-Saavedra, J.; Morales, A.R. Histologic markers in primary and metastatic tumors of the liver. Cancer 1988, 62, 1994–1998. [Google Scholar] [CrossRef] [PubMed]
- Moll, R.; Divo, M.; Langbein, L. The human keratins: Biology and pathology. Histochem. Cell Biol. 2008, 129, 705–733. [Google Scholar] [CrossRef] [Green Version]
- Schweizer, J.; Bowden, P.E.; Coulombe, P.A.; Langbein, L.; Lane, E.B.; Magin, T.M.; Maltais, L.; Omary, M.B.; Parry, D.A.; Rogers, M.A.; et al. New consensus nomenclature for mammalian keratins. J. Cell Biol. 2006, 174, 169–174. [Google Scholar] [CrossRef] [Green Version]
- Lin, W.L.; Chen, F.L.; Han, C.P. Anti-cytokeratin CAM5.2 (BD Biosciences) and CK8 give no remarkable advantages to the pancytokeratin cocktail of antibodies (AE1/AE3, CAM5.2, MNF116, CK8, and CK18) in detecting disseminated tumor cells in biologic subtypes of stage I-III breast cancer patients. Ann. Surg. Oncol. 2011, 18, S261–S262, author reply S263–S264. [Google Scholar] [CrossRef]
- Tang, W.; Guo, Q.; Qu, X.; Inagaki, Y.; Seyama, Y.; Midorikawa, Y.; Gai, R.; Kokudo, N.; Sugawara, Y.; Nakata, M.; et al. KL-6 mucin is a useful immunohistochemical marker for cholangiocarcinoma. Oncol. Rep. 2007, 17, 737–741. [Google Scholar] [CrossRef] [Green Version]
- Xu, J.; Sasaki, M.; Harada, K.; Sato, Y.; Ikeda, H.; Kim, J.H.; Yu, E.; Nakanuma, Y. Intrahepatic cholangiocarcinoma arising in chronic advanced liver disease and the cholangiocarcinomatous component of hepatocellular cholangiocarcinoma share common phenotypes and cholangiocarcinogenesis. Histopathology 2011, 59, 1090–1099. [Google Scholar] [CrossRef]
- Zhang, F.; Chen, X.P.; Zhang, W.; Dong, H.H.; Xiang, S.; Zhang, W.G.; Zhang, B.X. Combined hepatocellular cholangiocarcinoma originating from hepatic progenitor cells: Immunohistochemical and double-fluorescence immunostaining evidence. Histopathology 2008, 52, 224–232. [Google Scholar] [CrossRef]
- Kim, R.; Kim, S.B.; Cho, E.H.; Park, S.H.; Park, S.B.; Hong, S.K.; Chae, G. CD44 expression in patients with combined hepatocellular cholangiocarcinoma. Ann. Surg. Treat. Res. 2015, 89, 9–16. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Malvi, D.; de Biase, D.; Fittipaldi, S.; Grillini, M.; Visani, M.; Pession, A.; D’Errico, A.; Vasuri, F. Immunomorphology and molecular biology of mixed primary liver cancers: Is Nestin a marker of intermediate-cell carcinoma? Histopathology 2020, 76, 265–274. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.I.; Lee, J.W.; Kim, J.M.; Kim, J.K.; Chung, H.J.; Kim, Y.S. Prognosis of hepatocellular carcinoma expressing cytokeratin 19: Comparison with other liver cancers. World J. Gastroenterol. 2012, 18, 4751–4757. [Google Scholar] [CrossRef] [PubMed]
- Wakizaka, K.; Yokoo, H.; Kamiyama, T.; Kakisaka, T.; Ohira, M.; Tani, M.; Kato, K.; Fujii, Y.; Sugiyama, K.; Nagatsu, A.; et al. CD133 and epithelial cell adhesion molecule expressions in the cholangiocarcinoma component are prognostic factors for combined hepatocellular cholangiocarcinoma. Hepatol. Res. 2020, 50, 258–267. [Google Scholar] [CrossRef]
- Ikeda, H.; Harada, K.; Sato, Y.; Sasaki, M.; Yoneda, N.; Kitamura, S.; Sudo, Y.; Ooi, A.; Nakanuma, Y. Clinicopathologic significance of combined hepatocellular-cholangiocarcinoma with stem cell subtype components with reference to the expression of putative stem cell markers. Am. J. Clin. Pathol. 2013, 140, 329–340. [Google Scholar] [CrossRef] [Green Version]
- Huang, J.; Zhang, X.; Zhang, M.; Zhu, J.D.; Zhang, Y.L.; Lin, Y.; Wang, K.S.; Qi, X.F.; Zhang, Q.; Liu, G.Z.; et al. Up-regulation of DLK1 as an imprinted gene could contribute to human hepatocellular carcinoma. Carcinogenesis 2007, 28, 1094–1103. [Google Scholar] [CrossRef] [Green Version]
- Yanai, H.; Nakamura, K.; Hijioka, S.; Kamei, A.; Ikari, T.; Ishikawa, Y.; Shinozaki, E.; Mizunuma, N.; Hatake, K.; Miyajima, A. Dlk-1, a cell surface antigen on foetal hepatic stem/progenitor cells, is expressed in hepatocellular, colon, pancreas and breast carcinomas at a high frequency. J. Biochem. 2010, 148, 85–92. [Google Scholar] [CrossRef]
- Xu, X.; Liu, R.F.; Zhang, X.; Huang, L.Y.; Chen, F.; Fei, Q.L.; Han, Z.G. DLK1 as a potential target against cancer stem/progenitor cells of hepatocellular carcinoma. Mol. Cancer Ther. 2012, 11, 629–638. [Google Scholar] [CrossRef] [Green Version]
- Foster, B.M.; Zaidi, D.; Young, T.R.; Mobley, M.E.; Kerr, B.A. CD117/c-kit in Cancer Stem Cell-Mediated Progression and Therapeutic Resistance. Biomedicines 2018, 6, 31. [Google Scholar] [CrossRef] [Green Version]
- Sasaki, M.; Sato, Y.; Nakanuma, Y. Is nestin a diagnostic marker for combined hepatocellular-cholangiocarcinoma? Histopathology 2022, 80, 859–868. [Google Scholar] [CrossRef] [PubMed]
- Nomoto, K.; Tsuneyama, K.; Cheng, C.; Takahashi, H.; Hori, R.; Murai, Y.; Takano, Y. Intrahepatic cholangiocarcinoma arising in cirrhotic liver frequently expressed p63-positive basal/stem-cell phenotype. Pathol. Res. Pract. 2006, 202, 71–76. [Google Scholar] [CrossRef]
- Saarnio, J.; Parkkila, S.; Parkkila, A.K.; Pastorekova, S.; Haukipuro, K.; Pastorek, J.; Juvonen, T.; Karttunen, T.J. Transmembrane carbonic anhydrase, MN/CA IX, is a potential biomarker for biliary tumours. J. Hepatol. 2001, 35, 643–649. [Google Scholar] [CrossRef]
- Patil, P.A.; Taddei, T.; Jain, D.; Zhang, X. HNF-1beta is a More Sensitive and Specific Marker Than C-Reactive Protein for Identifying Biliary Differentiation in Primary Hepatic Carcinomas. Arch. Pathol. Lab. Med. 2022, 146, 220–226. [Google Scholar] [CrossRef] [PubMed]
- Lau, S.K.; Prakash, S.; Geller, S.A.; Alsabeh, R. Comparative immunohistochemical profile of hepatocellular carcinoma, cholangiocarcinoma, and metastatic adenocarcinoma. Hum. Pathol. 2002, 33, 1175–1181. [Google Scholar] [CrossRef]
- Endo, T.; Yoshikawa, M.; Ebara, M.; Kato, K.; Sunaga, M.; Fukuda, H.; Hayasaka, A.; Kondo, F.; Sugiura, N.; Saisho, H. Immunohistochemical metallothionein expression in hepatocellular carcinoma: Relation to tumor progression and chemoresistance to platinum agents. J. Gastroenterol. 2004, 39, 1196–1201. [Google Scholar] [CrossRef] [PubMed]
- Huang, G.W.; Yang, L.Y. Metallothionein expression in hepatocellular carcinoma. World J. Gastroenterol. 2002, 8, 650–653. [Google Scholar] [CrossRef]
- Stenram, U.; Ohlsson, B.; Tranberg, K.G. Immunohistochemical expression of metallothionein in resected hepatic primary tumors and colorectal carcinoma metastases. Apmis 1999, 107, 420–424. [Google Scholar] [CrossRef] [PubMed]
- Sasaki, M.; Nakanuma, Y. Expression of mucin core protein of mammary type in primary liver cancer. Hepatology 1994, 20, 1192–1197. [Google Scholar] [CrossRef]
- Sasaki, M.; Nakanuma, Y.; Ho, S.B.; Kim, Y.S. Cholangiocarcinomas arising in cirrhosis and combined hepatocellular-cholangiocellular carcinomas share apomucin profiles. Am. J. Clin. Pathol. 1998, 109, 302–308. [Google Scholar] [CrossRef]
- Sasaki, M.; Nakanuma, Y.; Kim, Y.S. Characterization of apomucin expression in intrahepatic cholangiocarcinomas and their precursor lesions: An immunohistochemical study. Hepatology 1996, 24, 1074–1078. [Google Scholar] [CrossRef] [PubMed]
- Dorn, L.; Menezes, L.F.; Mikuz, G.; Otto, H.F.; Onuchic, L.F.; Sergi, C. Immunohistochemical detection of polyductin and co-localization with liver progenitor cell markers during normal and abnormal development of the intrahepatic biliary system and in adult hepatobiliary carcinomas. J. Cell Mol. Med. 2009, 13, 1279–1290. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Haratake, J.; Horie, A. An immunohistochemical study of sarcomatoid liver carcinomas. Cancer 1991, 68, 93–97. [Google Scholar] [CrossRef] [PubMed]
- Van Haele, M.; Moya, I.M.; Karaman, R.; Rens, G.; Snoeck, J.; Govaere, O.; Nevens, F.; Verslype, C.; Topal, B.; Monbaliu, D.; et al. YAP and TAZ Heterogeneity in Primary Liver Cancer: An Analysis of Its Prognostic and Diagnostic Role. Int. J. Mol. Sci. 2019, 20. [Google Scholar] [CrossRef] [Green Version]
- He, C.; Yin, H.F.; Liu, P.; Zhang, Y.; Zhang, J.B. Clinicopathologic features of combined hepatic carcinoma. Zhonghua Bing Li Xue Za Zhi 2013, 42, 824–828. [Google Scholar] [PubMed]
- Ishak, K.G. Tumors of the Liver and Intrahepatic Bile Ducts. AFIP Atlas Tumor Pathol. 1999, 25, 221. [Google Scholar]
- Akiba, J.; Nakashima, O.; Hattori, S.; Tanikawa, K.; Takenaka, M.; Nakayama, M.; Kondo, R.; Nomura, Y.; Koura, K.; Ueda, K.; et al. Clinicopathologic analysis of combined hepatocellular-cholangiocarcinoma according to the latest WHO classification. Am. J. Surg. Pathol. 2013, 37, 496–505. [Google Scholar] [CrossRef]
- Sun, D.W.; Zhang, Y.Y.; Sun, X.D.; Chen, Y.G.; Qiu, W.; Ji, M.; Lv, G.Y. Prognostic value of cytokeratin 19 in hepatocellular carcinoma: A meta-analysis. Clin. Chim. Acta 2015, 448, 161–169. [Google Scholar] [CrossRef]
- Niewczas, M.; Paczek, L.; Krawczyk, M.; Pawlak, J.; Bartlomiejczyk, I.; Gornicka, B. Enzymatic activity of cathepsin B, cathepsin B and L, plasmin, trypsin and collagenase in hepatocellular carcinoma. Pol. Arch. Med. Wewn. 2002, 108, 653–662. [Google Scholar]
- Ruan, J.; Zheng, H.; Rong, X.; Rong, X.; Zhang, J.; Fang, W.; Zhao, P.; Luo, R. Over-expression of cathepsin B in hepatocellular carcinomas predicts poor prognosis of HCC patients. Mol. Cancer 2016, 15, 17. [Google Scholar] [CrossRef] [Green Version]
- Terada, T.; Ohta, T.; Minato, H.; Nakanuma, Y. Expression of pancreatic trypsinogen/trypsin and cathepsin B in human cholangiocarcinomas and hepatocellular carcinomas. Hum. Pathol. 1995, 26, 746–752. [Google Scholar] [CrossRef] [PubMed]
- Xu, Z.Z.; Xiu, P.; Lv, J.W.; Wang, F.H.; Dong, X.F.; Liu, F.; Li, T.; Li, J. Integrin alphavbeta3 is required for cathepsin B-induced hepatocellular carcinoma progression. Mol. Med. Rep. 2015, 11, 3499–3504. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cai, X.; Zhai, J.; Kaplan, D.E.; Zhang, Y.; Zhou, L.; Chen, X.; Qian, G.; Zhao, Q.; Li, Y.; Gao, L.; et al. Background progenitor activation is associated with recurrence after hepatectomy of combined hepatocellular-cholangiocarcinoma. Hepatology 2012, 56, 1804–1816. [Google Scholar] [CrossRef]
- Fucich, L.F.; Cheles, M.K.; Thung, S.N.; Gerber, M.A.; Marrogi, A.J. Primary vs metastatic hepatic carcinoma. An immunohistochemical study of 34 cases. Arch. Pathol. Lab. Med. 1994, 118, 927–930. [Google Scholar] [PubMed]
- Ha, S.Y.; Song, D.H.; Hwang, S.H.; Cho, S.Y.; Park, C.K. Expression of prothymosin alpha predicts early recurrence and poor prognosis of hepatocellular carcinoma. Hepatobiliary Pancreat. Dis. Int. 2015, 14, 171–177. [Google Scholar] [CrossRef]
- Kim, G.J.; Kim, H.; Park, Y.N. Increased expression of Yes-associated protein 1 in hepatocellular carcinoma with stemness and combined hepatocellular-cholangiocarcinoma. PLoS ONE 2013, 8, e75449. [Google Scholar] [CrossRef]
- Lee, K.P.; Lee, J.H.; Kim, T.S.; Kim, T.H.; Park, H.D.; Byun, J.S.; Kim, M.C.; Jeong, W.I.; Calvisi, D.F.; Kim, J.M.; et al. The Hippo-Salvador pathway restrains hepatic oval cell proliferation, liver size, and liver tumorigenesis. Proc. Natl. Acad. Sci. USA 2010, 107, 8248–8253. [Google Scholar] [CrossRef] [Green Version]
- Li, X.; Tao, J.; Cigliano, A.; Sini, M.; Calderaro, J.; Azoulay, D.; Wang, C.; Liu, Y.; Jiang, L.; Evert, K.; et al. Co-activation of PIK3CA and Yap promotes development of hepatocellular and cholangiocellular tumors in mouse and human liver. Oncotarget 2015, 6, 10102–10115. [Google Scholar] [CrossRef] [Green Version]
- Xue, R.; Chen, L.; Zhang, C.; Fujita, M.; Li, R.; Yan, S.M.; Ong, C.K.; Liao, X.; Gao, Q.; Sasagawa, S.; et al. Genomic and Transcriptomic Profiling of Combined Hepatocellular and Intrahepatic Cholangiocarcinoma Reveals Distinct Molecular Subtypes. Cancer Cell 2019, 35, 932–947.e8. [Google Scholar] [CrossRef]
- Sasaki, M.; Nitta, T.; Sato, Y.; Nakanuma, Y. Loss of ARID1A Expression Presents a Novel Pathway of Carcinogenesis in Biliary Carcinomas. Am. J. Clin. Pathol. 2016, 145, 815–825. [Google Scholar] [CrossRef] [Green Version]
- Sasaki, M.; Yamato, T.; Nakanuma, Y. Expression of sialyl-Tn, Tn and T antigens in primary liver cancer. Pathol. Int. 1999, 49, 325–331. [Google Scholar] [CrossRef] [PubMed]
- Suceveanu, A.I.; Micu, I.S.; Baltatescu, G.I.; Petcu, L.C.; Dobrin, N.; Brinzan, C.; Nitipir, C.; Mazilu, L.; Botea, F.; Herlea, V.; et al. Overexpression of Survivin-1, TAG-72 and HERC5 in patients diagnosed with hepatocellular carcinoma in the Black Sea coast geographical area. Exp. Ther. Med. 2021, 21, 284. [Google Scholar] [CrossRef] [PubMed]
- Ng, I.O.; Shek, T.W.; Nicholls, J.; Ma, L.T. Combined hepatocellular-cholangiocarcinoma: A clinicopathological study. J. Gastroenterol. Hepatol. 1998, 13, 34–40. [Google Scholar] [CrossRef]
- Schulze, K.; Imbeaud, S.; Letouze, E.; Alexandrov, L.B.; Calderaro, J.; Rebouissou, S.; Couchy, G.; Meiller, C.; Shinde, J.; Soysouvanh, F.; et al. Exome sequencing of hepatocellular carcinomas identifies new mutational signatures and potential therapeutic targets. Nat. Genet. 2015, 47, 505–511. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zou, S.; Li, J.; Zhou, H.; Frech, C.; Jiang, X.; Chu, J.S.; Zhao, X.; Li, Y.; Li, Q.; Wang, H.; et al. Mutational landscape of intrahepatic cholangiocarcinoma. Nat. Commun. 2014, 5, 5696. [Google Scholar] [CrossRef] [Green Version]
- Sia, D.; Hoshida, Y.; Villanueva, A.; Roayaie, S.; Ferrer, J.; Tabak, B.; Peix, J.; Sole, M.; Tovar, V.; Alsinet, C.; et al. Integrative molecular analysis of intrahepatic cholangiocarcinoma reveals 2 classes that have different outcomes. Gastroenterology 2013, 144, 829–840. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ishii, Y.; Sasaki, T.; Serikawa, M.; Minami, T.; Okazaki, A.; Yukutake, M.; Ishigaki, T.; Kosaka, K.; Mouri, T.; Yoshimi, S.; et al. Elevated expression of cyclooxygenase-2 and microsomal prostaglandin E synthase-1 in primary sclerosing cholangitis: Iotamplications for cholangiocarcinogenesis. Int. J. Oncol. 2013, 43, 1073–1079. [Google Scholar] [CrossRef] [Green Version]
- Zhou, H.; Wang, H.; Zhou, D.; Wang, H.; Wang, Q.; Zou, S.; Tu, Q.; Wu, M.; Hu, H. Hepatitis B virus-associated intrahepatic cholangiocarcinoma and hepatocellular carcinoma may hold common disease process for carcinogenesis. Eur. J. Cancer 2010, 46, 1056–1061. [Google Scholar] [CrossRef]
- Akita, M.; Fujikura, K.; Ajiki, T.; Fukumoto, T.; Otani, K.; Azuma, T.; Itoh, T.; Ku, Y.; Zen, Y. Dichotomy in intrahepatic cholangiocarcinomas based on histologic similarities to hilar cholangiocarcinomas. Mod. Pathol. 2017, 30, 986–997. [Google Scholar] [CrossRef] [Green Version]
- Saha, S.K.; Parachoniak, C.A.; Ghanta, K.S.; Fitamant, J.; Ross, K.N.; Najem, M.S.; Gurumurthy, S.; Akbay, E.A.; Sia, D.; Cornella, H.; et al. Mutant IDH inhibits HNF-4alpha to block hepatocyte differentiation and promote biliary cancer. Nature 2014, 513, 110–114. [Google Scholar] [CrossRef] [Green Version]
- Durnez, A.; Verslype, C.; Nevens, F.; Fevery, J.; Aerts, R.; Pirenne, J.; Lesaffre, E.; Libbrecht, L.; Desmet, V.; Roskams, T. The clinicopathological and prognostic relevance of cytokeratin 7 and 19 expression in hepatocellular carcinoma. A possible progenitor cell origin. Histopathology 2006, 49, 138–151. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.; Park, Y.N. Hepatocellular carcinomas expressing ‘stemness’-related markers: Clinicopathological characteristics. Dig. Dis. 2014, 32, 778–785. [Google Scholar] [CrossRef]
- Fujii, H.; Zhu, X.G.; Matsumoto, T.; Inagaki, M.; Tokusashi, Y.; Miyokawa, N.; Fukusato, T.; Uekusa, T.; Takagaki, T.; Kadowaki, N.; et al. Genetic classification of combined hepatocellular-cholangiocarcinoma. Hum. Pathol. 2000, 31, 1011–1017. [Google Scholar] [CrossRef]
- Cazals-Hatem, D.; Rebouissou, S.; Bioulac-Sage, P.; Bluteau, O.; Blanche, H.; Franco, D.; Monges, G.; Belghiti, J.; Sa Cunha, A.; Laurent-Puig, P.; et al. Clinical and molecular analysis of combined hepatocellular-cholangiocarcinomas. J. Hepatol. 2004, 41, 292–298. [Google Scholar] [CrossRef] [PubMed]
- Homayounfar, K.; Gunawan, B.; Cameron, S.; Haller, F.; Baumhoer, D.; Uecker, S.; Sander, B.; Ramadori, G.; Lorf, T.; Fuzesi, L. Pattern of chromosomal aberrations in primary liver cancers identified by comparative genomic hybridization. Hum. Pathol. 2009, 40, 834–842. [Google Scholar] [CrossRef]
- Joseph, N.M.; Tsokos, C.G.; Umetsu, S.E.; Shain, A.H.; Kelley, R.K.; Onodera, C.; Bowman, S.; Talevich, E.; Ferrell, L.D.; Kakar, S.; et al. Genomic profiling of combined hepatocellular-cholangiocarcinoma reveals similar genetics to hepatocellular carcinoma. J. Pathol. 2019, 248, 164–178. [Google Scholar] [CrossRef] [PubMed]
- Fujimoto, A.; Furuta, M.; Shiraishi, Y.; Gotoh, K.; Kawakami, Y.; Arihiro, K.; Nakamura, T.; Ueno, M.; Ariizumi, S.; Nguyen, H.H.; et al. Whole-genome mutational landscape of liver cancers displaying biliary phenotype reveals hepatitis impact and molecular diversity. Nat. Commun. 2015, 6, 6120. [Google Scholar] [CrossRef] [Green Version]
- Gigante, E.; Ronot, M.; Bertin, C.; Ciolina, M.; Bouattour, M.; Dondero, F.; Cauchy, F.; Soubrane, O.; Vilgrain, V.; Paradis, V. Combining imaging and tumour biopsy improves the diagnosis of combined hepatocellular-cholangiocarcinoma. Liver Int. 2019, 39, 2386–2396. [Google Scholar] [CrossRef]
- Paterlini-Brechot, P.; Benali, N.L. Circulating tumor cells (CTC) detection: Clinical impact and future directions. Cancer Lett. 2007, 253, 180–204. [Google Scholar] [CrossRef]
- Guo, W.; Sun, Y.F.; Shen, M.N.; Ma, X.L.; Wu, J.; Zhang, C.Y.; Zhou, Y.; Xu, Y.; Hu, B.; Zhang, M.; et al. Circulating Tumor Cells with Stem-Like Phenotypes for Diagnosis, Prognosis, and Therapeutic Response Evaluation in Hepatocellular Carcinoma. Clin. Cancer Res. 2018, 24, 2203–2213. [Google Scholar] [CrossRef] [Green Version]
- Guo, W.; Yang, X.R.; Sun, Y.F.; Shen, M.N.; Ma, X.L.; Wu, J.; Zhang, C.Y.; Zhou, Y.; Xu, Y.; Hu, B.; et al. Clinical significance of EpCAM mRNA-positive circulating tumor cells in hepatocellular carcinoma by an optimized negative enrichment and qRT-PCR-based platform. Clin. Cancer Res. 2014, 20, 4794–4805. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bahnassy, A.A.; Zekri, A.R.; El-Bastawisy, A.; Fawzy, A.; Shetta, M.; Hussein, N.; Omran, D.; Ahmed, A.A.; El-Labbody, S.S. Circulating tumor and cancer stem cells in hepatitis C virus-associated liver disease. World J. Gastroenterol. 2014, 20, 18240–18248. [Google Scholar] [CrossRef] [PubMed]
- Bhan, I.; Mosesso, K.; Goyal, L.; Philipp, J.; Kalinich, M.; Franses, J.W.; Choz, M.; Oklu, R.; Toner, M.; Maheswaran, S.; et al. Detection and Analysis of Circulating Epithelial Cells in Liquid Biopsies From Patients With Liver Disease. Gastroenterology 2018, 155, 2016–2018.e11. [Google Scholar] [CrossRef] [PubMed]
- Kelley, R.K.; Magbanua, M.J.; Butler, T.M.; Collisson, E.A.; Hwang, J.; Sidiropoulos, N.; Evason, K.; McWhirter, R.M.; Hameed, B.; Wayne, E.M.; et al. Circulating tumor cells in hepatocellular carcinoma: A pilot study of detection, enumeration, and next-generation sequencing in cases and controls. BMC Cancer 2015, 15, 206. [Google Scholar] [CrossRef] [PubMed]
- Xue, F.; Shi, S.; Zhang, Z.; Xu, C.; Zheng, J.; Qin, T.; Qian, Z.; Zhao, X.; Tong, Y.; Xia, L.; et al. Application of a novel liquid biopsy in patients with hepatocellular carcinoma undergoing liver transplantation. Oncol. Lett. 2018, 15, 5481–5488. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yin, L.C.; Luo, Z.C.; Gao, Y.X.; Li, Y.; Peng, Q.; Gao, Y. Twist Expression in Circulating Hepatocellular Carcinoma Cells Predicts Metastasis and Prognoses. Biomed. Res. Int. 2018, 2018, 3789613. [Google Scholar] [CrossRef] [PubMed]
- Cheng, Y.; Luo, L.; Zhang, J.; Zhou, M.; Tang, Y.; He, G.; Lu, Y.; Wang, Z.; Pan, M. Diagnostic Value of Different Phenotype Circulating Tumor Cells in Hepatocellular Carcinoma. J. Gastrointest Surg. 2019, 23, 2354–2361. [Google Scholar] [CrossRef]
- Sun, Y.F.; Xu, Y.; Yang, X.R.; Guo, W.; Zhang, X.; Qiu, S.J.; Shi, R.Y.; Hu, B.; Zhou, J.; Fan, J. Circulating stem cell-like epithelial cell adhesion molecule-positive tumor cells indicate poor prognosis of hepatocellular carcinoma after curative resection. Hepatology 2013, 57, 1458–1468. [Google Scholar] [CrossRef]
- Zhou, Y.; Wang, B.; Wu, J.; Zhang, C.; Zhou, Y.; Yang, X.; Zhou, J.; Guo, W.; Fan, J. Association of preoperative EpCAM Circulating Tumor Cells and peripheral Treg cell levels with early recurrence of hepatocellular carcinoma following radical hepatic resection. BMC Cancer 2016, 16, 506. [Google Scholar] [CrossRef] [Green Version]
- Chen, K.; Zhang, H.; Zhang, L.N.; Ju, S.Q.; Qi, J.; Huang, D.F.; Li, F.; Wei, Q.; Zhang, J. Value of circulating cell-free DNA in diagnosis of hepatocelluar carcinoma. World J. Gastroenterol. 2013, 19, 3143–3149. [Google Scholar] [CrossRef]
- El-Shazly, S.F.; Eid, M.A.; El-Sourogy, H.A.; Attia, G.F.; Ezzat, S.A. Evaluation of serum DNA integrity as a screening and prognostic tool in patients with hepatitis C virus-related hepatocellular carcinoma. Int. J. Biol. Markers 2010, 25, 79–86. [Google Scholar] [CrossRef] [PubMed]
- Huang, Z.; Hua, D.; Hu, Y.; Cheng, Z.; Zhou, X.; Xie, Q.; Wang, Q.; Wang, F.; Du, X.; Zeng, Y. Quantitation of plasma circulating DNA using quantitative PCR for the detection of hepatocellular carcinoma. Pathol. Oncol. Res. 2012, 18, 271–276. [Google Scholar] [CrossRef]
- Iizuka, N.; Sakaida, I.; Moribe, T.; Fujita, N.; Miura, T.; Stark, M.; Tamatsukuri, S.; Ishitsuka, H.; Uchida, K.; Terai, S.; et al. Elevated levels of circulating cell-free DNA in the blood of patients with hepatitis C virus-associated hepatocellular carcinoma. Anticancer Res. 2006, 26, 4713–4719. [Google Scholar]
- Marchio, A.; Amougou Atsama, M.; Bere, A.; Komas, N.P.; Noah Noah, D.; Atangana, P.J.A.; Camengo-Police, S.M.; Njouom, R.; Bekondi, C.; Pineau, P. Droplet digital PCR detects high rate of TP53 R249S mutants in cell-free DNA of middle African patients with hepatocellular carcinoma. Clin. Exp. Med. 2018, 18, 421–431. [Google Scholar] [CrossRef]
- Piciocchi, M.; Cardin, R.; Vitale, A.; Vanin, V.; Giacomin, A.; Pozzan, C.; Maddalo, G.; Cillo, U.; Guido, M.; Farinati, F. Circulating free DNA in the progression of liver damage to hepatocellular carcinoma. Hepatol. Int. 2013, 7, 1050–1057. [Google Scholar] [CrossRef]
- Ren, N.; Qin, L.X.; Tu, H.; Liu, Y.K.; Zhang, B.H.; Tang, Z.Y. The prognostic value of circulating plasma DNA level and its allelic imbalance on chromosome 8p in patients with hepatocellular carcinoma. J. Cancer Res. Clin. Oncol. 2006, 132, 399–407. [Google Scholar] [CrossRef] [PubMed]
- Yan, L.; Chen, Y.; Zhou, J.; Zhao, H.; Zhang, H.; Wang, G. Diagnostic value of circulating cell-free DNA levels for hepatocellular carcinoma. Int. J. Infect. Dis. 2018, 67, 92–97. [Google Scholar] [CrossRef] [Green Version]
- Igetei, R.; Otegbayo, J.A.; Ndububa, D.A.; Lesi, O.A.; Anumudu, C.I.; Hainaut, P.; Gormally, E. Detection of p53 codon 249 mutation in Nigerian patients with hepatocellular carcinoma using a novel evaluation of cell-free DNA. Ann. Hepatol. 2008, 7, 339–344. [Google Scholar] [CrossRef] [PubMed]
- Liao, W.; Yang, H.; Xu, H.; Wang, Y.; Ge, P.; Ren, J.; Xu, W.; Lu, X.; Sang, X.; Zhong, S.; et al. Noninvasive detection of tumor-associated mutations from circulating cell-free DNA in hepatocellular carcinoma patients by targeted deep sequencing. Oncotarget 2016, 7, 40481–40490. [Google Scholar] [CrossRef] [Green Version]
- Qu, C.; Wang, Y.; Wang, P.; Chen, K.; Wang, M.; Zeng, H.; Lu, J.; Song, Q.; Diplas, B.H.; Tan, D.; et al. Detection of early-stage hepatocellular carcinoma in asymptomatic HBsAg-seropositive individuals by liquid biopsy. Proc. Natl. Acad. Sci. USA 2019, 116, 6308–6312. [Google Scholar] [CrossRef] [Green Version]
- Xiong, Y.; Xie, C.R.; Zhang, S.; Chen, J.; Yin, Z.Y. Detection of a novel panel of somatic mutations in plasma cell-free DNA and its diagnostic value in hepatocellular carcinoma. Cancer Manag. Res. 2019, 11, 5745–5756. [Google Scholar] [CrossRef] [PubMed]
- Chu, H.J.; Heo, J.; Seo, S.B.; Kim, G.H.; Kang, D.H.; Song, G.A.; Cho, M.; Yang, U.S. Detection of aberrant p16INK4A methylation in sera of patients with liver cirrhosis and hepatocellular carcinoma. J. Korean Med. Sci. 2004, 19, 83–86. [Google Scholar] [CrossRef] [Green Version]
- Dou, C.Y.; Fan, Y.C.; Cao, C.J.; Yang, Y.; Wang, K. Sera DNA Methylation of CDH1, DNMT3b and ESR1 Promoters as Biomarker for the Early Diagnosis of Hepatitis B Virus-Related Hepatocellular Carcinoma. Dig. Dis. Sci. 2016, 61, 1130–1138. [Google Scholar] [CrossRef] [PubMed]
- Han, L.Y.; Fan, Y.C.; Mu, N.N.; Gao, S.; Li, F.; Ji, X.F.; Dou, C.Y.; Wang, K. Aberrant DNA methylation of G-protein-coupled bile acid receptor Gpbar1 (TGR5) is a potential biomarker for hepatitis B Virus associated hepatocellular carcinoma. Int. J. Med. Sci. 2014, 11, 164–171. [Google Scholar] [CrossRef] [PubMed]
- Hu, N.; Fan, X.P.; Fan, Y.C.; Chen, L.Y.; Qiao, C.Y.; Han, L.Y.; Wang, K. Hypomethylated Ubiquitin-Conjugating Enzyme2 Q1 (UBE2Q1) Gene Promoter in the Serum Is a Promising Biomarker for Hepatitis B Virus-Associated Hepatocellular Carcinoma. Tohoku. J. Exp. Med. 2017, 242, 93–100. [Google Scholar] [CrossRef] [Green Version]
- Huang, G.; Krocker, J.D.; Kirk, J.L.; Merwat, S.N.; Ju, H.; Soloway, R.D.; Wieck, L.R.; Li, A.; Okorodudu, A.O.; Petersen, J.R.; et al. Evaluation of INK4A promoter methylation using pyrosequencing and circulating cell-free DNA from patients with hepatocellular carcinoma. Clin. Chem. Lab. Med. 2014, 52, 899–909. [Google Scholar] [CrossRef] [Green Version]
- Iizuka, N.; Oka, M.; Sakaida, I.; Moribe, T.; Miura, T.; Kimura, N.; Tamatsukuri, S.; Ishitsuka, H.; Uchida, K.; Terai, S.; et al. Efficient detection of hepatocellular carcinoma by a hybrid blood test of epigenetic and classical protein markers. Clin. Chim. Acta 2011, 412, 152–158. [Google Scholar] [CrossRef]
- Ji, X.F.; Fan, Y.C.; Gao, S.; Yang, Y.; Zhang, J.J.; Wang, K. MT1M and MT1G promoter methylation as biomarkers for hepatocellular carcinoma. World J. Gastroenterol. 2014, 20, 4723–4729. [Google Scholar] [CrossRef]
- Kanekiyo, S.; Iizuka, N.; Tsunedomi, R.; Tokumitsu, Y.; Hashimoto, N.; Tokuhisa, Y.; Maeda, Y.; Iida, M.; Sakamoto, K.; Tamesa, T.; et al. Preoperative serum methylation signature as prognostic tool after curative hepatectomy in patients with hepatocellular carcinoma. Anticancer Res. 2015, 35, 997–1007. [Google Scholar]
- Kisiel, J.B.; Dukek, B.A.; Kanipakam, R.V.S.R.; Ghoz, H.M.; Yab, T.C.; Berger, C.K.; Taylor, W.R.; Foote, P.H.; Giama, N.H.; Onyirioha, K.; et al. Hepatocellular Carcinoma Detection by Plasma Methylated DNA: Discovery, Phase I Pilot, and Phase II Clinical Validation. Hepatology 2019, 69, 1180–1192. [Google Scholar] [CrossRef]
- Kuo, C.C.; Lin, C.Y.; Shih, Y.L.; Hsieh, C.B.; Lin, P.Y.; Guan, S.B.; Hsieh, M.S.; Lai, H.C.; Chen, C.J.; Lin, Y.W. Frequent methylation of HOXA9 gene in tumor tissues and plasma samples from human hepatocellular carcinomas. Clin. Chem. Lab. Med. 2014, 52, 1235–1245. [Google Scholar] [CrossRef] [PubMed]
- Li, J.; Chen, L.; Zhang, X.; Zhang, Y.; Liu, H.; Sun, B.; Zhao, L.; Ge, N.; Qian, H.; Yang, Y.; et al. Detection of circulating tumor cells in hepatocellular carcinoma using antibodies against asialoglycoprotein receptor, carbamoyl phosphate synthetase 1 and pan-cytokeratin. PLoS ONE 2014, 9, e96185. [Google Scholar] [CrossRef] [Green Version]
- Li, J.; Han, X.; Yu, X.; Xu, Z.; Yang, G.; Liu, B.; Xiu, P. Clinical applications of liquid biopsy as prognostic and predictive biomarkers in hepatocellular carcinoma: Circulating tumor cells and circulating tumor DNA. J. Exp. Clin. Cancer Res. 2018, 37, 213. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lu, C.Y.; Chen, S.Y.; Peng, H.L.; Kan, P.Y.; Chang, W.C.; Yen, C.J. Cell-free methylation markers with diagnostic and prognostic potential in hepatocellular carcinoma. Oncotarget 2017, 8, 6406–6418. [Google Scholar] [CrossRef] [Green Version]
- Oussalah, A.; Rischer, S.; Bensenane, M.; Conroy, G.; Filhine-Tresarrieu, P.; Debard, R.; Forest-Tramoy, D.; Josse, T.; Reinicke, D.; Garcia, M.; et al. Plasma mSEPT9: A Novel Circulating Cell-free DNA-Based Epigenetic Biomarker to Diagnose Hepatocellular Carcinoma. EBioMedicine 2018, 30, 138–147. [Google Scholar] [CrossRef] [PubMed]
- Sun, F.K.; Fan, Y.C.; Zhao, J.; Zhang, F.; Gao, S.; Zhao, Z.H.; Sun, Q.; Wang, K. Detection of TFPI2 methylation in the serum of hepatocellular carcinoma patients. Dig. Dis. Sci. 2013, 58, 1010–1015. [Google Scholar] [CrossRef]
- Tangkijvanich, P.; Hourpai, N.; Rattanatanyong, P.; Wisedopas, N.; Mahachai, V.; Mutirangura, A. Serum LINE-1 hypomethylation as a potential prognostic marker for hepatocellular carcinoma. Clin. Chim. Acta 2007, 379, 127–133. [Google Scholar] [CrossRef]
- Wang, J.; Qin, Y.; Li, B.; Sun, Z.; Yang, B. Detection of aberrant promoter methylation of GSTP1 in the tumor and serum of Chinese human primary hepatocellular carcinoma patients. Clin. Biochem. 2006, 39, 344–348. [Google Scholar] [CrossRef]
- Wei, L.; Huang, Y.; Zhao, R.; Zhang, J.; Liu, Q.; Liang, W.; Ding, X.; Gao, B.; Li, B.; Sun, C.; et al. Detection of promoter methylation status of suppressor of cytokine signaling 3 (SOCS3) in tissue and plasma from Chinese patients with different hepatic diseases. Clin. Exp. Med. 2018, 18, 79–87. [Google Scholar] [CrossRef]
- Wen, L.; Li, J.; Guo, H.; Liu, X.; Zheng, S.; Zhang, D.; Zhu, W.; Qu, J.; Guo, L.; Du, D.; et al. Genome-scale detection of hypermethylated CpG islands in circulating cell-free DNA of hepatocellular carcinoma patients. Cell Res. 2015, 25, 1250–1264. [Google Scholar] [CrossRef]
- Xu, R.H.; Wei, W.; Krawczyk, M.; Wang, W.; Luo, H.; Flagg, K.; Yi, S.; Shi, W.; Quan, Q.; Li, K.; et al. Circulating tumour DNA methylation markers for diagnosis and prognosis of hepatocellular carcinoma. Nat. Mater. 2017, 16, 1155–1161. [Google Scholar] [CrossRef] [PubMed]
- Yeo, W.; Wong, W.L.; Wong, N.; Law, B.K.; Tse, G.M.; Zhong, S. High frequency of promoter hypermethylation of RASSF1A in tumorous and non-tumourous tissue of breast cancer. Pathology 2005, 37, 125–130. [Google Scholar] [CrossRef] [PubMed]
- Fukushima, K. Neocognitron: A self organizing neural network model for a mechanism of pattern recognition unaffected by shift in position. Biol. Cybern. 1980, 36, 193–202. [Google Scholar] [CrossRef] [PubMed]
- Schmauch, B.; Romagnoni, A.; Pronier, E.; Saillard, C.; Maille, P.; Calderaro, J.; Kamoun, A.; Sefta, M.; Toldo, S.; Zaslavskiy, M.; et al. A deep learning model to predict RNA-Seq expression of tumours from whole slide images. Nat. Commun. 2020, 11, 3877. [Google Scholar] [CrossRef]






| 4th Edition (2010) | 5th Edition (2019) |
|---|---|
| cHCC-CCA, classical type | cHCC-CCA, classical type |
| cHCC-CCC with stemcell-features, classical type | Intermediate cell carcinoma |
| cHCC-CCA with stemcell-features, intermediate typecHCC-CCA with stemcell-features, cholangiolocellular type | Included in the cholangiocarcinoma classification |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Roßner, F.; Sinn, B.V.; Horst, D. Pathology of Combined Hepatocellular Carcinoma-Cholangiocarcinoma: An Update. Cancers 2023, 15, 494. https://doi.org/10.3390/cancers15020494
Roßner F, Sinn BV, Horst D. Pathology of Combined Hepatocellular Carcinoma-Cholangiocarcinoma: An Update. Cancers. 2023; 15(2):494. https://doi.org/10.3390/cancers15020494
Chicago/Turabian StyleRoßner, Florian, Bruno Valentin Sinn, and David Horst. 2023. "Pathology of Combined Hepatocellular Carcinoma-Cholangiocarcinoma: An Update" Cancers 15, no. 2: 494. https://doi.org/10.3390/cancers15020494