
The Diagnostic Approach towards Combined Hepatocellular-Cholangiocarcinoma—State of the Art and Future Perspectives
 , , and
, , and
Abstract
:Simple Summary
Abstract
1. Introduction
2. Clinical Presentation
3. Laboratory Features
4. Radiological Features
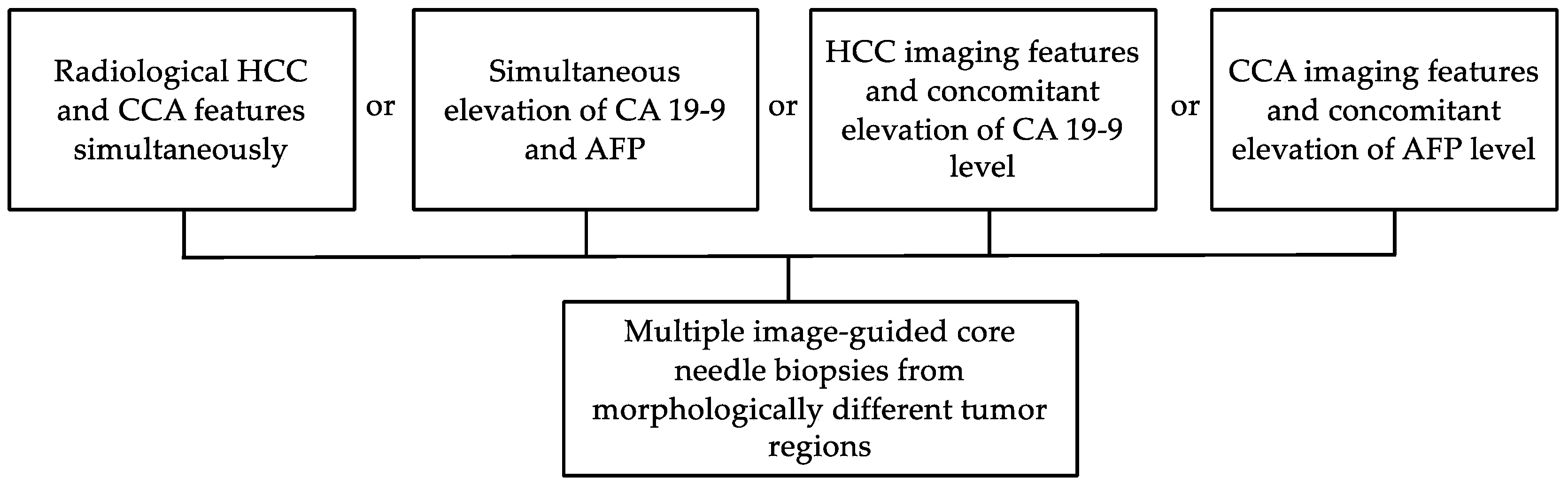
5. Role of Biopsy
6. Histopathological Assessment
7. Molecular Characteristics
8. Future Perspectives
8.1. Liquid Biopsies
8.2. Radiomics
8.3. Artificial Intelligence
9. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Brunt, E.; Aishima, S.; Clavien, P.A.; Fowler, K.; Goodman, Z.; Gores, G.; Gouw, A.; Kagen, A.; Klimstra, D.; Komuta, M.; et al. cHCC-CCA: Consensus terminology for primary liver carcinomas with both hepatocytic and cholangiocytic differentation. Hepatology 2018, 68, 113–126. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wakizaka, K.; Yokoo, H.; Kamiyama, T.; Ohira, M.; Kato, K.; Fujii, Y.; Sugiyama, K.; Okada, N.; Ohata, T.; Nagatsu, A.; et al. Clinical and pathological features of combined hepatocellular-cholangiocarcinoma compared with other liver cancers. J. Gastroenterol. Hepatol. 2019, 34, 1074–1080. [Google Scholar] [CrossRef] [PubMed]
- Spolverato, G.; Bagante, F.; Tsilimigras, D.; Ejaz, A.; Cloyd, J.; Pawlik, T.M. Management and outcomes among patients with mixed hepatocholangiocellular carcinoma: A population-based analysis. J. Surg. Oncol. 2019, 119, 278–287. [Google Scholar] [CrossRef]
- Koh, K.C.; Lee, H.; Choi, M.S.; Lee, J.H.; Paik, S.W.; Yoo, B.C.; Rhee, J.C.; Cho, J.W.; Park, C.K.; Kim, H.J. Clinicopathologic features and prognosis of combined hepatocellular cholangiocarcinoma. Am. J. Surg. 2005, 189, 120–125. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.H.; Chung, G.E.; Yu, S.J.; Hwang, S.Y.; Kim, J.S.; Kim, H.Y.; Yoon, J.H.; Lee, H.S.; Yi, N.J.; Suh, K.S.; et al. Long-term prognosis of combined hepatocellular and cholangiocarcinoma after curative resection comparison with hepatocellular carcinoma and cholangiocarcinoma. J. Clin. Gastroenterol. 2011, 45, 69–75. [Google Scholar] [CrossRef]
- Maximin, S.; Ganeshan, D.M.; Shanbhogue, A.K.; Dighe, M.K.; Yeh, M.M.; Kolokythas, O.; Bhargava, P.; Lalwani, N. Current update on combined hepatocellular-cholangiocarcinoma. Eur. J. Radiol. Open 2014, 1, 40–48. [Google Scholar] [CrossRef] [Green Version]
- Wells, H. Primary carcinoma of the liver. Am. J. Med. Sci. 1903, 126, 1827–1924. [Google Scholar] [CrossRef]
- Stavraka, C.; Rush, H.; Ross, P. Combined hepatocellular cholangiocarcinoma (cHCC-CC): An update of genetics, molecular biology, and therapeutic interventions. J. Hepatocell. Carcinoma. 2019, 6, 11–21. [Google Scholar] [CrossRef] [Green Version]
- Xue, R.; Chen, L.; Zhang, C.; Fujita, M.; Li, R.; Yan, S.M.; Ong, C.K.; Liao, X.; Gao, Q.; Sasagawa, S.; et al. Genomic and Transcriptomic Profiling of Combined Hepatocellular and Intrahepatic Cholangiocarcinoma Reveals Distinct Molecular Subtypes. Cancer Cell 2019, 35, 932–947.e8. [Google Scholar] [CrossRef]
- Schizas, D.; Mastoraki, A.; Routsi, E.; Papapanou, M.; Tsapralis, D.; Vassiliu, P.; Toutouzas, K.; Felekouras, E. Combined hepatocellular-cholangiocarcinoma: An update on epidemiology, classification, diagnosis and management. Hepatobiliary Pancreat. Dis. Int. 2020, 19, 515–523. [Google Scholar] [CrossRef]
- Gera, S.; Ettel, M.; Acosta-Gonzalez, G.; Xu, R. Clinical features, histology, and histogenesis of combined hepatocellular-cholangiocarcinoma. World J. Hepatol. 2017, 9, 300–309. [Google Scholar] [CrossRef] [PubMed]
- Wang, A.Q.; Zheng, Y.C.; Du, J.; Zhu, C.P.; Huang, H.C.; Wang, S.S.; Wu, L.C.; Wan, X.S.; Zhang, H.H.; Miao, R.Y.; et al. Combined hepatocellular cholangiocarcinoma: Controversies to be addressed. World J. Gastroenterol. 2016, 22, 4459–4465. [Google Scholar] [CrossRef] [PubMed]
- Connell, L.C.; Harding, J.J.; Shia, J.; Abou-Alfa, G.K. Combined intrahepatic cholangiocarcinoma and hepatocellular carcinoma. Chin. Clin. Oncol. 2016, 5, 66. [Google Scholar] [CrossRef] [PubMed]
- Kassahun, W.T.; Hauss, J. Management of combined hepatocellular and cholangiocarcinoma. Int. J. Clin Pr. 2008, 62, 1271–1278. [Google Scholar] [CrossRef]
- Chantajitr, S.; Wilasrusmee, C.; Lertsitichai, P.; Phromsopha, N. Combined hepatocellular and cholangiocarcinoma: Clinical features and prognostic study in a Thai population. J. Hepatobiliary Pancreat. Surg. 2006, 13, 537–542. [Google Scholar] [CrossRef] [PubMed]
- Zhou, Y.M.; Zhang, X.F.; Wu, L.P.; Sui, C.J.; Yang, J.M. Risk factors for combined hepatocellular-cholangiocarcinoma: A hospital-based case-control study. World J. Gastroenterol. 2014, 20, 12615–12620. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.D.; Park, S.-J.; Han, S.-S.; Kim, S.H.; Kim, Y.-K.; Lee, S.-A.; Ko, Y.H.; Hong, E.K. Clinicopathological features and prognosis of combined hepatocellular carcinoma and cholangiocarcinoma after surgery. Hepatobiliary Pancreat. Dis. Int. 2014, 13, 594–601. [Google Scholar] [CrossRef] [PubMed]
- Taguchi, J.; Nakashima, O.; Tanaka, M.; Hisaka, T.; Takazawa, T.; Kojiro, M. A clinicopathological study on combined hepatocellular and cholangiocarcinoma. J. Gastroenterol. Hepatol. 1996, 11, 758–764. [Google Scholar] [CrossRef] [PubMed]
- Ramai, D.; Ofosu, A.; Lai, J.K.; Reddy, M.; Adler, D.G. Combined Hepatocellular Cholangiocarcinoma: A Population-Based Retrospective Study. Am. J. Gastroenterol. 2019, 114, 1496–1501. [Google Scholar] [CrossRef]
- Garancini, M.; Goffredo, P.; Pagni, F.; Romano, F.; Roman, S.; Sosa, J.A.; Giardini, V. Combined hepatocellular-cholangiocarcinoma: A population-level analysis of an uncommon primary liver tumor. Liver Transpl. 2014, 20, 952–959. [Google Scholar] [CrossRef]
- Shetty, A.S.; Fowler, K.J.; Brunt, E.M.; Agarwal, S.; Narra, V.R.; Menias, C.O. Combined hepatocellular-cholangiocarcinoma: What the radiologist needs to know about biphenotypic liver carcinoma. Abdom. Imaging 2014, 39, 310–322. [Google Scholar] [CrossRef] [PubMed]
- Banales, J.M.; Inarrairaegui, M.; Arbelaiz, A.; Milkiewicz, P.; Muntane, J.; Munoz-Bellvis, L.; La Casta, A.; Gonzalez, L.M.; Arretxe, E.; Alonso, C.; et al. Serum Metabolites as Diagnostic Biomarkers for Cholangiocarcinoma, Hepatocellular Carcinoma, and Primary Sclerosing Cholangitis. Hepatology 2019, 70, 547–562. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Goodman, Z.D.; Ishak, K.G.; Langloss, J.M.; Sesterhenn, I.A.; Rabin, L. Combined hepatocellular-cholangiocarcinoma. A histologic and immunohistochemical study. Cancer 1985, 55, 124–135. [Google Scholar] [CrossRef] [PubMed]
- Li, R.; Yang, D.; Tang, C.L.; Cai, P.; Ma, K.S.; Ding, S.Y.; Zhang, X.H.; Guo, D.Y.; Yan, X.C. Combined hepatocellular carcinoma and cholangiocarcinoma (biphenotypic) tumors: Clinical characteristics, imaging features of contrast-enhanced ultrasound and computed tomography. BMC Cancer 2016, 16, 158. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yu, X.-H.; Xu, L.-B.; Zeng, H.; Zhang, R.; Wang, J.; Liu, C. Clinicopathological analysis of 14 patients with combined hepatocellular carcinoma and cholangiocarcinoma. Hepatobiliary Pancreat. Dis. Int. 2011, 10, 620–625. [Google Scholar] [CrossRef]
- Raevskaya, O.; Appelman, H.; Razumilava, N. A Contemporary Approach to Diagnosis and Treatment of Combined Hepatocellular-Cholangiocarcinoma. Curr. Hepatol. Rep. 2020, 19, 478–485. [Google Scholar] [CrossRef]
- Zhou, C.; Lu, X.; Wang, Y.; Qian, X.; Yang, C.; Zeng, M. Histopathological components correlated with MRI features and prognosis in combined hepatocellular carcinoma-cholangiocarcinoma. Eur. Radiol. 2022, 32, 6702–6711. [Google Scholar] [CrossRef] [PubMed]
- Park, S.H.; Lee, S.S.; Yu, E.; Kang, H.J.; Park, Y.; Kim, S.Y.; Lee, S.J.; Shin, Y.M.; Lee, M.G. Combined hepatocellular-cholangiocarcinoma: Gadoxetic acid-enhanced MRI findings correlated with pathologic features and prognosis. J. Magn. Reson. Imaging 2017, 46, 267–280. [Google Scholar] [CrossRef]
- Choi, S.H.; Jeon, S.K.; Lee, S.S.; Lee, J.M.; Hur, B.Y.; Kang, H.J.; Kim, H.; Park, Y. Radio-pathologic correlation of biphenotypic primary liver cancer (combined hepatocellular cholangiocarcinoma): Changes in the 2019 WHO classification and impact on LI-RADS classification at liver MRI. Eur. Radiol. 2021, 31, 9479–9488. [Google Scholar] [CrossRef]
- Yang, J.; Huang, J.Y.; Chen, X.; Ling, W.W.; Luo, Y.; Shi, Y.J.; Liu, J.B.; Lu, Q.; Lyshchik, A. Combined hepatocellular-cholangiocarcinoma: Can we use contrast-enhanced ultrasound Liver Imaging Reporting and Data System (LI-RADS) to predict the patient’s survival? Eur. Radiol. 2021, 31, 6397–6405. [Google Scholar] [CrossRef]
- Fowler, K.J.; Sheybani, A.; Parker, R.A., 3rd; Doherty, S.; E, M.B.; Chapman, W.C.; Menias, C.O. Combined hepatocellular and cholangiocarcinoma (biphenotypic) tumors: Imaging features and diagnostic accuracy of contrast-enhanced CT and MRI. AJR Am. J. Roentgenol. 2013, 201, 332–339. [Google Scholar] [CrossRef] [PubMed]
- Aoki, K.; Takayasu, K.; Kawano, T.; Muramatsu, Y.; Moriyama, N.; Wakao, F.; Yamamoto, J.; Shimada, K.; Takayama, T.; Kosuge, T.; et al. Combined hepatocellular carcinoma and cholangiocarcinoma: Clinical features and computed tomographic findings. Hepatology 1993, 18, 1090–1095. [Google Scholar] [CrossRef] [PubMed]
- Sanada, Y.; Shiozaki, S.; Aoki, H.; Takakura, N.; Yoshida, K.; Yamaguchi, Y. A clinical study of 11 cases of combined hepatocellular-cholangiocarcinoma Assessment of enhancement patterns on dynamics computed tomography before resection. Hepatol. Res. 2005, 32, 185–195. [Google Scholar] [CrossRef] [PubMed]
- Gigante, E.; Ronot, M.; Bertin, C.; Ciolina, M.; Bouattour, M.; Dondero, F.; Cauchy, F.; Soubrane, O.; Vilgrain, V.; Paradis, V. Combining imaging and tumour biopsy improves the diagnosis of combined hepatocellular-cholangiocarcinoma. Liver Int. 2019, 39, 2386–2396. [Google Scholar] [CrossRef] [PubMed]
- Chi, C.T.; Chau, G.Y.; Lee, R.C.; Chen, Y.Y.; Lei, H.J.; Hou, M.C.; Chao, Y.; Huang, Y.H. Radiological features and outcomes of combined hepatocellular-cholangiocarcinoma in patients undergoing surgical resection. J. Formos. Med Assoc. 2020, 119, 125–133. [Google Scholar] [CrossRef] [PubMed]
- Yang, J.; Zhang, Y.H.; Li, J.W.; Shi, Y.Y.; Huang, J.Y.; Luo, Y.; Liu, J.B.; Lu, Q. Contrast-enhanced ultrasound in association with serum biomarkers for differentiating combined hepatocellular-cholangiocarcinoma from hepatocellular carcinoma and intrahepatic cholangiocarcinoma. World J. Gastroenterol. 2020, 26, 7325–7337. [Google Scholar] [CrossRef]
- Chernyak, V.; Fowler, K.J.; Kamaya, A.; Kielar, A.Z.; Elsayes, K.M.; Bashir, M.R.; Kono, Y.; Do, R.K.; Mitchell, D.G.; Singal, A.G.; et al. Liver Imaging Reporting and Data System (LI-RADS) Version 2018: Imaging of Hepatocellular Carcinoma in At-Risk Patients. Radiology 2018, 289, 816–830. [Google Scholar] [CrossRef]
- Zou, X.; Luo, Y.; Morelli, J.N.; Hu, X.; Shen, Y.; Hu, D. Differentiation of hepatocellular carcinoma from intrahepatic cholangiocarcinoma and combined hepatocellular-cholangiocarcinoma in high-risk patients matched to MR field strength: Diagnostic performance of LI-RADS version 2018. Abdom. Radiol. 2021, 46, 3168–3178. [Google Scholar] [CrossRef]
- Liu, X.; Ni, X.; Li, Y.; Yang, C.; Wang, Y.; Ma, C.; Zhou, C.; Lu, X. Diagnostic Performance of LI-RADS Version 2018 for Primary Liver Cancer in Patients With Liver Cirrhosis on Enhanced MRI. Front. Oncol. 2022, 12, 934045. [Google Scholar] [CrossRef]
- Kim, M.Y.; Joo, I.; Kang, H.J.; Bae, J.S.; Jeon, S.K.; Lee, J.M. LI-RADS M (LR-M) criteria and reporting algorithm of v2018: Diagnostic values in the assessment of primary liver cancers on gadoxetic acid-enhanced MRI. Abdom. Radiol. 2020, 45, 2440–2448. [Google Scholar] [CrossRef]
- Sagrini, E.; Iavarone, M.; Stefanini, F.; Tovoli, F.; Vavassori, S.; Maggioni, M.; Renzulli, M.; Salvatore, V.; Stefanescu, H.; Colombo, M.; et al. Imaging of combined hepatocellular-cholangiocarcinoma in cirrhosis and risk of false diagnosis of hepatocellular carcinoma. United Eur. Gastroenterol. J. 2019, 7, 69–77. [Google Scholar] [CrossRef]
- Yoon, J.; Hwang, J.A.; Lee, S.; Lee, J.E.; Ha, S.Y.; Park, Y.N. Clinicopathologic and MRI features of combined hepatocellular-cholangiocarcinoma in patients with or without cirrhosis. Liver Int. 2021, 41, 1641–1651. [Google Scholar] [CrossRef] [PubMed]
- EASL Clinical Practice Guidelines: Management of hepatocellular carcinoma. J. Hepatol. 2018, 69, 182–236. [CrossRef] [PubMed] [Green Version]
- Abdelfattah, M.R.; Abaalkhail, F.; Al-Manea, H. Misdiagnosed or Incidentally Detected Hepatocellular Carcinoma in Explanted Livers: Lessons Learned. Ann. Transpl. 2015, 20, 366–372. [Google Scholar] [CrossRef] [PubMed]
- Potretzke, T.A.; Tan, B.R.; Doyle, M.B.; Brunt, E.M.; Heiken, J.P.; Fowler, K.J. Imaging Features of Biphenotypic Primary Liver Carcinoma (Hepatocholangiocarcinoma) and the Potential to Mimic Hepatocellular Carcinoma: LI-RADS Analysis of CT and MRI Features in 61 Cases. AJR Am. J. Roentgenol. 2016, 207, 25–31. [Google Scholar] [CrossRef] [PubMed]
- Nagtegaal, I.D.; Odze, R.D.; Klimstra, D.; Paradis, V.; Rugge, M.; Schirmacher, P.; Washington, K.M.; Carneiro, F.; Cree, I.A. The 2019 WHO classification of tumours of the digestive system. Histopathology 2020, 76, 182–188. [Google Scholar] [CrossRef] [Green Version]
- Kim, H.; Park, C.; Han, K.H.; Choi, J.; Kim, Y.B.; Kim, J.K.; Park, Y.N. Primary liver carcinoma of intermediate (hepatocyte-cholangiocyte) phenotype. J. Hepatol. 2004, 40, 298–304. [Google Scholar] [CrossRef]
- Sasaki, M.; Sato, H.; Kakuda, Y.; Sato, Y.; Choi, J.H.; Nakanuma, Y. Clinicopathological significance of ‘subtypes with stem-cell feature’ in combined hepatocellular-cholangiocarcinoma. Liver Int. 2015, 35, 1024–1035. [Google Scholar] [CrossRef]
- Moeini, A.; Sia, D.; Zhang, Z.; Camprecios, G.; Stueck, A.; Dong, H.; Montal, R.; Torrens, L.; Martinez-Quetglas, I.; Fiel, M.I.; et al. Mixed hepatocellular cholangiocarcinoma tumors: Cholangiolocellular carcinoma is a distinct molecular entity. J. Hepatol. 2017, 66, 952–961. [Google Scholar] [CrossRef] [Green Version]
- Balitzer, D.; Joseph, N.M.; Ferrell, L.; Shafizadeh, N.; Jain, D.; Zhang, X.; Yeh, M.; di Tommaso, L.; Kakar, S. Immunohistochemical and molecular features of cholangiolocellular carcinoma are similar to well-differentiated intrahepatic cholangiocarcinoma. Mod. Pathol. 2019, 32, 1486–1494. [Google Scholar] [CrossRef]
- Terada, T. Combined hepatocellular-cholangiocarcinoma with stem cell features, ductal plate malformation subtype: A case report and proposal of a new subtype. Int. J. Clin. Exp. Pathol. 2013, 6, 737–748. [Google Scholar] [PubMed]
- Akiba, J.; Nakashima, O.; Hattori, S.; Naito, Y.; Kusano, H.; Kondo, R.; Nakayama, M.; Tanikawa, K.; Todoroki, K.; Umeno, Y.; et al. The expression of arginase-1, keratin (K) 8 and K18 in combined hepatocellular-cholangiocarcinoma, subtypes with stem-cell features, intermediate-cell type. J. Clin. Pathol. 2016, 69, 846–851. [Google Scholar] [CrossRef] [PubMed]
- Maeda, T.; Adachi, E.; Kajiyama, K.; Sugimachi, K.; Tsuneyoshi, M. Combined hepatocellular and cholangiocarcinoma: Proposed criteria according to cytokeratin expression and analysis of clinicopathologic features. Hum. Pathol. 1995, 26, 956–964. [Google Scholar] [CrossRef] [PubMed]
- Zhao, Q.; Yu, W.L.; Lu, X.Y.; Dong, H.; Gu, Y.J.; Sheng, X.; Cong, W.M.; Wu, M.C. Combined hepatocellular and cholangiocarcinoma originating from the same clone: A pathomolecular evidence-based study. Chin. J. Cancer 2016, 35, 82. [Google Scholar] [CrossRef] [Green Version]
- Cazals-Hatem, D.; Rebouissou, S.; Bioulac-Sage, P.; Bluteau, O.; Blanche, H.; Franco, D.; Monges, G.; Belghiti, J.; Sa Cunha, A.; Laurent-Puig, P.; et al. Clinical and molecular analysis of combined hepatocellular-cholangiocarcinomas. J. Hepatol. 2004, 41, 292–298. [Google Scholar] [CrossRef]
- Joseph, N.M.; Tsokos, C.G.; Umetsu, S.E.; Shain, A.H.; Kelley, R.K.; Onodera, C.; Bowman, S.; Talevich, E.; Ferrell, L.D.; Kakar, S.; et al. Genomic profiling of combined hepatocellular-cholangiocarcinoma reveals similar genetics to hepatocellular carcinoma. J. Pathol. 2019, 248, 164–178. [Google Scholar] [CrossRef]
- Sasaki, M.; Sato, Y.; Nakanuma, Y. Mutational landscape of combined hepatocellular carcinoma and cholangiocarcinoma, and its clinicopathological significance. Histopathology 2017, 70, 423–434. [Google Scholar] [CrossRef]
- Borger, D.R.; Tanabe, K.K.; Fan, K.C.; Lopez, H.U.; Fantin, V.R.; Straley, K.S.; Schenkein, D.P.; Hezel, A.F.; Ancukiewicz, M.; Liebman, H.M.; et al. Frequent mutation of isocitrate dehydrogenase (IDH)1 and IDH2 in cholangiocarcinoma identified through broad-based tumor genotyping. Oncologist 2012, 17, 72–79. [Google Scholar] [CrossRef] [Green Version]
- Totoki, Y.; Tatsuno, K.; Covington, K.R.; Ueda, H.; Creighton, C.J.; Kato, M.; Tsuji, S.; Donehower, L.A.; Slagle, B.L.; Nakamura, H.; et al. Trans-ancestry mutational landscape of hepatocellular carcinoma genomes. Nat. Genet. 2014, 46, 1267–1273. [Google Scholar] [CrossRef]
- Cancer Genome Atlas Research Network. Comprehensive and Integrative Genomic Characterization of Hepatocellular Carcinoma. Cell 2017, 169, 1327–1341.e23. [Google Scholar] [CrossRef]
- Ignatiadis, M.; Sledge, G.W.; Jeffrey, S.S. Liquid biopsy enters the clinic-implementation issues and future challenges. Nat. Rev. Clin. Oncol. 2021, 18, 297–312. [Google Scholar] [CrossRef] [PubMed]
- Ye, Q.; Ling, S.; Zheng, S.; Xu, X. Liquid biopsy in hepatocellular carcinoma: Circulating tumor cells and circulating tumor DNA. Mol. Cancer 2019, 18, 114. [Google Scholar] [CrossRef] [PubMed]
- Guo, W.; Yang, X.R.; Sun, Y.F.; Shen, M.N.; Ma, X.L.; Wu, J.; Zhang, C.Y.; Zhou, Y.; Xu, Y.; Hu, B.; et al. Clinical significance of EpCAM mRNA-positive circulating tumor cells in hepatocellular carcinoma by an optimized negative enrichment and qRT-PCR-based platform. Clin. Cancer Res. 2014, 20, 4794–4805. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- An, Y.; Guan, Y.; Xu, Y.; Han, Y.; Wu, C.; Bao, C.; Zhou, B.; Wang, H.; Zhang, M.; Liu, W.; et al. The diagnostic and prognostic usage of circulating tumor DNA in operable hepatocellular carcinoma. Am. J. Transl. Res. 2019, 11, 6462–6474. [Google Scholar]
- Shen, N.; Zhang, D.; Yin, L.; Qiu, Y.; Liu, J.; Yu, W.; Fu, X.; Zhu, B.; Xu, X.; Duan, A.; et al. Bile cell-free DNA as a novel and powerful liquid biopsy for detecting somatic variants in biliary tract cancer. Oncol. Rep. 2019, 42, 549–560. [Google Scholar] [CrossRef]
- Mayerhoefer, M.E.; Materka, A.; Langs, G.; Häggström, I.; Szczypiński, P.; Gibbs, P.; Cook, G. Introduction to Radiomics. J. Nucl. Med. 2020, 61, 488–495. [Google Scholar] [CrossRef]
- Scapicchio, C.; Gabelloni, M.; Barucci, A.; Cioni, D.; Saba, L.; Neri, E. A deep look into radiomics. Radiol. Med. 2021, 126, 1296–1311. [Google Scholar] [CrossRef]
- Chu, L.C.; Park, S.; Kawamoto, S.; Yuille, A.L.; Hruban, R.H.; Fishman, E.K. Current Status of Radiomics and Deep Learning in Liver Imaging. J. Comput. Assist. Tomogr. 2021, 45, 343–351. [Google Scholar] [CrossRef]
- Yasaka, K.; Akai, H.; Abe, O.; Kiryu, S. Deep Learning with Convolutional Neural Network for Differentiation of Liver Masses at Dynamic Contrast-enhanced CT: A Preliminary Study. Radiology 2018, 286, 887–896. [Google Scholar] [CrossRef] [Green Version]
- Azer, S.A. Deep learning with convolutional neural networks for identification of liver masses and hepatocellular carcinoma: A systematic review. World J. Gastrointest. Oncol. 2019, 11, 1218–1230. [Google Scholar] [CrossRef]
- Bousabarah, K.; Letzen, B.; Tefera, J.; Savic, L.; Schobert, I.; Schlachter, T.; Staib, L.H.; Kocher, M.; Chapiro, J.; Lin, M. Automated detection and delineation of hepatocellular carcinoma on multiphasic contrast-enhanced MRI using deep learning. Abdom. Radiol. 2021, 46, 216–225. [Google Scholar] [CrossRef]
- Liu, X.; Khalvati, F.; Namdar, K.; Fischer, S.; Lewis, S.; Taouli, B.; Haider, M.A.; Jhaveri, K.S. Can machine learning radiomics provide pre-operative differentiation of combined hepatocellular cholangiocarcinoma from hepatocellular carcinoma and cholangiocarcinoma to inform optimal treatment planning? Eur. Radiol. 2021, 31, 244–255. [Google Scholar] [CrossRef] [PubMed]
- Le Berre, C.; Sandborn, W.J.; Aridhi, S.; Devignes, M.D.; Fournier, L.; Smail-Tabbone, M.; Danese, S.; Peyrin-Biroulet, L. Application of Artificial Intelligence to Gastroenterology and Hepatology. Gastroenterology 2020, 158, 76–94.e2. [Google Scholar] [CrossRef] [Green Version]
- Ruffle, J.K.; Farmer, A.D.; Aziz, Q. Artificial Intelligence-Assisted Gastroenterology- Promises and Pitfalls. Am. J. Gastroenterol. 2019, 114, 422–428. [Google Scholar] [CrossRef] [PubMed]
- LeCun, Y.; Bengio, Y.; Hinton, G. Deep learning. Nature 2015, 521, 436–444. [Google Scholar] [CrossRef] [PubMed]
- Calderaro, J.; Seraphin, T.P.; Luedde, T.; Simon, T.G. Artificial intelligence for the prevention and clinical management of hepatocellular carcinoma. J. Hepatol. 2022, 76, 1348–1361. [Google Scholar] [CrossRef] [PubMed]
- Haghbin, H.; Aziz, M. Artificial intelligence and cholangiocarcinoma: Updates and prospects. World J. Clin. Oncol. 2022, 13, 125–134. [Google Scholar] [CrossRef]
- Zhen, S.H.; Cheng, M.; Tao, Y.B.; Wang, Y.F.; Juengpanich, S.; Jiang, Z.Y.; Jiang, Y.K.; Yan, Y.Y.; Lu, W.; Lue, J.M.; et al. Deep Learning for Accurate Diagnosis of Liver Tumor Based on Magnetic Resonance Imaging and Clinical Data. Front. Oncol. 2020, 10, 680. [Google Scholar] [CrossRef]
- Bhinder, B.; Gilvary, C.; Madhukar, N.S.; Elemento, O. Artificial Intelligence in Cancer Research and Precision Medicine. Cancer Discov. 2021, 11, 900–915. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Combined Hepatocellular-Cholangiocarcinoma | Hepatocellular Carcinoma | Intrahepatic Cholangiocarcinoma |
|---|---|---|
| TP53 (45.3–80%) TERT promoter (23–70%) IDH1 or IDH2 (0–11.8%) AXIN1 (10%) CTNNB1 (6–10%) KMT2D (9%) KRAS (0–7.5%) FGFR2 (0–3%) BAP1 (0–3%) | TERT promoter (44–54%) TP53 (13–31%) CTNNB1 (6–31%) ALB (13–%) AXIN1 (6–8%) | IDH1 or IDH2 (9–30%) TP53 (5–22%) FGFR2 (6–20%) KRAS (5–19%) BAP1 (10–12%) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Eschrich, J.; Kobus, Z.; Geisel, D.; Halskov, S.; Roßner, F.; Roderburg, C.; Mohr, R.; Tacke, F. The Diagnostic Approach towards Combined Hepatocellular-Cholangiocarcinoma—State of the Art and Future Perspectives. Cancers 2023, 15, 301. https://doi.org/10.3390/cancers15010301
Eschrich J, Kobus Z, Geisel D, Halskov S, Roßner F, Roderburg C, Mohr R, Tacke F. The Diagnostic Approach towards Combined Hepatocellular-Cholangiocarcinoma—State of the Art and Future Perspectives. Cancers. 2023; 15(1):301. https://doi.org/10.3390/cancers15010301
Chicago/Turabian StyleEschrich, Johannes, Zuzanna Kobus, Dominik Geisel, Sebastian Halskov, Florian Roßner, Christoph Roderburg, Raphael Mohr, and Frank Tacke. 2023. "The Diagnostic Approach towards Combined Hepatocellular-Cholangiocarcinoma—State of the Art and Future Perspectives" Cancers 15, no. 1: 301. https://doi.org/10.3390/cancers15010301