
Mixed Hepatocellular Cholangiocarcinoma: A Comparison of Survival between Mixed Tumors, Intrahepatic Cholangiocarcinoma and Hepatocellular Carcinoma from a Single Center
 , , , , , and
, , , , , and
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
3. Results
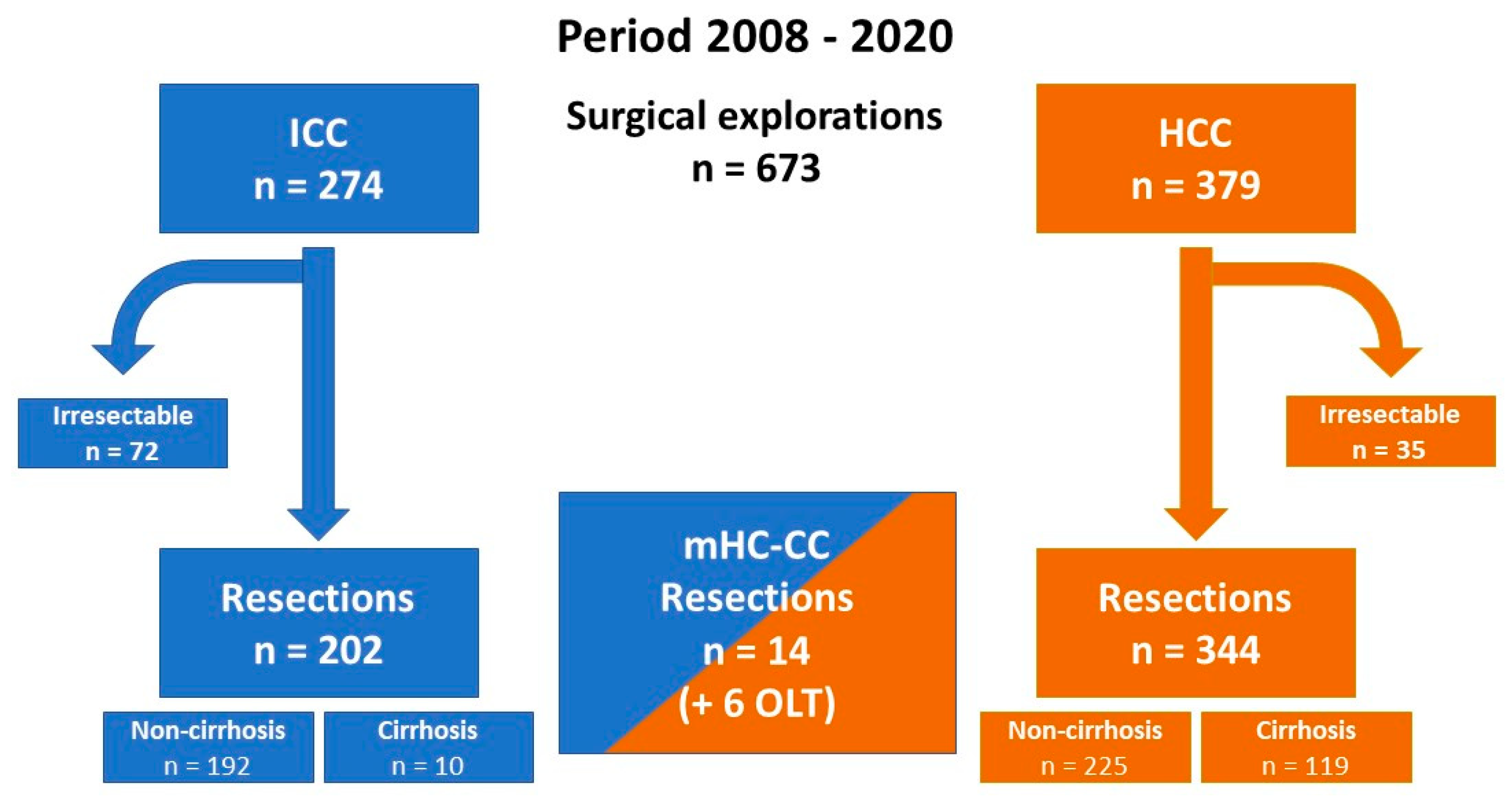
3.1. Surgical Procedures and Intraoperative Data
3.2. Vascular and Visceral Extensions
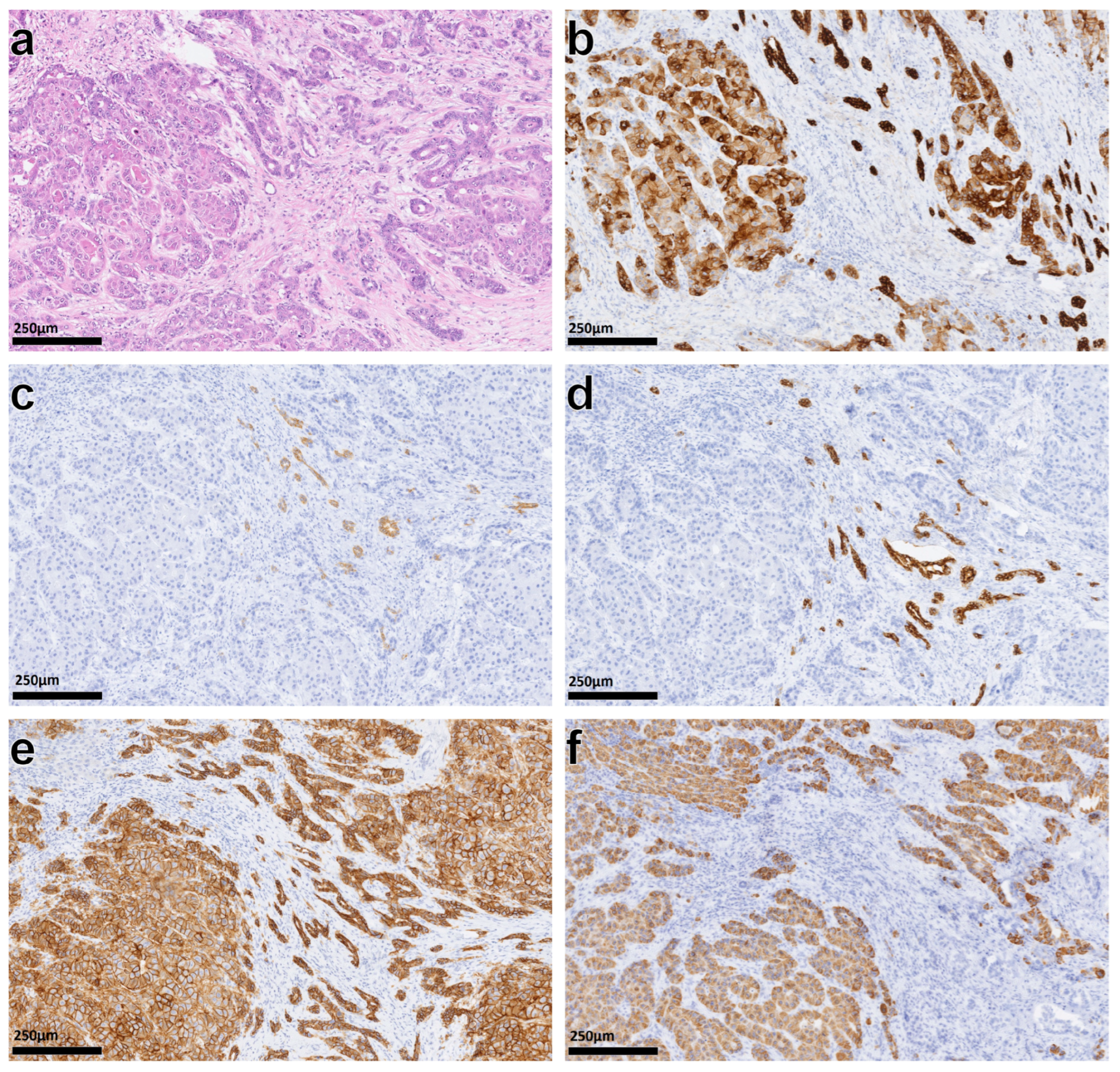
3.3. Histopathological Examination
3.4. Tumor Recurrence
3.5. Comparison of Survival
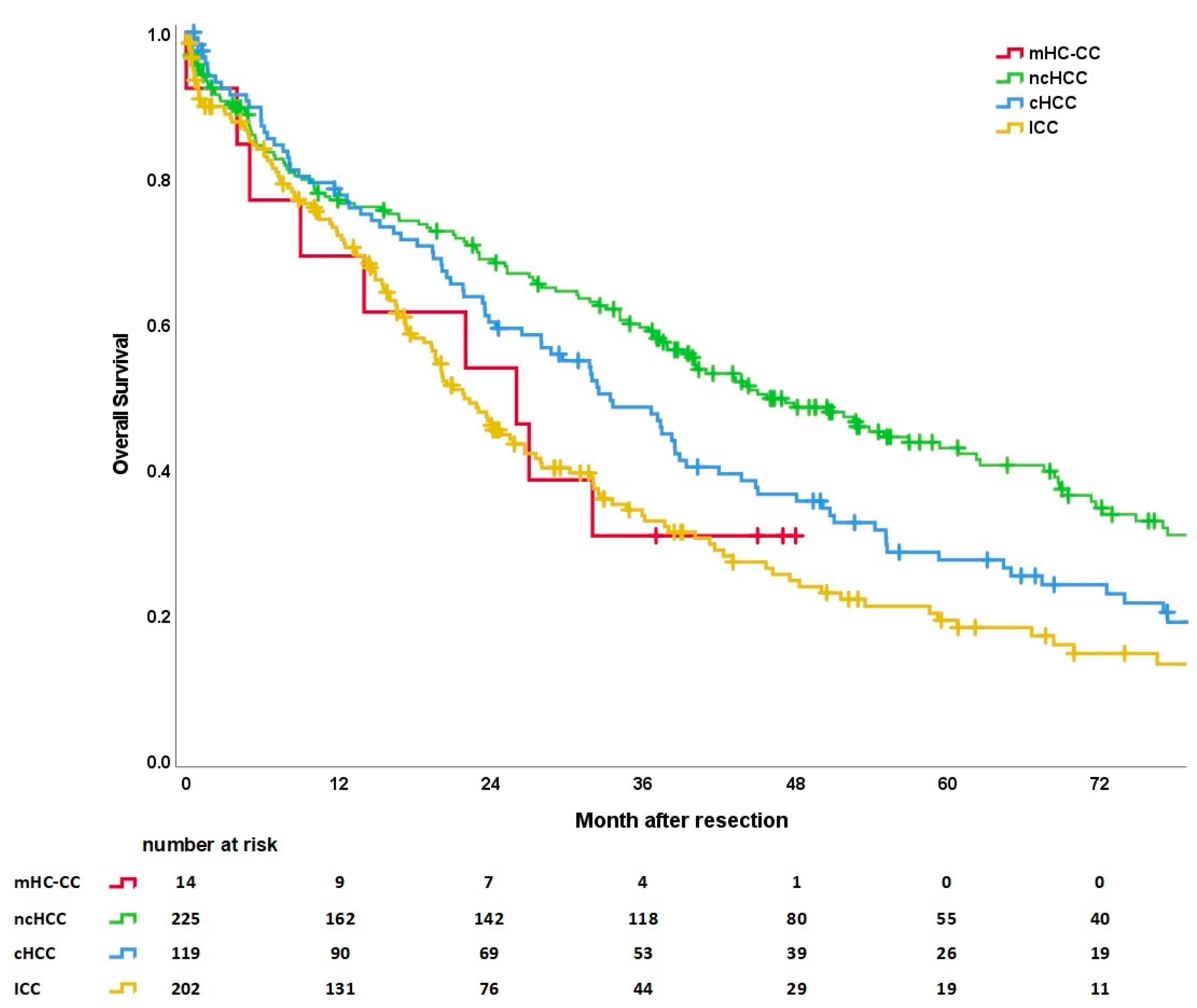
3.5.1. Overall Survival
3.5.2. mHC-CC Survival Resection vs. Transplant
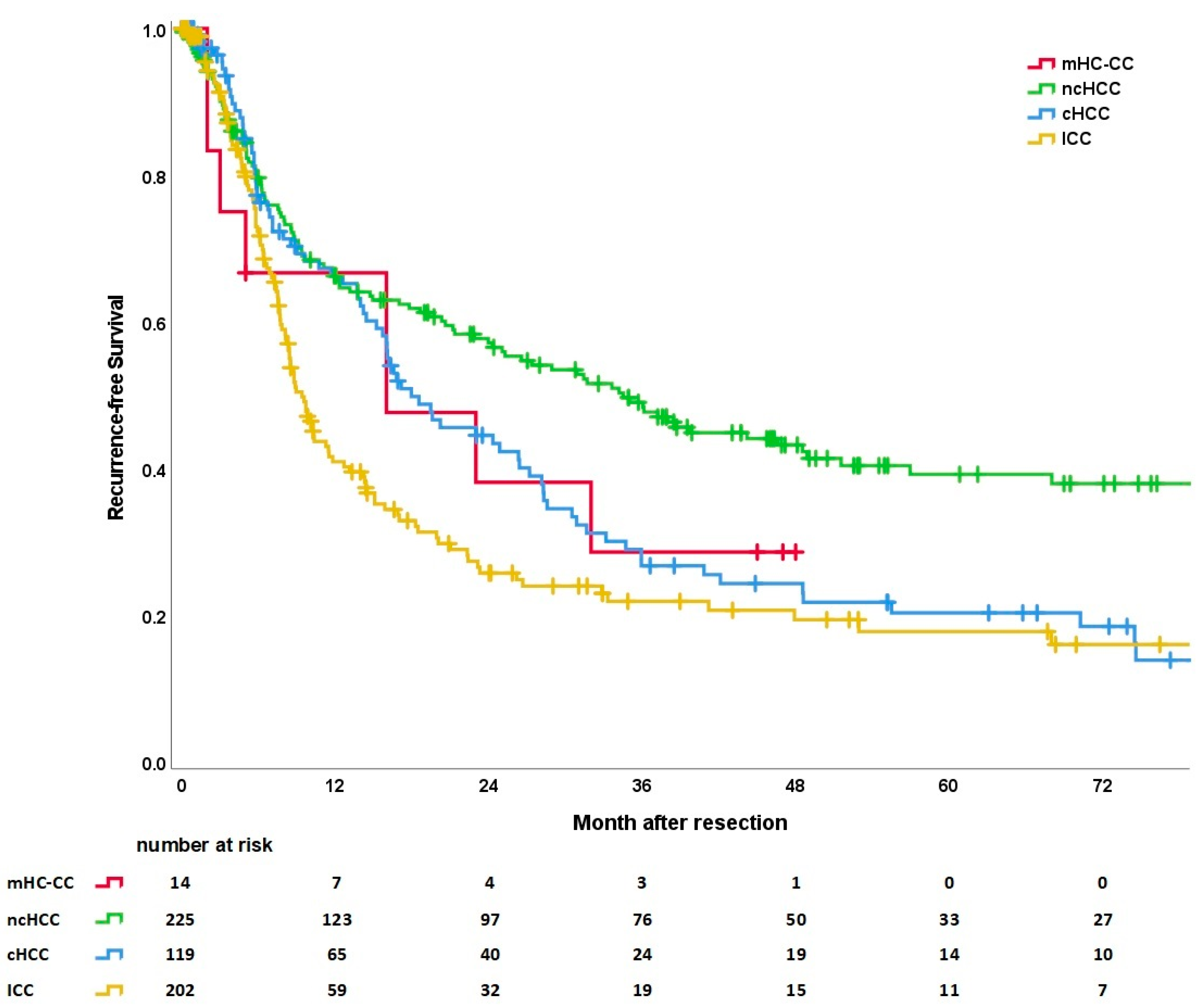
3.5.3. Recurrence-Free Survival
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Altekruse, S.F.; Devesa, S.S.; Dickie, L.A.; McGlynn, K.A.; Kleiner, D.E. Histological classification of liver and intrahepatic bile duct cancers in SEER registries. J. Regist. Manag. 2011, 38, 201–205. [Google Scholar]
- Jarnagin, W.R.; Weber, S.; Tickoo, S.K.; Koea, J.B.; Obiekwe, S.; Fong, Y.; DeMatteo, R.P.; Blumgart, L.H.; Klimstra, D. Combined hepatocellular and cholangiocarcinoma: Demographic, clinical, and prognostic factors. Cancer 2002, 94, 2040–2046. [Google Scholar] [CrossRef] [PubMed]
- Massarweh, N.N.; El-Serag, H.B. Epidemiology of Hepatocellular Carcinoma and Intrahepatic Cholangiocarcinoma. Cancer Control 2017, 24, 1073274817729245. [Google Scholar] [CrossRef] [PubMed]
- Xue, R.; Chen, L.; Zhang, C.; Fujita, M.; Li, R.; Yan, S.M.; Ong, C.K.; Liao, X.; Gao, Q.; Sasagawa, S.; et al. Genomic and Transcriptomic Profiling of Combined Hepatocellular and Intrahepatic Cholangiocarcinoma Reveals Distinct Molecular Subtypes. Cancer Cell 2019, 35, 932–947.e938. [Google Scholar] [CrossRef]
- Nagtegaal, I.D.; Odze, R.D.; Klimstra, D.; Paradis, V.; Rugge, M.; Schirmacher, P.; Washington, K.M.; Carneiro, F.; Cree, I.A.; Board, W.H.O.C.o.T.E. The 2019 WHO classification of tumours of the digestive system. Histopathology 2020, 76, 182–188. [Google Scholar] [CrossRef] [Green Version]
- Oldhafer, F.; Vondran, F.W.R.; Mittler, J.; Lang, H. Aktueller Stand der operativen Therapie des hepatozellulären Karzinoms. Onkologe 2022, 28, 278–286. [Google Scholar] [CrossRef]
- Lang, H.; Baumgart, J.; Heinrich, S.; Huber, T.; Heuft, L.K.; Margies, R.; Mittler, J.; Hahn, F.; Gerber, T.S.; Foerster, F.; et al. Liver Resection for Intrahepatic Cholangiocarcinoma-Single-Center Experience with 286 Patients Undergoing Surgical Exploration over a Thirteen Year Period. J. Clin. Med. 2021, 10, 3559. [Google Scholar] [CrossRef]
- Ejaz, A.; Cloyd, J.M.; Pawlik, T.M. Advances in the Diagnosis and Treatment of Patients with Intrahepatic Cholangiocarcinoma. Ann. Surg. Oncol. 2020, 27, 552–560. [Google Scholar] [CrossRef]
- Belghiti, J.; Kianmanesh, R. Surgical treatment of hepatocellular carcinoma. HPB 2005, 7, 42–49. [Google Scholar] [CrossRef] [Green Version]
- Bridgewater, J.; Galle, P.R.; Khan, S.A.; Llovet, J.M.; Park, J.W.; Patel, T.; Pawlik, T.M.; Gores, G.J. Guidelines for the diagnosis and management of intrahepatic cholangiocarcinoma. J. Hepatol. 2014, 60, 1268–1289. [Google Scholar] [CrossRef] [Green Version]
- Weber, S.M.; Ribero, D.; O’Reilly, E.M.; Kokudo, N.; Miyazaki, M.; Pawlik, T.M. Intrahepatic cholangiocarcinoma: Expert consensus statement. HPB 2015, 17, 669–680. [Google Scholar] [CrossRef] [PubMed]
- European Association for the Study of the Liver. Electronic address, e.e.e.; European Association for the Study of the, L. EASL Clinical Practice Guidelines: Management of hepatocellular carcinoma. J. Hepatol. 2018, 69, 182–236. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Leitlinienprogramm Onkologie (Deutsche Krebsgesellschaft, Deutsche Krebshilfe, AWMF): Diagnostik und Therapie des Hepatozellulären Karzinoms und biliärer Karzinome Langversion 3.0, 2022, AWMF-Registernummer: 032/053OL. Available online: https://www.leitlinienprogramm-onkologie.de/leitlinien/hcc-und-biliaere-karzinome/ (accessed on 3 December 2022).
- Klintmalm, G.B. Liver transplantation for hepatocellular carcinoma: A registry report of the impact of tumor characteristics on outcome. Ann. Surg. 1998, 228, 479–490. [Google Scholar] [CrossRef] [PubMed]
- Llovet, J.M.; Bru, C.; Bruix, J. Prognosis of hepatocellular carcinoma: The BCLC staging classification. Semin. Liver Dis. 1999, 19, 329–338. [Google Scholar] [CrossRef]
- Leoni, S.; Sansone, V.; Lorenzo, S.; Ielasi, L.; Tovoli, F.; Renzulli, M.; Golfieri, R.; Spinelli, D.; Piscaglia, F. Treatment of Combined Hepatocellular and Cholangiocarcinoma. Cancers 2020, 12, 794. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gupta, R.; Togashi, J.; Akamatsu, N.; Sakamoto, Y.; Kokudo, N. Impact of incidental/misdiagnosed intrahepatic cholangiocarcinoma and combined hepatocellular cholangiocarcinoma on the outcomes of liver transplantation: An institutional case series and literature review. Surg. Today 2017, 47, 908–917. [Google Scholar] [CrossRef] [PubMed]
- Bartsch, F.; Baumgart, J.; Hoppe-Lotichius, M.; Schmidtmann, I.; Heinrich, S.; Lang, H. Visceral infiltration of intrahepatic cholangiocarcinoma is most prognostic after curative resection-Retrospective cohort study of 102 consecutive liver resections from a single center. Int. J. Surg. 2018, 55, 193–200. [Google Scholar] [CrossRef] [PubMed]
- Buettner, S.; Koerkamp, B.G.; Ejaz, A.; Buisman, F.E.; Kim, Y.; Margonis, G.A.; Alexandrescu, S.; Marques, H.P.; Lamelas, J.; Aldrighetti, L.; et al. The effect of preoperative chemotherapy treatment in surgically treated intrahepatic cholangiocarcinoma patients-A multi-institutional analysis. J. Surg. Oncol. 2017, 115, 312–318. [Google Scholar] [CrossRef]
- de Jong, M.C.; Nathan, H.; Sotiropoulos, G.C.; Paul, A.; Alexandrescu, S.; Marques, H.; Pulitano, C.; Barroso, E.; Clary, B.M.; Aldrighetti, L.; et al. Intrahepatic cholangiocarcinoma: An international multi-institutional analysis of prognostic factors and lymph node assessment. J. Clin. Oncol. 2011, 29, 3140–3145. [Google Scholar] [CrossRef] [Green Version]
- Conci, S.; Ruzzenente, A.; Vigano, L.; Ercolani, G.; Fontana, A.; Bagante, F.; Bertuzzo, F.; Dore, A.; Pinna, A.D.; Torzilli, G.; et al. Patterns of Distribution of Hepatic Nodules (Single, Satellites or Multifocal) in Intrahepatic Cholangiocarcinoma: Prognostic Impact After Surgery. Ann. Surg. Oncol. 2018, 25, 3719–3727. [Google Scholar] [CrossRef]
- Penzkofer, L.; Mittler, J.; Heinrich, S.; Wachter, N.; Straub, B.K.; Kloeckner, R.; Stoehr, F.; Gairing, S.J.; Bartsch, F.; Lang, H. Outcome after Resection for Hepatocellular Carcinoma in Noncirrhotic Liver-A Single Centre Study. J. Clin. Med. 2022, 11, 5802. [Google Scholar] [CrossRef] [PubMed]
- Xie, Q.S.; Chen, Z.X.; Zhao, Y.J.; Gu, H.; Geng, X.P.; Liu, F.B. Systematic review of outcomes and meta-analysis of risk factors for prognosis after liver resection for hepatocellular carcinoma without cirrhosis. Asian J. Surg. 2021, 44, 36–45. [Google Scholar] [CrossRef]
- Proneth, A.; Zeman, F.; Schlitt, H.J.; Schnitzbauer, A.A. Is resection or transplantation the ideal treatment in patients with hepatocellular carcinoma in cirrhosis if both are possible? A systematic review and metaanalysis. Ann. Surg. Oncol. 2014, 21, 3096–3107. [Google Scholar] [CrossRef] [PubMed]
- Wu, C.C.; Cheng, S.B.; Ho, W.M.; Chen, J.T.; Liu, T.J.; P’Eng, F.K. Liver resection for hepatocellular carcinoma in patients with cirrhosis. Br. J. Surg. 2005, 92, 348–355. [Google Scholar] [CrossRef] [PubMed]
- Groeschl, R.T.; Turaga, K.K.; Gamblin, T.C. Transplantation versus resection for patients with combined hepatocellular carcinoma-cholangiocarcinoma. J. Surg. Oncol. 2013, 107, 608–612. [Google Scholar] [CrossRef] [PubMed]
- Jung, D.H.; Hwang, S.; Song, G.W.; Ahn, C.S.; Moon, D.B.; Kim, K.H.; Ha, T.Y.; Park, G.C.; Hong, S.M.; Kim, W.J.; et al. Longterm prognosis of combined hepatocellular carcinoma-cholangiocarcinoma following liver transplantation and resection. Liver Transplant. 2017, 23, 330–341. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gentile, D.; Donadon, M.; Lleo, A.; Aghemo, A.; Roncalli, M.; di Tommaso, L.; Torzilli, G. Surgical Treatment of Hepatocholangiocarcinoma: A Systematic Review. Liver Cancer 2020, 9, 15–27. [Google Scholar] [CrossRef]
- Gentile, D.; Donadon, M.; Di Tommaso, L.; Sama, L.; Franchi, E.; Costa, G.; Lleo, A.; Torzilli, G. Is the outcome after hepatectomy for transitional hepatocholangiocarcinoma different from that of hepatocellular carcinoma and mass-forming cholangiocarcinoma? A case-matched analysis. Updates Surg. 2020, 72, 671–679. [Google Scholar] [CrossRef]
- Nagino, M.; DeMatteo, R.; Lang, H.; Cherqui, D.; Malago, M.; Kawakatsu, S.; DeOliveira, M.L.; Adam, R.; Aldrighetti, L.; Boudjema, K.; et al. Proposal of a New Comprehensive Notation for Hepatectomy: The "New World" Terminology. Ann. Surg. 2021, 274, 1–3. [Google Scholar] [CrossRef]
- Mazzaferro, V.; Regalia, E.; Doci, R.; Andreola, S.; Pulvirenti, A.; Bozzetti, F.; Montalto, F.; Ammatuna, M.; Morabito, A.; Gennari, L. Liver transplantation for the treatment of small hepatocellular carcinomas in patients with cirrhosis. N. Engl. J. Med. 1996, 334, 693–699. [Google Scholar] [CrossRef]
- Dindo, D.; Demartines, N.; Clavien, P.A. Classification of surgical complications: A new proposal with evaluation in a cohort of 6336 patients and results of a survey. Ann. Surg. 2004, 240, 205–213. [Google Scholar] [CrossRef] [PubMed]
- Brierley, J.; Gospodarowicz, M.; Wittekind, C. International Union against Cancer. In TNM Classification of Malignant Tumours, 8th ed.; Wiley Blackwell: Oxford, UK, 2017. [Google Scholar]
- Punt, C.J.; Buyse, M.; Kohne, C.H.; Hohenberger, P.; Labianca, R.; Schmoll, H.J.; Pahlman, L.; Sobrero, A.; Douillard, J.Y. Endpoints in adjuvant treatment trials: A systematic review of the literature in colon cancer and proposed definitions for future trials. J. Natl. Cancer Inst. 2007, 99, 998–1003. [Google Scholar] [CrossRef] [PubMed]
- Kim, K.H.; Lee, S.G.; Park, E.H.; Hwang, S.; Ahn, C.S.; Moon, D.B.; Ha, T.Y.; Song, G.W.; Jung, D.H.; Kim, K.M.; et al. Surgical treatments and prognoses of patients with combined hepatocellular carcinoma and cholangiocarcinoma. Ann. Surg. Oncol. 2009, 16, 623–629. [Google Scholar] [CrossRef] [PubMed]
- Lang, H.; Sotiropoulos, G.C.; Fruhauf, N.R.; Domland, M.; Paul, A.; Kind, E.M.; Malago, M.; Broelsch, C.E. Extended hepatectomy for intrahepatic cholangiocellular carcinoma (ICC): When is it worthwhile? Single center experience with 27 resections in 50 patients over a 5-year period. Ann. Surg. 2005, 241, 134–143. [Google Scholar] [CrossRef] [PubMed]
- Glantzounis, G.K.; Paliouras, A.; Stylianidi, M.C.; Milionis, H.; Tzimas, P.; Roukos, D.; Pentheroudakis, G.; Felekouras, E. The role of liver resection in the management of intermediate and advanced stage hepatocellular carcinoma. A systematic review. Eur. J. Surg. Oncol. 2018, 44, 195–208. [Google Scholar] [CrossRef] [PubMed]
- Torzilli, G.; Belghiti, J.; Kokudo, N.; Takayama, T.; Capussotti, L.; Nuzzo, G.; Vauthey, J.N.; Choti, M.A.; De Santibanes, E.; Donadon, M.; et al. A snapshot of the effective indications and results of surgery for hepatocellular carcinoma in tertiary referral centers: Is it adherent to the EASL/AASLD recommendations?: An observational study of the HCC East-West study group. Ann. Surg. 2013, 257, 929–937. [Google Scholar] [CrossRef]
- Zhong, J.H.; Ke, Y.; Gong, W.F.; Xiang, B.D.; Ma, L.; Ye, X.P.; Peng, T.; Xie, G.S.; Li, L.Q. Hepatic resection associated with good survival for selected patients with intermediate and advanced-stage hepatocellular carcinoma. Ann. Surg. 2014, 260, 329–340. [Google Scholar] [CrossRef]
- Conci, S.; Vigano, L.; Ercolani, G.; Gonzalez, E.; Ruzzenente, A.; Isa, G.; Salaris, C.; Fontana, A.; Bagante, F.; Pedrazzani, C.; et al. Outcomes of vascular resection associated with curative intent hepatectomy for intrahepatic cholangiocarcinoma. Eur. J. Surg. Oncol. 2020, 46, 1727–1733. [Google Scholar] [CrossRef] [PubMed]
- Ali, S.M.; Clark, C.J.; Zaydfudim, V.M.; Que, F.G.; Nagorney, D.M. Role of major vascular resection in patients with intrahepatic cholangiocarcinoma. Ann. Surg. Oncol. 2013, 20, 2023–2028. [Google Scholar] [CrossRef] [PubMed]
- Young, A.L.; Adair, R.; Prasad, K.R.; Toogood, G.J.; Lodge, J.P. Hepatocellular carcinoma within a noncirrhotic, nonfibrotic, seronegative liver: Surgical approaches and outcomes. J. Am. Coll. Surg. 2012, 214, 174–183. [Google Scholar] [CrossRef]
- Taura, K.; Ikai, I.; Hatano, E.; Yasuchika, K.; Nakajima, A.; Tada, M.; Seo, S.; Machimoto, T.; Uemoto, S. Influence of coexisting cirrhosis on outcomes after partial hepatic resection for hepatocellular carcinoma fulfilling the Milan criteria: An analysis of 293 patients. Surgery 2007, 142, 685–694. [Google Scholar] [CrossRef]
- Lang, H.; Sotiropoulos, G.C.; Sgourakis, G.; Schmitz, K.J.; Paul, A.; Hilgard, P.; Zopf, T.; Trarbach, T.; Malago, M.; Baba, H.A.; et al. Operations for intrahepatic cholangiocarcinoma: Single-institution experience of 158 patients. J. Am. Coll. Surg. 2009, 208, 218–228. [Google Scholar] [CrossRef] [PubMed]
- Farges, O.; Fuks, D.; Boleslawski, E.; Le Treut, Y.P.; Castaing, D.; Laurent, A.; Ducerf, C.; Rivoire, M.; Bachellier, P.; Chiche, L.; et al. Influence of surgical margins on outcome in patients with intrahepatic cholangiocarcinoma: A multicenter study by the AFC-IHCC-2009 study group. Ann. Surg. 2011, 254, 824–829, discussion 830. [Google Scholar] [CrossRef] [PubMed]
- Song, S.; Moon, H.H.; Lee, S.; Kim, T.S.; Shin, M.; Kim, J.M.; Park, J.B.; Kwon, C.H.; Kim, S.J.; Lee, S.K.; et al. Comparison between resection and transplantation in combined hepatocellular and cholangiocarcinoma. Transplant. Proc. 2013, 45, 3041–3046. [Google Scholar] [CrossRef]
- Yin, X.; Zhang, B.H.; Qiu, S.J.; Ren, Z.G.; Zhou, J.; Chen, X.H.; Zhou, Y.; Fan, J. Combined hepatocellular carcinoma and cholangiocarcinoma: Clinical features, treatment modalities, and prognosis. Ann. Surg. Oncol. 2012, 19, 2869–2876. [Google Scholar] [CrossRef]
- Beaufrere, A.; Calderaro, J.; Paradis, V. Combined hepatocellular-cholangiocarcinoma: An update. J. Hepatol. 2021, 74, 1212–1224. [Google Scholar] [CrossRef] [PubMed]
- Zhang, X.F.; Beal, E.W.; Bagante, F.; Chakedis, J.; Weiss, M.; Popescu, I.; Marques, H.P.; Aldrighetti, L.; Maithel, S.K.; Pulitano, C.; et al. Early versus late recurrence of intrahepatic cholangiocarcinoma after resection with curative intent. Br. J. Surg. 2018, 105, 848–856. [Google Scholar] [CrossRef]
- Hu, L.S.; Zhang, X.F.; Weiss, M.; Popescu, I.; Marques, H.P.; Aldrighetti, L.; Maithel, S.K.; Pulitano, C.; Bauer, T.W.; Shen, F.; et al. Recurrence Patterns and Timing Courses Following Curative-Intent Resection for Intrahepatic Cholangiocarcinoma. Ann. Surg. Oncol. 2019, 26, 2549–2557. [Google Scholar] [CrossRef]
- Yoh, T.; Hatano, E.; Seo, S.; Okuda, Y.; Fuji, H.; Ikeno, Y.; Taura, K.; Yasuchika, K.; Okajima, H.; Kaido, T.; et al. Long-Term Survival of Recurrent Intrahepatic Cholangiocarcinoma: The Impact and Selection of Repeat Surgery. World J. Surg. 2018, 42, 1848–1856. [Google Scholar] [CrossRef]
- Weber, S.M.; Jarnagin, W.R.; Klimstra, D.; DeMatteo, R.P.; Fong, Y.; Blumgart, L.H. Intrahepatic cholangiocarcinoma: Resectability, recurrence pattern, and outcomes. J. Am. Coll. Surg. 2001, 193, 384–391. [Google Scholar] [CrossRef]
- Bartsch, F.; Paschold, M.; Baumgart, J.; Hoppe-Lotichius, M.; Heinrich, S.; Lang, H. Surgical Resection for Recurrent Intrahepatic Cholangiocarcinoma. World J. Surg. 2019, 43, 1105–1116. [Google Scholar] [CrossRef] [PubMed]
- Bartsch, F.; Eberhard, J.; Ruckert, F.; Schmelzle, M.; Lehwald-Tywuschik, N.; Fichtner-Feigl, S.; Gaedcke, J.; Oldhafer, K.J.; Oldhafer, F.; Diener, M.; et al. Repeated resection for recurrent intrahepatic cholangiocarcinoma: A retrospective German multicentre study. Liver Int. 2021, 41, 180–191. [Google Scholar] [CrossRef] [PubMed]
- Zhang, S.J.; Hu, P.; Wang, N.; Shen, Q.; Sun, A.X.; Kuang, M.; Qian, G.J. Thermal ablation versus repeated hepatic resection for recurrent intrahepatic cholangiocarcinoma. Ann. Surg. Oncol. 2013, 20, 3596–3602. [Google Scholar] [CrossRef] [PubMed]
- Kamphues, C.; Seehofer, D.; Eisele, R.M.; Denecke, T.; Pratschke, J.; Neumann, U.P.; Neuhaus, P. Recurrent intrahepatic cholangiocarcinoma: Single-center experience using repeated hepatectomy and radiofrequency ablation. J. Hepatobiliary Pancreat Sci. 2010, 17, 509–515. [Google Scholar] [CrossRef]
- Benavides, M.; Anton, A.; Gallego, J.; Gomez, M.A.; Jimenez-Gordo, A.; La Casta, A.; Laquente, B.; Macarulla, T.; Rodriguez-Mowbray, J.R.; Maurel, J. Biliary tract cancers: SEOM clinical guidelines. Clin. Transl. Oncol. 2015, 17, 982–987. [Google Scholar] [CrossRef] [Green Version]
- Alvaro, D.; Cannizzaro, R.; Labianca, R.; Valvo, F.; Farinati, F.; Italian Society of Gastroenterology (SIGE); Italian Association of Hospital Gastroenterology (AIGO); Italian Association of Medical Oncology (AIOM); Italian Association of Oncological Radiotherapy (AIRO). Cholangiocarcinoma: A position paper by the Italian Society of Gastroenterology (SIGE), the Italian Association of Hospital Gastroenterology (AIGO), the Italian Association of Medical Oncology (AIOM) and the Italian Association of Oncological Radiotherapy (AIRO). Dig. Liver Dis. 2010, 42, 831–838. [Google Scholar] [CrossRef]
- Tabrizian, P.; Jibara, G.; Shrager, B.; Schwartz, M.; Roayaie, S. Recurrence of hepatocellular cancer after resection: Patterns, treatments, and prognosis. Ann. Surg. 2015, 261, 947–955. [Google Scholar] [CrossRef]
- Nagao, T.; Inoue, S.; Yoshimi, F.; Sodeyama, M.; Omori, Y.; Mizuta, T.; Kawano, N.; Morioka, Y. Postoperative recurrence of hepatocellular carcinoma. Ann. Surg. 1990, 211, 28–33. [Google Scholar] [CrossRef]
- Yamamoto, J.; Kosuge, T.; Takayama, T.; Shimada, K.; Yamasaki, S.; Ozaki, H.; Yamaguchi, N.; Makuuchi, M. Recurrence of hepatocellular carcinoma after surgery. Br. J. Surg. 1996, 83, 1219–1222. [Google Scholar]
- Lo, C.M.; Lai, E.C.; Fan, S.T.; Choi, T.K.; Wong, J. Resection for extrahepatic recurrence of hepatocellular carcinoma. Br. J. Surg. 1994, 81, 1019–1021. [Google Scholar] [CrossRef]
- Hirsch, R.D.; Mills, C.; Sawhney, R.; Sood, S.; Bird, V.; Mishra, G.; Dev, A.; Kemp, W.; Lubel, J.; Roberts, S.K.; et al. SIRT Compared with DEB-TACE for Hepatocellular Carcinoma: A Real-world Study (the SITAR Study). J. Gastrointest. Cancer 2021, 52, 907–914. [Google Scholar] [CrossRef] [PubMed]
- Erridge, S.; Pucher, P.H.; Markar, S.R.; Malietzis, G.; Athanasiou, T.; Darzi, A.; Sodergren, M.H.; Jiao, L.R. Meta-analysis of determinants of survival following treatment of recurrent hepatocellular carcinoma. Br. J. Surg. 2017, 104, 1433–1442. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.H.; Chung, G.E.; Yu, S.J.; Hwang, S.Y.; Kim, J.S.; Kim, H.Y.; Yoon, J.H.; Lee, H.S.; Yi, N.J.; Suh, K.S.; et al. Long-term prognosis of combined hepatocellular and cholangiocarcinoma after curative resection comparison with hepatocellular carcinoma and cholangiocarcinoma. J. Clin. Gastroenterol. 2011, 45, 69–75. [Google Scholar] [CrossRef] [PubMed]
- Ishii, T.; Ito, T.; Sumiyoshi, S.; Ogiso, S.; Fukumitsu, K.; Seo, S.; Taura, K.; Uemoto, S. Clinicopathological features and recurrence patterns of combined hepatocellular-cholangiocarcinoma. World J. Surg. Oncol. 2020, 18, 319. [Google Scholar] [CrossRef]
- Panjala, C.; Senecal, D.L.; Bridges, M.D.; Kim, G.P.; Nakhleh, R.E.; Nguyen, J.H.; Harnois, D.M. The diagnostic conundrum and liver transplantation outcome for combined hepatocellular-cholangiocarcinoma. Am. J. Transplant. 2010, 10, 1263–1267. [Google Scholar] [CrossRef]
- Wu, D.; Shen, Z.Y.; Zhang, Y.M.; Wang, J.; Zheng, H.; Deng, Y.L.; Pan, C. Effect of liver transplantation in combined hepatocellular and cholangiocellular carcinoma: A case series. BMC Cancer 2015, 15, 232. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| ICC | mHC-CC | cHCC | ncHCC | |
|---|---|---|---|---|
| n = 202 | n = 20 | n = 119 | n = 225 | |
| Gender (Female/Male) | 98/104 | 5/15 | 24/95 | 50/175 |
| Age [Median (IQR)] | 64.4 (57.4–74) | 62.5 (56–67) | 69.9 (63.7–75) | 70.8 (63–76.1) |
| ASA classification | ||||
| ASA I | 2 | 0 | 0 | 1 |
| ASA II | 98 | 7 | 43 | 57 |
| ASA III | 105 | 13 | 73 | 158 |
| ASA IV | 6 | 0 | 3 | 9 |
| Resections | ||||
| Extended resections | 82 (40.6%) | 6 (30%) | 5 (4.2%) | 42 (18.6%) |
| Right trisectionectomy | 32 | 3 | 2 | 25 |
| Left trisectionecotmy | 32 | 1 | 1 | 8 |
| Mesohepatectomy | 11 | 1 | 2 | 9 |
| ALPPS | 7 | 1 | 0 | 0 |
| Major resections | 71 (35.1%) | 2 (10%) | 19 (16%) | 85 (37.8%) |
| Right hepatectomy | 27 | 2 | 10 | 51 |
| Left hepatectomy | 31 | 0 | 5 | 20 |
| Trisegmentectomy | 13 | 0 | 4 | 13 |
| Bisectionectomy | 0 | 0 | 0 | 1 |
| Minor resections | 49 (24.3%) | 6 (30%) | 95 (79.8%) | 98 (43.6%) |
| Bisegmentectomy | 33 | 4 | 33 | 47 |
| Monosegmentectomy | 14 | 1 | 37 | 29 |
| Atypical/wedge resections | 2 | 1 | 25 | 22 |
| Liver transplantation | - | 6 (30%) | - | - |
| Vascular resection/reconstruction * | 67 in 47 pat. | 2 in 2 pat. | 20 in 17 pat. | 52 in 45 pat. |
| PV/MHV/HA/IVC | 26/22/2/17 | 1/1/0/0 | 10/7/1/2 | 14/21/1/16 |
| Visceral resection/reconstruction * | 21 in 19 pat. | 2 in 2 pat. | 12 in 11 pat. | 28 in 27 pat. |
| Adrenal gland/Diaphragm/Duodenum/Stomach/Colon/Pericardium | 5/12/1/1 /1/1 | 1/1/0/0 /0/0 | 3/5/0/3 /1/0 | 7/18/1/0 /2/0 |
| Number of lesions | ||||
| n = 1/2/3/ multifocal (≥4) | 150/14/11/27 | 14/1/0/5 | 72/15/8/24 | 162/24/8/31 |
| Lymphadenectomy [number performed (%)] | 181 (89.6%) | 14 (70%) | 37 (31.1%) | 98 (43.6%) |
| Lymph nodes harvested [Median (IQR)] | 5 (2–8) | 1.5 (0–3) | 2 (1–3) | 2 (1–5) |
| ICC | mHC-CC | cHCC | ncHCC | |
|---|---|---|---|---|
| n = 202 | n = 20 | n = 119 | n = 225 | |
| Resection, n (%) | ||||
| R0 | 166 (82.2) | 18 (90) | 99 (83.2) | 198 (88.0) |
| R1 | 35 (17.3) | 2 (10) | 12 (10.1) | 16 (7.1) |
| R2 | 1 (0.5) | 0 | 7 (5.9) | 5 (2.2) |
| Rx | 0 | 0 | 1 (0.8) | 6 (2.7) |
| T stage, n (%) | ||||
| T1 (a/b) | 85 (34/51; 42.1) | 11 (55) | 53 (44.5) | 79 (35.1) |
| T2 | 76 (37.6) | 6 (30) | 29 (24.4) | 76 (33.8) |
| T3 | 15 (7.4) | 3 (15) | 30 (25.2) | 54 (24.0) |
| T4 | 26 (12.9) | 0 | 6 (5.0) | 15 (6.7) |
| N category, n (%) | ||||
| N0 | 123 (60.9) | 12 (60) | 36 (30.3) | 92 (40.9) |
| N1 | 58 (28.7) | 2 (10) | 1 (0.8) | 6 (2.7) |
| Nx | 21 (10.4) | 6 (30) | 82 (68.9) | 127 (56.4) |
| M category, n (%) | ||||
| M0 | 188 (93.1) | 20 (100) | 117 (98.3) | 212 (94.2) |
| M1 | 14 (6.9) | 0 | 2 (1.7) | 13 (5.7) |
| Tumour Grading, n (%) * | ||||
| G1 | 3 (1.5) | 1 (5) | 11 (9.2) | 15 (6.7) |
| G2 | 129 (63.9) | 8 (40) | 75 (63.0) | 132 (58.7) |
| G3 | 51 (25.2) | 7 (35) | 31 (26.1) | 69 (30.7) |
| G4 | 1 (0.5) | 0 | 0 | 6 (2.7) |
| Vascular Invasion, n (%) | ||||
| V0 | 155 (76.7) | 12 (60) | 76 (63.9) | 112 (49.8) |
| V1 | 43 (21.3) | 7 (35) | 31 (26.1) | 87 (38.7) |
| V2 | 4 (2) | 1 (5) | 12 (10.1) | 25 (11.1) |
| Largest nodule diameter (mm), [median, range] | 67 (4–200) | 48 (8–130) | 47 (12–160) | 85 (10–300) |
| ICC | mHC-CC | cHCC | ncHCC | |
|---|---|---|---|---|
| n = 202 | n = 14/6 OLT | n = 119 | n = 225 | |
| Recurrence, n (%) | 122 (60.4%) | 8/1 (45%) | 80 (67.2%) | 110 (48.9%) |
| Intrahepatic Rec. (n) | 52 (42.6%) | 4/0 (44.4%) | 66 (82.5%) | 66 (60%) |
| Extrahepatic Rec. (n) | 28 (23%) | 1/0 (11.1%) | 4 (5%) | 15 (13.6%) |
| Intra- + extrahepatic Rec. (n) | 42 (34.4%) | 3/1 (44.4%) | 10 (12.5%) | 29 (26.4%) |
| Pat. # | OP Year | Resection Type | Age | TNM Classification | Cirrhosis/Fibrosis | TTR | Rec. Localization | Rec. Therapy | OS | Status |
|---|---|---|---|---|---|---|---|---|---|---|
| Resection | ||||||||||
| 1 | 2011 | Right trisectionectomy | 64 | T3, N1 (2/2), L1, V1, Pn0, G3, R0 | none | - | - | - | 5 | dead |
| 2 | 2012 | Atypical resection | 63 | T1, Nx, L0, V0, Pn0, G2, R0 | cirrhosis | 16 | liver/bone | BSC | 22 | dead |
| 3 | 2013 | Bisegmentectomy | 62 | T1, N1 (9/10), L0, V0, Pn1, G3, R0 | septal fibrosis +ad | - | LFU | |||
| 4 | 2014 | Mesohepatectomy | 72 | T3, N0 (0/3), L0, V2, Pn0, G3, R1 | cirrhosis | 16 | liver | resection | 32 | dead |
| 5 | 2015 | Bisegmentectomy | 75 | T3, N0 (0/1), L0, V0, Pn0, G3, R0 | septal fibrosis -ad | 5 | liver, adrenal gl. | BSC | 9 | dead |
| 6 | 2016 | Left Trisectionectomy | 68 | T2, N0 (0/4), L0, V1, Pn0, G3, R0 | portal fibrosis | 2 | liver | chemo | 14 | dead |
| 7 | 2016 | Left Hepatectomy | 81 | T2, N0 (0/2), L0, V1, Pn0, G2, R0 | portal fibrosis | 23 | liver, kidney, adrenal gl. | BSC | 26 | dead |
| 8 | 2016 | Right trisectionectomy | 48 | T1, Nx, L0, V0, Pn0, Gx*, R0 | cirrhosis | 2 | lung, brain | BSC | 4 | dead |
| 9 | 2017 | ALPPS | 23 | T2, N0 (0/14), L1, V1, Pn0, G2, R1 | portal fibrosis | - | - | - | 0 | dead |
| 10 | 2018 | Right Trisectionectomy | 67 | T2, N0 (0/6), L0, V1, Pn0, G2, R0 | septal fibrosis -ad | 32 | liver | TACE | 37 | alive |
| 11 | 2018 | Monosegmentectomy | 67 | T1, Nx, L0, V0, Pn0, G2, R0 | cirrhosis | - | - | - | 48 | alive |
| 12 | 2018 | Right Hepatectomy | 64 | T1, N0 (0/3), L0, V0, Pn1, G3, R0 | septal fibrosis +ad | - | - | - | 45 | alive |
| 13 | 2018 | Bisegmentectomy | 61 | T1, Nx, L0, V0, Pn0, G3, R0 | septal fibrosis +ad | - | - | - | 47 | alive |
| 14 | 2019 | Bisegmentectomy | 45 | T1, N0 (0/2), L0, V1, Pn0, G2, R0 | none | 3 | liver | Chemo | 27 | alive |
| Transplant | ||||||||||
| 15 | 2011 | oLT | 37 | T1, N0 (0/2), L0, V0, Pn0, G2, R0 | cirrhosis | - | - | - | 131 | alive |
| 16 | 2013 | oLT | 59 | T2, N0 (0/1), L0, V0, Pn0, G1, R0 | cirrhosis | - | - | - | 110 | alive |
| 17 | 2016 | oLT | 56 | T2, Nx, L0, V1, Pn0, G2, R0 | cirrhosis | 44 | liver | radiation | 57 | dead |
| 18 | 2016 | oLT | 61 | T1, N0 (0/1), L0, V0, Pn0, G2, R0 | cirrhosis | - | - | - | 39 | dead |
| 19 | 2017 | oLT | 64 | T1, Nx, L0, V0, Pn0, G2, R0 | cirrhosis | - | - | - | 58 | alive |
| 20 | 2018 | oLT | 56 | T1, N0 (0/1), L0, V0, Pn0, G1, R0 | cirrhosis | - | - | - | 55 | alive |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Penzkofer, L.; Gröger, L.-K.; Hoppe-Lotichius, M.; Baumgart, J.; Heinrich, S.; Mittler, J.; Gerber, T.S.; Straub, B.K.; Weinmann, A.; Bartsch, F.; et al. Mixed Hepatocellular Cholangiocarcinoma: A Comparison of Survival between Mixed Tumors, Intrahepatic Cholangiocarcinoma and Hepatocellular Carcinoma from a Single Center. Cancers 2023, 15, 639. https://doi.org/10.3390/cancers15030639
Penzkofer L, Gröger L-K, Hoppe-Lotichius M, Baumgart J, Heinrich S, Mittler J, Gerber TS, Straub BK, Weinmann A, Bartsch F, et al. Mixed Hepatocellular Cholangiocarcinoma: A Comparison of Survival between Mixed Tumors, Intrahepatic Cholangiocarcinoma and Hepatocellular Carcinoma from a Single Center. Cancers. 2023; 15(3):639. https://doi.org/10.3390/cancers15030639
Chicago/Turabian StylePenzkofer, Lea, Lisa-Katharina Gröger, Maria Hoppe-Lotichius, Janine Baumgart, Stefan Heinrich, Jens Mittler, Tiemo S. Gerber, Beate K. Straub, Arndt Weinmann, Fabian Bartsch, and et al. 2023. "Mixed Hepatocellular Cholangiocarcinoma: A Comparison of Survival between Mixed Tumors, Intrahepatic Cholangiocarcinoma and Hepatocellular Carcinoma from a Single Center" Cancers 15, no. 3: 639. https://doi.org/10.3390/cancers15030639