
The Relationship between Mushroom Intake and Cognitive Performance: An Epidemiological Study in the European Investigation of Cancer—Norfolk Cohort (EPIC-Norfolk)


Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Cohort and Eligibility Criteria
2.2. Measurement of Mushroom Intake
2.3. Assessment of Cognitive Function
2.4. Assessment of Fruit and Vegetable Intake
2.5. Statistical Analysis
3. Results
3.1. Cohort Characteristics (Objective 1)
3.2. Change in Mushroom Consumption over Time (Objective 1)
3.3. Cohort Characteristics (Objective 2)
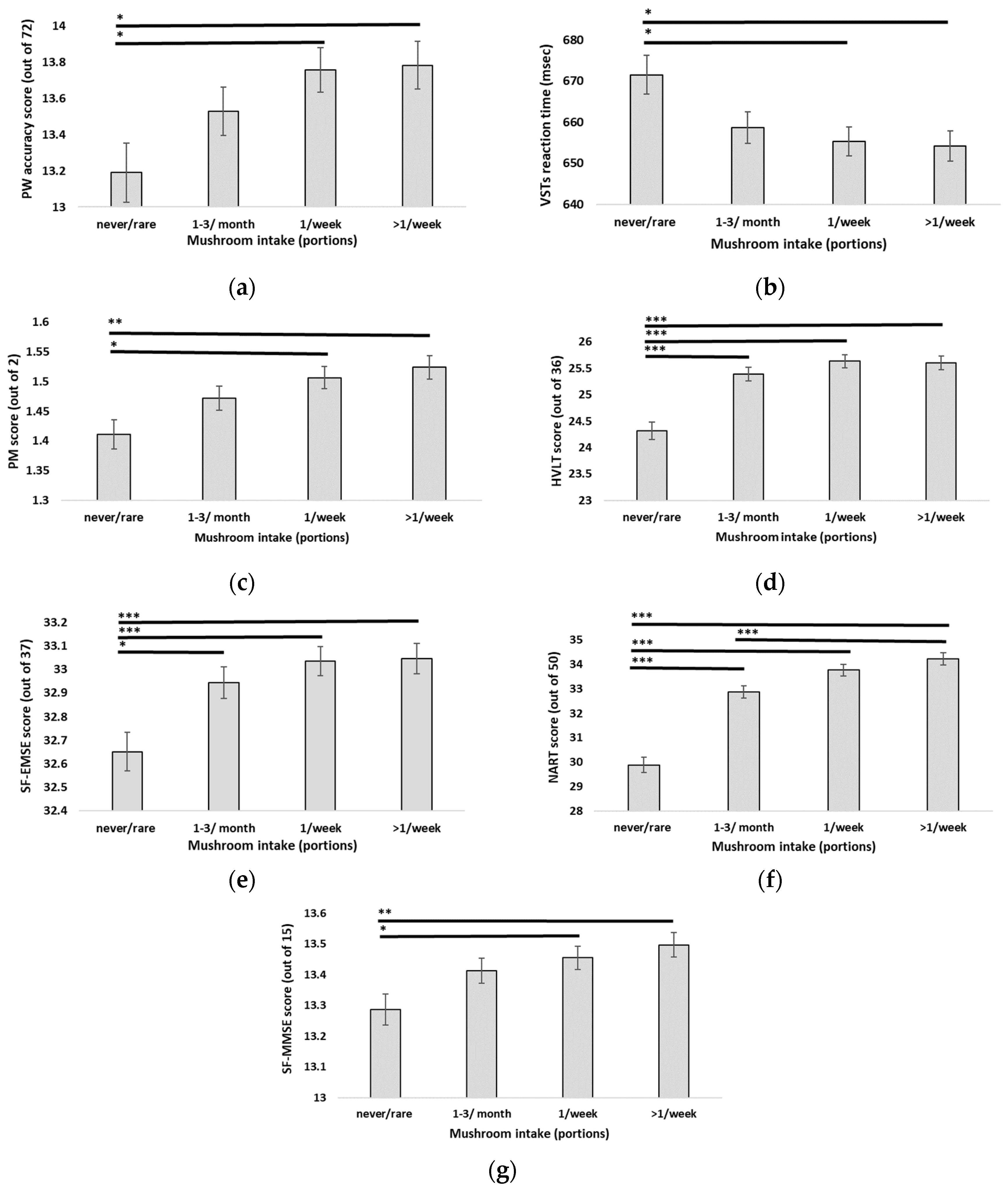
3.4. Relationship between Mushroom Intake and Cognitive Score Measurements (Objective 2)
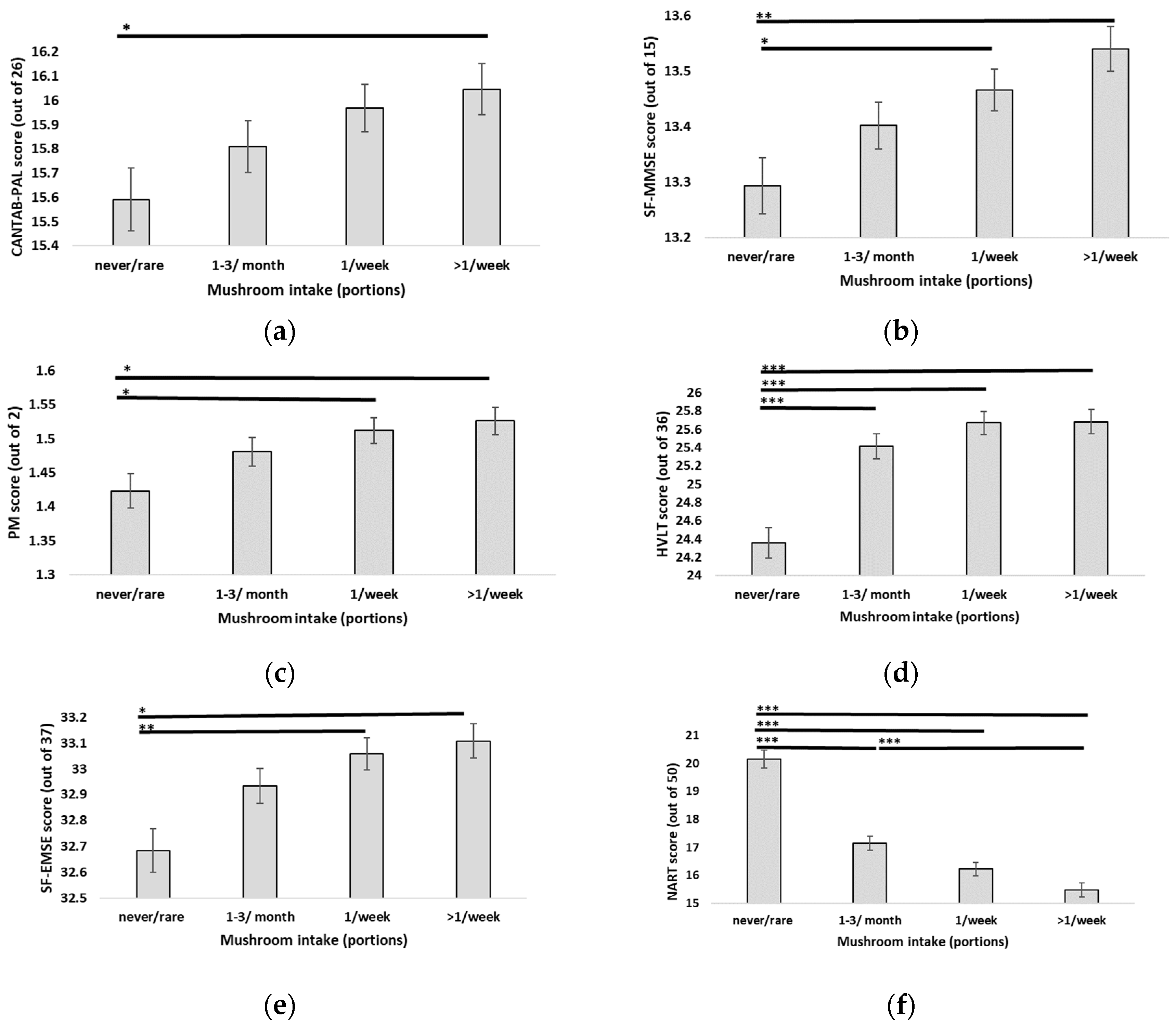
3.5. Accounting for Fruit and Vegetable Intake in the Relationship between Mushroom Intake and Cognitive Score Measurements (Objective 3)
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A. Description of the EPIC-COG Battery Tests Employed in the EPIC-Norfolk 3HC
| Cognitive Test | Domain | Description | Outcome Measure |
| Extended Mental State Exam-Short Form (SF-EMSE) | Global memory (attention, abstract reasoning, and retrospective memory) | Items assessing higher function skills. | Score (0–37) |
| Hopkins Verbal Learning Task (HVLT) | Episodic and recognition memory | Word recall task | Words identified/3 trials (0–36) |
| National Adult Reading Test (NART) | Intelligent Quotient and reading skills | Word pronunciation task | Score (0–50) |
| Cambridge Neuropsychological Test Automated Battery-Paired Associate Learning (CANTAB-PAL) | Episodic memory and learning skills | Six white boxes presented on a touch screen, displaying 8 different visual patterns | Score (0–26) |
| Pairwise Test (PW) | Executive function, attention and processing speed | Visual scanning and crossing of the 72 P and W letters | Number of letters identified/min (0–72) |
| Time and event-based test (PM) | Prospective memory | Explicit instructions about tasks at a specific point | Success (100%)/Partial success (50%)/Failure (0%) |
| Mini-Mental State Exam—Short Form (SF-MMSE) | Memory screening tool (orientation, attention, recall and visuospatial ability) | Items assessing cognitive skills | Score (0–15) |
References
- Mura, T.; Coley, N.; Amieva, H.; Berr, C.; Gabelle, A.; Ousset, P.J.; Vellas, B.; Andrieu, S.; GuidAge/DSA Study Group. Cognitive decline as an outcome and marker of progression toward dementia, in early preventive trials. Alzheimer’s Dement. 2022, 18, 676–687. [Google Scholar] [CrossRef]
- Ma, G.; Yang, W.; Zhao, L.; Pei, F.; Fang, D.; Hu, Q. A critical review on the health promoting effects of mushrooms nutraceuticals. Food Sci. Hum. Wellness 2018, 7, 125–133. [Google Scholar] [CrossRef]
- Liuzzi, G.M.; Petraglia, T.; Latronico, T.; Crescenzi, A.; Rossano, R. Antioxidant Compounds from Edible Mushrooms as Potential Candidates for Treating Age-Related Neurodegenerative Diseases. Nutrients 2023, 15, 1913. [Google Scholar] [CrossRef] [PubMed]
- Phan, C.W.; David, P.; Sabaratnam, V. Edible and Medicinal Mushrooms: Emerging Brain Food for the Mitigation of Neurodegenerative Diseases. J. Med. Food 2017, 20, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Toyomaki, A.; Koga, M.; Okada, E.; Nakai, Y.; Miyazaki, A.; Tamakoshi, A.; Kiso, Y.; Kusumi, I. The relationship between a low grain intake dietary pattern and impulsive behaviors in middle-aged Japanese people. PLoS ONE 2017, 12, e0181057. [Google Scholar] [CrossRef] [PubMed]
- Park, S.J.; Kim, M.S.; Lee, H.J. The association between dietary pattern and depression in middle-aged Korean adults. Nutr. Res. Pract. 2019, 13, 316–322. [Google Scholar] [CrossRef] [PubMed]
- Sun, K.; Hu, H.; Yang, C.; Wang, L.; Ai, Y.; Dong, X.; Shi, Y.; Li, M.; Yao, Q.; Zhang, Y. Dietary Intake is Positively Associated with Cognitive Function of a Chinese Older Adults Sample. J. Nutr. Health Aging 2018, 22, 805–810. [Google Scholar] [CrossRef] [PubMed]
- Shang, X.; Hodge, A.M.; Hill, E.; Zhu, Z.; He, M. Associations of Dietary Pattern and Sleep Duration with Cognitive Decline in Community-Dwelling Older Adults: A Seven-Year Follow-Up Cohort Study. J. Alzheimer’s Dis. 2021, 82, 1559–1571. [Google Scholar] [CrossRef] [PubMed]
- Okubo, H.; Inagaki, H.; Gondo, Y.; Kamide, K.; Ikebe, K.; Masui, Y.; Arai, Y.; Ishizaki, T.; Sasaki, S.; Nakagawa, T.; et al. Association between dietary patterns and cognitive function among 70-year-old Japanese elderly: A cross-sectional analysis of the SONIC study. Nutr. J. 2017, 16, 56. [Google Scholar] [CrossRef]
- Nurk, E.; Refsum, H.; Drevon, C.A.; Tell, G.S.; Nygaard, H.A.; Engedal, K.; Smith, A.D. Cognitive performance among the elderly in relation to the intake of plant foods. The Hordaland Health Study. Br. J. Nutr. 2010, 104, 1190–1201. [Google Scholar] [CrossRef]
- Zhang, Y.; Yang, X.; Jin, G. Polysaccharides from Pleurotus ostreatus alleviate cognitive impairment in a rat model of Alzheimer’s disease. Int. J. Biol. Macromol. 2016, 92, 935–941. [Google Scholar] [CrossRef]
- Feng, L.; Cheah, I.K.; Ng, M.M.; Li, J.; Chan, S.M.; Lim, S.L.; Mahendran, R.; Kua, E.H.; Halliwell, B. The Association between Mushroom Consumption and Mild Cognitive Impairment: A Community-Based Cross-Sectional Study in Singapore. J. Alzheimer’s Dis. 2019, 68, 197–203. [Google Scholar] [CrossRef] [PubMed]
- Ba, D.M.; Gao, X.; Al-Shaar, L.; Muscat, J.E.; Chinchilli, V.M.; Beelman, R.B.; Richie, J.P. Mushroom intake and depression: A population-based study using data from the US National Health and Nutrition Examination Survey (NHANES), 2005–2016. J. Affect. Disord. 2021, 294, 686–692. [Google Scholar] [CrossRef]
- Ba, D.M.; Gao, X.; Al-Shaar, L.; Muscat, J.; Chinchilli, V.M.; Ssentongo, P.; Beelman, R.B.; Richie, J. Mushroom intake and cognitive performance among US older adults: The National Health and Nutrition Examination Survey, 2011–2014. Br. J. Nutr. 2022, 128, 2241–2248. [Google Scholar] [CrossRef] [PubMed]
- Park, S.K.; Oh, C.M.; Ryoo, J.H.; Jung, J.Y. The protective effect of mushroom consumption on depressive symptoms in Korean population. Sci. Rep. 2022, 12, 21914. [Google Scholar] [CrossRef] [PubMed]
- Xu, X.; Parker, D.; Shi, Z.; Byles, J.; Hall, J.; Hickman, L. Dietary Pattern, Hypertension and Cognitive Function in an Older Population: 10-Year Longitudinal Survey. Front. Public Health 2018, 6, 201. [Google Scholar] [CrossRef] [PubMed]
- Mori, K.; Inatomi, S.; Ouchi, K.; Azumi, Y.; Tuchida, T. Improving effects of the mushroom Yamabushitake (Hericium erinaceus) on mild cognitive impairment: A double-blind placebo-controlled clinical trial. Phytother. Res. 2009, 23, 367–372. [Google Scholar] [CrossRef] [PubMed]
- Saitsu, Y.; Nishide, A.; Kikushima, K.; Shimizu, K.; Ohnuki, K. Improvement of cognitive functions by oral intake of Hericium erinaceus. Biomed. Res. 2019, 40, 125–131. [Google Scholar] [CrossRef] [PubMed]
- Li, I.-C.; Chang, H.-H.; Lin, C.-H.; Chen, W.-P.; Lu, T.-H.; Lee, L.-Y.; Chen, Y.W.; Chen, Y.P.; Chen, C.C.; Lin, D.P.C. Prevention of Early Alzheimer’s Disease by Erinacine A-Enriched Hericium erinaceus Mycelia Pilot Double-Blind Placebo-Controlled Study [Clinical Trial]. Front. Aging Neurosci. 2020, 12, 155. [Google Scholar] [CrossRef] [PubMed]
- Grozier, C.D.; Alves, V.A.; Killen, L.G.; Simpson, J.D.; O’Neal, E.K.; Waldman, H.S. Four Weeks of Hericium erinaceus Supplementation Does Not Impact Markers of Metabolic Flexibility or Cognition. Int. J. Exerc. Sci. 2022, 15, 1366–1380. [Google Scholar]
- Wang, G.H.; Wang, L.H.; Wang, C.; Qin, L.H. Spore powder of Ganoderma lucidum for the treatment of Alzheimer disease: A pilot study. Medicine 2018, 97, e0636. [Google Scholar] [CrossRef] [PubMed]
- Nagano, M.; Shimizu, K.; Kondo, R.; Hayashi, C.; Sato, D.; Kitagawa, K.; Ohnuki, K. Reduction of depression and anxiety by 4 weeks Hericium erinaceus intake. Biomed. Res. 2010, 31, 231–237. [Google Scholar] [CrossRef] [PubMed]
- Vigna, L.; Morelli, F.; Agnelli, G.M.; Napolitano, F.; Ratto, D.; Occhinegro, A.; Di Iorio, C.; Savino, E.; Girometta, C.; Brandalise, F.; et al. Improves Mood and Sleep Disorders in Patients Affected by Overweight or Obesity: Could Circulating Pro-BDNF and BDNF Be Potential Biomarkers? Evid. Based Complement. Alternat. Med. 2019, 2019, 7861297. [Google Scholar] [CrossRef] [PubMed]
- Day, N.; Oakes, S.; Luben, R.; Khaw, K.T.; Bingham, S.; Welch, A.; Wareham, N. EPIC-Norfolk: Study design and characteristics of the cohort. European Prospective Investigation of Cancer. Br. J. Cancer 1999, 80 (Suppl. S1), 95–103. [Google Scholar] [PubMed]
- Hayat, S.A.; Luben, R.; Khaw, K.T.; Brayne, C. The Relationship Between Cognitive Performance Using Tests Assessing a Range of Cognitive Domains and Future Dementia Diagnosis in a British Cohort: A Ten-Year Prospective Study. J. Alzheimer’s Dis. 2021, 81, 123–135. [Google Scholar] [CrossRef]
- Bingham, S.; Luben, R.; Welch, A.; Low, Y.L.; Khaw, K.T.; Wareham, N.; Day, N. Associations between dietary methods and biomarkers, and between fruits and vegetables and risk of ischaemic heart disease, in the EPIC Norfolk Cohort Study. Int. J. Epidemiol. 2008, 37, 978–987. [Google Scholar] [CrossRef]
- Mulligan, A.A.; Luben, R.N.; Bhaniani, A.; Parry-Smith, D.J.; O’Connor, L.; Khawaja, A.P.; Forouhi, N.G.; Khaw, K.T. A new tool for converting food frequency questionnaire data into nutrient and food group values: FETA research methods and availability. BMJ Open 2014, 4, e004503. [Google Scholar] [CrossRef]
- Khaled, K.; Hundley, V.; Bassil, M.; Bazzi, M.; Tsofliou, F. Validation of the European Prospective Investigation into Cancer (EPIC) FFQ for use among adults in Lebanon. Public Health Nutr. 2021, 24, 4007–4016. [Google Scholar] [CrossRef]
- McEvoy, C.T.; Hoang, T.; Sidney, S.; Steffen, L.M.; Jacobs, D.R.; Shikany, J.M.; Wilkins, J.T.; Yaffe, K. Dietary patterns during adulthood and cognitive performance in midlife: The CARDIA study. Neurology 2019, 92, e1589–e1599. [Google Scholar] [CrossRef]
- Hepsomali, P.; Groeger, J.A. Diet and general cognitive ability in the UK Biobank dataset. Sci. Rep. 2021, 11, 11786. [Google Scholar] [CrossRef]
- Saji, N.; Tsuduki, T.; Murotani, K.; Hisada, T.; Sugimoto, T.; Kimura, A.; Niida, S.; Toba, K.; Sakurai, T. Relationship between the Japanese-style diet, gut microbiota, and dementia: A cross-sectional study. Nutrition 2022, 94, 111524. [Google Scholar] [CrossRef]
- Wei, K.; Yang, J.; Lin, S.; Mei, Y.; An, N.; Cao, X.; Jiang, L.; Liu, C.; Li, C. Dietary Habits Modify the Association of Physical Exercise with Cognitive Impairment in Community-Dwelling Older Adults. J. Clin. Med. 2022, 11, 5122. [Google Scholar] [CrossRef]
- Cha, S.; Bell, L.; Shukitt-Hale, B.; Williams, C.M. A review of the effects of mushrooms on mood and neurocognitive health across the lifespan. Neurosci. Biobehav. Rev. 2024, in press. [CrossRef]
- Rai, S.N.; Mishra, D.; Singh, P.; Vamanu, E.; Singh, M.P. Therapeutic applications of mushrooms and their biomolecules along with a glimpse of in silico approach in neurodegenerative diseases. Biomed. Pharmacother. 2021, 137, 111377. [Google Scholar] [CrossRef]
- Thangthaeng, N.; Miller, M.G.; Gomes, S.M.; Shukitt-Hale, B. Daily supplementation with mushroom (Agaricus bisporus) improves balance and working memory in aged rats. Nutr. Res. 2015, 35, 1079–1084. [Google Scholar] [CrossRef]
- Morris, M.C.; Evans, D.A.; Tangney, C.C.; Bienias, J.L.; Wilson, R.S. Associations of vegetable and fruit consumption with age-related cognitive change. Neurology 2006, 67, 1370–1376. [Google Scholar] [CrossRef] [PubMed]
- Zhang, S.; Tomata, Y.; Sugiyama, K.; Sugawara, Y.; Tsuji, I. Mushroom consumption and incident dementia in elderly Japanese: The Ohsaki Cohort 2006 Study. J. Am. Geriatr. Soc. 2017, 65, 1462–1469. [Google Scholar] [CrossRef] [PubMed]
- Kim, C.S.; Byeon, S.; Shin, D.M. Sources of dietary fiber are differently associated with prevalence of depression. Nutrients 2020, 12, 2813. [Google Scholar] [CrossRef] [PubMed]
- Yoon, S.I.; Moon, H.R.; Lee, S.R.; Zhang, J.; Lee, S.; Cho, J.A. Nutrient Inadequacy in Korean Young Adults with Depression: A Case Control Study. Nutrients 2023, 15, 2195. [Google Scholar] [CrossRef] [PubMed]
- Ba, D.M.; Zhang, S.; Nishita, Y.; Tange, C.; Qiu, T.; Gao, X.; Muscat, J.; Otsuka, R. Mushroom consumption and hyperuricemia: Results from the National Institute for Longevity Sciences-Longitudinal Study of Aging and the National Health and Nutrition Examination Survey (2007–2018). Nutr. J. 2023, 22, 62. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| N = 5091 | 1HC | 2HC | 3HC |
|---|---|---|---|
| Weekly portions (mean (SE)) | 1.42 (0.02) | 1.34 (0.02) | 1.30 (0.02) |
| Non-consumers | 756 (14.85%) | 858 (16.85%) | 966 (18.97%) |
| Consumers | 4335 (85.15%) | 4233 (83.15%) | 4125 (81.03%) |
| Characteristic | N = 5418 |
|---|---|
| Sex | |
| Females | 2995 (55.28%) |
| Males | 2423 (44.72%) |
| Age | |
| <55 y old | 145 (2.68%) |
| 55–64 y old | 1961 (36.19%) |
| 65–74 y old | 2213 (40.84%) |
| 75–84 y old | 1030 (19.01%) |
| >85 y old | 69 (1.27%) |
| Body Mass Index (BMI) | |
| Underweight (<18.5) | 39 (0.72%) |
| Normal weight (18.5–24.9) | 1873 (34.57%) |
| Overweight (25.0–29.9) | 2500 (46.14%) |
| Obesity class I (30.0–34.9) | 781 (14.41%) |
| Obesity class II 35.0–39.9) | 178 (3.29%) |
| Obesity class III (≥40.0) | 47 (0.87%) |
| Physical activity status | |
| Active | 880 (16.24%) |
| Moderate active | 997 (18.40%) |
| Moderate inactive | 1607 (29.66%) |
| Inactive | 1934 (35.70%) |
| Ethnic origin | |
| White | 5403 (99.72%) |
| Non-white/Other | 15 (0.28%) |
| Mushroom frequency intake | |
| Never/rare | 935 (17.26%) |
| 1–3 portions/month | 1381 (25.49%) |
| 1 portion/week | 1642 (30.31%) |
| 2–4 portions/week | 1287 (23.75%) |
| 5–6 portions/week | 137 (2.53%) |
| 1 portion/day | 36 (0.66%) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cha, S.; Bell, L.; Williams, C.M. The Relationship between Mushroom Intake and Cognitive Performance: An Epidemiological Study in the European Investigation of Cancer—Norfolk Cohort (EPIC-Norfolk). Nutrients 2024, 16, 353. https://doi.org/10.3390/nu16030353
Cha S, Bell L, Williams CM. The Relationship between Mushroom Intake and Cognitive Performance: An Epidemiological Study in the European Investigation of Cancer—Norfolk Cohort (EPIC-Norfolk). Nutrients. 2024; 16(3):353. https://doi.org/10.3390/nu16030353
Chicago/Turabian StyleCha, Sara, Lynne Bell, and Claire M. Williams. 2024. "The Relationship between Mushroom Intake and Cognitive Performance: An Epidemiological Study in the European Investigation of Cancer—Norfolk Cohort (EPIC-Norfolk)" Nutrients 16, no. 3: 353. https://doi.org/10.3390/nu16030353