
Adverse Food Reactions in Inflammatory Bowel Disease: State of the Art and Future Perspectives

 , , ,
, , ,
Abstract
:1. Introduction
2. Methodology
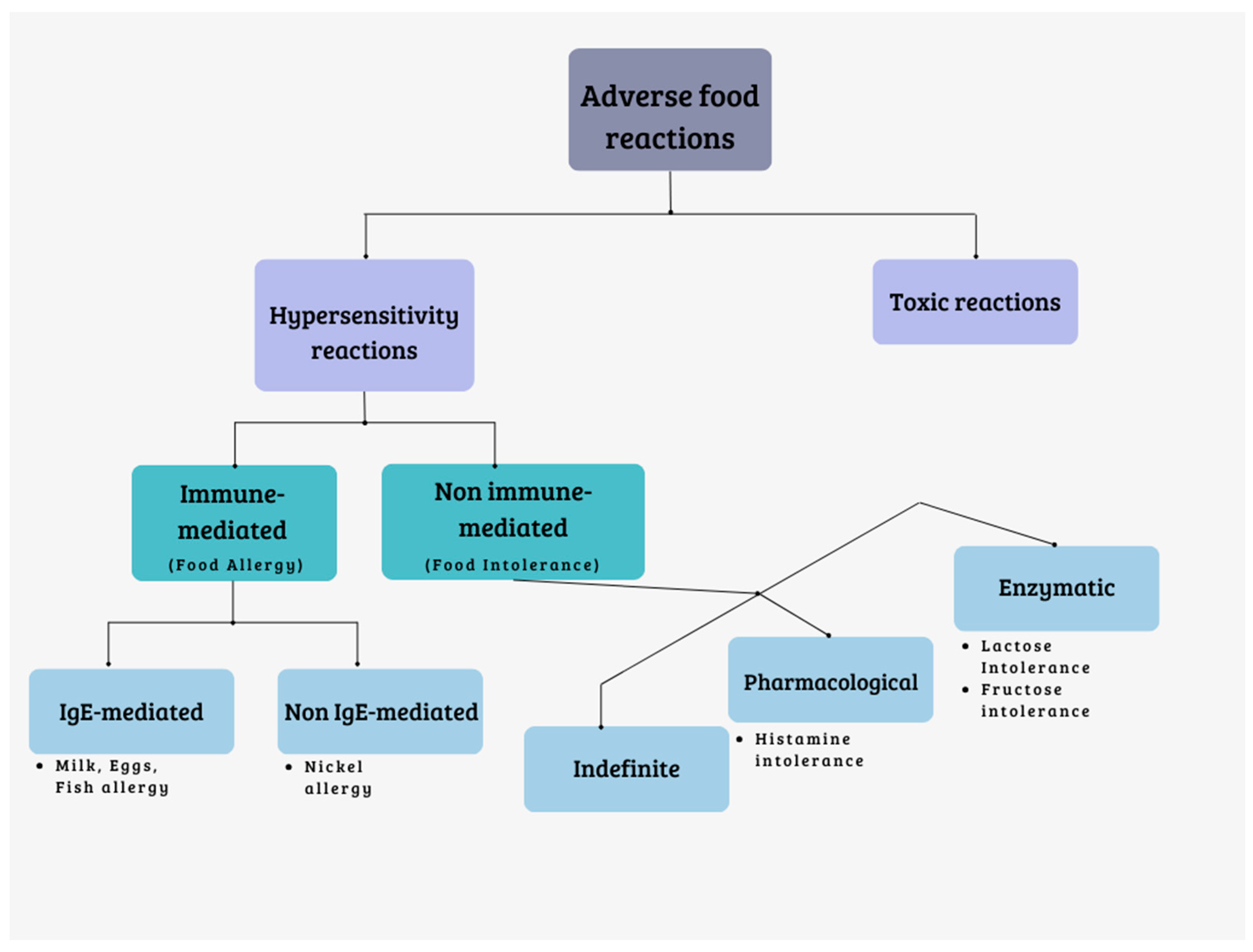
3. Food Allergies and Intolerances
- Reactions mediated by the immune system (food allergies).
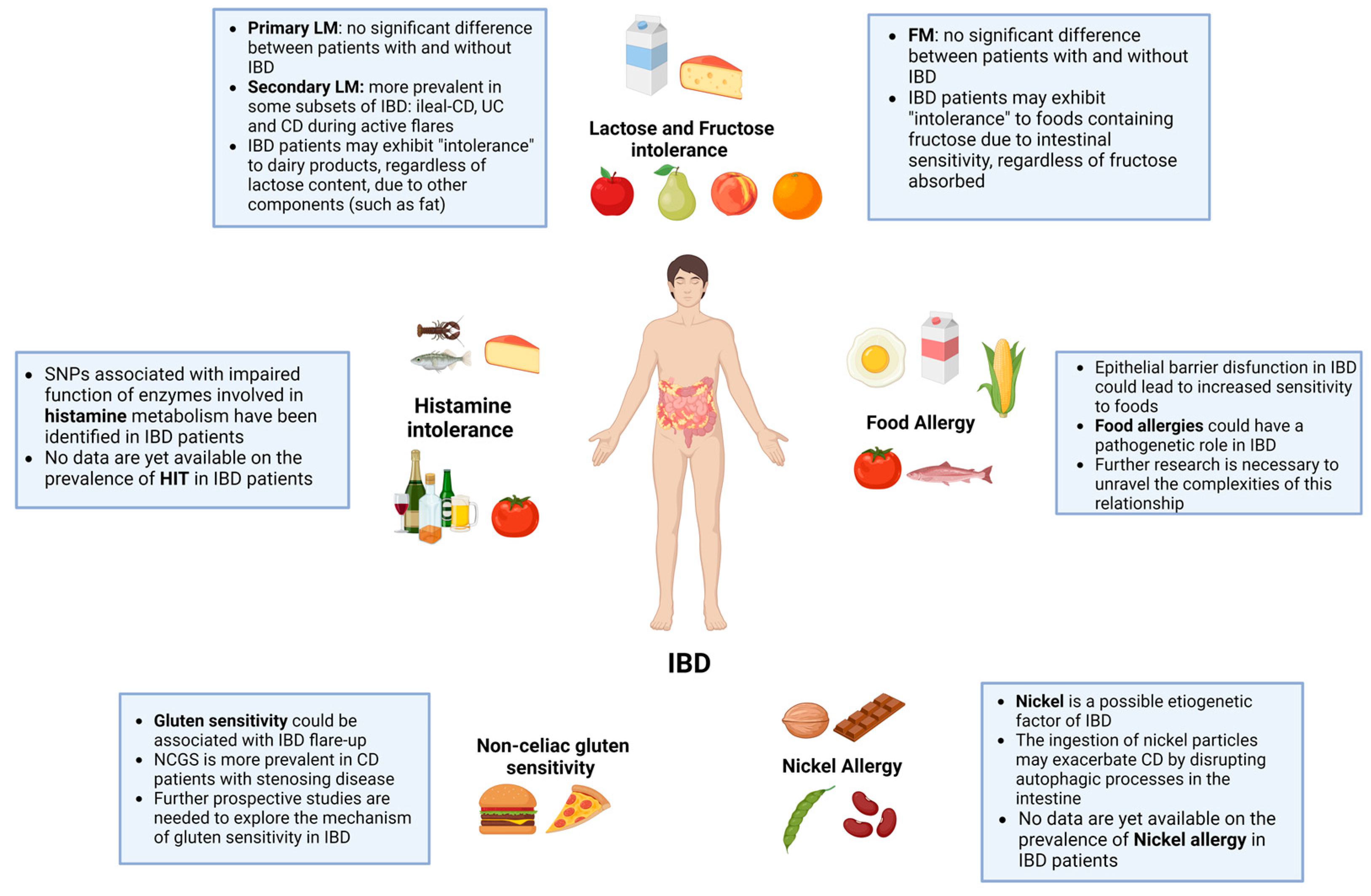
4. Food Intolerances and IBD
4.1. Lactose Intolerance and IBD
4.2. Fructose Intolerance and IBD
4.3. Histamine Intolerance and IBD
4.4. Non-Celiac Gluten Sensitivity and IBD
5. Food Allergies and IBD
Nickel and IBD
6. Conclusions and Future Directions
7. Limitations
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Bruner, L.P.; White, A.M.; Proksell, S. Inflammatory Bowel Disease. Prim. Care Clin. Off. Pract. 2023, 50, 411–427. [Google Scholar] [CrossRef]
- Ballegaard, M.; Bjergstrøm, A.; Brøndum, S.; Hylander, E.; Jensen, L.; Ladefoged, K. Self-Reported Food Intolerance in Chronic Inflammatory Bowel Disease. Scand. J. Gastroenterol. 1997, 32, 569–571. [Google Scholar] [CrossRef]
- Zallot, C.; Quilliot, D.; Chevaux, J.-B.; Peyrin-Biroulet, C.; Guéant-Rodriguez, R.M.; Freling, E.; Collet-Fenetrier, B.; Williet, N.; Ziegler, O.; Bigard, M.-A.; et al. Dietary Beliefs and Behavior Among Inflammatory Bowel Disease Patients. Inflamm. Bowel Dis. 2013, 19, 66–72. [Google Scholar] [CrossRef]
- Cohen, A.B.; Lee, D.; Long, M.D.; Kappelman, M.D.; Martin, C.F.; Sandler, R.S.; Lewis, J.D. Dietary Patterns and Self-Reported Associations of Diet with Symptoms of Inflammatory Bowel Disease. Dig. Dis. Sci. 2013, 58, 1322–1328. [Google Scholar] [CrossRef] [PubMed]
- Schnedl, W.J.; Michaelis, S.; Enko, D.; Mangge, H. Fecal Calprotectin Elevations Associated with Food Intolerance/Malabsorption Are Significantly Reduced with Targeted Diets. Nutrients 2023, 15, 1179. [Google Scholar] [CrossRef] [PubMed]
- Johansson, S.G.O.; Hourihane, J.O.; Bousquet, J.; Bruijnzeel-Koomen, C.; Dreborg, S.; Haahtela, T.; Kowalski, M.L.; Mygind, N.; Ring, J.; van Cauwenberge, P.; et al. A Revised Nomenclature for Allergy: An EAACI Position Statement from the EAACI Nomenclature Task Force. Allergy 2001, 56, 813–824. [Google Scholar] [CrossRef] [PubMed]
- Nucera, E. Appunti di Allergologia; Aracne Editrice: Rome, Italy, 2020. [Google Scholar]
- Bartha, I.; Almulhem, N.; Santos, A.F. Feast for Thought: A Comprehensive Review of Food Allergy 2021–2023. J. Allergy Clin. Immunol. 2023; in press. [Google Scholar] [CrossRef]
- Nwaru, B.I.; Hickstein, L.; Panesar, S.S.; Roberts, G.; Muraro, A.; Sheikh, A. Prevalence of Common Food Allergies in Europe: A Systematic Review and Meta-Analysis. Allergy 2014, 69, 992–1007. [Google Scholar] [CrossRef] [PubMed]
- García, B.E.; Lizaso, M.T. Cross-Reactivity Syndromes in Food Allergy. J. Investig. Allergol. Clin. Immunol. 2011, 21, 162–170. [Google Scholar]
- Spolidoro, G.C.I.; Ali, M.M.; Amera, Y.T.; Nyassi, S.; Lisik, D.; Ioannidou, A.; Rovner, G.; Khaleva, E.; Venter, C.; van Ree, R.; et al. Prevalence Estimates of Eight Big Food Allergies in Europe: Updated Systematic Review and Meta-analysis. Allergy 2023, 78, 2361–2417. [Google Scholar] [CrossRef]
- Cox, A.L.; Eigenmann, P.A.; Sicherer, S.H. Clinical Relevance of Cross-Reactivity in Food Allergy. J. Allergy Clin. Immunol. Pract. 2021, 9, 82–99. [Google Scholar] [CrossRef]
- Patriarca, G.; Schiavino, D.; Pecora, V.; Lombardo, C.; Pollastrini, E.; Aruanno, A.; Sabato, V.; Colagiovanni, A.; Rizzi, A.; De Pasquale, T.; et al. Food Allergy and Food Intolerance: Diagnosis and Treatment. Intern. Emerg. Med. 2009, 4, 11–24. [Google Scholar] [CrossRef]
- Gargano, D.; Appanna, R.; Santonicola, A.; De Bartolomeis, F.; Stellato, C.; Cianferoni, A.; Casolaro, V.; Iovino, P. Food Allergy and Intolerance: A Narrative Review on Nutritional Concerns. Nutrients 2021, 13, 1638. [Google Scholar] [CrossRef]
- Deng, Y.; Misselwitz, B.; Dai, N.; Fox, M. Lactose Intolerance in Adults: Biological Mechanism and Dietary Management. Nutrients 2015, 7, 8020–8035. [Google Scholar] [CrossRef]
- Misselwitz, B.; Butter, M.; Verbeke, K.; Fox, M.R. Update on Lactose Malabsorption and Intolerance: Pathogenesis, Diagnosis and Clinical Management. Gut 2019, 68, 2080–2091. [Google Scholar] [CrossRef]
- Srinivasan, R.; Minocha, A. When to Suspect Lactose Intolerance. Postgrad. Med. 1998, 104, 109–123. [Google Scholar] [CrossRef]
- Szilagyi, A.; Galiatsatos, P.; Xue, X. Systematic Review and Meta-Analysis of Lactose Digestion, Its Impact on Intolerance and Nutritional Effects of Dairy Food Restriction in Inflammatory Bowel Diseases. Nutr. J. 2015, 15, 67. [Google Scholar] [CrossRef]
- Eadala, P.; Matthews, S.B.; Waud, J.P.; Green, J.T.; Campbell, A.K. Association of Lactose Sensitivity with Inflammatory Bowel Disease - Demonstrated by Analysis of Genetic Polymorphism, Breath Gases and Symptoms. Aliment. Pharmacol. Ther. 2011, 34, 735–746. [Google Scholar] [CrossRef]
- Jasielska, M.; Grzybowska-Chlebowczyk, U. Lactose Malabsorption and Lactose Intolerance in Children with Inflammatory Bowel Diseases. Gastroenterol. Res. Pract. 2019, 2019, 2507242. [Google Scholar] [CrossRef] [PubMed]
- Nardone, O.M.; Manfellotto, F.; D’Onofrio, C.; Rocco, A.; Annona, G.; Sasso, F.; De Luca, P.; Imperatore, N.; Testa, A.; de Sire, R.; et al. Lactose Intolerance Assessed by Analysis of Genetic Polymorphism, Breath Test and Symptoms in Patients with Inflammatory Bowel Disease. Nutrients 2021, 13, 1290. [Google Scholar] [CrossRef] [PubMed]
- Pfefferkorn, M.D.; Fitzgerald, J.F.; Croffie, J.M.; Gupta, S.K.; Corkins, M.R.; Molleston, J.P. Lactase Deficiency: Not More Common in Pediatric Patients with Inflammatory Bowel Disease Than in Patients with Chronic Abdominal Pain. J. Pediatr. Gastroenterol. Nutr. 2002, 35, 339–343. [Google Scholar] [CrossRef] [PubMed]
- Nolan, D.J.; Han, D.Y.; Lam, W.J.; Morgan, A.R.; Fraser, A.G.; Tapsell, L.C.; Ferguson, L.R. Genetic Adult Lactase Persistence Is Associated with Risk of Crohn’s Disease in a New Zealand Population. BMC Res. Notes 2010, 3, 339. [Google Scholar] [CrossRef] [PubMed]
- Shrier, I.; Szilagyi, A.; Correa, J.A. Impact of Lactose Containing Foods and the Genetics of Lactase on Diseases: An Analytical Review of Population Data. Nutr. Cancer 2008, 60, 292–300. [Google Scholar] [CrossRef] [PubMed]
- Laing, B.B.; Lim, A.G.; Ferguson, L.R. A Personalised Dietary Approach—A Way Forward to Manage Nutrient Deficiency, Effects of the Western Diet, and Food Intolerances in Inflammatory Bowel Disease. Nutrients 2019, 11, 1532. [Google Scholar] [CrossRef] [PubMed]
- Asfari, M.M.; Sarmini, M.T.; Kendrick, K.; Hudgi, A.; Uy, P.; Sridhar, S.; Sifuentes, H. Association between Inflammatory Bowel Disease and Lactose Intolerance: Fact or Fiction. Korean J. Gastroenterol. 2020, 76, 185–190. [Google Scholar] [CrossRef] [PubMed]
- Wright, R.; Truelove, S.C. A Controlled Therapeutic Trial of Various Diets in Ulcerative Colitis. BMJ 1965, 2, 138–141. [Google Scholar] [CrossRef] [PubMed]
- Gudmand-Hoyer, E.; Jarnum, S. Incidence and Clinical Significance of Lactose Malabsorption in Ulcerative Colitis and Crohn’s Disease. Gut 1970, 11, 338–343. [Google Scholar] [CrossRef]
- Wiecek, S.; Wos, H.; Radziewicz-Winnicki, I.; Komraus, M.; Grzybowska-Chlebowczyk, U. Disaccharidase Activity in Children with Inflammatory Bowel Disease. Turk. J. Gastroenterol. 2014, 25, 185–191. [Google Scholar] [CrossRef]
- Mishkin, S. Controversies Regarding the Role of Dairy Products in Inflammatory Bowel Disease. Can. J. Gastroenterol. 1994, 8, 205–212. [Google Scholar] [CrossRef]
- Nolan-Clark, D.; Tapsell, L.C.; Hu, R.; Han, D.Y.; Ferguson, L.R. Effects of Dairy Products on Crohn’s Disease Symptoms Are Influenced by Fat Content and Disease Location but Not Lactose Content or Disease Activity Status in a New Zealand Population. J. Am. Diet. Assoc. 2011, 111, 1165–1172. [Google Scholar] [CrossRef]
- Shafiee, N.H.; Manaf, Z.A.; Mokhtar, N.M.; Raja Ali, R.A. Anti-Inflammatory Diet and Inflammatory Bowel Disease: What Clinicians and Patients Should Know? Intest. Res. 2021, 19, 171–185. [Google Scholar] [CrossRef]
- Suskind, D.L.; Wahbeh, G.; Gregory, N.; Vendettuoli, H.; Christie, D. Nutritional Therapy in Pediatric Crohn Disease. J. Pediatr. Gastroenterol. Nutr. 2014, 58, 87–91. [Google Scholar] [CrossRef] [PubMed]
- Melgaard, D.; Sørensen, J.; Riis, J.; Ovesen, T.S.; Leutscher, P.; Sørensen, S.; Knudsen, J.K.; Bundgaard-Nielsen, C.; Ejstrup, J.; Jensen, A.-M.; et al. Efficacy of FODMAP Elimination and Subsequent Blinded Placebo-Controlled Provocations in a Randomised Controlled Study in Patients with Ulcerative Colitis in Remission and Symptoms of Irritable Bowel Syndrome: A Feasibility Study. Nutrients 2022, 14, 1296. [Google Scholar] [CrossRef]
- Gibson, P.R. Use of the Low-FODMAP Diet in Inflammatory Bowel Disease. J. Gastroenterol. Hepatol. 2017, 32, 40–42. [Google Scholar] [CrossRef]
- Yanai, H.; Levine, A.; Hirsch, A.; Boneh, R.S.; Kopylov, U.; Eran, H.B.; Cohen, N.A.; Ron, Y.; Goren, I.; Leibovitzh, H.; et al. The Crohn’s Disease Exclusion Diet for Induction and Maintenance of Remission in Adults with Mild-to-Moderate Crohn’s Disease (CDED-AD): An Open-Label, Pilot, Randomised Trial. Lancet Gastroenterol. Hepatol. 2022, 7, 49–59. [Google Scholar] [CrossRef] [PubMed]
- Peng, Z.; Yi, J.; Liu, X. A Low-FODMAP Diet Provides Benefits for Functional Gastrointestinal Symptoms but Not for Improving Stool Consistency and Mucosal Inflammation in IBD: A Systematic Review and Meta-Analysis. Nutrients 2022, 14, 2072. [Google Scholar] [CrossRef] [PubMed]
- Campmans-Kuijpers, M.J.E.; Dijkstra, G. Food and Food Groups in Inflammatory Bowel Disease (IBD): The Design of the Groningen Anti-Inflammatory Diet (GrAID). Nutrients 2021, 13, 1067. [Google Scholar] [CrossRef]
- Reddavide, R.; Rotolo, O.; Caruso, M.G.; Stasi, E.; Notarnicola, M.; Miraglia, C.; Nouvenne, A.; Meschi, T.; De’ Angelis, G.L.; Di Mario, F.; et al. The Role of Diet in the Prevention and Treatment of Inflammatory Bowel Diseases. Acta Biomed. 2018, 89, 60–75. [Google Scholar] [CrossRef]
- Opstelten, J.L.; Leenders, M.; Dik, V.K.; Chan, S.S.M.; van Schaik, F.D.M.; Khaw, K.-T.; Luben, R.; Hallmans, G.; Karling, P.; Lindgren, S.; et al. Dairy Products, Dietary Calcium, and Risk of Inflammatory Bowel Disease: Results from a European Prospective Cohort Investigation. Inflamm. Bowel Dis. 2016, 22, 1403–1411. [Google Scholar] [CrossRef]
- Bernstein, C.N.; Leslie, W.D.; Leboff, M.S. AGA Technical Review on Osteoporosis in Gastrointestinal Diseases. Gastroenterology 2003, 124, 795–841. [Google Scholar] [CrossRef]
- Caniggia, A.; Nuti, R.; Lore, F.; Vattimo, A. Pathophysiology of the Adverse Effects of Glucoactive Corticosteroids on Calcium Metabolism in Man. J. Steroid Biochem. 1981, 15, 153–161. [Google Scholar] [CrossRef]
- Lim, H.-S.; Kim, S.-K.; Hong, S.-J. Food Elimination Diet and Nutritional Deficiency in Patients with Inflammatory Bowel Disease. Clin. Nutr. Res. 2018, 7, 48. [Google Scholar] [CrossRef]
- Rumessen, J.J. Fructose and Related Food Carbohydrates. Sources, Intake, Absorption, and Clinical Implications. Scand. J. Gastroenterol. 1992, 27, 819–828. [Google Scholar] [CrossRef]
- Riby, J.E.; Fujisawa, T.; Kretchmer, N. Fructose Absorption. Am. J. Clin. Nutr. 1993, 58, 748S–753S. [Google Scholar] [CrossRef]
- Jones, H.F.; Burt, E.; Dowling, K.; Davidson, G.; Brooks, D.A.; Butler, R.N. Effect of Age on Fructose Malabsorption in Children Presenting with Gastrointestinal Symptoms. J. Pediatr. Gastroenterol. Nutr. 2011, 52, 581–584. [Google Scholar] [CrossRef]
- Ravich, W.J.; Bayless, T.M.; Thomas, M. Fructose: Incomplete Intestinal Absorption in Humans. Gastroenterology 1983, 84, 26–29. [Google Scholar] [CrossRef] [PubMed]
- Barone, S.; Fussell, S.L.; Singh, A.K.; Lucas, F.; Xu, J.; Kim, C.; Wu, X.; Yu, Y.; Amlal, H.; Seidler, U.; et al. Slc2a5 (Glut5) Is Essential for the Absorption of Fructose in the Intestine and Generation of Fructose-Induced Hypertension. J. Biol. Chem. 2009, 284, 5056–5066. [Google Scholar] [CrossRef] [PubMed]
- Ebert, K.; Witt, H. Fructose Malabsorption. Mol. Cell Pediatr. 2016, 3, 10. [Google Scholar] [CrossRef]
- Gasbarrini, A.; Corazza, G.R.; Gasbarrini, G.; Montalto, M.; Di Stefano, M.; Basilisco, G.; Parodi, A.; Usai-Satta, P.; Vernia, P.; Anania, C.; et al. Methodology and Indications of H2-Breath Testing in Gastrointestinal Diseases: The Rome Consensus Conference. Aliment. Pharmacol. Ther. 2009, 29 (Suppl. 1), 1–49. [Google Scholar] [CrossRef]
- Doma, S.; Gaddipati, K.; Fernandez, A.; Friedenberg, F.; Bromer, M.; Parkman, H. Results of The Fructose Breath Test in Healthy Controls Using Different Doses of Fructose: Which Dose Is Best? Am. J. Gastroenterol. 2003, 98, S265–S266. [Google Scholar] [CrossRef]
- Jones, H.F.; Butler, R.N.; Moore, D.J.; Brooks, D.A. Developmental Changes and Fructose Absorption in Children: Effect on Malabsorption Testing and Dietary Management. Nutr. Rev. 2013, 71, 300–309. [Google Scholar] [CrossRef]
- Mishkin, D.; Sablauskas, L.; Yalovsky, M.; Mishkin, S. Fructose and Sorbitol Malabsorption in Ambulatory Patients with Functional Dyspepsia: Comparison with Lactose Maldigestion/Malabsorption. Dig. Dis. Sci. 1997, 42, 2591–2598. [Google Scholar] [CrossRef]
- Rumessen, J.J.; Gudmand-Høyer, E. Functional Bowel Disease: Malabsorption and Abdominal Distress after Ingestion of Fructose, Sorbitol, and Fructose-Sorbitol Mixtures. Gastroenterology 1988, 95, 694–700. [Google Scholar] [CrossRef]
- Choi, Y.K.; Johlin, F.C.; Summers, R.W.; Jackson, M.; Rao, S.S.C. Fructose Intolerance: An Under-Recognized Problem. Am. J. Gastroenterol. 2003, 98, 1348–1353. [Google Scholar] [CrossRef] [PubMed]
- Barrett, J.S.; Irving, P.M.; Shepherd, S.J.; Muir, J.G.; Gibson, P.R. Comparison of the Prevalence of Fructose and Lactose Malabsorption across Chronic Intestinal Disorders. Aliment. Pharmacol. Ther. 2009, 30, 165–174. [Google Scholar] [CrossRef]
- García-Herrera, J.; Abad, B.; Rodríguez-Yoldi, M.J. Effect of Lipopolysaccharide on D-Fructose Transport across Rabbit Jejunum. Inflamm. Res. 2003, 52, 177–184. [Google Scholar] [CrossRef] [PubMed]
- García-Herrera, J.; Navarro, M.A.; Marca, M.C.; de la Osada, J.; Rodríguez-Yoldi, M.J. The Effect of Tumor Necrosis Factor-α on d-Fructose Intestinal Transport in Rabbits. Cytokine 2004, 25, 21–30. [Google Scholar] [CrossRef] [PubMed]
- Helwig, U.; Koch, A.K.; Reichel, C.; Jessen, P.; Büning, J.; Schreiber, S.; Langhorst, J. A Prospective Multicenter Study on the Prevalence of Fructose Malabsorption in Patients with Chronic Inflammatory Bowel Disease. Digestion 2021, 102, 397–403. [Google Scholar] [CrossRef]
- Tiligada, E.; Ennis, M. Histamine Pharmacology: From Sir Henry Dale to the 21st Century. Br. J. Pharmacol. 2020, 177, 469–489. [Google Scholar] [CrossRef]
- Holeček, M. Histidine in Health and Disease: Metabolism, Physiological Importance, and Use as a Supplement. Nutrients 2020, 12, 848. [Google Scholar] [CrossRef]
- Kofla-Dłubacz, A.; Pytrus, T.; Akutko, K.; Sputa-Grzegrzółka, P.; Piotrowska, A.; Dzięgiel, P. Etiology of IBD—Is. It Still a Mystery? Int. J. Mol. Sci. 2022, 23, 12445. [Google Scholar] [CrossRef]
- Hirasawa, N. Expression of Histidine Decarboxylase and Its Roles in Inflammation. Int. J. Mol. Sci. 2019, 20, 376. [Google Scholar] [CrossRef]
- Huang, H.; Li, Y.; Liang, J.; Finkelman, F.D. Molecular Regulation of Histamine Synthesis. Front. Immunol. 2018, 9, 1392. [Google Scholar] [CrossRef]
- Lieberman, P. The Basics of Histamine Biology. Ann. Allergy Asthma Immunol. 2011, 106, S2–S5. [Google Scholar] [CrossRef] [PubMed]
- Borriello, F.; Iannone, R.; Marone, G. Histamine Release from Mast Cells and Basophils. In Handbook of Experimental Pharmacology; Springer: Cham, Switzerland, 2017; Volume 241, pp. 121–139. [Google Scholar] [CrossRef]
- Mirzahosseini, A.; Dalmadi, B.; Csutora, P. Histamine Receptor H4 Regulates Mast Cell Degranulation and IgE Induced FcεRI Upregulation in Murine Bone Marrow-Derived Mast Cells. Cell Immunol. 2013, 283, 38–44. [Google Scholar] [CrossRef] [PubMed]
- Elmore, B.O.; Bollinger, J.A.; Dooley, D.M. Human Kidney Diamine Oxidase: Heterologous Expression, Purification, and Characterization. J. Biol. Inorg. Chem. 2002, 7, 565–579. [Google Scholar] [CrossRef] [PubMed]
- Zhang, W.; Zhou, H.-H.; Liu, Z.-Q.; Chen, X.-P.; He, Y.-J. Pharmacogenomics in China. In Handbook of Pharmacogenomics and Stratified Medicine; Padmanabhan, Ed.; Elsevier: Amsterdam, The Netherlands, 2014; pp. 999–1013. [Google Scholar]
- Barcik, W.; Wawrzyniak, M.; Akdis, C.A.; O’Mahony, L. Immune Regulation by Histamine and Histamine-Secreting Bacteria. Curr. Opin. Immunol. 2017, 48, 108–113. [Google Scholar] [CrossRef] [PubMed]
- Smolinska, S.; Jutel, M.; Crameri, R.; O’Mahony, L. Histamine and Gut Mucosal Immune Regulation. Allergy 2014, 69, 273–281. [Google Scholar] [CrossRef] [PubMed]
- Gagic, M.; Jamroz, E.; Krizkova, S.; Milosavljevic, V.; Kopel, P.; Adam, V. Current Trends in Detection of Histamine in Food and Beverages. J. Agric. Food Chem. 2019, 67, 773–783. [Google Scholar] [CrossRef]
- Zhao, Y.; Zhang, X.; Jin, H.; Chen, L.; Ji, J.; Zhang, Z. Histamine Intolerance—A Kind of Pseudoallergic Reaction. Biomolecules 2022, 12, 454. [Google Scholar] [CrossRef]
- Thomas, C.M.; Hong, T.; van Pijkeren, J.P.; Hemarajata, P.; Trinh, D.V.; Hu, W.; Britton, R.A.; Kalkum, M.; Versalovic, J. Histamine Derived from Probiotic Lactobacillus Reuteri Suppresses TNF via Modulation of PKA and ERK Signaling. PLoS ONE 2012, 7, e31951. [Google Scholar] [CrossRef]
- Schnedl, W.J.; Enko, D. Histamine Intolerance Originates in the Gut. Nutrients 2021, 13, 1262. [Google Scholar] [CrossRef]
- Comas-Basté, O.; Sánchez-Pérez, S.; Veciana-Nogués, M.T.; Latorre-Moratalla, M.; Vidal-Carou, M. del C. Histamine Intolerance: The Current State of the Art. Biomolecules 2020, 10, 1181. [Google Scholar] [CrossRef] [PubMed]
- Sander, L.E. Selective Expression of Histamine Receptors H1R, H2R, and H4R, but Not H3R, in the Human Intestinal Tract. Gut 2006, 55, 498–504. [Google Scholar] [CrossRef] [PubMed]
- Jutel, M.; Blaser, K.; Akdis, C.A. The Role of Histamine in Regulation of Immune Responses. In Allergy and Asthma in Modern Society: A Scientific Approach; KARGER: Basel, Switzerland, 2006; pp. 174–187. [Google Scholar]
- Beermann, S.; Bernhardt, G.; Seifert, R.; Buschauer, A.; Neumann, D. Histamine H1- and H4-Receptor Signaling Cooperatively Regulate MAPK Activation. Biochem. Pharmacol. 2015, 98, 432–439. [Google Scholar] [CrossRef] [PubMed]
- Shah, R.; Richardson, P.; Yu, H.; Kramer, J.; Hou, J.K. Gastric Acid Suppression Is Associated with an Increased Risk of Adverse Outcomes in Inflammatory Bowel Disease. Digestion 2017, 95, 188–193. [Google Scholar] [CrossRef]
- D’sa, F.F.; Fernandes, E.Z.; Kesarkar, S.V.; Swaminathan, L.; Kunhikatta, V.; Rashid, M.; Thunga, G.; Chandran, V.P.; Nair, S. Use of Histamine-2 Receptor Antagonists and Risk of Inflammatory Bowel Diseases: A Systematic Review and Meta-analysis of Observational Studies. J. Clin. Pharm. Ther. 2022, 47, 1103–1111. [Google Scholar] [CrossRef]
- Smolinska, S.; Groeger, D.; Perez, N.R.; Schiavi, E.; Ferstl, R.; Frei, R.; Konieczna, P.; Akdis, C.A.; Jutel, M.; O’Mahony, L. Histamine Receptor 2 Is Required to Suppress Innate Immune Responses to Bacterial Ligands in Patients with Inflammatory Bowel Disease. Inflamm. Bowel Dis. 2016, 22, 1575–1586. [Google Scholar] [CrossRef]
- Schirmer, B.; Neumann, D. The Function of the Histamine H4 Receptor in Inflammatory and Inflammation-Associated Diseases of the Gut. Int. J. Mol. Sci. 2021, 22, 6116. [Google Scholar] [CrossRef]
- Dvorak, A.M.; Monahan, R.A.; Osage, J.E.; Dickersin, G.R. Crohn’s Disease: Transmission Electron Microscopic Studies. Hum. Pathol. 1980, 11, 606–619. [Google Scholar] [CrossRef]
- Levo, Y.; Livni, N. Mast-Cell Degranulation in Crohn’s Disease. Lancet 1978, 311, 1262. [Google Scholar] [CrossRef]
- Balázs, M.; Illyés, G.; Vadász, G. Mast Cells in Ulcerative Colitis. Virchows Arch. B Cell Pathol. Incl. Mol. Pathol. 1989, 57, 353–360. [Google Scholar] [CrossRef] [PubMed]
- Nolte, H.; Spjeldnaes, N.; Kruse, A.; Windelborg, B. Histamine Release from Gut Mast Cells from Patients with Inflammatory Bowel Diseases. Gut 1990, 31, 791–794. [Google Scholar] [CrossRef] [PubMed]
- Fox, C.C.; Lichtenstein, L.M.; Roche, J.K. Intestinal Mast Cell Responses in Idiopathic Inflammatory Bowel Disease. Dig. Dis. Sci. 1993, 38, 1105–1112. [Google Scholar] [CrossRef] [PubMed]
- Gelbmann, C.M.; Mestermann, S.; Gross, V.; Köllinger, M.; Schölmerich, J.; Falk, W. Strictures in Crohn’s Disease Are Characterised by an Accumulation of Mast Cells Colocalised with Laminin but Not with Fibronectin or Vitronectin. Gut 1999, 45, 210–217. [Google Scholar] [CrossRef] [PubMed]
- He, S.-H. Key Role of Mast Cells and Their Major Secretory Products in Inflammatory Bowel Disease. World J. Gastroenterol. 2004, 10, 309. [Google Scholar] [CrossRef] [PubMed]
- Araki, Y.; Andoh, A.; Fujiyama, Y.; Bamba, T. Development of Dextran Sulphate Sodium-Induced Experimental Colitis Is Suppressed in Genetically Mast Cell-Deficient Ws/Ws Rats. Clin. Exp. Immunol. 2001, 119, 264–269. [Google Scholar] [CrossRef]
- Zhao, P.; Dong, L.; Luo, J.; Guan, H.; Ma, H.; Wang, X. Possible Role of Mast Cells and Neuropeptides in the Recovery Process of Dextran Sulfate Sodium-Induced Colitis in Rats. Chin. Med. Sci. J. 2013, 28, 28–33. [Google Scholar] [CrossRef]
- Winterkamp, S.; Weidenhiller, M.; Otte, P.; Stolper, J.; Schwab, D.; Hahn, E.G.; Raithel, M. Urinary Excretion of N-Methylhistamine as a Marker of Disease Activity in Inflammatory Bowel Disease. Am. J. Gastroenterol. 2002, 97, 3071–3077. [Google Scholar] [CrossRef]
- Petersen, J.; Raithel, M.; Schwelberger, H.G. Characterisation of Functional Polymorphisms of the Human Diamine Oxidase Gene. Inflamm. Res. 2005, 54, S58–S59. [Google Scholar] [CrossRef]
- Petersen, J.; Raithel, M.; Schwelberger, H.G. Analysis of Diamine Oxidase Gene Polymorphisms in Patients with Inflammatory Bowel Disease. Inflamm. Res. 2001, 50, 68–69. [Google Scholar] [CrossRef] [PubMed]
- Petersen, J.; Raithel, M.; Schwelberger, H.G. Histamine N-Methyltransferase and Diamine Oxidase Gene Polymorphisms in Patients with Inflammatory and Neoplastic Intestinal Diseases. Inflamm. Res. 2002, 51, 91–92. [Google Scholar] [CrossRef]
- García-Martín, E. Severity of Ulcerative Colitis Is Associated with a Polymorphism at Diamine Oxidase Gene but Not at Histamine N-Methyltransferase Gene. World J. Gastroenterol. 2006, 12, 615. [Google Scholar] [CrossRef] [PubMed]
- Honzawa, Y.; Nakase, H.; Matsuura, M.; Chiba, T. Clinical Significance of Serum Diamine Oxidase Activity in Inflammatory Bowel Disease. Inflamm. Bowel Dis. 2011, 17, E23–E25. [Google Scholar] [CrossRef]
- Limketkai, B.N.; Sepulveda, R.; Hing, T.; Shah, N.D.; Choe, M.; Limsui, D.; Shah, S. Prevalence and Factors Associated with Gluten Sensitivity in Inflammatory Bowel Disease. Scand. J. Gastroenterol. 2018, 53, 147–151. [Google Scholar] [CrossRef]
- Catassi, C.; Elli, L.; Bonaz, B.; Bouma, G.; Carroccio, A.; Castillejo, G.; Cellier, C.; Cristofori, F.; de Magistris, L.; Dolinsek, J.; et al. Diagnosis of Non-Celiac Gluten Sensitivity (NCGS): The Salerno Experts’ Criteria. Nutrients 2015, 7, 4966–4977. [Google Scholar] [CrossRef]
- Aziz, I.; Branchi, F.; Pearson, K.; Priest, J.; Sanders, D.S. A Study Evaluating the Bidirectional Relationship Between Inflammatory Bowel Disease and Self-Reported Non-Celiac Gluten Sensitivity. Inflamm. Bowel Dis. 2015, 21, 847–853. [Google Scholar] [CrossRef] [PubMed]
- Biesiekierski, J.R.; Newnham, E.D.; Irving, P.M.; Barrett, J.S.; Haines, M.; Doecke, J.D.; Shepherd, S.J.; Muir, J.G.; Gibson, P.R. Gluten Causes Gastrointestinal Symptoms in Subjects Without Celiac Disease: A Double-Blind Randomized Placebo-Controlled Trial. Am. J. Gastroenterol. 2011, 106, 508–514. [Google Scholar] [CrossRef] [PubMed]
- Levine, A.; Sigall Boneh, R.; Wine, E. Evolving Role of Diet in the Pathogenesis and Treatment of Inflammatory Bowel Diseases. Gut 2018, 67, 1726–1738. [Google Scholar] [CrossRef]
- Wagner, S.J.; Schmidt, A.; Effenberger, M.J.P.; Gruber, L.; Danier, J.; Haller, D. Semisynthetic Diet Ameliorates Crohn’s Disease–Like Ileitis in TNFΔARE/WT Mice Through Antigen-Independent Mechanisms of Gluten. Inflamm. Bowel Dis. 2013, 19, 1285–1294. [Google Scholar] [CrossRef]
- Herfarth, H.H.; Martin, C.F.; Sandler, R.S.; Kappelman, M.D.; Long, M.D. Prevalence of a Gluten-Free Diet and Improvement of Clinical Symptoms in Patients with Inflammatory Bowel Diseases. Inflamm. Bowel Dis. 2014, 20, 1194–1197. [Google Scholar] [CrossRef]
- Schreiner, P.; Martinho-Grueber, M.; Studerus, D.; Vavricka, S.R.; Tilg, H.; Biedermann, L. Nutrition in Inflammatory Bowel Disease. Digestion 2020, 101, 120–135. [Google Scholar] [CrossRef]
- Morton, H.; Pedley, K.C.; Stewart, R.J.C.; Coad, J. Inflammatory Bowel Disease: Are Symptoms and Diet Linked? Nutrients 2020, 12, 2975. [Google Scholar] [CrossRef]
- Kotlyar, D.S. Non-Pulmonary Allergic Diseases and Inflammatory Bowel Disease: A Qualitative Review. World J. Gastroenterol. 2014, 20, 11023. [Google Scholar] [CrossRef]
- Van Limbergen, J.; Russell, R.K.; Nimmo, E.R.; Zhao, Y.; Liao, H.; Drummond, H.E.; Davies, G.; Gillett, P.M.; McGrogan, P.; Bisset, W.M.; et al. Filaggrin Loss-of-Function Variants Are Associated with Atopic Comorbidity in Pediatric Inflammatory Bowel Disease. Inflamm. Bowel Dis. 2009, 15, 1492–1498. [Google Scholar] [CrossRef]
- Li, L.-J.; Zeng, L.; Li, X.-X.; Mo, L.-H.; Geng, X.-R.; Zheng, P.-Y.; Liu, Z.-G.; Feng, B.-S.; Yang, P.-C. Induction of Colitis in Mice with Food Allergen-Specific Immune Response. Sci. Rep. 2016, 6, 32765. [Google Scholar] [CrossRef]
- Johnson, E.; Therkelsen, S.P.; Nentwich, I.; Nissen-Meyer, L.S.H.; Hetland, G. IgE-Sensitization to Food and Inhalant Allergens in IBD Patients Compared with Normal Blood Donors at Oslo University Hospital, Norway. Scand. J. Gastroenterol. 2019, 54, 1107–1110. [Google Scholar] [CrossRef]
- Imanzadeh, F.; Nasri, P.; Sadeghi, S.; Sayyari, A.; Dara, N.; Abdollah, K.; Nilipoor, Y.; Mansuri, M.; Khatami, K.; Rouhani, P.; et al. Food Allergy among Iranian Children with Inflammatory Bowel Disease: A Preliminary Report. J. Res. Med. Sci. 2015, 20, 855. [Google Scholar] [CrossRef] [PubMed]
- Buczyńska, A.; Grzybowska-Chlebowczyk, U.; Pawlicki, K. IgE-Dependent Food Sensitisation and Its Role in Clinical and Laboratory Presentation of Paediatric Inflammatory Bowel Disease. Nutrients 2023, 15, 1804. [Google Scholar] [CrossRef]
- Kawaguchi, T.; Mori, M.; Saito, K.; Suga, Y.; Hashimoto, M.; Sako, M.; Yoshimura, N.; Uo, M.; Danjo, K.; Ikenoue, Y.; et al. Food Antigen-Induced Immune Responses in Crohn’s Disease Patients and Experimental Colitis Mice. J. Gastroenterol. 2015, 50, 394–405. [Google Scholar] [CrossRef] [PubMed]
- Xiao, N.; Liu, F.; Zhou, G.; Sun, M.; Ai, F.; Liu, Z. Food-Specific IgGs Are Highly Increased in the Sera of Patients with Inflammatory Bowel Disease and Are Clinically Relevant to the Pathogenesis. Intern. Med. 2018, 57, 2787–2798. [Google Scholar] [CrossRef] [PubMed]
- Cai, C.; Shen, J.; Zhao, D.; Qiao, Y.; Xu, A.; Jin, S.; Ran, Z.; Zheng, Q. Serological Investigation of Food Specific Immunoglobulin G Antibodies in Patients with Inflammatory Bowel Diseases. PLoS ONE 2014, 9, e112154. [Google Scholar] [CrossRef] [PubMed]
- Dincer, D.; Ulukal Karanci, E.; Akin, M.; Adanir, H. NSAID, Antiaggregant, and/or Anticoagulant-Related Upper Gastrointestinal Bleeding: Is There Any Change in Prophylaxis Rate after a 10-Year Period? Turk. J. Gastroenterol. 2019, 30, 505–510. [Google Scholar] [CrossRef] [PubMed]
- Jansen, A.; Mandić, A.D.; Bennek, E.; Frehn, L.; Verdier, J.; Tebrügge, I.; Lutz, H.; Streetz, K.; Trautwein, C.; Sellge, G. Anti-Food and Anti-Microbial IgG Subclass Antibodies in Inflammatory Bowel Disease. Scand. J. Gastroenterol. 2016, 51, 1453–1461. [Google Scholar] [CrossRef] [PubMed]
- Zilbauer, M.; James, K.R.; Kaur, M.; Pott, S.; Li, Z.; Burger, A.; Thiagarajah, J.R.; Burclaff, J.; Jahnsen, F.L.; Perrone, F.; et al. A Roadmap for the Human Gut Cell Atlas. Nat. Rev. Gastroenterol. Hepatol. 2023, 20, 597–614. [Google Scholar] [CrossRef] [PubMed]
- Vestergaard, M.V.; Allin, K.H.; Eriksen, C.; Zakerska-Banaszak, O.; Arasaradnam, R.P.; Alam, M.T.; Kristiansen, K.; Brix, S.; Jess, T. Gut Microbiota Signatures in Inflammatory Bowel Disease. United Eur. Gastroenterol. J. 2023. [Google Scholar] [CrossRef] [PubMed]
- Ahlström, M.G.; Thyssen, J.P.; Wennervaldt, M.; Menné, T.; Johansen, J.D. Nickel Allergy and Allergic Contact Dermatitis: A Clinical Review of Immunology, Epidemiology, Exposure, and Treatment. Contact Dermat. 2019, 81, 227–241. [Google Scholar] [CrossRef] [PubMed]
- Thyssen, J.P.; Menné, T.; Johansen, J.D. Nickel Release from Inexpensive Jewelry and Hair Clasps Purchased in an EU Country—Are Consumers Sufficiently Protected from Nickel Exposure? Sci. Total Environ. 2009, 407, 5315–5318. [Google Scholar] [CrossRef] [PubMed]
- Thyssen, J.P.; Menné, T.; Lidén, C.; White, I.R.; White, J.; Spiewak, R.; Johansen, J.D. Excessive Nickel Release from Earrings Purchased from Independent Shops and Street Markets—A Field Study from Warsaw and London. J. Eur. Acad. Dermatol. Venereol. 2011, 25, 1021–1026. [Google Scholar] [CrossRef]
- Jensen, P.; Hamann, D.; Hamann, C.R.; Jellesen, M.S.; Jacob, S.E.; Thyssen, J.P. Nickel and Cobalt Release From Children’s Toys Purchased in Denmark and the United States. Dermatitis 2014, 25, 356–365. [Google Scholar] [CrossRef]
- Aquino, M.; Rosner, G. Systemic Contact Dermatitis. Clin. Rev. Allergy Immunol. 2019, 56, 9–18. [Google Scholar] [CrossRef]
- Tramontana, M.; Bianchi, L.; Hansel, K.; Agostinelli, D.; Stingeni, L. Nickel Allergy: Epidemiology, Pathomechanism, Clinical Patterns, Treatment and Prevention Programs. Endocr. Metab. Immune Disord. Drug Targets 2020, 20, 992–1002. [Google Scholar] [CrossRef] [PubMed]
- Martin, S.F. New Concepts in Cutaneous Allergy. Contact Dermat. 2015, 72, 2–10. [Google Scholar] [CrossRef] [PubMed]
- Kaplan, D.H.; Igyártó, B.Z.; Gaspari, A.A. Early Immune Events in the Induction of Allergic Contact Dermatitis. Nat. Rev. Immunol. 2012, 12, 114–124. [Google Scholar] [CrossRef]
- Cavani, A.; Nasorri, F.; Prezzi, C.; Sebastiani, S.; Albanesi, C.; Girolomoni, G. Human CD4+ T Lymphocytes with Remarkable Regulatory Functions on Dendritic Cells and Nickel-Specific Th1 Immune Responses. J. Investig. Dermatol. 2000, 114, 295–302. [Google Scholar] [CrossRef] [PubMed]
- Jensen, C.S.; Menné, T.; Lisby, S.; Kristiansen, J.; Veien, N.K. Experimental Systemic Contact Dermatitis from Nickel: A Dose–Response Study. Contact Dermat. 2003, 49, 124–132. [Google Scholar] [CrossRef] [PubMed]
- Guo, H.; Liu, H.; Jian, Z.; Cui, H.; Fang, J.; Zuo, Z.; Deng, J.; Li, Y.; Wang, X.; Zhao, L.; et al. Nickel Induces Inflammatory Activation via NF-ΚB, MAPKs, IRF3 and NLRP3 Inflammasome Signaling Pathways in Macrophages. Aging 2019, 11, 11659–11672. [Google Scholar] [CrossRef] [PubMed]
- Schöfer, H.; Rosenberger, G.; Hottenrott, C.; Strohm, W.D.; Burmester, H.J.; Gonnermann, B.; Hensel, O. Sensitization to Nickel Sulfate in Patients with Ileitis Terminalis (Crohn Disease). Derm. Beruf Umw. 1988, 36, 157–162. [Google Scholar]
- Kageyama, Y.; Shimokawa, Y.; Kawauchi, K.; Morimoto, M.; Aida, K.; Akiyama, T.; Nakamura, T. Higher Prevalence of Nickel and Palladium Hypersensitivity in Patients with Ulcerative Colitis. Int. Arch. Allergy Immunol. 2020, 181, 456–461. [Google Scholar] [CrossRef]
- Ogasawara, H.; Hayasaka, M.; Maemoto, A.; Furukawa, S.; Ito, T.; Kimura, O.; Endo, T. Levels of Major and Trace Metals in the Scalp Hair of Crohn’s Disease Patients: Correlations among Transition Metals. BioMetals 2021, 34, 197–210. [Google Scholar] [CrossRef]
- Matsuda, H.; Nibe-Shirakihara, Y.; Tamura, A.; Aonuma, E.; Arakawa, S.; Otsubo, K.; Nemoto, Y.; Nagaishi, T.; Tsuchiya, K.; Shimizu, S.; et al. Nickel Particles Are Present in Crohn’s Disease Tissue and Exacerbate Intestinal Inflammation in IBD Susceptible Mice. Biochem. Biophys. Res. Commun. 2022, 592, 74–80. [Google Scholar] [CrossRef]
- Rizzi, A.; Nucera, E.; Laterza, L.; Gaetani, E.; Valenza, V.; Corbo, G.M.; Inchingolo, R.; Buonomo, A.; Schiavino, D.; Gasbarrini, A. Irritable Bowel Syndrome and Nickel Allergy: What Is the Role of the Low Nickel Diet? J. Neurogastroenterol. Motil. 2017, 23, 101–108. [Google Scholar] [CrossRef] [PubMed]
- Roach, K.; Roberts, J. A Comprehensive Summary of Disease Variants Implicated in Metal Allergy. J. Toxicol. Environ. Health Part B 2022, 25, 279–341. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Condition | Mechanism | Common Causative Foods or Substances | References | |
|---|---|---|---|---|
| Food allergy | Reactions mediated by the immune system | Milk, eggs, peanuts, fish, shellfish, plant-based food | [9] | |
| Food intolerance | Enzyme deficiency | Inability to metabolize determined substances present in food | Lactose, fructose, trehalose, sucrose, sorbitol | [13,14] |
| Pharmacological intolerance | Direct: caused by chemical substances naturally present in food Indirect: caused by the release of mediators from cells induced by certain foods | Foods rich in histamine (fermented cheeses, salami, oily fish, spinach, tomatoes), methylxanthines (coffee, chocolate, tea, cola), phenylethylamine (cheese, red wine), tyramine (potatoes, cabbage, tuna) | [13,14] | |
| Indefinite intolerance | Exact mechanism unknown | Food additives (preservatives, dyes, sweeteners, antioxidants), processed foods (canned meat products, syrups, fruit juices) | [13,14] |
| Condition | Mechanism | Available Data | References |
|---|---|---|---|
| Lactose intolerance | Damage to the small bowel mucosa with consequent lactase deficiency and lactose malabsorption | Humans | [17,18,28,29] |
| Fructose intolerance | Inflammation may lead to downregulation of the primary intestinal fructose transporter (GLUT5 receptor) | Rabbits | [57,58] |
| Histamine intolerance | SNP associated with altered function of enzymes involved in histamine metabolism and reduced DAO activity may lead to HIT | Humans | [97,98] |
| Non-celiac gluten sensitivity | Fermentable carbohydrates in gluten-containing foods may result in increased intraluminal gas leading to increased gastrointestinal symptoms in IBD patients with stenosing disease | Humans | [99,101] |
| Nickel allergy | Altered macrophage autophagy mechanisms may lead to accumulation of nickel particles able to worsen colitis | THP-1 cells, murine models | [135] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Capobianco, I.; Di Vincenzo, F.; Puca, P.; Becherucci, G.; Mentella, M.C.; Petito, V.; Scaldaferri, F. Adverse Food Reactions in Inflammatory Bowel Disease: State of the Art and Future Perspectives. Nutrients 2024, 16, 351. https://doi.org/10.3390/nu16030351
Capobianco I, Di Vincenzo F, Puca P, Becherucci G, Mentella MC, Petito V, Scaldaferri F. Adverse Food Reactions in Inflammatory Bowel Disease: State of the Art and Future Perspectives. Nutrients. 2024; 16(3):351. https://doi.org/10.3390/nu16030351
Chicago/Turabian StyleCapobianco, Ivan, Federica Di Vincenzo, Pierluigi Puca, Guia Becherucci, Maria Chiara Mentella, Valentina Petito, and Franco Scaldaferri. 2024. "Adverse Food Reactions in Inflammatory Bowel Disease: State of the Art and Future Perspectives" Nutrients 16, no. 3: 351. https://doi.org/10.3390/nu16030351