
Changes in Lean Tissue Mass, Fat Mass, Biological Parameters and Resting Energy Expenditure over 24 Months Following Sleeve Gastrectomy

 , , , , , ,
, , , , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Subjects and Method
2.1.1. Subjects
2.1.2. Methods
2.1.3. Comorbidity Definitions
2.1.4. Regional and Whole Body FM and LTM
2.1.5. Assays
2.1.6. Resting Energy Expenditure (REE)
2.1.7. Statistical Analysis
3. Results
3.1. Anthropometric Parameters
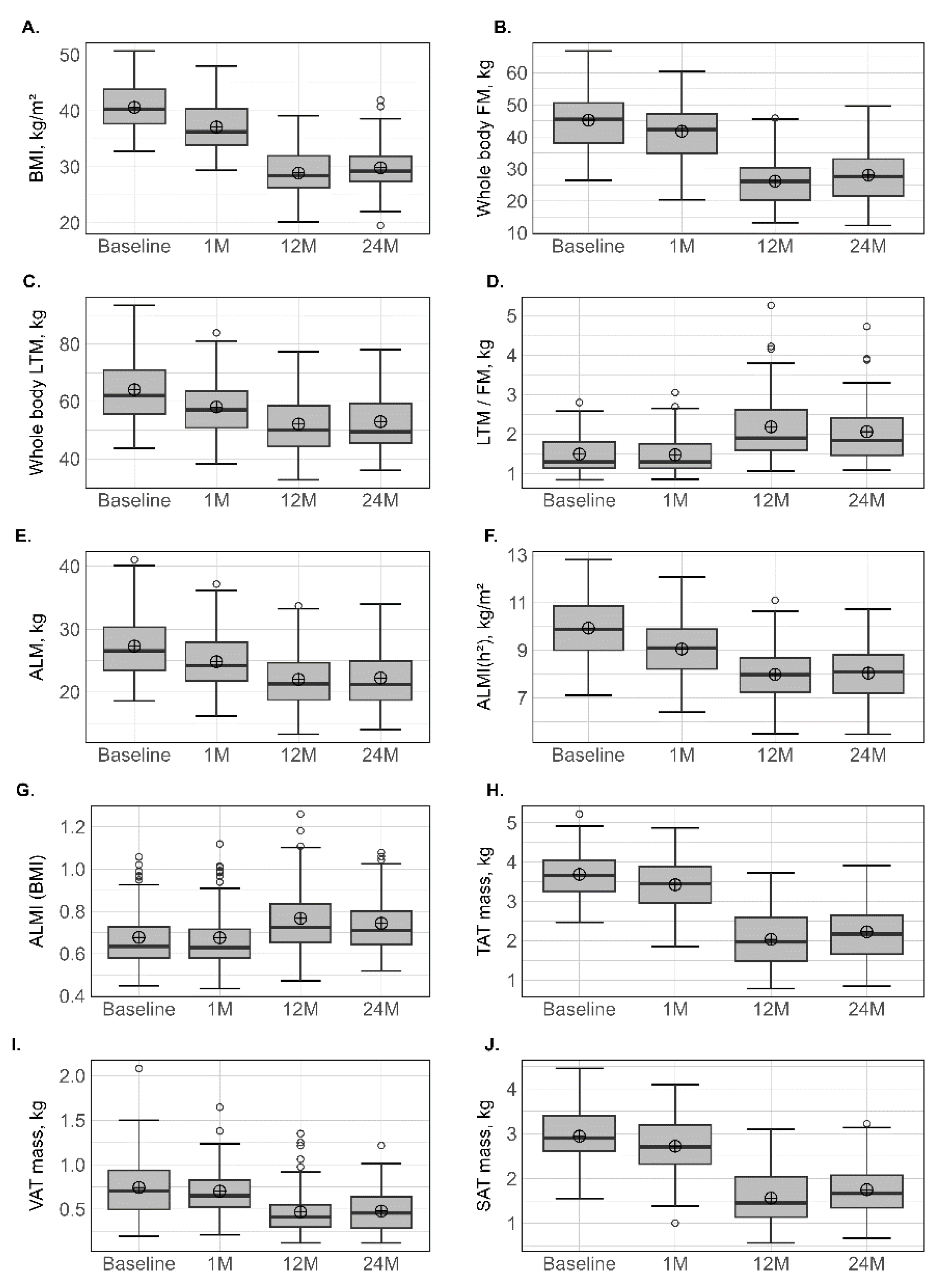
3.2. Body Composition
3.3. Sarcopenia Prevalence
3.4. Android, Gynoid and Abdominal Body Composition
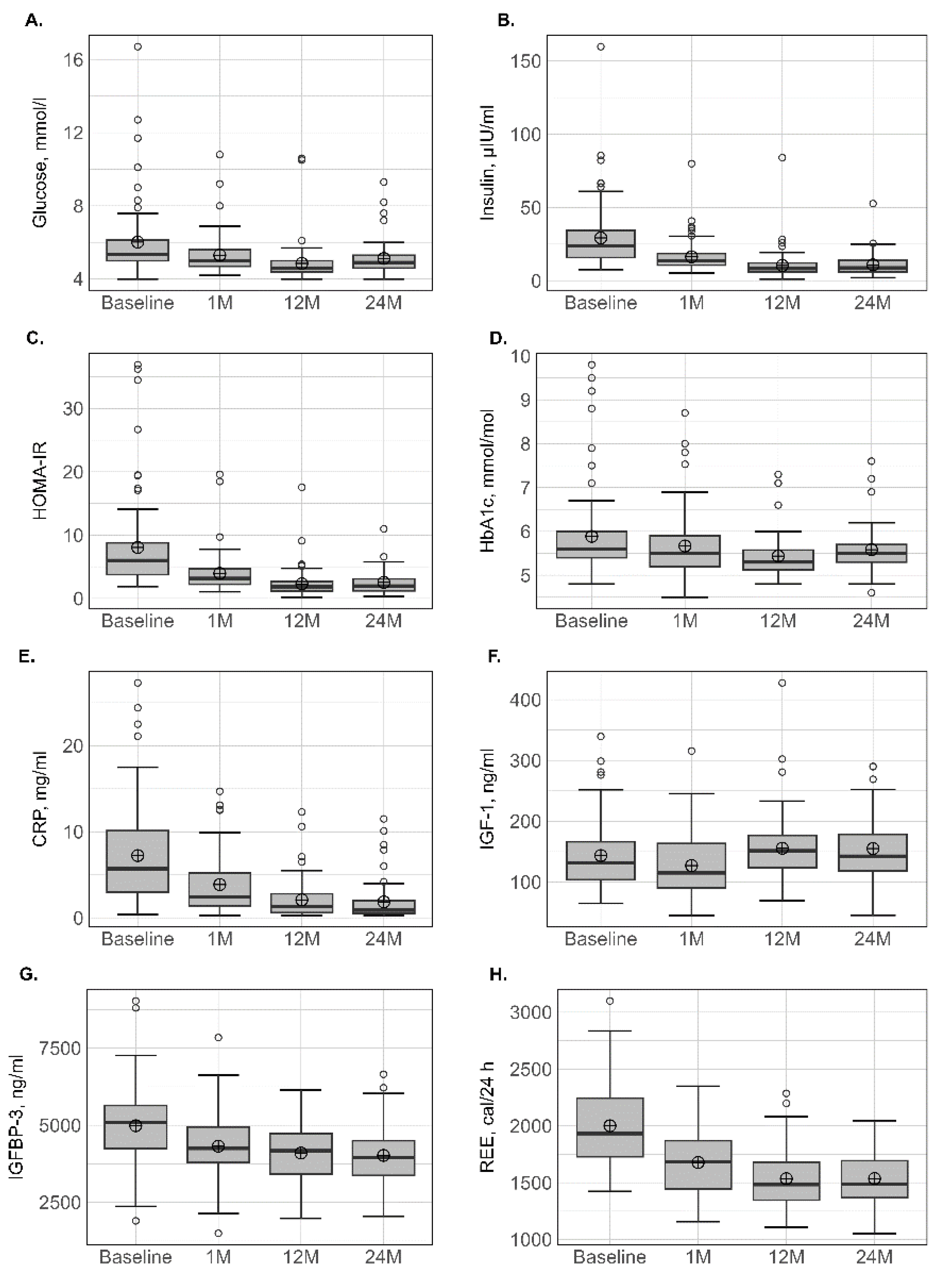
3.5. Biological Parameters
3.6. Correlations between Basal Parameters and Body Composition Change
4. Discussion
5. Limitations and Strength
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Jensen, M.D.; Ryan, D.H.; Apovian, C.M.; Ard, J.D.; Comuzzie, A.G.; Donato, K.A.; Hu, F.B.; Hubbard, V.S.; Jakicic, J.M.; Kushner, R.F.; et al. 2013 AHA/ACC/TOS guideline for the management of overweight and obesity in adults: A report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines and the Obesity Society. J. Am. Coll. Cardiol. 2013, 63, 2985–3023. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Albanopoulos, K.; Tsamis, D.; Natoudi, M.; Alevizos, L.; Zografos, G.; Leandros, E. The impact of laparoscopic sleeve gastrectomy on weight loss and obesity-associated comorbidities: The results of 3 years of follow-up. Surg. Endosc. 2016, 30, 699–705. [Google Scholar] [CrossRef] [PubMed]
- Beamish, A.J.; Olbers, T.; Kelly, A.S.; Inge, T.H. Cardiovascular effects of bariatric surgery. Nat. Rev. Cardiol. 2016, 13, 730–743. [Google Scholar] [CrossRef] [PubMed]
- Kennedy-Dalby, A.; Adam, S.; Ammori, B.J.; Syed, A.A. Weight loss and metabolic outcomes of bariatric surgery in men versus women—A matched comparative observational cohort study. Eur. J. Intern. Med. 2014, 25, 922–925. [Google Scholar] [CrossRef]
- Voorwinde, V.; Steenhuis, I.H.M.; Janssen, I.M.C.; Monpellier, V.M.; van Stralen, M.M. Definitions of Long-Term Weight Regain and Their Associations with Clinical Outcomes. Obes. Surg. 2020, 30, 527–536. [Google Scholar] [CrossRef] [Green Version]
- Frisard, M.I.; Greenway, F.L.; Delany, J.P. Comparison of methods to assess body composition changes during a period of weight loss. Obes. Res. 2005, 13, 845–854. [Google Scholar] [CrossRef] [Green Version]
- Schiavo, L.; Pilone, V.; Tramontano, S.; Rossetti, G.; Iannelli, A. May Bioelectrical Impedance Analysis Method Be Used in Alternative to the Dual-Energy X-Ray Absorptiometry in the Assessment of Fat Mass and Fat-Free Mass in Patients with Obesity? Pros, Cons, and Perspectives. Obes. Surg. 2020, 30, 3212–3215. [Google Scholar] [CrossRef]
- Johnson Stoklossa, C.A.; Forhan, M.; Padwal, R.S.; Gonzalez, M.C.; Prado, C.M. Practical Considerations for Body Composition Assessment of Adults with Class II/III Obesity Using Bioelectrical Impedance Analysis or Dual-Energy X-Ray Absorptiometry. Curr. Obes. Rep. 2016, 5, 389–396. [Google Scholar] [CrossRef]
- Shepherd, J.A.; Baim, S.; Bilezikian, J.P.; Schousboe, J.T. Executive summary of the 2013 International Society for Clinical Densitometry Position Development Conference on Body Composition. J. Clin. Densitom. 2013, 16, 489–495. [Google Scholar] [CrossRef]
- Maimoun, L.; Lefebvre, P.; Aouinti, S.; Picot, M.C.; Mariano-Goulart, D.; Nocca, D.; Montpellier Study Group of Bariatric, S. Acute and longer-term body composition changes after bariatric surgery. Surg. Obes. Relat. Dis. 2019, 15, 1965–1973. [Google Scholar] [CrossRef]
- Maimoun, L.; Lefebvre, P.; Jaussent, A.; Fouillade, C.; Mariano-Goulart, D.; Nocca, D. Body composition changes in the first month after sleeve gastrectomy based on gender and anatomic site. Surg. Obes. Relat. Dis. 2017, 13, 780–787. [Google Scholar] [CrossRef]
- Sivakumar, J.; Chen, Q.; Sutherland, T.R.; Read, M.; Ward, S.; Chong, L.; Hii, M.W. Body Composition Differences Between Excess Weight Loss ≥ 50% and < 50% at 12 Months Following Bariatric Surgery. Obes. Surg. 2022, 32, 2556–2566. [Google Scholar] [CrossRef]
- Haghighat, N.; Ashtary-Larky, D.; Bagheri, R.; Aghakhani, L.; Asbaghi, O.; Amini, M.; Moeinvaziri, N.; Hosseini, B.; Wong, A.; Shamekhi, Z.; et al. Preservation of fat-free mass in the first year after bariatric surgery: A systematic review and meta-analysis of 122 studies and 10,758 participants. Surg. Obes. Relat. Dis. 2022, 18, 964–982. [Google Scholar] [CrossRef]
- Barzin, M.; Heidari Almasi, M.; Mahdavi, M.; Khalaj, A.; Valizadeh, M.; Hosseinpanah, F. Body Composition Changes Following Sleeve Gastrectomy Vs. One-Anastomosis Gastric Bypass: Tehran Obesity Treatment Study (TOTS). Obes. Surg. 2021, 31, 5286–5294. [Google Scholar] [CrossRef]
- Sherf-Dagan, S.; Zelber-Sagi, S.; Buch, A.; Bar, N.; Webb, M.; Sakran, N.; Raziel, A.; Goitein, D.; Keidar, A.; Shibolet, O. Prospective Longitudinal Trends in Body Composition and Clinical Outcomes 3 Years Following Sleeve Gastrectomy. Obes. Surg. 2019, 29, 3833–3841. [Google Scholar] [CrossRef]
- Gomez-Ambrosi, J.; Andrada, P.; Valenti, V.; Rotellar, F.; Silva, C.; Catalan, V.; Rodriguez, A.; Ramirez, B.; Moncada, R.; Escalada, J.; et al. Dissociation of body mass index, excess weight loss and body fat percentage trajectories after 3 years of gastric bypass: Relationship with metabolic outcomes. Int. J. Obes. 2017, 41, 1379–1387. [Google Scholar] [CrossRef]
- Angrisani, L.; Santonicola, A.; Iovino, P.; Formisano, G.; Buchwald, H.; Scopinaro, N. Bariatric Surgery Worldwide 2013. Obes. Surg. 2015, 25, 1822–1832. [Google Scholar] [CrossRef]
- Shantavasinkul, P.C.; Omotosho, P.; Muehlbauer, M.J.; Natoli, M.; Corsino, L.; Tong, J.; Portenier, D.; Torquati, A. Metabolic profiles, energy expenditures, and body compositions of the weight regain versus sustained weight loss patients who underwent Roux-en-Y gastric bypass. Surg. Obes. Relat. Dis. 2021, 17, 2015–2025. [Google Scholar] [CrossRef]
- Marks, B.L.; Rippe, J.M. The importance of fat free mass maintenance in weight loss programmes. Sport. Med. 1996, 22, 273–281. [Google Scholar] [CrossRef]
- Montague, C.T.; O’Rahilly, S. The perils of portliness: Causes and consequences of visceral adiposity. Diabetes 2000, 49, 883–888. [Google Scholar] [CrossRef] [Green Version]
- Despres, J.P.; Lemieux, I. Abdominal obesity and metabolic syndrome. Nature 2006, 444, 881–887. [Google Scholar] [CrossRef] [PubMed]
- Rao, V.N.; Fudim, M.; Mentz, R.J.; Michos, E.D.; Felker, G.M. Regional adiposity and heart failure with preserved ejection fraction. Eur. J. Heart Fail. 2020, 22, 1540–1550. [Google Scholar] [CrossRef] [PubMed]
- Fontana, L.; Eagon, J.C.; Trujillo, M.E.; Scherer, P.E.; Klein, S. Visceral fat adipokine secretion is associated with systemic inflammation in obese humans. Diabetes 2007, 56, 1010–1013. [Google Scholar] [CrossRef] [Green Version]
- Favre, L.; Marino, L.; Roth, A.; Acierno, J., Jr.; Hans, D.; Demartines, N.; Pitteloud, N.; Suter, M.; Collet, T.H. The Reduction of Visceral Adipose Tissue after Roux-en-Y Gastric Bypass Is more Pronounced in Patients with Impaired Glucose Metabolism. Obes. Surg. 2018, 28, 4006–4013. [Google Scholar] [CrossRef] [Green Version]
- Santini, S.; Vionnet, N.; Pasquier, J.; Suter, M.; Hans, D.; Gonzalez-Rodriguez, E.; Pitteloud, N.; Favre, L. Long-term body composition improvement in post-menopausal women following bariatric surgery: A cross-sectional and case-control study. Eur. J. Endocrinol. 2022, 186, 255–263. [Google Scholar] [CrossRef]
- Ray, K.K.; Colhoun, H.M.; Szarek, M.; Baccara-Dinet, M.; Bhatt, D.L.; Bittner, V.A.; Budaj, A.J.; Diaz, R.; Goodman, S.G.; Hanotin, C.; et al. Effects of alirocumab on cardiovascular and metabolic outcomes after acute coronary syndrome in patients with or without diabetes: A prespecified analysis of the ODYSSEY OUTCOMES randomised controlled trial. Lancet Diabetes Endocrinol. 2019, 7, 618–628. [Google Scholar] [CrossRef] [Green Version]
- Geldsetzer, P.; Manne-Goehler, J.; Marcus, M.E.; Ebert, C.; Zhumadilov, Z.; Wesseh, C.S.; Tsabedze, L.; Supiyev, A.; Sturua, L.; Bahendeka, S.K.; et al. The state of hypertension care in 44 low-income and middle-income countries: A cross-sectional study of nationally representative individual-level data from 1.1 million adults. Lancet 2019, 394, 652–662. [Google Scholar] [CrossRef] [Green Version]
- Katzmarzyk, P.T.; Greenway, F.L.; Heymsfield, S.B.; Bouchard, C. Clinical utility and reproducibility of visceral adipose tissue measurements derived from dual-energy X-ray absorptiometry in White and African American adults. Obesity 2013, 21, 2221–2224. [Google Scholar] [CrossRef]
- Cruz-Jentoft, A.J.; Bahat, G.; Bauer, J.; Boirie, Y.; Bruyere, O.; Cederholm, T.; Cooper, C.; Landi, F.; Rolland, Y.; Sayer, A.A.; et al. Sarcopenia: Revised European consensus on definition and diagnosis. Age Ageing 2019, 48, 601. [Google Scholar] [CrossRef] [Green Version]
- McLean, R.R.; Shardell, M.D.; Alley, D.E.; Cawthon, P.M.; Fragala, M.S.; Harris, T.B.; Kenny, A.M.; Peters, K.W.; Ferrucci, L.; Guralnik, J.M.; et al. Criteria for clinically relevant weakness and low lean mass and their longitudinal association with incident mobility impairment and mortality: The foundation for the National Institutes of Health (FNIH) sarcopenia project. J. Gerontol. A Biol. Sci. Med. Sci. 2014, 69, 576–583. [Google Scholar] [CrossRef]
- Fielding, R.A.; Vellas, B.; Evans, W.J.; Bhasin, S.; Morley, J.E.; Newman, A.B.; Abellan van Kan, G.; Andrieu, S.; Bauer, J.; Breuille, D.; et al. Sarcopenia: An undiagnosed condition in older adults. Current consensus definition: Prevalence, etiology, and consequences. International working group on sarcopenia. J. Am. Med. Dir. Assoc. 2011, 12, 249–256. [Google Scholar] [CrossRef] [Green Version]
- Roza, A.M.; Shizgal, H.M. The Harris Benedict equation reevaluated: Resting energy requirements and the body cell mass. Am. J. Clin. Nutr. 1984, 40, 168–182. [Google Scholar] [CrossRef] [Green Version]
- Buhler, J.; Rast, S.; Beglinger, C.; Peterli, R.; Peters, T.; Gebhart, M.; Meyer-Gerspach, A.C.; Wolnerhanssen, B.K. Long-Term Effects of Laparoscopic Sleeve Gastrectomy and Roux-en-Y Gastric Bypass on Body Composition and Bone Mass Density. Obes. Facts 2021, 14, 131–140. [Google Scholar] [CrossRef]
- Martinez, M.C.; Meli, E.F.; Candia, F.P.; Filippi, F.; Vilallonga, R.; Cordero, E.; Hernandez, I.; Eguinoa, A.Z.; Burgos, R.; Vila, A.; et al. The Impact of Bariatric Surgery on the Muscle Mass in Patients with Obesity: 2-Year Follow-up. Obes. Surg. 2022, 32, 625–633. [Google Scholar] [CrossRef]
- Golzarand, M.; Toolabi, K.; Djafarian, K. Changes in Body Composition, Dietary Intake, and Substrate Oxidation in Patients Underwent Laparoscopic Roux-en-Y Gastric Bypass and Laparoscopic Sleeve Gastrectomy: A Comparative Prospective Study. Obes. Surg. 2019, 29, 406–413. [Google Scholar] [CrossRef]
- Coluzzi, I.; Raparelli, L.; Guarnacci, L.; Paone, E.; Del Genio, G.; le Roux, C.W.; Silecchia, G. Food Intake and Changes in Eating Behavior After Laparoscopic Sleeve Gastrectomy. Obes. Surg. 2016, 26, 2059–2067. [Google Scholar] [CrossRef]
- Harvie, M.N.; Pegington, M.; Mattson, M.P.; Frystyk, J.; Dillon, B.; Evans, G.; Cuzick, J.; Jebb, S.A.; Martin, B.; Cutler, R.G.; et al. The effects of intermittent or continuous energy restriction on weight loss and metabolic disease risk markers: A randomized trial in young overweight women. Int. J. Obes. 2011, 35, 714–727. [Google Scholar] [CrossRef] [Green Version]
- Tam, C.S.; Frost, E.A.; Xie, W.; Rood, J.; Ravussin, E.; Redman, L.M.; Pennington, C.T. No effect of caloric restriction on salivary cortisol levels in overweight men and women. Metabolism 2014, 63, 194–198. [Google Scholar] [CrossRef] [Green Version]
- Juiz-Valina, P.; Pena-Bello, L.; Cordido, M.; Outeirino-Blanco, E.; Pertega, S.; Varela-Rodriguez, B.; Garcia-Brao, M.J.; Mena, E.; Sangiao-Alvarellos, S.; Cordido, F. Altered GH-IGF-1 Axis in Severe Obese Subjects is Reversed after Bariatric Surgery-Induced Weight Loss and Related with Low-Grade Chronic Inflammation. J. Clin. Med. 2020, 9, 2614. [Google Scholar] [CrossRef]
- Kojta, I.; Chacinska, M.; Blachnio-Zabielska, A. Obesity, Bioactive Lipids, and Adipose Tissue Inflammation in Insulin Resistance. Nutrients 2020, 12, 1305. [Google Scholar] [CrossRef]
- Pellitero, S.; Granada, M.L.; Martinez, E.; Balibrea, J.M.; Guanyabens, E.; Serra, A.; Moreno, P.; Navarro, M.; Romero, R.; Alastrue, A.; et al. IGF1 modifications after bariatric surgery in morbidly obese patients: Potential implications of nutritional status according to specific surgical technique. Eur. J. Endocrinol. 2013, 169, 695–703. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ohira, M.; Watanabe, Y.; Yamaguchi, T.; Onda, H.; Yamaoka, S.; Abe, K.; Nakamura, S.; Tanaka, S.; Kawagoe, N.; Nabekura, T.; et al. The Relationship between Serum Insulin-Like Growth Factor-1 Levels and Body Composition Changes after Sleeve Gastrectomy. Obes. Facts 2021, 14, 641–649. [Google Scholar] [CrossRef] [PubMed]
- De Marinis, L.; Bianchi, A.; Mancini, A.; Gentilella, R.; Perrelli, M.; Giampietro, A.; Porcelli, T.; Tilaro, L.; Fusco, A.; Valle, D.; et al. Growth hormone secretion and leptin in morbid obesity before and after biliopancreatic diversion: Relationships with insulin and body composition. J. Clin. Endocrinol. Metab. 2004, 89, 174–180. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maimoun, L.; Serrand, C.; Mura, T.; Renard, E.; Nocca, D.; Lefebvre, P.; Boudousq, V.; Avignon, A.; Mariano-Goulart, D.; Sultan, A. Definition of an adapted cut-off for determining low lean tissue mass in older women with obesity: A comparison to current cut-offs. Sci. Rep. 2022, 12, 16905. [Google Scholar] [CrossRef]
- Ruthes, E.M.P.; Lenardt, B.C.C.; Lass, A.D.; Petroski, C.A.; de Mello, M.F.; de Andrade Junior, A.B.; Souza, C.J.F.; de Matos, O.; Castelo-Branco, C. Lean mass and strength profile of women submitted to bariatric surgery: Comparison of the EWGSOP2 and FNIH classification for sarcopenia—ASBS program phase II. Gynecol. Endocrinol. 2022, 38, 868–873. [Google Scholar] [CrossRef]
- Vassilev, G.; Galata, C.; Finze, A.; Weiss, C.; Otto, M.; Reissfelder, C.; Blank, S. Sarcopenia after Roux-en-Y Gastric Bypass: Detection by Skeletal Muscle Mass Index vs. Bioelectrical Impedance Analysis. J. Clin. Med. 2022, 11, 1468. [Google Scholar] [CrossRef]
- Voican, C.S.; Lebrun, A.; Maitre, S.; Lainas, P.; Lamouri, K.; Njike-Nakseu, M.; Gaillard, M.; Tranchart, H.; Balian, A.; Dagher, I.; et al. Predictive score of sarcopenia occurrence one year after bariatric surgery in severely obese patients. PLoS ONE 2018, 13, e0197248. [Google Scholar] [CrossRef]
- Johnstone, A.M.; Murison, S.D.; Duncan, J.S.; Rance, K.A.; Speakman, J.R. Factors influencing variation in basal metabolic rate include fat-free mass, fat mass, age, and circulating thyroxine but not sex, circulating leptin, or triiodothyronine. Am. J. Clin. Nutr. 2005, 82, 941–948. [Google Scholar] [CrossRef] [Green Version]
- Fidilio, E.; Comas, M.; Giribes, M.; Cardenas, G.; Vilallonga, R.; Palma, F.; Pelaez, R.B.; Simo, R.; Ciudin, A. Evaluation of Resting Energy Expenditure in Subjects with Severe Obesity and Its Evolution after Bariatric Surgery. Obes. Surg. 2021, 31, 4347–4355. [Google Scholar] [CrossRef]
- Moize, V.; Andreu, A.; Rodriguez, L.; Flores, L.; Ibarzabal, A.; Lacy, A.; Jimenez, A.; Vidal, J. Protein intake and lean tissue mass retention following bariatric surgery. Clin Nutr 2013, 32, 550–555. [Google Scholar] [CrossRef]
- Hassannejad, A.; Khalaj, A.; Mansournia, M.A.; Rajabian Tabesh, M.; Alizadeh, Z. The Effect of Aerobic or Aerobic-Strength Exercise on Body Composition and Functional Capacity in Patients with BMI ≥35 after Bariatric Surgery: A Randomized Control Trial. Obes. Surg. 2017, 27, 2792–2801. [Google Scholar] [CrossRef]
- Siervo, M.; Faber, P.; Lara, J.; Gibney, E.R.; Milne, E.; Ritz, P.; Lobley, G.E.; Elia, M.; Stubbs, R.J.; Johnstone, A.M. Imposed rate and extent of weight loss in obese men and adaptive changes in resting and total energy expenditure. Metabolism 2015, 64, 896–904. [Google Scholar] [CrossRef]
- Faria, S.L.; Kelly, E.; Faria, O.P. Energy expenditure and weight regain in patients submitted to Roux-en-Y gastric bypass. Obes. Surg. 2009, 19, 856–859. [Google Scholar] [CrossRef]
- Faria, S.L.; Faria, O.P.; Buffington, C.; de Almeida Cardeal, M.; Rodrigues de Gouvea, H. Energy expenditure before and after Roux-en-Y gastric bypass. Obes. Surg. 2012, 22, 1450–1455. [Google Scholar] [CrossRef]
- Bazzocchi, A.; Ponti, F.; Cariani, S.; Diano, D.; Leuratti, L.; Albisinni, U.; Marchesini, G.; Battista, G. Visceral Fat and Body Composition Changes in a Female Population After RYGBP: A Two-Year Follow-Up by DXA. Obes. Surg. 2015, 25, 443–451. [Google Scholar] [CrossRef]
- Heath, M.L.; Kow, L.; Slavotinek, J.P.; Valentine, R.; Toouli, J.; Thomson, C.H. Abdominal adiposity and liver fat content 3 and 12 months after gastric banding surgery. Metabolism 2009, 58, 753–758. [Google Scholar] [CrossRef]
- Zang, Y.; Zhu, C.; Wen, X.; Wang, X.; Li, L.; Rampersad, S.; Lu, L.; Zhou, D.; Qian, C.; Cui, R.; et al. Laparoscopic sleeve gastrectomy improves body composition and alleviates insulin resistance in obesity related acanthosis nigricans. Lipids Health Dis. 2017, 16, 209. [Google Scholar] [CrossRef] [Green Version]
- Gletsu-Miller, N.; Hansen, J.M.; Jones, D.P.; Go, Y.M.; Torres, W.E.; Ziegler, T.R.; Lin, E. Loss of total and visceral adipose tissue mass predicts decreases in oxidative stress after weight-loss surgery. Obesity 2009, 17, 439–446. [Google Scholar] [CrossRef]
- Sun, J.; Lv, H.; Li, M.; Zhao, L.; Liu, Y.; Zeng, N.; Wei, X.; Chen, Q.; Ren, P.; Liu, Y.; et al. How much abdominal fat do obese patients lose short term after laparoscopic sleeve gastrectomy? A quantitative study evaluated with MRI. Quant. Imaging Med. Surg. 2021, 11, 4569–4582. [Google Scholar] [CrossRef]
- Guida, B.; Cartaldi, M.; Busetto, M.; Aiello, M.L.; Musella, M.; Capone, D.; Parolisi, S.; Policastro, V.; Ragozini, G.; Belfiore, A. Predictors of fat-free mass loss 1 years after laparoscopic sleeve gastrectomy. J. Endocrinol. Investig. 2018, 41, 1307–1315. [Google Scholar] [CrossRef]
- Nuijten, M.A.H.; Monpellier, V.M.; Eijsvogels, T.M.H.; Janssen, I.M.C.; Hazebroek, E.J.; Hopman, M.T.E. Rate and Determinants of Excessive Fat-Free Mass Loss after Bariatric Surgery. Obes. Surg. 2020, 30, 3119–3126. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Baseline | 1-Month | 12-Months | 24-Months | % Relative Variation (Δ 1 m-Baseline/Baseline) | % Relative Variation (Δ 12 m-Baseline/Baseline) | % Relative Variation (Δ 24 m-Baseline/Baseline) | |
|---|---|---|---|---|---|---|---|
| Number of patients, n | 83 | 83 | 76 | 60 | |||
| Age, yr | 40.9 ± 12.3 | - | - | - | - | - | - |
| Height, m | 165.2 ± 7.6 | - | - | - | - | - | - |
| Weight, kg | 110.9 ± 13.0 | 100.9 ± 12.3 | 79.1 ± 14.2 | 81.9 ± 14.0 | −9.1 ± 2.1 *** | −29.3 ± 8.4 *** | −27.5 ± 9.6 *** |
| BMI, kg/m2 | 40.7 ± 4.2 | 37.1 ± 4.2 | 28.9 ± 4.3 | 29.8 ± 4.5 | −9.1 ± 2.1 *** | −29.3 ± 8.4 *** | −27.6 ± 9.8 *** |
| Ideal body weight, kg | 60.00 ± 6.01 | - | - | - | - | - | - |
| Neck circumference, cm | 42.4 ± 4.0 | 40.1 ± 3.8 | 35.9 ± 3.6 | 36.4 ± 3.6 | −4.8 ± 3.5 *** | −15.2 ± 4.7 *** | −15.0 ± 5.4 *** |
| Waist circumference, cm | 114.2 ± 12.9 | 107 ± 11.4 | 89.3 ± 13.5 | 91.1 ± 11.8 | −6.4 ± 5.1 *** | −21.6 ± 9.5 *** | −20.7 ± 8.9 *** |
| Hip circumference, cm | 128.2 ± 11.7 | 121.8 ± 11.9 | 99.4 ± 15.6 | 103.9 ± 14.1 | −5.0 ± 4.3 *** | −22.6 ± 11.0 *** | −19.3 ± 10.0 *** |
| Waist/hip circumference ratio | 0.9 ± 0.1 | 0.9 ± 0.1 | 0.9 ± 0.1 | 0.9 ± 0.1 | 1.3 ± 7.7 ** | 2.5 ± 13.8 | 0.96 ± 11.1 |
| Type 2 diabetes mellitus, n (%) | 17 (20.48) | 13 (15.85) | 5 (6.67) | 6 (9.68) | |||
| Hypertension, n (%) | 37 (44.58) | 23 (28.75) | 12 (15.58) | 10 (13.70) | |||
| Sleep apnoea, n (%) | 53 (63.86) | 34 (53.13) | 25 (37.88) | 9 (15.52) |
| Baseline | 1-Month | 12-Months | 24-Months | % Relative Variation (Δ 1 m-Baseline/Baseline) | % Relative Variation (Δ 12 m-Baseline/Baseline) | % Relative Variation (Δ 24 m-Baseline/Baseline) | |
|---|---|---|---|---|---|---|---|
| Number of patients, n | 83 | 83 | 76 | 60 | |||
| LTM (kg) | |||||||
| Upper limb | 3.3 ± 0.9 | 3.0 ± 8.4 | 2.7 ± 0.8 | 2.7 ± 0.8 | −9.8 ± 5.9 *** | −20.6 ± 7.5 *** | −20.7 ± 7.5 *** |
| Trunk | 33.6 ± 6.3 | 30.1 ± 5.6 | 27.0 ± 5.7 | 27.6 ± 5.5 | −10.4 ± 4.8 | −20.1 ± 7. 1 *** | −19.9 ± 7.9 *** |
| Lower limbs | 10.3 ± 1.8 | 9.4 ± 1.7 | 8.3 ± 1.7 | 8.4 ± 1.6 | −8.9 ± 5.1 *** | −20.2 ± 8.3 *** | −20.0 ± 8.0 *** |
| Whole body | 64.3 ± 11.6 | 58.1 ± 10.4 | 52.9 ± 10.6 | 52.3 ± 10.4 | −9.6 ± 4.0 *** | −19.4 ± 6.5 *** | −19.5 ± 7.1 ** |
| FM (kg) | |||||||
| Upper limbs | 2.9 ± 0.7 | 2.7 ± 0.7 | 1.7 ± 0.6 | 1.8 ± 0.6 | −5.3 ± 7.7 *** | −39.8 ± 13.9 *** | −38.7 ± 15.3 *** |
| Trunk | 21.8 ± 4.4 | 19.8 ± 4.1 | 11.6 ± 4.4 | 12.8 ± 7.3 | −9.0 ± 4.9 *** | −47.9 ± 14.1 *** | −42.3 ± 16.4 *** |
| Lower limbs | 8.2 ± 2.5 | 7.6 ± 2.3 | 5.0 ± 1.7 | 5.3 ± 1.8 | −7.2 ± 3.7 *** | −39.0 ± 12.1 *** | −34.8 ± 14.1 *** |
| Whole body | 45.2 ± 9.2 | 41.7 ± 8.9 | 26.2 ± 8.1 | 28.1 ± 8.4 | −7.9 ± 3.5 *** | −42.7 ± 12.5 *** | −38.2 ± 14.6 *** |
| FM (%) | |||||||
| Upper limbs | 45.4 ± 9.8 | 46.4 ± 10.0 | 38.2 ± 10.1 | 38.3 ± 10.2 | −2.3 ± 4.6 *** | −16.6 ± 9.8 *** | −15.4 ± 11.6 *** |
| Trunk | 39.0 ± 5.8 | 39.3 ± 6.1 | 29.0 ± 7.1 | 30.5 ± 7.3 | 0.6 ± 5.4 | −26.0 ± 12.7 *** | −21.0 ± 14.9 *** |
| Lower limbs | 42.4 ± 9.5 | 43.1 ± 9.5 | 35.7 ± 9.1 | 37.1 ± 9.5 | 1.5 ± 5.8 * | −16.3 ± 9.5 *** | -12.2 ± 9.3 ** |
| Whole body | 40.4 ± 7.0 | 40.8 ± 7.2 | 32.2 ± 7.2 | 33.4 ± 7.5 | 0.8 ± 4.1 | −20.8 ± 9.9 *** | −16.7 ± 11.6 *** |
| LTM/FM | |||||||
| Upper limbs | 1.3 ± 0.6 | 1.2 ± 0.6 | 1.7 ± 0.9 | 1.7 ± 0.9 | −4.3 ± 9.0 *** | 37.7 ± 29.7 *** | 37.7 ± 38.7 *** |
| Trunk | 1.6 ± 0.4 | 1.6 ± 0.4 | 2.6 ± 1.0 | 2.4 ±1.0 | −1.1 ± 8.7 | 64.1± 46.7 *** | 52.1 ± 53.7 *** |
| Lower limbs | 1.4 ± 0.7 | 1.4 ± 0.7 | 1.9 ± 1.0 | 1.8 ± 0.9 | −1.7 ± 7.4 * | 35.2 ± 27.5 *** | 27.6 ± 26.1 *** |
| Whole body | 1.5 ± 0.5 | 1.5 ± 0.5 | 2.2 ± 0.8 | 2.1 ± 0.8 | −1.6 ± 6.9 * | 46.4 ± 30.6 *** | 37.7 ± 35.5 *** |
| Sarcopenia index | |||||||
| ALM, kg | 27.40 ± 5.33 | 24.84 ± 4.85 | 22.02 ± 4.97 | 22.25 ± 4.74 | −9.2 ± 4.6 *** | −20.3 ± 7.7 *** | −20.2 ± 7.6 *** |
| ALMI(h2), kg/m2 | 9.97 ± 1.29 | 9.05 ± 1.17 | 7.98 ± 1.21 | 8.04 ± 1.16 | −9.2 ± 4.6 *** | −20.3 ± 7.7 *** | −20.3 ± 7.6 *** |
| ALMI(BMI) | 0.68 ± 0.14 | 0.68 ± 0.15 | 0.77 ± 0.16 | 0.74 ± 0.15 | −0.2 ± 4.0 | 13.3 ± 8.9 *** | 10.8 ± 9.0 *** |
| Baseline | 1-Month | 12-Months | 24-Months | % Relative Variation (Δ 1 m-Baseline/Baseline) | % Relative Variation (Δ 12 m-Baseline/Baseline) | % Relative Variation (Δ 24 m-Baseline/Baseline) | |
|---|---|---|---|---|---|---|---|
| Number of patients, n | 83 | 83 | 76 | 60 | |||
| Android region | |||||||
| Total mass, kg | 9.9 ± 1.7 | 8.7 ± 1.5 | 6.3 ± 1.8 | 6.6 ± 1.8 | −11.8 ± 4.3 *** | −36.6 ± 10.8 *** | −34.7 ± 12.0 *** |
| LTM, kg | 5.7 ± 1.1 | 5.0 ± 1.0 | 4.3 ± 1.1 | 4.4 ± 1.0 | −12.9 ± 5.8 *** | −24.5± 8.9 *** | −24.8 ± 10.2 *** |
| FM, kg | 4.2 ± 0.9 | 3.7 ± 0.9 | 2.0 ± 0.9 | 2.2 ± 0.9 | −10.4 ± 7.2 *** | −53.2 ± 15.3 *** | −48.2 ± 17.6 *** |
| Fat, % | 42.1 ± 5.4 | 42.8 ± 6.0 | 30.5 ± 7.1 | 32.3 ± 7.6 | 1.7 ± 6.6 * | −27.7 ± 13.7 *** | −22.7 ± 16.4 *** |
| Gynoid region | |||||||
| Total mass, kg | 18.6 ± 2.6 | 16.9 ± 2.4 | 13.4 ± 2.5 | 13.9 ± 2.5 | −9.0 ± 4.9 *** | −28.2 ± 10.3 *** | −25.9 ± 11.5 *** |
| LTM, kg | 11.2 ± 1.9 | 10.0 ± 1.7 | 8.9 ± 1.7 | 9.0 ± 1.7 | −10.6 ± 6.1 *** | −21.0 ± 9.0 *** | −21.3 ± 10.7 *** |
| FM, kg | 7.4 ± 2.0 | 6.9 ± 1.8 | 4.5 ± 1.4 | 4.9 ± 1.6 | −6.3 ± 6.1 *** | −38.5 ± 13.2 *** | −32.2 ± 15.1 *** |
| Fat, % | 39.3 ± 8.2 | 40.7 ± 8.0 | 33.3 ± 7.3 | 35.1 ± 7.6 | 3.0 ± 5.2 *** | −15.1 ± 8.3 *** | −9.2 ± 10.9 *** |
| Abdominal adipose tissue | |||||||
| TAT mass, kg | 3.67 ± 0.59 | 3.42 ± 0.63 | 2.03 ± 0.71 | 2.23 ± 0.75 | −7.69 ± 5.73 *** | −45.75 ± 14.74 *** | −40.33 ± 16.67 *** |
| VAT mass, kg | 0.74 ± 0.33 | 0.70 ± 0.26 | 0.47 ± 0.26 | 0.48 ± 0.24 | −7.16 ± 18.45 *** | −34.80 ± 35.12 *** | −38.40 ± 26.08 *** |
| SAT mass, kg | 2.95 ± 0.61 | 2.72 ± 0.60 | 1.57 ± 0.62 | 1.75 ± 0.63 | −7.98 ± 8.36 *** | −46.89 ± 18.23 *** | −39.40 ± 19.93 *** |
| Baseline | 1-Month | 12-Months | 24-Months | % Relative Variation (Δ 1-m Baseline/Baseline) | % Relative Variation (Δ 12-m Baseline/Baseline) | % Relative Variation (Δ 24-m Baseline/Baseline) | |
|---|---|---|---|---|---|---|---|
| Number of patients, n | 83 | 83 | 76 | 60 | |||
| Glucose homeostasis | |||||||
| Glucose, mmol/l | 6.1 ± 2.1 | 5.3 ± 1.0 | 4.9 ± 1.1 | 5.1 ± 0.9 | −8.2 ± 13.9 *** | −15.6 ± 14.2 *** | −15.3 ± 13.7 *** |
| Insulin, µIU/mL | 29.3 ± 22.0 | 16.3 ± 10.6 | 10.4 ± 10.2 | 10.8 ± 7.8 | −34.2 ± 37.4 *** | −61.4 ± 22.8 *** | −59.2 ± 24.7 *** |
| HOMA−IR | 8.1 ± 7.1 | 4.0 ± 3.1 | 2.3 ± 2.3 | 2.5 ± 1.9 | −38.1 ± 39.0 | −66.2 ± 23.8 | −65.5 ± 21.6 |
| HbA1c, % | 5.9 ± 1.0 | 5.7 ± 0.7 | 5.4 ± 0.5 | 5.6 ± 0.6 | −3.3 ± 4.5 *** | −6.4 ± 8.4 *** | −5.9 ± 9.3 *** |
| HbA1c, mmol/mol | 41.3 ± 10.7 | 38.3 ± 7.7 | 35.8 ± 5.4 | 37.5 ± 6.7 | −5.8 ± 6.7 *** | −11.0 ± 11.0 *** | −9.4 ± 12.0 |
| Lipid profile | |||||||
| Total cholesterol, g/l | 2.0 ± 0.5 | 1.8 ± 0.4 | 1.9 ± 0.6 | 1.9 ± 0.3 | −7.3 ± 20.0 *** | 3.3 ± 31.6 | 0.3 ± 16.6 |
| HDL, g/l | 0.5 ± 0.1 | 0.5 ± 0.1 | 0.6 ± 0.2 | 0.6 ± 0.1 | −5.5 ± 17.1 *** | 28.9 ± 33.9 | 32.1 ± 24.7 *** |
| LDL, g/l | 1.2 ± 0.4 | 1.0 ± 0.3 | 1.1 ± 0.3 | 1.1 ± 0.3 | −10.1 ± 20.4 *** | −1.6 ±29.3 *** | −0.5 ± 35.4 |
| Triglycerides, g/l | 1.6 ± 0.8 | 1.4 ± 0.6 | 1.0 ± 0.4 | 0.9 ± 0.4 | −2.3 ± 31.0 (p = 0.06) | −28.9 ± 26.2 *** | −30.3 ± 25.7 *** |
| Other parameters | |||||||
| CRP, mg/ml | 7.3 ± 5.7 | 3.8 ± 3.4 | 2.1 ± 2.2 | 1.9 ± 2.4 | −36.4 ± 42.7 *** | −66.4 ± 32.4 *** | −64.7 ± 55.6 *** |
| IGF-1, ng/ml | 143.6 ± 55.5 | 127.0 ± 51. 9 | 155.5 ± 55.5 | 155.0 ± 52.5 | −10.8 ± 24.1 *** | 12.5 ± 23.3 *** | 16.0 ± 29.7 *** |
| IGFBP-3, ng/ml | 4972.5 ± 1324.0 | 4321.8 ± 1140.14 | 4099.6 ± 958.0 | 4022.6 ± 961.0 | −12.3 ± 14.4 *** | −15.3 ± 11.8 *** | −12.9 ± 16.7 *** |
| Albumin, g/l | 44.5 ± 2.9 | 44.5 ± 4.3 | 45.6 ± 6.4 | 45.1 ± 4.3 | −1.1 ± 7.2 | −0.8 ± 7.3 | 1.2 ± 8.5 |
| REE, cal/24 h | 2010.2 ± 366.6 | 1677.8 ± 282.6 | 1535.6 ± 253.4 | 1536.5 ± 239.6 | −15.7 ± 10.0 *** | −23.2 ± 8.3 *** | −24.0 ± 9.3 *** |
| Predicted REE values, % | 4.5 ± 12.9 | −6.5 ± 11.7 | −3.0 ± 8.5 | −3.5 ± 9.0 | - | - | - |
| Baseline | % Relative Variation (Δ 1 m-Baseline/Baseline) | % Relative Variation (Δ 12 m-Baseline/Baseline) | % Relative Variation (Δ 24 m-Baseline/Baseline) | |||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Baseline Parameters | LTM | FM | SAT | VAT | TAT | LTM | FM | SAT | VAT | TAT | LTM | FM | SAT | VAT | TAT | LTM | FM | SAT | VAT | TAT |
| Age | 0.12 | −0.30 ** | −0.44 *** | 0.64 *** | −0.09 | 0.10 | −0.09 | −0.09 | −0.30 ** | −0.19 | 0.29 * | 0.35 ** | 0.22 | 0.12 | 0.25 | 0.26 * | 0.29 * | 0.35 ** | 0.02 | 0.31 * |
| BMI | 0.22 * | 0.79 *** | 0.63 *** | 0.17 | 0.72 *** | 0.26 * | −0.03 | 0.14 | 0.11 | 0.19 | −0.05 | 0.04 | 0.01 | 0.06 | 0.13 | −0.2 | −0.10 | 0.01 | −0.23 | −0.07 |
| WB LTM | − | −0.19 | −0.26 | 0.36 | −0.08 | −0.10 | −0.27 * | −0.08 | −0.33 ** | −0.27 * | 0.05 | 0.15 | 0.16 | 0.07 | 0.15 | −0.02 | 0.07 | 0.06 | −0.08 | 0.04 |
| WB FM | −0.19 | − | 0.81*** | −0.02 | 0.83 *** | 0.34 ** | 0.11 | 0.24 | 0.22 | 0.34 ** | 0.03 | 0.07 | 0.14 | 0.10 | 0.18 | −0.1 | −0.09 | 0.05 | −0.18 | −0.02 |
| TAT | −0.08 | 0.83 *** | 0.83 *** | 0.25 * | - | 0.38 *** | 0.07 | 0.23 * | 0.03 | 0.25 * | 0.13 | 0.22 | 0.29 * | 0.12 | 0.33 ** | −0.02 | 0.08 | 0.22 | −0.14 | 0.15 |
| VAT | 0.36 ** | −0.02 | −0.27 * | - | 0.24 * | 0.17 | −0.04 | 0.18 | −0.55 *** | −0.06 | 0.30** | 0.45*** | 0.43*** | −0.03 | 0.42*** | 0.21 | 0.39 * | 0.48 *** | −0.10 | 0.41 ** |
| SAT | −0.26 * | 0.81 *** | - | −0.27* | 0.83 *** | 0.30 ** | 0.08 | 0.05 | 0.30 ** | 0.23 * | 0.015 | −0.02 | 0.02 | 0.14 | 0.08 | −0.07 | −0.13 | −0.09 | −0.06 | −0.09 |
| Glucose | 0.45 *** | −0.22* | −0.32 ** | 0.50 *** | −0.06 | 0.08 | −0.16 | −0.09 | −0.36 ** | −0.24 * | 0.12 | 0.20 | 0.18 | −0.05 | 0.16 | 0.04 | 0.21 | 0.28 * | 0.04 | 0.25 |
| Insulin | 0.37 *** | −0.03 | −0.09* | 0.20 * | 0.01 | −0.06 | 0.03 | 0.10 | −0.09 | 0.07 | −0.24 * | 0.08 | 0.16 | −0.1 | 0.13 | −0.04 | 0031 | 0.28 * | 0.18 | 0.30 |
| HOMA-IR | 0.47 *** | −0.12 | −0.22 * | 0.35 ** | −0.01 | 0.03 | −0.07 | 0.07 | −0.23 * | −0.03 | −0.18 | 0.13 | 0.21 | −0.2 | 0.16 | 0.01 | 0.36 | 0.38 ** | 0.14 | 0.37 |
| HbA1c | 0.40 *** | −0.18 | −0.32 ** | 0.53 *** | −0.02 | 0.13 | −0.07 | 0.07 | −0.33 ** | −0.06 | 0.09 | 0.25 * | 0.25 * | 0.05 | 0.24 * | 0.01 | 0.28 | 0.37 ** | 0.06 | 0.33 * |
| Total cholesterol | −0.12 | −0.26 * | −0.16 | 0.11 * | −0.08 | −0.16 | 0.02 | −0.09 | 0.04 | 0.03 | 0.02 | −0.06 | −0.05 | −0.07 | −0.07 | 0.09 | 0.02 | 0.05 | 0.09 | 0.1 |
| HDL | −0.41 *** | 0.01 | 0.12 | −0.30 ** | −0.04 | −0.09 | 0.23 * | 0.02 | 0.20 | 0.16 | 0.05 | −0.04 | 0.01 | 0.18 | −0.01 | 0.03 | −0.16 | −0.15 | 0.13 | −0.10 |
| LDL | −0.15 | −0.14 | −0.09 | 0.05 | −0.06 | −0.09 | −0.04 | −0.08 | 0.07 | −0.02 | 0.02 | −0.1 | −0.12 | −0.08 | −0.11 | 0.08 | −0.02 | 0.02 | 0.10 | 0.04 |
| Triglycerides | 0.24 * | −0.26 * | −0.27 * | 0.39 *** | −0.01 | −0.05 | −0.06 | 0.10 | −0.28 * | −0.14 | 0.01 | 0.16 | 0.13 | −0.04 | 0.11 | 0.01 | 0.26 | 0.29 | 0.01 | 0.28 * |
| CRP | −0.30 ** | 0.36 ** | 0.32 ** | −0.12 | 0.24 * | 0.20 | 0.24 | 0.10 | 0.20 | 0.18 | 0.05 | 0.12 | 0.07 | 0.25 * | 0.18 | 0.01 | −0.09 | 0.02 | −0.04 | −0.03 |
| IGF-1 | −0.01 | 0.04 | 0.19 | −0.49 *** | −0.06 | −0.06 | −0.01 | −0.15 | 0.17 | −0.09 | −0.08 | −0.27 * | −0.25 * | −0.06 | −0.28 * | −0.04 | −0.20 | −0.24 | 0.01 | −0.21 |
| IGFBP-3 | 0.08 | 0.10 | 0.19 | −0.16 | 0.13 | −0.07 | 0.04 | 0.06 | 0.14 | 0.12 | −0.26 | −0.21 | −0.12 | −0.04 | −0.16 | −0.18 | −0.23 | −0.11 | −0.38* | −0.16 |
| Albumin | 0.42 *** | −0.34 ** | −0.23* | −0.01 | −0.23* | −0.10 | −0.31 ** | −0.20 | −0.21 * | −0.28* | −0.14 | −0.10 | −0.04 | −0.09 | −0.11 | −0.11 | 0.05 | −0.03 | 0.02 | 0.01 |
| REE | 0.84 *** | −0.09 | −0.17 | 0.37*** | 0.03 | 0.06 | −0.25 * | 0.01 | −0.36 *** | −0.18 | 0.08 | −0.18 | 0.22 | 0.01 | 0.19 | 0.01 | 0.15 | 0.17 | −0.06 | 0.14 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Maïmoun, L.; Aouinti, S.; Puech, M.; Lefebvre, P.; Deloze, M.; de Santa Barbara, P.; Renard, E.; Christol, J.-P.; Myzia, J.; Picot, M.-C.; et al. Changes in Lean Tissue Mass, Fat Mass, Biological Parameters and Resting Energy Expenditure over 24 Months Following Sleeve Gastrectomy. Nutrients 2023, 15, 1201. https://doi.org/10.3390/nu15051201
Maïmoun L, Aouinti S, Puech M, Lefebvre P, Deloze M, de Santa Barbara P, Renard E, Christol J-P, Myzia J, Picot M-C, et al. Changes in Lean Tissue Mass, Fat Mass, Biological Parameters and Resting Energy Expenditure over 24 Months Following Sleeve Gastrectomy. Nutrients. 2023; 15(5):1201. https://doi.org/10.3390/nu15051201
Chicago/Turabian StyleMaïmoun, Laurent, Safa Aouinti, Marion Puech, Patrick Lefebvre, Melanie Deloze, Pascal de Santa Barbara, Eric Renard, Jean-Paul Christol, Justine Myzia, Marie-Christine Picot, and et al. 2023. "Changes in Lean Tissue Mass, Fat Mass, Biological Parameters and Resting Energy Expenditure over 24 Months Following Sleeve Gastrectomy" Nutrients 15, no. 5: 1201. https://doi.org/10.3390/nu15051201