
What Is the Current Direction of the Research on Carotenoids and Human Health? An Overview of Registered Clinical Trials

 , ,
, ,  ,
,  , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Database Search Strategy
2.2. Study Selection
2.3. Data Extraction and Analysis
3. Results
3.1. Selected Clinical Trials
3.2. Trials on Carotenoid-Rich Foods
3.3. Trials on Supplements
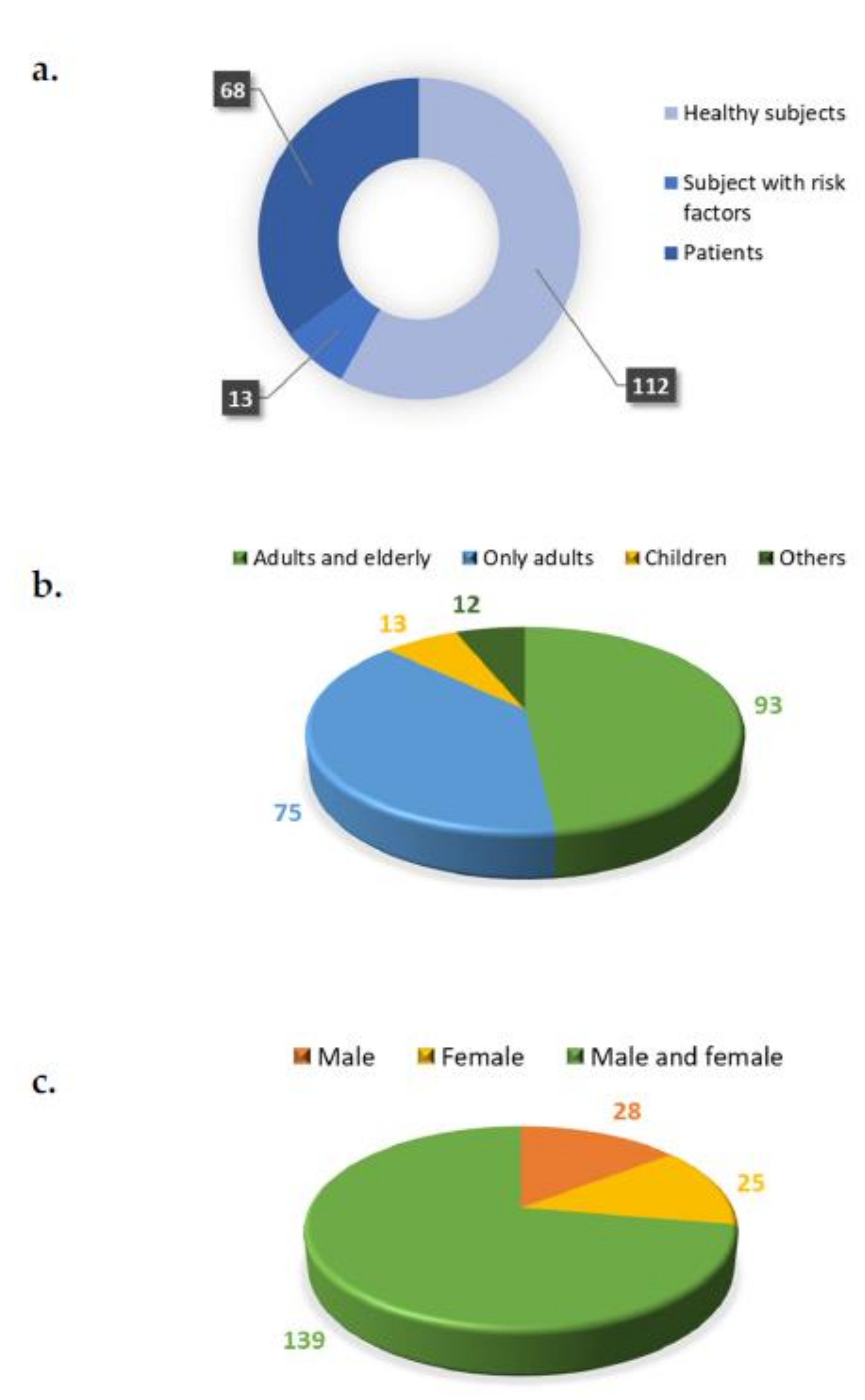
3.4. Characteristics of Subjects Recruited in the Trials
3.5. Main Goals of the Registered Trials
3.6. Main Outcomes of the Registered Trials
4. Discussion
5. Strengths and Limitations of the Study
6. Future-Study Directions
7. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Desmarchelier, C.; Borel, P. Overview of carotenoid bioavailability determinants: From dietary factors to host genetic variations. Trends Food Sci. Technol. 2017, 69, 270–280. [Google Scholar] [CrossRef] [Green Version]
- Rodriguez-Concepcion, M.; Avalos, J.; Bonet, M.L.; Boronat, A.; Gomez-Gomez, L.; Hornero-Mendez, D.; Limon, M.C.; Meléndez-Martínez, A.J.; Olmedilla-Alonso, B.; Palou, A.; et al. A global perspective on carotenoids: Metabolism, biotechnology, and benefits for nutrition and health. Prog. Lipid Res. 2018, 70, 62–93. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Porrini, M.; Riso, P. Factors influencing the bioavailability of antioxidants in foods: A critical appraisal. Nutr. Metab. Cardiovasc. Dis. 2008, 18, 647–650. [Google Scholar] [CrossRef]
- Moran, N.E.; Mohn, E.S.; Hason, N.; Erdman, J.W.; Johnson, E.J. Intrinsic and extrinsic factors impacting absorption, metabolism, and health effects of dietary carotenoids. Adv. Nutr. 2018, 9, 465–492. [Google Scholar] [PubMed] [Green Version]
- Chacón-Ordóñez, T.; Carle, R.; Schweiggert, R. Bioaccessibility of carotenoids from plant and animal foods. J. Sci. Food Agric. 2019, 99, 3220–3239. [Google Scholar] [CrossRef] [PubMed]
- Pellegrini, N.; Chiavaro, E.; Gardana, C.; Mazzeo, T.; Contino, D.; Gallo, M.; Riso, P.; Fogliano, V.; Porrini, M. Effect of different cooking methods on color, phytochemical concentration, and antioxidant capacity of raw and frozen brassica vegetables. J. Agric. Food Chem. 2010, 58, 4310–4321. [Google Scholar] [CrossRef] [PubMed]
- Meléndez-Martínez, A.J.; Böhm, V.; Borge, G.I.A.; Cano, M.P.; Fikselová, M.; Gruskiene, R.; Lavelli, V.; Loizzo, M.R.; Mandić, A.I.; Brahm, P.M.; et al. Carotenoids: Considerations for Their Use in Functional Foods, Nutraceuticals, Nutricosmetics, Supplements, Botanicals, and Novel Foods in the Context of Sustainability, Circular Economy, and Climate Change. Annu. Rev. Food Sci. Technol. 2021, 12, 433–460. [Google Scholar] [CrossRef]
- Riso, P.; Brusamolino, A.; Moro, M.; Porrini, M. Absorption of bioactive compounds from steamed broccoli and their effect on plasma glutathione S-transferase activity. Int. J. Food Sci. Nutr. 2009, 60, 56–71. [Google Scholar] [CrossRef]
- Riso, P.; Visioli, F.; Gardana, C.; Grande, S.; Brusamolino, A.; Galvano, F.; Galvano, G.; Porrini, M. Effects of blood orange juice intake on antioxidant bioavailability and on different markers related to oxidative stress. J. Agric. Food Chem. 2005, 53, 941–947. [Google Scholar] [CrossRef]
- Riso, P.; Brusamolino, A.; Scalfi, L.; Porrini, M. Bioavailability of carotenoids from spinach and tomatoes. Nutr. Metab. Cardiovasc. Dis. 2004, 14, 150–156. [Google Scholar] [CrossRef]
- Böhm, V.; Lietz, G.; Olmedilla-Alonso, B.; Phelan, D.; Reboul, E.; Bánati, D.; Borel, P.; Corte-Real, J.; De Lera, A.R.; Desmarchelier, C.; et al. From carotenoid intake to carotenoid blood and tissue concentrations-implications for dietary intake recommendations. Nutr. Rev. 2021, 79, 544–573. [Google Scholar] [CrossRef] [PubMed]
- Meléndez-Martínez, A.J.; Mandić, A.I.; Bantis, F.; Böhm, V.; Borge, G.I.A.; Brnčić, M.; Bysted, A.; Cano, M.P.; Dias, M.G.; Elgersma, A.; et al. A comprehensive review on carotenoids in foods and feeds: Status quo, applications, patents, and research needs. Crit. Rev. Food Sci. Nutr. 2021. [Google Scholar] [CrossRef] [PubMed]
- Bahonar, A.; Saadatnia, M.; Khorvash, F.; Maracy, M.; Khosravi, A. Carotenoids as potential antioxidant agents in stroke prevention: A systematic review. Int. J. Prev. Med. 2017, 8, 6–12. [Google Scholar]
- Lem, D.W.; Gierhart, D.L.; Davey, P.G. Carotenoids in the Management of Glaucoma: A Systematic Review of the Evidence. Nutrients 2021, 13, 1949. [Google Scholar] [CrossRef] [PubMed]
- Peraita-Costa, I.; Carrillo Garcia, P.; Morales-Suárez-Varela, M. Is There an Association between β-Carotene and Breast Cancer? A Systematic Review on Breast Cancer Risk. Nutr. Cancer 2022, 74, 39–54. [Google Scholar] [CrossRef]
- Beydoun, M.A.; Chen, X.; Jha, K.; Beydoun, H.A.; Zonderman, A.B.; Canas, J.A. Carotenoids, vitamin A, and their association with the metabolic syndrome: A systematic review and meta-analysis. Nutr. Rev. 2019, 77, 32–45. [Google Scholar] [CrossRef] [PubMed]
- Dulińska-Litewka, J.; Sharoni, Y.; Hałubiec, P.; Łazarczyk, A.; Szafrański, O.; McCubrey, J.A.; Gąsiorkiewicz, B.; Laidler, P.; Bohn, T. Recent progress in discovering the role of carotenoids and their metabolites in prostatic physiology and pathology with a focus on prostate cancer—A review—Part i: Molecular mechanisms of carotenoid action. Antioxidants 2021, 10, 585. [Google Scholar] [CrossRef] [PubMed]
- Dulińska-Litewka, J.; Hałubiec, P.; Łazarczyk, A.; Szafrański, O.; Sharoni, Y.; McCubrey, J.A.; Gąsiorkiewicz, B.; Bohn, T. Recent Progress in Discovering the Role of Carotenoids and Metabolites in Prostatic Physiology and Pathology—A Review—Part II: Carotenoids in the Human Studies. Antioxidants 2021, 10, 319. [Google Scholar] [CrossRef]
- Li, N.; Wu, X.; Zhuang, W.; Xia, L.; Chen, Y.; Wu, C.; Rao, Z.; Du, L.; Zhao, R.; Yi, M.; et al. Tomato and lycopene and multiple health outcomes: Umbrella review. Food Chem. 2021, 343, 128396. [Google Scholar] [CrossRef] [PubMed]
- Eggersdorfer, M.; Wyss, A. Carotenoids in human nutrition and health. Arch. Biochem. Biophys. 2018, 652, 18–26. [Google Scholar] [CrossRef]
- Cheng, H.M.; Koutsidis, G.; Lodge, J.K.; Ashor, A.; Siervo, M.; Lara, J. Tomato and lycopene supplementation and cardiovascular risk factors: A systematic review and meta-analysis. Atherosclerosis 2017, 257, 100–108. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hajizadeh-Sharafabad, F.; Zahabi, E.S.; Malekahmadi, M.; Zarrin, R.; Alizadeh, M. Carotenoids supplementation and inflammation: A systematic review and meta-analysis of randomized clinical trials. Crit. Rev. Food Sci. Nutr. 2021. [Google Scholar] [CrossRef] [PubMed]
- Fathalipour, M.; Fathalipour, H.; Safa, O.; Nowrouzi-Sohrabi, P.; Mirkhani, H.; Hassanipour, S. The therapeutic role of carotenoids in diabetic retinopathy: A systematic review. Diabetes Metab. Syndr. Obes. Targets Ther. 2020, 13, 2347–2358. [Google Scholar] [CrossRef] [PubMed]
- Marino, M.; Del Bo’, C.; Martini, D.; Porrini, M.; Riso, P. A Review of Registered Clinical Trials on Dietary (Poly)Phenols: Past Efforts and Possible Future Directions. Foods 2020, 9, 1606. [Google Scholar] [CrossRef]
- Marino, M.; Martini, D.; Venturi, S.; Tucci, M.; Porrini, M.; Riso, P.; Del Bo’, C. An Overview of Registered Clinical Trials on Glucosinolates and Human Health: The Current Situation. Front. Nutr. 2021, 8, 798. [Google Scholar] [CrossRef]
- Available online: https://www.bccresearch.com/market-research/food-and-beverage/the-global-market-for-carotenoids.html (accessed on 7 February 2022).
- Buscemi, S.; Corleo, D.; Di Pace, F.; Petroni, M.; Satriano, A.; Marchesini, G. The Effect of Lutein on Eye and Extra-Eye Health. Nutrients 2018, 10, 1321. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, L.H.; Lee, J.C.Y.; Leung, H.H.; Lam, W.C.; Fu, Z.; Lo, A.C.Y. Lutein supplementation for eye diseases. Nutrients 2020, 12, 1–27. [Google Scholar] [CrossRef]
- Bernstein, P.S.; Li, B.; Vachali, P.P.; Gorusupudi, A.; Shyam, R.; Henriksen, B.S.; Nolan, J.M. Lutein, zeaxanthin, and meso-zeaxanthin: The basic and clinical science underlying carotenoid-based nutritional interventions against ocular disease. Prog. Retin. Eye Res. 2016, 50, 34–66. [Google Scholar] [CrossRef] [Green Version]
- Richer, S.; Stiles, W.; Statkute, L.; Pulido, J.; Frankowski, J.; Rudy, D.; Pei, K.; Tsipursky, M.; Nyland, J. Double-masked, placebo-controlled, randomized trial of lutein and antioxidant supplementation in the intervention of atrophic age-related macular degeneration: The Veterans LAST study (Lutein Antioxidant Supplementation Trial). Optometry 2004, 75, 216–229. [Google Scholar] [CrossRef]
- Parisi, V.; Tedeschi, M.; Gallinaro, G.; Varano, M.; Saviano, S.; Piermarocchi, S. Carotenoids and Antioxidants in Age-Related Maculopathy Italian Study. Ophthalmology 2008, 115, 324–333.e2. [Google Scholar] [CrossRef]
- Chew, E.Y.; Clemons, T.E.; SanGiovanni, J.P.; Danis, R.P.; Ferris, F.L.; Elman, M.J.; Antoszyk, A.N.; Ruby, A.J.; Orth, D.; Bressler, S.B.; et al. Secondary analyses of the effects of lutein/zeaxanthin on age-related macular degeneration progression AREDS2 report no. 3. JAMA Ophthalmol. 2014, 132, 142–149. [Google Scholar] [PubMed]
- Tierney, A.C.; Rumble, C.E.; Billings, L.M.; George, E.S. Effect of Dietary and Supplemental Lycopene on Cardiovascular Risk Factors: A Systematic Review and Meta-Analysis. Adv. Nutr. 2020, 11, 1453–1488. [Google Scholar] [CrossRef]
- Yao, Y.; Goh, H.M.; Kim, J.E. The Roles of Carotenoid Consumption and Bioavailability in Cardiovascular Health. Antioxidants 2021, 10, 1978. [Google Scholar] [CrossRef] [PubMed]
- Huang, Y.; Chen, H.; Su, Y.; Liu, H.; Hu, J.; Hong, K. Increased blood alpha-carotene, all-trans-Beta-carotene and lycopene levels are associated with beneficial changes in heart rate variability: A CVD-stratified analysis in an adult population-based study. Nutr. J. 2021, 20, 43. [Google Scholar] [CrossRef]
- Fassett, R.G.; Coombes, J.S. Astaxanthin in cardiovascular health and disease. Molecules 2012, 17, 2030–2048. [Google Scholar] [CrossRef] [PubMed]
- Riso, P.; Brusamolino, A.; Contino, D.; Martini, D.; Vendrame, S.; Del Bo’, C.; Porrini, M. Lycopene absorption in humans after the intake of two different single-dose lycopene formulations. Pharmacol. Res. 2010, 62, 318–321. [Google Scholar] [CrossRef]
- Riso, P.; Visioli, F.; Grande, S.; Guarnieri, S.; Gardana, C.; Simonetti, P.; Porrini, M. Effect of a tomato-based drink on markers of inflammation, immunomodulation, and oxidative stress. J. Agric. Food Chem. 2006, 54, 2563–2566. [Google Scholar] [CrossRef]
- Li, H.; Chen, A.; Zhao, L.; Bhagavathula, A.S.; Amirthalingam, P.; Rahmani, J.; Salehisahlabadi, A.; Abdulazeem, H.M.; Adebayo, O.; Yin, X. Effect of tomato consumption on fasting blood glucose and lipid profiles: A systematic review and meta-analysis of randomized controlled trials. Phyther. Res. 2020, 34, 1956–1965. [Google Scholar] [CrossRef] [PubMed]
- Khalighi Sikaroudi, M.; Saraf-Bank, S.; Clayton, Z.S.; Soltani, S. A positive effect of egg consumption on macular pigment and healthy vision: A systematic review and meta-analysis of clinical trials. J. Sci. Food Agric. 2021, 101, 4003–4009. [Google Scholar] [CrossRef]
- Lee, G.J.; Oda, K.; Morton, K.R.; Orlich, M.; Sabate, J. Egg intake moderates the rate of memory decline in healthy older adults. J. Nutr. Sci. 2021, 10, e79. [Google Scholar] [CrossRef]
- An, R.; Li, D.; McCaffrey, J.; Khan, N. Whole egg consumption and cognitive function among US older adults. J. Hum. Nutr. Diet. 2021. [Google Scholar] [CrossRef] [PubMed]
- Bishop, N.J.; Zuniga, K.E. Egg Consumption, Multi-Domain Cognitive Performance, and Short-Term Cognitive Change in a Representative Sample of Older U.S. Adults. J. Am. Coll. Nutr. 2019, 38, 537–546. [Google Scholar] [CrossRef]
- Mah, E.; Oliver Chen, C.Y.; Liska, D.A.J. The effect of egg consumption on cardiometabolic health outcomes: An umbrella review. Public Health Nutr. 2020, 23, 935–955. [Google Scholar] [CrossRef] [PubMed]
- Li, M.Y.; Chen, J.H.; Chen, C.; Kang, Y.N. Association between egg consumption and cholesterol concentration: A systematic review and meta-analysis of randomized controlled trials. Nutrients 2020, 12, 1–15. [Google Scholar] [CrossRef] [PubMed]
- Šamec, D.; Urlić, B.; Salopek-Sondi, B. Kale (Brassica oleracea var. acephala) as a superfood: Review of the scientific evidence behind the statement. Crit. Rev. Food Sci. Nutr. 2019, 59, 2411–2422. [Google Scholar] [CrossRef] [PubMed]
- Riso, P.; Vendrame, S.; Del Bo’, C.; Martini, D.; Martinetti, A.; Seregni, E.; Visioli, F.; Parolini, M.; Porrini, M. Effect of 10-day broccoli consumption on inflammatory status of young healthy smokers. Int. J. Food Sci. Nutr. 2014, 65, 106–111. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Riso, P.; Del Bo’, C.; Vendrame, S.; Brusamolino, A.; Martini, D.; Bonacina, G.; Porrini, M. Modulation of plasma antioxidant levels, glutathione S-transferase activity and DNA damage in smokers following a single portion of broccoli: A pilot study. J. Sci. Food Agric. 2014, 94, 522–528. [Google Scholar] [CrossRef]
- Riso, P.; Martini, D.; Møller, P.; Loft, S.; Bonacina, G.; Moro, M.; Porrini, M. DNA damage and repair activity after broccoli intake in young healthy smokers. Mutagenesis 2010, 25, 595–602. [Google Scholar] [CrossRef] [Green Version]
- Roberts, J.L.; Moreau, R. Functional properties of spinach (Spinacia oleracea L.) phytochemicals and bioactives. Food Funct. 2016, 7, 3337–3353. [Google Scholar] [CrossRef]
- Dahl, W.J.; Foster, L.M.; Tyler, R.T. Review of the health benefits of peas (Pisum sativum L.). Br. J. Nutr. 2012, 108, S3–S10. [Google Scholar] [CrossRef] [Green Version]
- Varghese, S.; Kubatka, P.; Rodrigo, L.; Gazdikova, K.; Caprnda, M.; Fedotova, J.; Zulli, A.; Kruzliak, P.; Büsselberg, D. Chili pepper as a body weight-loss food. Int. J. Food Sci. Nutr. 2017, 68, 392–401. [Google Scholar] [CrossRef] [PubMed]
- Frankenfeld, C.L.; Hullar, M.A.J.; Maskarinec, G.; Monroe, K.R.; Shepherd, J.A.; Franke, A.A.; Randolph, T.W.; Wilkens, L.R.; Boushey, C.J.; Le Marchand, L.; et al. The Gut Microbiome Is Associated with Circulating Dietary Biomarkers of Fruit and Vegetable Intake in a Multiethnic Cohort. J. Acad. Nutr. Diet. 2022, 122, 78–98. [Google Scholar] [CrossRef] [PubMed]
- Schmidt, K.M.; Haddad, E.N.; Sugino, K.Y.; Vevang, K.R.; Peterson, L.A.; Koratkar, R.; Gross, M.D.; Kerver, J.M.; Comstock, S.S. Dietary and plasma carotenoids are positively associated with alpha diversity in the fecal microbiota of pregnant women. J. Food Sci. 2021, 86, 602–613. [Google Scholar] [CrossRef] [PubMed]
- Bohn, T.; Bonet, M.L.; Borel, P.; Keijer, J.; Landrier, J.F.; Milisav, I.; Ribot, J.; Riso, P.; Winklhofer-Roob, B.; Sharoni, Y.; et al. Mechanistic aspects of carotenoid health benefits-Where are we now? Nutr. Res. Rev. 2021, 34, 276–302. [Google Scholar] [CrossRef] [PubMed]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| PICOS | Inclusion Criteria |
|---|---|
| Population | Healthy or diseased children, adults and/or older subjects |
| Intervention | Carotenoids present in food or as supplements, alone or in combination with other carotenoids |
| Comparison | Control group without carotenoids |
| Outcome | Bioavailability and/or any effect on human health |
| Study design | No restriction |
| All | Food | Supplements | Food and Supplements | |
|---|---|---|---|---|
| (n = 193) | (n = 83) | (n = 105) | (n = 5) | |
| Goal | ||||
| Human health | 140 | 49 | 89 | 2 |
| Bioavailability | 52 | 33 | 16 | 3 |
| Both | 1 | 1 | 0 | 0 |
| Duration | ||||
| Acute | 33 | 20 | 11 | 2 |
| Chronic | 158 | 61 | 94 | 3 |
| Both | 2 | 2 | 0 | 0 |
| Subjects | ||||
| Healthy | 112 | 65 | 43 | 4 |
| With risk factors | 13 | 5 | 8 | 0 |
| Patients | 68 | 13 | 54 | 1 |
| Primary outcome | ||||
| Bioavailability | 69 | 42 | 23 | 4 |
| Eye-related outcomes | 43 | 7 | 35 | 1 |
| Carotenoid concentration in breast milk, prostatic tissue and skin | 16 | 9 | 7 | 0 |
| Endothelial and vascular function | 16 | 9 | 7 | 0 |
| Oxidative stress and antioxidant status | 13 | 4 | 9 | 0 |
| Lipid profile and blood pressure | 10 | 7 | 3 | 0 |
| Cognitive function | 9 | 6 | 3 | 0 |
| Inflammation | 7 | 6 | 1 | 0 |
| Glucose metabolism | 6 | 4 | 2 | 0 |
| Others | 52 | 16 | 36 | 0 |
| Country | ||||
| United States of America | 74 | 35 | 37 | 2 |
| Israel | 13 | 0 | 13 | 0 |
| United Kingdom | 12 | 4 | 8 | 0 |
| Italy | 8 | 3 | 5 | 0 |
| The Netherlands | 7 | 3 | 3 | 1 |
| Ireland | 6 | 1 | 5 | 0 |
| France | 6 | 4 | 2 | 0 |
| China | 5 | 1 | 4 | 0 |
| Not provided | 14 | 7 | 6 | 1 |
| Others | 48 | 25 | 22 | 1 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Martini, D.; Negrini, L.; Marino, M.; Riso, P.; Del Bo, C.; Porrini, M. What Is the Current Direction of the Research on Carotenoids and Human Health? An Overview of Registered Clinical Trials. Nutrients 2022, 14, 1191. https://doi.org/10.3390/nu14061191
Martini D, Negrini L, Marino M, Riso P, Del Bo C, Porrini M. What Is the Current Direction of the Research on Carotenoids and Human Health? An Overview of Registered Clinical Trials. Nutrients. 2022; 14(6):1191. https://doi.org/10.3390/nu14061191
Chicago/Turabian StyleMartini, Daniela, Letizia Negrini, Mirko Marino, Patrizia Riso, Cristian Del Bo, and Marisa Porrini. 2022. "What Is the Current Direction of the Research on Carotenoids and Human Health? An Overview of Registered Clinical Trials" Nutrients 14, no. 6: 1191. https://doi.org/10.3390/nu14061191