
Use of Head and Chest Circumference Ratio as an Index of Fetal Growth Retardation in Preterm Infants
 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Subjects
2.2. Statistical Analysis
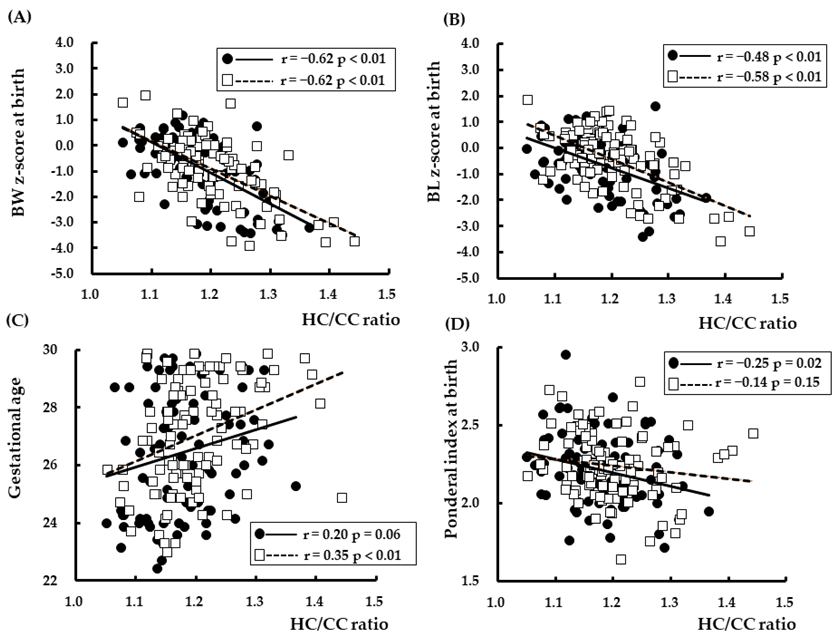
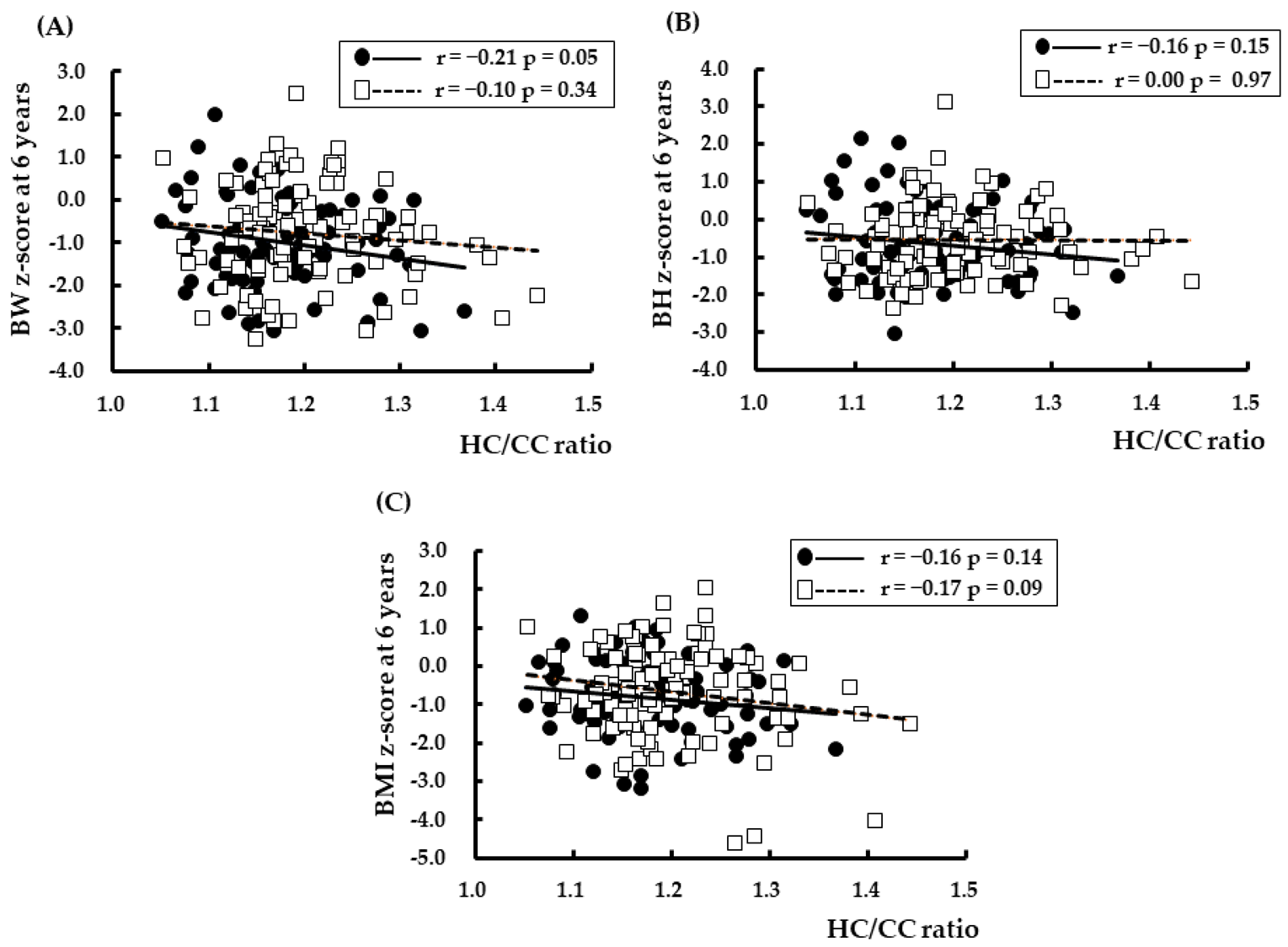
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Smith, L.K.; Morisaki, N.; Morken, N.H.; Gissler, M.; Deb-Rinker, P.; Rouleau, J.; Hakansson, S.; Kramer, M.R.; Kramer, M.S. An International Comparison of Death Classification at 22 to 25 Weeks’ Gestational Age. Pediatrics 2018, 142. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Isayama, T. The clinical management and outcomes of extremely preterm infants in Japan: Past, present, and future. Transl. Pediatr. 2019, 8, 199–211. [Google Scholar] [CrossRef]
- Saigal, S.; Doyle, L.W. An overview of mortality and sequelae of preterm birth from infancy to adulthood. Lancet 2008, 371, 261–269. [Google Scholar] [CrossRef]
- Johnson, M.J.; Wootton, S.A.; Leaf, A.A.; Jackson, A.A. Preterm birth and body composition at term equivalent age: A systematic review and meta-analysis. Pediatrics 2012, 130, e640–e649. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Williamson, A.L.; Derado, J.; Barney, B.J.; Saunders, G.; Olsen, I.E.; Clark, R.H.; Lawson, M.L. Longitudinal BMI Growth Curves for Surviving Preterm NICU Infants Based on a Large US Sample. Pediatrics 2018, 142, e20174169. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Baschat, A.A.; Hecher, K. Fetal growth restriction due to placental disease. Semin. Perinatol. 2004, 28, 67–80. [Google Scholar] [CrossRef] [PubMed]
- Victora, C.G.; Adair, L.; Fall, C.; Hallal, P.C.; Martorell, R.; Richter, L.; Sachdev, H.S.; Maternal Child Undernutrition Study Group. Maternal and child undernutrition: Consequences for adult health and human capital. Lancet 2008, 371, 340–357. [Google Scholar] [CrossRef] [Green Version]
- Pallotto, E.K.; Kilbride, H.W. Perinatal outcome and later implications of intrauterine growth restriction. Clin. Obstet. Gynecol. 2006, 49, 257–269. [Google Scholar] [CrossRef] [PubMed]
- Murano, Y.; Shoji, H.; Ikeda, N.; Okawa, N.; Hayashi, K.; Kantake, M.; Morisaki, N.; Shimizu, T.; Gilmour, S. Analysis of Factors Associated With Body Mass Index at Ages 18 and 36 Months Among Infants Born Extremely Preterm. JAMA Netw. Open 2021, 4, e2128555. [Google Scholar] [CrossRef] [PubMed]
- Zeitlin, J.; Ancel, P.Y.; Saurel-Cubizolles, M.J.; Papiernik, E. The relationship between intrauterine growth restriction and preterm delivery: An empirical approach using data from a European case-control study. BJOG 2000, 107, 750–758. [Google Scholar] [CrossRef]
- Shoji, H.; Murano, Y.; Nojiri, S.; Arai, Y.; Awata, K.; Ikeda, N.; Ohkawa, N.; Nishizaki, N.; Suganuma, H.; Hisata, K.; et al. Growth Trajectories during the First 6 Years in Survivors Born at Less Than 25 Weeks of Gestation Compared with Those between 25 and 29 Weeks. J. Clin. Med. 2022, 11, 1418. [Google Scholar] [CrossRef] [PubMed]
- Bhargava, S.K.; Ramji, S.; Kumar, A.; Mohan, M.; Marwah, J.; Sachdev, H.P. Mid-arm and chest circumferences at birth as predictors of low birth weight and neonatal mortality in the community. Br. Med. J. (Clin. Res. Ed.) 1985, 291, 1617–1619. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Landicho, B.; Lechtig, A.; Klein, R.E. Anthropometric indicators of low birth weight. J. Trop. Pediatr. 1985, 31, 301–305. [Google Scholar] [CrossRef]
- Rondo, P.H.; Tomkins, A.M. Chest circumference as an indicator of intrauterine growth retardation. Early Hum. Dev. 1996, 44, 161–167. [Google Scholar] [CrossRef]
- Song, Y.; Zhang, S.; Song, W. Significance of neonatal body indices in identifying fetal macrosomia. J. Perinatol. 2013, 33, 103–106. [Google Scholar] [CrossRef] [PubMed]
- Itabashi, K.; Miura, F.; Uehara, R.; Nakamura, Y. New Japanese neonatal anthropometric charts for gestational age at birth. Pediatr. Int. 2014, 56, 702–708. [Google Scholar] [CrossRef]
- Kato, N.; Murata, M.; Kawano, M.; Taniguchi, T.; Ohtake, T. Growth standard for children from 0 up to 18 years of age. Shonihokenkenkyu 2004, 63, 345–348. [Google Scholar]
- Software for BMI and BMI Percentile SDS. Available online: http://jspe.umin.jp/medical/taikaku.html (accessed on 1 October 2022).
- Salomon, L.J.; Alfirevic, Z.; Berghella, V.; Bilardo, C.; Hernandez-Andrade, E.; Johnsen, S.L.; Kalache, K.; Leung, K.Y.; Malinger, G.; Munoz, H.; et al. Practice guidelines for performance of the routine mid-trimester fetal ultrasound scan. Ultrasound Obstet. Gynecol. 2011, 37, 116–126. [Google Scholar] [CrossRef] [PubMed]
- Sindhu, K.N.; Ramamurthy, P.; Ramanujam, K.; Henry, A.; Bondu, J.D.; John, S.M.; Babji, S.; Koshy, B.; Bose, A.; Kang, G.; et al. Low head circumference during early childhood and its predictors in a semi-urban settlement of Vellore, Southern India. BMC Pediatr. 2019, 19, 182. [Google Scholar] [CrossRef] [Green Version]
- Egashira, T.; Hashimoto, M.; Shiraishi, T.A.; Shichijo, A.; Egashira, M.; Mizukami, T.; Takayanagi, T. A longer body length and larger head circumference at term significantly influences a better subsequent psychomotor development in very-low-birth-weight infants. Brain Dev. 2019, 41, 313–319. [Google Scholar] [CrossRef] [PubMed]
- Bach, C.C.; Henriksen, T.B.; Larsen, R.T.; Aagaard, K.; Matthiesen, N.B. Head circumference at birth and school performance: A nationwide cohort study of 536,921 children. Pediatr. Res. 2020, 87, 1112–1118. [Google Scholar] [CrossRef] [PubMed]
- Gidi, N.W.; Berhane, M.; Girma, T.; Abdissa, A.; Lim, R.; Lee, K.; Nguyen, C.; Russell, F. Anthropometric measures that identify premature and low birth weight newborns in Ethiopia: A cross-sectional study with community follow-up. Arch. Dis. Child. 2020, 105, 326–331. [Google Scholar] [CrossRef] [Green Version]
- Goto, E. Meta-analysis: Identification of low birthweight by other anthropometric measurements at birth in developing countries. J. Epidemiol. 2011, 21, 354–362. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Raymond, E.G.; Tafari, N.; Troendle, J.F.; Clemens, J.D. Development of a practical screening tool to identify preterm, low-birthweight neonates in Ethiopia. Lancet 1994, 344, 524–527. [Google Scholar] [CrossRef]
- Terada, H.; Hoshi, H. Longitudinal study on the physical growth in Japanese. 3. Growth in chest and head circumferences during the first three years of life. Kaibogaku Zasshi 1965, 40, 368–380. [Google Scholar]
- Sundaram, K.R.; Seth, V.; Jena, T.K.; Shukla, D.K. Age at which chest circumference overtakes head circumference in children. Indian J. Pediatr. 1995, 62, 89–94. [Google Scholar] [CrossRef] [PubMed]
- Shoji, H.; Watanabe, A.; Awaji, A.; Ikeda, N.; Hosozawa, M.; Ohkawa, N.; Nishizaki, N.; Hisata, K.; Kantake, M.; Obinata, K.; et al. Intrauterine growth restriction affects z-scores of anthropometric parameters during the first 6 years in very low-birth-weight-children born at less than 30 weeks of gestation. J. Dev. Orig. Health Dis. 2020, 11, 44–48. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Boys | Girls | ||||
|---|---|---|---|---|---|
| All (100) | SGA (30) | All (87) | SGA (23) | ||
| At birth | Gestational age (weeks) | 27.0 ± 1.9 (23.0–29.8) | 27.5 ± 1.7 (24.9–29.9) | 26.5 ± 2.1 (22.4–29.8) | 27.2 ± 1.6 (23.6–29.9) |
| Body weight (g) | 888 ± 260 (338–1462) | 718 ± 190 (338–1104) | 791 ± 261 (328–1426) | 636 ± 191 (328–1072) | |
| Body weight z-scores | −0.9 ± 1.2 (−3.9–1.9) | −2.4 ± 0.8 (−3.9–−1.4) | −0.8 ± 1.3 (−3.4–1.2) | −2.7 ± 0.7 (−3.5–−1.3) | |
| Body length (cm) | 33.8 ± 3.4 (24.0–40.0) | 32.0 ± 3.1 (24.0–40.0) | 32.6 ± 3.7 (25–40.5) | 30.7 ± 3.3 (25–37.8) | |
| Body length z-scores | −0.4 ± 1.1 (−3.6–1.8) | −1.5 ± 1.0 (−3.6–0.4) | −0.6 ± 1.1 (−3.4–1.6) | −2.0 ± 0.7 (−3.4–−0.2) | |
| Head circumference (cm) | 24.4 ± 2.4 (19.6–29) | 23.5 ± 2.0 (20–27.9) | 23.2 ± 2.4 (18.5–30.2) | 22.6 ± 2.1 (18.5–27.0) | |
| Head circumference z-scores | 0.0 ± 0.8 (−3.6–1.8) | −0.8 ± 0.7 (−2.2–0.4) | −0.4 ± 0.8 (−2.3–2.3) | −1.2 ± 0.5 (−2.3–−0.1) | |
| Chest circumference (cm) | 20.4 ± 2.2 (14.0–25.0) | 18.7 ± 1.9 (14.0–23.3) | 19.7 ± 2.3 (15–26.5) | 18.3 ± 2.0 (15–22.5) | |
| HC/CC ratio | 1.2 ± 0.7 (1.1–1.4) | 1.3 ± 0.1 (1.1–1.4) | 1.2 ± 0.1 (1.1–1.4) | 1.2 ± 0.1 (1.1–1.4) | |
| Ponderal index (g/cm3) | 2.2 ± 0.2 (1.6–2.8) | 2.2 ± 0.2 (1.6–2.8) | 2.2 ± 0.2 (1.7–3.0) | 2.1 ± 0.3 (1.7–2.7) | |
| At 6 years | Body weight (g) | 17.8 ± 2.8 (12.9–26) | 16.9 ± 2.7 (12.9–24) | 17.0 ± 2.3 (12.7–26.2) | 16.4 ± 2.0 (12.7–19.4) |
| Body weight z-scores | −0.8 ± 1.2 (−3.2–2.5) | −1.3 ± 1.1 (−3.1–1.2) | −1.0 ± 1.0 (−3.0–2.0) | −1.3 ± 1.0 (−3.0–0.1) | |
| Body height (cm) | 109 ± 4.8 (100–122) | 109 ± 4.9 (100–120) | 109 ± 4.9 (97.4–121) | 107 ± 4.1 (100–115) | |
| Body height z-scores | −0.5 ± 1.0 (−2.4–3.1) | −0.8 ± 0.8 (−2.3–0.9) | −0.7 ± 1.0 (−3.0–2.2) | −0.9 ± 0.9 (−2.5–1.0) | |
| BMI (kg/m2) | 14.7 ± 1.5 (11.4–19.6) | 14.3 ± 1.7 (11.4–19.6) | 14.3 ± 1.2 (11.9–17.9) | 14.1 ± 1.1 (12.5–16.5) | |
| BMI z-scores | −0.7 ± 1.2 (−4.6–2.1) | −1.2 ± 1.5 (−4.6–2.1) | −0.8 ± 1.0 (−3.1–1.3) | −1.0 ± 0.9 (−2.4–0.6) | |
| Variables | Coefficient | 95% CI | p | |
|---|---|---|---|---|
| At birth | ||||
| Body weight z-score | HC/CC ratio | −11.08 | −13.13–−9.03 | <0.01 |
| Gestational age | −0.13 | −0.22–−0.04 | <0.01 | |
| Sex | 0.13 | −0.22–0.04 | 0.73 | |
| Body length z-score | HC/CC ratio | −8.12 | −10.06–−6.19 | <0.01 |
| Gestational age | −0.07 | –0.15–0.01 | 0.08 | |
| Sex | −0.19 | −0.51–0.13 | 0.23 | |
| HC z-score | HC/CC ratio | −2.28 | –3.99–−0.57 | <0.01 |
| Gestational age | 0.04 | −0.02–0.10 | 0.19 | |
| Sex | −0.41 | −0.65–−0.17 | <0.01 | |
| Ponderal index | HC/CC ratio | −5.73 | −10.15–−1.32 | 0.01 |
| Gestational age | −0.16 | −0.32–−0.01 | 0.04 | |
| Sex | −0.25 | −0.88–0.38 | 0.43 | |
| At 6 years | ||||
| Body weight | HC/CC ratio | –2.01 | −4.26–0.24 | 0.08 |
| Gestational age | 0.12 | 0.04–0.19 | <0.01 | |
| Sex | −0.21 | −0.53–0.10 | 0.19 | |
| Body height | HC/CC ratio | −0.92 | −2.97–1.13 | 0.38 |
| Gestational age | 0.07 | 0.00–0.14 | 0.05 | |
| Sex | −0.13 | −0.41–0.16 | 0.39 | |
| BMI z-score | HC/CC ratio | −2.43 | −4.68–−0.18 | 0.03 |
| Gestational age | 0.09 | 0.01–0.17 | 0.02 | |
| Sex | −0.15 | −0.47–0.17 | 0.37 |
| Variables | Coefficient | 95% CI | p | |
|---|---|---|---|---|
| At birth | ||||
| Body weight z-score | HC/CC ratio | −10.91 | −13.06–−8.76 | <0.01 |
| Gestational age | −0.02 | −0.10–0.05 | 0.59 | |
| HC z-score | HC/CC ratio | −2.75 | −4.41–−1.08 | <0.01 |
| Sex | −0.47 | −0.70–−0.23 | <0.01 | |
| Ponderal index | HC/CC ratio | −4.76 | −9.36–−0.15 | 0.04 |
| Gestational age | −0.12 | −0.28–0.04 | 0.15 | |
| At 6 years | ||||
| BMI z-score | HC/CC ratio | −3.45 | −5.75–−1.15 | <0.01 |
| Gestational age | 0.12 | 0.04–0.20 | <0.01 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shoji, H.; Murano, Y.; Saitoh, Y.; Ikeda, N.; Ohkawa, N.; Nishizaki, N.; Hisata, K.; Kantake, M.; Obinata, K.; Yoneoka, D.; et al. Use of Head and Chest Circumference Ratio as an Index of Fetal Growth Retardation in Preterm Infants. Nutrients 2022, 14, 4942. https://doi.org/10.3390/nu14224942
Shoji H, Murano Y, Saitoh Y, Ikeda N, Ohkawa N, Nishizaki N, Hisata K, Kantake M, Obinata K, Yoneoka D, et al. Use of Head and Chest Circumference Ratio as an Index of Fetal Growth Retardation in Preterm Infants. Nutrients. 2022; 14(22):4942. https://doi.org/10.3390/nu14224942
Chicago/Turabian StyleShoji, Hiromichi, Yayoi Murano, Yukika Saitoh, Naho Ikeda, Natsuki Ohkawa, Naoto Nishizaki, Ken Hisata, Masato Kantake, Kaoru Obinata, Daisuke Yoneoka, and et al. 2022. "Use of Head and Chest Circumference Ratio as an Index of Fetal Growth Retardation in Preterm Infants" Nutrients 14, no. 22: 4942. https://doi.org/10.3390/nu14224942