
Parental Self-Efficacy and Child Diet Quality between Ages 2 and 5: The STEPS Study
 , , and
, , and
Abstract
:
1. Introduction
2. Materials and Methods
2.1. Study Design and Subjects
2.2. Outcome Variable: Child Diet Quality
2.3. Parental Self-Efficacy
2.4. Covariates
2.5. Statistical Analysis
3. Results
3.1. Description of Participants
3.2. Parental Self-Efficacy
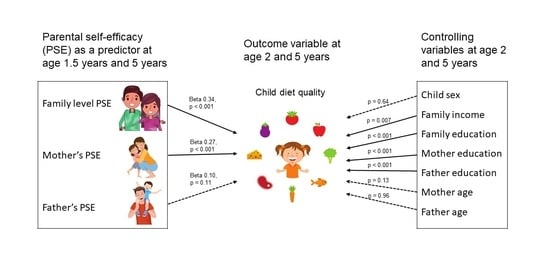
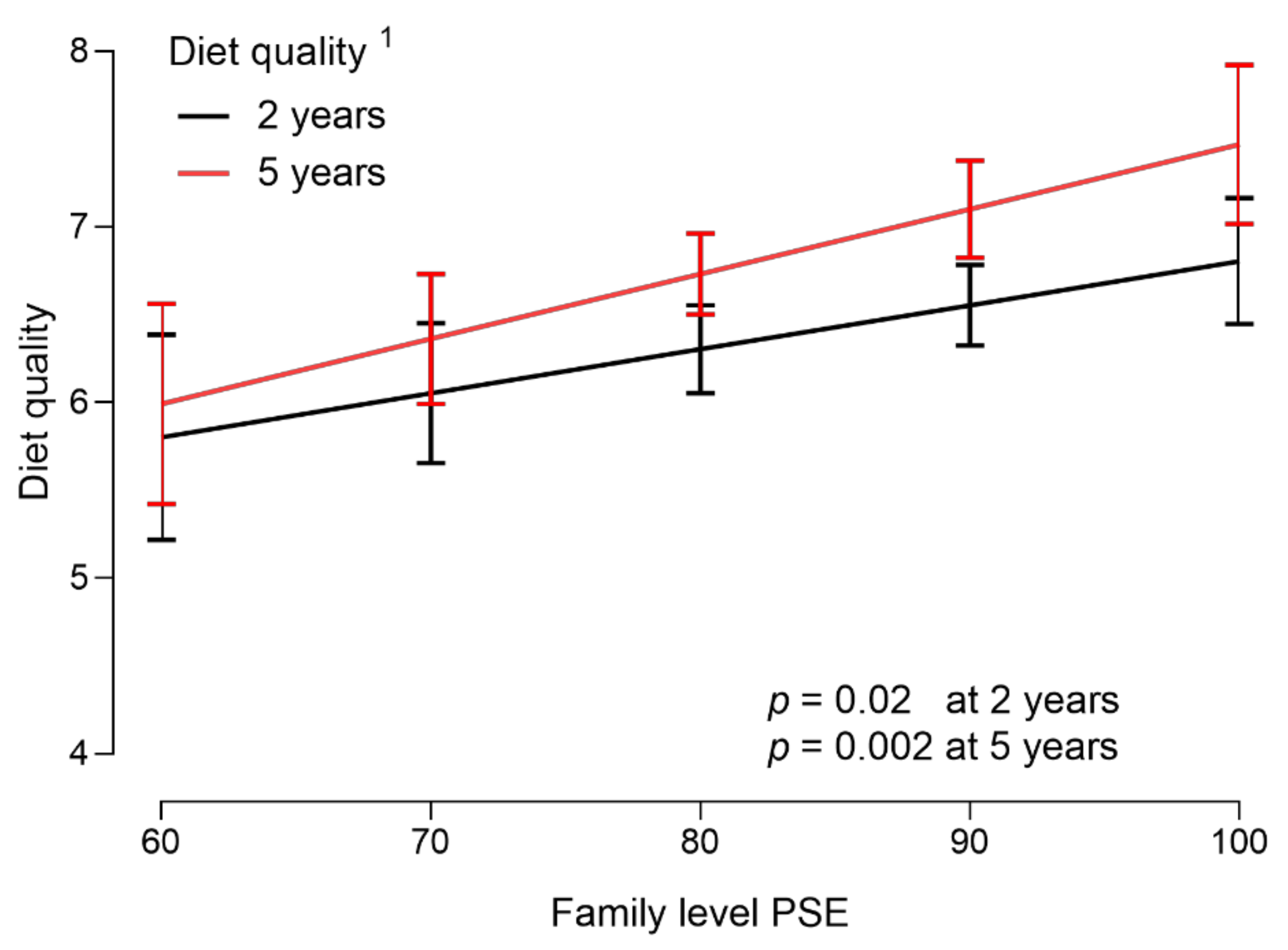
3.3. Association of Diet Quality with Family-Level PSE
3.4. Association of Diet Quality with Mother’s PSE
3.5. Association of Diet Quality with Father’s PSE
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Shrestha, R.; Copenhaver, M. Long-Term Effects of Childhood Risk Factors on Cardiovascular Health During Adulthood. Clin. Med. Rev. Vasc. Health 2015, 7, 1–5. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Saavedra Jose, M.D.A.M. Nutrition in the First 1000 Days of Life: Society’s Greatest Opportunity. In Early Nutrition and Long-Term Health; Woodhead Publishing: Sawston, UK, 2017. [Google Scholar]
- Fleming, T.P.; Watkins, A.J.; Velazquez, M.A.; Mathers, J.C.; Prentice, A.M.; Stephenson, J.; Barker, M.; Saffery, R.; Yajnik, C.S.; Eckert, J.J.; et al. Origins of Lifetime Health around the Time of Conception: Causes and Consequences. Lancet 2018, 391, 1842–1852. [Google Scholar] [CrossRef]
- Saavedra Jose, M.D.A.M. Nutritional and Developmental Appropriateness of Introduction of Foods. In Early Nutrition and Long-Term Health; Woodhead Publishing: Sawston, UK, 2017. [Google Scholar]
- Ventura, A.K.; Birch, L.L. Does Parenting Affect Children’s Eating and Weight Status? Int. J. Behav. Nutr. Phys. Act. 2008, 5, 15. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vepsäläinen, H.; Nevalainen, J.; Fogelholm, M.; Korkalo, L.; Roos, E.; Ray, C.; Erkkola, M.; DAGIS Consortium Group. Like Parent, like Child? Dietary Resemblance in Families. Int. J. Behav. Nutr. Phys. Act. 2018, 15, 62. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Scaglioni, S.; De Cosmi, V.; Ciappolino, V.; Parazzini, F.; Brambilla, P.; Agostoni, C. Factors Influencing Children’s Eating Behaviours. Nutrients 2018, 10, 706. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tuomasjukka, S.; Kyllönen, J.; Ketola, M.; Lagström, H.; Katsaus, A. Ravitsemusohjauksessa on Huomioitava Muutakin Kuin Suositukset. Duodecim 2010, 126, 1295–1302. [Google Scholar] [PubMed]
- Hart, L.M.; Damiano, S.R.; Cornell, C.; Paxton, S.J. What Parents Know and Want to Learn about Healthy Eating and Body Image in Preschool Children: A Triangulated Qualitative Study with Parents and Early Childhood Professionals. BMC Public Health 2015, 15, 596. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Rosso, S.; Ducrot, P.; Chabanet, C.; Nicklaus, S.; Schwartz, C. Increasing Parental Knowledge About Child Feeding: Evaluation of the Effect of Public Health Policy Communication Media in France. Front. Public Health 2022, 10, 326. [Google Scholar] [CrossRef] [PubMed]
- Bandura, A. Self-Efficacy Mechanism in Human Agency. Am. Psychol. 1982, 37, 122–147. [Google Scholar] [CrossRef]
- Coleman, P.K.; Karraker, K.H. Self-Efficacy and Parenting Quality: Findings and Future Applications. Dev. Rev. 1998, 18, 47–85. [Google Scholar] [CrossRef]
- Bandura, A. Self-Efficacy: The Exercise of Control; Freeman: New York, NY, USA, 1997; ISBN 0-7167-2626-2. [Google Scholar]
- Sevigny, P.R.; Loutzenhiser, L. Predictors of Parenting Self-Efficacy in Mothers and Fathers of Toddlers. Child. Care. Health Dev. 2010, 36, 179–189. [Google Scholar] [CrossRef]
- Parekh, N.; Henriksson, P.; Delisle Nyström, C.; Silfvernagel, K.; Ruiz, J.R.; Ortega, F.B.; Pomeroy, J.; Löf, M. Associations of Parental Self-Efficacy With Diet, Physical Activity, Body Composition, and Cardiorespiratory Fitness in Swedish Preschoolers: Results From the MINISTOP Trial. Health Educ. Behav. Off. Publ. Soc. Public Health Educ. 2018, 45, 238–246. [Google Scholar] [CrossRef] [PubMed]
- Möhler, R.; Wartha, O.; Steinacker, J.M.; Szagun, B.; Kobel, S. Parental Self-Efficacy as a Predictor of Children’s Nutrition and the Potential Mediator Effect between the Health Promotion Program “Join the Healthy Boat” and Children’s Nutrition. Int. J. Environ. Res. Public Health 2020, 17, 9463. [Google Scholar] [CrossRef] [PubMed]
- Ice, C.L.; Neal, W.A.; Cottrell, L. Parental Efficacy and Role Responsibility for Assisting in Child’s Healthful Behaviors. Educ. Urban Soc. 2012, 46, 699–715. [Google Scholar] [CrossRef]
- Sagui-Henson, S.; Armstrong, L.; Mitchell, A.; Basquin, C.; Levens, S. The Effects of Parental Emotion Regulation Ability on Parenting Self-Efficacy and Child Diet. J. Child Fam. Stud. 2020, 29, 2290–2302. [Google Scholar] [CrossRef]
- Campbell, K.; Hesketh, K.; Silverii, A.; Abbott, G. Maternal Self-Efficacy Regarding Children’s Eating and Sedentary Behaviours in the Early Years: Associations with Children’s Food Intake and Sedentary Behaviours. Int. J. Pediatr. Obes. 2010, 5, 501–508. [Google Scholar] [CrossRef] [PubMed]
- Koh, G.A.; Scott, J.A.; Woodman, R.J.; Kim, S.W.; Daniels, L.A.; Magarey, A.M. Maternal Feeding Self-Efficacy and Fruit and Vegetable Intakes in Infants. Results from the SAIDI Study. Appetite 2014, 81, 44–51. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Knowlden, A.P.; Sharma, M. Social Cognitive Maternal-Mediated Nutritional Correlates of Childhood Obesity. Int. Q. Community Health Educ. 2015, 35, 177–191. [Google Scholar] [CrossRef]
- Russell, C.G.; Worsley, A. Why Don’t They like That? And Can I Do Anything about It? The Nature and Correlates of Parents’ Attributions and Self-Efficacy Beliefs about Preschool Children’s Food Preferences. Appetite 2013, 66, 34–43. [Google Scholar] [CrossRef] [Green Version]
- Rohde, J.F.; Bohman, B.; Berglind, D.; Hansson, L.M.; Frederiksen, P.; Mortensen, E.L.; Heitmann, B.L.; Rasmussen, F. Cross-Sectional Associations between Maternal Self-Efficacy and Dietary Intake and Physical Activity in Four-Year-Old Children of First-Time Swedish Mothers. Appetite 2018, 125, 131–138. [Google Scholar] [CrossRef]
- Xu, H.; Wen, L.M.; Rissel, C.; Flood, V.M.; Baur, L.A. Parenting Style and Dietary Behaviour of Young Children. Findings from the Healthy Beginnings Trial. Appetite 2013, 71, 171–177. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Spence, A.C.; Campbell, K.J.; Crawford, D.A.; McNaughton, S.A.; Hesketh, K.D. Mediators of Improved Child Diet Quality Following a Health Promotion Intervention: The Melbourne InFANT Program. Int. J. Behav. Nutr. Phys. Act. 2014, 11, 137. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Walsh, A.D.; Hesketh, K.D.; Hnatiuk, J.A.; Campbell, K.J. Paternal Self-Efficacy for Promoting Children’s Obesity Protective Diets and Associations with Children’s Dietary Intakes. Int. J. Behav. Nutr. Phys. Act. 2019, 16, 53. [Google Scholar] [CrossRef] [PubMed]
- Lagström, H.; Rautava, P.; Kaljonen, A.; Räihä, H.; Pihlaja, P.; Korpilahti, P.; Peltola, V.; Rautakoski, P.; Österbacka, E.; Simell, O.; et al. Cohort Profile: Steps to the Healthy Development and Well-Being of Children (the STEPS Study). Int. J. Epidemiol. 2013, 42, 1273–1284. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tarro, S.; Lahdenperä, M.; Vahtera, J.; Pentti, J.; Lagström, H. Diet Quality in Preschool Children and Associations with Individual Eating Behavior and Neighborhood Socioeconomic Disadvantage. The STEPS Study. Appetite 2022, 172, 105950. [Google Scholar] [CrossRef]
- Hasunen, K.; Kalavainen, M.; Keinonen, H.; Lagström, H.A.; Lyytikäinen, A.N.; Terttu Peltola, S.T. The Child, Family and Food. Nutrition Recommendations for Infants and Young Children as Well as Pregnant and Breastfeeding Mothers. Helsinki, Finland: Publications of the Ministry of Social Affairs and Health. CiNii 2004, 11, 254. [Google Scholar]
- Coleman, P.K.; Karraker, K.H. Maternal Self-Efficacy Beliefs, Competence in Parenting, and Toddlers’ Behavior and Developmental Status. Infant Ment. Health J. 2003, 24, 126–148. [Google Scholar] [CrossRef]
- Junttila, N.; Aromaa, M.; Rautava, P.; Piha, J.; Räihä, H. Measuring Multidimensional Parental Self-Efficacy of Mothers and Fathers of Children Ages 1.5 and 3 Years. Fam. Relat. 2015, 64, 665–680. [Google Scholar] [CrossRef]
- Northstone, K.; Emmett, P.; The ALSPAC Study Team. Multivariate Analysis of Diet in Children at Four and Seven Years of Age and Associations with Socio-Demographic Characteristics. Eur. J. Clin. Nutr. 2005, 59, 751–760. [Google Scholar] [CrossRef] [Green Version]
- Van der Velde, L.A.; Nguyen, A.N.; Schoufour, J.D.; Geelen, A.; Jaddoe, V.W.V.; Franco, O.H.; Voortman, T. Diet Quality in Childhood: The Generation R Study. Eur. J. Nutr. 2019, 58, 1259–1269. [Google Scholar] [CrossRef] [Green Version]
- Lazarou, C.; Newby, P.K. Use of Dietary Indexes among Children in Developed Countries. Adv. Nutr. 2011, 2, 295–303. [Google Scholar] [CrossRef]
- Kyttälä, P.; Erkkola, M.; Lehtinen-Jacks, S.; Ovaskainen, M.-L.; Uusitalo, L.; Veijola, R.; Simell, O.; Knip, M.; Virtanen, S.M. Finnish Children Healthy Eating Index (FCHEI) and Its Associations with Family and Child Characteristics in Pre-School Children. Public Health Nutr. 2014, 17, 2519–2527. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Suomen virallinen tilasto (SVT): Syntyneet [verkkojulkaisu]. Available online: http://www.stat.fi/til/synt/meta.html (accessed on 13 October 2022).
- Benedetto, L.; Ingrassia, M. Parental Self-efficacy in Promoting Children Care and Parenting Quality. In Parenting—Empirical Advances and Intervention Resources; Benedetto, L., Ingrassia, M., Eds.; IntechOpen: Rijeka, Croatia, 2017; pp. 31–57. [Google Scholar]
- Wake, M.; Nicholson, J.M.; Hardy, P.; Smith, K. Preschooler Obesity and Parenting Styles of Mothers and Fathers: Australian National Population Study. Pediatrics 2007, 120, e1520–e1527. [Google Scholar] [CrossRef] [PubMed]
- Blissett, J.; Meyer, C.; Haycraft, E. Maternal and Paternal Controlling Feeding Practices with Male and Female Children. Appetite 2006, 47, 212–219. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Möller, E.L.; Majdandžić, M.; de Vente, W.; Bögels, S.M. The Evolutionary Basis of Sex Differences in Parenting and Its Relationship with Child Anxiety in Western Societies. J. Exp. Psychopathol. 2012, 4, 88–117. [Google Scholar] [CrossRef]
- National Institute for Health and Welfare Parenthood and Caregiving in Finland. Available online: https://stm.fi/documents/1271139/5825735/STM_vanhemmuusjahoiva_UK_verkko.pdf/96300958-a813-4166-8469-8c741896d627/STM_vanhemmuusjahoiva_UK_verkko.pdf (accessed on 13 October 2022).
- Matarma, T.; Lagström, H.; Hurme, S.; Tammelin, T.H.; Kulmala, J.; Barnett, L.M.; Koski, P. Motor Skills in Association with Physical Activity, Sedentary Time, Body Fat, and Day Care Attendance in 5-6-Year-Old Children—The STEPS Study. Scand. J. Med. Sci. Sports 2018, 28, 2668–2676. [Google Scholar] [CrossRef]
- Datar, A.; Nicosia, N.; Shier, V. Maternal Work and Children’s Diet, Activity, and Obesity. Soc. Sci. Med. 2014, 107, 196–204. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Smith, K.E.; Haedt-Matt, A.; Dougherty, E.N.; Ivins-Lukse, M.; Goldschmidt, A.B. The Interactive Effects of Parental Self-Efficacy and Child Eating Styles in Relation to Naturalistically-Assessed Craving, Overeating, and Loss of Control Eating. Int. J. Eat. Disord. 2020, 53, 1450–1459. [Google Scholar] [CrossRef] [PubMed]
- Trevino, S.D.; Kelly, N.R.; Budd, E.L.; Giuliani, N.R. Parent Gender Affects the Influence of Parent Emotional Eating and Feeding Practices on Child Emotional Eating. Front. Psychol. 2021, 12, 654237. [Google Scholar] [CrossRef] [PubMed]
- Stone, R.A.; Blissett, J.; Haycraft, E.; Farrow, C. Predicting Preschool Children’s Emotional Eating: The Role of Parents’ Emotional Eating, Feeding Practices and Child Temperament. Matern. Child Nutr. 2022, 18, e13341. [Google Scholar] [CrossRef]
- Buja, A.; Manfredi, M.; Zampieri, C.; Minnicelli, A.; Bolda, R.; Brocadello, F.; Gatti, M.; Baldovin, T.; Baldo, V. Is Emotional Eating Associated with Behavioral Traits and Mediterranean Diet in Children? A Cross-Sectional Study. BMC Public Health 2022, 22, 1794. [Google Scholar] [CrossRef]
- Dubois, L.; Girard, M.; Potvin Kent, M.; Farmer, A.; Tatone-Tokuda, F. Breakfast Skipping Is Associated with Differences in Meal Patterns, Macronutrient Intakes and Overweight among Pre-School Children. Public Health Nutr. 2009, 12, 19–28. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mou, Y.; Jansen, P.W.; Raat, H.; Nguyen, A.N.; Voortman, T. Associations of Family Feeding and Mealtime Practices with Children’s Overall Diet Quality: Results from a Prospective Population-Based Cohort. Appetite 2021, 160, 105083. [Google Scholar] [CrossRef]
- Mahmood, L.; Flores-Barrantes, P.; Moreno, L.A.; Manios, Y.; Gonzalez-Gil, E.M. The Influence of Parental Dietary Behaviors and Practices on Children’s Eating Habits. Nutrients 2021, 13, 1138. [Google Scholar] [CrossRef] [PubMed]
- Couch, S.C.; Glanz, K.; Zhou, C.; Sallis, J.F.; Saelens, B.E. Home Food Environment in Relation to Children’s Diet Quality and Weight Status. J. Acad. Nutr. Diet. 2014, 114, 1569–1579.e1. [Google Scholar] [CrossRef] [Green Version]
- Feldman, S.; Eisenberg, M.E.; Neumark-Sztainer, D.; Story, M. Associations between Watching TV during Family Meals and Dietary Intake Among Adolescents. J. Nutr. Educ. Behav. 2007, 39, 257–263. [Google Scholar] [CrossRef]
- Heerman, W.J.; Taylor, J.L.; Wallston, K.A.; Barkin, S.L. Parenting Self-Efficacy, Parent Depression, and Healthy Childhood Behaviors in a Low-Income Minority Population: A Cross-Sectional Analysis. Matern. Child Health J. 2017, 21, 1156–1165. [Google Scholar] [CrossRef] [Green Version]
- Harpaz, G.; Grinshtain, Y.; Yaffe, Y. Parental Self-Efficacy Predicted by Parents’ Subjective Well-Being and Their Parenting Styles with Possible Role of Help-Seeking Orientation from Teachers. J. Psychol. 2021, 155, 571–587. [Google Scholar] [CrossRef] [PubMed]
- Sanders, M.R.; Woolley, M.L. The Relationship between Maternal Self-Efficacy and Parenting Practices: Implications for Parent Training. Child. Care. Health Dev. 2005, 31, 65–73. [Google Scholar] [CrossRef]
- Watson, A.; Dumuid, D.; Maher, C.; Fraysse, F.; Mauch, C.; Tomkinson, G.R.; Ferguson, T.; Olds, T. Parenting Styles and Their Associations with Children’s Body Composition, Activity Patterns, Fitness, Diet, Health, and Academic Achievement. Child. Obes. 2022. [Google Scholar] [CrossRef]
- Kiefner-Burmeister, A.; Hinman, N. The Role of General Parenting Style in Child Diet and Obesity Risk. Curr. Nutr. Rep. 2020, 9, 14–30. [Google Scholar] [CrossRef] [PubMed]
- Corsini, N.; Wilson, C.; Kettler, L.; Danthiir, V. Development and Preliminary Validation of the Toddler Snack Food Feeding Questionnaire. Appetite 2010, 54, 570–578. [Google Scholar] [CrossRef] [PubMed]
- Duraccio, K.M.; Zaugg, K.K.; Nottingham, K.; Jensen, C.D. Maternal Self-Efficacy Is Associated with Mother-Child Feeding Practices in Middle Childhood. Eat. Behav. 2021, 40, 101475. [Google Scholar] [CrossRef] [PubMed]
- Wittkowski, A.; Garrett, C.; Calam, R.; Weisberg, D. Self-Report Measures of Parental Self-Efficacy: A Systematic Review of the Current Literature. J. Child Fam. Stud. 2017, 26, 2960–2978. [Google Scholar] [CrossRef] [PubMed]
- Bohman, B.; Ghaderi, A.; Rasmussen, F. Psychometric Properties of a New Measure of Parental Self-Efficacy for Promoting Healthy Physical Activity and Dietary Behaviors in Children. Eur. J. Psychol. Assess. 2013, 29, 291–298. [Google Scholar] [CrossRef]
- Norman, Å.; Bohman, B.; Nyberg, G.; Schäfer Elinder, L. Psychometric Properties of a Scale to Assess Parental Self-Efficacy for Influencing Children’s Dietary, Physical Activity, Sedentary, and Screen Time Behaviors in Disadvantaged Areas. Health Educ. Behav. 2017, 45, 132–140. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Norman, Å.; Wright, J.; Patterson, E. Brief Parental Self-Efficacy Scales for Promoting Healthy Eating and Physical Activity in Children: A Validation Study. BMC Public Health 2021, 21, 540. [Google Scholar] [CrossRef] [PubMed]
- Leppälä, J.; Lagström, H.; Kaljonen, A.; Laitinen, K. Construction and Evaluation of a Self-Contained Index for Assessment of Diet Quality. Scand. J. Public Health 2010, 38, 794–802. [Google Scholar] [CrossRef]
- Pierce, T.; Boivin, M.; Frenette, E.; Forget-Dubois, N.; Dionne, G.; Tremblay, R.E. Maternal Self-Efficacy and Hostile-Reactive Parenting from Infancy to Toddlerhood. Infant Behav. Dev. 2010, 33, 149–158. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
| Study Sample | 2 Years | 5 Years | 2 and 5 Years | |
|---|---|---|---|---|
| N | N | N | N | |
| Child diet quality | 1683 * | 785 | 645 | 499 |
| Family-level PSE | 762 | 462 | 371 | |
| Mother’s PSE | 1797 | 883 | 725 | 593 |
| Father’s PSE | 1658 | 770 | 544 | 429 |
| Family-level PSE + Diet quality | 575 | 396 | 270 | |
| Mother’s PSE + Diet quality | 665 | 597 | 411 | |
| Father’s PSE + Diet quality | 581 | 416 | 286 | |
| Variable | Diet Quality 2 | ||||||
|---|---|---|---|---|---|---|---|
| 2 Years | 5 Years | ||||||
| n (%) | Mean (SD) | p | n (%) | Mean (SD) | p | ||
| All | 575 | 6.10 (1.69) | 396 | 6.48 (1.63) | <0.001 | ||
| Sex | Boy | 308 (54%) | 6.17 (1.76) | 0.34 | 206 (52%) | 6.52 (1.63) | 0.64 |
| Girl | 267 (46%) | 6.03 (1.60) | 190 (48%) | 6.45 (1.64) | |||
| Mother age | |||||||
| 17–29 | 227 (40%) | 6.15 (1.61) | 0.55 | 140 (35%) | 6.66 (1.58) | 0.13 | |
| 30–45 | 347 (60%) | 6.06 (1.74) | 256 (65%) | 6.39 (1.65) | |||
| Father age | |||||||
| 17–29 | 155 (27%) | 5.97 (1.68) | 0.25 | 103 (26%) | 6.50 (1.64) | 0.96 | |
| 30–45 | 420 (73%) | 6.15 (1.69) | 293 (74%) | 6.48 (1.63) | |||
| Family income | |||||||
| EUR <3000 | 297 (54%) | 5.91 (1.69) | 0.005 | 135 (34%) | 6.18 (1.62) | 0.007 | |
| EUR ≥3000 | 248 (46%) | 6.32 (1.67) | 258 (66%) | 6.65 (1.62) | |||
| Mother education | |||||||
| Low | 181 (32%) | 5.77 (1.69) | <0.001 | 117 (30%) | 6.01 (1.59) | <0.001 | |
| Advanced | 381 (68%) | 6.29 (1.65) | 276 (70%) | 6.68 (1.62) | |||
| Father education | |||||||
| Low | 267 (48%) | 5.90 (1.62) | 0.007 | 180 (46%) | 6.17 (1.57) | <0.001 | |
| Advanced | 293 (52%) | 6.28 (1.71) | 210 (54%) | 6.77 (1.64) | |||
| Family education 3 | |||||||
| Low | 132 (23%) | 5.60 (1.66) | <0.001 | 83 (21%) | 5.75 (1.47) | <0.001 | |
| Advanced | 436 (77%) | 6.26 (1.67) | 312 (79%) | 6.68 (1.62) | |||
| Number of siblings | |||||||
| 0–1 | 479 (83%) | 6.20 (1.68) | 0.002 | 274 (69%) | 6.57 (1.59) | 0.12 | |
| 2 or more | 96 (17%) | 5.63 (1.68) | 122 (31%) | 6.30 (1.71) | |||
| Variable | 1.5 Years | 5 Years | ||
|---|---|---|---|---|
| n | Mean (SD) | Mean (SD) | p 1 | |
| Family-level PSE | 371 | 84.4 (6.7) | 81.9 (6.8) | <0.001 |
| Presence | 17.3 (1.6) | 16.4 (1.6) | <0.001 | |
| Emotional support | 17.4 (1.4) | 17.4 (1.5) | 0.73 | |
| Routines | 16.9 (1.9) | 17.1 (1.9) | 0.032 | |
| Playing | 15.6 (2.2) | 14.3 (2.4) | <0.001 | |
| Teaching | 17.2 (1.6) | 16.8 (1.6) | <0.001 | |
| Mother’s PSE | 593 | 85.7 (8.0) | 83.1 (9.0) | <0.001 |
| Presence | 17.5 (2.1) | 16.5 (2.5) | <0.001 | |
| Emotional support | 17.8 (1.9) | 17.9 (1.9) | 0.24 | |
| Routines | 17.4 (2.2) | 17.6 (2.3) | 0.06 | |
| Playing | 15.4 (3.0) | 13.8 (3.4) | <0.001 | |
| Teaching | 17.4 (2.1) | 17.2 (2.2) | 0.004 | |
| Father’s PSE | 429 | 83.1 (9.2) | 80.9 (8.9) | <0.001 |
| Presence | 17.1 (2.3) | 16.2 (2.4) | <0.001 | |
| Emotional support | 17.0 (2.1) | 16.8 (2.0) | 0.11 | |
| Routines | 16.2 (2.6) | 16.5 (2.4) | 0.09 | |
| Playing | 15.8 (2.9) | 15.0 (3.0) | <0.001 | |
| Teaching | 17.0 (2.3) | 16.4 (2.3) | <0.001 |
| Variable | Diet Quality 1 | |||||
|---|---|---|---|---|---|---|
| 2 Years | 5 Years | |||||
| n | Estimate (95 % CL) 2 | p | n | Estimate (95 % CL) 2 | p | |
| Family-level PSE | 538 | 0.24 (0.04–0.45) 3 | 0.02 | 392 | 0.37 (0.14–0.60) 3 | 0.002 |
| Presence | 0.08 (−0.03–0.16) | 0.06 | 0.07 (−0.02–0.15) | 0.14 | ||
| Emotional support | −0.02 (−0.12–0.07) | 0.64 | 0.14 (0.04–0.24) | 0.008 | ||
| Routines | 0.09 (0.02–0.17) | 0.01 | 0.16 (0.08–0.24) | <0.001 | ||
| Playing | 0.06 (−0.006–0.12) | 0.08 | 0.08 (0.02–0.15) | 0.01 | ||
| Teaching | 0.12 (0.04–0.21) | 0.004 | 0.08 (−0.02–0.18) | 0.098 | ||
| Mother’s PSE | 615 | 0.32 (0.16–0.49) 3 | 0.001 | 580 | 0.24 (0.09–0.39) 3 | 0.002 |
| Presence | 0.10 (0.04–0.16) | 0.002 | 0.04 (−0.01–0.10) | 0.13 | ||
| Emotional support | 0.04 (−0.03–0.11) | 0.31 | 0.07 (0.009–0.14) | 0.03 | ||
| Routines | 0.08 (0.02–0.14) | 0.009 | 0.11 (0.05–0.16) | <0.001 | ||
| Playing | 0.05 (0.009–0.10) | 0.02 | 0.04 (0.006–0.08) | 0.02 | ||
| Teaching | 0.11 (0.05–0.18) | <0.001 | 0.07 (0.01–0.13) | 0.02 | ||
| Father’s PSE | 537 | 0.09 (−0.07–0.24) 3 | 0.28 | 389 | 0.14 (−0.04–0.32) 3 | 0.13 |
| Presence | 0.01 (−0.05–0.07) | 0.85 | 0.02 (−0.04–0.09) | 0.47 | ||
| Emotional support | −0.03 (−0.10–0.04) | 0.42 | 0.03 (−0.05–0.11) | 0.44 | ||
| Routines | 0.06 (0.01–0.11) | 0.03 | 0.09 (0.02–0.15) | 0.01 | ||
| Playing | 0.03 (−0.02–0.07) | 0.30 | 0.03 (−0.02–0.08) | 0.26 | ||
| Teaching | 0.07 (0.002–0.13) | 0.04 | 0.02 (−0.05–0.09) | 0.62 | ||
| Estimate 1 | p-Value | |||
|---|---|---|---|---|
| Model | PSE | PSE | Age | Age × PSE Interaction |
| Family-level PSE (n = 270) | 0.340 2 | <0.001 | <0.001 | 0.57 |
| Presence | 0.065 | 0.05 | <0.001 | 0.79 |
| Emotional support | 0.069 | 0.07 | <0.001 | 0.27 |
| Routines | 0.14 | <0.001 | <0.001 | 0.52 |
| Playing | 0.069 | 0.006 | <0.001 | 0.38 |
| Teaching | 0.098 | 0.006 | <0.001 | 0.63 |
| Mother’s PSE (n = 411) | 0.265 2 | <0.001 | <0.001 | 0.14 |
| Presence | 0.054 | 0.02 | <0.001 | 0.04 |
| Emotional support | 0.066 | 0.009 | <0.001 | 0.63 |
| Routines | 0.089 | <0.001 | <0.001 | 0.84 |
| Playing | 0.043 | 0.007 | <0.001 | 0.43 |
| Teaching | 0.059 | 0.01 | <0.001 | 0.28 |
| Father’s PSE (n = 286) | 0.104 2 | 0.11 | <0.001 | 0.52 |
| Presence | 0.014 | 0.58 | <0.001 | 0.70 |
| Emotional support | −0.004 | 0.88 | <0.001 | 0.34 |
| Routines | 0.081 | <0.001 | <0.001 | 0.76 |
| Playing | 0.009 | 0.67 | <0.001 | 0.32 |
| Teaching | 0.034 | 0.19 | <0.001 | 0.81 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tarro, S.; Lahdenperä, M.; Junttila, N.; Lampimäki, A.; Lagström, H. Parental Self-Efficacy and Child Diet Quality between Ages 2 and 5: The STEPS Study. Nutrients 2022, 14, 4891. https://doi.org/10.3390/nu14224891
Tarro S, Lahdenperä M, Junttila N, Lampimäki A, Lagström H. Parental Self-Efficacy and Child Diet Quality between Ages 2 and 5: The STEPS Study. Nutrients. 2022; 14(22):4891. https://doi.org/10.3390/nu14224891
Chicago/Turabian StyleTarro, Saija, Mirkka Lahdenperä, Niina Junttila, Antti Lampimäki, and Hanna Lagström. 2022. "Parental Self-Efficacy and Child Diet Quality between Ages 2 and 5: The STEPS Study" Nutrients 14, no. 22: 4891. https://doi.org/10.3390/nu14224891