
Is Responsive Feeding Difficult? A Case Study in Teso South Sub-County, Kenya
Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Collection Tools
2.1.1. Focus Group Discussions (FGDs)
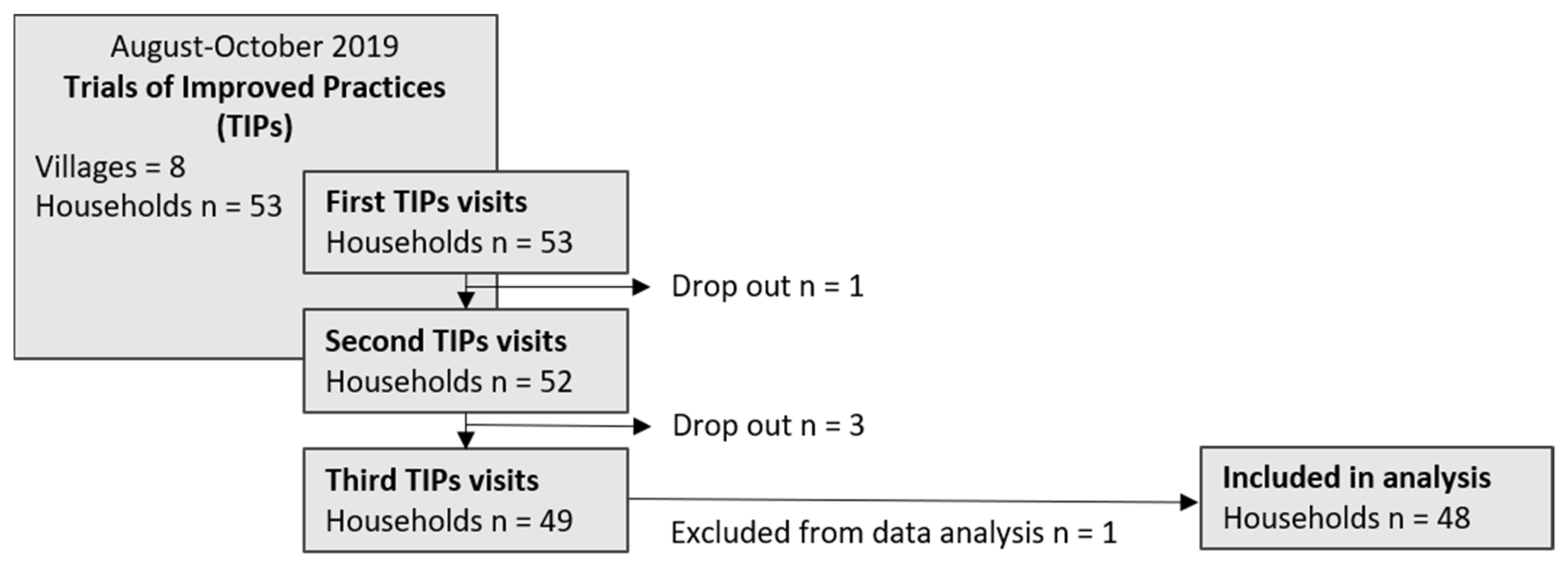
2.1.2. Trials of Improved Practices (TIPs)
2.2. Child Feeding Practices Tested during the Trials of Improved Practices
- “Make child feeding a priority in your household. Serve young children first. Make sure they get and eat their share” [15].
- “Separate the child’s bowl from the mother’s in order to know how much the child has eaten” [15].
- “Interact with the child during mealtimes and actively and lovingly encourage the child to eat; do not force or threaten your child to eat” [15].
2.3. Data Analysis
3. Results
3.1. Main Characteristics of Study Participants
3.2. Common Child Feeding Practices
3.2.1. Serving Priorities within Households during Mealtimes Hinder or Support Adequate Food Intake
“I am served first, my wife serves herself then eldest son to youngest child”.(FGD Men)
“Father [is] served first, then eldest son, then mother and other children come last”.(FGD Youth)
“Youngest child first, older children, my husband and myself”.(FGD Women)
“I serve the youngest child first because she won’t allow other people to eat as she waits, then I serve my husband, other children, then I serve last”.(FGD Women)
“I serve my husband and take his food to the main house then I serve myself and children come later”.(FGD Women)
“I get food on the table so we just eat together as a family”.(FGD Men)
3.2.2. Different Persons Involved in Feeding May Enhance Child’s Food Intake
“There are children who eat well only when they are fed by their fathers”.(FGD Men)
3.2.3. Food Served on a Shared Plate Hinders Adequate Food Intake
3.2.4. Caregiver Strategies for Child’s Food Intake Include Positive and Harmful Practices
“I give him glucose to boost his appetite first”.(FGD Women p7: l.299)
3.3. Implementation Rate of Recommendations
“[The] child [is] still small and cannot feed on its own”.(woman, 32 yr (with child, 1 yr))
“The child completely refused to take porridge”.(woman, 45 yr (with child, 7 yr))
“Serving starts from the oldest to the youngest”.(woman, 27 yr (with child, 4 yr))
“It is too much work having two plates at once since I eat with my son at the same time”.(woman, 26 yr (with child, 2 yr))
“[I am] willing to try that since I am the one who serves the meals”.(woman, 27 yr (with child, 4 yr))
“willing to do so because [they] now understand[] the importance of child feeding”.(woman, 27 yr (with child, 4 yr))
“[I] always wants to serve my husband first because of respect”.(woman, 32 yr (with child, 1 yr))
“even though she serves the husband first, the child still gets adequate share of the meal”.(woman, 32 yr (with child, 5 yr))
“[I] sometimes also feels bad about doing it and also beating had negative effects on child feeding”.(woman, 52 yr (with child, 7 yr))
“I don’t like when the child cries after seeing my husband eating food before her”.(woman, 30 yr (with child, 4 yr))
“When the children are served first, they don’t have to disturb their father”.(woman, 37 yr (with child, 2 yr))
“Since the child started eating from his own bowl, he has really improved and added some kilos”.(woman, 26 yr (with child, 2 yr))
3.4. Households’ Reflection of Experiences Made during TIPs
4. Discussion
4.1. Persons Involved in Feeding
4.2. Serving Priorities during Mealtimes
4.3. Caregivers’ Strategies for Children’s Food Intake
4.4. Reactions and Influence of Children
“The child eats even better than when force was being used during meals”.(woman, 27 yr (with child, 4 yr))
4.5. Lifestyle and Daily Routines
4.6. Perceptions and Tradition
4.7. Positive Outcomes of the Improved Responsive Feeding Practices
4.8. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Birch, L.L.; Fisher, J.A. Appetite and Eating Behavior in Children. Pediatr. Clin. North Am. 1995, 42, 931–953. [Google Scholar] [CrossRef]
- Liu, Y.H.; Stein, M.T. Feeding Behaviour of Infants and Young Children and Its Impact on Child Psychosocial and Emotional Development, 2nd ed.; Encyclopedia on Early Childhood Development: La Jolla, CA, USA, 2013; pp. 1–7. [Google Scholar]
- Patrick, H.; Nicklas, T.A.; Hughes, S.O.; Morales, M. The Benefits of Authoritative Feeding Style: Caregiver Feeding Styles and Children’s Food Consumption Patterns. Appetite 2005, 44, 243–249. [Google Scholar] [CrossRef]
- Schwartz, C.; Scholtens, P.A.M.J.; Lalanne, A.; Weenen, H.; Nicklaus, S. Development of Healthy Eating Habits Early in Life. Review of Recent Evidence and Selected Guidelines. Appetite 2011, 57, 796–807. [Google Scholar] [CrossRef]
- Habron, J.; Booley, S.; Najaar, B.; Day, C. Responsive Feeding: Establishing Healthy Eating Behaviour Early on in Life. South Afr. J. Clin. Nutr. 2013, 26 (Suppl. 3), 141–149. [Google Scholar]
- Guiding Principles for Complementary Feeding of the Breastfed Child; PAHO: Washington, DC, USA, 2003; p. 40.
- WHO Infant and Young Child Feeding. Available online: https://www.who.int/news-room/fact-sheets/detail/infant-and-young-child-feeding (accessed on 3 November 2022).
- KNBS; Kenya National Bureau of Statistics; Ministry of Health; Kenya; National AIDS Control Council; Kenya; Kenya Medical Research Institute; National Council for Population and Development Kenya. Kenya Demographic and Health Survey 2014; Republic of Kenya, Kenya National Bureau of Statistics: Nairobi, Kenya, 2015.
- de Onis, M.; Borghi, E.; Arimond, M.; Webb, P.; Croft, T.; Saha, K.; De-Regil, L.M.; Thuita, F.; Heidkamp, R.; Krasevec, J.; et al. Prevalence Thresholds for Wasting, Overweight and Stunting in Children under 5 Years. Public Health Nutr. 2019, 22, 175–179. [Google Scholar] [CrossRef] [Green Version]
- Waswa, L.M.; Jordan, I.; Herrmann, J.; Krawinkel, M.B.; Keding, G.B. Community-Based Educational Intervention Improved the Diversity of Complementary Diets in Western Kenya: Results from a Randomized Controlled Trial. Public Health Nutr. 2015, 18, 3406–3419. [Google Scholar] [CrossRef] [Green Version]
- Wawire, S. Complementary Feeding Practices: Using Trial for Improved Practice (TIPs) to Improve Complementary Feeding in Migori and Kisumu, Kenya; USAID: Washington, DC, USA, 2017.
- Wawire, S.; Ahoya, B.; Gathi, C.; Kavle, J.; Odero, E.; Ogutu, K.; Muniko, T.; Straubinger, S. A Counseling Guide for Complementary Feeding for Children 6-23 Months in Kisumu and Migori, Kenya; USAID: Washington, DC, USA; MCSP: Washington DC, USA; Nairobi, Kenya, 2017; p. 36.
- BLE EaTSANE Projekt (Teilprojekt 2). Available online: https://service.ble.de/ptdb/index2.php?detail_id=536951&site_key=141&stichw=Eatsane&zeilenzahl_zaehler=2#newContent (accessed on 6 October 2019).
- BLE EaTSANE Projekt (Teilprojekt 1). Available online: https://service.ble.de/ptdb/index2.php?detail_id=535051&site_key=141&stichw=Eatsane&zeilenzahl_zaehler=2#newContent (accessed on 6 October 2019).
- Kretz, E.; Jordan, I.; Itaru, A.; Glas, M.G.; Fischer, S.; Pircher, T.; Hilger, T.; Waswa, L.M. Determinants of Children’s Fruit Intake in Teso South Sub-County, Kenya—A Multi-Phase Mixed Methods Study among Households with Children 0–8 Years of Age. Nutrients 2021, 13, 2417. [Google Scholar] [CrossRef]
- Jordan, I.; Röhlig, A.; Glas, M.G.; Waswa, L.M.; Mugisha, J.; Krawinkel, M.B.; Nuppenau, E.-A. Dietary Diversity of Women across Agricultural Seasons in the Kapchorwa District, Uganda: Results from a Cohort Study. Foods 2022, 11, 344. [Google Scholar] [CrossRef]
- Krueger, R.A.; Casey, M.A. Focus Groups: A Practical Guide for Applied Research, 5th ed.; SAGE: Thousand Oaks, CA, USA, 2015; ISBN 978-1-4833-6524-4. [Google Scholar]
- The Manoff Group Trials of Improved Practices (TIPs)—Giving Participants a Voice in Program Design. Available online: https://www.manoffgroup.com/wp-content/uploads/summarytips.pdf (accessed on 8 July 2019).
- Dickin, K.; Griffiths, M.; Piwoz, E. Designing by Dialogue—A Program Planners’ Guide to Consultative Research for Improving Young Child Feeding; Academy for Educational Development with Support by the USAID Bureau for Africa’s Health and Human Resources Analysis for Africa (HHRAA): Washington, DC, USA, 1997.
- Mayring, P. Qualitative Content Analysis: Theoretical Foundation, Basic Procedures and Software Solution; GESIS and SSOAR: Klagenfurt, Austria, 2014; Available online: https://nbn-resolving.org/urn:nbn:de:0168-ssoar-395173 (accessed on 3 November 2022).
- Burrows, T.; Collins, C.; Adam, M.; Duncanson, K.; Rollo, M. Dietary Assessment of Shared Plate Eating: A Missing Link. Nutrients 2019, 11, 789. [Google Scholar] [CrossRef] [Green Version]
- Engle, P.L.; Nieves, I. Intra-Household Food Distribution among Guatemalan Families in a Supplementary Feeding Program: Behavior Patterns. Soc. Sci. Med. 1993, 36, 1605–1612. [Google Scholar] [CrossRef]
- Shankar, A.V.; Gittelsohn, J.; West, K.P.; Stallings, R.; Gnywali, T.; Faruque, F. Eating from a Shared Plate Affects Food Consumption in Vitamin A-Deficient Nepali Children. J. Nutr. 1998, 128, 1127–1133. [Google Scholar] [CrossRef]
- Uwaezuoke, S.N.; Kenechukwu, K.I.; Nwolisa, C.E.; Ndu, I.K.; Eneh, C.E. Picky Eating in Preschool-Aged Children: Prevalence and Mothers? Perceptions in South-East Nigeria. Curr. Pediatr. Res. 2016. Available online: https://www.currentpediatrics.com/articles/articles/picky-eating-in-preschoolaged-children-prevalence-and-mothers-perceptionsin-southeast-nigeria.html (accessed on 3 November 2022).
- Silva, G.A.P.; Costa, K.A.O.; Giugliani, E.R.J. Infant Feeding: Beyond the Nutritional Aspects. J. Pediatr. (Rio. J.) 2016, 92, S2–S7. [Google Scholar] [CrossRef] [Green Version]
- Pelto, G.H.; Levitt, E.; Thairu, L. Improving Feeding Practices: Current Patterns, Common Constraints, and the Design of Interventions. Food Nutr. Bull. 2003, 24, 45–82. [Google Scholar] [CrossRef]
- Aubel, J. The Role and Influence of Grandmothers on Child Nutrition: Culturally Designated Advisors and Caregivers. Matern. Child Nutr. 2012, 8, 19–35. [Google Scholar] [CrossRef]
- Muehlhoff, E.; Wijesinha-Bettoni, R.; Westaway, E.; Jeremias, T.; Nordin, S.; Garz, J. Linking Agriculture and Nutrition Education to Improve Infant and Young Child Feeding: Lessons for Future Programmes. Matern. Child Nutr. 2017, 13, e12411. [Google Scholar] [CrossRef] [Green Version]
- Gittelsohn, J. Opening the Box: Intrahousehold Food Allocation in Rural Nepal. Soc. Sci. Med. 1991, 33, 1141–1154. [Google Scholar] [CrossRef]
- Fadare, O.; Mavrotas, G.; Akerele, D.; Oyeyemi, M. Micronutrient-Rich Food Consumption, Intra-Household Food Allocation and Child Stunting in Rural Nigeria. Public Health Nutr. 2019, 22, 444–454. [Google Scholar] [CrossRef]
- Daniels, L.A. Feeding Practices and Parenting: A Pathway to Child Health and Family Happiness. Ann. Nutr. Metab. 2019, 74, 29–42. [Google Scholar] [CrossRef]
- Williams, P.A.; Schnefke, C.H.; Flax, V.L.; Nyirampeta, S.; Stobaugh, H.; Routte, J.; Musanabaganwa, C.; Ndayisaba, G.; Sayinzoga, F.; Muth, M.K. Using Trials of Improved Practices to Identify Practices to Address the Double Burden of Malnutrition among Rwandan Children. Public Health Nutr. 2019, 22, 3175–3186. [Google Scholar] [CrossRef]
- Bekele, H.; Turyashemererwa, F. Feasibility and Acceptability of Food-based Complementary Feeding Recommendations Using Trials of Improved Practices among Poor Families in Rural Eastern and Western Uganda. Food Sci. Nutr. 2019, 7, 1311–1327. [Google Scholar] [CrossRef] [Green Version]
- Cooke, L.J.; Wardle, J.; Gibson, E.L.; Sapochnik, M.; Sheiham, A.; Lawson, M. Demographic, Familial and Trait Predictors of Fruit and Vegetable Consumption by Pre-School Children. Public Health Nutr. 2004, 7, 295–302. [Google Scholar] [CrossRef]
- Ha, P.B.; Bentley, M.E.; Pachón, H.; Sripaipan, T.; Caulfield, L.E.; Marsh, D.R.; Schroeder, D.G. Caregiver Styles of Feeding and Child Acceptance of Food in Rural Viet Nam. Food Nutr. Bull. 2002, 23, 95–100. [Google Scholar] [CrossRef] [Green Version]
- Momsen, J.H. Women and Development in the Third World; Routledge Introductions to Development; Routledge: London, UK; New York, NY, USA, 1991; ISBN 978-0-415-01695-7. [Google Scholar]
- Jones, A.D.; Cruz Agudo, Y.; Galway, L.; Bentley, J.; Pinstrup-Andersen, P. Heavy Agricultural Workloads and Low Crop Diversity Are Strong Barriers to Improving Child Feeding Practices in the Bolivian Andes. Soc. Sci. Med. 2012, 75, 1673–1684. [Google Scholar] [CrossRef] [Green Version]
- Wyatt, A.J.; Yount, K.M.; Null, C.; Ramakrishnan, U.; Webb Girard, A. Dairy Intensification, Mothers and Children: An Exploration of Infant and Young Child Feeding Practices among Rural Dairy Farmers in Kenya. Matern. Child Nutr. 2015, 11, 88–103. [Google Scholar] [CrossRef]
- Contento, I.R. Nutrition Education: Linking Research, Theory, and Practice, 3rd ed.; Jones & Bartlett Learning: Burlington, MA, USA, 2016; ISBN 978-1-284-07800-8. [Google Scholar]
- Lokossou, Y.U.A.; Tambe, A.B.; Azandjèmè, C.; Mbhenyane, X. Socio-Cultural Beliefs Influence Feeding Practices of Mothers and Their Children in Grand Popo, Benin. J. Health Popul. Nutr. 2021, 40, 33. [Google Scholar] [CrossRef]
- Chakona, G. Social Circumstances and Cultural Beliefs Influence Maternal Nutrition, Breastfeeding and Child Feeding Practices in South Africa. Nutr. J. 2020, 19, 47. [Google Scholar] [CrossRef]
- Zhang, X.; Rosenthal, D.M.; Benton, L.; Lakhanpaul, M. Cultural Influences on Complementary Feeding Beliefs amongst New Chinese Immigrant Mothers in England: A Mixed Methods Study. Int. J. Environ. Res. Public Health 2020, 17, 5468. [Google Scholar] [CrossRef]
- Chiutsi-Phiri, G.; Heil, E.; Kalimbira, A.A.; Masangano, C.; Mtimuni, B.M.; Krawinkel, M.B.; Jordan, I. Reduced Morbidity Motivated Adoption of Infant and Young Child Feeding Practices after Nutrition Education Intervention in Rural Malawi. Ecol. Food Nutr. 2017, 56, 329–348. [Google Scholar] [CrossRef]
- Heller, R.L.; Mobley, A.R. Instruments Assessing Parental Responsive Feeding in Children Ages Birth to 5 Years: A Systematic Review. Appetite 2019, 138, 23–51. [Google Scholar] [CrossRef]
- Podsakoff, P.M.; MacKenzie, S.B.; Lee, J.-Y.; Podsakoff, N.P. Common Method Biases in Behavioral Research: A Critical Review of the Literature and Recommended Remedies. J. Appl. Psychol. 2003, 88, 879–903. [Google Scholar] [CrossRef]


{kind=link}
| Reason | Explanation | Example | <2 yrs1 | >2 yrs2 |
|---|---|---|---|---|
| Reasons for a shared plate | ||||
| Tradition | It was stated that it was a common way to eat, as it had always been practiced. | “[Children] never had own plates” (FGD Men p4: l.164 col.1); “[They share the] same plate with me since they are my children” (FGD Men p4: l.183–184 col.2). | √ | √ |
| Age | Children were perceived to be too young to eat from a separate plate. | “Because they are young” (FGD Men p4: l.162 col.1) | √ | |
| Eating well | Better food intake by the child was attributed to the practice. | “When children eat with their mother from the same plate they will eat well” (FGD Women p5: l.199–201 col.1) | √ | |
| Assistance | The practice was stated to enable the mother to help her child eat, which she could easily do this way. | “I eat with him from the same plate so that I can help him feed” (FGD Women p5: l.202–203 col.1) | √ | |
| Training | Children were assumed to be trained by the practice in terms of social behavior. | “Eats with other people from the same plate so that he/she doesn’t become mean” (FGD Women p5: l.195–197 col.2) | √ | |
| Reasons for a separate plate | ||||
| Age | Children were perceived to be too young to share a plate or old enough to eat from a separate one. | “We feel she is still too young to eat from our plates.” (FGD Men p4: l.171–173 col.1) | √ | √ |
| Ability | Children were perceived to be able to eat by themselves. | “Because they can eat by themselves” (FGD Men p5: l.188 col.2); “If they can pick by themselves, they are served on their own plate” (FGD Men p4: l.181–182 col.1). | √ | √ |
| Less pressure | The inability to eat on their own in a timely manner was assumed to put children under pressure when a plate was shared with others, e.g., older children. | “Because if served on the same plate with others they will finish for him” (FGD Women p5: l.219–221 col.1); “Because if he/she shares with other people he eats very fast” (FGD Youth p5: l.237–238 col.2). | √ | √ |
| Cooling the food | It was stated that the food should cool on a separate plate before being served to the child. | “So that the food cools down a little bit” (FGD Women p5: l.208–209 col.2); “It shouldn’t burn [the child]” (FGD Women p5: l.205–206 col.1). | √ | √ |
| Preference of the child | Children were assumed to prefer their own plate or to be used to it. | “He cries if you don’t serve him food from his own plate” (FGD Men p4: l.178–179 col.1) | √ | √ |
| Assistance | Children were perceived to need assistance, which was provided. | “Because he can’t share with others and can’t feed by himself” (FGD Women p5: l.207–209 col.1) | √ | |
| Vulnerability | It was assumed that young children were too vulnerable to share a plate because of a susceptibility to infections. | “Because they are very sensitive and so they should be served from their own plates” (FGD Men p5: l.191–193 col.1) | √ | |
| Portion size | Children were assumed to need to be served only a small portion size. | “Because he needs to eat little” (FGD Women p5: l.204–205 col.1) | √ | |
| Time saving | Allowing the child to eat independently from his/her own plate was experienced as a time saver for the caregiver. | “Because he eats while playing thus taking too much time” (FGD Women p5: l.216–217 col.2) | √ | |
| Training | Children were assumed to be trained how to eat independently. | “As to make them used to their food in their plates” (FGD Men p4: l.163–164 col.2) | √ | |
| Hygiene | Sharing a plate was seen as a hygienic problem when children partook in a communal meal. | “Sometimes they have a running nose and they pick their nose as they eat and even play in the midst of eating” (FGD Men p4: l.172–175 col.2) | √ | |
| Strategy | Explanation | Example |
|---|---|---|
| 1. Encouragement | ||
| Provide company | Company was provided by family members or friends who sat with the child and motivated her/ him to eat. | “I call her friends and since they eat, she also eats” (FGD Men p6: l.270) |
| Show care and affection | A positive effect on the child’s eating behavior was experienced by showing love and affection to the child. | “I wash the baby, soothe him a little bit then he will eat” (FGD Youth p7: l.331–332) |
| Reward the child | The child was rewarded for a good eating behavior. | “I show her what she likes and promise to give it to her only if she eats” (FGD Youth p7: l.334–335) |
| 2. Search for alternatives | ||
| Provide other foods | Caregivers provided extra foods that the child was more likely to eat or mixed disliked foods with the child’s favorite ones. | “I provide other alternatives that they like” (FGD Men p6: l.273) |
| Feed frequently small meals | The child was frequently fed small meals. | “I give small frequent meals” (FGD Men p6: l.283) |
| Let other people feed | Instead of the mother herself, another person took over the feeding. | “I let other people feed him because he doesn’t eat well whenever I am the one feeding him” (FGD Women p7: l.317–318) |
| Feed only when hungry | Caregivers waited to feed the child until she/he was hungry and subsequently ate voluntarily. | “I let her play until becomes hungry and then she will eat” (FGD Women p7: l.306) |
| Boost the appetite | Caregivers tried to boost the child’s appetite by offering sugar or multivitamins. | “I give him glucose to boost his appetite first” (FGD Women p7: l.299) |
| 3. Violent behavior | ||
| Force | Caregivers forced the child to eat, in particular when porridge was fed to the child. | “I force them to eat porridge from my palm” (FGD Women p7: l.300) |
| Beating | Caregivers reported beating the child if they refused to eat. | “I beat them up until they take the porridge or eat the food” (FGD Women p7: l.301) |
| Threatening | Caregivers threatened the child with a punishment that included beating or withholding favorite things. | “I scare him/her with a cane” (FGD Men p6: l.276) |
| 4. Lures | ||
| False promises | False promises were mentioned as a way to lure the child to eat well. | “I lie to her that if she eats her food, I will buy her mandazi” (FGD Women p7: l.324) (note: mandazi is an African donut) |
| 5. Others | ||
| Observe and try to solve the problem | Caregivers observed the child to find out about underlying problems that could be addressed. | “I find out why my child doesn’t want to eat and then address the problem, e.g., when sick, I take him for medicine” (FGD Men p7: l.284–285) |
| Inadequate Practice | HH with Inadequate Practice | Recommended Improved Practice [15] | HH Implementing the Improved Practice | HH Modifying the Improved Practice | HH Planning to Continue with the Improved Practice |
|---|---|---|---|---|---|
| n | n (%) | n (%) | n (%) | ||
| Children are not given priority when food is served; husband is served first. | 10 | Make child feeding a priority in your household. Serve young children first. Make sure they get and eat their share. | 10 (100%) | 3 (30%) | 5 (50%) |
| The child is fed from the mother’s plate; children share one plate. | 4 | Separate the child’s bowl from the mother’s in order to know how much the child has eaten. | 4 (100%) | 0 (0%) | 3 (75%) |
| The child is forced to eat; the child is left alone to eat. | 4 | Interact with the child during mealtimes and actively and lovingly encourage her/him to eat; do not force or threaten your child to eat. | 4 (100%) | 0 (0%) | 2 (50%) |
| Experiences and Perceptions Regarding the Changes Made in Child Feeding Practices | Example | Mentioned by Women | Mentioned by Men |
|---|---|---|---|
| Child’s food intake | |||
| Child is eating on her/his own without force. | “My child is eating at his own without being forced” (W_FGD Women1 p2: l.71–72 col.2) | √ | |
| Mother is able to monitor the child’s food intake. | “I did not know how much my child could eat but right now am sure of how much he is eating” (W_FGD Women1 p4: l.143–146 col.2) | √ | |
| Health effects on the child | |||
| Child is healthier. | “The bigger children were finishing food for the smaller one and his health was not good but now he feeds slowly at his own pace and the body is ok” (W_FGD Women2 p5: l.217–222 col.2) | √ | √ |
| Child’s behavior | |||
| Child is satisfied. | “I used to force my child to eat but nowadays I negotiate with my child and even help him feed. The child used to cry even sleeps without eating but nowadays he eats very well knowing the next day he will get a good meal” (W_FGD Women2 p5: l.205–208 col.1 and 2) | √ | √ |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kretz, E.C.; Itaru, A.; Glas, M.G.; Waswa, L.M.; Jordan, I. Is Responsive Feeding Difficult? A Case Study in Teso South Sub-County, Kenya. Nutrients 2022, 14, 4677. https://doi.org/10.3390/nu14214677
Kretz EC, Itaru A, Glas MG, Waswa LM, Jordan I. Is Responsive Feeding Difficult? A Case Study in Teso South Sub-County, Kenya. Nutrients. 2022; 14(21):4677. https://doi.org/10.3390/nu14214677
Chicago/Turabian StyleKretz, Eleonore C., Annet Itaru, Maria Gracia Glas, Lydiah Maruti Waswa, and Irmgard Jordan. 2022. "Is Responsive Feeding Difficult? A Case Study in Teso South Sub-County, Kenya" Nutrients 14, no. 21: 4677. https://doi.org/10.3390/nu14214677