
Relationship between Nutritional Status, Food Consumption and Sarcopenia in Post-Stroke Rehabilitation: Preliminary Data

 ,
,  , , ,
, , ,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Participants
2.2. Rehabilitation Treatment
2.3. Clinical Assessment and Activity of Daily-Living Assessment
2.4. Malnutritional Risk Screening
2.5. Nutritional Status Assessment
- (i).
- Anthropometric measurements comprised body height and weight evaluations. Height was recorded at T0 in all patients able to stand, reporting data in meters (m), up to the nearest 0.1 cm. In other cases, the referred height was recorded and checked with the knee-height [31]. Body weight was checked at T0 and T1, as well as weekly, for monitoring any consistent weight changes. Weight was evaluated to the nearest 0.1 kg on a calibrated weighing scale or, for non-autonomous patients, on a weighing chair. Measurements were taken after overnight fasting in the morning, without heavy clothing or shoes. The Body Mass Index (BMI) at T0 and at T1 was then calculated and expressed in kg/m2.
- (ii).
- (iii).
- We estimated the amount of food intake during the 6 weeks of study, through the visual estimation of plate waste [34,35,36]. The meals were formulated and prepared by the company canteen, according to the Italian guidelines “National Recommended Energy and Nutrient Intake Levels for the Italian population” (LARN, [37]). For dysphagic patients, the meals were served as texture-modified food, or fluid. The nurses and speech therapists reported the meal waste (breakfast, lunch, and dinner), for 6 days a week, for 6 weeks (108 meals in total for each patient), assigning a score from 0 to 4 on a 5-point scale (0 = none wasted; 1= ¼, 2 = ½, 3 =¾, and 4 = all wasted). The daily average plate-waste score was then calculated for all the meals consumed (n = 108) for all patients.
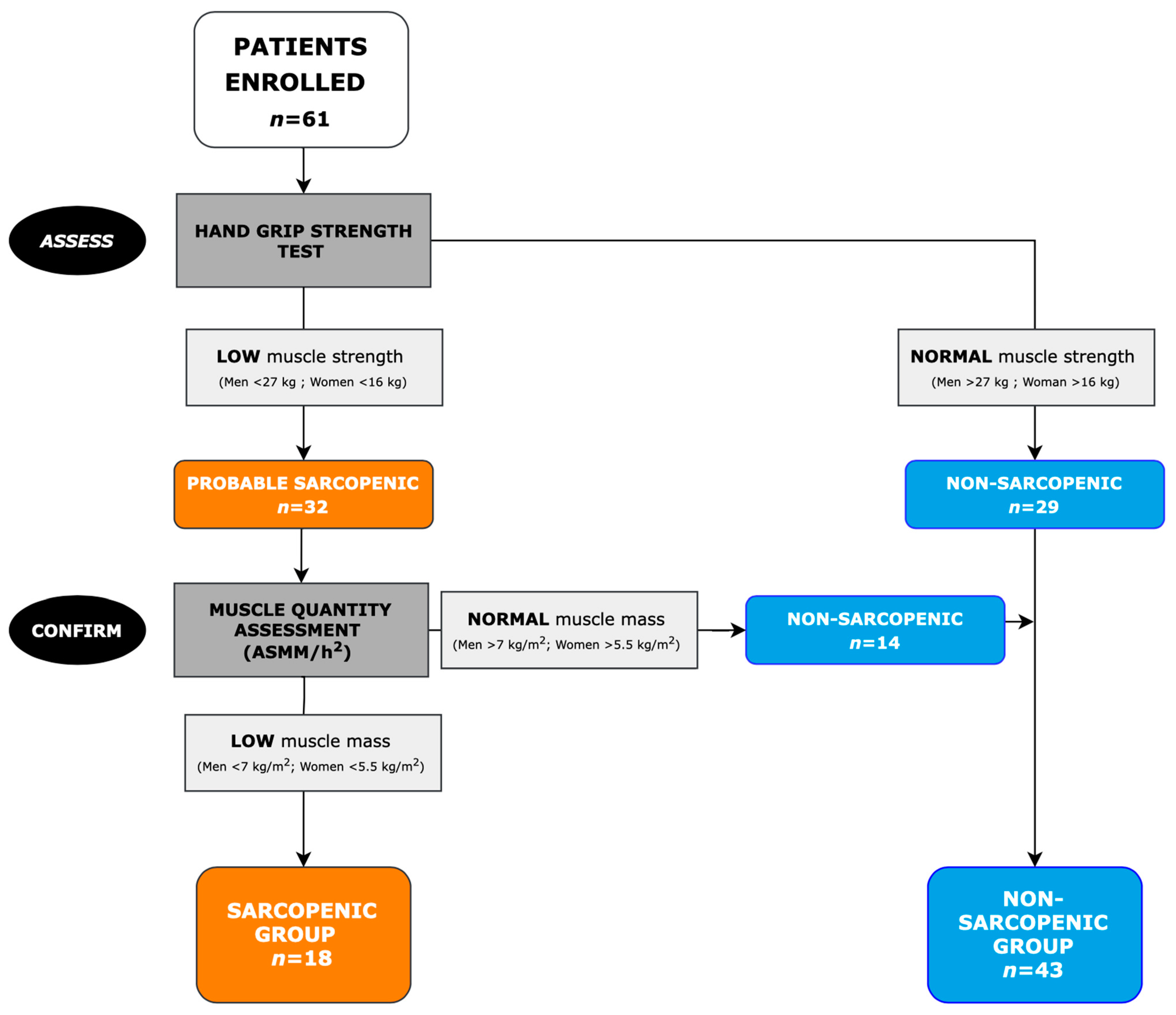
2.6. Sarcopenia Assessment
- Muscle-strength observation.
- Evaluation of muscle quantity.
2.7. Statistical Analysis
3. Results
3.1. Participants and Baseline Characteristics
3.2. Sarcopenia Analysis
3.3. Nutritional Status
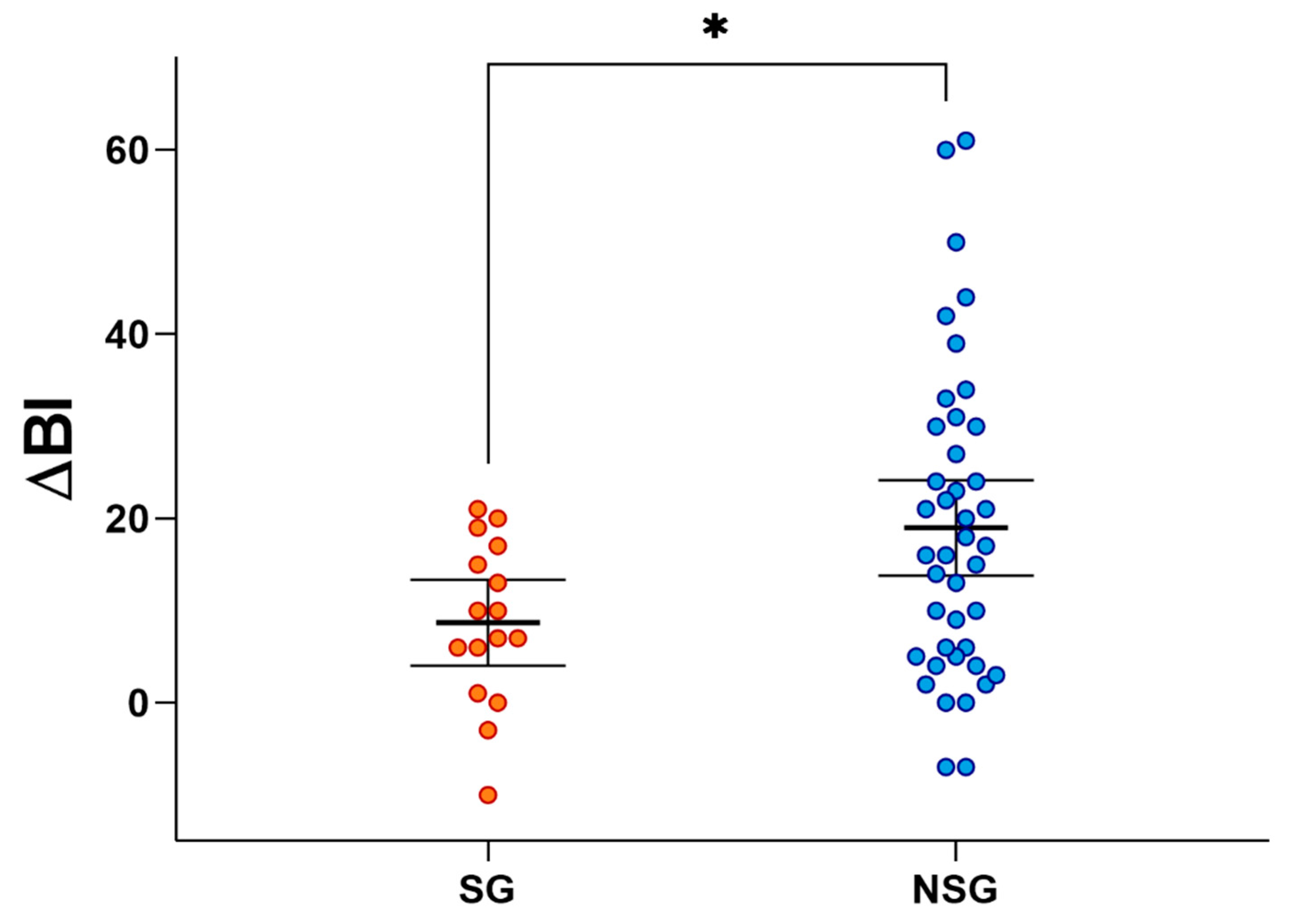
3.4. Functional Recovery
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Kim, J.; Thayabaranathan, T.; Donnan, G.A.; Howard, G.; Howard, V.J.; Rothwell, P.M.; Feigin, V.; Norrving, B.; Owolabi, M.; Pandian, J.; et al. Global Stroke Statistics 2019. Int. J. Stroke 2020, 15, 819–838. [Google Scholar] [CrossRef] [PubMed]
- Go, A.S.; Mozaffarian, D.; Roger, V.L.; Benjamin, E.; Berry, J.D.; Blaha, M.J.; Dai, S.; Ford, E.S.; Fox, C.S.; Franco, S.; et al. Executive Summary: Heart Disease and Stroke Statistics—2014 Update. Circulation 2014, 129, 399–410. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Feigin, V.L.; Stark, B.A.; Johnson, C.O.; Roth, G.A.; Bisignano, C.; Abady, G.G.; Abbasifard, M.; Abbasi-Kangevari, M.; Abd-Allah, F.; Abedi, V.; et al. Global, regional, and national burden of stroke and its risk factors, 1990–2019: A systematic analysis for the Global Burden of Disease Study 2019. Lancet Neurol. 2021, 20, 795–820. [Google Scholar] [CrossRef]
- Cruz-Jentoft, A.J.; Sayer, A.A. Sarcopenia. Lancet 2019, 393, 2636–2646. [Google Scholar] [CrossRef]
- Li, W.; Yue, T.; Liu, Y. New understanding of the pathogenesis and treatment of stroke-related sarcopenia. Biomed. Pharmacother. 2020, 131, 110721. [Google Scholar] [CrossRef]
- Scherbakov, N.; von Haehling, S.; Anker, S.D.; Dirnagl, U.; Doehner, W. Stroke induced Sarcopenia: Muscle wasting and disability after stroke. Int. J. Cardiol. 2013, 170, 89–94. [Google Scholar] [CrossRef]
- Scherbakov, N.; Sandek, A.; Doehner, W. Stroke-Related Sarcopenia: Specific Characteristics. J. Am. Med. Dir. Assoc. 2015, 16, 272–276. [Google Scholar] [CrossRef]
- Matsushita, T.; Nishioka, S.; Taguchi, S.; Yamanouchi, A. Sarcopenia as a predictor of activities of daily living capability in stroke patients undergoing rehabilitation. Geriatr. Gerontol. Int. 2019, 19, 1124–1128. [Google Scholar] [CrossRef]
- Jang, A.; Bae, C.H.; Han, S.J.; Bae, H. Association Between Length of Stay in the Intensive Care Unit and Sarcopenia Among Hemiplegic Stroke Patients. Ann. Rehabil. Med. 2021, 45, 49–56. [Google Scholar] [CrossRef]
- Park, J.G.; Lee, K.W.; Kim, S.B.; Lee, J.H.; Kim, Y.H. Effect of Decreased Skeletal Muscle Index and Hand Grip Strength on Functional Recovery in Subacute Ambulatory Stroke Patients. Ann. Rehabil. Med. 2019, 43, 535–543. [Google Scholar] [CrossRef]
- Park, S.; Ham, J.-O.; Lee, B.K. A positive association between stroke risk and sarcopenia in men aged ≥ 50 years, but not women: Results from the Korean National Health and Nutrition Examination Survey 2008–2010. J. Nutr. Health Aging 2014, 18, 806–812. [Google Scholar] [CrossRef] [PubMed]
- Ohyama, K.; Watanabe, M.; Nosaki, Y.; Hara, T.; Iwai, K.; Mokuno, K. Correlation Between Skeletal Muscle Mass Deficit and Poor Functional Outcome in Patients with Acute Ischemic Stroke. J. Stroke Cerebrovasc. Dis. 2020, 29, 104623. [Google Scholar] [CrossRef] [PubMed]
- Matsushita, T.; Nishioka, S.; Taguchi, S.; Yamanouchi, A.; Okazaki, Y.; Oishi, K.; Nakashima, R.; Fujii, T.; Tokunaga, Y.; Onizuka, S. Effect of Improvement in Sarcopenia on Functional and Discharge Outcomes in Stroke Rehabilitation Patients. Nutrients 2021, 13, 2192. [Google Scholar] [CrossRef]
- Lee, Y.-C.; Chiu, E.-C. Nutritional status as a predictor of comprehensive activities of daily living function and quality of life in patients with stroke. NeuroRehabilitation 2021, 48, 337–343. [Google Scholar] [CrossRef] [PubMed]
- Nishioka, S.; Wakabayashi, H.; Nishioka, E.; Yoshida, T.; Mori, N.; Watanabe, R. Nutritional Improvement Correlates with Recovery of Activities of Daily Living among Malnourished Elderly Stroke Patients in the Convalescent Stage: A Cross-Sectional Study. J. Acad. Nutr. Diet. 2016, 116, 837–843. [Google Scholar] [CrossRef]
- Shimazu, S.; Yoshimura, Y.; Kudo, M.; Nagano, F.; Bise, T.; Shiraishi, A.; Sunahara, T. Frequent and personalized nutritional support leads to improved nutritional status, activities of daily living, and dysphagia after stroke. Nutrition 2020, 83, 111091. [Google Scholar] [CrossRef]
- Zielińska-Nowak, E.; Cichon, N.; Saluk-Bijak, J.; Bijak, M.; Miller, E. Nutritional Supplements and Neuroprotective Diets and Their Potential Clinical Significance in Post-Stroke Rehabilitation. Nutrients 2021, 13, 2704. [Google Scholar] [CrossRef]
- Lieber, A.C.; Hong, E.; Putrino, D.; Nistal, D.A.; Pan, J.S.; Kellner, C.P. Nutrition, Energy Expenditure, Dysphagia, and Self-Efficacy in Stroke Rehabilitation: A Review of the Literature. Brain Sci. 2018, 8, 218. [Google Scholar] [CrossRef] [Green Version]
- Shiraishi, A.; Yoshimura, Y.; Wakabayashi, H.; Tsuji, Y. Prevalence of stroke-related sarcopenia and its association with poor oral status in post-acute stroke patients: Implications for oral sarcopenia. Clin. Nutr. 2018, 37, 204–207. [Google Scholar] [CrossRef]
- Yoshimura, Y. Recent Advances in Clinical Nutrition in Stroke Rehabilitation. Nutrients 2022, 14, 1130. [Google Scholar] [CrossRef]
- Irisawa, H.; Mizushima, T. Correlation of Body Composition and Nutritional Status with Functional Recovery in Stroke Rehabilitation Patients. Nutrients 2020, 12, 1923. [Google Scholar] [CrossRef] [PubMed]
- Irisawa, H.; Mizushima, T. Assessment of changes in muscle mass, strength, and quality and activities of daily living in elderly stroke patients. Int. J. Rehabilitation Res. 2022, 45, 161–167. [Google Scholar] [CrossRef] [PubMed]
- Lathuilière, A.; Mareschal, J.; Graf, C.E. How to Prevent Loss of Muscle Mass and Strength among Older People in Neuro-Rehabilitation? Nutrients 2019, 11, 881. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Honaga, K.; Mori, N.; Akimoto, T.; Tsujikawa, M.; Kawakami, M.; Okamoto, T.; Sakata, Y.; Hamano, H.; Takeda, Y.; Kondo, K. Investigation of the Effect of Nutritional Supplementation with Whey Protein and Vitamin D on Muscle Mass and Muscle Quality in Subacute Post-Stroke Rehabilitation Patients: A Randomized, Single-Blinded, Placebo-Controlled Trial. Nutrients 2022, 14, 685. [Google Scholar] [CrossRef]
- Park, M.K.; Lee, S.J.; Choi, E.; Lee, S.; Lee, J. The Effect of Branched Chain Amino Acid Supplementation on Stroke-Related Sarcopenia. Front. Neurol. 2022, 13, 744945. [Google Scholar] [CrossRef]
- Aprile, I.; Cruciani, A.; Germanotta, M.; Gower, V.; Pecchioli, C.; Cattaneo, D.; Vannetti, F.; Padua, L.; Gramatica, F. Upper Limb Robotics in Rehabilitation: An Approach to Select the Devices, Based on Rehabilitation Aims, and Their Evaluation in a Feasibility Study. Appl. Sci. 2019, 9, 3920. [Google Scholar] [CrossRef] [Green Version]
- Aprile, I.; Germanotta, M.; Cruciani, A.; Loreti, S.; Pecchioli, C.; Cecchi, F.; Montesano, A.; Galeri, S.; Diverio, M.; Falsini, C.; et al. Upper Limb Robotic Rehabilitation After Stroke: A Multicenter, Randomized Clinical Trial. J. Neurol. Phys. Ther. 2020, 44, 3–14. [Google Scholar] [CrossRef]
- Hudon, C.; Fortin, M.; Vanasse, A. Cumulative Illness Rating Scale was a reliable and valid index in a family practice context. J. Clin. Epidemiol. 2005, 58, 603–608. [Google Scholar] [CrossRef]
- Shah, S.; Vanclay, F.; Cooper, B. Improving the sensitivity of the Barthel Index for stroke rehabilitation. J. Clin. Epidemiol. 1989, 42, 703–709. [Google Scholar] [CrossRef]
- Cederholm, T.; Jensen, G.L.; Correia, M.I.T.D.; Gonzalez, M.C.; Fukushima, R.; Higashiguchi, T.; Baptista, G.; Barazzoni, R.; Blaauw, R.; Coats, A.J.; et al. GLIM criteria for the diagnosis of malnutrition—A consensus report from the global clinical nutrition community. J. Cachexia Sarcopenia Muscle 2019, 10, 207–217. [Google Scholar] [CrossRef]
- Chumlea, W.C.; Roche, A.F.; Steinbaugh, M.L. Estimating Stature from Knee Height for Persons 60 to 90 Years of Age. J. Am. Geriatr. Soc. 1985, 33, 116–120. [Google Scholar] [CrossRef] [PubMed]
- Cereda, E.; Pusani, C.; Limonta, D.; Vanotti, A. The ability of the Geriatric Nutritional Risk Index to assess the nutritional status and predict the outcome of home-care resident elderly: A comparison with the Mini Nutritional Assessment. Br. J. Nutr. 2009, 102, 563–570. [Google Scholar] [CrossRef] [PubMed]
- Bouillanne, O.; Morineau, G.; Dupont, C.; Coulombel, I.; Vincent, J.-P.; Nicolis, I.; Benazeth, S.; Cynober, L.; Aussel, C. Geriatric Nutritional Risk Index: A new index for evaluating at-risk elderly medical patients. Am. J. Clin. Nutr. 2005, 82, 777–783. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sherwin, A.J.; Nowson, C.A.; McPhee, J.; Alexander, J.L.; Wark, J.D.; Flicker, L. Nutrient Intake at Meals in Residential Care Facilites for the Aged: Validated Visual Estimation of Plate Waste. Aust. J. Nutr. Diet. 1998, 55, 188–193. [Google Scholar]
- Dubois, S. Accuracy of visual estimates of plate waste in the determination of food consumption. J. Am. Diet. Assoc. 1990, 90, 382–387. [Google Scholar] [CrossRef]
- Valero Díaz, A.; Caracuel García, A. Evaluation of Factors Affecting Plate Waste of Inpatients in Different Healthcare Settings. Nutr. Hosp. 2013, 28, 419–427. [Google Scholar] [CrossRef]
- SINU (Italian Society of Human Nutrition). Nutrients and Energy Reference Intake for Italian Population; 4th Revision; SINU (Italian Society of Human Nutrition): Milano, Italy, 2014. [Google Scholar]
- Cruz-Jentoft, A.J.; Bahat, G.; Bauer, J.; Boirie, Y.; Bruyère, O.; Cederholm, T.; Cooper, C.; Landi, F.; Rolland, Y.; Sayer, A.A.; et al. Sarcopenia: Revised European Consensus on Definition and Diagnosis. Age Ageing 2019, 48, 16–31. [Google Scholar] [CrossRef] [Green Version]
- Reijnierse, E.M.; de Jong, N.; Trappenburg, M.C.; Blauw, G.J.; Butler-Browne, G.; Gapeyeva, H.; Hogrel, J.-Y.; McPhee, J.S.; Narici, M.V.; Sipilä, S.; et al. Assessment of maximal handgrip strength: How many attempts are needed? J. Cachex Sarcopenia Muscle 2017, 8, 466–474. [Google Scholar] [CrossRef]
- Di Vincenzo, O.; Marra, M.; Di Gregorio, A.; Pasanisi, F.; Scalfi, L. Bioelectrical impedance analysis (BIA) -derived phase angle in sarcopenia: A systematic review. Clin. Nutr. 2020, 40, 3052–3061. [Google Scholar] [CrossRef]
- Su, Y.; Yuki, M.; Otsuki, M. Prevalence of stroke-related sarcopenia: A systematic review and meta-analysis. J. Stroke Cerebrovasc. Dis. 2020, 29, 105092. [Google Scholar] [CrossRef]
- Kyle, U.G.; Bosaeus, I.; De Lorenzo, A.D.; Deurenberg, P.; Elia, M.; Gomez, J.M.; Heitmann, B.L.; Kent-Smith, L.; Melchior, J.-C.; Pirlich, M.; et al. Bioelectrical impedance analysis? Part I: Review of principles and methods. Clin. Nutr. 2004, 23, 1226–1243. [Google Scholar] [CrossRef] [PubMed]
- Fragala, M.S.; Kenny, A.M.; Kuchel, G.A. Muscle Quality in Aging: A Multi-Dimensional Approach to Muscle Functioning with Applications for Treatment. Sports Med. 2015, 45, 641–658. [Google Scholar] [CrossRef] [PubMed]
- Lim, S.-K.; Lim, J.-Y. Phase angle as a predictor of functional outcomes in patients undergoing in-hospital rehabilitation after hip fracture surgery. Arch. Gerontol. Geriatr. 2020, 89, 104060. [Google Scholar] [CrossRef] [PubMed]
- Bourgeois, B.; Fan, B.; Johannsen, N.; Gonzalez, M.C.; Ng, B.K.; Sommer, M.J.; Shepherd, J.; Heymsfield, S.B. Improved strength prediction combining clinically available measures of skeletal muscle mass and quality. J. Cachex Sarcopenia Muscle 2018, 10, 84–94. [Google Scholar] [CrossRef] [Green Version]
- Bise, T.; Yoshimura, Y.; Wakabayashi, H.; Nagano, F.; Kido, Y.; Shimazu, S.; Shiraishi, A.; Matsumoto, A. Association between BIA-derived Phase Angle and Sarcopenia and Improvement in Activities of Daily Living and Dysphagia in Patients undergoing Post-Stroke Rehabilitation. J. Nutr. Health Aging 2022, 26, 590–597. [Google Scholar] [CrossRef]
- Abd-El-Gawad, W.M.; Abou-Hashem, R.M.; El Maraghy, M.O.; Amin, G.E. The validity of Geriatric Nutrition Risk Index: Simple tool for prediction of nutritional-related complication of hospitalized elderly patients. Comparison with Mini Nutritional Assessment. Clin. Nutr. 2014, 33, 1108–1116. [Google Scholar] [CrossRef]
- Kang, M.K.; Kim, T.J.; Kim, Y.; Nam, K.-W.; Jeong, H.-Y.; Kim, S.K.; Lee, J.S.; Ko, S.-B.; Yoon, B.-W. Geriatric nutritional risk index predicts poor outcomes in patients with acute ischemic stroke—Automated undernutrition screen tool. PLoS ONE 2020, 15, e0228738. [Google Scholar] [CrossRef] [Green Version]
- Williams, P.; Walton, K. Plate waste in hospitals and strategies for change. e-SPEN Eur. e-Journal Clin. Nutr. Metab. 2011, 6, e235–e241. [Google Scholar] [CrossRef] [Green Version]
- Yoshimura, Y.; Wakabayashi, H.; Momosaki, R.; Nagano, F.; Bise, T.; Shimazu, S.; Shiraishi, A. Stored Energy Increases Body Weight and Skeletal Muscle Mass in Older, Underweight Patients after Stroke. Nutrients 2021, 13, 3274. [Google Scholar] [CrossRef]
- Aquilani, R.; Scocchi, M.; Iadarola, P.; Franciscone, P.; Verri, M.; Boschi, F.; Pasini, E.; Viglio, S. Protein supplementation may enhance the spontaneous recovery of neurological alterations in patients with ischaemic stroke. Clin. Rehabil. 2008, 22, 1042–1050. [Google Scholar] [CrossRef]
- Nguyen, L.; Do, B.; Vu, D.; Pham, K.; Vu, M.-T.; Nguyen, H.; Tran, T.; Le, H.; Nguyen, T.; Nguyen, Q.; et al. Physical Activity and Diet Quality Modify the Association between Comorbidity and Disability among Stroke Patients. Nutrients 2021, 13, 1641. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Baseline Characteristics | Mean (±SD) or Number (%) |
|---|---|
| Age (years) | 68 ± 11 |
| Sex | |
| Men | 30 (49.2%) |
| Women | 31 (50.8%) |
| Index stroke type | |
| Ischemic | 42 (70%) |
| Hemorrhagic | 18 (30%) |
| Affected side | |
| Right | 30 (49.2%) |
| Left | 31 (50.8%) |
| Days from stroke onset to enrollment | 105 ± 61 |
| Neglect | 11 (18%) |
| Aphasia | 12 (19.6%) |
| Smokers and former smokers | 25 (41%) |
| Dysphagia | 24 (39.3%) |
| Comorbidities | |
| Hypertension | 54 (88.5%) |
| Type 2 Diabetes | 21 (34.4%) |
| Dyslipidemia | 31 (50.8%) |
| Hearth disease (heart failure or prior heart attack) | 7 (11.5%) |
| Atrial fibrillation | 7 (11.5%) |
| Prior Cancers | 6 (9.8%) |
| Peripheral Vascular Disease (PVD) | 12 (19.7%) |
| Chronic Obstructive Pulmonary Disease (COPD) | 7 (11.5%) |
| Thyroid Disease | 14 (23%) |
| More than 2 comorbidities | 47 (77%) |
| Cumulative Illness Rating Scale (CIRS) CIRS severity CIRS comorbidity | 2.4 ± 0.4 6.0 ± 1.9 |
| Activities of Daily Living (ADL) Assessment | |
| Modified Barthel Index (0–100) | 45 ± 18 |
| Anthropometric Measurements | |
| Height (m) | 1.66 ± 0.11 |
| Weight (kg) | 68.0 ± 17 |
| BMI (kg/m2) | 24.4 ± 5.3 |
| Nutritional status | |
| Mini Nutritional Assessment Short-Form (MNA®-SF) | 7 ± 2 |
| Albumin (g/L) | 37.4 ± 6.5 |
| Geriatric Nutritional Risk Index (GNRI) | 104.9 ± 14.1 |
| Sarcopenic Group (SG) | Non-Sarcopenic Group (NSG) | p Value | |
|---|---|---|---|
| MNA®-SF (T0) | 6 ± 2 | 8 ± 2 | <0.001 ** |
| BMI (T0) | 20.6 ± 2.2 | 26.0 ± 5.5 | <0.001 ** |
| BMI (T1) | 20.7 ± 2.3 | 26.0 ± 5.2 | <0.001 ** |
| GNRI (T0) | 96.9 ± 15.2 | 108.2 ± 12.4 | 0.010 * |
| GNRI (T1) | 100.1 ± 11.2 | 109.7 ± 12.3 | 0.015 * |
| Delta GNRI | 2.2 ± 9.0 | 1.1 ± 6.9 | 0.309 |
| GNRI < 92 (T0) | 33% | 9.3% | 0.030 * |
| GNRI < 92 (T1) | 29% | 9.7% | 0.073 |
| Dysphagia | 50% | 35% | 0.207 |
| Plate waste (daily average) | 1.10 ± 0.64 | 0.72 ± 0.57 | 0.020 * |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Siotto, M.; Germanotta, M.; Guerrini, A.; Pascali, S.; Cipollini, V.; Cortellini, L.; Ruco, E.; Khazrai, Y.M.; De Gara, L.; Aprile, I. Relationship between Nutritional Status, Food Consumption and Sarcopenia in Post-Stroke Rehabilitation: Preliminary Data. Nutrients 2022, 14, 4825. https://doi.org/10.3390/nu14224825
Siotto M, Germanotta M, Guerrini A, Pascali S, Cipollini V, Cortellini L, Ruco E, Khazrai YM, De Gara L, Aprile I. Relationship between Nutritional Status, Food Consumption and Sarcopenia in Post-Stroke Rehabilitation: Preliminary Data. Nutrients. 2022; 14(22):4825. https://doi.org/10.3390/nu14224825
Chicago/Turabian StyleSiotto, Mariacristina, Marco Germanotta, Alessandro Guerrini, Simona Pascali, Valeria Cipollini, Laura Cortellini, Elisabetta Ruco, Yeganeh Manon Khazrai, Laura De Gara, and Irene Aprile. 2022. "Relationship between Nutritional Status, Food Consumption and Sarcopenia in Post-Stroke Rehabilitation: Preliminary Data" Nutrients 14, no. 22: 4825. https://doi.org/10.3390/nu14224825