
Effects of Diet and Lifestyle on Audio-Vestibular Dysfunction in the Elderly: A Literature Review

Abstract
:
1. Introduction
2. Materials and Methods
2.1. Search Strategy
2.2. Quality Assessments
3. Results
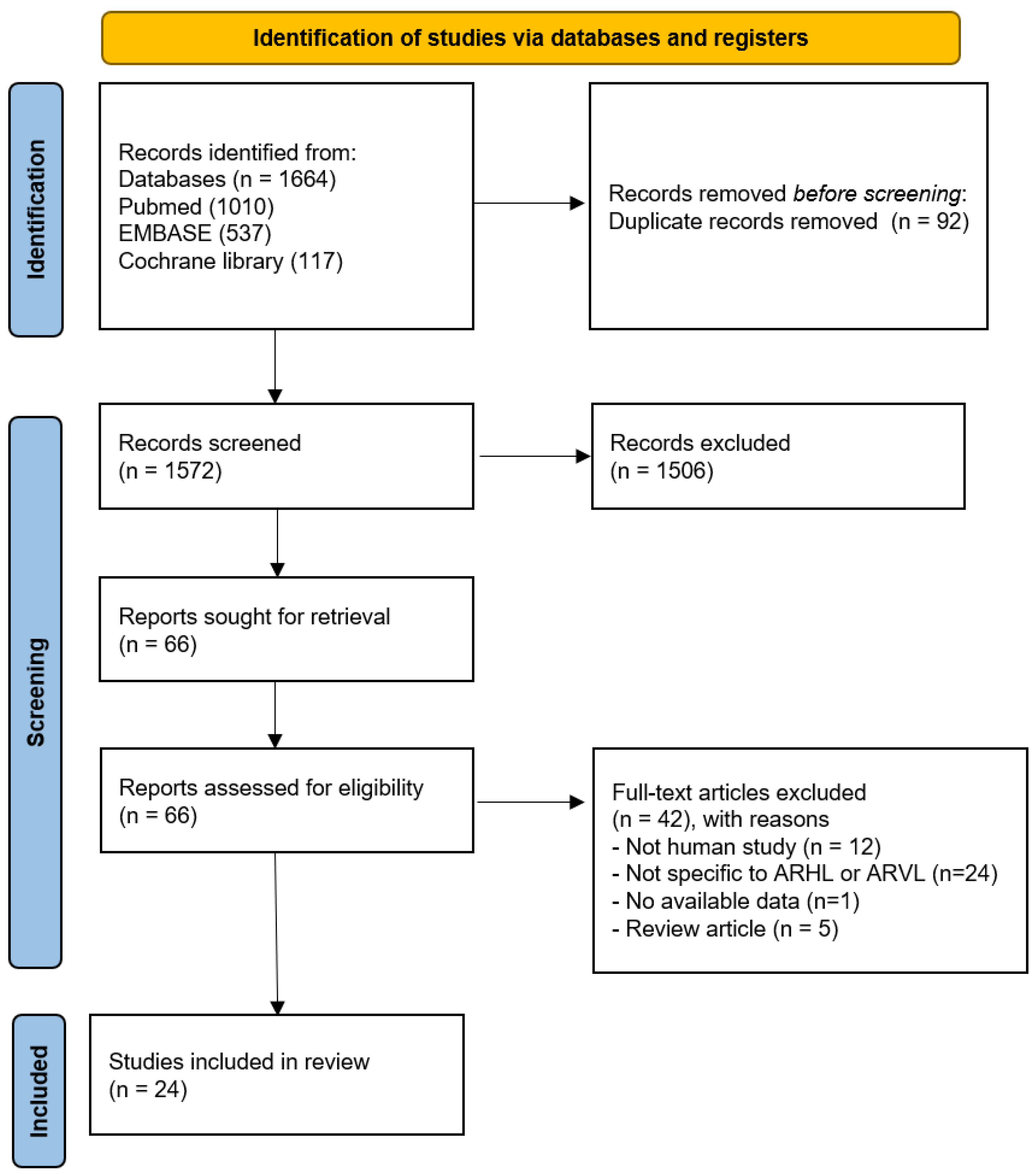
3.1. Literature Search
3.2. Quality Assessment
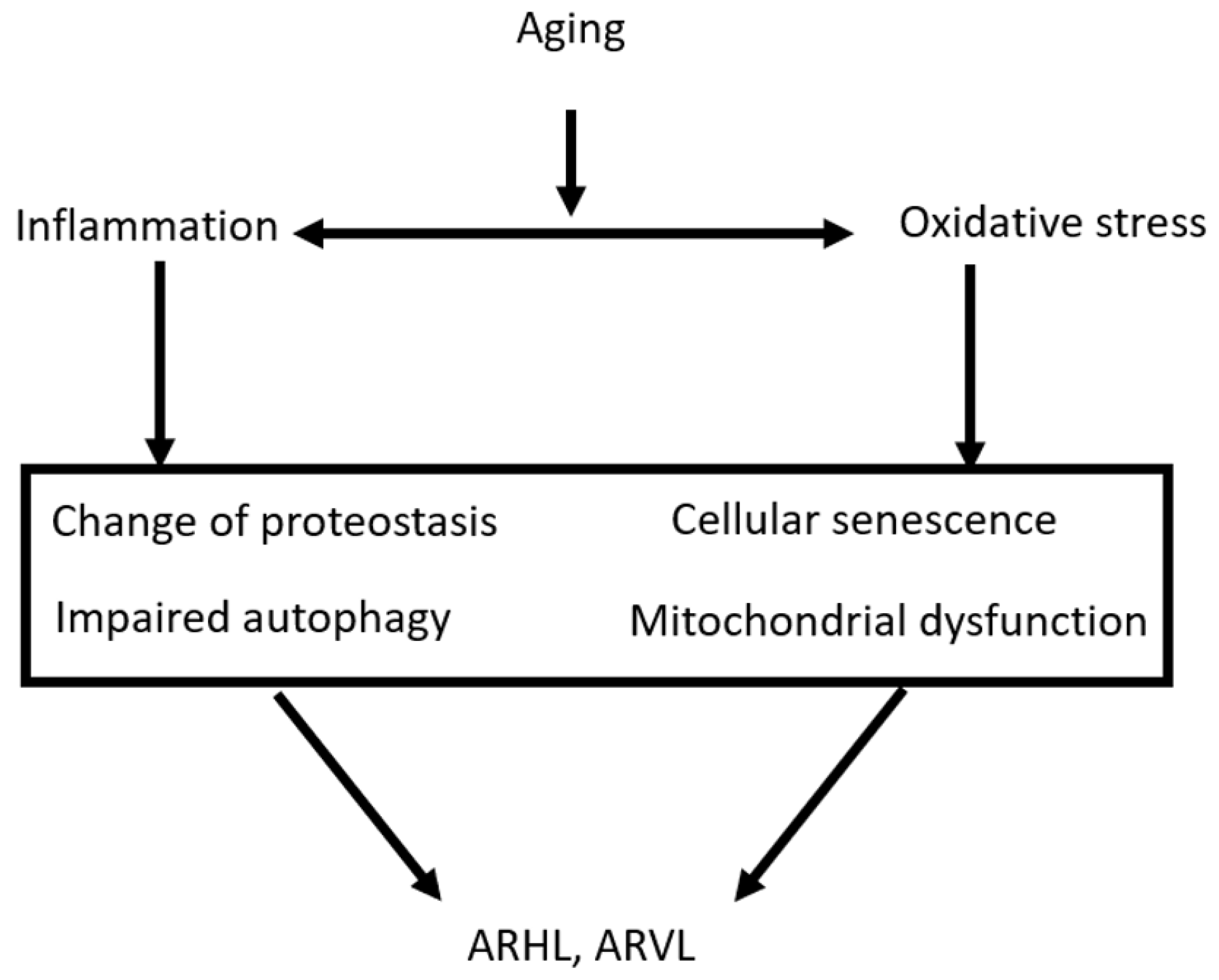
3.3. Pathophysiology and Etiology of Age-Related Hearing and Vestibular Loss
3.3.1. Inflammation
3.3.2. Oxidative Stress
3.3.3. Other Factors: Genetics, Environment, and Medication
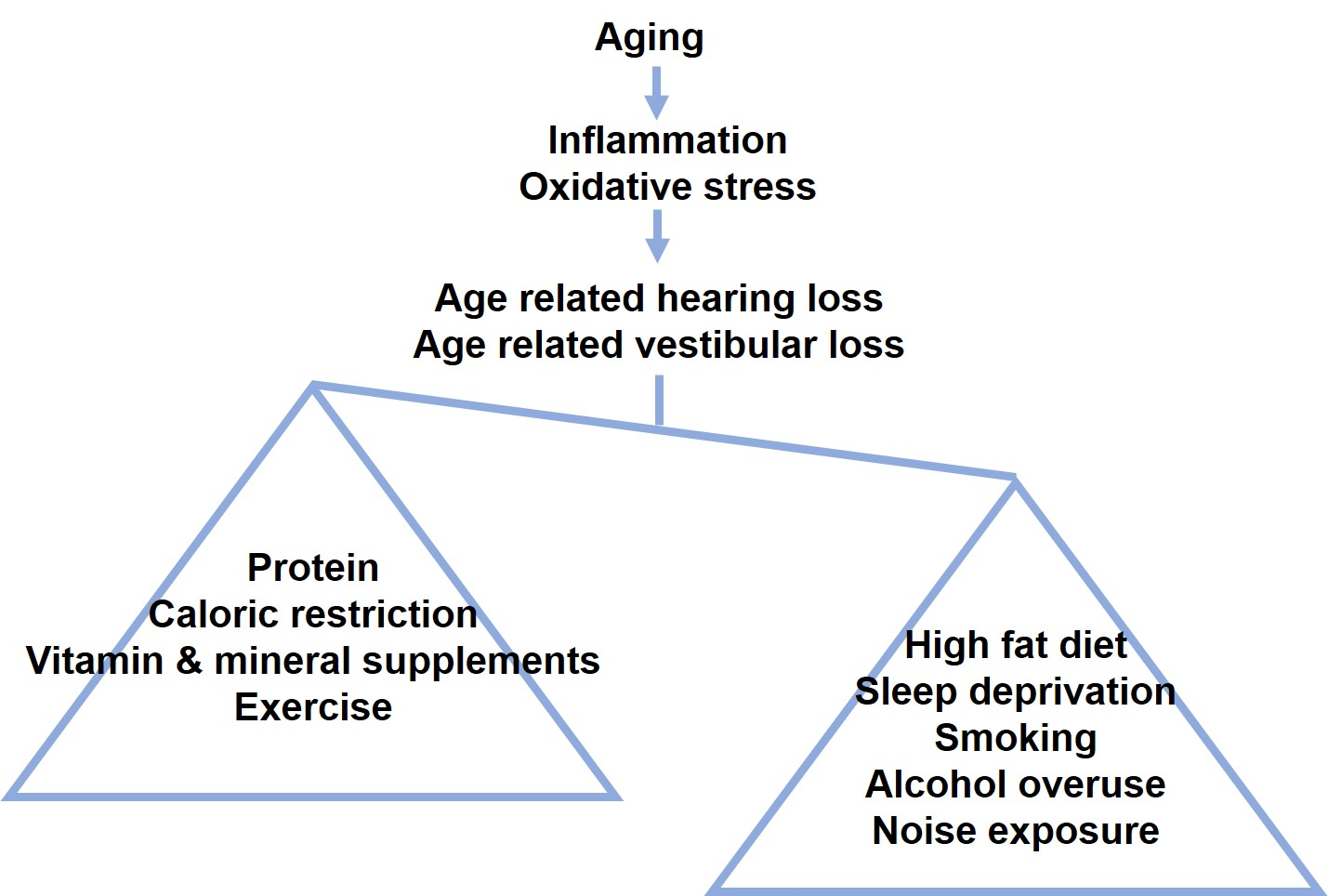
3.4. The Effects of Diet on the Audio-Vestibular Dysfunction of the Elderly
3.4.1. Low Fat and Low Cholesterol Diet
3.4.2. High Protein Diet
3.4.3. Low Sugar and Caloric Restriction Diet
3.4.4. Mediterranean Diet
3.4.5. Different Types of Nutritional Supplements (Vit. A, B, C, D, E, Ca, Mg, Melatonin, and Herbal Remedies)
3.5. The Effects of Lifestyle on the Audio-Vestibular Dysfunction of the Elderly
3.5.1. Exercise
3.5.2. Sleep
3.5.3. Smoking and Alcohol
3.5.4. Noise Protection
4. Discussions
5. Conclusions
Supplementary Materials
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organization. Ageing and Health. Available online: https://www.who.int/news-room/fact-sheets/detail/ageing-and-health (accessed on 4 October 2022).
- Rechel, B.; Jagger, C.; McKee, M.; Cylus, J.; Normand, C.; Figueras, J.; North, J.; White, C. (Eds.) Living Longer, but in Better or Worse Health? European Observatory on Health Systems and Policies: Copenhagen, Denmark, 2020. [Google Scholar]
- Tchkonia, T.; Palmer, A.K.; Kirkland, J.L. New Horizons: Novel Approaches to Enhance Healthspan Through Targeting Cellular Senescence and Related Aging Mechanisms. J. Clin. Endocrinol. Metab. 2021, 106, e1481–e1487. [Google Scholar] [CrossRef] [PubMed]
- Nirmalasari, O.; Mamo, S.K.; Nieman, C.L.; Simpson, A.; Zimmerman, J.; Nowrangi, M.A.; Lin, F.R.; Oh, E.S. Age-related hearing loss in older adults with cognitive impairment. Int. Psychogeriatr. 2017, 29, 115–121. [Google Scholar] [CrossRef] [PubMed]
- Lin, F.R.; Niparko, J.K.; Ferrucci, L. Hearing loss prevalence in the United States. Arch. Intern. Med. 2011, 171, 1851–1852. [Google Scholar] [CrossRef] [Green Version]
- Man, J.; Chen, H.; Zhang, T.; Yin, X.; Yang, X.; Lu, M. Global, regional, and national burden of age-related hearing loss from 1990 to 2019. Aging 2021, 13, 25944–25959. [Google Scholar] [CrossRef] [PubMed]
- Sadeghi, S.G.; Géléoc, G. Editorial: Commonalities and Differences in Vestibular and Auditory Pathways. Front. Neurosci. 2022, 16, 876798. [Google Scholar] [CrossRef] [PubMed]
- Iwasaki, S.; Yamasoba, T. Dizziness and Imbalance in the Elderly: Age-related Decline in the Vestibular System. Aging Dis. 2014, 6, 38–47. [Google Scholar] [CrossRef] [Green Version]
- Arshad, Q.; Seemungal, B.M. Age-Related Vestibular Loss: Current Understanding and Future Research Directions. Front. Neurol. 2016, 7, 231. [Google Scholar] [CrossRef] [Green Version]
- Coto, J.; Alvarez, C.L.; Cejas, I.; Colbert, B.M.; Levin, B.E.; Huppert, J.; Rundek, T.; Balaban, C.; Blanton, S.H.; Lee, D.J.; et al. Peripheral vestibular system: Age-related vestibular loss and associated deficits. J. Otol. 2021, 16, 258–265. [Google Scholar] [CrossRef] [PubMed]
- Tinetti, M.E.; Williams, C.S.; Gill, T.M. Dizziness among older adults: A possible geriatric syndrome. Ann. Intern. Med. 2000, 132, 337–344. [Google Scholar] [CrossRef]
- Ciorba, A.; Bianchini, C.; Pelucchi, S.; Pastore, A. The impact of hearing loss on the quality of life of elderly adults. Clin. Interv. Aging 2012, 7, 159–163. [Google Scholar] [CrossRef]
- Rauch, S.D.; Velazquez-Villaseñor, L.; Dimitri, P.S.; Merchant, S.N. Decreasing hair cell counts in aging humans. Ann. N. Y. Acad. Sci. 2001, 942, 220–227. [Google Scholar] [CrossRef] [PubMed]
- Rodrigo, L.; Campos-Asensio, C.; Rodríguez, M.Á.; Crespo, I.; Olmedillas, H. Role of nutrition in the development and prevention of age-related hearing loss: A scoping review. J. Formos. Med. Assoc. Taiwan Yi Zhi 2021, 120 Pt 1, 107–120. [Google Scholar] [CrossRef] [PubMed]
- Wells, G.A.; Shea, B.; O’Connell, D.; Peterson, J.; Welch, V.; Losos, M.; Tugwell, P. The Newcastle-Ottawa Scale (NOS) for Assessing the Quality of Nonrandomised Studies in Meta-Analysis. Available online: http://www.ohri.ca/programs/clinical_epidemiology/oxford.htm (accessed on 10 October 2022).
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Paplou, V.; Schubert, N.; Pyott, S.J. Age-Related Changes in the Cochlea and Vestibule: Shared Patterns and Processes. Front. Neurosci. 2021, 15, 680856. [Google Scholar] [CrossRef] [PubMed]
- Gonzalez-Gonzalez, S. The role of mitochondrial oxidative stress in hearing loss. Neurol. Disord. Ther. 2017, 1, 1–5. [Google Scholar]
- Franceschi, C.; Bonafè, M.; Valensin, S.; Olivieri, F.; De Luca, M.; Ottaviani, E.; De Benedictis, G. Inflamm-aging. An evolutionary perspective on immunosenescence. Ann. N. Y. Acad. Sci. 2000, 908, 244–254. [Google Scholar] [CrossRef]
- Ferrucci, L.; Fabbri, E. Inflammageing: Chronic inflammation in ageing, cardiovascular disease, and frailty. Nat. Rev. Cardiol. 2018, 15, 505–522. [Google Scholar] [CrossRef]
- Santoro, A.; Bientinesi, E.; Monti, D. Immunosenescence and inflammaging in the aging process: Age-related diseases or longevity? Ageing Res. Rev. 2021, 71, 101422. [Google Scholar] [CrossRef]
- Hashimoto, S.; Billings, P.; Harris, J.P.; Firestein, G.S.; Keithley, E.M. Innate immunity contributes to cochlear adaptive immune responses. Audiol. Neuro-Otol. 2005, 10, 35–43. [Google Scholar] [CrossRef]
- Shi, X. Pathophysiology of the cochlear intrastrial fluid-blood barrier (review). Hear. Res. 2016, 338, 52–63. [Google Scholar] [CrossRef] [Green Version]
- Hirose, K.; Discolo, C.M.; Keasler, J.R.; Ransohoff, R. Mononuclear phagocytes migrate into the murine cochlea after acoustic trauma. J. Comp. Neurol. 2005, 489, 180–194. [Google Scholar] [CrossRef] [PubMed]
- Tornabene, S.V.; Sato, K.; Pham, L.; Billings, P.; Keithley, E.M. Immune cell recruitment following acoustic trauma. Hear. Res. 2006, 222, 115–124. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Q.; Liu, H.; Soukup, G.A.; He, D.Z. Identifying microRNAs involved in aging of the lateral wall of the cochlear duct. PLoS ONE 2014, 9, e112857. [Google Scholar] [CrossRef] [Green Version]
- Kusunoki, T.; Cureoglu, S.; Schachern, P.A.; Baba, K.; Kariya, S.; Paparella, M.M. Age-related histopathologic changes in the human cochlea: A temporal bone study. Otolaryngology-Head Neck Surg. Off. J. Am. Acad. Otolaryngology-Head Neck Surg. 2004, 131, 897–903. [Google Scholar] [CrossRef] [PubMed]
- Keithley, E.M. Pathology and mechanisms of cochlear aging. J. Neurosci. Res. 2020, 98, 1674–1684. [Google Scholar] [CrossRef] [Green Version]
- Seidman, M.D. Effects of dietary restriction and antioxidants on presbyacusis. Laryngoscope 2000, 110 Pt 1, 727–738. [Google Scholar] [CrossRef] [Green Version]
- López-Lluch, G.; Navas, P. Calorie restriction as an intervention in ageing. J. Physiol. 2016, 594, 2043–2060. [Google Scholar] [CrossRef]
- Amorim, J.A.; Coppotelli, G.; Rolo, A.P.; Palmeira, C.M.; Ross, J.M.; Sinclair, D.A. Mitochondrial and metabolic dysfunction in ageing and age-related diseases. Nat. Rev. Endocrinol. 2022, 18, 243–258. [Google Scholar] [CrossRef] [PubMed]
- Liguori, I.; Russo, G.; Curcio, F.; Bulli, G.; Aran, L.; Della-Morte, D.; Gargiulo, G.; Testa, G.; Cacciatore, F.; Bonaduce, D.; et al. Oxidative stress, aging, and diseases. Clin. Interv. Aging 2018, 13, 757–772. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Benkafadar, N.; François, F.; Affortit, C.; Casas, F.; Ceccato, J.C.; Menardo, J.; Venail, F.; Malfroy-Camine, B.; Puel, J.L.; Wang, J. ROS-Induced Activation of DNA Damage Responses Drives Senescence-Like State in Postmitotic Cochlear Cells: Implication for Hearing Preservation. Mol. Neurobiol. 2019, 56, 5950–5969. [Google Scholar] [CrossRef] [Green Version]
- Cui, H.; Kong, Y.; Zhang, H. Oxidative stress, mitochondrial dysfunction, and aging. J. Signal Transduct. 2012, 2012, 646354. [Google Scholar] [CrossRef] [PubMed]
- Yamasoba, T.; Lin, F.R.; Someya, S.; Kashio, A.; Sakamoto, T.; Kondo, K. Current concepts in age-related hearing loss: Epidemiology and mechanistic pathways. Hear. Res. 2013, 303, 30–38. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ahmadmehrabi, S.; Brant, J.; Epstein, D.J.; Ruckenstein, M.J.; Rader, D.J. Genetics of postlingual sensorineural hearing loss. Laryngoscope 2021, 131, 401–409. [Google Scholar] [CrossRef] [PubMed]
- Nagtegaal, A.P.; Broer, L.; Zilhao, N.R.; Jakobsdottir, J.; Bishop, C.E.; Brumat, M.; Christiansen, M.W.; Cocca, M.; Gao, Y.; Heard-Costa, N.L.; et al. Genome-wide association meta-analysis identifies five novel loci for age-related hearing impairment. Sci. Rep. 2019, 9, 15192. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, W.; Johansson, Å.; Rask-Andersen, H.; Rask-Andersen, M. A combined genome-wide association and molecular study of age-related hearing loss in H. sapiens. BMC Med. 2021, 19, 302. [Google Scholar] [CrossRef]
- Wells, H.R.R.; Freidin, M.B.; Zainul Abidin, F.N.; Payton, A.; Dawes, P.; Munro, K.J.; Morton, C.C.; Moore, D.R.; Dawson, S.J.; Williams, F.M.K. GWAS Identifies 44 Independent Associated Genomic Loci for Self-Reported Adult Hearing Difficulty in UK Biobank. Am. J. Hum. Genet. 2019, 105, 788–802. [Google Scholar] [CrossRef] [Green Version]
- Wells, H.; Newman, T.A.; Williams, F. Genetics of age-related hearing loss. J. Neurosci. Res. 2020, 98, 1698–1704. [Google Scholar] [CrossRef]
- Trpchevska, N.; Freidin, M.B.; Broer, L.; Oosterloo, B.C.; Yao, S.; Zhou, Y.; Vona, B.; Bishop, C.; Bizaki-Vallaskangas, A.; Canlon, B.; et al. Genome-wide association meta-analysis identifies 48 risk variants and highlights the role of the stria vascularis in hearing loss. Am. J. Hum. Genet. 2022, 109, 1077–1091. [Google Scholar] [CrossRef]
- Jahn, K. The Aging Vestibular System: Dizziness and Imbalance in the Elderly. Adv. Oto-Rhino-Laryngol. 2019, 82, 143–149. [Google Scholar] [CrossRef]
- Ciorba, A.; Hatzopoulos, S.; Bianchini, C.; Aimoni, C.; Skarzynski, H.; Skarzynski, P. Genetics of presbycusis and presbystasis. Int. J. Immunopathol. Pharmacol. 2015, 29–35. [Google Scholar] [CrossRef]
- Someya, S.; Tanokura, M.; Weindruch, R.; Prolla, T.A.; Yamasoba, T. Effects of caloric restriction on age-related hearing loss in rodents and rhesus monkeys. Curr. Aging Sci. 2010, 3, 20–25. [Google Scholar] [CrossRef] [PubMed]
- Han, C.; Ding, D.; Lopez, M.C.; Manohar, S.; Zhang, Y.; Kim, M.J.; Park, H.; White, K.; Kim, Y.H.; Linser, P.; et al. Effects of Long-term exercise on age-related hearing loss in mice. J. Neurosci. 2016, 36, 11308–11319. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yang, C.H.; Schrepfer, T.; Schacht, J. Age-related hearing impairment and the triad of acquired hearing loss. Front. Cell. Neurosci. 2015, 9, 276. [Google Scholar] [CrossRef] [PubMed]
- Stewart, C.E.; Holt, A.G.; Altschuler, R.A.; Cacace, A.T.; Hall, C.D.; Murnane, O.D.; King, W.M.; Akin, F.W. Effects of noise exposure on the vestibular system: A systematic review. Front. Neurol. 2020, 11, 593919. [Google Scholar] [CrossRef] [PubMed]
- Liberman, M.C. Noise-induced and age-related hearing loss: New perspectives and potential therapies. F1000Research 2017, 6, 927. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fadel, J.R.; Jolivalt, C.G.; Reagan, L.P. Food for thought: The role of appetitive peptides in age-related cognitive decline. Ageing Res. Rev. 2013, 12, 764–776. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sardone, R.; Lampignano, L.; Guerra, V.; Zupo, R.; Donghia, R.; Castellana, F.; Battista, P.; Bortone, I.; Procino, F.; Castellana, M.; et al. Relationship between Inflammatory Food Consumption and Age-Related Hearing Loss in a Prospective Observational Cohort: Results from the Salus in Apulia Study. Nutrients 2020, 12, 426. [Google Scholar] [CrossRef] [Green Version]
- Du, Z.; Yang, Y.; Hu, Y.; Sun, Y.; Zhang, S.; Peng, W.; Zhong, Y.; Huang, X.; Kong, W. A long-term high-fat diet increases oxidative stress, mitochondrial damage and apoptosis in the inner ear of D-galactose-induced aging rats. Hear. Res. 2012, 287, 15–24. [Google Scholar] [CrossRef]
- Gopinath, B.; Flood, V.M.; Teber, E.; McMahon, C.M.; Mitchell, P. Dietary intake of cholesterol is positively associated and use of cholesterol-lowering medication is negatively associated with prevalent age-related hearing loss. J. Nutr. 2011, 141, 1355–1361. [Google Scholar] [CrossRef] [Green Version]
- Park, D.J.; Ha, S.; Choi, J.S.; Lee, S.H.; Park, J.E.; Seo, Y.J. Induced Short-Term Hearing Loss due to Stimulation of Age-Related Factors by Intermittent Hypoxia, High-Fat Diet, and Galactose Injection. Int. J. Mol. Sci. 2020, 21, 7068. [Google Scholar] [CrossRef]
- Fujita, T.; Yamashita, D.; Uehara, N.; Inokuchi, G.; Hasegawa, S.; Otsuki, N.; Nibu, K. A high-fat diet delays age-related hearing loss progression in C57BL/6J mice. PLoS ONE 2015, 10, e0117547. [Google Scholar] [CrossRef]
- Weng, T.; Devine, E.E.; Xu, H.; Yan, Z.; Dong, P. A clinical study of serum lipid disturbance in Chinese patients with sudden deafness. Lipids Health Dis. 2013, 12, 95. [Google Scholar] [CrossRef] [Green Version]
- Avcı, D. Increased Serum Lipid Levels in Patients with Subjective Tinnitus. Iran. J. Otorhinolaryngol. 2021, 33, 31–36. [Google Scholar] [CrossRef] [PubMed]
- Spankovich, C.; Le Prell, C.G. Healthy diets, healthy hearing: National Health and Nutrition Examination Survey, 1999–2002. Int. J. Audiol. 2013, 52, 369–376. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rosenhall, U.; Idrizbegovic, E.; Hederstierna, C.; Rothenberg, E. Dietary habits and hearing. Int. J. Audiol. 2015, 54 (Suppl. S1), S53–S56. [Google Scholar] [CrossRef] [PubMed]
- Evans, M.B.; Tonini, R.; Shope, C.D.; Oghalai, J.S.; Jerger, J.F.; Insull, W., Jr.; Brownell, W.E. Dyslipidemia and auditory function. Otol. Neurotol. Off. Publ. Am. Otol. Soc. Am. Neurotol. Soc. Eur. Acad. Otol. Neurotol. 2006, 27, 609–614. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Suzuki, K.; Kaneko, M.; Murai, K. Influence of serum lipids on auditory function. Laryngoscope 2000, 110 Pt 1, 1736–1738. [Google Scholar] [CrossRef]
- Gopinath, B.; Flood, V.M.; McMahon, C.M.; Burlutsky, G.; Brand-Miller, J.; Mitchell, P. Dietary glycemic load is a predictor of age-related hearing loss in older adults. J. Nutr. 2010, 140, 2207–2212. [Google Scholar] [CrossRef] [Green Version]
- Spankovich, C.; Le Prell, C.G. Associations between dietary quality, noise, and hearing: Data from the National Health and Nutrition Examination Survey, 1999–2002. Int. J. Audiol. 2014, 53, 796–809. [Google Scholar] [CrossRef] [Green Version]
- Dawes, P.; Cruickshanks, K.J.; Marsden, A.; Moore, D.R.; Munro, K.J. Relationship Between Diet, Tinnitus, and Hearing Difficulties. Ear Hear. 2020, 41, 289–299. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Arita, Y.; Kihara, S.; Ouchi, N.; Takahashi, M.; Maeda, K.; Miyagawa, J.; Hotta, K.; Shimomura, I.; Nakamura, T.; Miyaoka, K.; et al. Paradoxical decrease of an adipose-specific protein, adiponectin, in obesity. Biochem. Biophys. Res. Commun. 1999, 257, 79–83. [Google Scholar] [CrossRef] [PubMed]
- Yokota, T.; Oritani, K.; Takahashi, I.; Ishikawa, J.; Matsuyama, A.; Ouchi, N.; Kihara, S.; Funahashi, T.; Tenner, A.J.; Tomiyama, Y.; et al. Adiponectin, a new member of the family of soluble defense collagens, negatively regulates the growth of myelomonocytic progenitors and the functions of macrophages. Blood 2000, 96, 1723–1732. [Google Scholar]
- Shibata, R.; Sato, K.; Pimentel, D.R.; Takemura, Y.; Kihara, S.; Ohashi, K.; Funahashi, T.; Ouchi, N.; Walsh, K. Adiponectin protects against myocardial ischemia-reperfusion injury through AMPK- and COX-2-dependent mechanisms. Nat. Med. 2005, 11, 1096–1103. [Google Scholar] [CrossRef] [Green Version]
- Hwang, J.H.; Hsu, C.J.; Liu, T.C.; Yang, W.S. Association of plasma adiponectin levels with hearing thresholds in adults. Clin. Endocrinol. 2011, 75, 614–620. [Google Scholar] [CrossRef]
- Wu, C.C.; Tsai, C.H.; Lu, Y.C.; Lin, H.C.; Hwang, J.H.; Lin, Y.H.; Yang, W.S.; Chen, P.J.; Liao, W.C.; Lee, Y.L.; et al. Contribution of adiponectin and its type 1 receptor to age-related hearing impairment. Neurobiol. Aging 2015, 36, 2085–2093. [Google Scholar] [CrossRef]
- Tang, T.H.; Hwang, J.H.; Yang, T.H.; Hsu, C.J.; Wu, C.C.; Liu, T.C. Can Nutritional Intervention for Obesity and Comorbidities Slow Down Age-Related Hearing Impairment? Nutrients 2019, 11, 1668. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rosen, S.; Olin, P.; Rosen, H.V. Dietary prevention of hearing loss. Acta Oto-Laryngol. 1970, 70, 242–247. [Google Scholar]
- Dullemeijer, C.; Verhoef, P.; Brouwer, I.A.; Kok, F.J.; Brummer, R.J.; Durga, J. Plasma very long-chain n-3 polyunsaturated fatty acids and age-related hearing loss in older adults. J. Nutr. Health Aging 2010, 14, 347–351. [Google Scholar] [CrossRef]
- Gopinath, B.; Flood, V.M.; Rochtchina, E.; McMahon, C.M.; Mitchell, P. Consumption of omega-3 fatty acids and fish and risk of age-related hearing loss. Am. J. Clin. Nutr. 2010, 92, 416–421. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Curhan, S.G.; Eavey, R.D.; Wang, M.; Rimm, E.B.; Curhan, G.C. Fish and fatty acid consumption and the risk of hearing loss in women. Am. J. Clin. Nutr. 2014, 100, 1371–1377. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lautermann, J.; Schacht, J. Reduzierter Ernährungszustand verstärkt Ototoxizität [Reduced nutritional status enhances ototoxicity]. Laryngo-Rhino-Otol. 1995, 74, 724–727. [Google Scholar] [CrossRef]
- Kim, S.Y.; Sim, S.; Kim, H.J.; Choi, H.G. Low-fat and low-protein diets are associated with hearing discomfort among the elderly of Korea. Br. J. Nutr. 2015, 114, 1711–1717. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jung, S.Y.; Kim, S.H.; Yeo, S.G. Association of Nutritional Factors with Hearing Loss. Nutrients 2019, 11, 307. [Google Scholar] [CrossRef]
- Lee, D.Y.; Kim, Y.H. Relationship Between Diet and Tinnitus: Korea National Health and Nutrition Examination Survey. Clin. Exp. Otorhinolaryngol. 2018, 11, 158–165. [Google Scholar] [CrossRef] [PubMed]
- Hofmeister, M. Do dietary factors significantly influence tinnitus? Aust. J. Gen. Pract. 2019, 48, 153–157. [Google Scholar] [CrossRef] [Green Version]
- Schultz, A.R.; Neves-Souza, R.D.; Costa, V.; Meneses-Barriviera, C.L.; Franco, P.P.; Marchiori, L.L. Is There a Possible Association between Dietary Habits and Benign Paroxysmal Positional Vertigo in the Elderly? The Importance of Diet and Counseling. Int. Arch. Otorhinolaryngol. 2015, 19, 293–297. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Børsheim, E.; Bui, Q.U.; Tissier, S.; Kobayashi, H.; Ferrando, A.A.; Wolfe, R.R. Effect of amino acid supplementation on muscle mass, strength and physical function in elderly. Clin. Nutr. 2008, 27, 189–195. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Longe, J.L. High-protein diet. In The Gale Encyclopedia of Diets: A Guide to Health and Nutrition; Gale: Detroit, MI, USA, 2008; pp. 524–526. [Google Scholar]
- Friedman, A.N. High-protein diets: Potential effects on the kidney in renal health and disease. Am. J. Kidney Dis. Off. J. Natl. Kidney Found. 2004, 44, 950–962. [Google Scholar] [CrossRef] [PubMed]
- Ludwig, D.S.; Ebbeling, C.B. The carbohydrate-insulin model of obesity: Beyond “calories in, calories out”. JAMA Intern. Med. 2018, 178, 1098–1103. [Google Scholar] [CrossRef]
- Xipeng, L.; Ruiyu, L.; Meng, L.; Yanzhuo, Z.; Kaosan, G.; Liping, W. Effects of diabetes on hearing and cochlear structures. J. Otol. 2013, 8, 82–87. [Google Scholar] [CrossRef] [Green Version]
- Akinpelu, O.V.; Ibrahim, F.; Waissbluth, S.; Daniel, S.J. Histopathologic changes in the cochlea associated with diabetes mellitus—A review. Otol. Neurotol. Off. Publ. Am. Otol. Soc. Am. Neurotol. Soc. Eur. Acad. Otol. Neurotol. 2014, 35, 764–774. [Google Scholar] [CrossRef]
- Fukushima, H.; Cureoglu, S.; Schachern, P.A.; Paparella, M.M.; Harada, T.; Oktay, M.F. Effects of type 2 diabetes mellitus on cochlear structure in humans. Arch. Otolaryngology-Head Neck Surg. 2006, 132, 934–938. [Google Scholar] [CrossRef] [Green Version]
- Ho, S.C.; Liu, J.H.; Wu, R.Y. Establishment of the mimetic aging effect in mice caused by D-galactose. Biogerontology 2003, 4, 15–18. [Google Scholar] [CrossRef]
- Chen, P.; Chen, F.; Zhou, B. Antioxidative, anti-inflammatory and anti-apoptotic effects of ellagic acid in liver and brain of rats treated by D-galactose. Sci. Rep. 2018, 8, 1465. [Google Scholar] [CrossRef] [Green Version]
- Verschuur, C.; Agyemang-Prempeh, A.; Newman, T.A. Inflammation is associated with a worsening of presbycusis: Evidence from the MRC national study of hearing. Int. J. Audiol. 2014, 53, 469–475. [Google Scholar] [CrossRef]
- Puga, A.M.; Pajares, M.A.; Varela-Moreiras, G.; Partearroyo, T. Interplay between Nutrition and Hearing Loss: State of Art. Nutrients 2018, 11, 35. [Google Scholar] [CrossRef] [Green Version]
- Albernaz, P.L. Hearing Loss, Dizziness, and Carbohydrate Metabolism. Int. Arch. Otorhinolaryngol. 2016, 20, 261–270. [Google Scholar] [CrossRef] [Green Version]
- Lampignano, L.; Quaranta, N.; Bortone, I.; Tirelli, S.; Zupo, R.; Castellana, F.; Donghia, R.; Guerra, V.; Griseta, C.; Pesole, P.L.; et al. Dietary Habits and Nutrient Intakes Are Associated to Age-Related Central Auditory Processing Disorder in a Cohort From Southern Italy. Front. Aging Neurosci. 2021, 13, 629017. [Google Scholar] [CrossRef]
- Lavinsky, L.; Oliveira, M.W.; Bassanesi, H.J.; D’Avila, C.; Lavinsky, M. Hyperinsulinemia and tinnitus: A historical cohort. Int. Tinnitus J. 2004, 10, 24–30. [Google Scholar]
- Dhanda, N.; Taheri, S. A narrative review of obesity and hearing loss. Int. J. Obes. 2017, 41, 1066–1073. [Google Scholar] [CrossRef]
- Ooi, T.C.; Ishak, W.S.; Sharif, R.; Shahar, S.; Rajab, N.F.; Singh, D.; Mukari, S. Multidimensional Risk Factors of Age-Related Hearing Loss Among Malaysian Community-Dwelling Older Adults. Clin. Interv. Aging 2021, 16, 2033–2046. [Google Scholar] [CrossRef] [PubMed]
- Spankovich, C. The role of nutrition in healthy hearing: Human evidence. In Free Radicals in ENT Pathology; Humana Press: Cham, Switzerland, 2015; pp. 111–126. [Google Scholar]
- Spankovich, C.; Hood, L.J.; Silver, H.J.; Lambert, W.; Flood, V.M.; Mitchell, P. Associations between diet and both high and low pure tone averages and transient evoked otoacoustic emissions in an older adult population-based study. J. Am. Acad. Audiol. 2011, 22, 49–58. [Google Scholar] [CrossRef] [PubMed]
- Batista, S.M.; Moreira, E.A.M.; Fiates, G.M.R.; de Assis, M.A.A.; Teixeira, E. Effect of low Glycaemic Index Diets on Satiety. Br. Food J. 2014, 116, 1233–1246. [Google Scholar] [CrossRef]
- Tang, D.; Tran, Y.; Shekhawat, G.S.; Burlutsky, G.; Mitchell, P.; Gopinath, B. Dietary Fibre Intake and the 10-Year Incidence of Tinnitus in Older Adults. Nutrients 2021, 13, 4126. [Google Scholar] [CrossRef]
- Nomura, A.M.; Hankin, J.H.; Henderson, B.E.; Wilkens, L.R.; Murphy, S.P.; Pike, M.C.; Le Marchand, L.; Stram, D.O.; Monroe, K.R.; Kolonel, L.N. Dietary fiber and colorectal cancer risk: The multiethnic cohort study. Cancer Causes Control. 2007, 18, 753–764. [Google Scholar]
- Pucheu, S.; Radziwon, K.E.; Salvi, R. New Therapies to Prevent or Cure Auditory Disorders; Springer: Berlin/Heidelberg, Germany, 2020. [Google Scholar]
- Gredilla, R.; Barja, G. Minireview: The role of oxidative stress in relation to caloric restriction and longevity. Endocrinology 2005, 146, 3713–3717. [Google Scholar] [CrossRef]
- Hwangbo, D.S.; Lee, H.Y.; Abozaid, L.S.; Min, K.J. Mechanisms of Lifespan Regulation by Calorie Restriction and Intermittent Fasting in Model Organisms. Nutrients 2020, 12, 1194. [Google Scholar] [CrossRef]
- Zhang, L.; Xu, H.; Ding, N.; Li, X.; Chen, X.; Chen, Z. Beneficial Effects on Brain Micro-Environment by Caloric Restriction in Alleviating Neurodegenerative Diseases and Brain Aging. Front. Physiol. 2021, 12, 715443. [Google Scholar] [CrossRef]
- Someya, S.; Yamasoba, T.; Weindruch, R.; Prolla, T.A.; Tanokura, M. Caloric restriction suppresses apoptotic cell death in the mammalian cochlea and leads to prevention of presbycusis. Neurobiol. Aging 2007, 28, 1613–1622. [Google Scholar] [CrossRef]
- Someya, S.; Yu, W.; Hallows, W.C.; Xu, J.; Vann, J.M.; Leeuwenburgh, C.; Tanokura, M.; Denu, J.M.; Prolla, T.A. Sirt3 mediates reduction of oxidative damage and prevention of age-related hearing loss under caloric restriction. Cell 2010, 143, 802–812. [Google Scholar] [CrossRef] [Green Version]
- Mannström, P.; Ulfhake, B.; Kirkegaard, M.; Ulfendahl, M. Dietary restriction reduces age-related degeneration of stria vascularis in the inner ear of the rat. Exp. Gerontol. 2013, 48, 1173–1179. [Google Scholar] [CrossRef] [Green Version]
- Someya, S.; Rothenberger, C.; Kim, M.J. Lifestyle Intervention to Prevent Age-Related Hearing Loss: Calorie Restriction. In New Therapies to Prevent or Cure Auditory Disorders; Pucheu, S., Radziwon, K., Salvi, R., Eds.; Springer: Cham, Switzerland, 2020. [Google Scholar] [CrossRef]
- Davis, C.; Bryan, J.; Hodgson, J.; Murphy, K. Definition of the Mediterranean Diet; a Literature Review. Nutrients 2015, 7, 9139–9153. [Google Scholar] [CrossRef] [Green Version]
- Estruch, R.; Ros, E.; Salas-Salvadó, J.; Covas, M.I.; Corella, D.; Arós, F.; Gómez-Gracia, E.; Ruiz-Gutiérrez, V.; Fiol, M.; Lapetra, J.; et al. PREDIMED Study Investigators Primary Prevention of Cardiovascular Disease with a Mediterranean Diet Supplemented with Extra-Virgin Olive Oil or Nuts. N. Engl. J. Med. 2018, 378, e34. [Google Scholar] [CrossRef]
- Salas-Salvadó, J.; Bulló, M.; Babio, N.; Martínez-González, M.Á.; Ibarrola-Jurado, N.; Basora, J.; Estruch, R.; Covas, M.I.; Corella, D.; Arós, F.; et al. Reduction in the incidence of type 2 diabetes with the Mediterranean diet: Results of the PREDIMED-Reus nutrition intervention randomized trial. Diabetes Care 2011, 34, 14–19. [Google Scholar] [CrossRef]
- Petersson, S.D.; Philippou, E. Mediterranean diet, cognitive function, and dementia: A systematic review of the evidence. Adv. Nutr. 2016, 7, 889–904. [Google Scholar] [CrossRef] [Green Version]
- Schwingshackl, L.; Schwedhelm, C.; Galbete, C.; Hoffmann, G. Adherence to Mediterranean Diet and Risk of Cancer: An Updated Systematic Review and Meta-Analysis. Nutrients 2017, 9, 1063. [Google Scholar] [CrossRef]
- Trichopoulou, A.; Orfanos, P.; Norat, T.; Bueno-de-Mesquita, B.; Ocké, M.C.; Peeters, P.H.; van der Schouw, Y.T.; Boeing, H.; Hoffmann, K.; Boffetta, P.; et al. Modified Mediterranean diet and survival: EPIC-elderly prospective cohort study. BMJ (Clin. Res. Ed.) 2005, 330, 991. [Google Scholar] [CrossRef] [Green Version]
- Shannon, O.M.; Ashor, A.W.; Scialo, F.; Saretzki, G.; Martin-Ruiz, C.; Lara, J.; Matu, J.; Griffiths, A.; Robinson, N.; Lillà, L.; et al. Mediterranean diet and the hallmarks of ageing. Eur. J. Clin. Nutr. 2021, 75, 1176–1192. [Google Scholar] [CrossRef]
- Leitão, C.; Mignano, A.; Estrela, M.; Fardilha, M.; Figueiras, A.; Roque, F.; Herdeiro, M.T. The Effect of Nutrition on Aging-A Systematic Review Focusing on Aging-Related Biomarkers. Nutrients 2022, 14, 554. [Google Scholar] [CrossRef]
- Curhan, S.G.; Wang, M.; Eavey, R.D.; Stampfer, M.J.; Curhan, G.C. Adherence to Healthful Dietary Patterns Is Associated with Lower Risk of Hearing Loss in Women. J. Nutr. 2018, 148, 944–951. [Google Scholar] [CrossRef] [Green Version]
- Urpi-Sarda, M.; Casas, R.; Chiva-Blanch, G.; Romero-Mamani, E.S.; Valderas-Martínez, P.; Arranza, S.; Andres-Lacueva, C.; Llorach, R.; Medina-Remón, A.; Lamuela-Raventos, R.M.; et al. Virgin olive oil and nuts as key foods of the mediterranean diet effects on inflammatory biomarkers related to atherosclerosis. Pharmacol. Res. 2012, 65, 577–583. [Google Scholar] [CrossRef] [PubMed]
- Vasilopoulou, E.; Georga, K.; Joergensen, M.; Naska, A.; Trichopoulou, A. The antioxidant properties of Greek foods and the flavonoid content of the Mediterranean menu. Curr. Med. Chem.-Immunol. Endocr. Metab. Agents 2005, 5, 33–45. [Google Scholar] [CrossRef]
- Rafnsson, S.B.; Dilis, V.; Trichopoulou, A. Antioxidant nutrients and age-related cognitive decline: A systematic review of population-based cohort studies. Eur. J. Nutr. 2013, 52, 1553–1567. [Google Scholar] [CrossRef] [PubMed]
- Durga, J.; Verhoef, P.; Anteunis, L.J.; Schouten, E.; Kok, F.J. Effects of folic acid supplementation on hearing in older adults: A randomized, controlled trial. Ann. Intern. Med. 2007, 146, 1–9. [Google Scholar] [CrossRef]
- Shargorodsky, J.; Curhan, S.G.; Eavey, R.; Curhan, G.C. A prospective study of vitamin intake and the risk of hearing loss in men. Otolaryngol. Head Neck Surg. 2010, 142, 231–236. [Google Scholar] [CrossRef] [Green Version]
- Kang, J.W.; Choi, H.S.; Kim, K.; Choi, J.Y. Dietary vitamin intake correlates with hearing thresholds in the older population: The Korean National Health and Nutrition Examination Survey. Am. J. Clin. Nutr. 2014, 99, 1407–1413. [Google Scholar] [CrossRef] [Green Version]
- Houston, D.K.; Johnson, M.A.; Nozza, R.J.; Gunter, E.W.; Shea, K.J.; Cutler, G.M.; Edmonds, J.T. Age-related hearing loss, vitamin B-12, and folate in elderly women. Am. J. Clin. Nutr. 1999, 69, 564–571. [Google Scholar] [CrossRef] [Green Version]
- Curhan, S.G.; Stankovic, K.M.; Eavey, R.D.; Wang, M.; Stampfer, M.J.; Curhan, G.C. Carotenoids, vitamin A, vitamin C, vitamin E, and folate and risk of self-reported hearing loss in women. Am. J. Clin. Nutr. 2015, 102, 1167–1175. [Google Scholar] [CrossRef] [Green Version]
- Le, T.; Keithley, E.M. Effects of antioxidants on the aging inner ear. Hear. Res. 2007, 226, 194–202. [Google Scholar] [CrossRef]
- Tavanai, E.; Mohammadkhani, G. Role of antioxidants in prevention of age-related hearing loss: A review of literature. Eur. Arch. Oto-Rhino-Laryngol. Off. J. Eur. Fed. Oto-Rhino-Laryngol. Soc. (EUFOS) Affil. Ger. Soc. Oto-Rhino-Laryngol.—Head Neck Surg. 2017, 274, 1821–1834. [Google Scholar] [CrossRef]
- Chuang, H.Y.; Kuo, C.H.; Chiu, Y.W.; Ho, C.K.; Chen, C.J.; Wu, T.N. A case-control study on the relationship of hearing function and blood concentrations of lead, manganese, arsenic, and selenium. Sci. Total Environ. 2007, 387, 79–85. [Google Scholar] [CrossRef] [PubMed]
- Cevette, M.J.; Barrs, D.M.; Patel, A.; Conroy, K.P.; Sydlowski, S.; Noble, B.N.; Nelson, G.A.; Stepanek, J. Phase 2 study examining magnesium-dependent tinnitus. Int. Tinnitus J. 2011, 16, 168–173. [Google Scholar] [PubMed]
- Ochi, K.; Kinoshita, H.; Kenmochi, M.; Nishino, H.; Ohashi, T. Zinc deficiency and tinnitus. Auris Nasus Larynx 2003, 30, S25–S28. [Google Scholar] [CrossRef]
- Yeh, C.W.; Tseng, L.H.; Yang, C.H.; Hwang, C.F. Effects of oral zinc supplementation on patients with noise-induced hearing loss associated tinnitus: A clinical trial. Biomed. J. 2019, 42, 46–52. [Google Scholar] [CrossRef] [PubMed]
- Gopinath, B.; Flood, V.M.; McMahon, C.M.; Burlutsky, G.; Spankovich, C.; Hood, L.J.; Mitchell, P. Dietary antioxidant intake is associated with the prevalence but not incidence of age-related hearing loss. J. Nutr. Health Aging 2011, 15, 896–900. [Google Scholar] [CrossRef] [PubMed]
- Walden, B.E.; Henselman, L.W.; Morris, E.R. The role of magnesium in the susceptibility of soldiers to noise-induced hearing loss. J. Acoust. Soc. Am. 2000, 108, 453–456. [Google Scholar] [CrossRef] [PubMed]
- Vinpocetine. Available online: https://www.mskcc.org/cancer-care/integrative-medicine/herbs/vinpocetine (accessed on 4 October 2022).
- Szatmari, S.Z.; Whitehouse, P.J. Vinpocetine for cognitive impairment and dementia. Cochrane Database Syst. Rev. 2003, 2003, CD003119. [Google Scholar] [CrossRef]
- Gutiérrez-Farfán, I.; Reyes-Legorreta, C.; Solís-Olguín, M.; Alatorre-Miguel, E.; Verduzco-Mendoza, A.; Durand-Rivera, A. Evaluation of vinpocetine as a therapy in patients with sensorineural hearing loss: A phase II, open-label, single-center study. J. Pharmacol. Sci. 2021, 145, 313–318. [Google Scholar] [CrossRef]
- Hong, B.N.; Kim, S.Y.; Yi, T.H.; Kang, T.H. Post-exposure treatment with ginsenoside compound K ameliorates auditory functional injury associated with noise-induced hearing loss in mice. Neurosci. Lett. 2011, 487, 217–222. [Google Scholar] [CrossRef]
- Castañeda, R.; Natarajan, S.; Jeong, S.Y.; Hong, B.N.; Kang, T.H. Traditional oriental medicine for sensorineural hearing loss: Can ethnopharmacology contribute to potential drug discovery? J. Ethnopharmacol. 2019, 231, 409–428. [Google Scholar] [CrossRef]
- Ahn, J.H.; Yoo, M.H.; Lee, H.J.; Chung, J.W.; Yoon, T.H. Coenzyme Q10 in combination with steroid therapy for treatment of sudden sensorineural hearing loss: A controlled prospective study. Clin. Otolaryngol. Off. J. ENT-UK Off. J. Neth. Soc. Oto-Rhino-Laryngol. Cervico-Facial Surg. 2010, 35, 486–489. [Google Scholar] [CrossRef]
- Von Boetticher, A. Ginkgo biloba extract in the treatment of tinnitus: A systematic review. Neuropsychiatr. Dis. Treat. 2011, 7, 441–447. [Google Scholar] [PubMed] [Green Version]
- Hilton, M.; Zimmermann, E.; Hunt, W. Ginkgo biloba for tinnitus. Cochrane Database Syst. Rev. 2013, 28, CD003852. [Google Scholar] [CrossRef] [PubMed]
- Miroddi, M.; Bruno, R.; Galletti, F.; Calapai, F.; Navarra, M.; Gangemi, S.; Calapai, G. Clinical pharmacology of melatonin in the treatment of tinnitus: A review. Eur. J. Clin. Pharmacol. 2015, 71, 263–270. [Google Scholar] [CrossRef]
- Lee, S.Y.; Jung, G.; Jang, M.J.; Suh, M.W.; Lee, J.H.; Oh, S.H.; Park, M.K. Association of Coffee Consumption with Hearing and Tinnitus Based on a National Population-Based Survey. Nutrients 2018, 10, 1429. [Google Scholar] [CrossRef] [Green Version]
- Ghahraman, M.A.; Farahani, S.; Tavanai, E. A comprehensive review of the effects of caffeine on the auditory and vestibular systems. Nutr. Neurosci. 2021, 25, 2181–2194. [Google Scholar] [CrossRef]
- Warburton, D.E.; Nicol, C.W.; Bredin, S.S. Health benefits of physical activity: The evidence. CMAJ Can. Med. Assoc. J. = J. De L’assoc. Med. Can. 2006, 174, 801–809. [Google Scholar] [CrossRef] [Green Version]
- Cruz-Jentoft, A.J.; Sayer, A.A. Sarcopenia. Lancet 2019, 393, 2636–2646. [Google Scholar] [CrossRef]
- Montero-Fernández, N.; Serra-Rexach, J.A. Role of exercise on sarcopenia in the elderly. Eur. J. Phys. Rehabil. Med. 2013, 49, 131–143. [Google Scholar]
- Kang, S.H.; Jung, D.J.; Cho, K.H.; Park, J.W.; Lee, K.Y.; Do, J.Y. Association between sarcopenia and hearing thresholds in postmenopausal women. Int. J. Med. Sci. 2017, 14, 470–476. [Google Scholar] [CrossRef] [Green Version]
- Kawakami, R.; Sawada, S.S.; Kato, K.; Gando, Y.; Momma, H.; Oike, H.; Miyachi, M.; Lee, I.-M.; Blair, S.N.; Tashiro, M.; et al. A prospective cohort study of muscular and performance fitness and risk of hearing loss: The Niigata Wellness Study. Am. J. Med. 2021, 134, 235–242. [Google Scholar] [CrossRef] [PubMed]
- Chen, D.S.; Betz, J.; Yaffe, K.; Ayonayon, H.N.; Kritchevsky, S.; Martin, K.R.; Harris, T.B.; Purchase-Helzner, E.; Satterfield, S.; Xue, Q.L.; et al. Association of hearing impairment with declines in physical functioning and the risk of disability in older adults. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2015, 70, 654–661. [Google Scholar] [CrossRef] [Green Version]
- Li, L.; Simonsick, E.M.; Ferrucci, L.; Lin, F.R. Hearing loss and gait speed among older adults in the United States. Gait Posture 2013, 38, 25–29. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ho, K.C.; Gupta, P.; Fenwick, E.K.; Man, R.; Gan, A.; Lamoureux, E.L. Association between age-related sensory impairment with sarcopenia and its related components in older adults: A systematic review. J. Cachexia Sarcopenia Muscle 2022, 13, 811–823. [Google Scholar] [CrossRef]
- Yoo, S.Z.; No, M.H.; Heo, J.W.; Park, D.H.; Kang, J.H.; Kim, S.H.; Kwak, H.B. Role of exercise in age-related sarcopenia. J. Exerc. Rehabil. 2018, 14, 551–558. [Google Scholar] [CrossRef]
- Denison, H.J.; Cooper, C.; Sayer, A.A.; Robinson, S.M. Prevention and optimal management of sarcopenia: A review of combined exercise and nutrition interventions to improve muscle outcomes in older people. Clin. Interv. Aging 2015, 10, 859–869. [Google Scholar] [CrossRef] [Green Version]
- Heeringa, A.N.; Köppl, C. The aging cochlea: Towards unraveling the functional contributions of strial dysfunction and synaptopathy. Hear. Res. 2019, 376, 111–124. [Google Scholar] [CrossRef]
- Ishiyama, G. Imbalance and vertigo: The aging human vestibular periphery. Semin. Neurol. 2009, 29, 491–499. [Google Scholar] [CrossRef]
- Gabriel, G.A.; Harris, L.R.; Gnanasegaram, J.J.; Cushing, S.L.; Gordon, K.A.; Haycock, B.C.; Campos, J.L. Age-related changes to vestibular heave and pitch perception and associations with postural control. Sci. Rep. 2022, 12, 6426. [Google Scholar] [CrossRef]
- Karapolat, H.; Celebisoy, N.; Kirazli, Y.; Ozgen, G.; Gode, S.; Gokcay, F.; Bilgen, C.; Kirazli, T. Is vestibular rehabilitation as effective in bilateral vestibular dysfunction as in unilateral vestibular dysfunction? Eur. J. Phys. Rehabil. Med. 2014, 50, 657–663. [Google Scholar]
- Marouane, E.; El Mahmoudi, N.; Rastoldo, G.; Péricat, D.; Watabe, I.; Lapôtre, A.; Tonetto, A.; Xavier, F.; Dumas, O.; Chabbert, C.; et al. Sensorimotor Rehabilitation Promotes Vestibular Compensation in a Rodent Model of Acute Peripheral Vestibulopathy by Promoting Microgliogenesis in the Deafferented Vestibular Nuclei. Cells 2021, 10, 3377. [Google Scholar] [PubMed]
- Battilana, F.; Steurer, S.; Rizzi, G.; Delgado, A.C.; Tan, K.R.; Handschin, C. Exercise-linked improvement in age-associated loss of balance is associated with increased vestibular input to motor neurons. Aging Cell 2020, 19, e13274. [Google Scholar] [CrossRef] [PubMed]
- Crowley, K. Sleep and sleep disorders in older adults. Neuropsychol. Rev. 2011, 21, 41–53. [Google Scholar] [CrossRef] [PubMed]
- Jiang, K.; Spira, A.P.; Reed, N.S.; Lin, F.R.; Deal, J.A. Sleep Characteristics and Hearing Loss in Older Adults: The National Health and Nutrition Examination Survey 2005–2006. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2022, 77, 632–639. [Google Scholar] [CrossRef]
- Schuknecht, H.F.; Gacek, M.R. Cochlear pathology in presbycusis. Ann. Otol. Rhinol. Laryngol. 1993, 102 Pt 2, 1–16. [Google Scholar] [CrossRef]
- Martines, F.; Ballacchino, A.; Sireci, F.; Mucia, M.; La Mattina, E.; Rizzo, S.; Salvago, P. Audiologic profile of OSAS and simple snoring patients: The effect of chronic nocturnal intermittent hypoxia on auditory function. Eur. Arch. Oto-Rhino-Laryngol. Off. J. Eur. Fed. Oto-Rhino-Laryngol. Soc. (EUFOS) Affil. Ger. Soc. Oto-Rhino-Laryngol.—Head Neck Surg. 2016, 273, 1419–1424. [Google Scholar] [CrossRef]
- Ekin, S.; Turan, M.; Arısoy, A.; Gunbatar, H.; Sunnetcioglu, A.; Asker, S.; Yıldız, H. Is There a Relationship Between Obstructive Sleep Apnea (OSA) and Hearing Loss? Med. Sci. Monit. Int. Med. J. Exp. Clin. Res. 2016, 22, 3124–3128. [Google Scholar] [CrossRef] [Green Version]
- Seo, Y.J.; Ju, H.M.; Lee, S.H.; Kwak, S.H.; Kang, M.J.; Yoon, J.H.; Kim, C.H.; Cho, H.J. Damage of Inner Ear Sensory Hair Cells via Mitochondrial Loss in a Murine Model of Sleep Apnea With Chronic Intermittent Hypoxia. Sleep 2017, 40, zsx106. [Google Scholar] [CrossRef] [Green Version]
- Maffei, G.; Miani, P. Experimental tobacco poisoning: Resultant structural modifications of the cochlea and tuba acustica. Arch. Otolaryngol. Head Neck Surg. 1962, 75, 386. [Google Scholar] [CrossRef]
- Lowe, G.; Drummond, M.; Forbes, C.; Barbenel, J. The effects of age and cigarette-smoking on blood and plasma viscosity in men. Scott. Med. J. 1980, 25, 13. [Google Scholar] [CrossRef]
- Browning, G.; Gatehouse, S.; Lowe, G. Blood viscosity as a factor in sensorineural hearing impairment. Lancet. 1986, 327, 121–123. [Google Scholar] [CrossRef]
- Pouryaghoub, G.; Mehrdad, R.; Mohammadi, S. Interaction of smoking and occupational noise exposure on hearing loss: A cross-sectional study. BMC Public Health 2007, 7, 1–5. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ferrite, S.; Santana, V. Joint effects of smoking, noise exposure and age on hearing loss. Occup. Med. 2005, 55, 48–53. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Itoh, A.; Nakashima, T.; Arao, H.; Wakai, K.; Tamakoshi, A.; Kawamura, T.; Ohno, Y. Smoking and drinking habits as risk factors for hearing loss in the elderly: Epidemiological study of subjects undergoing routine health checks in Aichi, Japan. Public Health 2001, 115, 192–196. [Google Scholar] [CrossRef] [PubMed]
- Wada, M.; Takeshima, T.; Nakamura, Y.; Nagasaka, S.; Kamesaki, T.; Kajii, E.; Kotani, K. Association between smoking and the peripheral vestibular disorder: A retrospective cohort study. Sci. Rep. 2017, 7, 16889. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Snetselaar, L.G.; de Jesus, J.M.; DeSilva, D.M.; Stoody, E.E. Dietary Guidelines for Americans, 2020–2025: Understanding the Scientific Process, Guidelines, and Key Recommendations. Nutr. Today 2021, 56, 287–295. [Google Scholar] [CrossRef]
- Dawes, P.; Cruickshanks, K.J.; Moore, D.R.; Edmondson-Jones, M.; McCormack, A.; Fortnum, H.; Munro, K.J. Cigarette smoking, passive smoking, alcohol consumption, and hearing loss. J. Assoc. Res. Otolaryngol. JARO 2014, 15, 663–674. [Google Scholar] [CrossRef] [Green Version]
- Gopinath, B.; Flood, V.M.; McMahon, C.M.; Burlutsky, G.; Smith, W.; Mitchell, P. The effects of smoking and alcohol consumption on age-related hearing loss: The Blue Mountains Hearing Study. Ear Hear. 2010, 31, 277–282. [Google Scholar] [CrossRef]
- Bellé, M.; Sartori, S.; Rossi, A.G. Alcoholism: Effects on the cochleo-vestibular apparatus. Braz. J. Otorhinolaryngol. 2007, 73, 110–116. [Google Scholar] [CrossRef] [Green Version]
- Schmidt, P.M.; Giordani, A.M.; Rossi, A.G.; Cóser, P.L. Balance assessment in alcoholic subjects. Braz. J. Otorhinolaryngol. 2010, 76, 148–155. [Google Scholar] [CrossRef] [Green Version]
- Gopinath, B.; McMahon, C.; Tang, D.; Burlutsky, G.; Mitchell, P. Workplace noise exposure and the prevalence and 10-year incidence of age-related hearing loss. PLoS ONE 2021, 16, e0255356. [Google Scholar] [CrossRef] [PubMed]
- Fernandez, K.A.; Jeffers, P.W.; Lall, K.; Liberman, M.C.; Kujawa, S.G. Aging after noise exposure: Acceleration of cochlear synaptopathy in “recovered” ears. J. Neurosci. Off. J. Soc. Neurosci. 2015, 35, 7509–7520. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Niu, X.; Canlon, B. Protective mechanisms of sound conditioning. Adv. Oto-Rhino-Laryngol. 2002, 59, 96–105. [Google Scholar] [CrossRef]
- Alvarado, J.C.; Fuentes-Santamaría, V.; Gabaldón-Ull, M.C.; Juiz, J.M. Age-Related Hearing Loss Is Accelerated by Repeated Short-Duration Loud Sound Stimulation. Front. Neurosci. 2019, 13, 77. [Google Scholar] [CrossRef]
- Jayakody, D.; Friedland, P.L.; Martins, R.N.; Sohrabi, H.R. Impact of Aging on the Auditory System and Related Cognitive Functions: A Narrative Review. Front. Neurosci. 2018, 12, 125. [Google Scholar] [CrossRef] [Green Version]
- Mangabeira-Albernaz, P.L.; Covell, W.P.; Eldredge, D.H. Changes in the vestilbular labyrinth with intense sound. Laryngoscope 1959, 69, 1478–1493. [Google Scholar] [CrossRef]
- Hsu, W.C.; Wang, J.D.; Lue, J.H.; Day, A.S.; Young, Y.H. Physiological and morphological assessment of the saccule in Guinea pigs after noise exposure. Arch. Otolaryngology-Head Neck Surg. 2008, 134, 1099–1106. [Google Scholar] [CrossRef] [Green Version]
- Stewart, C.E.; Bauer, D.S.; Kanicki, A.C.; Altschuler, R.A.; King, W.M. Intense noise exposure alters peripheral vestibular structures and physiology. J. Neurophysiol. 2020, 123, 658–669. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
| Study Included | Age (Mean) | N | Male | Female | Category | Test | Odds Ratio | 95% CI | Relative Risk | 95% CI | p-Value | Outcomes | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Fat | Gopinath/2010 [72] | >50 | 2442 | 1053 | 1389 | Cross sectional | PTA, questionnaire | 0.76 | 0.60–0.97 | NA | Inverse association between higher intakes of long-chain n-3 PUFAs and HL. | ||
| Curhan/2014 [73] | NA | 65,215 | 0 | 65,215 | Prospective cohort | Self-reported hearing loss, questionnaire | 0.85 | 0.80–0.91 | <0.001 | Higher intake of long-chain omega-3 PUFAs are associated with lower risk of HL in women. | |||
| Rosenhall/2015 [58] | 70–75 | 524 | 249 | 275 | Cross sectional | PTA, dietary history | NA | NA | <0.05 | Good hearing and a high consumption of fish in the male group. | |||
| Kim/2015 [75] | 68.3 | 4615 | 2049 | 2566 | Cross sectional | PTA, nutritional survey | 0.82 | 0.71–0.96 | 0.011 | Low fat intakes are associated with hearing discomfort. | |||
| Dawes/2020 [63] | 40–69 (55.8) | 34,576 | 15,974 | 18,602 | Cross sectional | Self-reported hearing problems, questionnaire | 1.16 | 1.08–1.24 | <0.05 | Substantial impact of diet on levels of tinnitus and hearing difficulties. | |||
| Cholesterol | Gopinath/2011 [52] | >67 | 2447 | 1053 | 1394 | Cross sectional and cohort | PTA, questionnaire | 1.34 | 1.00–1.80 | 0.04 | High cholesterol diet could have adverse influences on hearing. | ||
| Protein | Kim/2015 [75] | 68.3 | 4615 | 2049 | 2566 | Cross sectional | PTA, nutritional survey | 0.81 | 0.67–0.96 | 0.017 | Low protein intakes are associated with hearing discomfort. | ||
| Carbohydrates | Gopinath/2010 [61] | >65 | 2448 | NA | NA | Cross sectional | PTA, questionnaire | 1.77 | 1.04–3.00 | 0.03 | Higher intake of total carbohydrate was a predictor of incident HL. | ||
| Rosenhall/2015 [58] | 70–75 | 524 | 249 | 275 | Cross sectional | PTA, dietary history | NA | NA | <0.05 | Poor high frequency hearing and a high consumption of food rich in low molecular carbohydrates in both genders. | |||
| Sardone/2020 [50] | >65 | 734 | 425 | 309 | Cross sectional | PTA, questionnaire | NA | NA | 0.05 | High-sugar content food is associated with positive ARHL-status. | |||
| Lampignano/2021 [92] | >65 | 734 | 403 | 331 | Cohort | PTA, questionnaire | 0.998 | 0.996–0.999 | NA | Lesser carbohydrate intake is associated with age-related central auditory processing disorder. | |||
| Tang/2021 [99] | >50 | 1730 | NA | NA | Longitudinal cohort | Questionnaire | 1.54 | 1.07–2.22 | NA | Modest associations between intake of dietary fiber and incident tinnitus. | |||
| Mediterranean diet | Dawes/2020 [63] | 40–69 (55.8) | 34,576 | 15,974 | 18,602 | Cross sectional | Self-reported hearing problems, questionnaire | 0.89 | 0.83–0.96 | 0.024 | Dietary patterns high in fruit and vegetables and meat and low in fat was associated with reduced odds of hearing difficulties. | ||
| Vitamins | Durga/2007 [121] | 60 | 728 | 522 | 206 | Randomized controlled trial | Audiometry | NA | NA | 0.02 | Folic acid supplementation slowed the decline in hearing of the speech frequencies. | ||
| Gopinath/2011 [132] | >50 | 2956 | NA | NA | Cross-sectional and 5-year longitudinal analyses | PTA, questionnaire | 0.53 | 0.30–0.92 | 0.04 | Dietary vitamin A intake was significantly associated with the prevalence of HL. | |||
| Gopinath/2011 [132] | >50 | 2956 | NA | NA | Cross-sectional and 5-year longitudinal analyses | PTA, questionnaire | 0.86 | 0.78–0.98 | NA | Dietary vitamin E intake was significantly associated with the prevalence of HL. | |||
| Kang/2014 [123] | 50–80 (62.53) | 1910 | 810 | 1100 | Cross sectional | PTA, questionnaire | −0.012 | −0.022–0.002 | <0.05 | Dietary intake of vitamin C was associated with better hearing in the older population. | |||
| Minerals & others | Lee/2018 [143] | >65 | 2184 | NA | NA | Cross sectional | PTA, questionnaire | 0.76 | 0.56–1.03 | 0.0778 | No significant decreases in bilateral HL were observed in the >65 years age groups. | ||
| Dawes/2020 [63] | 40–69 (55.8) | 34,576 | 15,974 | 18,602 | Cross sectional | Self-reported hearing problems, questionnaire | 1.2 | 1.08–1.34 | 0.02 | Higher intakes of calcium were associated with increased odds of tinnitus. | |||
| Dawes/2020 [63] | 40–69 (55.8) | 34,576 | 15,974 | 18,602 | Cross sectional | Self-reported hearing problems, questionnaire | 1.2 | 1.05–1.37 | 0.007 | Higher intakes of iron were associated with increased odds of tinnitus. |
| Study Included | Age | N | Male | Female | Category | Test | Odds Ratio | 95% CI | p-Value | Outcomes | |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Exercise | Kawakami/2021 [149] | 43–54 | 2765 | 1767 | 998 | Prospective cohort | Muscular and performance fitness index, PTA | 0.79 | 0.71–0.88 | <0.001 | Higher muscular and performance fitness is associated with a lower incidence of HL. |
| Sleep deprivation | Martines/2016 [164] | 38–55 | 160 | 103 | 57 | Cross sectional | Polysomnography, PTA, TEOAE | NA | NA | <0.05 | A more marked high-frequency hearing loss in case of severe OSAS. |
| Ekin/2016 [165] | 20–60 | 66 | 40 | 26 | Cross sectional | Polysomnography, PTA | NA | NA | <0.001 | Snoring may cause hearing loss at extended high frequencies. | |
| Jiang/2021 [162] | >70 | 632 | 325 | 307 | Cross sectional | PTA, questionnaire | NA | –0.34–5.24 | >0.05 | Longer sleep duration is marginally associated with poorer high-frequency hearing among older adults sleeping >8 hours. | |
| Smoking and alcohol | Itoh/2001 [172] | >60 | 496 | 454 | 42 | Cross sectional | PTA, questionnaire | 2.1 | 1.53–2.89 | <0.001 | Current smokers had a significantly increased risk of HL. |
| Itoh/2001 [172] | >60 | 496 | 454 | 42 | Cross sectional | PTA, questionnaire | 0.96 | 0.57–1.64 | 0.021 | Heavy drinkers showed no increased risk of HL. | |
| Ferrite & Santana/2005 [171] | 20–55 | 535 | 535 | 0 | Cross sectional | PTA, questionnaire | 7.65 | 4.43–13.23 | NA | Synergistic effect of smoking, noise exposure and age on HL. | |
| Pouryaghoub/2007 [170] | 24–67 | 206 | 206 | 0 | Cross sectional | PTA | 7.4 | 4.1–13.4 | <0.001 | Smoking can accelerate noise induced HL. | |
| Gopinath/2010 [176] | Mean 66.6 | 2815 | 1218 | 1597 | Cross sectional | PTA, questionnaire | 0.75 | 0.57–0.98 | 0.04 | A protective association between the moderate consumption of alcohol and hearing in older adults. | |
| Wada/2017 [173] | mean 65.3 | 393 | 133 | 260 | Retrospective cohort | Medical record | 2.7 | 1.32–5.53 | 0.006 | Smoking history of >30 pack-years increased the risk of new onset peripheral vestibular disorder. | |
| Noise | Gopinath/2021 [179] | >50 | 1932 | NA | NA | Cross sectional | PTA, questionnaire | 1.39 | 1.13–1.71 | NA | Workplace noise exposure increased the risk of incident hearing loss in older adults. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chen, H.-L.; Tan, C.-T.; Wu, C.-C.; Liu, T.-C. Effects of Diet and Lifestyle on Audio-Vestibular Dysfunction in the Elderly: A Literature Review. Nutrients 2022, 14, 4720. https://doi.org/10.3390/nu14224720
Chen H-L, Tan C-T, Wu C-C, Liu T-C. Effects of Diet and Lifestyle on Audio-Vestibular Dysfunction in the Elderly: A Literature Review. Nutrients. 2022; 14(22):4720. https://doi.org/10.3390/nu14224720
Chicago/Turabian StyleChen, Hsin-Lin, Ching-Ting Tan, Chen-Chi Wu, and Tien-Chen Liu. 2022. "Effects of Diet and Lifestyle on Audio-Vestibular Dysfunction in the Elderly: A Literature Review" Nutrients 14, no. 22: 4720. https://doi.org/10.3390/nu14224720