
Diverticular Disease—An Updated Management Review

 , , , , and
, , , , and
Abstract
:1. Introduction and Epidemiology
2. Definitions and Presentation
2.1. Asymptomatic Diverticulosis
2.2. Diverticular Bleeding
2.3. Symptomatic Uncomplicated Diverticular Disease
2.4. Segmental Colitis Associated with Diverticulosis
2.5. Diverticulitis
2.6. Uncomplicated Diverticulitis
2.7. Complicated Diverticulitis
3. Etiology
3.1. Risk Factors
3.2. Pathogenesis
4. Management
4.1. Symptomatic Uncomplicated Diverticular Disease
4.2. Segmental Colitis Associated with Diverticulosis
4.3. Uncomplicated Diverticulitis
4.4. Complicated Diverticulitis
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Rezapour, M.; Ali, S.; Stollman, N. Diverticular Disease: An Update on Pathogenesis and Management. Gut Liver 2018, 12, 125–132. [Google Scholar] [CrossRef] [PubMed]
- Strate, L.L.; Morris, A.M. Epidemiology, Pathophysiology, and Treatment of Diverticulitis. Gastroenterology 2019, 156, 1282–1298.e1281. [Google Scholar] [CrossRef]
- Munie, S.T.; Nalamati, S.P.M. Epidemiology and Pathophysiology of Diverticular Disease. Clin. Colon. Rectal Surg. 2018, 31, 209–213. [Google Scholar] [CrossRef]
- Hawkins, A.T.; Wise, P.E.; Chan, T.; Lee, J.T.; Glyn, T.; Wood, V.; Eglinton, T.; Frizelle, F.; Khan, A.; Hall, J.; et al. Diverticulitis: An Update From the Age Old Paradigm. Curr. Probl. Surg. 2020, 57, 100862. [Google Scholar] [CrossRef] [PubMed]
- Shahedi, K.; Fuller, G.; Bolus, R.; Cohen, E.; Vu, M.; Shah, R.; Agarwal, N.; Kaneshiro, M.; Atia, M.; Sheen, V.; et al. Long-term risk of acute diverticulitis among patients with incidental diverticulosis found during colonoscopy. Clin. Gastroenterol. Hepatol. 2013, 11, 1609–1613. [Google Scholar] [CrossRef] [PubMed]
- Lamanna, L.; Moran, P.E. Diverticular Disease: Traditional and Evolving Paradigms. Gastroenterol. Nurs. 2018, 41, 111–119. [Google Scholar] [CrossRef]
- Bollom, A.; Austrie, J.; Hirsch, W.; Nee, J.; Friedlander, D.; Ellingson, K.; Cheng, V.; Lembo, A. Emergency Department Burden of Diverticulitis in the USA, 2006–2013. Dig. Dis. Sci. 2017, 62, 2694–2703. [Google Scholar] [CrossRef]
- Steele, S.R.; Steele, S.R.; Hull, T.L.; Hyman, N.; Maykel, J.A.; Read, T.E.; Whitlow, C.B. The ASCRS Textbook of Colon and Rectal Surgery, 4th ed.; Springer: Cham, Switzerland, 2022. [Google Scholar]
- Lembcke, B. Diagnosis, Differential Diagnoses, and Classification of Diverticular Disease. Viszeralmedizin 2015, 31, 95–102. [Google Scholar] [CrossRef]
- Tursi, A. Diverticulosis today: Unfashionable and still under-researched. Therap. Adv. Gastroenterol. 2016, 9, 213–228. [Google Scholar] [CrossRef]
- Schembri, J.; Bonello, J.; Christodoulou, D.K.; Katsanos, K.H.; Ellul, P. Segmental colitis associated with diverticulosis: Is it the coexistence of colonic diverticulosis and inflammatory bowel disease? Ann. Gastroenterol. 2017, 30, 257–261. [Google Scholar] [CrossRef] [Green Version]
- DiSiena, M.S.; Birk, J.W. Diverticular Disease: The Old, the New, and the Ever-Changing View. South Med. J. 2018, 111, 144–150. [Google Scholar] [CrossRef] [PubMed]
- Schultz, J.K.; Azhar, N.; Binda, G.A.; Barbara, G.; Biondo, S.; Boermeester, M.A.; Chabok, A.; Consten, E.C.J.; van Dijk, S.T.; Johanssen, A.; et al. European Society of Coloproctology: Guidelines for the management of diverticular disease of the colon. Colorectal. Dis. 2020, 22 (Suppl. 2), 5–28. [Google Scholar] [CrossRef] [PubMed]
- Hanna, M.H.; Kaiser, A.M. Update on the management of sigmoid diverticulitis. World J. Gastroenterol. 2021, 27, 760–781. [Google Scholar] [CrossRef]
- Peery, A.F.; Shaukat, A.; Strate, L.L. AGA Clinical Practice Update on Medical Management of Colonic Diverticulitis: Expert Review. Gastroenterology 2021, 160, 906–911.e901. [Google Scholar] [CrossRef] [PubMed]
- Naomi Piscopo, P.E. Diverticular Disease: A Review on Pathophysiology and Recent Evidence. Ulst. Med. J. 2020, 89, 83–88. [Google Scholar]
- Zullo, A. Medical hypothesis: Speculating on the pathogenesis of acute diverticulitis. Ann. Gastroenterol. 2018, 31, 747–749. [Google Scholar] [CrossRef]
- Maguire, L.H.; Handelman, S.K.; Du, X.; Chen, Y.; Pers, T.H.; Speliotes, E.K. Genome-wide association analyses identify 39 new susceptibility loci for diverticular disease. Nat. Genet. 2018, 50, 1359–1365. [Google Scholar] [CrossRef] [PubMed]
- Hall, J.; Hardiman, K.; Lee, S.; Lightner, A.; Stocchi, L.; Paquette, I.M.; Steele, S.R.; Feingold, D.L. The American Society of Colon and Rectal Surgeons Clinical Practice Guidelines for the Treatment of Left-Sided Colonic Diverticulitis. Dis. Colon Rectum 2020, 63, 728–747. [Google Scholar] [CrossRef]
- MD, A.T. Advances in the management of colonic diverticulitis. Can. Med. Assoc. J. 2012. [Google Scholar] [CrossRef]
- Tursi, A. Current and Evolving Concepts on the Pathogenesis of Diverticular Disease. J. Gastrointestin. Liver Dis. 2019, 28, 225–235. [Google Scholar] [CrossRef]
- Longo, S.; Altobelli, E.; Castellini, C.; Vernia, F.; Valvano, M.; Magistroni, M.; Mancusi, A.; Viscido, A.; Ashktorab, H.; Latella, G. Non-steroidal anti-inflammatory drugs and acetylsalicylic acid increase the risk of complications of diverticular disease: A meta-analysis of case-control and cohort studies. Int. J. Colorectal. Dis. 2022, 37, 521–529. [Google Scholar] [CrossRef] [PubMed]
- Mohammed Ilyas, M.I.; Szilagy, E.J. Management of Diverticular Bleeding: Evaluation, Stabilization, Intervention, and Recurrence of Bleeding and Indications for Resection after Control of Bleeding. Clin. Colon Rectal Surg. 2018, 31, 243–250. [Google Scholar] [CrossRef]
- Scaioli, E.; Colecchia, A.; Marasco, G.; Schiumerini, R.; Festi, D. Pathophysiology and Therapeutic Strategies for Symptomatic Uncomplicated Diverticular Disease of the Colon. Dig. Dis. Sci. 2016, 61, 673–683. [Google Scholar] [CrossRef]
- Walter Elisei, A.T. Recent advances in the treatment of colonic diverticular disease and prevention of acute diverticulitis. Ann. Gastroenterol. 2016, 29, 24–32. [Google Scholar]
- Wilkins, T.; Embry, K.; George, R. Diagnosis and Management of Acute Diverticulitis. Am. Fam. Physician 2013, 87, 612–620. [Google Scholar] [PubMed]
- Minordi, L.M.; Larosa, L.; Berte, G.; Pecere, S.; Manfredi, R. CT of the acute colonic diverticulitis: A pictorial essay. Diagn. Interv. Radiol. 2020, 26, 546–551. [Google Scholar] [CrossRef] [PubMed]
- Hinchey, E.J.; Schaal, P.G.; Richards, G.K. Treatment of perforated diverticular disease of the colon. Adv. Surg. 1978, 12, 85–109. [Google Scholar]
- Wasvary, H.; Turfah, F.; Kadro, O.; Beauregard, W. Same hospitalization resection for acute diverticulitis. Am. Surg. 1999, 65, 632–635; discussion 636. [Google Scholar]
- Kaiser, A.M.; Jiang, J.K.; Lake, J.P.; Ault, G.; Artinyan, A.; Gonzalez-Ruiz, C.; Essani, R.; Beart, R.W., Jr. The management of complicated diverticulitis and the role of computed tomography. Am. J. Gastroenterol. 2005, 100, 910–917. [Google Scholar] [CrossRef]
- Cameron, J.L.; Cameron, A.M. Current Surgical Therapy, 13th ed.; Elsevier: Philadelphia, PA, USA, 2020; 1508p. [Google Scholar]
- Stollman, N.; Smalley, W.; Hirano, I.; American Gastroenterological Association Institute Committee. American Gastroenterological Association Institute Guideline on the Management of Acute Diverticulitis. Gastroenterology 2015, 149, 1944–1949. [Google Scholar] [CrossRef]
- Neil, S.; Painter, D.P.B. Diverticular Disease of the Colon: A Deficiency Disease of Western Civilization. Br. Med. J. 1971, 4, 450–454. [Google Scholar]
- Barbaro, M.R.; Cremon, C.; Fuschi, D.; Marasco, G.; Palombo, M.; Stanghellini, V.; Barbara, G. Pathophysiology of Diverticular Disease: From Diverticula Formation to Symptom Generation. Int. J. Mol. Sci. 2022, 23, 6698. [Google Scholar] [CrossRef] [PubMed]
- Peery, A.F.; Sandler, R.S.; Ahnen, D.J.; Galanko, J.A.; Holm, A.N.; Shaukat, A.; Mott, L.A.; Barry, E.L.; Fried, D.A.; Baron, J.A. Constipation and a low-fiber diet are not associated with diverticulosis. Clin. Gastroenterol. Hepatol. 2013, 11, 1622–1627. [Google Scholar] [CrossRef] [PubMed]
- Ma, W.; Nguyen, L.H.; Song, M.; Jovani, M.; Liu, P.H.; Cao, Y.; Tam, I.; Wu, K.; Giovannucci, E.L.; Strate, L.L.; et al. Intake of Dietary Fiber, Fruits, and Vegetables and Risk of Diverticulitis. Am. J. Gastroenterol. 2019, 114, 1531–1538. [Google Scholar] [CrossRef] [PubMed]
- Carabotti, M.; Falangone, F.; Cuomo, R.; Annibale, B. Role of Dietary Habits in the Prevention of Diverticular Disease Complications: A Systematic Review. Nutrients 2021, 13, 1288. [Google Scholar] [CrossRef] [PubMed]
- Desai, M.; Fathallah, J.; Nutalapati, V.; Saligram, S. Antibiotics Versus No Antibiotics for Acute Uncomplicated Diverticulitis: A Systematic Review and Meta-analysis. Dis. Colon Rectum 2019, 62, 1005–1012. [Google Scholar] [CrossRef]
- Ticinesi, A.; Nouvenne, A.; Corrente, V.; Tana, C.; Di Mario, F.; Meschi, T. Diverticular Disease: A Gut Microbiota Perspective. J. Gastrointestin. Liver Dis. 2019, 28, 327–337. [Google Scholar] [CrossRef]
- Granlund, J.; Svensson, T.; Olen, O.; Hjern, F.; Pedersen, N.L.; Magnusson, P.K.; Schmidt, P.T. The genetic influence on diverticular disease--a twin study. Aliment. Pharmacol. Ther. 2012, 35, 1103–1107. [Google Scholar] [CrossRef]
- Strate, L.L.; Erichsen, R.; Baron, J.A.; Mortensen, J.; Pedersen, J.K.; Riis, A.H.; Christensen, K.; Sorensen, H.T. Heritability and familial aggregation of diverticular disease: A population-based study of twins and siblings. Gastroenterology 2013, 144, 736–742.e731; quiz e714. [Google Scholar] [CrossRef]
- Chabok, A.; Pahlman, L.; Hjern, F.; Haapaniemi, S.; Smedh, K.; Group, A.S. Randomized clinical trial of antibiotics in acute uncomplicated diverticulitis. Br. J. Surg. 2012, 99, 532–539. [Google Scholar] [CrossRef]
- Shabanzadeh, D.M.; Wille-Jorgensen, P. Antibiotics for uncomplicated diverticulitis. Cochrane Database Syst Rev 2012, 11, CD009092. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, A.M.; Moahammed, A.T.; Mattar, O.M.; Mohamed, E.M.; Faraag, E.A.; AlSafadi, A.M.; Hirayama, K.; Huy, N.T. Surgical treatment of diverticulitis and its complications: A systematic review and meta-analysis of randomized control trials. Surgeon 2018, 16, 372–383. [Google Scholar] [CrossRef] [PubMed]
- Oberkofler, C.E.; Rickenbacher, A.; Raptis, D.A.; Lehmann, K.; Villiger, P.; Buchli, C.; Grieder, F.; Gelpke, H.; Decurtins, M.; Tempia-Caliera, A.A.; et al. A multicenter randomized clinical trial of primary anastomosis or Hartmann’s procedure for perforated left colonic diverticulitis with purulent or fecal peritonitis. Ann. Surg. 2012, 256, 819–826; discussion 826–817. [Google Scholar] [CrossRef] [PubMed]
- Binda, G.A.; Karas, J.R.; Serventi, A.; Sokmen, S.; Amato, A.; Hydo, L.; Bergamaschi, R.; Study Group on, D. Primary anastomosis vs nonrestorative resection for perforated diverticulitis with peritonitis: A prematurely terminated randomized controlled trial. Colorectal. Dis. 2012, 14, 1403–1410. [Google Scholar] [CrossRef] [PubMed]
- Meyer, J.; Orci, L.A.; Combescure, C.; Balaphas, A.; Morel, P.; Buchs, N.C.; Ris, F. Risk of Colorectal Cancer in Patients With Acute Diverticulitis: A Systematic Review and Meta-analysis of Observational Studies. Clin. Gastroenterol. Hepatol. 2019, 17, 1448–1456.e1417. [Google Scholar] [CrossRef] [Green Version]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| SCAD | SUDD | Uncomplicated Diverticulitis | Complicated Diverticulitis | |
|---|---|---|---|---|
| Location | Sigmoid colon [11] | Nonluminal [12] | Bowel wall and surrounding tissue [13] | Bowel wall and surrounding tissue [13] |
| Epidemiology | Male > female, mean age 65 years [12] | Male = female [12] | Male > female in young patients, female > male in older patients [14] | Male > female in young patients, female > male in older patients [14] |
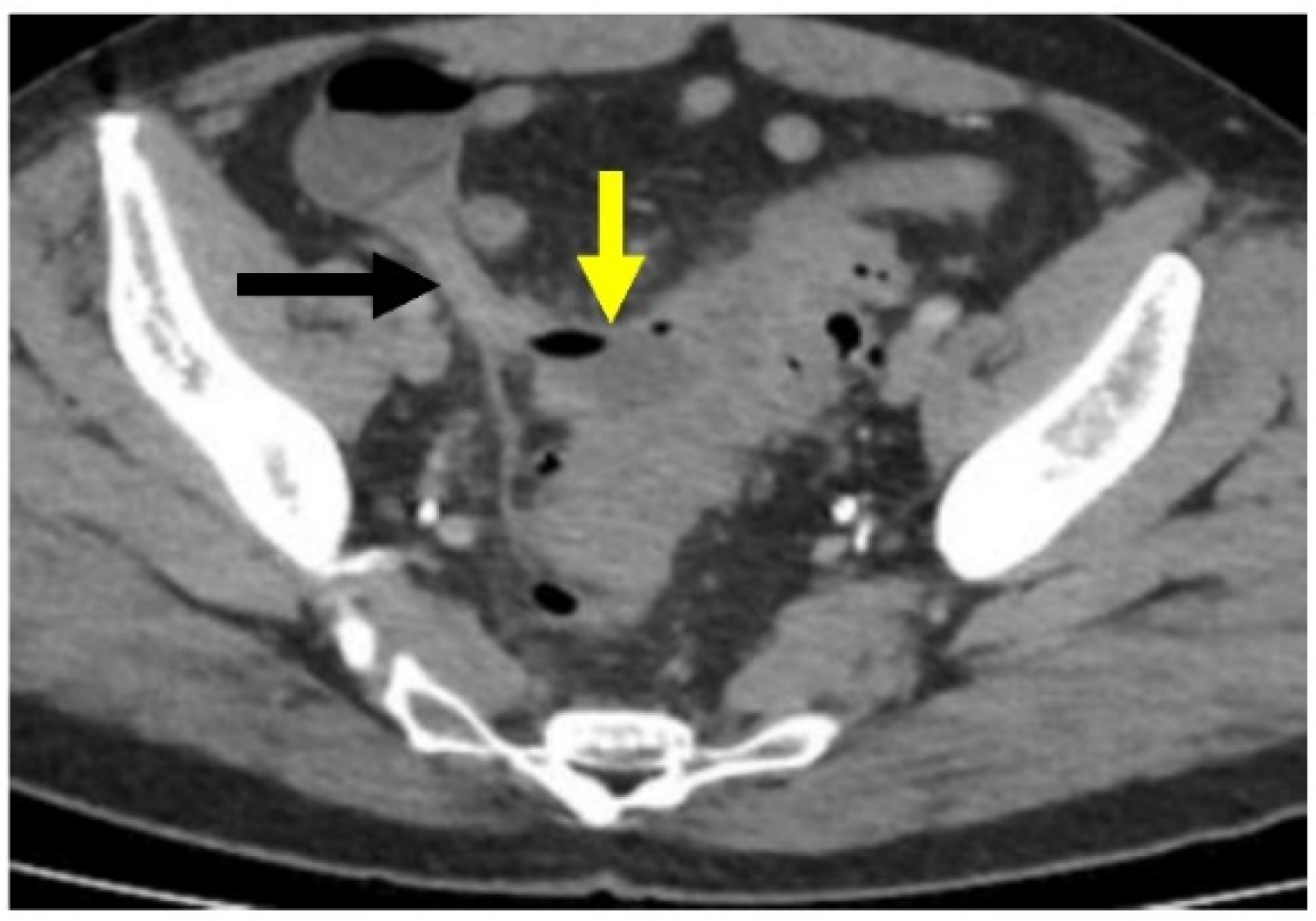
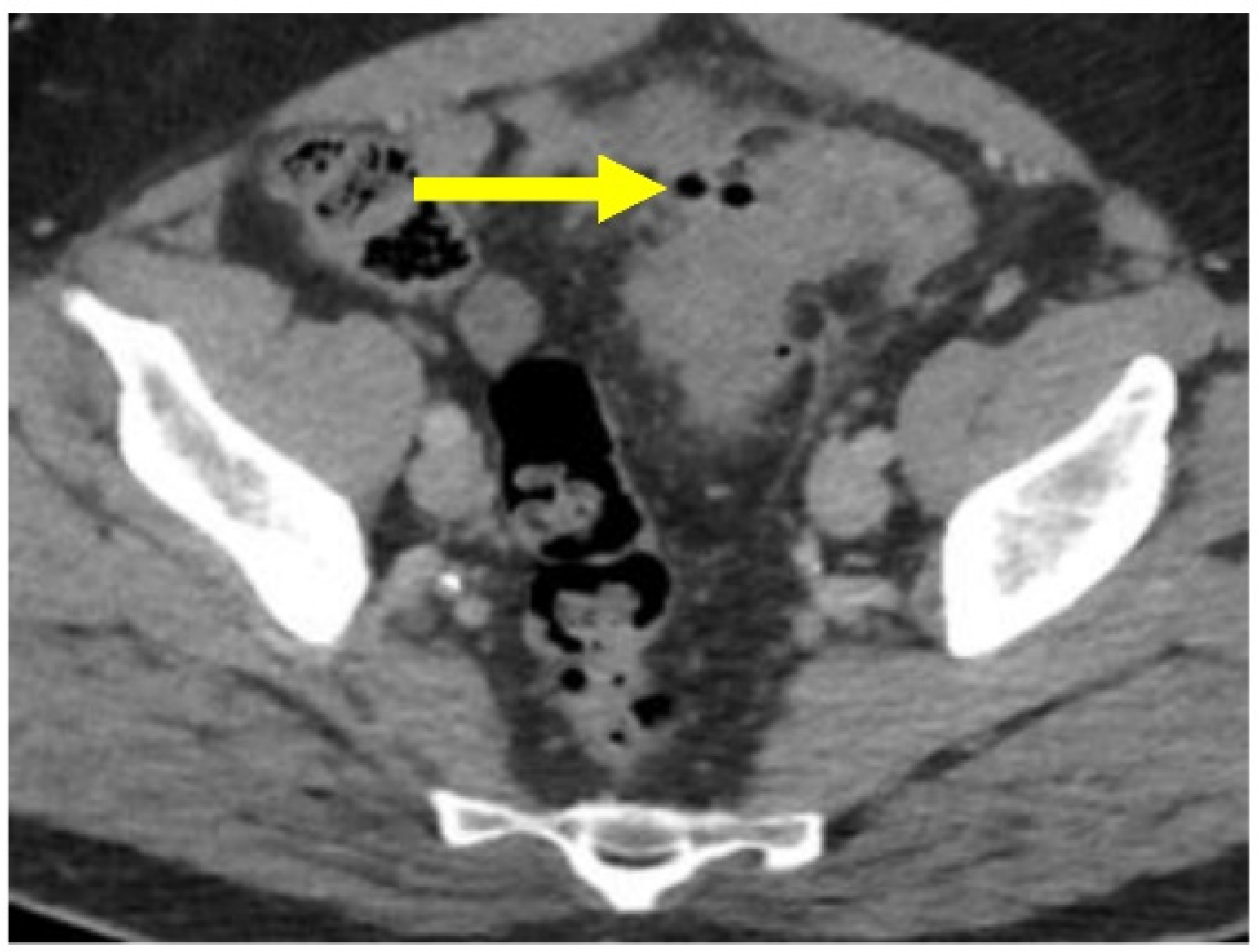
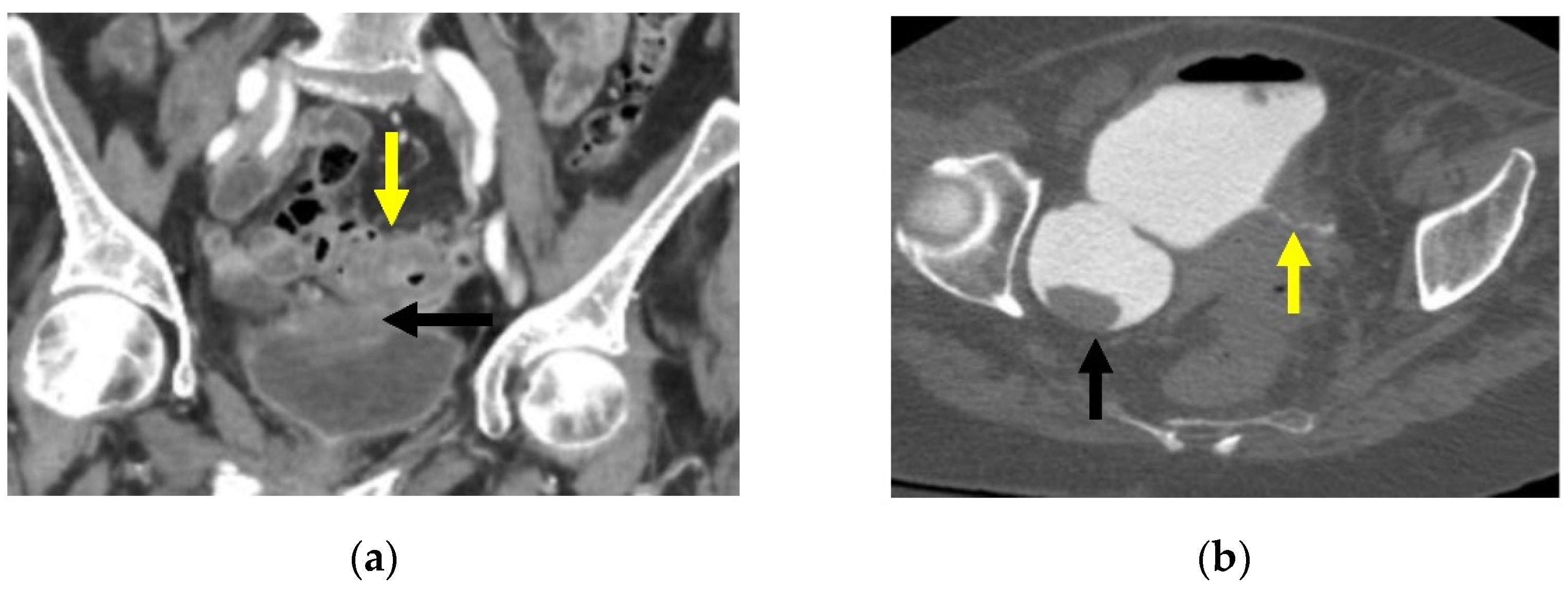
| Presentation | Rectal sparing diverticular colitis [15] | Asymptomatic | Thickening of colon wall and peri-colonic inflammatory changes [15] | Abscess, peritonitis, obstruction, stricture, and/or fistula [2,15] |
| Diagnosis | Endoscopy, confirmation with biopsy [12] | Clinical: persistent abdominal pain without acute symptoms of diverticulitis [12,16] | Clinical and/or computed tomography (CT) scan of abdomen and pelvis with contrast [15] | Clinical and/or computed tomography (CT) scan of abdomen and pelvis with contrast [15] |
| Pathogenesis | ||||
| Management |
|
|
|
| Hinchey Classification [28] | Modified Hinchey Classification [4,29,31] |
|---|---|
| I—Pericolic abscess or phlegmon | Ia—Confined pericolic abscess |
| Ib—Confined pericolic phlegmon | |
| II—Pelvic, abdominal, or retroperitoneal abscess | II—Distant pelvic, intra-abdominal, or retroperitoneal abscess |
| III—Generalized purulent peritonitis | III—Generalized purulent peritonitis |
| IV—Generalized fecal peritonitis | IV—Fecal peritonitis |
| For Intervention | Against Intervention | |
|---|---|---|
| High-fiber diets |
| |
| Antibiotic use in the treatment of uncomplicated diverticulitis |
| |
| Elective surgery [19] |
|
|
| Urgent/emergent surgery [19] |
|
|
| Type of surgery—primary anastomosis +/− diverting loop ileostomy (vs Hartmann’s procedure) [4] | For primary anastomosis
| Against primary anastomosis
|
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kishnani, S.; Ottaviano, K.; Rosenberg, L.; Arker, S.H.; Lee, H.; Schuster, M.; Tadros, M.; Valerian, B. Diverticular Disease—An Updated Management Review. Gastroenterol. Insights 2022, 13, 326-339. https://doi.org/10.3390/gastroent13040033
Kishnani S, Ottaviano K, Rosenberg L, Arker SH, Lee H, Schuster M, Tadros M, Valerian B. Diverticular Disease—An Updated Management Review. Gastroenterology Insights. 2022; 13(4):326-339. https://doi.org/10.3390/gastroent13040033
Chicago/Turabian StyleKishnani, Sujata, Kathryn Ottaviano, Lisa Rosenberg, Soe Htet Arker, Hwajeong Lee, Michael Schuster, Micheal Tadros, and Brian Valerian. 2022. "Diverticular Disease—An Updated Management Review" Gastroenterology Insights 13, no. 4: 326-339. https://doi.org/10.3390/gastroent13040033