
Abdominal and Thoracic Imaging Features in Children with MIS-C
 , , , ,
, , , , 
Abstract
:1. Introduction
2. Materials and Methods
- (1)
- (2)
- (3)
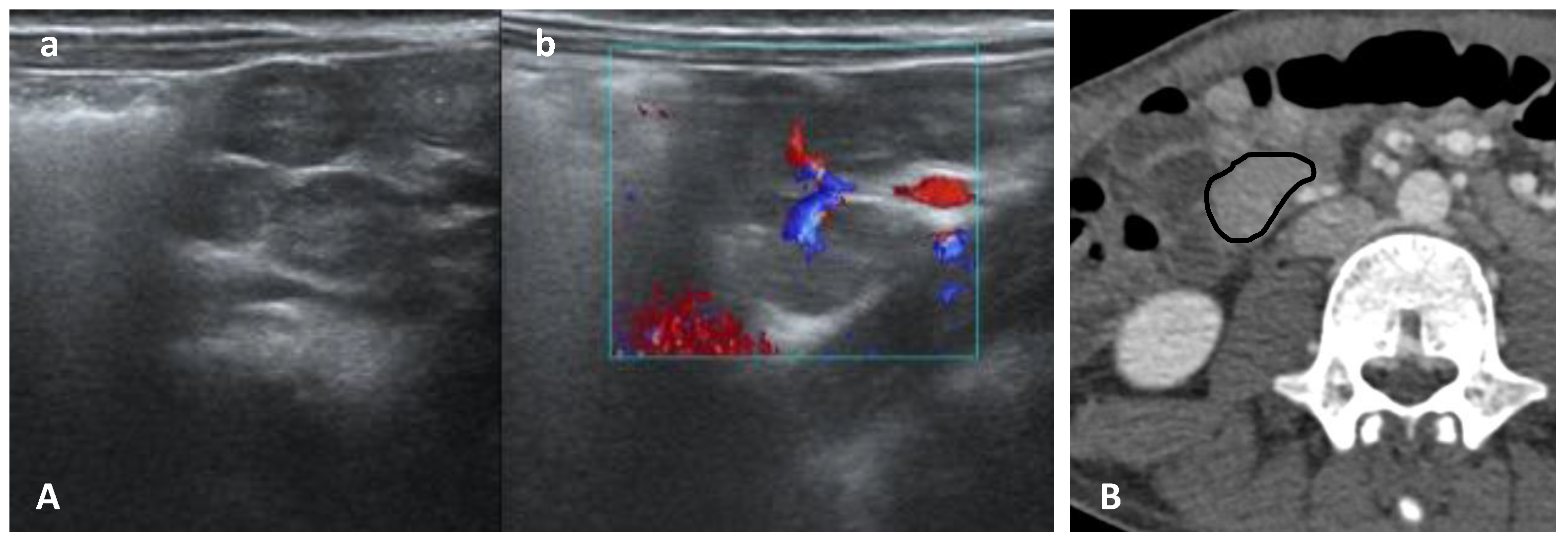
- Cervical, mediastinal, and axillary lymphadenopathy.
- (4)
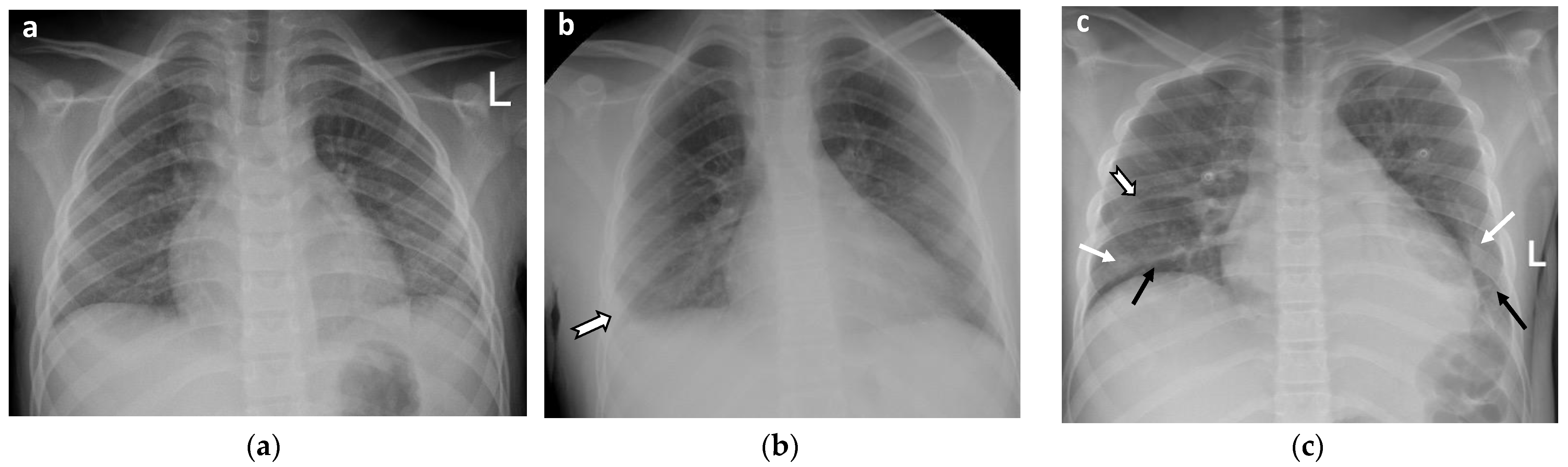
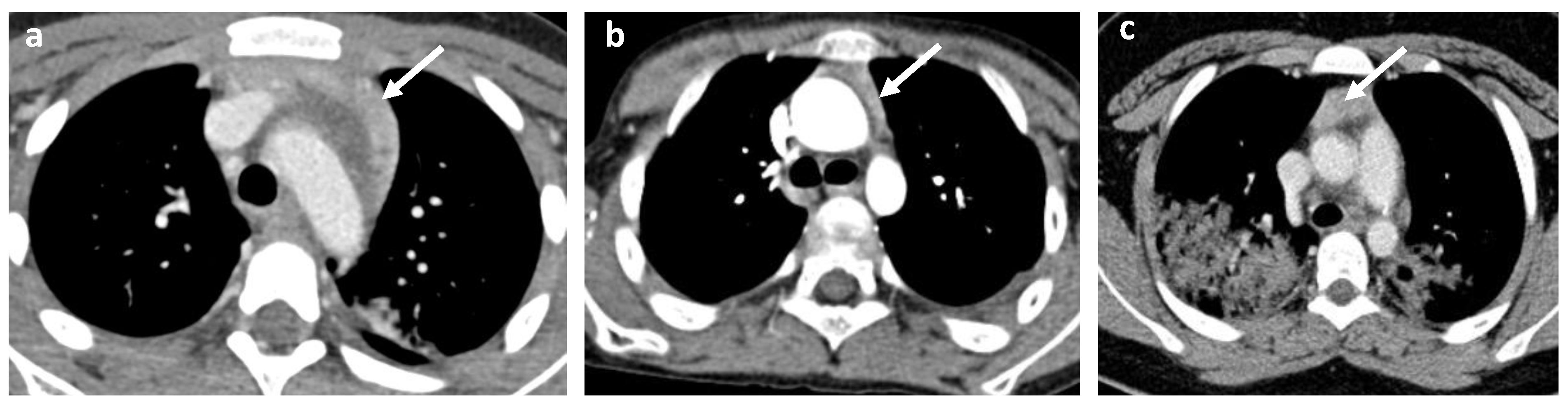
- Cardiovascular abnormalities including cardiomegaly (Figure 1c) and signs of pericarditis, myocarditis, and pericardial effusion.
- (1)
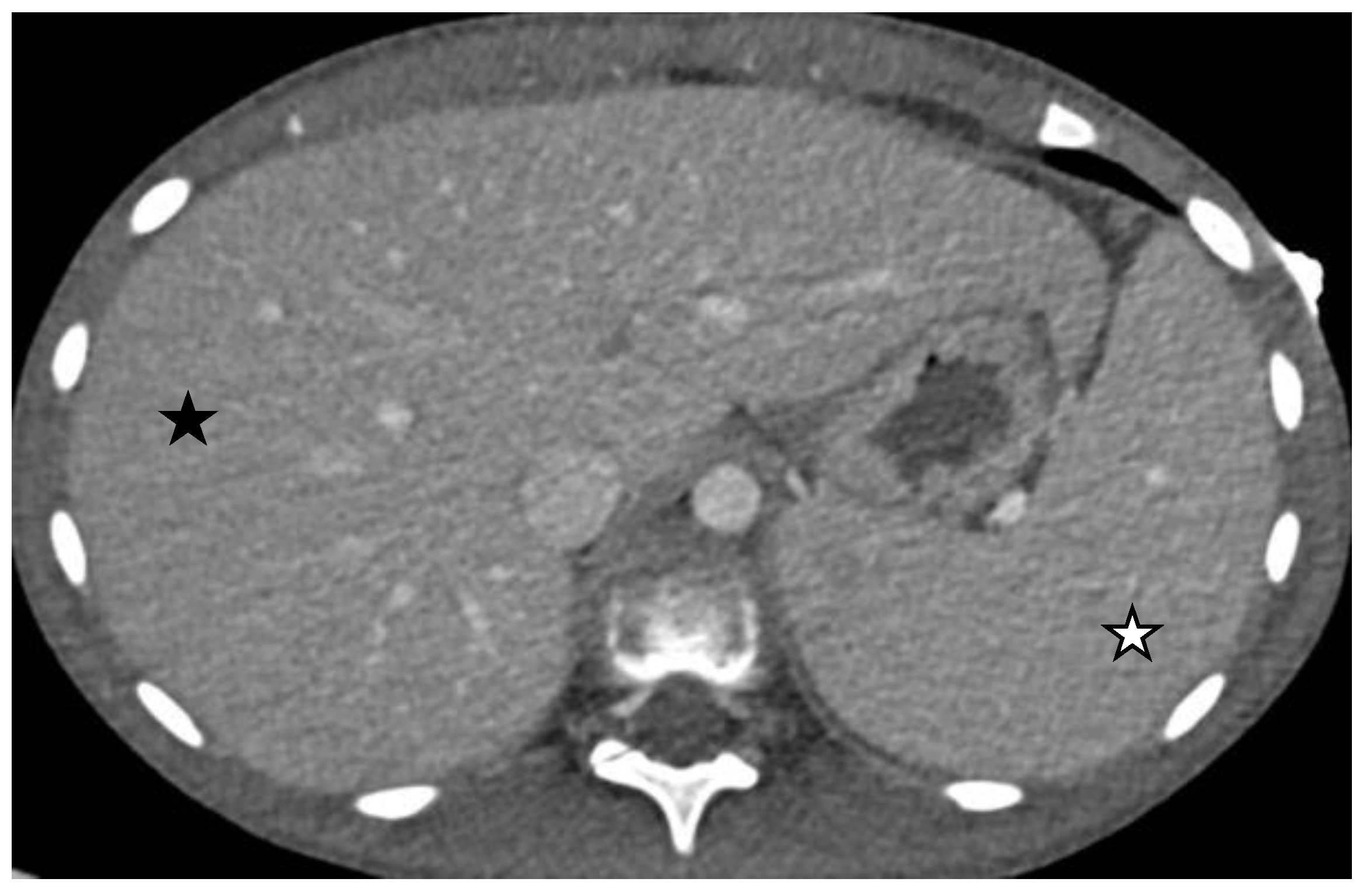
- Size abnormalities of the liver and spleen (Figure 3), kidneys, and pancreas.
- (2)
- Parenchymal abnormalities of the solid organs (heterogeneous echotexture of the liver or spleen, increased echogenicity of the renal parenchyma compared to the liver, and abnormal or heterogeneous attenuation).
- (3)
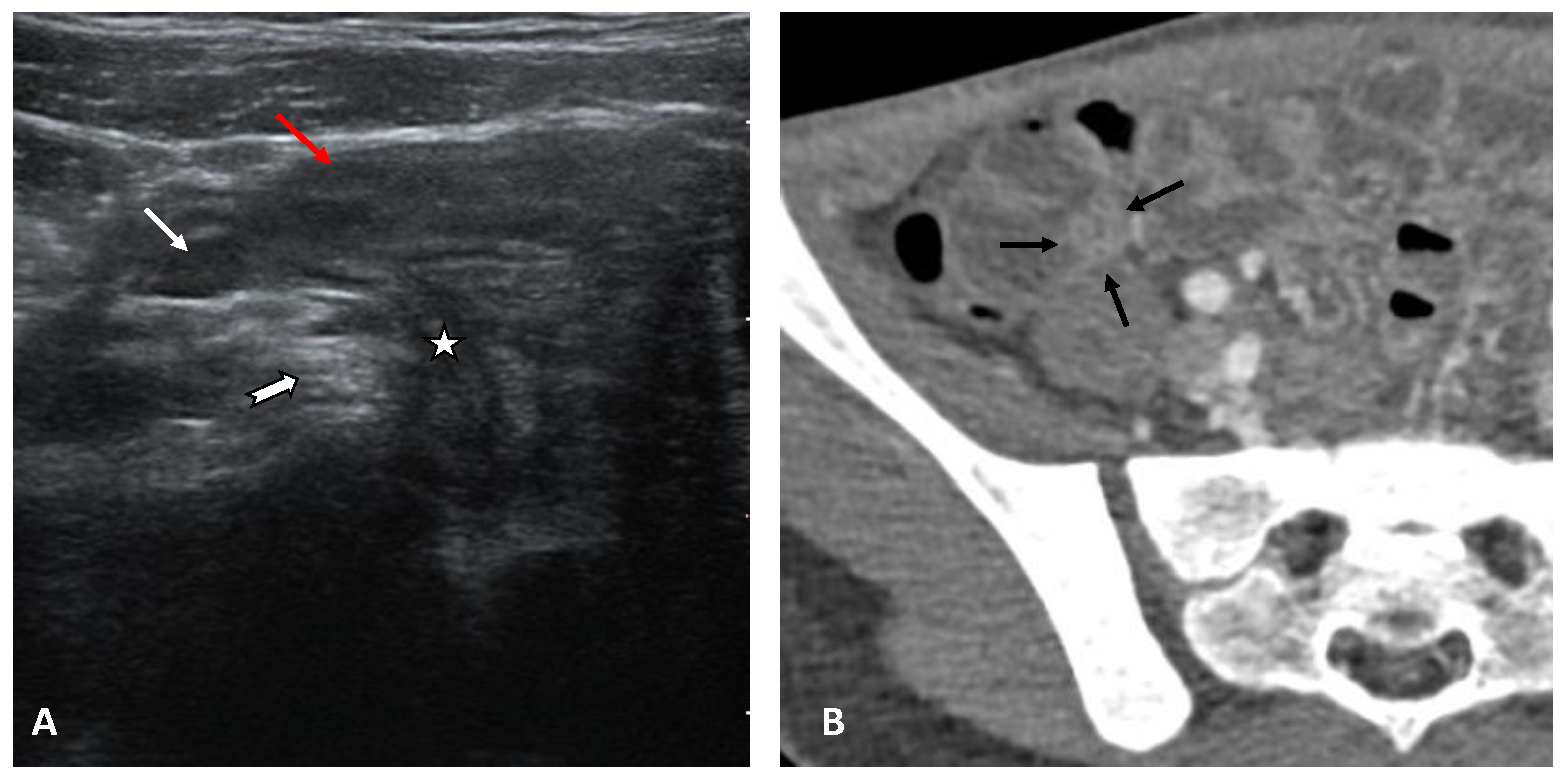
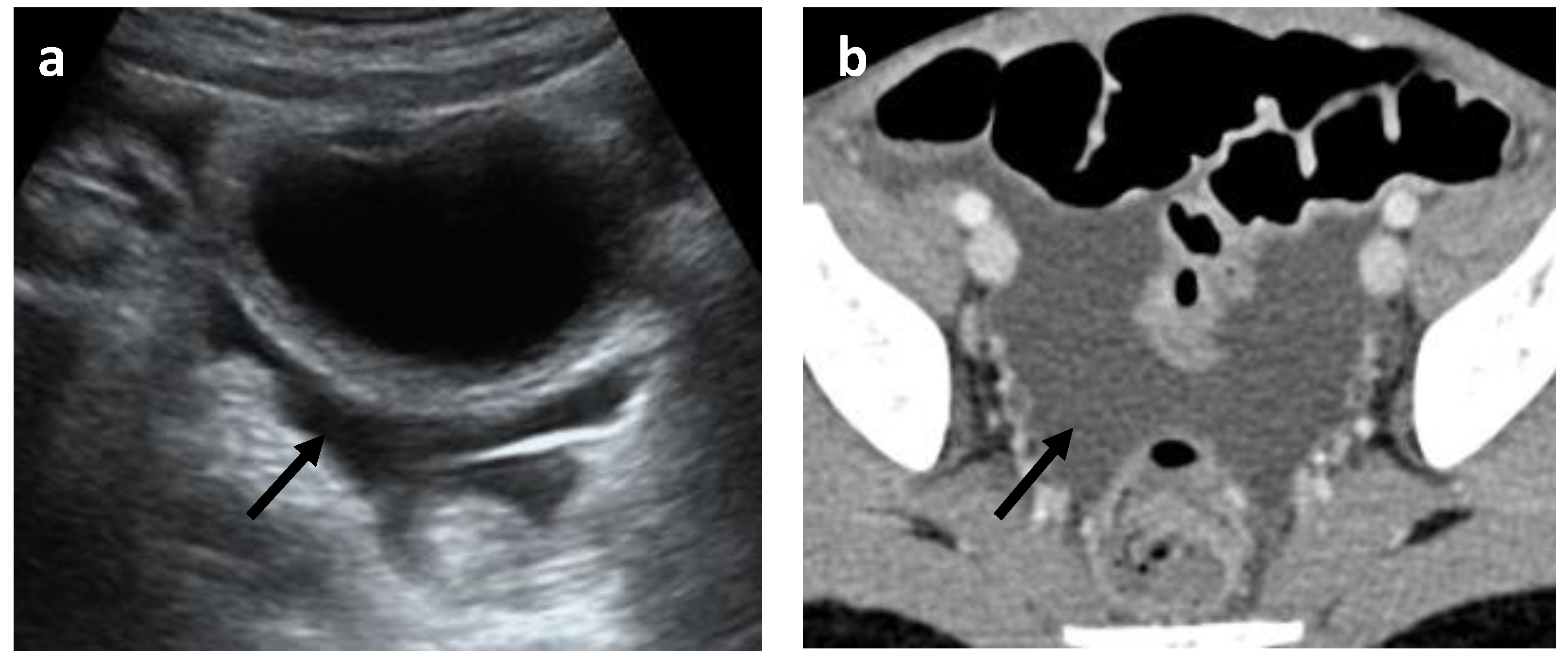
- Abnormalities of the hollow visceral organs, including distension and wall thickening of the gallbladder (Figure 4), stomach, bowel, small bowel (Figure 5A, and urinary bladder (on CT and ultrasound). They were considered thickened if >3 mm. Additionally, the cross-sectional diameter of appendix is considered enlarged if >6 mm (Figure 5B).
- (4)
- Peritoneal abnormalities—ascites (Figure 6), fluid collections, and pneumoperitoneum.
- (5)
- Mesenteric and retroperitoneal lymphadenopathy (Figure 7) with mesenteric lymph nodes considered enlarged if >5 mm in short axis and retroperitoneal lymph nodes considered enlarged if >9 mm in short axis.
3. Results
3.1. Demography
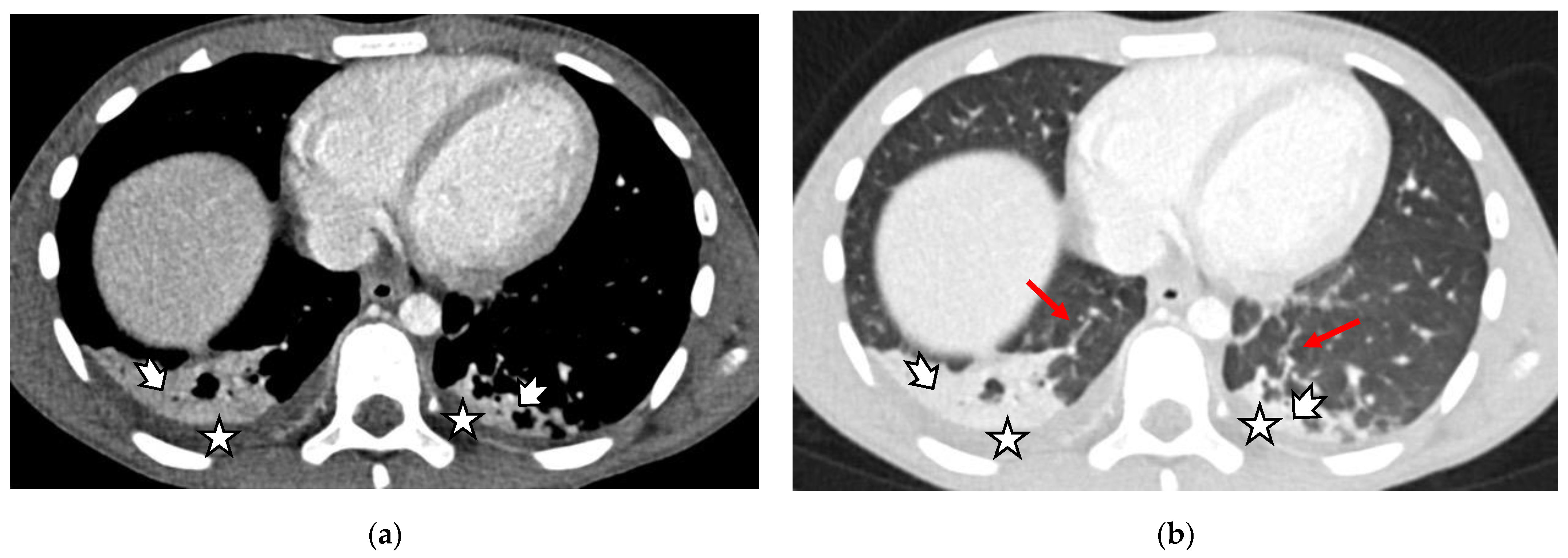
3.2. Main Pulmonary Imaging Findings
3.3. Main Gastrointestinal Imaging Findings
3.4. Other Imaging Modalities and Findings
4. Discussion
5. Practical Implications and Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- CDC Health Advisory. Case Definition for MIS-C. Available online: https://www.cdc.gov/mis/mis-c/hcp/ (accessed on 9 August 2022).
- Payne, A.B.; Gilani, Z.; Godfred-Cato, S.; Belay, E.D.; Feldstein, L.R.; Patel, M.M.; Randolph, A.G.; Newhams, M.; Thomas, D.; Magleby, R.; et al. Incidence of Multisystem Inflammatory Syndrome in Children Among US Persons Infected With SARS-CoV-2. JAMA Netw. Open 2021, 4, e2116420. [Google Scholar] [CrossRef] [PubMed]
- Feldstein, L.R.; Tenforde, M.W.; Friedman, K.G.; Newhams, M.; Rose, E.B.; Dapul, H.; Soma, V.L.; Maddux, A.B.; Mourani, P.M.; Bowens, C.; et al. Characteristics and Outcomes of US Children and Adolescents with Multisystem Inflammatory Syndrome in Children (MIS-C) Compared With Severe Acute COVID-19. JAMA 2021, 325, 1074. [Google Scholar] [CrossRef]
- Toubiana, J.; Poirault, C.; Corsia, A.; Bajolle, F.; Fourgeaud, J.; Angoulvant, F.; Debray, A.; Basmaci, R.; Salvador, E.; Biscardi, S.; et al. Kawasaki-like Multisystem Inflammatory Syndrome in Children during the Covid-19 Pandemic in Paris, France: Prospective Observational Study. BMJ 2020, 369, m2094. [Google Scholar] [CrossRef] [PubMed]
- Sivit, C.J.; Newman, K.D.; Chandra, R.S. Visualization of Enlarged Mesenteric Lymph Nodes at US Examination. Pediatr. Radiol. 1993, 23, 471–475. [Google Scholar] [CrossRef] [PubMed]
- Rostad, B.S.; Shah, J.H.; Rostad, C.A.; Jaggi, P.; Richer, E.J.; Linam, L.E.; Alazraki, A.L.; Riedesel, E.L.; Milla, S.S. Chest Radiograph Features of Multisystem Inflammatory Syndrome in Children (MIS-C) Compared to Pediatric COVID-19. Pediatr. Radiol. 2021, 51, 231–238. [Google Scholar] [CrossRef] [PubMed]
- Blumfield, E.; Levin, T.L.; Kurian, J.; Lee, E.Y.; Liszewski, M.C. Imaging Findings in Multisystem Inflammatory Syndrome in Children (MIS-C) Associated with Coronavirus Disease (COVID-19). Am. J. Roentgenol. 2021, 216, 507–517. [Google Scholar] [CrossRef]
- Capone, C.A.; Misra, N.; Ganigara, M.; Epstein, S.; Rajan, S.; Acharya, S.S.; Hayes, D.A.; Kearney, M.B.; Romano, A.; Friedman, R.A.; et al. Six Month Follow-up of Patients With Multi-System Inflammatory Syndrome in Children. Pediatrics 2021, 148, e2021050973. [Google Scholar] [CrossRef] [PubMed]
- Harwood, R.; Partridge, R.; Minford, J.; Almond, S. Paediatric Abdominal Pain in the Time of COVID-19: A New Diagnostic Dilemma. J. Surg. Case Rep. 2020, 2020, rjaa337. [Google Scholar] [CrossRef] [PubMed]
- Musolino, A.M.; Boccuzzi, E.; Buonsenso, D.; Supino, M.C.; Mesturino, M.A.; Pitaro, E.; Ferro, V.; Nacca, R.; Sinibaldi, S.; Palma, P.; et al. The Role of Lung Ultrasound in Diagnosing COVID-19-Related Multisystemic Inflammatory Disease: A Preliminary Experience. J. Clin. Med. 2022, 11, 234. [Google Scholar] [CrossRef] [PubMed]
- Hameed, S.; Elbaaly, H.; Reid, C.E.L.; Santos, R.M.F.; Shivamurthy, V.; Wong, J.; Jogeesvaran, K.H. Spectrum of Imaging Findings at Chest Radiography, US, CT, and MRI in Multisystem Inflammatory Syndrome in Children Associated with COVID-19. Radiology 2021, 298, E1–E10. [Google Scholar] [CrossRef]
- Kurian, J.; Blumfield, E.; Levin, T.L.; Liszewski, M.C. Imaging Findings in Acute Pediatric Coronavirus Disease 2019 (COVID-19) Pneumonia and Multisystem Inflammatory Syndrome in Children (MIS-C). Pediatr. Radiol. 2022, 52, 1985–1997. [Google Scholar] [CrossRef]
- Ibrahim, H.M.; Mohammad, S.A.; Fouda, E.; Abouelfotouh, K.; Habeeb, N.M.; Rezk, A.R.; Magdy, S.; Allam, A.M.; Mahmoud, S.A. Clinical Characteristics and Pulmonary Computerized Imaging Findings of Critically Ill Egyptian Patients with Multisystem Inflammatory Syndrome in Children. Glob. Pediatr. Health 2022, 9, 2333794X2210853. [Google Scholar] [CrossRef]
- Liguori, C.; Farina, D.; Vaccher, F.; Ferrandino, G.; Bellini, D.; Carbone, I. Myocarditis: Imaging up to Date. Radiol. Med. 2020, 125, 1124–1134. [Google Scholar] [CrossRef] [PubMed]
- Wu, E.Y.; Campbell, M.J. Cardiac Manifestations of Multisystem Inflammatory Syndrome in Children (MIS-C) Following COVID-19. Curr. Cardiol. Rep. 2021, 23, 168. [Google Scholar] [CrossRef] [PubMed]
- Lazova, S.; Alexandrova, T.; Gorelyova-Stefanova, N.; Atanasov, K.; Tzotcheva, I.; Velikova, T. Liver Involvement in Children with COVID-19 and Multisystem Inflammatory Syndrome: A Single-Center Bulgarian Observational Study. Microorganisms 2021, 9, 1958. [Google Scholar] [CrossRef] [PubMed]
- Lazova, S.; Tzotcheva, I.; Alexandrova, T.; Gorelyova-Stefanova, N.; Rangelov, E.; Ganev, B.; Velikova, T. Acute Gastrointestinal Symptoms in Children with Multisystem Inflammatory Syndrome—A Literature Review with the Presentation of Two Clinical Cases. A Pediatr. 2021, 2, 64–69. [Google Scholar]
- Sayed, A.; Zeidan, N.; Fahmy, D.; Ibrahim, H. Diagnostic Reliability of Pediatric Appendicitis Score, Ultrasound and Low-Dose Computed Tomography Scan in Children with Suspected Acute Appendicitis. Ther. Clin. Risk Manag. 2017, 13, 847–854. [Google Scholar] [CrossRef]
- Tullie, L.; Ford, K.; Bisharat, M.; Watson, T.; Thakkar, H.; Mullassery, D.; Giuliani, S.; Blackburn, S.; Cross, K.; De Coppi, P.; et al. Gastrointestinal Features in Children with COVID-19: An Observation of Varied Presentation in Eight Children. Lancet Child Adolesc. Health 2020, 4, e19–e20. [Google Scholar] [CrossRef]
- Ucan, B.; Kaynak Sahap, S.; Cinar, H.G.; Tasci Yildiz, Y.; Uner, C.; Polat, M.; Derinkuyu, B.E. Multisystem Inflammatory Syndrome in Children Associated with SARS-CoV-2: Extracardiac Radiological Findings. Br. J. Radiol. 2022, 95, 20210570. [Google Scholar] [CrossRef] [PubMed]
- Belhadjer, Z.; Méot, M.; Bajolle, F.; Khraiche, D.; Legendre, A.; Abakka, S.; Auriau, J.; Grimaud, M.; Oualha, M.; Beghetti, M.; et al. Acute Heart Failure in Multisystem Inflammatory Syndrome in Children in the Context of Global SARS-CoV-2 Pandemic. Circulation 2020, 142, 429–436. [Google Scholar] [CrossRef] [PubMed]
- Dasgupta, K.; Finch, S.E. A Case of Pediatric Multisystem Inflammatory Syndrome Temporally Associated with COVID-19 in South Dakota. S. D. Med. 2020, 73, 246–251. [Google Scholar]
- Moteki, T.; Horikoshi, H. New CT Criterion for Acute Appendicitis: Maximum Depth of Intraluminal Appendiceal Fluid. Am. J. Roentgenol. 2007, 188, 1313–1319. [Google Scholar] [CrossRef] [PubMed]
- Miller, J.; Cantor, A.; Zachariah, P.; Ahn, D.; Martinez, M.; Margolis, K.G. Gastrointestinal Symptoms as a Major Presentation Component of a Novel Multisystem Inflammatory Syndrome in Children That Is Related to Coronavirus Disease 2019: A Single Center Experience of 44 Cases. Gastroenterology 2020, 159, 1571–1574.e2. [Google Scholar] [CrossRef] [PubMed]
- Meshaka, R.; Whittam, F.C.; Guessoum, M.; Eleti, S.; Shelmerdine, S.C.; Arthurs, O.J.; McHugh, K.; Hiorns, M.P.; Humphries, P.D.; Calder, A.D.; et al. Abdominal US in Pediatric Inflammatory Multisystem Syndrome Associated with SARS-CoV-2 (PIMS-TS). Radiology 2022, 303, 173–181. [Google Scholar] [CrossRef] [PubMed]
- Cuvelier, P.; Roux, H.; Couëdel-Courteille, A.; Dutrieux, J.; Naudin, C.; Charmeteau de Muylder, B.; Cheynier, R.; Squara, P.; Marullo, S. Protective Reactive Thymus Hyperplasia in COVID-19 Acute Respiratory Distress Syndrome. Crit. Care 2021, 25, 4. [Google Scholar] [CrossRef]
- Samir, A.; Bastawi, R.A.; Baess, A.I.; Sweed, R.A.; Eldin, O.E. Thymus CT-Grading and Rebound Hyperplasia during COVID-19 Infection: A CT Volumetric Study with Multivariate Linear Regression Analysis. Egypt. J. Radiol. Nucl. Med. 2022, 53, 112. [Google Scholar] [CrossRef]
- Güneş, H.; Dinçer, S.; Acıpayam, C.; Yurttutan, S.; Özkars, M.Y. What Chances Do Children Have against COVID-19? Is the Answer Hidden within the Thymus? Eur. J. Pediatr. 2021, 180, 983–986. [Google Scholar] [CrossRef] [PubMed]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | Number | Percent | |
|---|---|---|---|
| Number | 51 | ||
| Sex, %male | 37 | 72.5% | |
| Mean age, years | 8.72 (1–16) | ||
| Digestive symptoms | Vomiting | 26 | 51% |
| Diarrhoea | 23 | 45% | |
| Any | 37 | 72.5% | |
| Respiratory symptoms Cough, chest pain, different degrees of respiratory distress | 23 | 45% | |
| Heart involvement | Any (clinical, laboratory, imaging, and functional evidence) | 26 | 51% |
| Myocarditis | 6 | 12% | |
| Myocarditis rapidly progressing to cardiovascular shock | 3 | 5.9% | |
| Renal involvement (severe acute renal failure) | 1 | 2% | |
| Performed Imaging Tests | Number | Percent | |
| Chest X-ray | 36 | 70.5% | |
| Abdominal X-ray | 10 | 19.6% | |
| Thoracic CT | 22 | 43.1% | |
| Abdominal CT | 20 | 39.2% | |
| Thoracic and abdominal CT | 19 | 37.2% | |
| Abdominal US | 51 | 100% | |
| Thoracic US | 35 | 68.6% | |
| Echocardiography | 37 | 72.5% | |
| Neck US | 5 | 9.8% | |
| Testicular US | 3 | 5.9% | |
| Imaging Test, N Tested | Pathological Findings | Number | % Tested | % All |
|---|---|---|---|---|
| Chest CT scan findings, N 22 | CT ground glass | 12 | 54.5% | 23.5% |
| Crazy paving pattern | 1 | 4.5% | 2.0% | |
| Subsegmental atelectasis | 5 | 22.7% | 9.8% | |
| Posterior basal consolidation | 16 | 72.7% | 31.4% | |
| Air bronchogram | 3 | 13.6% | 5.9% | |
| Pleural effusion | 14 | 63.6% | 27.5% | |
| Pericardial effusion | 4 | 18.2% | 7.8% | |
| Cervical lymphadenitis | 10 | 45.5% | 19.6% | |
| Mediastinal lymphadenitis | 4 | 18.2% | 7.8% | |
| Axillar lymphadenitis | 3 | 13.6% | 5.9% | |
| Thymic enhancement | 5 | 22.7% | 9.8% | |
| Chest X-ray findings, N 36 | Lung and/or heart pathology | 16 | 44.4% | 31.4% |
| Thoracic US, N 35 | Pleural effusion | 30 | 86% | 58.82% |
| Small | 24 | 69% | 47.06% | |
| Moderate | 4 | 11% | 7.84% | |
| Large | 1 | 3% | 1.96% | |
| Fibrinous | 1 | 3% | 1.96% | |
| Bilateral | 20 | 57% | 39.22% | |
| Echocardiography, N 37 | Pericarditis | 29 | 78% | 56.86% |
| Small pericardial effusion | 16 | 43% | 31.37% |
| Imaging Test, N Tested | Pathological Findings | Number | % Tested | % All |
|---|---|---|---|---|
| Abdominal CT scan, N 20 | Mesenteric lymphadenitis | 14 | 70% | 27.5% |
| Colitis | 5 | 25% | 9.8% | |
| Terminal ileitis | 10 | 50% | 19.6% | |
| Terminal ileitis and appendicitis | 4 | 20% | 7.8% | |
| Hepatic enlargement | 8 | 40% | 15.7% | |
| Splenic enlargement | 9 | 45% | 17.6% | |
| Renal pathology, any | 5 | 25% | 9.8% | |
| Renal enlargement | 3 | 15% | 5.9% | |
| Pyelectasis | 1 | 5% | 2.0% | |
| Nephrocalcinosis | 1 | 5% | 2.0% | |
| Pancreatic oedema | 1 | 5% | 2.0% | |
| Gallbladder wall thickening | 2 | 10% | 3.9% | |
| Ascites | 17 | 85% | 33.3% | |
| Abdominal X-ray, N 10 | Enteric gas | 3 | 30% | 5.9% |
| Hydroaeric | 1 | 10% | 2% | |
| Enteric gas plus hydroaeric | 5 | 50% | 9.8% | |
| Pneumoperitoneum | 1 | 1% | 2.0% | |
| Abdominal US, N 51 | Gallbladder sludge | 2 | 3.9% | 3.9% |
| Gallbladder wall thickening | 2 | 3.9% | 3.9% | |
| Gallbladder concernments | 1 | 2.0% | 2% | |
| Mesenteric lymphadenitis | 28 | 54.9% | 54.9% | |
| Mesenteric lymphadenitis Diffuse | 9 | 17.6% | 17.6% | |
| Mesenteric lymphadenitis Ileocecal | 7 | 13.7% | 13.7% | |
| Mesenteric lymphadenitis Diffuse and ileocecal | 4 | 7.8% | 7.8% | |
| Enteritis/enterocolitis | 4 | 7.8% | 7.8% | |
| Gas/liquid intestinal | 7 | 13.7% | 13.7% | |
| Ascites | 33 | 64.7% | 64.7% | |
| Hepatic enlargement | 5 | 9.8% | 9.8% | |
| Splenic enlargements | 5 | 9.8% | 9.8% | |
| Renal pathology, any | 5 | 9.8% | 9.8% | |
| Renal pathology, enlarged | 2 | 3.9% | 3.9% | |
| Renal pathology, hyperechogenic | 1 | 2% | 2% | |
| Renal pathology, hydronephrosis | 1 | 2% | 2% | |
| Renal pathology, hydrocalicosis | 1 | 2% | 2% |
| Imaging Test, N Tested | Pathological Findings | Number | % Tested | % All |
|---|---|---|---|---|
| Neck US, N 5 | Lymphadenopathy | 3 | 60% | 5.88% |
| Lymphadenitis and parotitis | 2 | 40% | 3.92% | |
| Testicular US, N 3 | Unilateral hydrocele | 3 | 100% | 5.88% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ilieva, E.; Kostadinova, V.; Tzotcheva, I.; Rimpova, N.; Paskaleva, Y.; Lazova, S. Abdominal and Thoracic Imaging Features in Children with MIS-C. Gastroenterol. Insights 2022, 13, 313-325. https://doi.org/10.3390/gastroent13040032
Ilieva E, Kostadinova V, Tzotcheva I, Rimpova N, Paskaleva Y, Lazova S. Abdominal and Thoracic Imaging Features in Children with MIS-C. Gastroenterology Insights. 2022; 13(4):313-325. https://doi.org/10.3390/gastroent13040032
Chicago/Turabian StyleIlieva, Elena, Vilyana Kostadinova, Iren Tzotcheva, Nadezhda Rimpova, Yordanka Paskaleva, and Snezhina Lazova. 2022. "Abdominal and Thoracic Imaging Features in Children with MIS-C" Gastroenterology Insights 13, no. 4: 313-325. https://doi.org/10.3390/gastroent13040032