

Prediction of Poor Outcome after Successful Thrombectomy in Patients with Severe Acute Ischemic Stroke: A Pilot Retrospective Study
 , , , ,
, , , ,
Abstract
:1. Introduction
2. Material and Methods
2.1. Patient Selection
2.2. Data Extraction
2.3. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- GBD 2019 Stroke Collaborators. Global, regional, and national burden of stroke and its risk factors, 1990–2019: A systematic analysis for the Global Burden of Disease Study 2019. Lancet Neurol. 2021, 20, 795–820. [Google Scholar] [CrossRef] [PubMed]
- Lakomkin, N.; Dhamoon, M.; Carroll, K.; Singh, I.P.; Tuhrim, S.; Lee, J.; Fifi, J.T. Prevalence of large vessel occlusion in patients presenting with acute ischemic stroke: A 10-year systematic review of the literature. J. Neurointerv. Surg. 2019, 11, 241–245. [Google Scholar] [CrossRef]
- Rennert, R.C.; Wali, A.R.; A Steinberg, J.; Santiago-Dieppa, D.R.; Olson, S.; Pannell, J.S.; A Khalessi, A. Epidemiology, Natural History, and Clinical Presentation of Large Vessel Ischemic Stroke. Neurosurgery 2019, 85, S4–S8. [Google Scholar] [CrossRef]
- Nogueira, R.G.; Jadhav, A.P.; Haussen, D.C.; Bonafe, A.; Budzik, R.F.; Bhuva, P.; Yavagal, D.R.; Ribo, M.; Cognard, C.; Hanel, R.A.; et al. Thrombectomy 6 to 24 Hours after Stroke with a Mismatch between Deficit and Infarct. N. Engl. J. Med. 2018, 378, 11–21. [Google Scholar] [CrossRef] [PubMed]
- Albers, G.W.; Lansberg, M.G.; Kemp, S.; Tsai, J.P.; Lavori, P.; Christensen, S.; Mlynash, M.; Kim, S.; Hamilton, S.; Yeatts, S.D.; et al. A multicenter randomized controlled trial of endovascular therapy following imaging evaluation for ischemic stroke (DEFUSE 3). Int. J. Stroke 2017, 12, 896–905. [Google Scholar] [CrossRef]
- Heit, J.J.; Mlynash, M.; Christensen, S.; Kemp, S.M.; Lansberg, M.G.; Marks, M.P.; Olivot, J.M.; Gregory, A.W. What predicts poor outcome after successful thrombectomy in late time windows? J. Neurointerv. Surg. 2021, 13, 421–425. [Google Scholar] [CrossRef] [PubMed]
- Jindal, G.; Carvalho, H.D.P.; Wessell, A.; Le, E.; Naragum, V.; Miller, T.R.; Wozniak, M.; Shivashankar, R.; A Cronin, C.; Schrier, C.; et al. Beyond the first pass: Revascularization remains critical in stroke thrombectomy. J. NeuroInterv. Surg. 2019, 11, 1095–1099. [Google Scholar] [CrossRef]
- Linfante, I.; Starosciak, A.K.; Walker, G.R.; Dabus, G.; Castonguay, A.C.; Gupta, R.; Sun, C.H.J.; Martin, C.; Holloway, W.E.; Mueller-Kronast, N.; et al. Predictors of poor outcome despite recanalization: A multiple regression analysis of the NASA registry. J. Neurointerv. Surg. 2016, 8, 224–229. [Google Scholar] [CrossRef] [PubMed]
- Olivot, J.-M.; Heit, J.J.; Mazighi, M.; Raposo, N.; Albucher, J.F.; Rousseau, V.; Guenego, A.; Thalamas, C.; Mlynash, M.; Drif, A.; et al. What predicts poor outcome after successful thrombectomy in early time window? J. Neurointerv. Surg. 2022, 14, 1051–1055. [Google Scholar]
- Tonetti, D.; Desai, S.M.; Casillo, S.; Stone, J.; Brown, M.; Jankowitz, B.; Jovin, T.G.; A Gross, B.; Jadhav, A. Successful reperfusion, rather than number of passes, predicts clinical outcome after mechanical thrombectomy. J. NeuroInterv. Surg. 2019, 12, 548–551. [Google Scholar] [CrossRef]
- Huber, T.; Kleine, J.F.; Kaesmacher, J.; Bette, S.; Poppert, H.; Zimmer, C.; Boeckh-Behrens, T. Blood Leukocytes as Prognostic Parameter in Stroke Thrombectomy. Cerebrovasc. Dis. 2016, 42, 32–40. [Google Scholar] [CrossRef]
- Sabença, F.; Carvalho, A.; Rocha, M.; Araújo, A.; Rodrigues, M.; Cunha, A.; Ribeiro, M.; Castro, S.; Costa, H.; Barros, P.; et al. Mean platelet volume and mechanical thrombectomy. J. Stroke Cerebrovasc. Dis. 2020, 29, 104971. Available online: https://www.strokejournal.org/article/S1052-3057(20)30389-X/fulltext (accessed on 27 July 2022). [CrossRef]
- Kim, J.-T.; Jahan, R.; Saver, J.L.; SWIFT Investigators. Impact of Glucose on Outcomes in Patients Treated With Mechanical Thrombectomy: A Post Hoc Analysis of the Solitaire Flow Restoration With the Intention for Thrombectomy Study. Stroke 2016, 47, 120–127. [Google Scholar] [CrossRef]
- Miyamoto, N.; Tanaka, Y.; Ueno, Y.; Kawamura, M.; Shimada, Y.; Tanaka, R.; Hattori, N.; Urabe, T. Demographic, Clinical, and Radiologic Predictors of Neurologic Deterioration in Patients with Acute Ischemic Stroke. J. Stroke Cerebrovasc. Dis. 2011, 22, 205–210. [Google Scholar] [CrossRef] [PubMed]
- Beume, L.-A.; Hieber, M.; Kaller, C.P.; Nitschke, K.; Bardutzky, J.; Urbach, H.; Weiller, C.; Rijntjes, M. Large Vessel Occlusion in Acute Stroke. Stroke 2018, 49, 2323–2329. [Google Scholar] [CrossRef] [PubMed]
- Zaidat, O.O.; Yoo, A.J.; Khatri, P.; Tomsick, T.A.; von Kummer, R.; Saver, J.L.; Marks, M.P.; Prabhakaran, S.; Kallmes, D.F.; Fitzsimmons, B.F.M.; et al. Recommendations on angiographic revascularization grading standards for acute ischemic stroke: A consensus statement. Stroke 2013, 44, 2650–2663. [Google Scholar] [CrossRef] [PubMed]
- Yoshimura, S.; Sakai, N.; Yamagami, H.; Uchida, K.; Beppu, M.; Toyoda, K.; Matsumaru, Y.; Matsumoto, Y.; Kimura, K.; Takeuchi, M.; et al. Endovascular Therapy for Acute Stroke with a Large Ischemic Region. N. Engl. J. Med. 2022, 386, 1303–1313. [Google Scholar] [CrossRef]
- A Barber, P.; Demchuk, A.M.; Zhang, J.; Buchan, A.M. Validity and reliability of a quantitative computed tomography score in predicting outcome of hyperacute stroke before thrombolytic therapy. Lancet 2000, 355, 1670–1674. [Google Scholar] [CrossRef] [PubMed]
- Hacke, W.; Kaste, M.; Fieschi, C.; von Kummer, R.; Davalos, A.; Meier, D.; Larrue, V.; Bluhmki, E.; Davis, S.; Donnan, G.; et al. Randomised double-blind placebo-controlled trial of thrombolytic therapy with intravenous alteplase in acute ischaemic stroke (ECASS II). Lancet 1998, 352, 1245–1251. [Google Scholar] [CrossRef]
- Gandhi, C.D.; Al Mufti, F.; Singh, I.P.; Abruzzo, T.; Albani, B.; A Ansari, S.; Arthur, A.S.; Bain, M.; Baxter, B.W.; Bulsara, K.R.; et al. Neuroendovascular management of emergent large vessel occlusion: Update on the technical aspects and standards of practice by the Standards and Guidelines Committee of the Society of NeuroInterventional Surgery. J. NeuroInterv. Surg. 2018, 10, 315–320. [Google Scholar] [CrossRef]
- Powers, W.J.; Rabinstein, A.A.; Ackerson, T.; Adeoye, O.M.; Bambakidis, N.C.; Becker, K.; Biller, J.; Brown, M.; Demaerschalk, B.M.; Hoh, B.; et al. Guidelines for the Early Management of Patients with Acute Ischemic Stroke: 2019 Update to the 2018 Guidelines for the Early Management of Acute Ischemic Stroke: A Guideline for Healthcare Professionals from the American Heart Association/American Stroke Association. Stroke 2019, 50, e344–e418. [Google Scholar] [PubMed]
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2022; Available online: https://www.R-project.org/ (accessed on 19 July 2022).
- RStudio Team. RStudio: Integrated Development for R. RStudio; PBC: Boston, MA, USA, 2022; Available online: http://www.rstudio.com/ (accessed on 19 July 2022).
- Peng, F.; Zheng, W.; Li, F.; Wang, J.; Liu, Z.; Chen, X.; Xiao, L.; Sun, W.; Liu, X. Elevated mean platelet volume is associated with poor outcome after mechanical thrombectomy. J. NeuroInterv. Surg. 2017, 10, 25–28. [Google Scholar] [CrossRef] [PubMed]
- Shi, Z.-S.; Liebeskind, D.S.; Xiang, B.; Ge, S.G.; Feng, L.; Albers, G.W.; Budzik, R.; Devlin, T.; Gupta, R.; Jansen, O.; et al. Predictors of Functional Dependence Despite Successful Revascularization in Large-Vessel Occlusion Strokes. Stroke 2014, 45, 1977–1984. [Google Scholar] [CrossRef] [PubMed]
- Kaplan, Z.S.; Jackson, S.P. The Role of Platelets in Atherothrombosis. Hematology 2011, 2011, 51–61. [Google Scholar] [CrossRef]
- Vasudeva, K.; Munshi, A. Genetics of platelet traits in ischaemic stroke: Focus on mean platelet volume and platelet count. Int. J. Neurosci. 2018, 129, 511–522. [Google Scholar] [CrossRef] [PubMed]
- Karolczak, K.; Soltysik, B.; Kostka, T.; Witas, P.J.; Watala, C. Platelet and Red Blood Cell Counts, as well as the Concentrations of Uric Acid, but Not Homocysteinaemia or Oxidative Stress, Contribute Mostly to Platelet Reactivity in Older Adults. Oxidative Med. Cell. Longev. 2019, 2019, 9467562. [Google Scholar] [CrossRef]
- Viallard, J.-F.; Solanilla, A.; Gauthier, B.; Contin, C.; Déchanet, J.; Grosset, C.; Moreau, J.-F.; Praloran, V.; Nurden, P.; Pellegrin, J.-L.; et al. Increased soluble and platelet-associated CD40 ligand in essential thrombocythemia and reactive thrombocytosis. Blood 2002, 99, 2612–2614. [Google Scholar] [CrossRef]
- Stokes, K.Y.; Granger, D.N. Platelets: A critical link between inflammation and microvascular dysfunction. J. Physiol. 2012, 590, 1023–1103. [Google Scholar] [CrossRef] [PubMed]
- Yilmaz, G.; Arumugam, T.V.; Stokes, K.Y.; Granger, D.N. Role of T lymphocytes and interferon-gamma in ischemic stroke. Circulation 2006, 113, 2105–2112. [Google Scholar] [CrossRef]
- Terao, S.; Yilmaz, G.; Stokes, K.Y.; Russell, J.; Ishikawa, M.; Kawase, T.; Granger, D.N. Blood cell-derived RANTES mediates cerebral microvascular dysfunction, inflammation, and tissue injury after focal ischemia-reperfusion. Stroke 2008, 39, 2560–2570. [Google Scholar] [CrossRef]
- von Hundelshausen, P.; Weber, K.S.; Huo, Y.; Proudfoot, A.E.; Nelson, P.J.; Ley, K.; Weber, C. RANTES deposition by platelets triggers monocyte arrest on inflamed and atherosclerotic endothelium. Circulation 2001, 103, 1772–1777. [Google Scholar] [CrossRef]
- Chen, Z.; He, Y.; Su, Y.; Sun, Y.; Zhang, Y.; Chen, H. Association of inflammatory and platelet volume markers with clinical outcome in patients with anterior circulation ischaemic stroke after endovascular thrombectomy. Neurol. Res. 2021, 43, 503–510. [Google Scholar] [CrossRef] [PubMed]
- Dourado Sotero, F.; Calçada, A.; Aguiar de Sousa, D.; Dias, M.; Fonseca, A.C.; Pinho EMelo, T.; Canhão, P. Mean Platelet Volume is a Prognostic Marker in Acute Ischemic Stroke Patients Treated with Intravenous Thrombolysis. J. Stroke Cereb. Dis. 2021, 30, 105718. [Google Scholar] [CrossRef]
- Staszewski, J.; Pogoda, A.; Data, K.; Walczak, K.; Nowocień, M.; Frankowska, E.; Stępień, A. The mean platelet volume on admission predicts unfavorable stroke outcomes in patients treated with IV thrombolysis. Clin. Interv. Aging 2019, 14, 493–503. [Google Scholar] [CrossRef] [PubMed]
- Pyo, J.-S.; Cho, W.J. Mean Platelet Volume, Platelet Distribution Width, and Platelet Count in Varicocele: A Systematic Review and Meta-Analysis. Cell. Physiol. Biochem. 2016, 38, 2239–2246. [Google Scholar] [CrossRef] [PubMed]
- Gasparyan, A.Y.; Ayvazyan, L.; Mikhailidis, D.P.; Kitas, G.D. Mean platelet volume: A link between thrombosis and inflammation? Curr. Pharm. Des. 2011, 17, 47–58. [Google Scholar] [CrossRef]
- Colkesen, Y.; Muderrisoglu, H. The role of mean platelet volume in predicting thrombotic events. Clin. Chem. Lab. Med. 2012, 50, 631–634. [Google Scholar]
- Xie, D.; Xiang, W.; Weng, Y.; Li, J.; Xu, L.; Zhang, X.; Chen, Z. Platelet volume indices for the prognosis of acute ischemic stroke patients with intravenous thrombolysis. Int. J. Neurosci. 2018, 129, 344–349. [Google Scholar] [CrossRef] [PubMed]
- Wu, X.; Liu, G.; Zhou, W.; Ou, A.; Liu, X.; Wang, Y.; Zhou, S.; Luo, W.; Liu, B. Outcome prediction for patients with anterior circulation acute ischemic stroke following endovascular treatment: A single-center study. Exp. Ther. Med. 2019, 18, 3869–3876. [Google Scholar] [CrossRef]
- Lyden, P.; Raman, R.; Liu, L.; Emr, M.; Warren, M.; Marler, J. National Institutes of Health Stroke Scale Certification Is Reliable Across Multiple Venues. Stroke 2009, 40, 2507–2511. [Google Scholar] [CrossRef]
- Lyden, P. Using the National Institutes of Health Stroke Scale: A Cautionary Tale. Stroke 2017, 48, 513–519. [Google Scholar] [CrossRef] [PubMed]
- Chang, A.; Beheshtian, E.; Llinas, E.J.; Idowu, O.R.; Marsh, E.B. Intravenous Tissue Plasminogen Activator in Combination With Mechanical Thrombectomy: Clot Migration, Intracranial Bleeding, and the Impact of “Drip and Ship” on Effectiveness and Outcomes. Front. Neurol. 2020, 11, 585929. [Google Scholar] [CrossRef] [PubMed]
- Alawieh, A.; Pierce, A.K.; Vargas, J.; Turk, A.S.; Turner, R.D.; Chaudry, M.I.; Spiotta, A.M. The golden 35 min of stroke intervention with ADAPT: Effect of thrombectomy procedural time in acute ischemic stroke on outcome. J. NeuroInterv. Surg. 2017, 10, 213–220. [Google Scholar] [CrossRef] [PubMed]
- Albers, G.W. Late Window Paradox. Stroke 2018, 49, 768–771. [Google Scholar] [CrossRef]
- Koton, S.; Geva, D.; Streifler, J.Y.; Harnof, S.; Pougach, Y.; Azrilin, O.; Hadar, S.; Bornstein, N.M.; Tanne, D. Declining Rate and Severity of Hospitalized Stroke From 2004 to 2013: The National Acute Stroke Israeli Registry. Stroke 2018, 49, 1348–1354. [Google Scholar] [CrossRef] [PubMed]
- Li, J.; Pan, Y.; Xu, J.; Li, S.; Wang, M.; Quan, K.; Meng, X.; Li, H.; Lin, J.; Wang, Y.; et al. Residual Inflammatory Risk Predicts Poor Prognosis in Acute Ischemic Stroke or Transient Ischemic Attack Patients. Stroke 2021, 52, 2827–2836. [Google Scholar] [CrossRef]
- Jin, R.; Liu, L.; Zhang, S.; Nanda, A.; Li, G. Role of Inflammation and Its Mediators in Acute Ischemic Stroke. J. Cardiovasc. Transl. Res. 2013, 6, 834–851. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
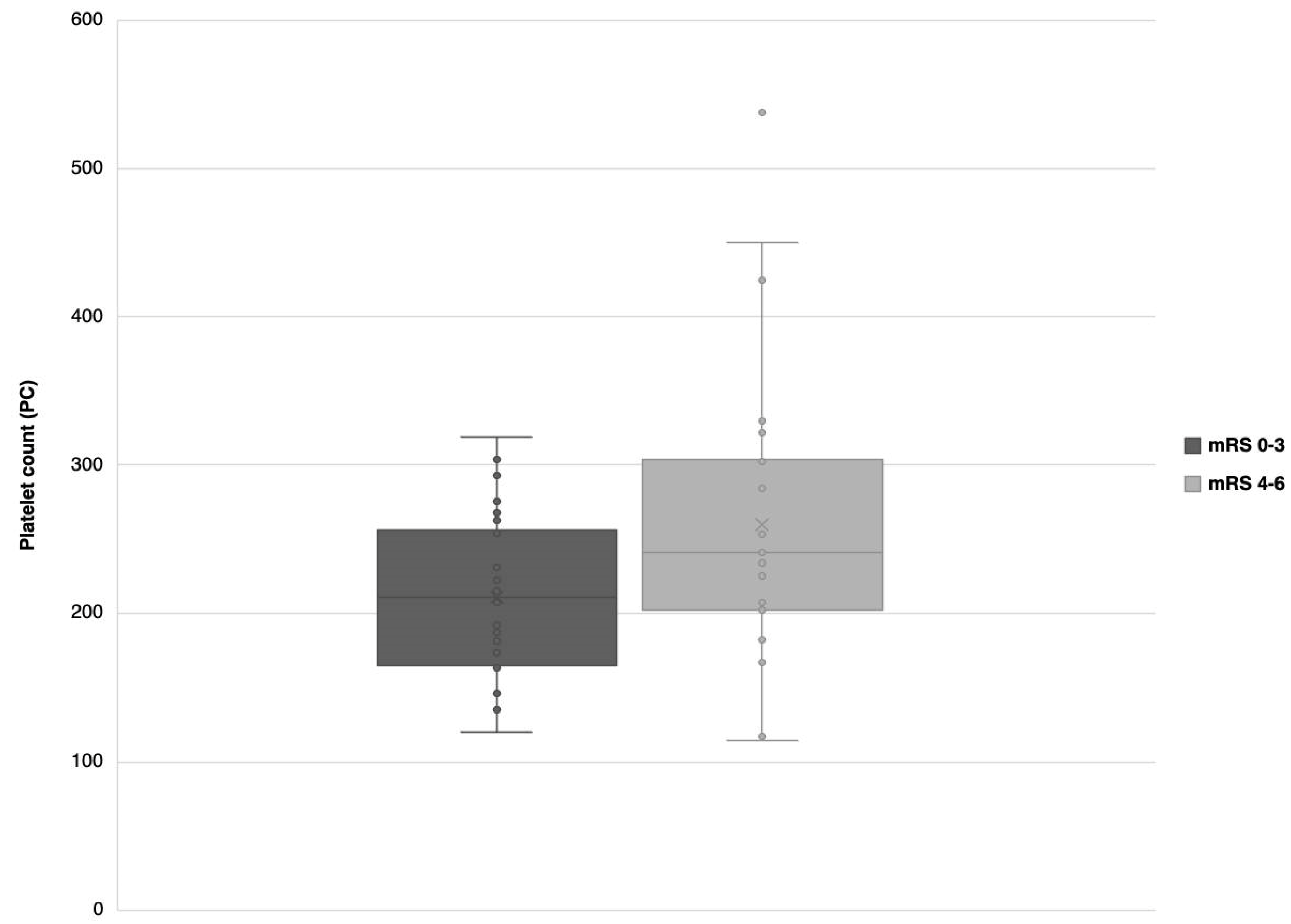
| Total | Favorable Outcome (mRS Score 0–3, n = 26) | Unfavorable Outcome (mRS Score 4–6, n = 27) | p-Value | |
|---|---|---|---|---|
| Age | 67.89 ± 18.1 | 61.04 ± 17.86 | 74.48 ± 16.02 | 0.006 *† |
| Sex | 1.000 | |||
| Female | 30 (56.6%) | 15 (57.7%) | 15 (55.6%) | |
| Male | 23 (43.4%) | 11 (42.3%) | 12 (44.4%) | |
| Race | 0.586 | |||
| White | 27 (50.9%) | 14 (53.8%) | 13 (48.1%) | |
| Black/African American | 25 (47.2%) | 11 (42.3%) | 14 (51.9%) | |
| Other | 1 (1.9%) | 1 (3.8%) | 0 | |
| BMI | 26.42 (9.7) | 26.51 (9.1) | 26.42 (9.4) | 0.965 |
| Smoking status | 0.587 | |||
| No | 27 (50.9%) | 12 (46.2%) | 15 (55.6%) | |
| Yes | 26 (49.1%) | 14 (53.8%) | 12 (44.4%) | |
| Alcohol use | 0.148 † | |||
| No | 36 (67.9%) | 15 (57.7%) | 21 (77.8%) | |
| Yes | 17 (32.1%) | 11 (42.3%) | 6 (22.2%) | |
| Hypertension | 0.526 | |||
| No | 12 (22.6%) | 7 (26.9%) | 5 (18.5%) | |
| Yes | 41 (77.4%) | 19 (73.1%) | 22 (81.5%) | |
| Hyperlipidemia | 0.779 | |||
| No | 33 (62.3%) | 17 (65.4%) | 16 (59.3%) | |
| Yes | 20 (37.7%) | 9 (34.6%) | 11 (40.7%) | |
| Diabetes mellitus | 0.119 † | |||
| No | 39 (73.6%) | 22 (84.6%) | 17 (63%) | |
| Yes | 14 (26.4%) | 4 (15.4%) | 10 (37%) | |
| Heart disease | 0.264 | |||
| No | 32 (60.4%) | 18 (69.2%) | 18 (66.7%) | |
| Yes | 21 (39.6%) | 8 (30.8%) | 13 (48.1%) | |
| Atrial fibrillation | 1.000 | |||
| No | 35 (66%) | 17 (65.4%) | 18 (66.7%) | |
| Yes | 18 (34%) | 9 (34.6%) | 9 (33.3%) | |
| History of malignancy | 0.467 | |||
| No | 45 (84.9%) | 21 (80.8%) | 24 (88.9%) | |
| Yes | 8 (15.1%) | 5 (19.2%) | 3 (11.1%) | |
| Prior cerebrovascular accident | 1.000 | |||
| No | 38 (71.7%) | 19 (73.1%) | 19 (70.4%) | |
| Yes | 15 (28.3%) | 7 (26.9%) | 8 (29.6%) | |
| Heart rate | 85.62 ± 19.8 | 85.35 ± 22.31 | 85.89 ± 17.48 | 0.922 |
| Systolic blood pressure | 143 (29) | 142.5 (24) | 144 (32.5) | 0.810 |
| Diastolic blood pressure | 83 (24) | 83.5 (20.5) | 82 (23) | 0.423 |
| Respiratory rate | 19 (6) | 18 (5.75) | 19 (4.5) | 0.781 |
| Anticoagulant use | 1.000 | |||
| No | 31 (58.5%) | 15 (57.7%) | 16 (59.3%) | |
| Yes | 22 (41.5%) | 11 (42.3%) | 11 (40.7%) | |
| Admission NIHSS | 25 (4) | 24.5 (3) | 25 (5) | 0.687 |
| IV tPA treatment | 0.412 | |||
| No | 30 (56.6%) | 13 (50%) | 17 (63%) | |
| Yes | 23 (43.4%) | 13 (50%) | 10 (37%) | |
| Time from symptom onset to CT in minutes | 150 (187) | 132 (126.8) | 186 (234.5) | 0.838 |
| Glucose | 120 (41) | 118 (33) | 122 (43) | 0.831 |
| Sodium | 139.28 ± 3.98 | 139.35 ± 3.39 | 139.22 ± 4.54 | 0.911 |
| Potassium | 4.08 ± 0.55 | 4 ± 0.52 | 4.16 ± 0.58 | 0.309 |
| Calcium | 8.8 (1.1) | 9.05 (1.3) | 8.7 (1) | 0.076 † |
| BUN:Creatinine ratio | 15.4 (10) | 13.5 (7.8) | 21 (11.8) | 0.020 *† |
| Hemoglobin | 12.6 (2) | 12.85 (1.7) | 12.6 (2.1) | 0.563 |
| Hematocrit | 38.8 (6.3) | 38.85 (4.8) | 38.8 (6.6) | 0.957 |
| Mean corpuscular volume | 90.6 (10.7) | 90.8 (10.2) | 89.8 (8.2) | 0.298 |
| Platelet count | 231 (86) | 211 (81.3) | 241 (98.5) | 0.026 *† |
| Mean platelet volume | 10.59 ± 0.97 | 10.71 ± 1 | 10.48 ± 0.96 | 0.395 |
| Neutrophil count | 6888 (6206) | 6705 (5674) | 6919 (6529) | 0.531 |
| Neutrophil:Platelet ratio | 33.1 (2.8) | 36.35 (21.1) | 30.75 (19.6) | 0.115 † |
| Baseline NCCT ASPECTS | 9 (3) | 9 (2.8) | 9 (2.5) | 0.812 |
| Occlusion site on CT | 0.624 | |||
| Distal intracranial ICA only | 8 (15.1%) | 2 (7.7%) | 6 (22.2%) | |
| M1 only | 33 (61.1%) | 18 (69.2%) | 15 (55.6%) | |
| M1 and M2 | 5 (9.4%) | 2 (7.7%) | 3 (11.1%) | |
| ICA and M1 | 3 (5.7%) | 2 (7.7%) | 1 (3.7%) | |
| M2 only | 4 (7.5%) | 2 (7.7%) | 2 (7.4%) | |
| Occlusion laterality | 0.372 | |||
| Left | 37 (69.8%) | 20 (76.9%) | 17 (63%) | |
| Right | 16 (30.2%) | 6 (23.1%) | 10 (37%) | |
| Hemorrhagic transformation on post-procedural follow up within 48 h | 0.704 | |||
| No | 45 (84.9%) | 23 (88.5%) | 22 (81.5%) | |
| Yes | 8 (15.1%) | 3 (11.5%) | 5 (18.5%) | |
| Time from last known normal to groin puncture in minutes | 208 (141) | 246 (165.5) | 190 (131) | 0.168 † |
| Time from groin puncture to recanalization in minutes | 35 (42) | 31.5 (42) | 42 (42) | 0.444 |
| Number of passes in thrombectomy | 1 (2) | 1 (2) | 1 (1.5) | 0.861 |
| mTICI score category | 0.351 | |||
| 2b | 21 (39.6%) | 12 (46.2%) | 9 (33.3%) | |
| 2c | 8 (15.1%) | 2 (7.7%) | 6 (22.2%) | |
| 3 | 24 (45.3%) | 12 (46.2%) | 12 (44.4%) | |
| Variable | OR (95% CI) | p-Value |
|---|---|---|
| Age | 1.051 (1.015–1.121) | 0.025 ‡ |
| Platelet count | 1.014 (1.003–1.029) | 0.031 ‡ |
| Calcium | 0.343 (0.074–1.005) | 0.115 |
| BUN:Creatinine ratio | 1.077 (0.976–1.206) | 0.157 |
| Neutrophil:platelet ratio | 0.940 (0.976–1.022) | 0.342 |
| Alcohol use (yes) | 0.423 (0.063–2.446) | 0.344 |
| Time from last known normal to groin puncture in minutes | 1.001 (0.998–1.004) | 0.572 |
| Diabetes mellitus (yes) | 1.400 (0.226–9.342) | 0.716 |
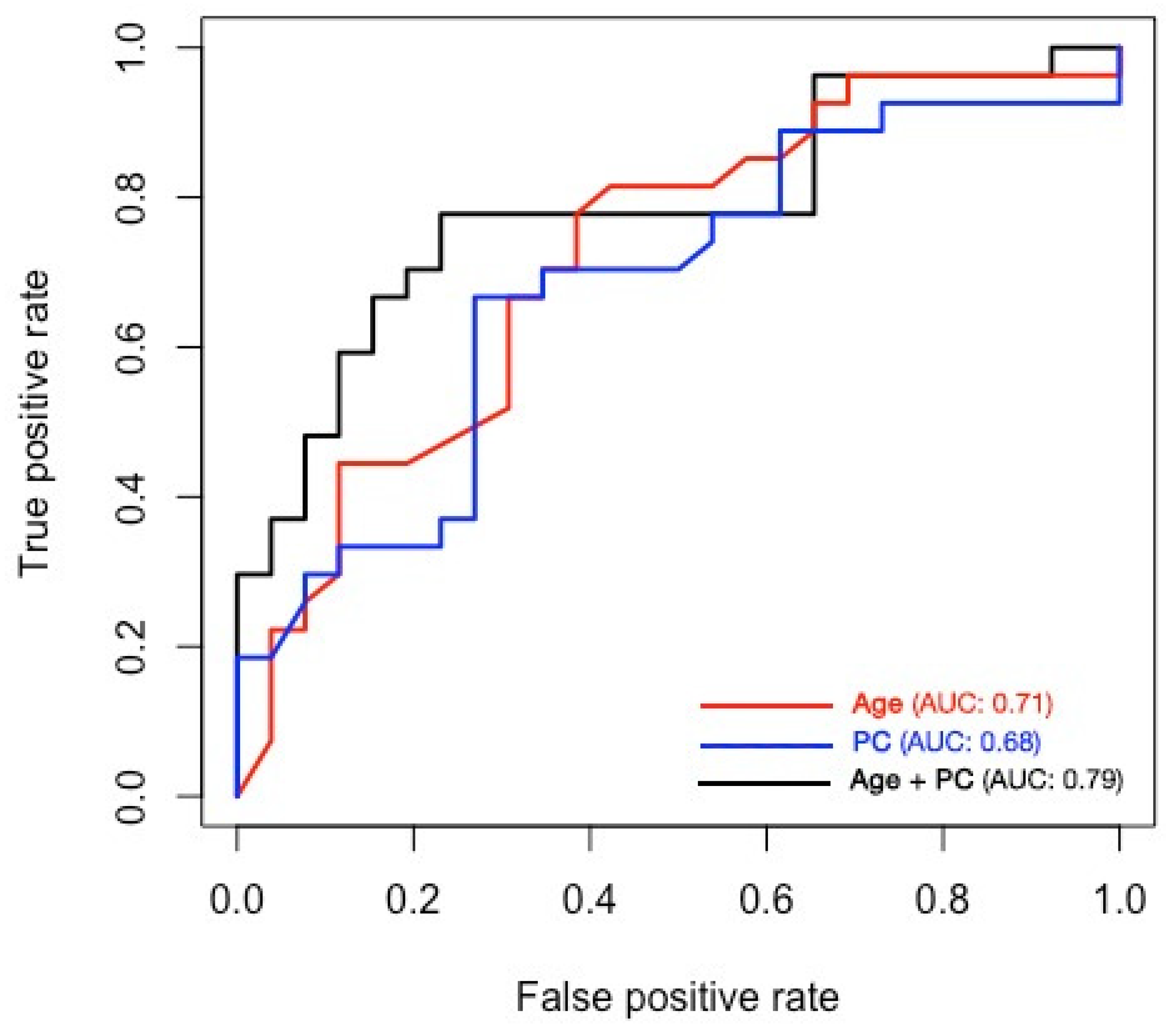
| Variable | B-Coefficient (95% CI) | OR (95% CI) | p-Value |
|---|---|---|---|
| Model 1 | |||
| Intercept | −3.231 [(−6.141)–(−0.832)] | - | - |
| Age | 0.048 (0.014–0.089) | 1.049 (1.014–1.092) | 0.011 |
| Model 2 | |||
| Intercept | −2.169 [(−4.513)–(−0.231)] | - | - |
| Platelet Count | 0.009 (0.002–0.019) | 1.010 (1.002–1.020) | 0.038 |
| Model 3 | |||
| Intercept | −6.484 [(−11.385)–(−2.764)] | - | - |
| Age | 0.055 (0.018–0.102) | 1.057 (1.018–1.107) | 0.009 |
| Platelet Count | 0.012 (0.003–0.024) | 1.012 (1.003–1.024) | 0.029 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ozkara, B.B.; Karabacak, M.; Kotha, A.; Aslan, A.; Hamam, O.; Edpuganti, N.; Hoseinyazdi, M.; Wang, R.; Cristiano, B.C.; Yedavalli, V.S. Prediction of Poor Outcome after Successful Thrombectomy in Patients with Severe Acute Ischemic Stroke: A Pilot Retrospective Study. Neurol. Int. 2023, 15, 225-237. https://doi.org/10.3390/neurolint15010015
Ozkara BB, Karabacak M, Kotha A, Aslan A, Hamam O, Edpuganti N, Hoseinyazdi M, Wang R, Cristiano BC, Yedavalli VS. Prediction of Poor Outcome after Successful Thrombectomy in Patients with Severe Acute Ischemic Stroke: A Pilot Retrospective Study. Neurology International. 2023; 15(1):225-237. https://doi.org/10.3390/neurolint15010015
Chicago/Turabian StyleOzkara, Burak B., Mert Karabacak, Apoorva Kotha, Alperen Aslan, Omar Hamam, Namratha Edpuganti, Meisam Hoseinyazdi, Richard Wang, Brian C. Cristiano, and Vivek S. Yedavalli. 2023. "Prediction of Poor Outcome after Successful Thrombectomy in Patients with Severe Acute Ischemic Stroke: A Pilot Retrospective Study" Neurology International 15, no. 1: 225-237. https://doi.org/10.3390/neurolint15010015