
Exploring the Impact of Cerebral Microbleeds on Stroke Management
 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Search Strategy
2.2. Selection Criteria
2.3. Data Extraction
2.4. Data Analysis
3. Results
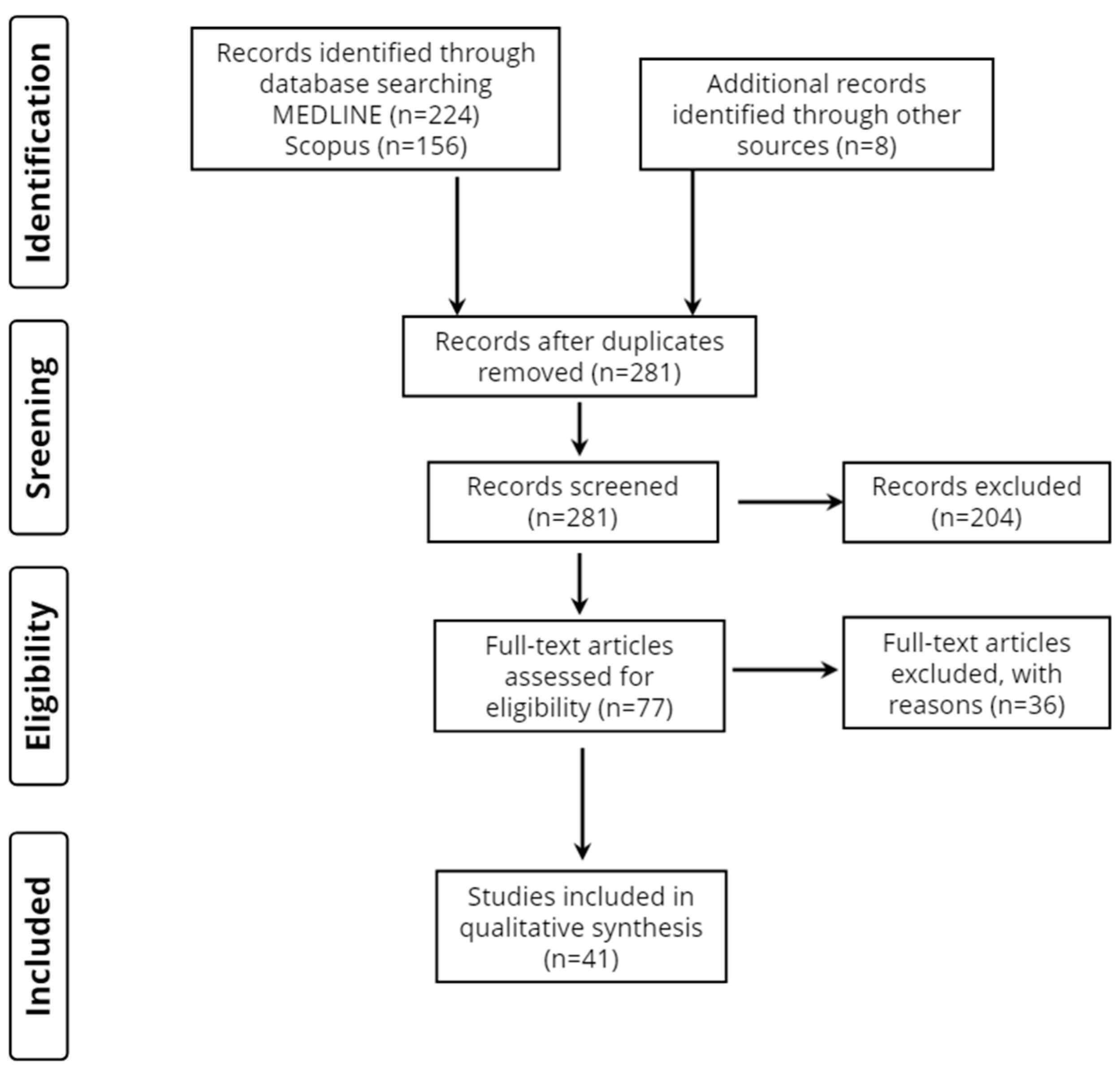
3.1. Database Searches
3.2. Study Characteristics
3.3. Stroke Patient Groups and Demographic Profile
3.4. Reference Groups
3.5. Time of MRI Execution
3.6. Method of Cerebral Microbleed Assessment
3.7. Scales of Stroke Severity and Prognosis/Clinical Outcome
4. Discussion
4.1. Reperfusion Therapy
4.1.1. Intravenous Thrombolysis
4.1.2. Mechanical Thrombectomy
4.1.3. Any Form of Reperfusion Therapy
4.2. Acute Ischemic Stroke/Transient Ischemic Attack
4.2.1. Hemorrhagic Transformation
4.2.2. Short- and Long-Term Outcomes
4.2.3. Chronic Outcomes
4.2.4. Stroke Recurrence
4.2.5. CMBs and Antithrombotic Therapy
4.2.6. Post-Stroke Depression, Cognitive Impairment, and Fatigue
4.3. Hemorrhagic Stroke
4.3.1. Intracerebral Hemorrhage
4.3.2. Subarachnoid Hemorrhage
5. Current Guidelines
6. Study Limitations
7. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
References
- Roth, G.A.; Mensah, G.A.; Johnson, C.O.; Addolorato, G.; Ammirati, E.; Baddour, L.M.; Barengo, N.C.; Beaton, A.Z.; Benjamin, E.J.; Benziger, C.P.; et al. Global Burden of Cardiovascular Diseases and Risk Factors, 1990–2019: Update from the GBD 2019 Study. J. Am. Coll. Cardiol. 2020, 76, 2982–3021. [Google Scholar] [CrossRef]
- Benjamin, E.J.; Virani, S.S.; Callaway, C.W.; Chamberlain, A.M.; Chang, A.R.; Cheng, S.; Chiuve, S.E.; Cushman, M.; Delling, F.N.; Deo, R.; et al. Heart Disease and Stroke Statistics-2018 Update: A Report from the American Heart Association. Circulation 2018, 137, e67–e492. [Google Scholar] [CrossRef] [PubMed]
- Grefkes, C.; Fink, G.R. Recovery from stroke: Current concepts and future perspectives. Neurol. Res. Pract. 2020, 2, 17. [Google Scholar] [CrossRef] [PubMed]
- United Nations DoEaSA Population Division. World Population Prospects, the 2006 Revision, Highlights; United Nations: New York, NY, USA, 2007. [Google Scholar]
- Kokkotis, C.; Giarmatzis, G.; Giannakou, E.; Moustakidis, S.; Tsatalas, T.; Tsiptsios, D.; Vadikolias, K.; Aggelousis, N. An Explainable Machine Learning Pipeline for Stroke Prediction on Imbalanced Data. Diagnostics 2022, 12, 2392. [Google Scholar] [CrossRef]
- Kim, B.; Winstein, C. Can Neurological Biomarkers of Brain Impairment Be Used to Predict Poststroke Motor Recovery? A Systematic Review. Neurorehabil. Neural Repair. 2017, 31, 3–24. [Google Scholar] [CrossRef]
- Stinear, C.M. Prediction of motor recovery after stroke: Advances in biomarkers. Lancet Neurol. 2017, 16, 826–836. [Google Scholar] [CrossRef] [PubMed]
- Quinn, T.J.; Singh, S.; Lees, K.R.; Bath, P.M.; Myint, P.K.; Collaborators, V. Validating and comparing stroke prognosis scales. Neurology 2017, 89, 997–1002. [Google Scholar] [CrossRef]
- Saposnik, G.; Guzik, A.K.; Reeves, M.; Ovbiagele, B.; Johnston, S.C. Stroke Prognostication using Age and NIH Stroke Scale: SPAN-100. Neurology 2013, 80, 21–28. [Google Scholar] [CrossRef] [PubMed]
- Karatzetzou, S.; Tsiptsios, D.; Terzoudi, A.; Aggeloussis, N.; Vadikolias, K. Transcranial magnetic stimulation implementation on stroke prognosis. Neurol. Sci. 2022, 43, 873–888. [Google Scholar] [CrossRef]
- Gkantzios, A.; Tsiptsios, D.; Karatzetzou, S.; Kitmeridou, S.; Karapepera, V.; Giannakou, E.; Vlotinou, P.; Aggelousis, N.; Vadikolias, K. Stroke and Emerging Blood Biomarkers: A Clinical Prospective. Neurol. Int. 2022, 14, 784–803. [Google Scholar] [CrossRef]
- Christidi, F.; Tsiptsios, D.; Fotiadou, A.; Kitmeridou, S.; Karatzetzou, S.; Tsamakis, K.; Sousanidou, A.; Psatha, E.A.; Karavasilis, E.; Seimenis, I.; et al. Diffusion Tensor Imaging as a Prognostic Tool for Recovery in Acute and Hyperacute Stroke. Neurol. Int. 2022, 14, 841–874. [Google Scholar] [CrossRef]
- Greenberg, S.M.; Vernooij, M.W.; Cordonnier, C.; Viswanathan, A.; Salman, R.A.; Warach, S.; Launer, L.J.; van Buchem, M.A.; Breter, M.M. Cerebral microbleeds: A guide to detection and interpretation. Lancet Neurol. 2009, 8, 165–174. [Google Scholar] [CrossRef]
- Scharf, J.; Bräuherr, E.; Forsting, M.; Sartor, K. Significance of hemorrhagic lacunes on MRI in patients with hypertensive cerebrovascular disease and intracerebral haemorrhage. Neuroradiology 1994, 36, 504–508. [Google Scholar] [CrossRef] [PubMed]
- Offenbacher, H.; Fazekas, F.; Schmidt, R.; Koch, M.; Fazekas, G.; Kapeller, P. MR of cerebral abnormalities concomitant with primary intracerebral hematomas. AJNR Am. J. Neuroradiol. 1996, 17, 573–578. [Google Scholar] [PubMed]
- Horita, Y.; Imaizumi, T.; Niwa, J.; Yoshikawa, J.; Miyata, K.; Makabe, T.; Moriyama, R.; Kurokawa, K.; Mikami, M.; Nakamura, M. Analysis of dot-like hemosiderin spots using brain dock system. No Shinkei Geka 2003, 31, 263–267. [Google Scholar] [PubMed]
- Roob, G.; Schmidt, R.; Kapeller, P.; Lechner, A.; Hartung, H.P.; Fazekas, F. MRI evidence of past cerebral microbleeds in a healthy elderly population. Neurology 1999, 52, 991–994. [Google Scholar] [CrossRef]
- Harris, T.B.; Launer, L.J.; Eiriksdottir, G.; Kjartansson, O.; Jonsson, P.V.; Sigurdsson, G.; Thorgeirsson, G.; Aspelund, T.; Garcia, M.E.; Cotch, M.F.; et al. Age, Gene/Environment Susceptibility-Reykjavik Study: Multidisciplinary applied phenomics. Am. J. Epidemiol. 2007, 165, 1076–1087. [Google Scholar] [CrossRef] [PubMed]
- Jeerakathil, T.; Wolf, P.A.; Beiser, A.; Hald, J.K.; Au, R.; Kase, C.S.; Massaro, J.M.; DeCarli, C. Cerebral microbleeds: Prevalence and associations with cardiovascular risk factors in the Framingham Study. Stroke 2004, 35, 1831–1835. [Google Scholar] [CrossRef]
- Cordonnier, C.; Salman, R.A.; Wardlaw, J. Spontaneous brain microbleeds: Systematic review, subgroup analyses and standards for study design and reporting. Brain 2007, 130, 1988–2003. [Google Scholar] [CrossRef] [PubMed]
- Tsushima, Y.; Tanizaki, Y.; Aoki, J.; Endo, K. MR detection of microhemorrhages in neurologically healthy adults. Neuroradiology 2002, 44, 31–36. [Google Scholar] [CrossRef]
- Fazekas, F.; Kleinert, R.; Roob, G.; Kleinert, G.; Kapeller, P.; Schmidt, R.; Hartung, H.P. Histopathologic analysis of foci of signal loss on gradient-echo T2*-weighted MR images in patients with spontaneous intracerebral hemorrhage: Evidence of microangiopathy-related microbleeds. AJNR Am. J. Neuroradiol. 1999, 20, 637–642. [Google Scholar]
- Fisher, M.; French, S.; Ji, P.; Kim, R.C. Cerebral microbleeds in the elderly: A pathological analysis. Stroke 2010, 41, 2782–2785. [Google Scholar] [CrossRef]
- De Reuck, J.; Deramecourt, V.; Cordonnier, C.; Leys, D.; Maurage, C.A.; Pasquier, F. The impact of cerebral amyloid angiopathy on the occurrence of cerebrovascular lesions in demented patients with Alzheimer features: A neuropathological study. Eur. J. Neurol. 2011, 18, 913–918. [Google Scholar] [CrossRef] [PubMed]
- De Reuck, J.; Deramecourt, V.; Cordonnier, C.; Leys, D.; Pasquier, F.; Maurage, C.A. Prevalence of small cerebral bleeds in patients with a neurodegenerative dementia: A neuropathological study. J. Neurol. Sci. 2011, 300, 63–66. [Google Scholar] [CrossRef] [PubMed]
- Kikuta, K.; Takagi, Y.; Nozaki, K.; Okada, T.; Hashimoto, N. Histological analysis of microbleed after surgical resection in a patient with moyamoya disease. Neurol. Med. Chir. 2007, 47, 564–567. [Google Scholar] [CrossRef]
- Pantoni, L. Cerebral small vessel disease: From pathogenesis and clinical characteristics to therapeutic challenges. Lancet Neurol. 2010, 9, 689–701. [Google Scholar] [CrossRef] [PubMed]
- Thompson, C.S.; Hakim, A.M. Living beyond our physiological means: Small vessel disease of the brain is an expression of a systemic failure in arteriolar function: A unifying hypothesis. Stroke 2009, 40, e322–e330. [Google Scholar] [CrossRef] [PubMed]
- Imaizumi, T.; Miyata, K.; Inamura, S.; Kohama, I.; Nyon, K.S.; Nomura, T. The difference in location between traumatic cerebral microbleeds and microangiopathic microbleeds associated with stroke. J. Neuroimaging 2011, 21, 359–364. [Google Scholar] [CrossRef] [PubMed]
- Baumann, C.R.; Schuknecht, B.; Russo, G.L.; Cossu, M.; Citterio, A.; Andermann, F.; Siegel, A.M. Seizure outcome after resection of cavernous malformations is better when surrounding hemosiderin-stained brain also is removed. Epilepsia 2006, 47, 563–566. [Google Scholar] [CrossRef] [PubMed]
- Hammen, T.; Romstöck, J.; Dörfler, A.; Kerling, F.; Buchfelder, M.; Stefan, H. Prediction of postoperative outcome with special respect to removal of hemosiderin fringe: A study in patients with cavernous haemangiomas associated with symptomatic epilepsy. Seizure 2007, 16, 248–253. [Google Scholar] [CrossRef]
- Cianchetti, F.A.; Nishimura, N.; Schaffer, C.B. Cortical microhaemorrhages reduce stimulus-evoked calcium responses in nearby neurons. J. Cereb. Blood Flow Metab. 2009, 29, S217–S218. [Google Scholar]
- Seo, S.W.; Lee, B.H.; Kim, E.J.; Chin, J.; Cho, Y.S.; Yoon, U.; Na, D.L. Clinical significance of microbleeds in subcortical vascular dementia. Stroke 2007, 38, 1949–1951. [Google Scholar] [CrossRef] [PubMed]
- Goos, J.D.; Kester, M.I.; Barkhof, F.; Klein, M.; Blankenstein, M.A.; Scheltens, P.; van der Flier, W.M. Patients with Alzheimer disease with multiple microbleeds: Relation with cerebrospinal fluid biomarkers and cognition. Stroke 2009, 40, 3455–3460. [Google Scholar] [CrossRef] [PubMed]
- Yakushiji, Y.; Nishiyama, M.; Yakushiji, S.; Hirotsu, T.; Uchino, A.; Nakajima, J.; Eriguchi, M.; Nanri, Y.; Hara, M.; Horikawa, E.; et al. Brain microbleeds and global cognitive function in adults without neurological disorder. Stroke 2008, 39, 3323–3328. [Google Scholar] [CrossRef]
- Prins, N.D.; Scheltens, P. White matter hyperintensities, cognitive impairment and dementia: An update. Nat. Rev. Neurol. 2015, 11, 157–165. [Google Scholar] [CrossRef] [PubMed]
- de Laat, K.F.; van den Berg, H.A.; van Norden, A.G.; Gons, R.A.; Rikkert, M.G.; de Leeuw, F.E. Microbleeds are independently related to gait disturbances in elderly individuals with cerebral small vessel disease. Stroke 2011, 42, 494–497. [Google Scholar] [CrossRef]
- Gregoire, S.M.; Chaudhary, U.J.; Brown, M.M.; Yousry, T.A.; Kallis, C.; Jäger, H.R.; Werring, D.J. The Microbleed Anatomical Rating Scale (MARS): Reliability of a tool to map brain microbleeds. Neurology 2009, 73, 1759–1766. [Google Scholar] [CrossRef]
- Cordonnier, C.; Potter, G.M.; Jackson, C.A.; Doubal, F.; Keir, S.; Sudlow, C.L.; Wardlaw, J.M.; Salman, R.A. Improving interrater agreement about brain microbleeds: Development of the Brain Observer MicroBleed Scale (BOMBS). Stroke 2009, 40, 94–99. [Google Scholar] [CrossRef] [PubMed]
- Saba, L.; Raz, E.; Bassareo, P.P.; di Martino, M.; de Cecco, C.N.; Mercuro, G.; Grassi, R.; Suri, J.S.; Piga, M. Is there an association between cerebral microbleeds and leukoaraiosis? J. Stroke Cerebrovasc. Dis. 2015, 24, 284–289. [Google Scholar] [CrossRef] [PubMed]
- Puy, L.; Pasi, M.; Rodrigues, M.; van Veluw, S.J.; Tsivgoulis, G.; Shoamanesh, A.; Cordonnier, C. Cerebral microbleeds: From depiction to interpretation. J. Neurol. Neurosurg. Psychiatry 2021, 92, 598–607. [Google Scholar] [CrossRef]
- Zand, R.; Tsivgoulis, G.; Singh, M.; McCormack, M.; Goyal, N.; Ishfaq, M.F.; Shahripour, R.B.; Nearing, K.; Lucas Elijovich, L.; Alexandrov, A.W.; et al. Cerebral Microbleeds and Risk of Intracerebral Hemorrhage Post Intravenous Thrombolysis. J. Stroke Cerebrovasc. Dis. 2017, 26, 538–544. [Google Scholar] [CrossRef] [PubMed]
- Nagaraja, N.; Tasneem, N.; Shaban, A.; Dandapat, S.; Ahmed, U.; Policeni, B.; Olalde, H.; Hyungsub Shim, H.; Samaniego, A.E.; Pieper, C.; et al. Cerebral Microbleeds are an Independent Predictor of Hemorrhagic Transformation Following Intravenous Alteplase Administration in Acute Ischemic Stroke. J. Stroke Cerebrovasc. Dis. 2018, 27, 1403–1411. [Google Scholar] [CrossRef] [PubMed]
- Schlemm, L.; Braemswig, T.B.; Boutitie, F.; Vynckier, J.; Jensen, M.; Galinovic, I.; Simonsen, C.Z.; Cheng, B.; Cho, T.H.; Fiehler, J.; et al. Cerebral Microbleeds and Treatment Effect of Intravenous Thrombolysis in Acute Stroke: An Analysis of the WAKE-UP Randomized Clinical Trial. Neurology 2022, 98, e302–e314. [Google Scholar] [CrossRef]
- Chacon-Portillo, M.A.; Llinas, R.H.; Marsh, E.B. Cerebral microbleeds shouldn’t dictate treatment of acute stroke: A retrospective cohort study evaluating risk of intracerebral hemorrhage. BMC Neurol. 2018, 18, 33. [Google Scholar] [CrossRef] [PubMed]
- Yan, S.; Jin, X.; Zhang, X.; Zhang, S.; Liebeskind, D.S.; Lou, M. Extensive cerebral microbleeds predict parenchymal haemorrhage and poor outcome after intravenous thrombolysis. J. Neurol. Neurosurg. Psychiatry 2015, 86, 1267–1272. [Google Scholar] [CrossRef]
- Capuana, M.L.; Lorenzano, S.; Caselli, M.C.; Paciaroni, M.; Toni, D. Hemorrhagic risk after intravenous thrombolysis for ischemic stroke in patients with cerebral microbleeds and white matter disease. Neurol. Sci. 2021, 42, 1969–1976. [Google Scholar] [CrossRef] [PubMed]
- Turc, G.; Sallem, A.; Moulin, S.; Tisserand, M.; Machet, A.; Edjlali, M.; Baron, J.C.; Leclerc, X.; Leys, D.; Mas, J.L.; et al. Microbleed Status and 3-Month Outcome After Intravenous Thrombolysis in 717 Patients With Acute Ischemic Stroke. Stroke 2015, 46, 2458–2463. [Google Scholar] [CrossRef]
- Dannenberg, S.; Scheitz, J.F.; Rozanski, M.; Erdur, H.; Brunecker, P.; Werring, D.J.; Fiebach, J.B.; Nolte, C.H. Number of cerebral microbleeds and risk of intracerebral hemorrhage after intravenous thrombolysis. Stroke 2014, 45, 2900–2905. [Google Scholar] [CrossRef]
- Drelon, A.; Kuchcinski, G.; Caparros, F.; Dequatre-Ponchelle, N.; Moulin, S.; Cordonnier, C.; Bordet, R.; Pruvo, J.P.; Leys, D. Remote brain hemorrhage after IV thrombolysis: Role of preexisting lesions. Neurology 2020, 94, e961–e967. [Google Scholar] [CrossRef]
- Prats-Sánchez, L.; Camps-Renom, P.; Sotoca-Fernández, J.; Delgado-Mederos, R.; Martínez-Domeño, A.; Marín, R.; Almendrote, M.; Dorado, L.; Gomis, M.; Codas, J.; et al. Remote Intracerebral Hemorrhage After Intravenous Thrombolysis: Results from a Multicenter Study. Stroke 2016, 47, 2003–2009. [Google Scholar] [CrossRef]
- Shi, Z.S.; Duckwiler, G.R.; Jahan, R.; Tateshima, S.; Gonzalez, N.R.; Szeder, V.; Saver, J.L.; Kim, D.; Ali, L.K.; Starkman, S.; et al. Mechanical thrombectomy for acute ischemic stroke with cerebral microbleeds. J. Neurointerv. Surg. 2016, 8, 563–567. [Google Scholar] [CrossRef]
- Lee, S.J.; Hwang, Y.H.; Hong, J.M.; Choi, J.W.; Park, J.H.; Park, B.; Dong-Hun Kang, D.H.; Kim, Y.W.; Kim, Y.S.; Hong, J.H.; et al. Influence of cerebral microbleeds on mechanical thrombectomy outcomes. Sci. Rep. 2022, 12, 3637. [Google Scholar] [CrossRef] [PubMed]
- Choi, K.H.; Kim, J.H.; Kang, K.W.; Kim, J.T.; Choi, S.M.; Lee, S.H.; Park, M.S.; Kim, B.C.; Kim, M.K.; Cho, K.H. Impact of Microbleeds on Outcome Following Recanalization in Patients With Acute Ischemic Stroke. Stroke 2019, 50, 127–134. [Google Scholar] [CrossRef] [PubMed]
- Gratz, P.P.; El-Koussy, M.; Hsieh, K.; von Arx, S.; Mono, M.L.; Heldner, M.R.; Fischer, U.; Mattle, H.P.; Zubler, C.; Schroth, G.; et al. Preexisting cerebral microbleeds on susceptibility-weighted magnetic resonance imaging and post-thrombolysis bleeding risk in 392 patients. Stroke 2014, 45, 1684–1688. [Google Scholar] [CrossRef]
- Takahashi, W.; Moriya, Y.; Mizuma, A.; Uesugi, T.; Ohnuki, Y.; Takizawa, S. Cerebral microbleeds on T2*-weighted images and hemorrhagic transformation after antithrombotic therapies for ischemic stroke. J. Stroke Cerebrovasc. Dis. 2013, 22, e528-32. [Google Scholar] [CrossRef]
- Zand, R.; Shahjouei, S.; Tsivgoulis, G.; Singh, M.; McCormack, M.; Noorbakhsh-Sabet, N.; Goyal, N.; Alexandrov, A.V. Cerebral Microbleeds are Associated with Higher Mortality Among Ischemic Stroke Patients. J. Stroke Cerebrovasc. Dis. 2018, 27, 3036–3042. [Google Scholar] [CrossRef] [PubMed]
- Liu, C.; Dong, Z.; Xu, L.; Khursheed, A.; Dong, L.; Liu, Z.; Yang, J.; Liu, J. MR image features predicting hemorrhagic transformation in acute cerebral infarction: A multimodal study. Neuroradiology 2015, 57, 1145–1152. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.H.; Hong, K.S.; Lee, J.S.; Kim, Y.J.; Song, T.J.; Kim, Y.D.; Park, M.S.; Kim, E.G.; Cha, J.K.; Sung, S.M.; et al. Prediction of hemorrhagic transformation in patients with mild atrial fibrillation-associated stroke treated with early anticoagulation: Post hoc analysis of the Triple AXEL Trial. Clin. Neurol. Neurosurg. 2018, 174, 156–162. [Google Scholar] [CrossRef] [PubMed]
- Aoki, J.; Iguchi, Y.; Urabe, T.; Yamagami, H.; Todo, K.; Fujimoto, S.; Idomari, K.; Kaneko, N.; Iwanaga, T.; Terasaki, T.; et al. Microbleeds and clinical outcome in acute mild stroke patients treated with antiplatelet therapy: ADS post-hoc analysis. J. Clin. Neurosci. 2021, 89, 216–222. [Google Scholar] [CrossRef] [PubMed]
- Tang, W.K.; Liu, X.X.; Chen, Y.K.; Abrigo, J.; Chu, W.C.; Mok, V.C.; Ungvari, G.S.; Wong, K.S. Cerebral microbleeds and fatigue in stroke. Eur. Neurol. 2014, 71, 213–216. [Google Scholar] [CrossRef] [PubMed]
- Nam, K.W.; Kwon, H.M.; Lee, Y.S.; Kim, J.M.; Ko, S.B. Effects of cerebral small vessel disease on the outcomes in cryptogenic stroke with active cancer. Sci. Rep. 2021, 11, 17510. [Google Scholar] [CrossRef] [PubMed]
- Ryu, W.S.; Jeong, S.W.; Kim, D.E. Total small vessel disease burden and functional outcome in patients with ischemic stroke. PLoS ONE 2020, 15, e0242319. [Google Scholar] [CrossRef] [PubMed]
- Sakuta, K.; Yaguchi, H.; Nakada, R.; Sato, T.; Kitagawa, T.; Takatsu, H.; Miyagawa, S.; Komatsu, T.; Sakai, K.; Mitsumura, H.; et al. Cerebral Microbleeds Load and Long-Term Outcomes in Minor Ischemic Stroke. J. Stroke Cerebrovasc. Dis. 2021, 30, 105973. [Google Scholar] [CrossRef]
- Kim, T.W.; Lee, S.J.; Koo, J.; Choi, H.S.; Park, J.W.; Lee, K.S.; Kim, H.S. Cerebral microbleeds and functional outcomes after ischemic stroke. Can. J. Neurol. Sci. 2014, 41, 577–582. [Google Scholar] [CrossRef]
- Tang, W.K.; Chen, Y.; Liang, H.; Chu, W.C.; Mok, V.C.; Ungvari, G.S.; Wong, K.S. Cerebral microbleeds as a predictor of 1-year outcome of poststroke depression. Stroke 2014, 45, 77–81. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Zhang, J.; Shen, Y.; Xu, X. The safety of antithrombotic therapy in patients with cerebral microbleeds and cardiogenic cerebral embolism due to nonvalvular atrial fibrillation. BMC Cardiovasc. Disord. 2019, 19, 77. [Google Scholar] [CrossRef] [PubMed]
- Hert, L.; Polymeris, A.A.; Schaedelin, S.; Lieb, J.; Seiffge, D.J.; Traenka, C.; Fladt, J.; Thilemann, S.; Gensicke, H.; De Marchis, G.M.; et al. Small vessel disease is associated with an unfavourable outcome in stroke patients on oral anticoagulation. Eur. Stroke J. 2020, 5, 63–72. [Google Scholar] [CrossRef]
- Song, T.J.; Kim, J.; Song, D.; Nam, H.S.; Kim, Y.D.; Lee, H.S.; Heo, J.H. Association of cerebral microbleeds with mortality in stroke patients having atrial fibrillation. Neurology 2014, 83, 1308–1315. [Google Scholar] [CrossRef] [PubMed]
- Lau, K.K.; Wong, Y.K.; Teo, K.C.; Chang, R.S.; Tse, M.Y.; Hoi, C.P.; Chan, C.Y.; Chan, O.L.; Cheung, R.H.; Wong, E.K.; et al. Long-Term Prognostic Implications of Cerebral Microbleeds in Chinese Patients With Ischemic Stroke. J. Am. Heart Assoc. 2017, 6, e007360. [Google Scholar] [CrossRef] [PubMed]
- Imaizumi, T.; Inamura, S.; Kanno, A.; Nomura, T.; Kim, S.N. Association of Ultrasonography and MRI Findings with Stroke Recurrence: Differences Between Patients with Past Histories of Atherothrombotic Versus Lacunar Infarctions. J. Stroke Cerebrovasc. Dis. 2019, 28, 104391. [Google Scholar] [CrossRef]
- Imaizumi, T.; Inamura, S.; Kohama, I.; Yoshifuji, K.; Nomura, T.; Komatsu, K. Antithrombotic drug uses and deep intracerebral hemorrhages in stroke patients with deep cerebral microbleeds. J. Stroke Cerebrovasc. Dis. 2013, 22, 869–875. [Google Scholar] [CrossRef] [PubMed]
- Gregoire, S.M.; Scheffler, G.; Jäger, H.R.; Yousry, T.A.; Brown, M.M.; Kallis, C.; Cipolotti, L.; Werring, D.J. Strictly lobar microbleeds are associated with executive impairment in patients with ischemic stroke or transient ischemic attack. Stroke 2013, 44, 1267–1272. [Google Scholar] [CrossRef] [Green Version]
- Brundel, M.; Kwa, V.I.; Bouvy, W.H.; Algra, A.; Kappelle, L.J.; Biessels, G.J.; MICRO Study Group. Cerebral microbleeds are not associated with long-term cognitive outcome in patients with transient ischemic attack or minor stroke. Cerebrovasc. Dis. 2014, 37, 195–202. [Google Scholar] [CrossRef]
- Lau, K.K.; Li, L.; Schulz, U.; Simoni, M.; Chan, K.H.; Ho, S.L.; Cheung, R.T.; Küker, W.; Mak, H.K.; Rothwell, P.M. Total small vessel disease score and risk of recurrent stroke: Validation in 2 large cohorts. Neurology 2017, 88, 2260–2267. [Google Scholar] [CrossRef]
- Fluri, F.; Jax, F.; Amort, M.; Wetzel, S.G.; Lyrer, P.A.; Katan, M.; Hatz, F.; Engelter, S.T. Significance of microbleeds in patients with transient ischaemic attack. Eur. J. Neurol. 2012, 19, 522–524. [Google Scholar] [CrossRef]
- Shoamanesh, A.; Morotti, A.; Romero, J.M.; Oliveira-Filho, J.; Schlunk, F.; Jessel, M.J.; Ayres, A.M.; Vashkevich, A.; Schwab, K.; Afzal, M.R.; et al. Cerebral Microbleeds and the Effect of Intensive Blood Pressure Reduction on Hematoma Expansion and Functional Outcomes: A Secondary Analysis of the ATACH-2 Randomized Clinical Trial. JAMA Neurol. 2018, 75, 850–859. [Google Scholar] [CrossRef] [PubMed]
- Warrier, A.R.; Bhatia, R.; Garg, A.; Srivastava, M.V.; Dash, D.; Tripathi, M.; Singh, M.B.; Singh, V.; Vishnubhatla, S.; Prasad, K. Do Imaging Markers of Cerebral Small Vessel Disease Predict Hematoma Volume and Outcome in Acute Intracerebral Hemorrhage? Ann. Indian Acad. Neurol. 2021, 24, 204–210. [Google Scholar] [CrossRef] [PubMed]
- Miki, K.; Natori, Y.; Kai, Y.; Yamada, T.; Mori, M.; Noguchi, N.; Koga, H. Absence of Microbleeds Reduces the Risk for Recurrent Intracerebral Hemorrhage. J. Stroke Cerebrovasc. Dis. 2020, 29, 104585. [Google Scholar] [CrossRef] [PubMed]
- Xu, M.; Li, B.; Zhong, D.; Cheng, Y.; Wu, Q.; Zhang, S.; Zhang, S.; Wu, B.; Liu, M. Cerebral Small Vessel Disease Load Predicts Functional Outcome and Stroke Recurrence After Intracerebral Hemorrhage: A Median Follow-Up of 5 Years. Front. Aging Neurosci. 2021, 13, 628271. [Google Scholar] [CrossRef] [PubMed]
- Pasi, M.; Casolla, B.; Kyheng, M.; Boulouis, G.; Kuchcinski, G.; Moulin, S.; Labreuche, J.; Henon, H.; Leys, D.; Cordonnier, C. Long-term functional decline of spontaneous intracerebral haemorrhage survivors. J. Neurol. Neurosurg. Psychiatry 2021, 92, 249–254. [Google Scholar] [CrossRef] [PubMed]
- Jeon, S.B.; Parikh, G.; Choi, H.A.; Badjatia, N.; Lee, K.; Schmidt, J.M.; Lantigua, H.; Connolly, E.S.; Mayer, S.A.; Claassen, J. Cerebral microbleeds in patients with acute subarachnoid hemorrhage. Neurosurgery 2014, 74, 176–181. [Google Scholar] [CrossRef] [PubMed]
- Tsivgoulis, G.; Kargiotis, O.; De Marchis, G.; Kohrmann, M.; Sandset, E.C.; Karapanayiotides, T.; de Sousa, D.A.; Sarraj, A.; Safouris, A.; Psychogios, K.; et al. Off-label use of intravenous thrombolysis for acute ischemic stroke: A critical appraisal of randomized and real-world evidence. Ther. Adv. Neurol. Disord. 2021, 14, 1756286421997368. [Google Scholar] [CrossRef]
- Berge, E.; Whiteley, W.; Audebert, H.; De Marchis, G.M.; Fonseca, A.C.; Padiglioni, C.; de la Ossa, N.P.; Strbian, D.; Tsivgoulis, G.; Turc, G. European Stroke Organisation (ESO) guidelines on intravenous thrombolysis for acute ischaemic stroke. Eur. Stroke J. 2021, 6, I–LXII. [Google Scholar] [CrossRef] [PubMed]
- Klijn, C.J.; Paciaroni, M.; Berge, E.; Korompoki, E.; Kõrv, J.; Lal, A.; Putaala, J.; Werring, D.J. Antithrombotic treatment for secondary prevention of stroke and other thromboembolic events in patients with stroke or transient ischemic attack and non-valvular atrial fibrillation: A European Stroke Organisation guideline. Eur. Stroke J. 2019, 4, 198–223. [Google Scholar] [CrossRef] [PubMed]
- Greenberg, S.M.; Ziai, W.C.; Cordonnier, C.; Dowlatshahi, D.; Francis, B.; Goldstein, J.N.; Hemphill, J.C., III; Johnson, R.; Keigher, K.M.; Mack, W.J.; et al. 2022 Guideline for the Management of Patients With Spontaneous Intracerebral Hemorrhage: A Guideline from the American Heart Association/American Stroke Association. Stroke 2022, 53, e282–e361. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Authors, Year of Publication | Type of Study | Number of Participants/ Mean Age | Demographics: Gender (M/F), Education (Years), BMI | Cerebrovascular Risk Factors (n) | Medication (n) | Previous Stroke (n) | Follow-Up Time | Method of CMB Assessment | Time of MRI Imaging/ Time to Recanalization | Scale of Stroke Severity and Prognosis/ Clinical Outcome | Main Results |
|---|---|---|---|---|---|---|---|---|---|---|---|
| I. Reperfusion Therapy | |||||||||||
| A. Intravenous Thrombolysis | |||||||||||
| Longitudinal | 672/ 62 ± 14 | 350M/322F | Hypertension (518), diabetes mellitus (229), hyperlipidemia (215), atrial fibrillation (67), tobacco use (255) | - | 181 | Until discharge | Number and topographical distribution (strictly lobar or deep/infratentorial) | Pretreatment or within 24 h of treatment | NIHSS at admission, mRS at discharge | CMB presence did not invoke sICH more frequently after IVT, but CMB burden (>10 CMBs) had a statistically significant impact on sICH occurrence. |
| Longitudinal | 366/ 67 ± 15 | 199M/167F | Hypertension (216), diabetes mellitus (83), hyperlipidemia (146), atrial fibrillation (59), smoking (98), alcohol (109), peripheral vascular disease (10), myocardial infarction (15), coronary artery disease (57), congestive heart failure (12), valvular heart disease (8) | Antiplatelet (165), anticoagulant (18) | 67 | Until discharge | Brain Observer Microbleed Scale | On admission | NIHSS at baseline | Presence of CMBs significantly increased the risk for HT in AIS patients receiving IVT, regardless of lobar or deep location. |
| Longitudinal | 459/ 68 (IQR 59–74) | 288M/171F | Hypertension (242), diabetes mellitus (73), hypercholesterolemia (161), atrial fibrillation (50) | Platelet aggregation inhibitors (137), statins (137) | 58 | 90 days | Number and topographical distribution (lobar, deep, or infratentorial) | At baseline/3.1 h (IQR 2.5–3.8) | NIHSS at baseline, mRS at day 90 | The presence of CMBs had no impact on the 90-day functional outcome of AIS receiving IVT and although sICH was more common in patients with CMBs, the relationship failed to reach statistical significance. |
| Longitudinal | 292/ 63 ± 15 | 141M/151F | Hypertension (230), diabetes mellitus (77), tobacco (85), alcohol (70), atrial fibrillation (58), hyperlipidemia (149) | - | 63 | 90 days | Microbleed Anatomical Rating Scale | On admission | NIHSS at admission, at discharge, and day 90, mRS at discharge and day 90 | Presence or location of CMBs did not influence ICH occurrence in AIS patients under thrombolysis, but the number >10 did. |
| Longitudinal | 333 | 223M/110F | Hypertension (227), diabetes mellitus (67), atrial fibrillation (124), hyperlipidemia (159) | Previous use of aspirin or warfarin (45) | - | 3 months | Number and topographical distribution (lobar, deep, or infratentorial) | Pretreatment/234 ± 92 min | NIHSS at baseline, mRS at 3 months | Patients with ≥3 CMBs had a significantly increased risk of PH and poor functional outcomes after IVT. |
| Longitudinal | 434/ 68.3 ± 13.5 | 264M/170F | Hypertension (285), diabetes mellitus (74), atrial fibrillation (70), hypercholesterolemia (138), smoking (146), congestive heart failure (10) | Antiplatelet (137), oral anticoagulation (16) | 60 | 3 months | Number, size, and topographical distribution (lobar, deep, or infratentorial) | Pretreatment or within 24h of treatment/180 (IQR 135.0–222.25) min | NIHSS at baseline, mRS at 3 months | AIS patients receiving IVT were more likely to develop ICH, especially severe if they had CMBs, but no correlation between CMBs and poor functional outcomes or mortality was found. |
| Longitudinal | 717/ 74 (IQR 60–83) | 351M/366F | Hypertension (452), diabetes mellitus (113), atrial fibrillation (166), smoking (128) | - | 71 | 3 months | Number and topographical distribution (lobar, deep, or infratentorial) | Pretreatment/ 152 (IQR 120–195) min | NIHSS at baseline, mRS at 3 months | CMB burden on pre-IVT MRI was not associated with sICH and with poor functional outcomes, after adjusting for age, hypertension, and atrial fibrillation, even when CMB location and presumed underlying vasculopathy was considered. |
| Longitudinal | 326/ 76 (IQR 68–84) | 159M/167F | Hypertension (277), diabetes mellitus (74), atrial fibrillation (128), hyperlipidemia (171) | Statin (73), Antiplatelet (149), oral anticoagulation (5) | 80 | 3 months | Number | Pretreatment/within 4.5 h of symptom onset | NIHSS at baseline, mRS at 3 months | With a growing number of CMBs, the rate of ICH and PH was increasing. |
| Longitudinal | 944 | - | - | - | - | 3 months | Number and topographical distribution (lobar or deep) | At admission/with a time window of 4.5 h | NIHSS at baseline, mRS at 3 months | Even though patients with r-ICH had more often strictly lobar CMBs and more in number; r-ICHs were better predicted by clinical variables. |
| Longitudinal | 992/ 74.0 ± 12.6 | 525M/467F | Hypertension (718), diabetes mellitus (239), atrial fibrillation (239) | Antiplatelets (372), anticoagulation (67), statins (352) | 142 | 3 months | Number and topographical distribution (lobar, deep, or mixed) | Within the first 14 days of the onset of stroke/within the first 4.5 h of symptom onset | NIHSS at baseline, mRS at 3 months | Patients with strictly lobar CMBs or RSI had a significantly increased risk for rPH. |
| B. Mechanical Thrombectomy | |||||||||||
| Longitudinal | 206/ 66.8 ± 17.6 | 87M/119F | Hypertension (135), diabetes mellitus (43), atrial fibrillation (82), dyslipidemia (64), coronary artery disease (43) | Aspirin (55), clopidogrel (13), warfarin (30), statins (59), antihypertensive drugs (103) | 34 | Until discharge | Microbleed Anatomic Rating Scale | Pretreatment | NIHSS at baseline, mRS at discharge | The number and topographical distribution of CMBs did not affect HT, functional outcomes, or in-hospital mortality of patients undergoing MT. |
| Longitudinal | 577/ 67 ± 13 | 322M/255F | Hypertension (359), diabetes mellitus (159), atrial fibrillation (285), dyslipidemia (174), smoking (135) | - | 102 | 3 months | Number | Pretreatment/within 24 h of symptom onset | NIHSS at baseline, mRS at 3 months | An increasing number of CMBs increases the rate of hemorrhagic complications and poor functional outcomes, partially mediated by WMH, HT, and lower successful reperfusion rates, listed in order of total CMB influence proportion. |
| C. Any Reperfusion Therapy | |||||||||||
| Longitudinal | 1532 | 855M/677F | Hypertension (1034), diabetes mellitus (438), atrial fibrillation (629), smoking (508) | - | 208 | 3 months | Number and topographical distribution (lobar or deep/infratentorial) | On admission/Within 6 h of symptom onset | NIHSS at baseline, mRS at 3 months | Although there was no correlation between CMB presence and poor functional outcomes, in patients achieving recanalization, high CMB burden and lobar distribution were significantly associated with unfavorable functional outcomes. Furthermore, hemorrhagic complications were more common in participants with CMBs. |
| Longitudinal | 392 (174 IVT, 150 ET, and 68 both)/68.1 ± 13.7 | 223M/169F | Hypertension (249), diabetes mellitus (66), atrial fibrillation (142), smoking (167), hypercholesterolemia (213) | Antithrombotic therapy (173) | 41 | 3 months | Microbleed Anatomic Rating Scale | Pretreatment | NIHSS at baseline, mRS at 3 months | The burden and location of CMBs were not associated with ICH occurrence, functional outcome, or survival rate. A higher CMB burden slightly increased the risk of ICH outside of the infarct. |
| II. Ischemic Stroke | |||||||||||
| A. Acute Ischemic Stroke | |||||||||||
| Longitudinal | 187/ 74 ± 11 | 112M/75F | - | Antiplatelet (51), anticoagulant (136) | - | 2 days | Number | At admission | NIHSS at baseline | CMBs did not suggest the occurrence of HT in patients who were on antithrombotic therapy. |
| Longitudinal | 772/ 61.9 ± 14.2 | 398M/374F | Hypertension (601), diabetes mellitus (258), hyperlipidemia (250), smoking (284), atrial fibrillation (195) | NM | 195 | Until discharge | Number | NM | NIHSS at baseline | The presence of CMBs was not associated with in-hospital mortality of AIS patients, but if their number was ≥4, CMBs significantly increased the possibility of death. |
| Longitudinal | 87/ 67.29 ± 12.45 | 49M/38F | NM | NM | NM | 2 weeks | Presence | Within 24 h after symptom onset | - | Among the MR imaging features, CMBs, relative apparent diffusion, and venous anomalies were independent risk factors for HT of acute cerebral infarction. |
| Longitudinal | 183/ 70.4 ± 10.4 | 107M/76F | Hypertension (34), hyperlipidemia (34), diabetes mellitus (117) | Warfarin (88), rivaroxaban (95), single antiplatelet (40), dual antiplatelet (5) | - | 4 weeks | Presence | NM | - | Microbleeds did not correlate with hemorrhagic transformation in anticoagulated mild atrial fibrillation-related stroke patients. |
| Longitudinal | 1102/ 68 (IQR 60–77) | 737M/365F | Hypertension (859), diabetes mellitus (258) | Cilostazol and aspirin therapy (439), aspirin (104) | 123 | 3 months | Number | On admission | NIHSS at baseline, mRS at 3 months | The number of CMBs did not affect either the short-term or the 3 months clinical outcome. Furthermore, dual antiplatelet therapy with cilostazol and aspirin did not influence safety outcomes compared to aspirin alone, regardless of CMB burden. |
| Longitudinal | 199 | 140M/59F, education 5.6 ± 5.2 (PSF) vs. 5.5 ± 4.5 (non-PSF) | Hypertension (155) | - | 58 | 3 months | Topographical distribution (lobar, deep, or posterior fossa groups) | Within 7 days of admission | NIHSS within 2 days of admission, MMSE, GDS, BI, and the Chinese version of the Fatigue Severity Scale at 3 months | The existence of deep CMBs was significantly associated with post-stroke fatigue. |
| Cross-sectional | 179/ 67 ± 10 | 108M/79F | Hypertension (77), diabetes mellitus (55), dyslipidemia (76), smoking (61) | - | - | 3 months | Number (absence, single, multiple) | Within 24 h of admission | NIHSS at baseline, mRS at 3 months | CMB number was not associated with either END or with a 3-month unfavorable outcomes. |
| Longitudinal | 477/ 66 ± 14 | 294M/183F | Hypertension (359), diabetes mellitus (182), hyperlipidemia (143), smoking (221), coronary artery disease (75) | - | 99 | 3 months | Presence | NM | NIHSS at baseline, mRS at 3 months | Total SVD scores were significantly associated with functional outcomes at three months following ischemic stroke and CMB presence was independently associated with higher 3-month mRS scores. |
| Longitudinal | 240 (NIHSS score < 4 on admission)/ 66 (IQR 57–76) | 187M/53F, BMI 23.7 (IQR 21.7–26.0) | Hypertension (165), diabetes mellitus (74), dyslipidemia (126), smoking (61), ischemic heart disease (20), peripheral arterial disease (6) | Single antiplatelet agent (150), dual antiplatelet agent (90), edaravone combined (94) | 43 | 90 days | Number | On admission | NIHSS at baseline, mRS at day 90 | In minor non-cardiogenic stroke patients treated with antiplatelet therapy, a higher CMB number led more frequently to poorer functional outcomes. |
| Longitudinal | 225/ 67.6 ± 13.7 | 123M/102F | Hypertension (141), diabetes mellitus (64), dyslipidemia (87), ischemic heart disease (19), atrial fibrillation (53) | Antiplatelet agents (48), anticoagulant agents (4), statin (12) | 44 | 6 months | Presence and topographical distribution (lobar, deep, or infratentorial) | Within 24 h of admission | NIHSS and mRS at admission, 24 h after admission, discharge, and 6 months after admission | The presence of CMBs was associated with poor functional outcomes both at discharge and at 6 months, but after adjustment for confounding factors, only infratentorial CMBs were correlated with poor outcomes. |
| Longitudinal | 135/ 65.7 ± 11.0 | 66M/69F, education 5.9 ± 4.6 | Hypertension (95), diabetes mellitus (58), hyperlipidemia (67), smoking (84) | - | 26 | 15 months | Topographical distribution (lobar, deep, and posterior fossa groups) | Within 7 days of admission | NIHSS and mRS within 2 days of admission, MMSE and LSNS at 3 months, GDS at 3 and 15 months | Stroke patients with lobar CMBs had a lower remission rate of post-stroke depression. |
| Longitudinal | 232 | 155M/77F | Hypertension (153), diabetes mellitus (85), smoking (85), atrial fibrillation (232) | Warfarin (44), rivaroxaban (9), dabigatran (88), aspirin (55), clopidogrel (36) | - | Mean of 22.4 ± 13.4 months | Number and topographical distribution (in a brain lobe of the cortex or a subcortical region, in a deep brain tissue region, or both) | At admission | NIHSS at admission | No difference in the occurrence of cerebral hemorrhage events or all-cause death was established between patients taking antithrombotic therapy for cardiogenic cerebral embolism with or without CMBs. |
| Longitudinal | 320/ 78.2 ± 9.2 | 170M/150F | Hypertension (241), diabetes mellitus (62), smoking (81), hypercholesterolemia (122), alcohol (78) | DOAC (216), DOAC/antiplatelet (18), VKA (61), VKA/antiplatelet (15), antiplatelet (5) | - | Median of 754 (IQR 708–828) days | Number and topographical distribution (superficial or deep) | NM | NIHSS at baseline | Stroke patients with CMBs on anticoagulants for atrial fibrillation were at a higher risk of the composite endpoint (ischemic stroke, intracranial hemorrhage, death), but not for disability. |
| Longitudinal | 504/ 70 ± 11 | 288M/216F | Hypertension (392), diabetes mellitus (124), smoking (65), congestive heart failure (79), metabolic syndrome (180), coronary artery disease (109), peripheral artery disease (27), aortic atheroma (31) | Antiplatelet (224), anticoagulant (122), lipid-lowering agents (102) | 93 | Median of 2.5 years | Number, topographical distribution (strictly lobar, strictly nonlobar, and mixed) | Within 3 days of admission | NIHSS at admission | CMB presence raised the mortality rate, the greatest CMB burden predicted independently all-cause and ischemic stroke mortality and CMBs with strictly lobar distribution increased the hazard of hemorrhagic stroke mortality. |
| Longitudinal | 1003/ 69 ± 12 | 601M/402F | Hypertension (657), diabetes mellitus (284), hyperlipidemia (256), smoking (297), atrial fibrillation (130) | Antiplatelet (218), warfarin (20), NOAC (3) | - | Mean of 37 ± 20 months | Microbleed Anatomical Rating Scale | Median of 4 days | mRS at discharge | Having ≥5 microbleeds independently predicted ICH occurrence, but not AIS recurrence. Furthermore, increasing the microbleed burden raised the risk of both ICH and all-cause mortality in antiplatelet users. |
| Longitudinal | 362 ATI and 309 LI | ATI: 211M/151F, LI: 169M/140F | ATI: hypertension (236), diabetes mellitus (101), smoking (109), LI: hypertension (193), diabetes mellitus (95), smoking (83) | ATI: statin (75), anti-platelet drugs (278), warfarin or DOAC (17), LI: statin (70), anti-platelet drugs (287), warfarin or DOAC (18) | - | Mean of 41 ± 52 months for ATI, mean of 51 ± 33 months for LI | Microbleed Anatomical Rating Scale | On enrollment | - | Stroke recurrence rates were significantly elevated in ATI patients with lobar or mixed (deep and lobar) CMBs and LI patients with either deep or mixed CMBs. |
| Longitudinal | 807/ 69.8 ± 12.0 | 456M/351F | - | Cilostazol (142), aspirin (203), clopidogrel sulfate (92), ticlopidine hydrochloride (34), warfarin (not stated) | - | 0.5 to 71 months (mean of 31.6 ± 22.2 months) | Microbleed Anatomical Rating Scale | On admission | - | ICH occurrence was not more frequent in stroke patients with CMBs on antithrombotic therapy. |
| B. Acute Ischemic Stroke or Transient Ischemic Attack | |||||||||||
| Longitudinal | 320 | 190M/130F, median education 10 years | Hypertension (238), diabetes mellitus (63) | Antithrombotic (125) | 91 | 3 months | Microbleed Anatomic Rating Scale | NM | Stroop test, Word Fluency, Trail Making Test Part B, Weigl Color Form Sorting Task, and Modified Card Sorting Test | Of the cognitive domains studied, only executive impairment was related to CMBs. |
| Longitudinal | 397/ 65 ± 12 | 137M/260F | Hypertension (185), diabetes mellitus (40), hypercholesterolemia (144), smoking (86), history of a cardiovascular event (41) | Antiplatelet (70), anticoagulant (5) | - | 4 years | Microbleed Anatomical Rating Scale | Within 3 months after the ischemic event | mRS at baseline, TICS, or IQCODE after a mean interval of 3.8 years | Microbleeds, unlike the other markers of SVD, did not influence the long-term cognitive performance of stroke patients. |
| Longitudinal | 2002 | 1121M/881F | Hypertension (1203), diabetes mellitus (411), hyperlipidemia (630), smoking (812), atrial fibrillation (288) | - | 341 | 120 months | Microbleed Anatomical Rating Scale | NM | mRS at 1 month after recurrence | Increasing total SVD scores were correlated with a higher risk of recurrent ischemic stroke and ICH. In particular, microbleeds, especially when there were ≥5, raised the risk of recurrent stroke and especially of ICH. |
| C. Transient Ischemic Attack | |||||||||||
| Longitudinal | 176 | 107M/69F | Hypertension (126), diabetes mellitus (31), hypercholesterolemia (71), smoking (39), atrial fibrillation (123), coronary heart disease (35), family history of stroke (40) | - | - | 3 months | Number and topographical distribution | Within 24 h of the event | - | AIS after TIA was more frequent in patients with CMBs. |
| III. Hemorrhagic Stroke | |||||||||||
| A. Intracerebral Hemorrhage | |||||||||||
| Longitudinal | 167/ 61.9 ± 13.2 | 98M/69F | Hypertension (125), smoking (71), cocaine use (10), congestive heart failure (7), atrial fibrillation (2), diabetes (31), ischemic heart failure 94), hyperlipidemia (45), peripheral vascular disease (3) | - | 26 | 3 months | Number and topographical distribution (strictly lobar, strictly deep, or mixed) | NM | GCS and NIHSS at baseline, mRS at 3 months | There was no association between CMBs and death or disability at 3 months or hematoma expansion within 24 h of symptom onset, regardless of intensive vs standard blood pressure lowering, even taking into consideration the number and location of CMBs. |
| Longitudinal | 60/ 54.08 ± 11.57 | 47M/13F | Hypertension (60), smoking (22), alcohol use (10), diabetes mellitus (6), tobacco use (18), dyslipidemia (12), coronary artery disease (12) | - | 0 | 3 months | Number | Within 5 days | mRS at 3 months | The presence of >3 CMBs increased the risk of poor outcomes but it did not influence hematoma volume or expansion. |
| Longitudinal | 317 | 158M/159F | Hypertension (279), hyperlipidemia (71), smoking (105), alcohol use (97), diabetes mellitus (48), coronary disease (33) | Antiplatelet (70), anticoagulant (27) | 49 | Mean period of 1663days | Number | NM | mRS at discharge | Patients without microbleeds had a reduced risk of ICH recurrence. |
| Longitudinal | 153/ 61.0 ± 12.2 | 111M/42F | Hypertension (123), hyperlipidemia (8), smoking (46), alcohol use (28), diabetes mellitus (16), cardiac disease (10) | - | 15 | Median of 4.9 years | Number and topographical distribution | At baseline | GCS at admission, mRS at the end of the follow-up | Patients with ≥10 CMBs had an increased risk of poor functional outcomes and death and when CMBs were lobar, patients experienced more frequent stroke recurrence. Notably, of all SVD markers, only CMBs ≥10 remained significantly related to mortality after adjusting for age, sex, and hypertension. |
| Longitudinal | 174/ 64.6 ± 13.5 | 108M/66F | Hypertension (107), dyslipidemia (56), smoking (38), alcohol use (57), diabetes mellitus (26), atrial fibrillation (25) | Antiplatelet (38), anticoagulants (24), antihypertensive (99), Statins (39) | 14 | Median of 9 years | Brain ObserverMicrobleed Scale | NM | NIHSS at baseline, mRS at 6 months, and 1, 2, 3, 4.5, 6, 8, and 10 years after the index ICH | Across the SVD markers, only strictly lobar or mixed CMBs independently predicted functional decline in patients with a favorable functional outcomes 6 months after ICH. |
| B. Subarachnoid Hemorrhage | |||||||||||
| Longitudinal | 39/ 56 (IQR 44-65) | 11M/28F | Hypertension (10), smoking (15), alcohol use (3), diabetes mellitus (4) | Antithrombotic agents (6) | 1 | 3 months | Microbleed Anatomic Rating Scale | Within 7 days | mRS and TICS at discharge and 3 months | Although patients with CMBs had higher mRS scores at discharge and 3 months, the relationship did not reach statistical significance. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sousanidou, A.; Tsiptsios, D.; Christidi, F.; Karatzetzou, S.; Kokkotis, C.; Gkantzios, A.; Bairaktaris, C.; Karapepera, V.; Bebeletsi, P.; Karagiannakidou, I.; et al. Exploring the Impact of Cerebral Microbleeds on Stroke Management. Neurol. Int. 2023, 15, 188-224. https://doi.org/10.3390/neurolint15010014
Sousanidou A, Tsiptsios D, Christidi F, Karatzetzou S, Kokkotis C, Gkantzios A, Bairaktaris C, Karapepera V, Bebeletsi P, Karagiannakidou I, et al. Exploring the Impact of Cerebral Microbleeds on Stroke Management. Neurology International. 2023; 15(1):188-224. https://doi.org/10.3390/neurolint15010014
Chicago/Turabian StyleSousanidou, Anastasia, Dimitrios Tsiptsios, Foteini Christidi, Stella Karatzetzou, Christos Kokkotis, Aimilios Gkantzios, Chrisostomos Bairaktaris, Vaia Karapepera, Paschalina Bebeletsi, Ioanna Karagiannakidou, and et al. 2023. "Exploring the Impact of Cerebral Microbleeds on Stroke Management" Neurology International 15, no. 1: 188-224. https://doi.org/10.3390/neurolint15010014