
Stroke Aetiology and Collateral Status in Acute Ischemic Stroke Patients Receiving Reperfusion Therapy—A Meta-Analysis

 , and
, and 
Abstract
:1. Introduction
2. Materials and Methods
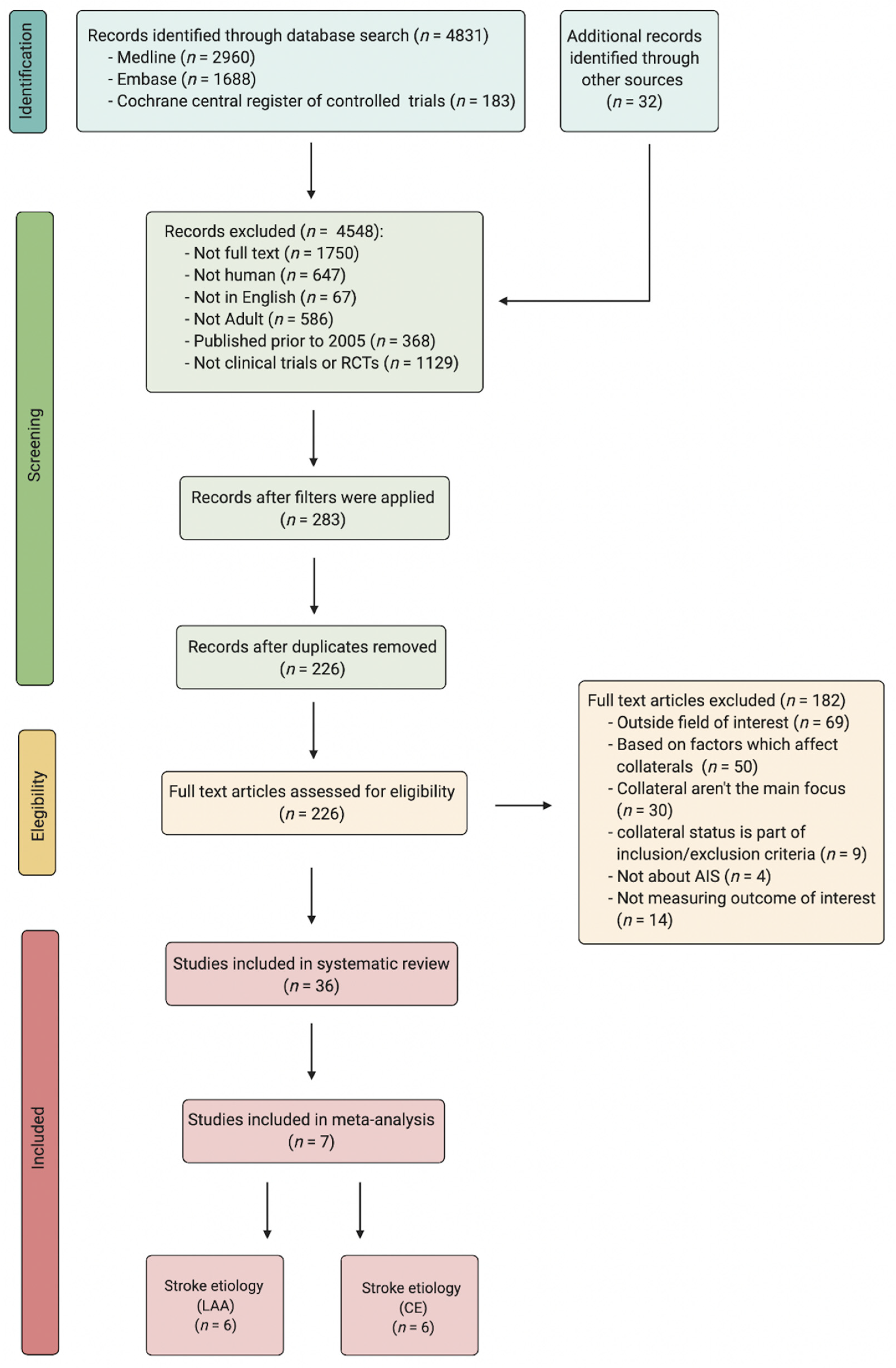
2.1. Literature Search: Identification and Selection of Studies
2.2. Inclusion and Exclusion Criteria
2.3. Data Extraction
2.4. Quality Assessment of Included Studies
2.5. Statistical Analysis
3. Results
3.1. Description of Included Studies
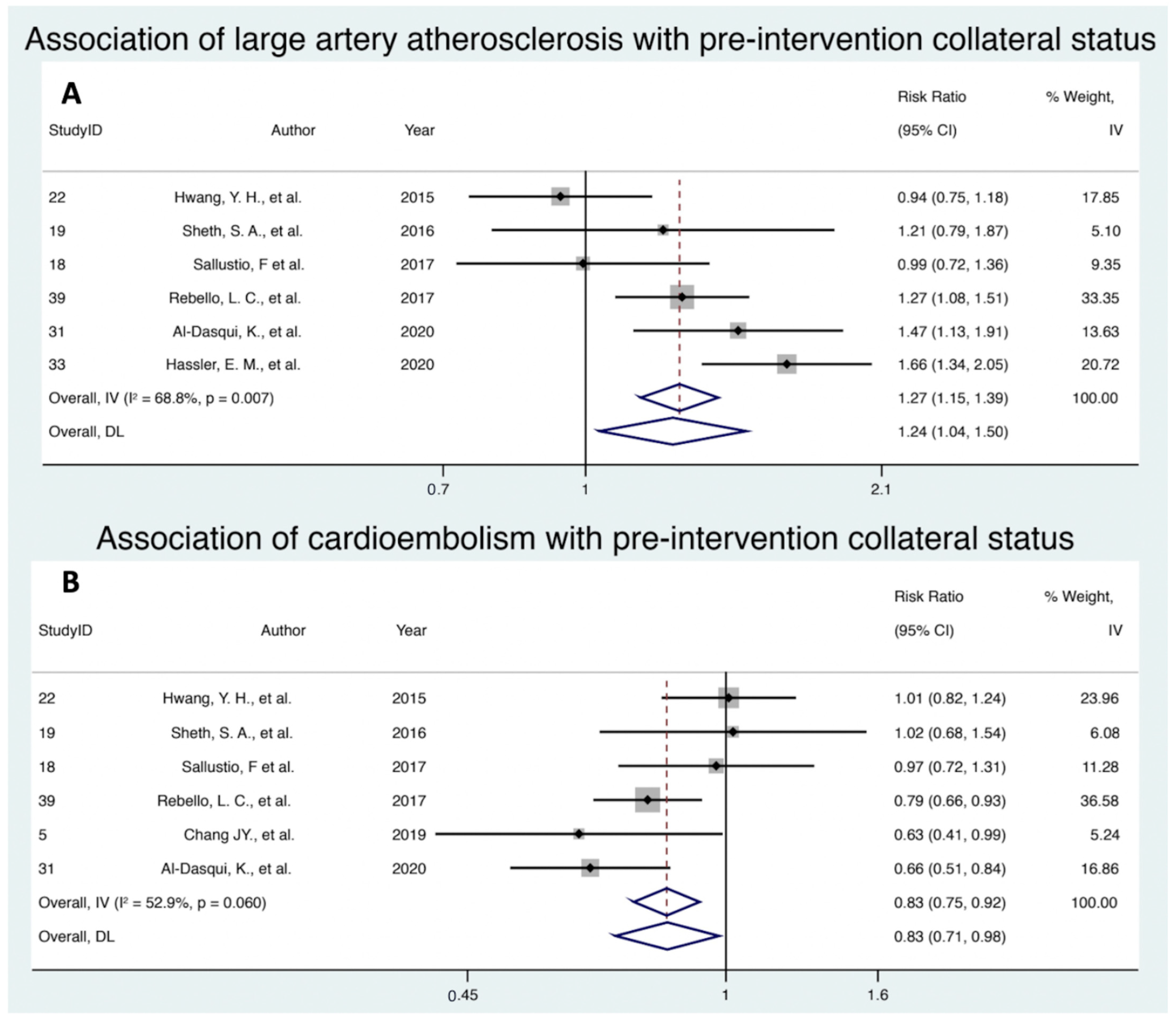
3.2. Association of Large Artery Atherosclerosis with Pre-Intervention Collateral Status
3.3. Association of Cardioembolism with Pre-Intervention Collateral Status
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ravindran, A.V.; Killingsworth, M.C.; Bhaskar, S. Cerebral collaterals in acute ischaemia: Implications for acute ischaemic stroke patients receiving reperfusion therapy. Eur. J. Neurosci. 2021, 53, 1238–1261. [Google Scholar] [CrossRef] [PubMed]
- Bang, O.Y.; Saver, J.L.; Alger, J.R.; Starkman, S.; Ovbiagele, B.; Liebeskind, D.S.; Investigators, U.C. Determinants of the distribution and severity of hypoperfusion in patients with ischemic stroke. Neurology 2008, 71, 1804–1811. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Al-Dasuqi, K.; Payabvash, S.; Torres-Flores, G.A.; Strander, S.M.; Nguyen, C.K.; Peshwe, K.U.; Kodali, S.; Silverman, A.; Malhotra, A.; Johnson, M.H.; et al. Effects of Collateral Status on Infarct Distribution Following Endovascular Therapy in Large Vessel Occlusion Stroke. Stroke 2020, 51, e193–e202. [Google Scholar] [CrossRef] [PubMed]
- Rebello, L.C.; Bouslama, M.; Haussen, D.C.; Grossberg, J.A.; Dehkharghani, S.; Anderson, A.; Belagaje, S.R.; Bianchi, N.A.; Grigoryan, M.; Frankel, M.R.; et al. Stroke etiology and collaterals: Atheroembolic strokes have greater collateral recruitment than cardioembolic strokes. Eur. J. Neurol. 2017, 24, 762–767. [Google Scholar] [CrossRef] [PubMed]
- Helisch, A.; Schaper, W. Arteriogenesis: The development and growth of collateral arteries. Microcirculation 2003, 10, 83–97. [Google Scholar] [CrossRef]
- Marnane, M.; Duggan, C.A.; Sheehan, O.C.; Merwick, A.; Hannon, N.; Curtin, D.; Harris, D.; Williams, E.B.; Horgan, G.; Kyne, L.; et al. Stroke subtype classification to mechanism-specific and undetermined categories by TOAST, A-S-C-O, and causative classification system: Direct comparison in the North Dublin population stroke study. Stroke 2010, 41, 1579–1586. [Google Scholar] [CrossRef] [Green Version]
- Stroup, D.F.; Berlin, J.A.; Morton, S.C.; Olkin, I.; Williamson, G.D.; Rennie, D.; Moher, D.; Becker, B.J.; Sipe, T.A.; Thacker, S.B. Meta-analysis of observational studies in epidemiology: A proposal for reporting. Meta-analysis Of Observational Studies in Epidemiology (MOOSE) group. JAMA 2000, 283, 2008–2012. [Google Scholar] [CrossRef]
- Chang, J.Y.; Jeon, S.B.; Jung, C.; Gwak, D.S.; Han, M.K. Postreperfusion Blood Pressure Variability After Endovascular Thrombectomy Affects Outcomes in Acute Ischemic Stroke Patients With Poor Collateral Circulation. Front. Neurol. 2019, 10, 346. [Google Scholar] [CrossRef]
- Sallustio, F.; Motta, C.; Pizzuto, S.; Diomedi, M.; Giordano, A.; D’Agostino, V.C.; Sama, D.; Mangiafico, S.; Saia, V.; Legramante, J.M.; et al. CT angiography-based collateral flow and time to reperfusion are strong predictors of outcome in endovascular treatment of patients with stroke. J. Neurointerv. Surg. 2017, 9, 940–943. [Google Scholar] [CrossRef]
- Sheth, S.A.; Sanossian, N.; Hao, Q.; Starkman, S.; Ali, L.K.; Kim, D.; Gonzalez, N.R.; Tateshima, S.; Jahan, R.; Duckwiler, G.R.; et al. Collateral flow as causative of good outcomes in endovascular stroke therapy. J. Neurointerv. Surg. 2016, 8, 2–7. [Google Scholar] [CrossRef] [Green Version]
- Hwang, Y.H.; Kang, D.H.; Kim, Y.W.; Kim, Y.S.; Park, S.P.; Liebeskind, D.S. Impact of time-to-reperfusion on outcome in patients with poor collaterals. Am. J. Neuroradiol. 2015, 36, 495–500. [Google Scholar] [CrossRef] [Green Version]
- Hassler, E.; Kneihsl, M.; Deutschmann, H.; Hinteregger, N.; Magyar, M.; Wiesspeiner, U.; Haidegger, M.; Fandler-Hofler, S.; Eppinger, S.; Niederkorn, K.; et al. Relationship between stroke etiology and collateral status in anterior circulation large vessel occlusion. J. Neurol. 2020, 267, 3362–3370. [Google Scholar] [CrossRef] [PubMed]
- Shen, Y.-W.; Zhang, X.-M.; Lv, M.; Chen, L.; Qin, T.-J.; Wang, F.; Yang, J.; Liu, P.-J.; Yang, J. Utility of gonadotropin-releasing hormone agonists for prevention of chemotherapy-induced ovarian damage in premenopausal women with breast cancer: A systematic review and meta-analysis. Onco Targets Ther. 2015, 8, 3349–3359. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Katyal, A.; Calic, Z.; Killingsworth, M.; Bhaskar, S.M.M. Diagnostic and prognostic utility of computed tomography perfusion imaging in posterior circulation acute ischemic stroke: A systematic review and meta-analysis. Eur. J. Neurol. 2021, 28, 2657–2668. [Google Scholar] [CrossRef]
- Saunders, R.; Struys, M.; Pollock, R.F.; Mestek, M.; Lightdale, J.R. Patient safety during procedural sedation using capnography monitoring: A systematic review and meta-analysis. BMJ Open 2017, 7, e013402. [Google Scholar] [CrossRef] [PubMed]
- Shi, C.; Killingsworth, M.C.; Bhaskar, S.M.M. Prognostic capacity of hyperdense middle cerebral artery sign in anterior circulation acute ischaemic stroke patients receiving reperfusion therapy: A systematic review and meta-analysis. Acta Neurol. Belg. 2021, 498. [Google Scholar] [CrossRef] [PubMed]
- Wan, X.; Wang, W.; Liu, J.; Tong, T. Estimating the sample mean and standard deviation from the sample size, median, range and/or interquartile range. BMC Med. Res. Methodol. 2014, 14, 135. [Google Scholar] [CrossRef] [Green Version]
- Douglas, D.A.A.; Birks, J.; Borenstein, M.; Campbell, M.; Deeks, J.; Egger, M.; Higgins, J.; Lau, J.; O’Rourke, K.; Rücker, G.; et al. Cochrane Handbook for Systematic Reviews of Interventions Version 6.2; Jonathan, J.P.H.J.D., Altman, D.G., Eds.; John Wiley & Sons: Chichester, UK, 2021. [Google Scholar]
- Bhaskar, S.; Bivard, A.; Stanwell, P.; Parsons, M.; Attia, J.R.; Nilsson, M.; Levi, C. Baseline collateral status and infarct topography in post-ischaemic perilesional hyperperfusion: An arterial spin labelling study. J. Cereb. Blood Flow Metab. 2017, 37, 1148–1162. [Google Scholar] [CrossRef] [Green Version]
- Leng, X.; Fang, H.; Leung, T.W.; Mao, C.; Xu, Y.; Miao, Z.; Liu, L.; Wong, K.S.; Liebeskind, D.S. Impact of Collateral Status on Successful Revascularization in Endovascular Treatment: A Systematic Review and Meta-Analysis. Cerebrovasc. Dis. 2016, 41, 27–34. [Google Scholar] [CrossRef]
- Qian, J.; Fan, L.; Zhang, W.; Wang, J.; Qiu, J.; Wang, Y. A meta-analysis of collateral status and outcomes of mechanical thrombectomy. Acta Neurol. Scand. 2020, 142, 191–199. [Google Scholar] [CrossRef]
- Zotter, M.; Piechowiak, E.I.; Balasubramaniam, R.; Von Martial, R.; Genceviciute, K.; Blanquet, M.; Slavova, N.; Sarikaya, H.; Arnold, M.; Gralla, J.; et al. Endovascular therapy in patients with large vessel occlusion due to cardioembolism versus large-artery atherosclerosis. Ther. Adv. Neurol. Disord. 2021, 14. [Google Scholar] [CrossRef]
- Sun, B.; Shi, Z.; Pu, J.; Yang, S.; Wang, H.; Yang, D.; Hao, Y.; Lin, M.; Ke, W.; Liu, W.; et al. Effects of mechanical thrombectomy for acute stroke patients with etiology of large artery atherosclerosis. J. Neurol. Sci. 2019, 396, 178–183. [Google Scholar] [CrossRef] [PubMed]
- Giray, S.; Ozdemir, O.; Baş, D.F.; İnanç, Y.; Arlıer, Z.; Kocaturk, O. Does stroke etiology play a role in predicting outcome of acute stroke patients who underwent endovascular treatment with stent retrievers? J. Neurol. Sci. 2017, 372, 104–109. [Google Scholar] [CrossRef] [PubMed]
- Guglielmi, V.; LeCouffe, N.E.; Zinkstok, S.M.; Compagne, K.C.J.; Eker, R.; Treurniet, K.M.; Tolhuisen, M.L.; van der Worp, H.B.; Jansen, I.G.H.; van Oostenbrugge, R.J.; et al. Collateral Circulation and Outcome in Atherosclerotic Versus Cardioembolic Cerebral Large Vessel Occlusion. Stroke 2019, 50, 3360–3368. [Google Scholar] [CrossRef] [PubMed]
- Schulz, U.G.; Rothwell, P.M. Differences in vascular risk factors between etiological subtypes of ischemic stroke: Importance of population-based studies. Stroke 2003, 34, 2050–2059. [Google Scholar] [CrossRef] [Green Version]
- Rha, J.H.; Saver, J.L. The impact of recanalization on ischemic stroke outcome: A meta-analysis. Stroke 2007, 38, 967–973. [Google Scholar] [CrossRef]
- Savarese, G.; Lund, L.H. Global Public Health Burden of Heart Failure. Card. Fail. Rev. 2017, 3, 7–11. [Google Scholar] [CrossRef]
- Guo, H.; Xu, W.; Zhang, X.; Zhang, S.; Dai, Z.; Li, S.; Xie, Y.; Li, Y.; Xue, J.; Liu, X. A Nomogram to Predict Symptomatic Intracranial Hemorrhage After Intravenous Thrombolysis in Chinese Patients. Neuropsychiatr. Dis. Treat. 2021, 17, 2183–2190. [Google Scholar] [CrossRef]
- Hu, Y.; Ji, C. Efficacy and safety of thrombolysis for acute ischemic stroke with atrial fibrillation: A meta-analysis. BMC Neurol. 2021, 21, 66. [Google Scholar] [CrossRef]
- Bhatt, D.L.; Steg, P.G.; Ohman, E.M.; Hirsch, A.T.; Ikeda, Y.; Mas, J.L.; Goto, S.; Liau, C.S.; Richard, A.J.; Röther, J.; et al. International prevalence, recognition, and treatment of cardiovascular risk factors in outpatients with atherothrombosis. JAMA 2006, 295, 180–189. [Google Scholar] [CrossRef] [Green Version]
- Hoshino, T.; Sissani, L.; Labreuche, J.; Ducrocq, G.; Lavallée, P.C.; Meseguer, E.; Guidoux, C.; Cabrejo, L.; Hobeanu, C.; Gongora-Rivera, F.; et al. Prevalence of Systemic Atherosclerosis Burdens and Overlapping Stroke Etiologies and Their Associations With Long-term Vascular Prognosis in Stroke With Intracranial Atherosclerotic Disease. JAMA Neurol. 2018, 75, 203–211. [Google Scholar] [CrossRef] [PubMed]
- Semerano, A.; Laredo, C.; Zhao, Y.; Rudilosso, S.; Renu, A.; Llull, L.; Amaro, S.; Obach, V.; Planas, A.M.; Urra, X.; et al. Leukocytes, Collateral Circulation, and Reperfusion in Ischemic Stroke Patients Treated With Mechanical Thrombectomy. Stroke 2019, 50, 3456–3464. [Google Scholar] [CrossRef] [PubMed]
- Katyal, A.; Bhaskar, S. CTP-guided reperfusion therapy in acute ischemic stroke: A meta-analysis. Acta Neurol. Scand. 2021, 143, 355–366. [Google Scholar] [CrossRef] [PubMed]
- Alexandre, A.M.; Pedicelli, A.; Valente, I.; Scarcia, L.; Giubbolini, F.; D’Argento, F.; Lozupone, E.; Distefano, M.; Pilato, F.; Colosimo, C. May endovascular thrombectomy without CT perfusion improve clinical outcome? Clin. Neurol. Neurosurg. 2020, 198, 106207. [Google Scholar] [CrossRef]
- Bhaskar, S.; Bivard, A.; Parsons, M.; Nilsson, M.; Attia, J.R.; Stanwell, P.; Levi, C. Delay of late-venous phase cortical vein filling in acute ischemic stroke patients: Associations with collateral status. J. Cereb. Blood Flow Metab. 2017, 37, 671–682. [Google Scholar] [CrossRef] [Green Version]
- Shaban, S.; Huasen, B.; Haridas, A.; Killingsworth, M.; Worthington, J.; Jabbour, P.; Bhaskar, S.M.M. Digital subtraction angiography in cerebrovascular disease: Current practice and perspectives on diagnosis, acute treatment and prognosis. Acta Neurol. Belg. 2021. [Google Scholar] [CrossRef]
- Anadani, M.; Finitsis, S.; Clarençon, F.; Richard, S.; Marnat, G.; Bourcier, R.; Sibon, I.; Dargazanli, C.; Arquizan, C.; Blanc, R.; et al. Collateral status reperfusion and outcomes after endovascular therapy: Insight from the Endovascular Treatment in Ischemic Stroke (ETIS) Registry. J. Neurointerv. Surg. 2021. [Google Scholar] [CrossRef]
- Smith, A.G.; Rowland Hill, C. Imaging assessment of acute ischaemic stroke: A review of radiological methods. Br. J. Radiol. 2018, 91, 20170573. [Google Scholar] [CrossRef]
- Verdolotti, T.; Pilato, F.; Cottonaro, S.; Monelli, E.; Giordano, C.; Guadalupi, P.; Benenati, M.; Ramaglia, A.; Costantini, A.M.; Alexandre, A.; et al. ColorViz, a New and Rapid Tool for Assessing Collateral Circulation during Stroke. Brain Sci. 2020, 10, 882. [Google Scholar] [CrossRef]
- Buschmann, I.; Schaper, W. The pathophysiology of the collateral circulation (arteriogenesis). J. Pathol. 2000, 190, 338–342. [Google Scholar] [CrossRef]
- Sharma, D.; Spring, K.J.; Bhaskar, S.M.M. Neutrophil-lymphocyte ratio in acute ischemic stroke: Immunopathology, management, and prognosis. Acta Neurol. Scand. 2021, 144, 486–499. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.Y.; Park, J.; Chang, J.Y.; Kim, S.H.; Lee, J.E. Inflammation after Ischemic Stroke: The Role of Leukocytes and Glial Cells. Exp. Neurobiol. 2016, 25, 241–251. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rastogi, A.; Weissert, R.; Bhaskar, S.M.M. Leukoaraiosis severity and post-reperfusion outcomes in acute ischaemic stroke: A meta-analysis. Acta Neurol. Scand. 2021. [Google Scholar] [CrossRef] [PubMed]
- Rastogi, A.; Weissert, R.; Bhaskar, S.M.M. Emerging role of white matter lesions in cerebrovascular disease. Eur. J. Neurosci. 2021, 54, 5531–5559. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Study ID i | Author | Year | Region | Study Type | Cohort | Reperfusion | Pre-Intervention Characteristics | Collateral Grading | Stroke Aetiology ii | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Reperfusion Modality | tPA n (%) | EVT n (%) | EVT ± tPA n (%) | Age, Years Mean ± SD | Sex, Male n (%) | Good Collaterals, n (%) | Imaging Modality | Collateral Grading Method | Definition of Good Collaterals iii | Definition of Poor Collaterals iii | LAA, n (%) | CE, n (%) | ||||||||||
| O | GC | PC | O | GC | BC | |||||||||||||||||
| 5 | Chang et al. [8] | 2019 | USA | Retrospective | 90 | EVT | NA | 90 (100) | NA | 72.3 ± 11.8 | 54 (60) | 41 (45.6) | mCTA | Menon et al. | 4 (when compared with the asymptomatic contralateral hemisphere, there is a delay of one phase in filling in of peripheral vessels, but prominence and extent is the same); 5 (there is no delay and normal or increased prominence of pial vessels/normal extent within the ischemic territory in the symptomatic hemisphere). | 0 (when compared with the asymptomatic contralateral hemisphere, there are no vessels visible in any phase within the ischemic vascular territory); 1 (there are just a few vessels visible in any phase within the occluded vascular territory); 2 (there is a delay of two phases in filling in of peripheral vessels and decreased prominence and extent or a one-phase delay and some ischemic regions with no vessels); 3 (there is a delay of two phases in filling of peripheral vessels or there is a one-phase delay and significantly reduced number of vessels in the ischemic territory). | NA | NA | NA | 54 (60) | 20 (22.2) | 34 (37.8) |
| 18 | Sallustio et al. [9] | 2017 | Italy | Retrospective | 135 | EVT ± tPA | 79 (58.5) | 135 (100) | 79 (58.5) | 68.3 ± 14.3 | 67 (49.6) | 75 (55.6) | Cerebral angiography | Christoforidis et al. | 1 (collaterals reconstituted the distal portion of the occluded vessel segment); 2 (collaterals reconstituted vessels in the proximal portion of the segment adjacent to the occluded vessel); 3 (collaterals reconstituted vessels in the distal portion of the segment adjacent to the occluded vessel); 4 (collaterals reconstituted vessels two segments distal to the occluded vessel); 5 (little or no significant reconstitution of the territory of the occluded vessel). | 47 (34.8) | 26 (19.3) | 21 (15.6) | 64 (47.4) | 35 (26) | 29 (21.5) | |
| “Good” | “Poor” | |||||||||||||||||||||
| 19 | Sheth et al. [10] | 2016 | USA | Retrospective | 117 | EVT ± tPA | 59 (50.4) | 96 (82.1) | NA iv | 66.7 ± 16.7 | 45 (38.5) | 51 (43.6) | Cerebral angiography | ASITN/SIR | 3 (collaterals with slow but complete angiographic blood flow of the ischemic bed by the late venous phase); 4 (complete and rapid collateral blood flow to the vascular bed in the entire ischemic territory by retrograde perfusion). | 0 (no collaterals visible to the ischemic site); 1 (slow collaterals to the periphery of the ischemic site with the persistence of some of the defect); 2 (rapid collaterals to the periphery of ischemic site with the persistence of some of the defect and only a portion of the ischemic territory). | 32 (27.3) | 16 (13.6) | 16 (13.7) | 59 (50.4) | 26 (22.2) | 33 (28.2) |
| 22 v | Hwang et al. [11] | 2015 | Korea | Retrospective | 207 | EVT ± tPA vi | 103 (49.8) | NA vii | NA vii | 67.1 ± 11.1 | 125 (60.4) | 131 (63.3) | Cerebral angiography | ASITN/SIR | 2 (Rapid collateral vessels to the periphery of ischemic site with the persistence of some of the defect and to only a portion of the ischemic territory); 3 (Collateral vessels with slow but complete angiographic blood flow of the ischemic bed by the late venous phase); 4 (Complete and rapid collateral blood flow to the vascular bed in the entire ischemic territory by retrograde perfusion). | 0 (No collateral vessels visible to the ischemic site); 1 (Slow collateral vessels to the periphery of the ischemic site with the persistence of some of the defect). | 66 (31.9) | 40 (19.3) | 26 (12.6) | 107 (51.7) | 68 (32.8) | 39 (18.8) |
| 31 viii | Al-Dasqui et al. [3] | 2020 | USA | Retrospective | 283 | EVT ± tPA | 130 (45.9) | 270 (95.4) | NA ix | 69.2 ± 15.2 | 159 (56.2) | 129 (45.6) | sCTA | Miteff | Good (major MCA branches reconstituted distal to the occlusion) | moderate (some MCA branches shown in the Sylvian fissure); poor (only distal superficial MCA branches reconstituted). | 52 (18.4) | 32 (11.3) | 20 (7.1) | 178 (62.9) | 68 (24) | 110 (38.9) |
| 33 | Hassler et al. [12] | 2020 | Austria | Retrospective | 281 | EVT ± tPA | 166 (59.1) | 281 (100) | 166 (59.1) | 68.6 ± 12.1 | 144 (51.2) | 143 (50.9) | sCTA, MRI | Tan | 2 (collateral supply filling >50% but <100%); 3 (100% collateral supply of the occluded MCA territory). | 0 (absent collateral supply of the affected MCA territory); 1 (collateral supply filling ≤ 50%). | 46 (16.4) | 35 (12.5) | 11 (3.9) | NA | NA | NA |
| 39 | Rebello et al. [4] | 2017 | USA | Retrospective | 122 | EVT ± tPA | 54 (44.3) | 122 (100) | 54 (44.3) | 69.7 ± 12.9 | 64 (52.5) | 94 (77) | sCTA | Souza et al. | 2 (diminished collaterals in <50% of the affected territory); 3 (collaterals equal to the contralateral side); 4 (increased collaterals). | 0 (absent collaterals in >50% of the affected territory); 1 (diminished collaterals in >50% of the affected territory). | 34 (27.9) | 31 (25.4) | 3 (2.5) | 88 (72.1) | 63 (51.6) | 25 (20.5) |
| Clinical Variable | Number of Patients with Data Available | Characteristics n (%) |
|---|---|---|
| Risk Factors | ||
| Atrial fibrillation | 952 | 466 (48.9) |
| Diabetes mellitus | 952 | 194 (20.3) |
| Hyperlipidaemia | 817 | 232 (28.4) |
| Hypertension | 952 | 654 (67.7) |
| Coronary artery disease | 297 | 44 (14.8) |
| Past stroke | 414 | 80 (19.3) |
| Smoker | 952 | 198 (20.8) |
| Aetiology | ||
| Larger artery atherosclerosis | 1145 | 277 (24.2) |
| Cardio embolism | 954 | 550 (57.7) |
| Undetermined | 490 | 87 (17.8) |
| Small vessel disease | 117 | 1 (0.8) |
| Outcome | Effect Measure | Treatment Subgroup | Summary Effects | Heterogeneity ¶ | Heterogeneity Variance Estimates | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| REDL | FEMH | FEIV | |||||||||||
| RR (95% CI) | Tests of Overall Effect | RR (95% CI) | Tests of Overall Effect | RR (95% CI) | Tests of Overall Effect | Cochran’s Q | H | I2 * | p-Value | τ2 † | |||
| LAA | RR | EVT ± tPA | 1.24 (1.04–1.50) | p = 0.02 z = 2.33 | 1.23 (1.11–1.36) | p < 0.0001 z = 3.87 | 1.27 (1.15–1.39) | p < 0.0001 z = 4.75 | 16.05 | 1.79 | 68.8 | 0.007 | 0.0346 |
| CE | RR | EVT ± tPA | 0.83 (0.71–0.98) | p = 0.027 z = −2.213 | 0.84 (0.75–0.94) | p = 0.002 z = −3.149 | 0.83 (0.75–0.92) | p < 0.0001 z = −3.526 | 10.61 | 1.46 | 52.9 | 0.060 | 0.0198 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sinha, A.; Stanwell, P.; Beran, R.G.; Calic, Z.; Killingsworth, M.C.; Bhaskar, S.M.M. Stroke Aetiology and Collateral Status in Acute Ischemic Stroke Patients Receiving Reperfusion Therapy—A Meta-Analysis. Neurol. Int. 2021, 13, 608-621. https://doi.org/10.3390/neurolint13040060
Sinha A, Stanwell P, Beran RG, Calic Z, Killingsworth MC, Bhaskar SMM. Stroke Aetiology and Collateral Status in Acute Ischemic Stroke Patients Receiving Reperfusion Therapy—A Meta-Analysis. Neurology International. 2021; 13(4):608-621. https://doi.org/10.3390/neurolint13040060
Chicago/Turabian StyleSinha, Akansha, Peter Stanwell, Roy G. Beran, Zeljka Calic, Murray C. Killingsworth, and Sonu M. M. Bhaskar. 2021. "Stroke Aetiology and Collateral Status in Acute Ischemic Stroke Patients Receiving Reperfusion Therapy—A Meta-Analysis" Neurology International 13, no. 4: 608-621. https://doi.org/10.3390/neurolint13040060