
Spectrum of Neuroimaging Findings in Post-COVID-19 Vaccination: A Case Series and Review of Literature

 , , and
, , and
Abstract
:1. Introduction
2. Methods
3. Case Summary
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Creech, C.B.; Walker, S.C.; Samuels, R.J. SARS-CoV-2 vaccines. JAMA 2021, 325, 1318–1320. [Google Scholar] [CrossRef]
- Coronavirus (COVID-19) Vaccinations. Available online: https://ourworldindata.org/covid-vaccinations (accessed on 25 September 2021).
- Meo, S.A.; Bukhari, I.A.; Akram, J.; Meo, A.S.; Klonoff, D.C. COVID-19 vaccines: Comparison of biological, pharmacological characteristics and adverse effects of Pfizer/BioNTech and Moderna Vaccines. Eur. Rev. Med. Pharmacol. Sci. 2021, 25, 1663–1669. [Google Scholar] [CrossRef] [PubMed]
- Polack, F.P.; Thomas, S.J.; Kitchin, N.; Absalon, J.; Gurtman, A.; Lockhart, S.; Perez, J.L.; Pérez Marc, G.; Moreira, E.D.; Zerbini, C.; et al. Safety and efficacy of the BNT162b2 mRNA Covid-19 vaccine. N. Engl. J. Med. 2020, 383, 2603–2615. [Google Scholar] [CrossRef]
- Baden, L.R.; El Sahly, H.M.; Essink, B.; Kotloff, K.; Frey, S.; Novak, R.; Diemert, D.; Spector, S.A.; Rouphael, N.; Creech, C.B.; et al. Efficacy and Safety of the mRNA-1273 SARS-CoV-2 Vaccine. N. Engl. J. Med. 2021, 384, 403–416. [Google Scholar] [CrossRef]
- Sadoff, J.; Gray, G.; Vandebosch, A.; Cárdenas, V.; Shukarev, G.; Grinsztejn, B.; Goepfert, P.A.; Truyers, C.; Fennema, H.; Spiessens, B.; et al. Safety and Efficacy of Single-Dose Ad26.COV2.S Vaccine against Covid-19. N. Engl. J. Med. 2021, 384, 2187–2201. [Google Scholar] [CrossRef]
- García-Grimshaw, M.; Ceballos-Liceaga, S.E.; Hernández-Vanegas, L.E.; Núñez, I.; Hernández-Valdivia, N.; Carrillo-García, D.A.; Michel-Chávez, A.; Galnáres-Olalde, J.A.; Carbajal-Sandoval, G.; Saniger-Alba, M.D.M.; et al. Neurologic adverse events among 704,003 first-dose recipients of the BNT162b2 mRNA COVID-19 vaccine in Mexico: A nationwide descriptive study. Clin. Immunol. 2021, 229, 108786. [Google Scholar] [CrossRef] [PubMed]
- About the Vaccine Adverse Event Reporting System (VAERS). Available online: https://wonder.cdc.gov/vaers.html (accessed on 25 September 2021).
- Fathizadeh, H.; Afshar, S.; Masoudi, M.R.; Gholizadeh, P.; Asgharzadeh, M.; Ganbarov, K.; Köse, Ş.; Yousefi, M.; Kafil, H.S. SARS-CoV-2 (Covid-19) vaccines structure, mechanisms and effectiveness: A review. Int. J. Biol. Macromol. 2021, 188, 740–750. [Google Scholar] [CrossRef]
- Understanding Viral Vector COVID-19 Vaccines. Available online: https://www.cdc.gov/coronavirus/2019-ncov/vaccines/different-vaccines/viralvector.html?CDC_AA_refVal=https%3A%2F%2Fwww.cdc.gov%2Fvaccines%2Fcovid-19%2Fhcp%2Fviral-vector-vaccine-basics.html (accessed on 25 September 2021).
- COVID-19 mRNA Pfizer- BioNTech Vaccine Analysis Print. Medicines and Healthcare Products Regulatory Agency (MHRA) COVID-19 mRNA Pfizer-BionNTech Vaccine Analysis Print. Available online: https://www.gov.uk/government/publications/regulatory-approval-of-pfizer-biontech-vaccine-for-covid-19/summary-public-assessment-report-for-pfizerbiontech-covid-19-vaccine (accessed on 25 September 2021).
- COVID-19 Moderna Vaccine Analysis Print. Medicines and Healthcare Products Regulatory Agency (MHRA) COVID-19 mRNA Moderna Vaccine Analysis Print. Available online: https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/1014844/Moderna.pdf (accessed on 25 September 2021).
- COVID-19 Vaccine AstraZeneca Analysis Print. Medicines and Healthcare Products Regulatory Agency (MHRA) COVID-19 Vaccine AstraZeneca Analysis Print. Available online: https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/1014843/AstraZeneca.pdf (accessed on 25 September 2021).
- Waheed, S.; Bayas, A.; Hindi, F.; Rizvi, Z.; Espinosa, P.S. Neurological Complications of COVID-19: Guillain-Barre Syndrome Following Pfizer COVID-19 Vaccine. Cureus 2021, 13. [Google Scholar] [CrossRef]
- Razok, A.; Shams, A.; Almeer, A.; Zahid, M. Post-COVID-19 vaccine Guillain-Barré syndrome; first reported case from Qatar. Ann. Med. Surg. 2021, 67, 102540. [Google Scholar] [CrossRef] [PubMed]
- Loza, A.M.M.; Holroyd, K.B.; Johnson, S.A.; Pilgrim, D.M.; Amato, A.A. Guillain-Barré Syndrome in the Placebo and Active Arms of a COVID-19 Vaccine Clinical Trial. Neurology 2021, 96, 1052–1054. [Google Scholar] [CrossRef]
- Patel, S.U.; Khurram, R.; Lakhani, A.; Quirk, B. Guillain-Barre syndrome following the first dose of the chimpanzee adenovirus-vectored COVID-19 vaccine, ChAdOx1. BMJ Case Rep. 2021, 14, e242956. [Google Scholar] [CrossRef]
- Azam, S.; Khalil, A.; Taha, A. Guillain-Barré Syndrome in a 67-year-old Male Post COVID-19 Vaccination (Astra Zeneca). Am. J. Med Case Rep. 2021, 9, 424–427. [Google Scholar] [CrossRef]
- Rossetti, A.; Gheihman, G.; O’Hare, M.; Kosowsky, J.M. Guillain-Barré Syndrome presenting as facial diplegia after COVID-19 vaccination: A case report. J. Emerg. Med. 2021, in press. [Google Scholar] [CrossRef] [PubMed]
- Prasad, A.; Hurlburt, G.; Podury, S.; Tandon, M.; Kingree, S.; Sriwastava, S. A Novel Case of Bifacial Diplegia Variant of Guillain-Barré Syndrome Following Janssen COVID-19 Vaccination. Neurol. Int. 2021, 13, 404–409. [Google Scholar] [CrossRef] [PubMed]
- Queler, S.C.; Towbin, A.J.; Milani, C.; Whang, J.; Sneag, D.B. Parsonage-Turner Syndrome Following COVID-19 Vaccination: MR Neurography. Radiol. 2021, 17. [Google Scholar] [CrossRef] [PubMed]
- Keir, G.; Maria, N.I.; Kirsch, C.F. Unique Imaging Findings of Neurologic Phantosmia Following Pfizer-BioNtech COVID-19 Vaccination: A Case Report. Top. Magn. Reson. Imaging 2021, 30, 133–137. [Google Scholar] [CrossRef]
- Dutta, A.; Ghosh, R.; Bhattacharya, D.; Bhat, S.; Ray, A.; Pandit, A.; Das, S.; Dubey, S. Anti-PF4 antibody negative cerebral venous sinus thrombosis without thrombocytopenia following immunization with COVID-19 vaccine in an elderly non-comorbid Indian male, managed with conventional heparin-warfarin based anticoagulation. Diabetes Metab. Syndr. 2021, 15, 102184. [Google Scholar] [CrossRef]
- Castelli, G.P.; Pognani, C.; Sozzi, C.; Franchini, M.; Vivona, L. Cerebral venous sinus thrombosis associated with thrombocytopenia post-vaccination for COVID-19. Crit. Care 2021, 25, 1–2. [Google Scholar] [CrossRef] [PubMed]
- D’Agostino, V.; Caranci, F.; Negro, A.; Piscitelli, V.; Tuccillo, B.; Fasano, F.; Sirabella, G.; Marano, I.; Granata, V.; Grassi, R.; et al. A Rare Case of Cerebral Venous Thrombosis and Disseminated Intravascular Coagulation Temporally Associated to the COVID-19 Vaccine Administration. J. Pers. Med. 2021, 11, 285. [Google Scholar] [CrossRef]
- Mehta, P.R.; Mangion, S.A.; Benger, M.; Stanton, B.R.; Czuprynska, J.; Arya, R.; Sztriha, L.K. Cerebral venous sinus thrombosis and thrombocytopenia after COVID-19 vaccination—A report of two UK cases. Brain Behav. Immun. 2021, 95, 514–517. [Google Scholar] [CrossRef]
- Wolf, M.E.; Luz, B.; Niehaus, L.; Bhogal, P.; Bäzner, H.; Henkes, H. Thrombocytopenia and Intracranial Venous Sinus Thrombosis after “COVID-19 Vaccine AstraZeneca” Exposure. J. Clin. Med. 2021, 10, 1599. [Google Scholar] [CrossRef] [PubMed]
- Zakaria, Z.; Sapiai, N.A.; Ghani, A.R.I. Cerebral venous sinus thrombosis 2 weeks after the first dose of mRNA SARS-CoV-2 vaccine. Acta Neurochir. 2021, 163, 2359–2362. [Google Scholar] [CrossRef]
- Bayas, A.; Menacher, M.; Christ, M.; Behrens, L.; Rank, A.; Naumann, M. Bilateral superior ophthalmic vein thrombosis, ischaemic stroke, and immune thrombocytopenia after ChAdOx1 nCoV-19 vaccination. Lancet 2021, 397, e11. [Google Scholar] [CrossRef]
- Havla, J.; Schultz, Y.; Zimmermann, H.; Hohlfeld, R.; Danek, A.; Kümpfel, T. First manifestation of multiple sclerosis after immunization with the Pfizer-BioNTech COVID-19 vaccine. J. Neurol. 2021, 1–4. [Google Scholar] [CrossRef]
- Vogrig, A.; Janes, F.; Gigli, G.L.; Curcio, F.; Del Negro, I.; D’Agostini, S.; Fabris, M.; Valente, M. Acute disseminated encephalomyelitis after SARS-CoV-2 vaccination. Clin. Neurol. Neurosurg. 2021, 208, 106839. [Google Scholar] [CrossRef] [PubMed]
- Greinacher, A.; Thiele, T.; Warkentin, T.E.; Weisser, K.; Kyrle, P.A.; Eichinger, S. Thrombotic Thrombocytopenia after ChAdOx1 nCov-19 Vaccination. N. Engl. J. Med. 2021, 384, 2092–2101. [Google Scholar] [CrossRef]
- Schultz, N.H.; Sørvoll, I.H.; Michelsen, A.E.; Munthe, L.A.; Lund-Johansen, F.; Ahlen, M.T.; Wiedmann, M.; Aamodt, A.-H.; Skattør, T.H.; Tjønnfjord, G.E.; et al. Thrombosis and Thrombocytopenia after ChAdOx1 nCoV-19 Vaccination. N. Engl. J. Med. 2021, 384, 2124–2130. [Google Scholar] [CrossRef] [PubMed]
- Suresh, P.; Petchey, W. ChAdOx1 nCOV-19 vaccine-induced immune thrombotic thrombocytopenia and cerebral venous sinus thrombosis (CVST). BMJ Case Rep. 2021, 14, e243931. [Google Scholar] [CrossRef]
- Nardone, R.; Versace, V.; Brigo, F.; Tezzon, F.; Zuccoli, G.; Pikija, S.; Hauer, L.; Sellner, J. Herpes Simplex Virus Type 2 Myelitis: Case Report and Review of the Literature. Front. Neurol. 2017, 8, 199. [Google Scholar] [CrossRef]
- Minami, K.; Tsuda, Y.; Maeda, H.; Yanagawa, T.; Izumi, G.; Yoshikawa, N. Acute transverse myelitis caused by Coxsackie virus B5 infection. J. Paediatr. Child Health 2004, 40, 66–68. [Google Scholar] [CrossRef]
- Lim, S.; Park, S.; Choi, H.; Kim, D.; Kim, H.; Yang, B.; Lee, J. Transverse myelitis after measles and rubella vaccination. J. Paediatr. Child Health 2004, 40, 583–584. [Google Scholar] [CrossRef]
- Kozic, D.; Turkulov, V.; Bjelan, M.; Petrovic, K.; Popovic-Petrovic, S.; Vanhoenacker, F.M. Extensive myelitis after oral polio vaccination: MRI features. J. Belg. Radiol. 2014, 97, 358. [Google Scholar] [CrossRef] [PubMed]
- Fonseca, L.F.; Noce, T.R.; Teixeira, M.L.G.; Teixeira, A.L.; Lana-Peixoto, M.A. Early-onset acute transverse myelitis following hepatitis B vaccination and respiratory infection: Case report. Arq. Neuro-Psiquiatria 2003, 61, 265–268. [Google Scholar] [CrossRef]
- Akkad, W.; Salem, B.; Freeman, J.W.; Huntington, M.K. Longitudinally Extensive Transverse Myelitis Following Vaccination with Nasal Attenuated Novel Influenza A(H1N1) Vaccine. Arch. Neurol. 2010, 67, 1018–1020. [Google Scholar] [CrossRef] [PubMed]
- Lehmann, P.V.; Forsthuber, T.; Miller, A.; Sercarz, E.E. Spreading of T-cell autoimmunity to cryptic determinants of an autoantigen. Nat. Cell Biol. 1992, 358, 155–157. [Google Scholar] [CrossRef]
- Blank, M.; Barzilai, O.; Shoenfeld, Y. Molecular mimicry and auto-immunity. Clin. Rev. Allergy Immunol. 2007, 32, 111–118. [Google Scholar] [CrossRef]
- Transverse Myelitis Consortium Working Group Proposed diagnostic criteria and nosology of acute transverse myelitis. Neurol. 2002, 59, 499–505. [CrossRef]
- Pagenkopf, C.; Südmeyer, M. A case of longitudinally extensive transverse myelitis following vaccination against Covid-19. J. Neuroimmunol. 2021, 358, 577606. [Google Scholar] [CrossRef] [PubMed]
- Bot, J.C.; Barkhof, F.; Polman, C.H.; Nijeholt, G.L.À.; de Groot, V.; Bergers, E.; Ader, H.J.; Castelijns, J.A. Spinal cord abnormalities in recently diagnosed MS patients: Added value of spinal MRI examination. Neurology 2004, 62, 226–233. [Google Scholar] [CrossRef]
- Malhotra, H.S.; Gupta, P.; Prabhu, V.; Garg, R.K.; Dandu, H.; Agarwal, V. COVID-19 vaccination-associated myelitis. QJM: Int. J. Med. 2021, 114, 591–593. [Google Scholar] [CrossRef] [PubMed]
- Fitzsimmons, W.; Nance, C.S. Sudden Onset of Myelitis after COVID-19 Vaccination: An Under-Recognized Severe Rare Adverse Event. SSRN 2021, 7, 3841558. [Google Scholar] [CrossRef]
- James, J.; Jose, J.; Gafoor, V.A.; Smita, B.; Balaram, N. Guillain-Barré syndrome following ChAdOx1 nCoV-19 COVID-19 vaccination: A case series. Neurol. Clin. Neurosci. 2021, 9, 402–405. [Google Scholar] [CrossRef] [PubMed]
- Livingston, E.H.; Malani, P.N.; Creech, C.B. The Johnson & Johnson Vaccine for COVID-19. JAMA 2021, 325, 1575. [Google Scholar] [CrossRef] [PubMed]
- Baxter, R.; Lewis, E.; Fireman, B.; DeStefano, F.; Gee, J.; Klein, N.P. Case-centered Analysis of Optic Neuritis after Vaccines: Table 1. Clin. Infect. Dis. 2016, 63, 79–81. [Google Scholar] [CrossRef]
- Alvarez, L.M.; Ning, N.Y.; Davagnanam, I.; Ashenhurst, M.; Acheson, J.; Abdel-Hay, A.; Alshowaeir, D.; Bakheet, M.; Balaguer, O.; Batra, R.; et al. Post Vaccination Optic Neuritis: Observations from the SARS-CoV-2 Pandemic. Available online: https://ssrn.com/abstract=3889990 (accessed on 25 September 2021).
- Maleki, A.; Look-Why, S.; Manhapra, A.; Foster, C.S. COVID-19 Recombinant mRNA Vaccines and Serious Ocular Inflammatory Side Effects: Real or Coincidence? J. Ophthalmic Vis. Res. 2021, 16, 490–501. [Google Scholar] [CrossRef]
- Blauenfeldt, R.A.; Kristensen, S.R.; Ernstsen, S.L.; Kristensen, C.C.H.; Simonsen, C.Z.; Hvas, A.M. Thrombocytopenia with acute ischemic stroke and bleeding in a patient newly vaccinated with an adenoviral vector-based COVID-19 vaccine. J. Thromb. Haemost. 2021, 19, 1771–1775. [Google Scholar] [CrossRef]
- Bjørnstad-Tuveng, T.H.; Rudjord, A.; Anker, P. Fatal cerebral haemorrhage after COVID-19 vaccine. Tidsskr. Nor Laegeforen. 2021, 29, 141. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Author/Country | Patient Age/Gender | Vaccination | Time Duration from COVID-19 Vaccination to Neurological Symptom Onset | Diagnosis | Neurological Presentation | CSF Findings Cell Count, Protein, Glucose, Oligoclonal Bands | MRI Brain/Spine Finding | CT Finding | CTA/MRA Finding | CT/MR VENOGRAPHY Findings | Treatment | Outcome |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Waheed et al./US [14] | 82 years/F | Pfizer | 14 days | GBS | Generalized malaise, body aches and difficulty walking | Showed albumino-cytologic dissociation Protein of 88 mg/dL, Cell Count: WBC of 4/mm3 | MRI L spine: Enhancement of cauda equina nerve roots | Normal | N/A | N/A | IVIG | Recovered |
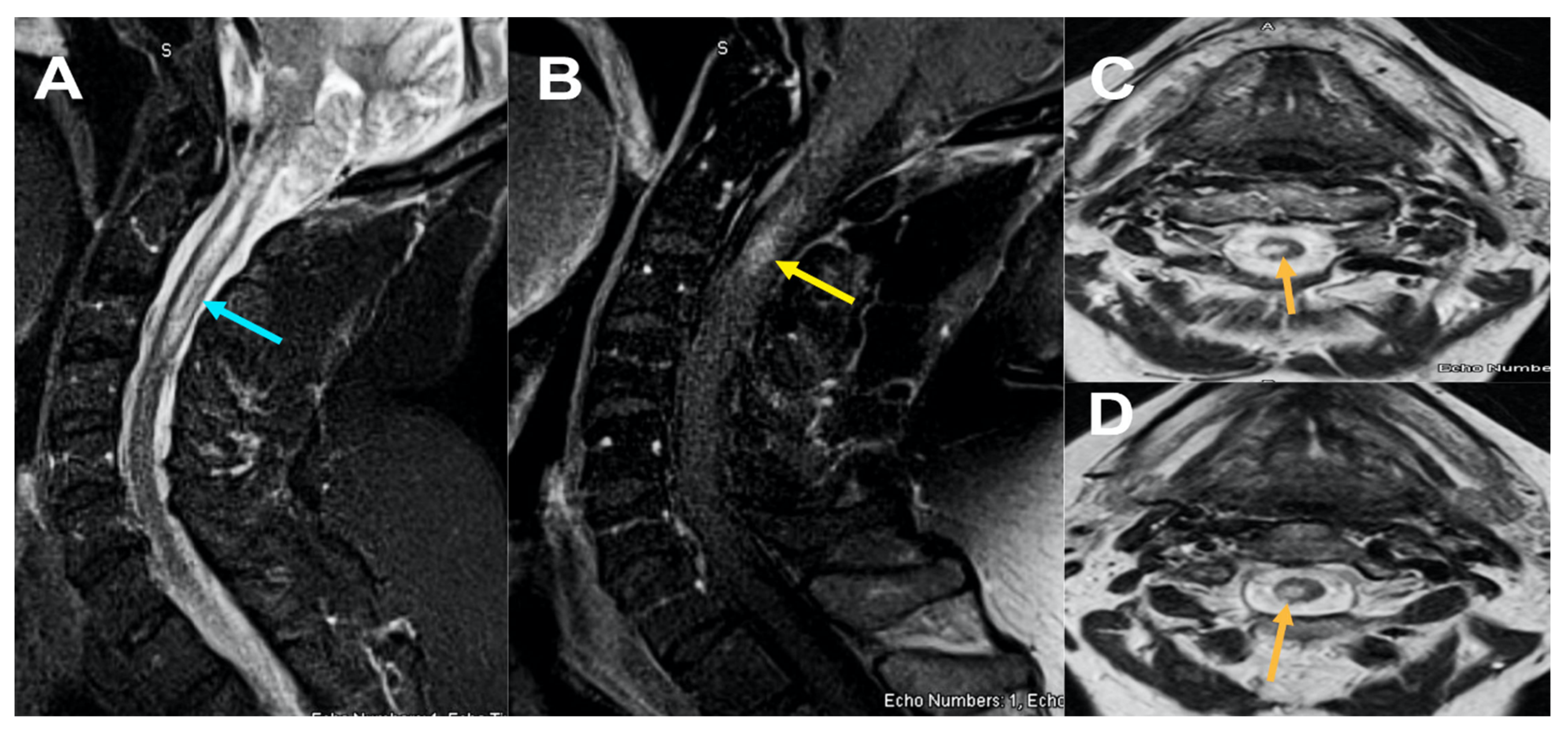
| Malhotra et al./India [46] | 36 years/M | AstraZeneca | 8 days | Transverse Myelitis | Abnormal sensation in the lower limbs. | Protein: 54 mg/dL Cell count: normal Oligoclonal bands negative | MRI spine: T2-hyperintense lesion at C6-C7 with enhancement | N/A | N/A | N/A | IV steroids | Recovered |
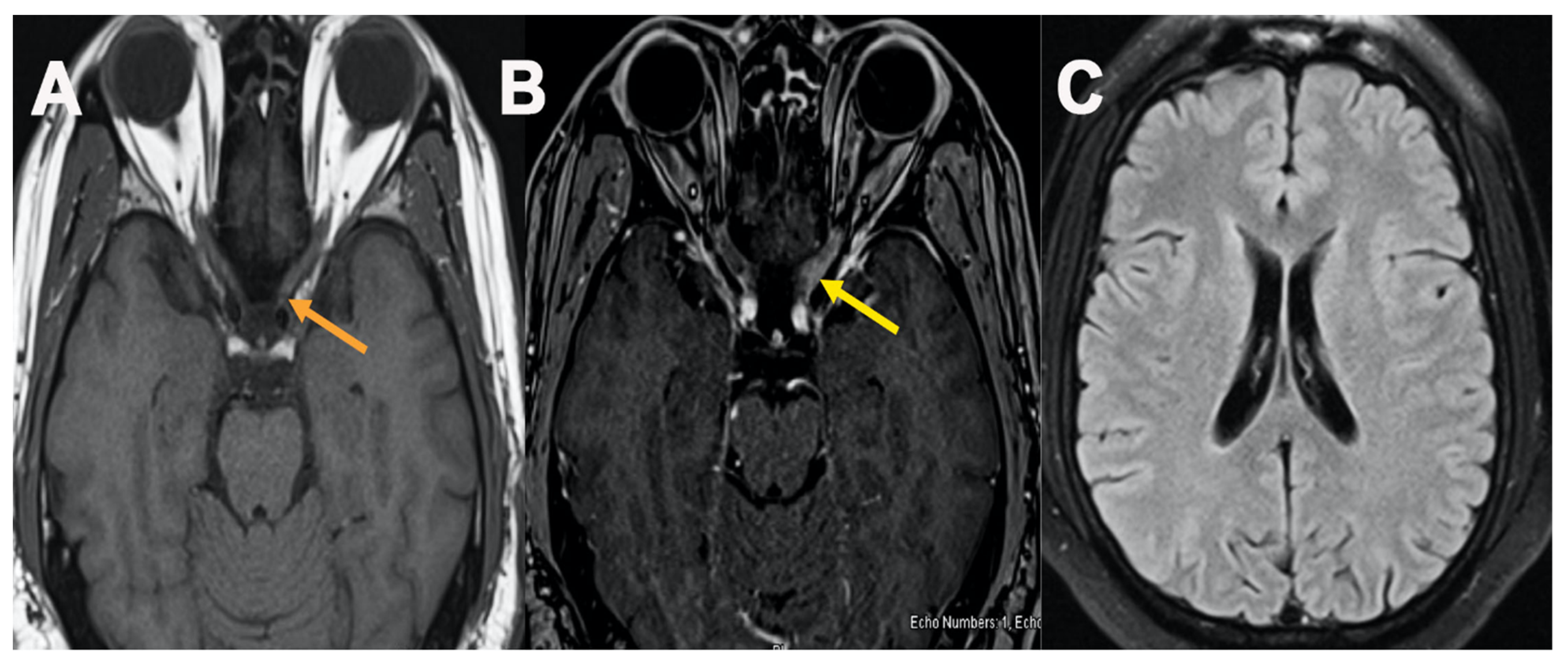
| Keir et al./US [22] | 57 years/F | Pfizer | Post-second dose | Phantosmia | Smelling smoke, hyposmia and headaches | N/A | MRI brain: enhancement of the left greater than right olfactory bulb and bilateral olfactory tracts and hyperintensity in olfactory bulbs and tracts | Normal | CTA no vessel occlusion or aneurysm | N/A | None | Recovered |
| Razok et al./Qatar [15] | 73 years/M | Pfizer | 20 days | GBS | Progressive lower limb weakness | Protein: 80 mg/dL (elevated) Cell Count: Normal Glucose: Normal Oligoclonal band: negative | MRI L spine: bilateral nerve root enhancement in the lumbar region and the upper part of the cauda equina | Normal | N/A | N/A | IVIG | Recovered |
| Jose et al./India [48] | 66 years/M | AstraZeneca | 12 days | GBS | Sensorimotor weakness Proximal lower limb with mild hand grip weakness | Cell protein: 84 mg/dL (elevated) Cell count: Normal Glucose: Normal | MRI L Spine: normal | N/A | N/A | N/A | IVIG and Steroids | Partially recovered |
| Prasad et al./US [20] | 41 years/M | Janssen | 21 days | GBS/BFP variant | Difficulty feeding and ambulating | Cell count: 50/mm3 Protein: 562 mg/dL Glucose: 67 mg/dL | MRI L spine with contrast showed thickening of cauda equina nerve roots | N/A | N/A | N/A | IVIG | Recovered |
| Márquez Loza AM et al./US [16] | 60 years/M | Janssen | 10 days | GBS | Pain in her back and leg. Nausea, vomiting, headache and diplopia | CSF Protein: 140 mg/dL, Cell count: 9 nucleated cells/mm3 Glucose: Normal | MRI L spine: demonstrated enhancement of the cauda equina | N/A | N/A | N/A | IVIG | Recovered |
| Queler SC et al./US [21] | 49 years/M | Pfizer | 13 hr post-first dose | Parsonage-Turner Syndrome | Severe, electric shooting pain in his left volar forearm | N/A | MR neurography: hyperintensity of the anteromedially positioned fascicular bundle of the median nerve were detected | N/A | N/A | N/A | Gabapentin and oral steroids | Partial Recovery with weakness |
| Queler SC et al./US [21] | 44 years/M | Moderna | 18 days | Parsonage-Turner Syndrome | Sudden onset, intense, cramping pain in the left lateral deltoid region | N/A | MR Neurography: hyperintensity and multiple, focal, hourglass-like constrictions of the suprascapular nerve with edema | N/A | N/A | N/A | Gabapentin | Improved |
| Havla et al./Germany [30] | 28 years/F | Pfizer | 6 days | Multiple sclerosis | Left abdominal neuropathic pain, sensory impairment below the T6 level | CSF cell count: 7/mm3 Oligoclonal band: Positive | MRI brain: Multiple confluent T2/FLAIR lesions in periventricular, cortical, juxtacortical, splenium of corpus callosum and infratentorial region no enhancement. MRI spine: contrast-enhancing lesion at the T6 level | N/A | N/A | N/A | IV steroids and plasmapheresis | Improved |
| Patel et al./UK [17] | 37 years/M | AstraZeneca | 14 days | GBS | Persistent back pain, distal paraesthesia in hands and feet, symmetrical progressive ascending muscle weakness | CSF protein:177 mg/dL Glucose: 70 mg/dL Cell Count: < 1/mm3 | MRI L spine: illustrated globally thickened cauda equina nerve root particularly at the level of S1 | N/A | N/A | N/A | IVIG | Improved |
| Azam et al./UK [18] | 67 years/M | AstraZeneca | 15 days | GBS BFP variant | progressive worsening of the gait, bilateral leg, bilateral facial weakness, and difficulty in chewing food | CSF Protein: 390 mg/dL Glucose: 86 mg/dL | MRI brain: showed enhancement of the facial nerve bilaterally at the fundus of the internal auditory meatus extending into the labyearsinthine segment | Normal | N/A | N/A | IVIG | Improved |
| Fitzsimmons et al./US [47] | 63 years/M | Moderna | 2 days | Transversemyelitis | Shooting pain and numbness in lower legs and buttocks. Difficulty urinating and constipation | CSF: glucose 74 mg/dL CSF total protein 37 mg/dL Cell count: total nucleated cell counts 3/mm3 | MRI brain: Few punctate hyperintensities in bilateral corona radiata. MRI spine: Increased T2 cord signal distal spinal cord and conus with questionable associated enhancement | N/A | N/A | N/A | Oral and IV steroids | Recovered |
| Schultz et al./Norway [33] | 54 years/F | AstraZeneca | 7 days | CVST | Hemiparesis on the left side of her body | N/A | N/A | Right frontal hemorrhage | N/A | A CT scan with venography showed a massive cerebral vein thrombosis with global edema and growth of hematoma | Oral steroids, IVIG, Heparin, decompressive Hemicraniectomy | Deceased |
| Vogrig et al/Italy [31] | 56 years/F | Pfizer | 14 days | ADEM | Left side unsteady gait and clumsiness of left arm. | CSF cell count: pleocytosis (80 cells/mm3) CSF protein: Normal Glucose: Normal | MRI brain hyperintensity involving the frontal white matter, with the largest lesion on the left side | N/A | N/A | N/A | Oral Steroids | Recovered |
| Dutta et al./India [23] | 51 years/ M | AstraZeneca | 5 days after first dose | CVST | Holocephalic headache, vomiting | N/A | N/A | N/A | N/A | MR Venography:Thrombosis in superior sagittal sinus and transverse sinus with presence of extensive venous collaterals | LMWH | Improved |
| Rossetti et al./US [19] | 38 years/M | Janssen | 14 weeks | GBS/BFP | Bilateral hand and foot paresthesias, dysarthria, bilateral facial weakness | CSF Glucose: 73 mg/dL CSF protein: 181 mg/dL Cell Count: 7/mm3 | MRI brain: bilateral internal auditory canal fundi which carry CN-VII and CN-VIII | N/A | N/A | N/A | IVIG | Improved |
| Bayas et al./Germany [29] | 55 years/F | AstraZeneca | 10 days | SOVT | Conjunctival congestion, retro-orbital pain, and diplopia | N/A | MRI brain: Showed superior ophthalmic vein thrombosis (SOVT) | N/A | N/A | N/A | Heparin | Recovered |
| Blauenfeldt et al./Denmark [53] | 60 years/F | AstraZeneca | 7 days | Ischemic stroke | Persistent abdominal pain. Left-sided weakness and eye deviation to the right | N/A | MRI brain: Diffusion restriction and infarction in the entire area supplied by the right middle cerebral artery | Midline shift of 12 mm | N/A | N/A | Dalteparin, hemicraniectomy | Deceased |
| Castelli et al./Italy [24] | 50 years/M | AstraZeneca | 11 days after First Dose | CVST | Severe headache, loss of strength in the right lower limb, unstable walking and slight visual impairment | N/A | N/A | Intraparenchymal hemorrhage in the left hemisphere. | CTA multiple bleeding within the parenchymal and left transverse and sigmoid sinuses, thrombosis | N/A | Bilateral decompressive craniectomy | Deceased |
| Agostino et al./Italy [25] | 54 years/F | AstraZeneca | 12 days | CVST | Acute cerebrovascular accident | N/A | MRI brain: restricted diffusion in pons, mesencephalon, the right superior cerebellar hemisphere with the vermis and the right posterior temporal lobe | Presence of multiple subacute intra-axial hemorrhages | CTA partial thrombosis of the vein of Galen; MRA: acute basilar thrombosis associated with superior coronal and sagittal sinus thrombosis. | N/A | No | Deceased |
| Mehta et al./UK [26] | 32 years/M | AstraZeneca | 9 days post first dose | CVST | Thunderclap headache and subsequent left-sided incoordination and hemiparesis | N/A | N/A | Clot expanding the middle to anterior third of the superior sagittal sinus, seen as an area of hyper density | N/A | Superior sagittal sinus and cortical vein thrombosis and cortical oedema with areas of parenchymal and subarachnoid hemorrhage | No | Deceased |
| Mehta et al./UK [26] | 25 years/M | AstraZeneca | 6 days | CVST | Meningitis headache, photophobia, vomiting, petechial rash, gum bleeding, left hemiparesis, left hemisensory loss | N/A | N/A | Large volume clot within the superior sagittal sinus | N/A | Large filling defect in the anterior two thirds of the superior sagittal sinus | Unfractionated heparin | Deceased |
| Wolf et al./Germany [27] | 22 years/F | AstraZeneca | 4 days | CVST | Frontally accentuated headaches, self-limited generalized epileptic seizures | N/A | MRI brain: Blood in the subarachnoid space adjacent to the falx cerebri bilateral. The superior sagittal sinus, the left transverse sinus, and the sigmoid sinus were thrombosed | N/A | MRA: Revealed thrombotic occlusion of the superior sagittal sinus | N/A | Enoxaparin | Recovered |
| Wolf et al./Germany [27] | 46 years/F | AstraZeneca | 8 days | CVST | Severe headaches, focal neurologic symptoms with mild aphasia and hemianopia to the right | N/A | MRI brain: Thrombotic occlusion of the superior sagittal sinus and the left transverse sinus and sigmoid sinus. | N/A | Occlusion of the superior sagittal sinus and the left transverse sinus and the sigmoid sinus | N/A | Enoxaparin, Dabigatran, Endovascular recanalization | Recovered |
| Wolf et al./Germany [27] | 36 years/F | AstraZeneca | 7 days | CVST | Severe headaches | N/A | MRI Brain showed a thrombotic occlusion of the straight sinus and a non-occlusive thrombus in the superior sagittal sinus. | N/A | occlusion of the straight sinus and a non-occlusive thrombus of the superior sagittal sinus. | N/A | Enoxaparin, Dabigatran, Endovascular recanalization | Recovered |
| Bjornstad-Tweng et al./Norway [54] | 30 years/F | AstraZeneca | 7 days | Cerebral hemorrhage | Severe headaches, slurred speech, uncoordinated movements and reduced consciousness | N/A | N/A | Showed right-sided hemorrhage and incipient herniation. | CT angiography showed no evidence of an aneurysm. | N/A | Tranexamic acid | Deceased |
| Pagenkopf et al./Germany [44] | 45 years/M | AstraZeneca | 8 days | Transverse myelitis | Headache, thoracic back pain and general weakness, urinary retention; acute flaccid tetraparesis, emphasizing lower limbs, and a sensory level at Th9 | CSF Cell Count: pleocytosis of 481 cells/μL Protein: (140 mg/dL), Glucose: normal Negative oligoclonal bands. | MRI brain: Normal MRI Spine: hyperintense signal of the spinal cord with wide axial and longitudinal extent reaching from C3 to Th2 without gadolinium enhancement | N/A | N/A | N/A | IV corticosteroids | Improved |
| Zakaria Z et al./Malaysia [28] | 49 years/M | Pfizer | 16 days | CVST | Moderate headache and dizziness | N/A | N/A | Showed cordlike hyper-attenuation within the left transverse and sigmoid sinus suggestive of cord or dense clot sign | N/A | Long segment-filling defect and empty delta sign within the superior sagittal sinus (SSS), extending in left transverse sinus, and sigmoid sinus to proximal internal jugular vein | Apixaban, Clopidogrel | Recovered |
| Neurological Complications | Pfizer-BioNTech BNT162b | Moderna mRNA-1273 | AstraZeneca Vaccine |
|---|---|---|---|
| Cerebrovascular accident | 322 | 7 | 1168 |
| Ischemic stroke | 33 | 1 | 140 |
| Hemorrhagic stroke | 9 | 0 | 39 |
| Guillain-Barré syndrome | 44 | 3 | 393 |
| Transverse myelitis | 26 | 0 | 81 |
| Bell’s palsy | 402 | 32 | 551 |
| Cerebral venous sinus thrombosis | 28 | 1 | 205 |
| Optic neuritis | 24 | 3 | 51 |
| Neurological Complications | Pfizer-BioNTech BNT162b | Moderna mRNA-1273 | Janssen |
|---|---|---|---|
| Cerebrovascular accident | 198 | 155 | 5 |
| Ischemic stroke | 175 | 114 | 47 |
| Hemorrhagic stroke | 59 | 34 | 14 |
| Guillain-Barré syndrome | 49 | 49 | 81 |
| Transverse myelitis | 87 | 63 | 25 |
| Bell’s palsy | 1647 | 1322 | 194 |
| Cerebral venous sinus thrombosis | 25 | 22 | 29 |
| Optic neuritis | 40 | 39 | 8 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sriwastava, S.; Shrestha, A.K.; Khalid, S.H.; Colantonio, M.A.; Nwafor, D.; Srivastava, S. Spectrum of Neuroimaging Findings in Post-COVID-19 Vaccination: A Case Series and Review of Literature. Neurol. Int. 2021, 13, 622-639. https://doi.org/10.3390/neurolint13040061
Sriwastava S, Shrestha AK, Khalid SH, Colantonio MA, Nwafor D, Srivastava S. Spectrum of Neuroimaging Findings in Post-COVID-19 Vaccination: A Case Series and Review of Literature. Neurology International. 2021; 13(4):622-639. https://doi.org/10.3390/neurolint13040061
Chicago/Turabian StyleSriwastava, Shitiz, Ashish K. Shrestha, Syed Hassan Khalid, Mark A. Colantonio, Divine Nwafor, and Samiksha Srivastava. 2021. "Spectrum of Neuroimaging Findings in Post-COVID-19 Vaccination: A Case Series and Review of Literature" Neurology International 13, no. 4: 622-639. https://doi.org/10.3390/neurolint13040061