
PLGA Nanoparticles Loaded with Sorafenib Combined with Thermosensitive Hydrogel System and Microwave Hyperthermia for Multiple Sensitized Radiotherapy
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
2.1. Reagents
2.2. Cell Culture
2.3. Preparation and Characterization of Sorafenib-Loaded PLGA Nanoparticles (SP NPs) and Sorafenib-Loaded PLA Nanoparticles (SA NPs)
2.4. Drug Release Study
2.5. Preparation and Characterization of SPH
2.6. Microwave Heating and Drug Release Study Experiment In Vitro
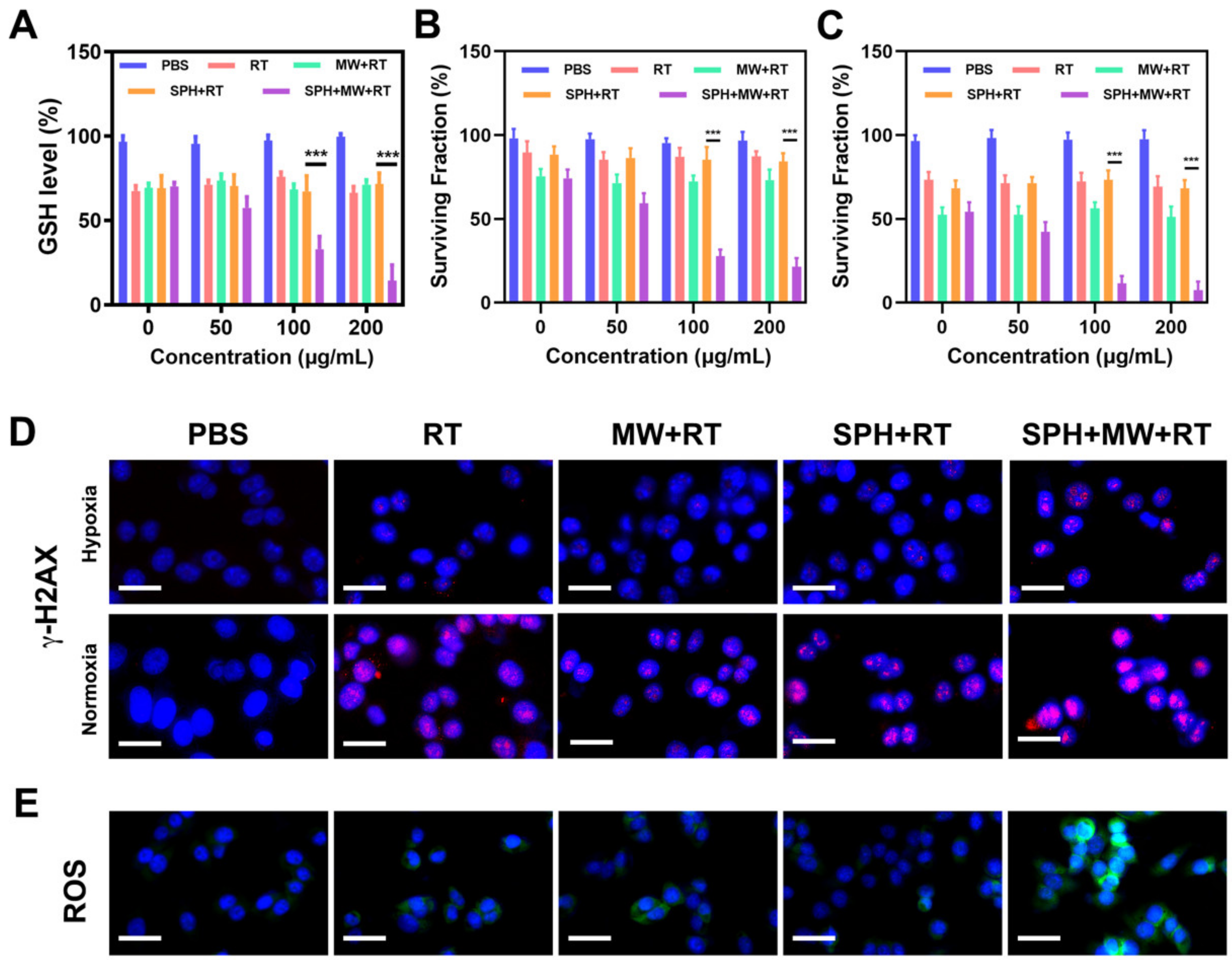
2.7. In Vitro Colony Formation Assay
2.8. In Vitro ROS Generation
2.9. Detection of Intracellular GSH
2.10. γ-H2AX Immunofluorescence Analysis In Vitro
2.11. Animal Tumor Models
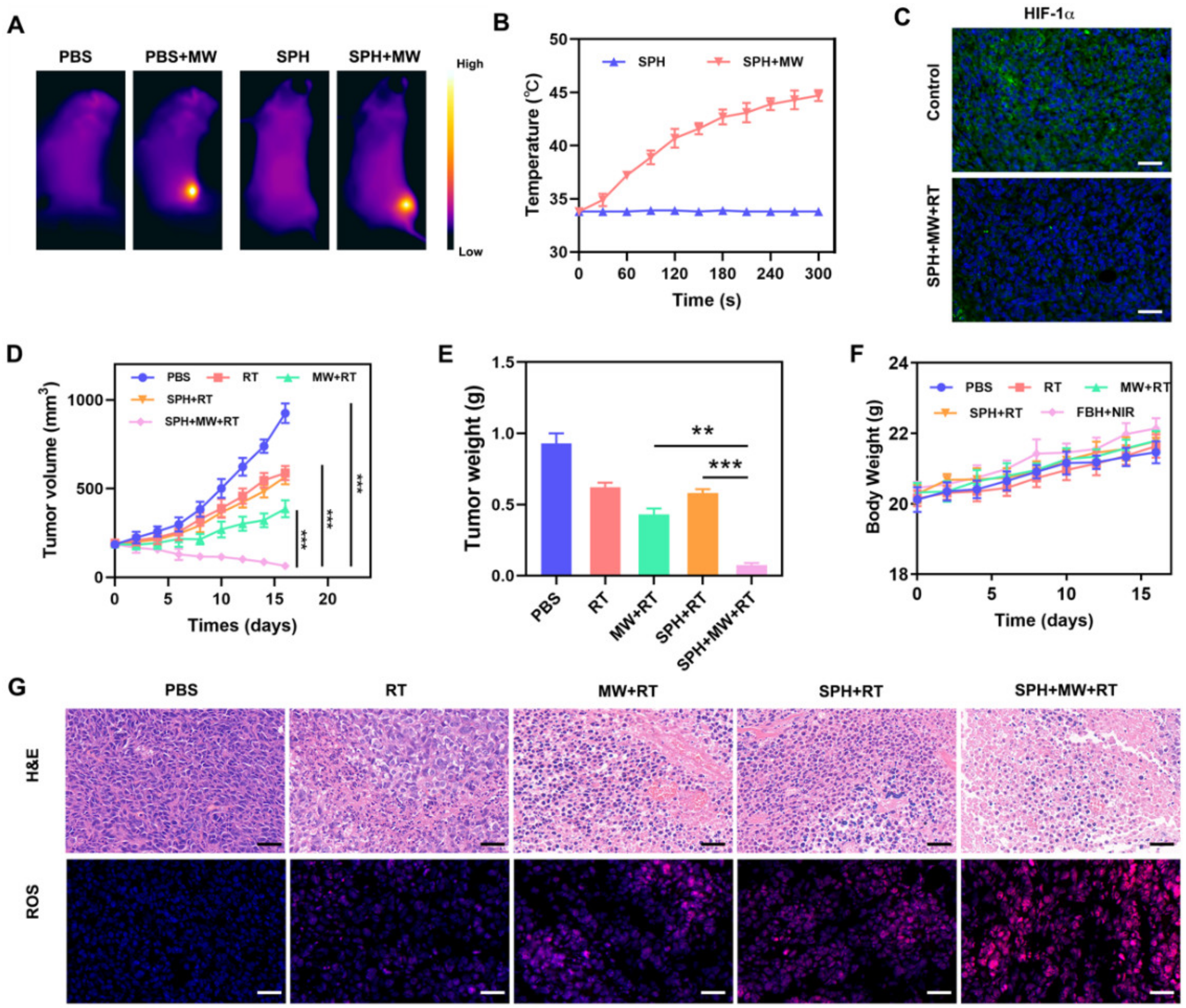
2.12. In Vivo Infrared Thermography
2.13. In Vivo Antitumor Study
2.14. In Vivo Tumor Vascular and Hypoxia Microenvironment Study
2.15. In Vivo Toxicity
2.16. Statistical Analysis
3. Results and Discussion
4. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Yamada, D.; Ohde, S.; Kajiura, Y.; Yagishita, K.; Nozaki, F.; Suzuki, K.; Kanomata, N.; Yamauchi, H.; Tsunoda, H. Relationship between Breast Density, Breast Cancer Subtypes, and Prognosis. Clin. Breast Cancer 2022, 22, 560–566. [Google Scholar] [CrossRef] [PubMed]
- Sakai, T.; Ozkurt, E.; DeSantis, S.; Wong, S.M.; Rosenbaum, L.; Zheng, H.; Golshan, M. National trends of synchronous bilateral breast cancer incidence in the United States. Breast Cancer Res. Treat. 2019, 178, 161–167. [Google Scholar] [CrossRef] [PubMed]
- Masuda, H.; Zhang, D.W.; Bartholomeusz, C.; Doihara, H.; Hortobagyi, G.N.; Ueno, N.T. Role of epidermal growth factor receptor in breast cancer. Breast Cancer Res. Treat. 2012, 136, 331–345. [Google Scholar] [CrossRef]
- Onega, T.; Zhu, W.; Weiss, J.E.; Goodrich, M.; Tosteson, A.N.A.; DeMartini, W.; Virnig, B.A.; Henderson, L.M.; Buist, D.S.M.; Wernli, K.J.; et al. Preoperative breast MRI and mortality in older women with breast cancer. Breast Cancer Res. Treat. 2018, 170, 149–157. [Google Scholar] [CrossRef]
- Schiavon, G.; Hrebien, S.; Garcia-Murillas, I.; Cutts, R.J.; Pearson, A.; Tarazona, N.; Fenwick, K.; Kozarewa, I.; Lopez-Knowles, E.; Ribas, R.; et al. Analysis of ESR1 mutation in circulating tumor DNA demonstrates evolution during therapy for metastatic breast cancer. Sci. Transl. Med. 2015, 7, 313ra182. [Google Scholar] [CrossRef] [PubMed]
- Miller, K.D.; Siegel, R.L.; Lin, C.C.; Mariotto, A.B.; Kramer, J.L.; Rowland, J.H.; Stein, K.D.; Alteri, R.; Jemal, A. Cancer treatment and survivorship statistics, 2016. CA Cancer J. Clin. 2016, 66, 271–289. [Google Scholar] [CrossRef]
- Deng, J.; Xu, S.; Hu, W.; Xun, X.; Zheng, L.; Su, M. Tumor targeted, stealthy and degradable bismuth nanoparticles for enhanced X-ray radiation therapy of breast cancer. Biomaterials 2018, 154, 24–33. [Google Scholar] [CrossRef]
- Babaei, M.; Ganjalikhani, M. The potential effectiveness of nanoparticles as radio sensitizers for radiotherapy. BioImpacts BI 2014, 4, 15–20. [Google Scholar] [CrossRef]
- Wardman, P. Chemical radiosensitizers for use in radiotherapy. Clin. Oncol. R. Coll. Radiol. 2007, 19, 397–417. [Google Scholar] [CrossRef]
- Luukkaa, M.; Jokilehto, T.; Kronqvist, P.; Vahlberg, T.; Grénman, R.; Jaakkola, P.; Minn, H. Expression of the cellular oxygen sensor PHD2 (EGLN-1) predicts radiation sensitivity in squamous cell cancer of the head and neck. Int. J. Radiat. Biol. 2009, 85, 900–908. [Google Scholar] [CrossRef]
- Saga, T.; Sakahara, H.; Nakamoto, Y.; Sato, N.; Ishimori, T.; Mamede, M.; Kobayashi, H.; Masunaga, S.; Sasai, K.; Kuroki, M.; et al. Enhancement of the therapeutic outcome of radio-immunotherapy by combination with whole-body mild hyperthermia. Eur. J. Cancer 2001, 37, 1429–1434. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Yu, M.; Xiao, L.; Xu, S.; Yi, Q.; Jin, W. Radiosensitizing effect of oleanolic acid on tumor cells through the inhibition of GSH synthesis in vitro. Oncol. Rep. 2013, 30, 917–924. [Google Scholar] [CrossRef] [PubMed]
- Quintana-Cabrera, R.; Bolaños, J.P. Glutathione and γ-glutamylcysteine in the antioxidant and survival functions of mitochondria. Biochem. Soc. Trans. 2013, 41, 106–110. [Google Scholar] [CrossRef] [PubMed]
- Xu, J.; Gao, J.; Wei, Q. Combination of Photodynamic Therapy with Radiotherapy for Cancer Treatment. J. Nanomater. 2016, 2016, 8507924. [Google Scholar] [CrossRef]
- Sarihan, S.; Kayisogullari, U.; Ercan, I.; Engin, K. Randomized Phase 2 Study of Radiotherapy Alone versus Radiotherapy with Paclitaxel in Non-Small Cell Lung Cancer. J. Int. Med. Res. 2004, 32, 375–383. [Google Scholar] [CrossRef] [PubMed]
- Falk, M.H.; Issels, R.D. Hyperthermia in oncology. Int. J. Hyperth. 2001, 17, 1–18. [Google Scholar] [CrossRef]
- Ayala-Orozco, C.; Urban, C.; Bishnoi, S.; Urban, A.; Charron, H.; Mitchell, T.; Shea, M.; Nanda, S.; Schiff, R.; Halas, N.; et al. Sub-100nm gold nanomatryoshkas improve photo-thermal therapy efficacy in large and highly aggressive triple negative breast tumors. J. Control. Release 2014, 191, 90–97. [Google Scholar] [CrossRef]
- Kuthala, N.; Vankayala, R.; Li, Y.N.; Chiang, C.S.; Hwang, K.C. Engineering Novel Targeted Boron-10-Enriched Theranostic Nanomedicine to Combat against Murine Brain Tumors via MR Imaging-Guided Boron Neutron Capture Therapy. Adv. Mater. 2017, 29, 1700850. [Google Scholar] [CrossRef]
- Yang, H.; Liu, Z.; Li, X.; Zhang, Z.; Chen, D.; Lian, H. Artesunate-Loaded and Near-Infrared Dye-Conjugated Albumin Nanoparticles as High-Efficiency Tumor-Targeted Photo-Chemo Theranostic Agent. Nanoscale Res. Lett. 2018, 13, 319. [Google Scholar] [CrossRef]
- Gardner, R.A.; Vargas, H.I.; Block, J.B.; Vogel, C.L.; Fenn, A.J.; Kuehl, G.V.; Doval, M. Focused microwave phased array thermotherapy for primary breast cancer. Ann. Surg. Oncol. 2002, 9, 326–332. [Google Scholar] [CrossRef]
- Rychlik, O.; Vrba, J. Planar spiral applicator for local microwave thermotherapy. In Proceedings of the 14th Conference on Microwave Techniques, Prague, Czech Republic, 23–24 April 2008; pp. 271–273. [Google Scholar]
- Vrba, J.; Lapes, M.; Oppl, L. Technical aspects of microwave thermotherapy. Bioelectrochem. Bioenerg. 1999, 48, 305–309. [Google Scholar] [CrossRef] [PubMed]
- Sun, M.R.; Kiourti, A.; Wang, H.; Zhao, S.T.; Zhao, G.; Lu, X.B.; Volakis, J.L.; He, X.M. Enhanced Microwave Hyperthermia of Cancer Cells with Fullerene. Mol. Pharm. 2016, 13, 2184–2192. [Google Scholar] [CrossRef] [PubMed]
- Song, J.J.; Sun, X.H.; Du, Y.X.; Wu, Q.; Niu, M.; Fu, C.H.; Tan, L.F.; Ren, X.L.; Chen, L.F.; Meng, X.W. Micro-Opening Ridged Waveguide Tumor Hyperthermia Antenna Combined with Microwave-Sensitive MOF Material for Tumor Microwave Hyperthermia Therapy. ACS Appl. Bio Mater. 2022, 5, 4154–4164. [Google Scholar] [CrossRef] [PubMed]
- Fhager, A.; Trefna, H.D.; Shafiemehr, M.; Persson, M. On the Use of Microwave Based Thermal Monitoring in Hyperthermia. In Proceedings of the 2015 9th European Conference on Antennas and Propagation (EuCAP), Lisbon, Portugal, 13–17 April 2015. [Google Scholar]
- Chen, X.; Tan, L.F.; Liu, T.L.; Meng, X.W. Micro-Nanomaterials for Tumor Microwave Hyperthermia Design Preparation, and Application. Curr. Drug Deliv. 2017, 14, 307–322. [Google Scholar] [CrossRef]
- Maamoun, W.; Badawi, M.I.; Aly, A.A.; Khedr, Y. Nanoparticles in enhancing microwave imaging and microwave Hyperthermia effect for liver cancer treatment. Rev. Adv. Mater. Sci. 2021, 60, 223–236. [Google Scholar] [CrossRef]
- Zölzer, F.; Streffer, C. G2-Phase Delays after Irradiation and/or Heat Treatment as Assessed by Two-Parameter Flow Cytometry. Radiat. Res. 2001, 155, 50–56. [Google Scholar] [CrossRef]
- Zanotto-Filho, A.; Rajamanickam, S.; Loranc, E.; Masamsetti, V.P.; Gorthi, A.; Romero, J.C.; Tonapi, S.; Gonçalves, R.M.; Reddick, R.L.; Benavides, R.; et al. Sorafenib improves alkylating therapy by blocking induced inflammation, invasion and angiogenesis in breast cancer cells. Cancer Lett. 2018, 425, 101–115. [Google Scholar] [CrossRef]
- Arai, H.; Battaglin, F.; Wang, J.; Lo, J.H.; Soni, S.; Zhang, W.; Lenz, H.J. Molecular insight of regorafenib treatment for colorectal cancer. Cancer Treat. Rev. 2019, 81, 101912. [Google Scholar] [CrossRef]
- Pearson, H.; Marshall, L.V.; Carceller, F. Sorafenib in pediatric hepatocellular carcinoma from a clinician perspective. Pediatr. Hematol. Oncol. 2020, 37, 412–423. [Google Scholar] [CrossRef]
- Wilhelm, S.M.; Adnane, L.; Newell, P.; Villanueva, A.; Llovet, J.M.; Lynch, M. Preclinical overview of sorafenib, a multikinase inhibitor that targets both Raf and VEGF and PDGF receptor tyrosine kinase signaling. Mol. Cancer Ther. 2008, 7, 3129–3140. [Google Scholar] [CrossRef] [Green Version]
- Liu, L.; Cao, Y.; Chen, C.; Zhang, X.; McNabola, A.; Wilkie, D.; Wilhelm, S.; Lynch, M.; Carter, C. Sorafenib blocks the RAF/MEK/ERK pathway, inhibits tumor angiogenesis, and induces tumor cell apoptosis in hepatocellular carcinoma model PLC/PRF/5. Cancer Res. 2006, 66, 11851–11858. [Google Scholar] [CrossRef] [PubMed]
- Liu, G.; Kuang, S.; Cao, R.; Wang, J.; Peng, Q.; Sun, C. Sorafenib kills liver cancer cells by disrupting SCD1-mediated synthesis of monounsaturated fatty acids via the ATP-AMPK-mTOR-SREBP1 signaling pathway. FASEB J. 2019, 33, 10089–10103. [Google Scholar] [CrossRef] [PubMed]
- Tesei, A.; Leonetti, C.; Zupi, G.; Scarsella, M.; Brigliadori, G.; Ulivi, P.; Fabbri, F.; Arienti, C.; Amadori, D.; Passardi, A.; et al. Low-dose taxotere enhances the ability of sorafenib to induce apoptosis in gastric cancer models. J. Cell. Mol. Med. 2011, 15, 316–326. [Google Scholar] [CrossRef] [PubMed]
- Chi, Y.; Yang, J.L.; Yang, S.; Sun, Y.K.; Jia, B.; Shi, Y.K. Phase I dose-finding study of sorafenib with FOLFOX4 as first-line treatment in patients with unresectable locally advanced or metastatic gastric cancer. Chin. J. Cancer Res. 2015, 27, 239–246. [Google Scholar] [CrossRef]
- Kim, H.M.; Kim, S.A.; Park, S.B.; Cho, J.H.; Song, S.Y. Sorafenib inhibits 5-fluorouracil-resistant gastric cancer cell growth. Scand. J. Gastroenterol. 2017, 52, 577–584. [Google Scholar] [CrossRef]
- Corrado, A.; Ferrari, S.M.; Politti, U.; Mazzi, V.; Miccoli, M.; Materazzi, G.; Antonelli, A.; Ulisse, S.; Fallahi, P.; Miccoli, P. Aggressive thyroid cancer: Targeted therapy with sorafenib. Minerva Endocrinol. 2017, 42, 64–76. [Google Scholar] [CrossRef]
- Hu, X.; He, Y.; Han, Z.; Liu, W.; Liu, D.; Zhang, X.; Chen, L.; Qi, L.; Chen, L.; Luo, Y.; et al. PNO1 inhibits autophagy-mediated ferroptosis by GSH metabolic reprogramming in hepatocellular carcinoma. Cell Death Dis. 2022, 13, 1010. [Google Scholar] [CrossRef]
- Zhou, Z.; Liang, H.; Yang, R.; Yang, Y.; Dong, J.; Di, Y.; Sun, M. GSH Depletion-Induced Activation of Dimersomes for Potentiating the Ferroptosis and Immunotherapy of “Cold” Tumor. Angew. Chem. 2022, 61, e202202843. [Google Scholar] [CrossRef]
- Feng, W.; Shi, W.; Wang, Z.; Cui, Y.; Shao, X.; Liu, S.; Rong, L.; Liu, Y.; Zhang, H. Enhancing Tumor Therapy of Fe(III)-Shikonin Supramolecular Nanomedicine via Triple Ferroptosis Amplification. ACS Appl. Mater. Interfaces 2022, 14, 37540–37552. [Google Scholar] [CrossRef]
- Chen, Q.; Xu, L.; Liang, C.; Wang, C.; Peng, R.; Liu, Z. Photothermal therapy with immune-adjuvant nanoparticles together with checkpoint blockade for effective cancer immunotherapy. Nat. Commun. 2016, 7, 13193. [Google Scholar] [CrossRef]
- Zhu, D.; Chen, H.; Huang, C.; Li, G.; Wang, X.; Jiang, W.; Fan, K. H2O2 Self-Producing Single-Atom Nanozyme Hydrogels as Light-Controlled Oxidative Stress Amplifier for Enhanced Synergistic Therapy by Transforming “Cold” Tumors. Adv. Funct. Mater. 2022, 32, 2110268. [Google Scholar] [CrossRef]
- Lyu, M.; Zhu, D.; Duo, Y.; Li, Y.; Quan, H. Bimetallic nanodots for tri-modal CT/MRI/PA imaging and hypoxia-resistant thermoradiotherapy in the NIR-II biological windows. Biomaterials 2019, 233, 119656. [Google Scholar] [CrossRef]
- Tang, M.; Huang, Y.; Liang, X.; Tao, Y.; He, N.; Li, Z.; Guo, J.; Gui, S. Sorafenib-Loaded PLGA-TPGS Nanosystems Enhance Hepatocellular Carcinoma Therapy Through Reversing P-Glycoprotein-Mediated Multidrug Resistance. AAPS PharmSciTech 2022, 23, 130. [Google Scholar] [CrossRef]
- Zhu, D.; Zheng, Z.; Luo, G.; Suo, M.; Li, X.; Duo, Y.; Tang, B.Z. Single injection and multiple treatments: An injectable nanozyme hydrogel as AIEgen reservoir and release controller for efficient tumor therapy. Nano Today 2021, 37, 101091. [Google Scholar] [CrossRef]
- Wu, H.; Liu, L.; Song, L.; Ma, M.; Gu, N.; Zhang, Y. Enhanced Tumor Synergistic Therapy by Injectable Magnetic Hydrogel Mediated Generation of Hyperthermia and Highly Toxic Reactive Oxygen Species. ACS Nano 2019, 13, 14013–14023. [Google Scholar] [CrossRef] [PubMed]
- Zhu, D.; Zhang, T.; Li, Y.; Huang, C.; Suo, M.; Xia, L.; Xu, Y.; Li, G.; Tang, B.Z. Tumor-derived exosomes co-delivering aggregation-induced emission luminogens and proton pump inhibitors for tumor glutamine starvation therapy and enhanced type-I photodynamic therapy. Biomaterials 2022, 283, 121462. [Google Scholar] [CrossRef] [PubMed]
- Li, K.; Lin, C.; Li, M.; Xu, K.; He, Y.; Mao, Y.; Lu, L.; Geng, W.; Li, X.; Luo, Z.; et al. Multienzyme-like Reactivity Cooperatively Impairs Glutathione Peroxidase 4 and Ferroptosis Suppressor Protein 1 Pathways in Triple-Negative Breast Cancer for Sensitized Ferroptosis Therapy. ACS Nano 2022, 16, 2381–2398. [Google Scholar] [CrossRef]
- Huang, C.; Liu, Z.; Chen, M.; Du, L.; Liu, C.; Wang, S.; Zheng, Y.; Liu, W. Tumor-derived biomimetic nanozyme with immune evasion ability for synergistically enhanced low dose radiotherapy. J. Nanobiotechnol. 2021, 19, 457. [Google Scholar] [CrossRef]
- Dong, Z.; Feng, L.; Chao, Y.; Hao, Y.; Chen, M.; Gong, F.; Han, X.; Zhang, R.; Cheng, L.; Liu, Z. Amplification of Tumor Oxidative Stresses with Liposomal Fenton Catalyst and Glutathione Inhibitor for Enhanced Cancer Chemotherapy and Radiotherapy. Nano Lett. 2018, 19, 805–815. [Google Scholar] [CrossRef]
- Song, G.; Liang, C.; Yi, X.; Zhao, Q.; Cheng, L.; Yang, K.; Liu, Z. Perfluorocarbon-Loaded Hollow Bi2Se3 Nanoparticles for Timely Supply of Oxygen under Near-Infrared Light to Enhance the Radiotherapy of Cancer. Adv. Mater. 2016, 28, 2716–2723. [Google Scholar] [CrossRef]
- Song, G.; Chao, Y.; Chen, Y.; Liang, C.; Yi, X.; Yang, G.; Yang, K.; Cheng, L.; Zhang, Q.; Liu, Z. All-in-One Theranostic Nanoplatform Based on Hollow TaOx for Chelator-Free Labeling Imaging, Drug Delivery, and Synergistically Enhanced Radiotherapy. Adv. Funct. Mater. 2016, 26, 8243–8254. [Google Scholar] [CrossRef]
- Yi, X.; Chen, L.; Zhong, X.; Gao, R.; Qian, Y.; Wu, F.; Song, G.; Chai, Z.; Liu, Z.; Yang, K. Core–shell Au@MnO2 nanoparticles for enhanced radiotherapy via improving the tumor oxygenation. Nano Res. 2016, 9, 3267–3278. [Google Scholar] [CrossRef]
- Zhu, D.; Lyu, M.; Huang, Q.; Suo, M.; Liu, Y.; Jiang, W.; Duo, Y.; Fan, K. Stellate Plasmonic Exosomes for Penetrative Targeting Tumor NIR-II Thermo-Radiotherapy. ACS Appl. Mater. Interfaces 2020, 12, 36928–36937. [Google Scholar] [CrossRef] [PubMed]
- Gong, L.; Xie, J.; Zhu, S.; Gu, Z.; Zhao, Y. Application of Multifunctional Nanomaterials in Tumor Radiosensitization. Acta Phys. Chim. Sin. 2018, 34, 140–167. [Google Scholar]






Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wang, Z.; Liu, B.; Tu, J.; Xiang, J.; Xiong, H.; Wu, Y.; Ding, S.; Zhu, D.; Zhu, D.; Liu, F.; et al. PLGA Nanoparticles Loaded with Sorafenib Combined with Thermosensitive Hydrogel System and Microwave Hyperthermia for Multiple Sensitized Radiotherapy. Pharmaceutics 2023, 15, 487. https://doi.org/10.3390/pharmaceutics15020487
Wang Z, Liu B, Tu J, Xiang J, Xiong H, Wu Y, Ding S, Zhu D, Zhu D, Liu F, et al. PLGA Nanoparticles Loaded with Sorafenib Combined with Thermosensitive Hydrogel System and Microwave Hyperthermia for Multiple Sensitized Radiotherapy. Pharmaceutics. 2023; 15(2):487. https://doi.org/10.3390/pharmaceutics15020487
Chicago/Turabian StyleWang, Ziqi, Bo Liu, Jingyao Tu, Jingfeng Xiang, Hui Xiong, Yue Wu, Shuaijie Ding, Daoming Zhu, Dongyong Zhu, Fei Liu, and et al. 2023. "PLGA Nanoparticles Loaded with Sorafenib Combined with Thermosensitive Hydrogel System and Microwave Hyperthermia for Multiple Sensitized Radiotherapy" Pharmaceutics 15, no. 2: 487. https://doi.org/10.3390/pharmaceutics15020487