
The Potential of Films as Transmucosal Drug Delivery Systems
 , , ,
, , ,
Abstract
:1. Introduction
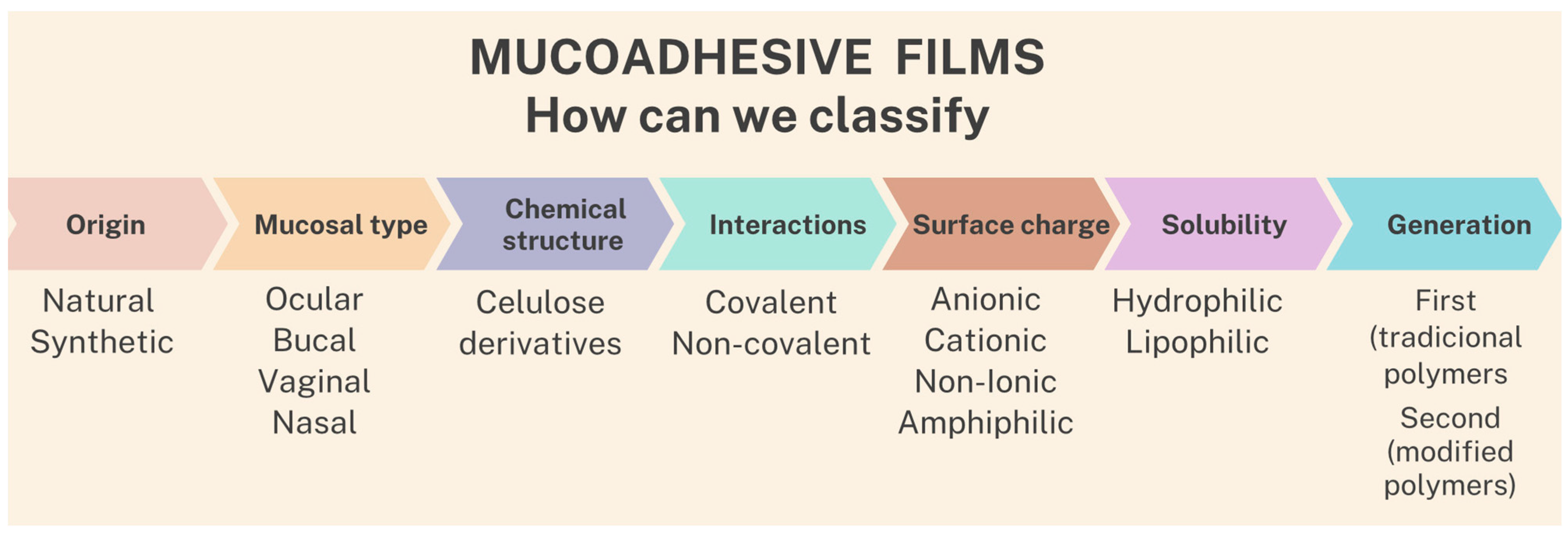
2. Classification of Films
2.1. Polymers
2.2. Plasticizers
3. Theories of Mucoadhesion Process
3.1. Absorption Theory
3.2. Electronic Theory
3.3. Fracture Theory
3.4. Wetting Theory
3.5. Diffusion Theory
4. Film Production Methods
4.1. Solvent Casting
4.2. Electrospinning
4.3. Hot-Melt Extrusion
4.4. Printing Technologies
4.4.1. Inkjet Printing
4.4.2. Three-Dimensional Printing
5. Different Routes of Administration and Applications
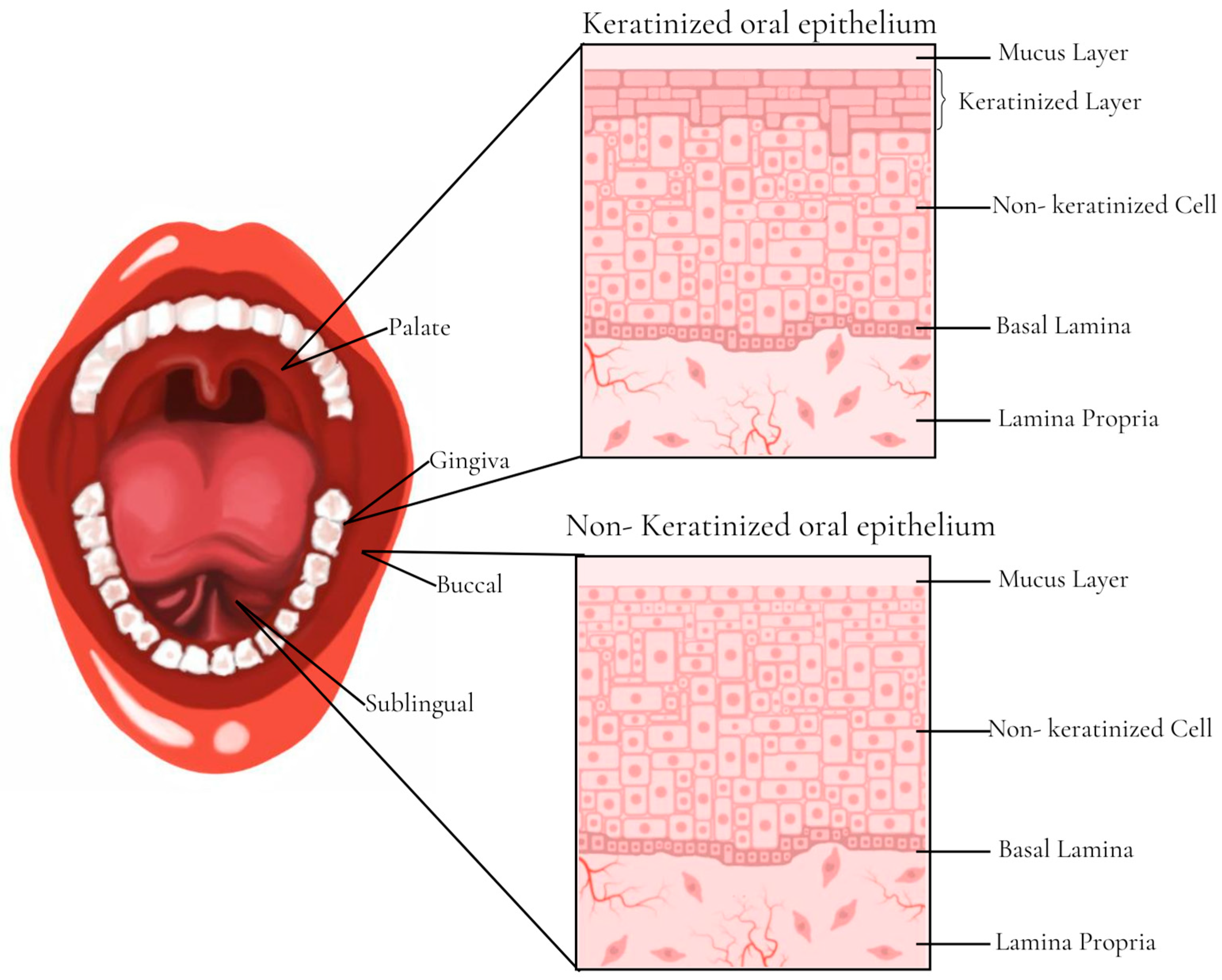
5.1. Buccal Films
5.1.1. Current Applications of Buccal Films
Fast-Dissolving Film of Levocetirizine Dihydrochloride
Mucoadhesive Film for Rizatriptan
Three-Dimensionally Printed Bilayer Mucoadhesive Buccal Film of Estradiol
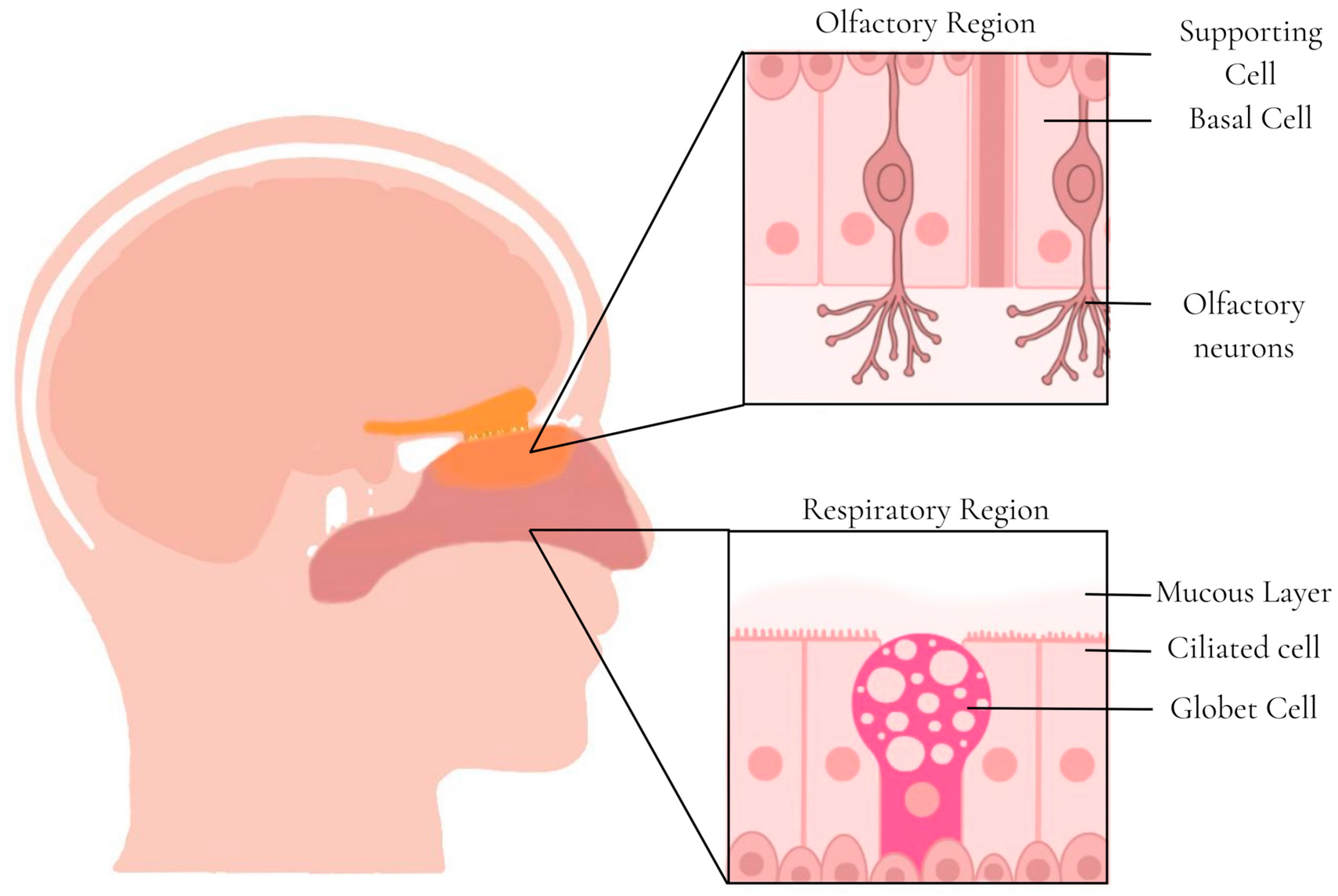
5.2. Nasal Films
5.2.1. Current Applications of Nasal Films
Mucoadhesive Nasal Film for Nose-to-Brain Delivery of Donezepil
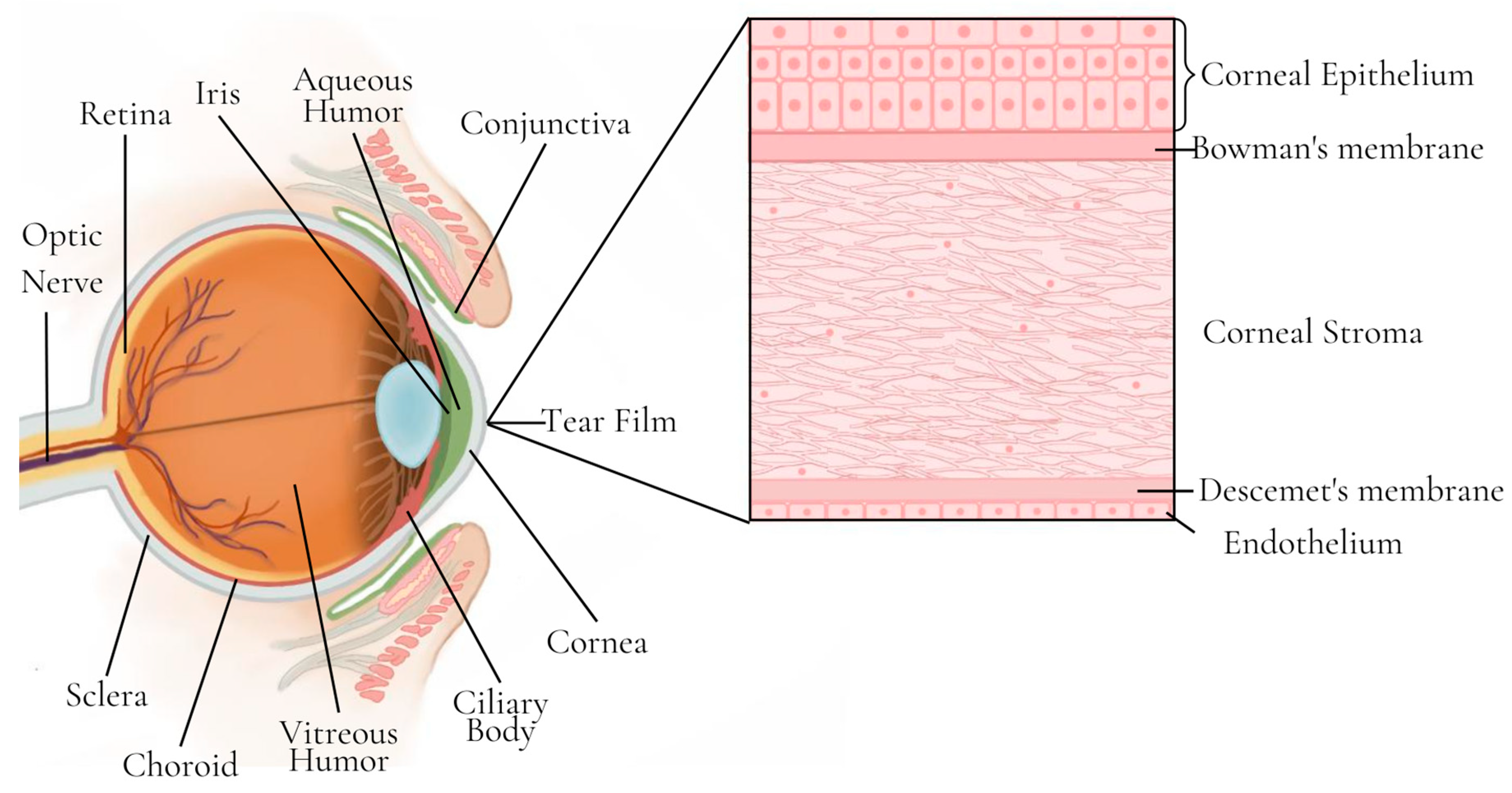
5.3. Ocular Films
Current Applications of Ocular Films
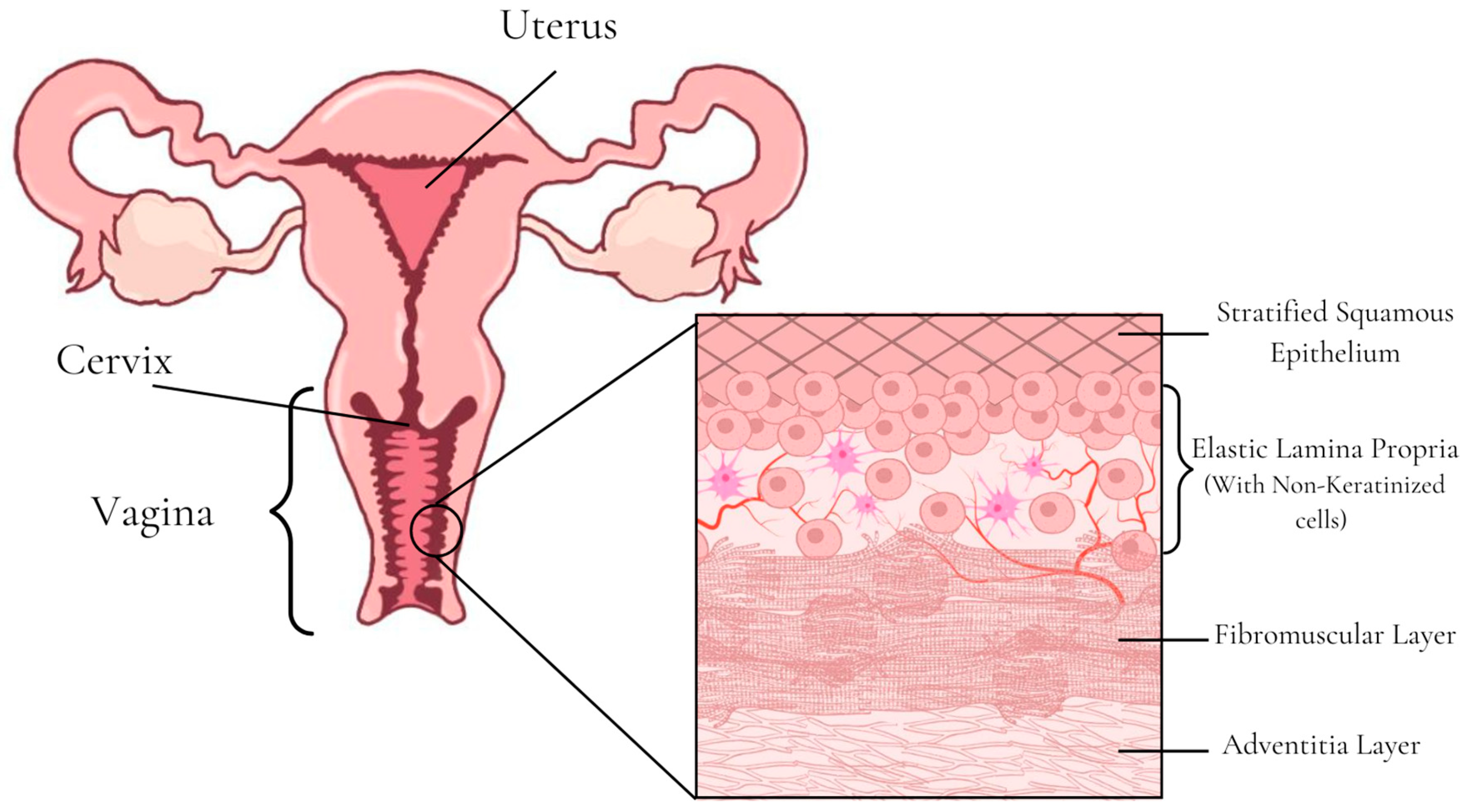
5.4. Vaginal Films
Current Applications of Vaginal Films
6. Final Considerations
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- Patil, H.; Tiwari, R.V.; Repka, M.A. Hot-Melt Extrusion: From Theory to Application in Pharmaceutical Formulation. AAPS PharmSciTech 2016, 17, 20–42. [Google Scholar] [CrossRef]
- Shipp, L.; Liu, F.; Kerai-Varsani, L.; Okwuosa, T.C. Buccal Films: A Review of Therapeutic Opportunities, Formulations & Relevant Evaluation Approaches. J. Control. Release 2022, 352, 1071–1092. [Google Scholar] [CrossRef]
- Morales, J.O.; McConville, J.T. Manufacture and Characterization of Mucoadhesive Buccal Films. Eur. J. Pharm. Biopharm. 2011, 77, 187–199. [Google Scholar] [CrossRef]
- Kumar, A.; Naik, P.K.; Pradhan, D.; Ghosh, G.; Rath, G. Mucoadhesive Formulations: Innovations, Merits, Drawbacks, and Future Outlook. Pharm. Dev. Technol. 2020, 25, 797–814. [Google Scholar] [CrossRef]
- Hombach, J.; Bernkop-Schnürch, A. Mucoadhesive Drug Delivery Systems. Handb. Exp. Pharmacol. 2010, 197, 251–266. [Google Scholar] [CrossRef]
- Bandi, S.P.; Bhatnagar, S.; Venuganti, V.V.K. Advanced Materials for Drug Delivery across Mucosal Barriers. Acta. Biomater. 2021, 119, 13–29. [Google Scholar] [CrossRef]
- Laffleur, F. Mucoadhesive Therapeutic Compositions: A Patent Review (2011–2014). Expert. Opin. Ther. Pat. 2016, 26, 377–388. [Google Scholar] [CrossRef]
- Tundisi, L.L.; Mostaço, G.B.; Carricondo, P.C.; Petri, D.F.S. Hydroxypropyl Methylcellulose: Physicochemical Properties and Ocular Drug Delivery Formulations. Eur. J. Pharm. Sci. 2021, 159, 105736. [Google Scholar] [CrossRef] [PubMed]
- Ghadermazi, R.; Hamdipour, S.; Sadeghi, K.; Ghadermazi, R.; Khosrowshahi Asl, A. Effect of Various Additives on the Properties of the Films and Coatings Derived from Hydroxypropyl Methylcellulose—A Review. Food Sci. Nutr. 2019, 7, 3363–3377. [Google Scholar]
- do Couto, R.O.; Cubayachi, C.; Calefi, P.L.; Lopez, R.F.V.; Pedrazzi, V.; De Gaitani, C.M.; de Freitas, O. Combining Amino Amide Salts in Mucoadhesive Films Enhances Needle-Free Buccal Anesthesia in Adults. J. Control. Release 2017, 266, 205–215. [Google Scholar] [CrossRef]
- do Couto, R.O.; Cubayachi, C.; Duarte, M.P.F.; Lopez, R.F.V.; Pedrazzi, V.; De Gaitani, C.M.; de Freitas, O. Towards the Advance of a Novel Iontophoretic Patch for Needle-Free Buccal Anesthesia. Mater. Sci. Eng. C 2021, 122, 111778. [Google Scholar] [CrossRef]
- Adami, L.E.; de Freitas, O.; de Figueiredo, F.A.T.; Ferreira, M.P.; Macedo, A.P.; Do Couto, R.O.; Pedrazzi, V. Needle-Free Anesthesia: Clinical Efficacy of a Mucoadhesive Patch for Atraumatic Anesthesia in Dental Procedures. Braz. Oral. Res. 2021, 35, e131. [Google Scholar] [CrossRef]
- Fefelova, N.A.; Nurkeeva, Z.S.; Mun, G.A.; Khutoryanskiy, V.V. Mucoadhesive Interactions of Amphiphilic Cationic Copolymers Based on [2-(Methacryloyloxy)Ethyl]Trimethylammonium Chloride. Int. J. Pharm. 2007, 339, 25–32. [Google Scholar] [CrossRef] [PubMed]
- Brannigan, R.P.; Khutoryanskiy, V.V. Progress and Current Trends in the Synthesis of Novel Polymers with Enhanced Mucoadhesive Properties. Macromol. Biosci. 2019, 19, e1900194. [Google Scholar] [CrossRef] [PubMed]
- Andrews, G.P.; Laverty, T.P.; Jones, D.S. Mucoadhesive Polymeric Platforms for Controlled Drug Delivery. Eur. J. Pharm. Biopharm. 2009, 71, 505–518. [Google Scholar] [CrossRef] [PubMed]
- Artursson, P.; Lindmark, T.; Davis, S.S.; Illum, L. Effect of Chitosan on the Permeability of Monolayers of Intestinal Epithelial Cells (Caco-2). Pharm. Res. 1994, 11, 1358–1361. [Google Scholar] [CrossRef]
- Lueßen Henrik, L.; de Leeuw, B.J.; Langemeÿer, M.W.E.; de Boer, A.G.; Verhoef, J.C.; Junginger, H.E. Mucoadhesive Polymers in Peroral Peptide Drug Delivery. VI. Carbomer and Chitosan Improve the Intestinal Absorption of the Peptide Drug Buserelin in Vivo. Pharm. Res. 1996, 13, 1668–1672. [Google Scholar] [CrossRef]
- Rinaudo, M. Chitin and Chitosan: Properties and Applications. Prog. Polym. Sci. 2006, 31, 603–632. [Google Scholar] [CrossRef]
- Guo, H.; Xu, W.; Chen, J.; Yan, L.; Ding, J.; Hou, Y.; Chen, X. Positively Charged Polypeptide Nanogel Enhances Mucoadhesion and Penetrability of 10-Hydroxycamptothecin in Orthotopic Bladder Carcinoma. J. Control. Release 2017, 259, 136–148. [Google Scholar] [CrossRef]
- Khutoryanskiy, V.V. Advances in Mucoadhesion and Mucoadhesive Polymers. Macromol. Biosci. 2011, 11, 748–764. [Google Scholar] [CrossRef]
- Clark, M.A.; Hirst, B.H.; Jepson, M.A. Lectin-Mediated Mucosal Delivery of Drugs and Microparticles. Adv. Drug Deliv. Rev. 2000, 43, 207–223. [Google Scholar] [CrossRef]
- Krull, S.M.; Patel, H.V.; Li, M.; Bilgili, E.; Davé, R.N. Critical Material Attributes (CMAs) of Strip Films Loaded with Poorly Water-Soluble Drug Nanoparticles: I. Impact of Plasticizer on Film Properties and Dissolution. Eur. J. Pharm. Sci. 2016, 92, 146–155. [Google Scholar] [CrossRef]
- Ili Balqis, A.M.; Nor Khaizura, M.A.R.; Russly, A.R.; Nur Hanani, Z.A. Effects of Plasticizers on the Physicochemical Properties of Kappa-Carrageenan Films Extracted from Eucheuma Cottonii. Int. J. Biol. Macromol. 2017, 103, 721–732. [Google Scholar] [CrossRef]
- Gao, C.; Pollet, E.; Avérous, L. Innovative Plasticized Alginate Obtained by Thermo-Mechanical Mixing: Effect of Different Biobased Polyols Systems. Carbohydr. Polym. 2017, 157, 669–676. [Google Scholar] [CrossRef] [PubMed]
- Panda, B.; Parihar, A.S.; Mallick, S. Effect of Plasticizer on Drug Crystallinity of Hydroxypropyl Methylcellulose Matrix Film. Int. J. Biol. Macromol. 2014, 67, 295–302. [Google Scholar] [CrossRef] [PubMed]
- Gal, A.; Nussinovitch, A. Plasticizers in the Manufacture of Novel Skin-Bioadhesive Patches. Int. J. Pharm. 2009, 370, 103–109. [Google Scholar] [CrossRef]
- Sun, Y.; Liu, Z.; Zhang, L.; Wang, X.; Li, L. Effects of Plasticizer Type and Concentration on Rheological, Physico-Mechanical and Structural Properties of Chitosan/Zein Film. Int. J. Biol. Macromol. 2020, 143, 334–340. [Google Scholar] [CrossRef] [PubMed]
- Rohani Shirvan, A.; Hemmatinejad, N.; Bahrami, S.H.; Bashari, A. Fabrication of Multifunctional Mucoadhesive Buccal Patch for Drug Delivery Applications. J. Biomed. Mater. Res. A 2021, 109, 2640–2656. [Google Scholar] [CrossRef]
- Swain, R.; Moharana, A.; Habibullah, S.; Nandi, S.; Bose, A.; Mohapatra, S.; Mallick, S. Ocular Delivery of Felodipine for the Management of Intraocular Pressure and Inflammation: Effect of Film Plasticizer and in Vitro in Vivo Evaluation. Int. J. Pharm. 2023, 642, 123153. [Google Scholar] [CrossRef]
- Notario-Pérez, F.; Cazorla-Luna, R.; Martín-Illana, A.; Galante, J.; Ruiz-Caro, R.; das Neves, J.; Veiga, M.D. Design, Fabrication and Characterisation of Drug-Loaded Vaginal Films: State-of-the-Art. J. Control. Release 2020, 327, 477–499. [Google Scholar] [CrossRef]
- Martín-Illana, A.; Cazorla-Luna, R.; Notario-Pérez, F.; Rubio, J.; Ruiz-Caro, R.; Tamayo, A.; Veiga, M.D. Eudragit®® L100/Chitosan Composite Thin Bilayer Films for Intravaginal PH-Responsive Release of Tenofovir. Int. J. Pharm. 2022, 616, 121554. [Google Scholar] [CrossRef]
- Nandi, S.; Ojha, A.; Nanda, A.; Sahoo, R.N.; Swain, R.; Pattnaik, K.P.; Mallick, S. Vildagliptin Platicized Hydrogel Film in the Control of Ocular Inflammation after Topical Application: Study of Hydration and Erosion Behaviour. Z. Für Phys. Chem. 2021, 236, 275–290. [Google Scholar] [CrossRef]
- Do Couto, R.O.; Sommerfeld, S.D.; Dube, K.; De Freitas, O.; Kohn, J. Preliminarily Development of a Moisture-Activated Bioresorbable Polymeric Platform for Drug Delivery. Quim. Nova 2015, 38, 902–909. [Google Scholar] [CrossRef]
- Ferreira, L.F.M.; Thomaz, D.V.; Duarte, M.P.F.; Lopez, R.F.V.; Pedrazzi, V.; de Freitas, O.; Do Couto, R.O. Quality by Design-Driven Investigation of the Mechanical Properties of Mucoadhesive Films for Needleless Anesthetics Administration. Rev. De Cienc. Farm. Basica E Apl. 2021, 42, e707. [Google Scholar] [CrossRef]
- Liu, D.; Jiang, P.; Nie, Z.; Wang, H.; Dai, Z.; Deng, J.; Cao, Z. Synthesis of an Efficient Bio-Based Plasticizer Derived from Waste Cooking Oil and Its Performance Testing in PVC. Polym. Test. 2020, 90, 106625. [Google Scholar] [CrossRef]
- Calvo, N.L.; Tejada, G.; Svetaz, L.A.; Quiroga, A.D.; Alvarez, V.A.; Lamas, M.C.; Leonardi, D. Development and Optimization of a New Tioconazole Vaginal Mucoadhesive Film Using an Experimental Design Strategy. Physicochemical and Biological Characterization. J. Pharm. Biomed. Anal. 2021, 205, 114303. [Google Scholar] [CrossRef] [PubMed]
- Smart, J.D. The Basics and Underlying Mechanisms of Mucoadhesion. Adv. Drug Deliv. Rev. 2005, 57, 1556–1568. [Google Scholar] [CrossRef]
- Shaikh, R.; Raj Singh, T.; Garland, M.; Woolfson, A.; Donnelly, R. Mucoadhesive Drug Delivery Systems. J. Pharm. Bioallied. Sci. 2011, 3, 89–100. [Google Scholar] [CrossRef] [PubMed]
- Alaei, S.; Omidian, H. Mucoadhesion and Mechanical Assessment of Oral Films. Eur. J. Pharm. Sci. 2021, 159, 105727. [Google Scholar] [CrossRef]
- Bagan, J.; Paderni, C.; Termine, N.; Campisi, G.; Lo Russo, L.; Compilato, D.; Fede, O. Di Mucoadhesive Polymers for Oral Transmucosal Drug Delivery: A Review. Curr. Pharm. Des. 2012, 18, 5497–5514. [Google Scholar] [CrossRef]
- Manohar, S.D.; Sridhar, D.A.; Mallikarjuna, S.C. Drug Delivery from the Oral Cavity: A Focus on Mucoadhesive Buccal Drug Delivery Systems. PDA J. Pharm. Sci. Technol. 2012, 66, 466–500. [Google Scholar] [CrossRef]
- Jawadi, Z.; Yang, C.; Haidar, Z.S.; Santa Maria, P.L.; Massa, S. Bio-Inspired Muco-Adhesive Polymers for Drug Delivery Applications. Polymers 2022, 14, 5459. [Google Scholar] [CrossRef]
- Dodou, D.; Breedveld, P.; Wieringa, P.A. Mucoadhesives in the Gastrointestinal Tract: Revisiting the Literature for Novel Applications. Eur. J. Pharm. Biopharm. 2005, 60, 1–16. [Google Scholar] [CrossRef]
- Roy, S.; Pal, K.; Anis, A.; Pramanik, K.; Prabhakar, B. Polymers in Mucoadhesive Drug-Delivery Systems: A Brief Note. Des. Monomers Polym. 2009, 12, 483–495. [Google Scholar] [CrossRef]
- Lee, J.W.; Park, J.H.; Robinson, J.R. Bioadhesive-Based Dosage Forms: The Next Generation. J. Pharm. Sci. 2000, 89, 850–866. [Google Scholar] [CrossRef]
- Boddupalli, B.M.; Mohammed, Z.N.K.; Nath, A.R.; Banji, D. Mucoadhesive Drug Delivery System: An Overview. J. Adv. Pharm. Technol. Res. 2010, 1, 381–387. [Google Scholar] [CrossRef]
- Ugwoke, M.I.; Agu, R.U.; Verbeke, N.; Kinget, R. Nasal Mucoadhesive Drug Delivery: Background, Applications, Trends and Future Perspectives. Adv. Drug Deliv. Rev. 2005, 57, 1640–1665. [Google Scholar] [CrossRef]
- Edsman, K.; Hägerström, H. Pharmaceutical Applications of Mucoadhesion for the Non-Oral Routes. J. Pharm. Pharmacol. 2010, 57, 3–22. [Google Scholar] [CrossRef]
- Musazzi, U.M.; Khalid, G.M.; Selmin, F.; Minghetti, P.; Cilurzo, F. Trends in the Production Methods of Orodispersible Films. Int. J. Pharm. 2020, 576, 118963. [Google Scholar] [CrossRef]
- Eleftheriadis, G.K.; Ritzoulis, C.; Bouropoulos, N.; Tzetzis, D.; Andreadis, D.A.; Boetker, J.; Rantanen, J.; Fatouros, D.G. Unidirectional Drug Release from 3D Printed Mucoadhesive Buccal Films Using FDM Technology: In Vitro and Ex Vivo Evaluation. Eur. J. Pharm. Biopharm. 2019, 144, 180–192. [Google Scholar] [CrossRef]
- Kataria, K.; Gupta, A.; Rath, G.; Mathur, R.B.; Dhakate, S.R. In Vivo Wound Healing Performance of Drug Loaded Electrospun Composite Nanofibers Transdermal Patch. Int. J. Pharm. 2014, 469, 102–110. [Google Scholar] [CrossRef]
- Zhou, Y.; Wang, M.; Yan, C.; Liu, H.; Yu, D.G. Advances in the Application of Electrospun Drug-Loaded Nanofibers in the Treatment of Oral Ulcers. Biomolecules 2022, 12, 1254. [Google Scholar] [CrossRef]
- Nadaf, A.; Gupta, A.; Hasan, N.; Fauziya, N.; Ahmad, S.; Kesharwani, P.; Ahmad, F.J. Recent Update on Electrospinning and Electrospun Nanofibers: Current Trends and Their Applications. RSC Adv. 2022, 12, 23808–23828. [Google Scholar] [CrossRef]
- Omari, S.; Ashour, E.A.; Elkanayati, R.; Alyahya, M.; Almutairi, M.; Repka, M.A. Formulation Development of Loratadine Immediate- Release Tablets Using Hot-Melt Extrusion and 3D Printing Technology. J. Drug Deliv. Sci. Technol. 2022, 74, 103505. [Google Scholar] [CrossRef]
- Bandari, S.; Nyavanandi, D.; Dumpa, N.; Repka, M.A. Coupling Hot Melt Extrusion and Fused Deposition Modeling: Critical Properties for Successful Performance. Adv. Drug Deliv. Rev. 2021, 172, 52–63. [Google Scholar] [CrossRef] [PubMed]
- Tian, Y.; Orlu, M.; Woerdenbag, H.J.; Scarpa, M.; Kiefer, O.; Kottke, D.; Sjöholm, E.; Öblom, H.; Sandler, N.; Hinrichs, W.L.J.; et al. Oromucosal Films: From Patient Centricity to Production by Printing Techniques. Expert Opin. Drug Deliv. 2019, 16, 981–993. [Google Scholar] [CrossRef]
- Elkasabgy, N.A.; Mahmoud, A.A.; Maged, A. 3D Printing: An Appealing Route for Customized Drug Delivery Systems. Int. J. Pharm. 2020, 588, 119732. [Google Scholar] [CrossRef]
- Sofi, H.S.; Abdal-hay, A.; Ivanovski, S.; Zhang, Y.S.; Sheikh, F.A. Electrospun Nanofibers for the Delivery of Active Drugs through Nasal, Oral and Vaginal Mucosa: Current Status and Future Perspectives. Mater. Sci. Eng. C 2020, 111, 110756. [Google Scholar] [CrossRef]
- De Caro, V.; Angellotti, G.; D’Agostino, F.; Di Prima, G. Buccal Thin Films as Potent Permeation Enhancers for Cytisine Transbuccal Delivery. Membranes 2022, 12, 1169. [Google Scholar] [CrossRef] [PubMed]
- Gaber, D.A.; Alburaykan, A.I.; Alruthea, L.M.; Aldohan, N.S.; Alharbi, R.F.; Aljohani, A.R.; Albilaihi, H.M.; Adogim, S.S. Development, in Vitro Evaluation, and in Vivo Study of Adhesive Buccal Films for the Treatment of Diabetic Pediatrics via Trans Mucosal Delivery of Gliclazide. Drug Des. Dev. Ther. 2022, 16, 4235–4250. [Google Scholar] [CrossRef]
- Nair, A.B.; Shah, J.; Jacob, S.; Al-Dhubiab, B.E.; Patel, V.; Sreeharsha, N.; Shinu, P. Development of Mucoadhesive Buccal Film for Rizatriptan: In Vitro and in Vivo Evaluation. Pharmaceutics 2021, 13, 728. [Google Scholar] [CrossRef]
- Kristó, K.; Módra, S.; Hornok, V.; Süvegh, K.; Ludasi, K.; Aigner, Z.; Kelemen, A.; Sovány, T.; Pintye-Hódi, K.; Regdon, G. Investigation of Surface Properties and Free Volumes of Chitosan-Based Buccal Mucoadhesive Drug Delivery Films Containing Ascorbic Acid. Pharmaceutics 2022, 14, 345. [Google Scholar] [CrossRef]
- Edmans, J.G.; Clitherow, K.H.; Murdoch, C.; Hatton, P.V.; Spain, S.G.; Colley, H.E. Mucoadhesive Electrospun Fibre-Based Technologies for Oral Medicine. Pharmaceutics 2020, 12, 504. [Google Scholar] [CrossRef] [PubMed]
- Şenel, S. An Overview of Physical, Microbiological and Immune Barriers of Oral Mucosa. Int. J. Mol. Sci. 2021, 22. [Google Scholar]
- Samiei, M.; Ahmadian, E.; Eftekhari, A.; Eghbal, M.A.; Rezaie, F.; Vinken, M. Cell Junctions and Oral Health. EXCLI J. 2019, 18, 317–330. [Google Scholar] [CrossRef]
- Groeger, S.; Meyle, J. Oral Mucosal Epithelial Cells. Front. Immunol. 2019, 10, 208. [Google Scholar] [CrossRef]
- Wan, H.; Gadmor, H.; Brown, L. Cell-Cell Interactions in the Oral Mucosa: Tight Junctions and Gap Junctions. In Oral Mucosa in Health and Disease: A Concise Handbook; Springer International Publishing: Cham, Switzerland, 2018; pp. 19–30. ISBN 9783319560656. [Google Scholar]
- Rübsam, M.; Broussard, J.A.; Wickström, S.A.; Nekrasova, O.; Green, K.J.; Niessen, C.M. Adherens Junctions and Desmosomes Coordinate Mechanics and Signaling to Orchestrate Tissue Morphogenesis and Function: An Evolutionary Perspective. Cold Spring Harb. Perspect. Biol. 2018, 10, a029207. [Google Scholar] [CrossRef]
- Batista, P.; Castro, P.; Madureira, A.R.; Sarmento, B.; Pintado, M. Development and Characterization of Chitosan Microparticles-in-Films for Buccal Delivery of Bioactive Peptides. Pharmaceuticals 2019, 12, 32. [Google Scholar] [CrossRef]
- Gandhi, N.V.; Deokate, U.A.; Angadi, S.S. Formulation, Optimization and Evaluation of Nanoparticulate Oral Fast Dissolving Film Dosage Form of Nitrendipine. AAPS PharmSciTech 2021, 22, 218. [Google Scholar] [CrossRef]
- Citra Rani, K.; Parfati, N.; Luh Dewi Aryani, N.; Nuniek Winantari, A.; Wahyu Fitriani, E.; Trias Pradana, A.; Nawatila, R.; Rizky Putranti, A.; Irine, F.; Angelica, F.; et al. Development, Evaluation, and Molecular Docking of Oral Dissolving Film of Atenolol. Pharmaceutics 2021, 13, 1727. [Google Scholar] [CrossRef]
- Jovanović, M.; Petrović, M.; Cvijić, S.; Tomić, N.; Stojanović, D.; Ibrić, S.; Uskoković, P. 3D Printed Buccal Films for Prolonged-Release of Propranolol Hydrochloride: Development, Characterization and Bioavailability Prediction. Pharmaceutics 2021, 13, 2143. [Google Scholar] [CrossRef]
- Castro, P.M.; Baptista, P.; Madureira, A.R.; Sarmento, B.; Pintado, M.E. Combination of PLGA Nanoparticles with Mucoadhesive Guar-Gum Films for Buccal Delivery of Antihypertensive Peptide. Int. J. Pharm. 2018, 547, 593–601. [Google Scholar] [CrossRef]
- Mady, O.Y.; Abulmeaty, M.M.A.; Donia, A.A.; Al-Khureif, A.A.; Al-Shoubki, A.A.; Abudawood, M.; Moety, D.A.A. Formulation and Bioavailability of Novel Mucoadhesive Buccal Films for Candesartan Cilexetil in Rats. Membranes 2021, 11, 659. [Google Scholar] [CrossRef]
- Rezaee, F.; Ganji, F. Formulation, Characterization, and Optimization of Captopril Fast-Dissolving Oral Films. AAPS PharmSciTech 2018, 19, 2203–2212. [Google Scholar] [CrossRef]
- Dalal, R.; Shah, J.; Gorain, B.; Choudhury, H.; Jacob, S.; Mehta, T.A.; Shah, H.; Nair, A.B. Development and Optimization of Asenapine Sublingual Film Using QbD Approach. AAPS PharmSciTech 2021, 22, 244. [Google Scholar] [CrossRef]
- Elshafeey, A.H.; El-Dahmy, R.M. Formulation and Development of Oral Fast-Dissolving Films Loaded with Nanosuspension to Augment Paroxetine Bioavailability: In Vitro Characterization, Ex Vivo Permeation, and Pharmacokinetic Evaluation in Healthy Human Volunteers. Pharmaceutics 2021, 13, 1869. [Google Scholar] [CrossRef] [PubMed]
- Mann, G.; Gurave, P.M.; Kaul, A.; Kadiyala, K.G.; Pokhriyal, M.; Srivastava, R.K.; Kumar, A.; Datta, A. Polymeric and Electrospun Patches for Drug Delivery through Buccal Route: Formulation and Biointerface Evaluation. J. Drug Deliv. Sci. Technol. 2022, 68, 103030. [Google Scholar] [CrossRef]
- El Sharawy, A.M.; Shukr, M.H.; Elshafeey, A.H. Formulation and Optimization of Duloxetine Hydrochloride Buccal Films: In Vitro and in Vivo Evaluation. Drug. Deliv. 2017, 24, 1762–1769. [Google Scholar] [CrossRef]
- Alkahtani, M.E.; Aodah, A.H.; Abu Asab, O.A.; Basit, A.W.; Orlu, M.; Tawfik, E.A. Fabrication and Characterization of Fast-Dissolving Films Containing Escitalopram/Quetiapine for the Treatment of Major Depressive Disorder. Pharmaceutics 2021, 13, 891. [Google Scholar] [CrossRef]
- Prajapati, V.D.; Chaudhari, A.M.; Gandhi, A.K.; Maheriya, P. Pullulan Based Oral Thin Film Formulation of Zolmitriptan: Development and Optimization Using Factorial Design. Int. J. Biol. Macromol. 2018, 107, 2075–2085. [Google Scholar] [CrossRef]
- Salama, A.H.; Basha, M.; Salama, A.A.A. Micellar Buccal Film for Safe and Effective Control of Seizures: Preparation, in Vitro Characterization, Ex Vivo Permeation Studies and in Vivo Assessment. Eur. J. Pharm. Sci. 2021, 166, 105978. [Google Scholar] [CrossRef]
- Salehi, S.; Boddohi, S. Design and Optimization of Kollicoat®® IR Based Mucoadhesive Buccal Film for Co-Delivery of Rizatriptan Benzoate and Propranolol Hydrochloride. Mater. Sci. Eng. C 2019, 97, 230–244. [Google Scholar] [CrossRef] [PubMed]
- Shah, K.A.; Li, G.; Song, L.; Gao, B.; Huang, L.; Luan, D.; Iqbal, H.; Cao, Q.; Menaa, F.; Lee, B.J.; et al. Rizatriptan-Loaded Oral Fast Dissolving Films: Design and Characterizations. Pharmaceutics 2022, 14, 2687. [Google Scholar] [CrossRef] [PubMed]
- Siddique, W.; Zaman, M.; Sarfraz, R.M.; Butt, M.H.; Rehman, A.U.; Fassih, N.; Albadrani, G.M.; Bayram, R.; Alfaifi, M.Y.; Abdel-Daim, M.M. The Development of Eletriptan Hydrobromide Immediate Release Buccal Films Using Central Composite Rotatable Design: An In Vivo and In Vitro Approach. Polymers 2022, 14, 3981. [Google Scholar] [CrossRef] [PubMed]
- Anita, L.; Kanni, P.; Ramnarayanan, C.; Karki, R.; Komarla, N.P.; Janadri, S. Extraction, Purification, and Development of Sublingual Film (SLIT Films) Comprising Cockroach Allergen for Treatment of Allergy. Curr. Drug Deliv. 2022, 20, 807–817. [Google Scholar] [CrossRef]
- Islam, N.; Irfan, M.; Khan, S.U.D.; Syed, H.K.; Iqbal, M.S.; Khan, I.U.; Mahdy, A.; Raafat, M.; Hossain, M.A.; Inam, S.; et al. Poloxamer-188 and d-α-Tocopheryl Polyethylene Glycol Succinate (Tpgs-1000) Mixed Micelles Integrated Orodispersible Sublingual Films to Improve Oral Bioavailability of Ebastine in Vitro and in Vivo Characterization. Pharmaceutics 2021, 13, 54. [Google Scholar] [CrossRef]
- Pamlényi, K.; Kristó, K.; Jójárt-Laczkovich, O.; Regdon, G., Jr. Formulation and Optimization of Sodium Alginate Polymer Film as a Buccal Mucoadhesive Drug Delivery System Containing Cetirizine Dihydrochloride. Pharmaceutics 2021, 13, 619. [Google Scholar] [CrossRef]
- Zayed, G.M.; El Rasoul, S.A.; Ibrahim, M.A.; Saddik, M.S.; Alshora, D.H. In Vitro and in Vivo Characterization of Domperidone-Loaded Fast Dissolving Buccal Films. Saudi Pharm. J. 2020, 28, 266–273. [Google Scholar] [CrossRef]
- Al-Kubati, S.S.; Ahmed, M.A.; Emad, N.A. Palatable Levocetirizine Dihydrochloride Solid Dispersed Fast-Dissolving Films: Formulation and In Vitro and In Vivo Characterization. Sci. World J. 2022, 2022, 1552602. [Google Scholar] [CrossRef]
- Jadhav, Y.G.; Galgatte, U.C.; Chaudhari, P.D. Overcoming Poor Solubility of Dimenhydrinate: Development, Optimization and Evaluation of Fast Dissolving Oral Film. Adv. Pharm. Bull. 2018, 8, 721–725. [Google Scholar] [CrossRef]
- Moonesan, M.; Ganji, F.; Soroushnia, A.; Bagheri, F. Fast-Dissolving Oral Films Containing Dextromethorphan/Phenylephrine for Sinusitis Treatment: Formulation, Characterization and Optimization. Prog. Biomater. 2022, 11, 243–252. [Google Scholar] [CrossRef]
- Thakkar, S.; More, N.; Sharma, D.; Kapusetti, G.; Kalia, K.; Misra, M. Fast Dissolving Electrospun Polymeric Films of Anti-Diabetic Drug Repaglinide: Formulation and Evaluation. Drug Dev. Ind. Pharm. 2019, 45, 1921–1930. [Google Scholar] [CrossRef]
- Khames, A. Hexyl Alginate Derivative, an Amphiphilic Innovative Buccal Film-Forming Material of Promising Mechanical and Release Characteristics for the Improvement of Repaglinide Bioavailability. Drug Des. Dev. Ther. 2019, 13, 925–940. [Google Scholar] [CrossRef]
- Abdella, S.; Afinjuomo, F.; Song, Y.; Upton, R.; Garg, S. 3D Printed Bilayer Mucoadhesive Buccal Film of Estradiol: Impact of Design on Film Properties, Release Kinetics and Predicted in Vivo Performance. Int. J. Pharm. 2022, 628, 122324. [Google Scholar] [CrossRef]
- El-Helaly, S.N.; Abd-Elrasheed, E.; Salim, S.A.; Fahmy, R.H.; Salah, S.; El-Ashmoony, M.M. Green Nanotechnology in the Formulation of a Novel Solid Dispersed Multilayered Core-Sheath Raloxifene-Loaded Nanofibrous Buccal Film; in Vitro and in Vivo Characterization. Pharmaceutics 2021, 13, 474. [Google Scholar] [CrossRef]
- Abou-taleb, H.A.; Mustafa, W.W.; Makram, T.S.; Abdelaty, L.N.; Salem, H.; Abdelkader, H. Vardenafil Oral Dispersible Films (ODFs) with Advanced Dissolution, Palatability, and Bioavailability. Pharmaceutics 2022, 14, 517. [Google Scholar] [CrossRef]
- Adeleke, O.A.; Tsai, P.C.; Karry, K.M.; Monama, N.O.; Michniak-Kohn, B.B. Isoniazid-Loaded Orodispersible Strips: Methodical Design, Optimization and in Vitro-in Silico Characterization. Int. J. Pharm. 2018, 547, 347–359. [Google Scholar] [CrossRef]
- AnjiReddy, K.; Karpagam, S. Hyperbranched Cellulose Polyester of Oral Thin Film and Nanofiber for Rapid Release of Donepezil; Preparation and in Vivo Evaluation. Int. J. Biol. Macromol. 2019, 124, 871–887. [Google Scholar] [CrossRef]
- Rodrigues, D.A.; Miguel, S.P.; Loureiro, J.; Ribeiro, M.; Roque, F.; Coutinho, P. Oromucosal Alginate Films with Zein Nanoparticles as a Novel Delivery System for Digoxin. Pharmaceutics 2021, 13, 30. [Google Scholar] [CrossRef]
- He, S.; Radeke, C.; Jacobsen, J.; Lind, J.U.; Mu, H. Multi-Material 3D Printing of Programmable and Stretchable Oromucosal Patches for Delivery of Saquinavir. Int. J. Pharm. 2021, 610, 121236. [Google Scholar] [CrossRef]
- Breithaupt, M.H.; Krohmer, E.; Taylor, L.; Koerner, E.; Hoppe-Tichy, T.; Burhenne, J.; Foerster, K.I.; Dachtler, M.; Huber, G.; Venkatesh, R.; et al. Oral Bioavailability of Microdoses and Therapeutic Doses of Midazolam as a 2-Dimensionally Printed Orodispersible Film in Healthy Volunteers. Eur. J. Clin. Pharmacol. 2022, 78, 1965–1972. [Google Scholar] [CrossRef]
- Ulusoy, S.; Bayar Muluk, S.; Karpischenko, S.; Passali, G.C.; Negm, H.; Passali, D.; Milkov, M.; Kopacheva-Barsova, G.; Konstantinidis, I.; Dilber, M.; et al. Mechanisms and Solutions for Nasal Drug Delivery—A Narrative Review. Eur. Rev. Med. Pharmacol. Sci. 2022, 26, 72–81. [Google Scholar] [CrossRef] [PubMed]
- Erdő, F.; Bors, L.A.; Farkas, D.; Bajza, Á.; Gizurarson, S. Evaluation of Intranasal Delivery Route of Drug Administration for Brain Targeting. Brain Res. Bull. 2018, 143, 155–170. [Google Scholar] [CrossRef] [PubMed]
- Lobaina Mato, Y. Nasal Route for Vaccine and Drug Delivery: Features and Current Opportunities. Int. J. Pharm. 2019, 572, 118813. [Google Scholar] [CrossRef]
- Crowe, T.P.; Greenlee, M.H.W.; Kanthasamy, A.G.; Hsu, W.H. Mechanism of Intranasal Drug Delivery Directly to the Brain. Life. Sci. 2018, 195, 44–52. [Google Scholar] [CrossRef]
- Inoue, D.; Yamashita, A.; To, H. Formulation and In Vitro Characterization of a Vacuum-Dried Drug–Polymer Thin Film for Intranasal Application. Polymers 2022, 14, 2954. [Google Scholar] [CrossRef]
- Papakyriakopoulou, P.; Rekkas, D.M.; Colombo, G.; Valsami, G. Development and In Vitro-Ex Vivo Evaluation of Novel Polymeric Nasal Donepezil Films for Potential Use in Alzheimer’s Disease Using Experimental Design. Pharmaceutics 2022, 14, 1742. [Google Scholar] [CrossRef]
- Kaikousidis, C.; Papakyriakopoulou, P.; Dokoumetzidis, A.; Valsami, G. Donepezil Brain and Blood Pharmacokinetic Modeling after Nasal Film and Oral Solution Administration in Mice. Pharmaceutics 2023, 15, 1409. [Google Scholar] [CrossRef]
- Mohamad, S.A.; Badawi, A.M.; Mansour, H.F. Insulin Fast-Dissolving Film for Intranasal Delivery via Olfactory Region, a Promising Approach for the Treatment of Anosmia in COVID-19 Patients: Design, in-Vitro Characterization and Clinical Evaluation. Int. J. Pharm. 2021, 601, 120600. [Google Scholar] [CrossRef]
- Göttel, B.; de Souza e Silva, J.M.; Santos de Oliveira, C.; Syrowatka, F.; Fiorentzis, M.; Viestenz, A.; Viestenz, A.; Mäder, K. Electrospun Nanofibers—A Promising Solid in-Situ Gelling Alternative for Ocular Drug Delivery. Eur. J. Pharm. Biopharm. 2020, 146, 125–132. [Google Scholar] [CrossRef] [PubMed]
- Aulton, M.E.; Taylor, K.M.G. Aulton Pharmaceutics—The Design and Manufacture of Medicines, 4th ed.; Elsevier: Beijing, China, 2013. [Google Scholar]
- Cegielska, O.; Sierakowski, M.; Sajkiewicz, P.; Lorenz, K.; Kogermann, K. Mucoadhesive Brinzolamide-Loaded Nanofibers for Alternative Glaucoma Treatment. Eur. J. Pharm. Biopharm. 2022, 180, 48–62. [Google Scholar] [CrossRef] [PubMed]
- Tighsazzadeh, M.; Mitchell, J.C.; Boateng, J.S. Development and Evaluation of Performance Characteristics of Timolol-Loaded Composite Ocular Films as Potential Delivery Platforms for Treatment of Glaucoma. Int. J. Pharm. 2019, 566, 111–125. [Google Scholar] [CrossRef] [PubMed]
- Andreadis, I.I.; Karavasili, C.; Thomas, A.; Komnenou, A.; Tzimtzimis, M.; Tzetzis, D.; Andreadis, D.; Bouropoulos, N.; Fatouros, D.G. In Situ Gelling Electrospun Ocular Films Sustain the Intraocular Pressure-Lowering Effect of Timolol Maleate: In Vitro, Ex Vivo, and Pharmacodynamic Assessment. Mol. Pharm. 2022, 19, 274–286. [Google Scholar] [CrossRef] [PubMed]
- Gandara-Loe, J.; Souza, B.E.; Missyul, A.; Giraldo, G.; Tan, J.C.; Silvestre-Albero, J. MOF-Based Polymeric Nanocomposite Films as Potential Materials for Drug Delivery Devices in Ocular Therapeutics. ACS Appl. Mater. Interfaces 2020, 12, 30189–30197. [Google Scholar] [CrossRef] [PubMed]
- Tatke, A.; Dudhipala, N.; Janga, K.Y.; Soneta, B.; Avula, B.; Majumdar, S. Melt-Cast Films Significantly Enhance Triamcinolone Acetonide Delivery to the Deeper Ocular Tissues. Pharmaceutics 2019, 11, 158. [Google Scholar] [CrossRef]
- Da Silva, G.R.; Lima, T.H.; Fernandes-Cunha, G.M.; Oréfice, R.L.; Da Silva-Cunha, A.; Zhao, M.; Behar-Cohen, F. Ocular Biocompatibility of Dexamethasone Acetate Loaded Poly(ɛ-Caprolactone) Nanofibers. Eur. J. Pharm. Biopharm. 2019, 142, 20–30. [Google Scholar] [CrossRef]
- Ghezzi, M.; Ferraboschi, I.; Fantini, A.; Pescina, S.; Padula, C.; Santi, P.; Sissa, C.; Nicoli, S. Hyaluronic Acid—PVA Films for the Simultaneous Delivery of Dexamethasone and Levofloxacin to Ocular Tissues. Int. J. Pharm. 2023, 638, 122911. [Google Scholar] [CrossRef]
- Singla, J.; Bajaj, T.; Goyal, A.K.; Rath, G. Development of Nanofibrous Ocular Insert for Retinal Delivery of Fluocinolone Acetonide. Curr. Eye Res. 2019, 44, 541–550. [Google Scholar] [CrossRef]
- de Souza SO, L.; Guerra MC, A.; Heneine LG, D.; de Oliveira, C.R.; Cunha Junior AD, S.; Fialho, S.L.; Oréfice, R.L. Biodegradable Core-Shell Electrospun Nanofibers Containing Bevacizumab to Treat Age-Related Macular Degeneration. J. Mater. Sci. Mater. Med. 2018, 29, 173. [Google Scholar] [CrossRef]
- Szymańska, E.; Wojasiński, M.; Dąbrowska, J.; Krzyżowska, M.; Nowicka, M.; Ciach, T.; Winnicka, K. Chitosan-Poly(Ethylene Oxide) Nanofibrous Mat as a Vaginal Platform for Tenofovir Disoproxyl Fumarate—The Effect of Vaginal PH on Drug Carrier Performance. Int. J. Biol. Macromol. 2022, 222, 856–867. [Google Scholar] [CrossRef]
- Martín-Illana, A.; Cazorla-Luna, R.; Notario-Pérez, F.; Bedoya, L.M.; Rubio, J.; Tamayo, A.; Ruiz-Caro, R.; Veiga, M.D. Smart Vaginal Bilayer Films of Tenofovir Based on Eudragit®® L100/Natural Polymer for the Prevention of the Sexual Transmission of HIV. Int. J. Pharm. 2021, 602, 120665. [Google Scholar] [CrossRef]
- Eisenbrey, J.; Kaushal, G.; Tong, X.; Kumar Patel, S.; Li, J.; Patton, D.; Xu, E.; Anderson, P.L.; Parikh, U.; Sweeney, Y.; et al. Development and Evaluation of Nanoparticles-in-Film Technology to Achieve Extended In Vivo Exposure of MK-2048 for HIV Prevention. Polymers 2022, 14, 2520. [Google Scholar] [CrossRef]
- Vartak, R.; Jablonski, J.; Deore, B.; Mediouni, S.; Sanhueza, C.A.; Valente, S.T.; Patel, K. Bictegravir Nanomicelles and Anionic Pullulan Loaded Vaginal Film: Dual Mechanistic Pre-Exposure Prophylaxis (PrEP) for HIV. Int. J. Biol. Macromol. 2022, 221, 416–425. [Google Scholar] [CrossRef]
- Martín-Illana, A.; Chinarro, E.; Cazorla-Luna, R.; Notario-Perez, F.; Veiga-Ochoa, M.D.; Rubio, J.; Tamayo, A. Optimized Hydration Dynamics in Mucoadhesive Xanthan-Based Trilayer Vaginal Films for the Controlled Release of Tenofovir. Carbohydr. Polym. 2022, 278, 118958. [Google Scholar] [CrossRef]
- Hijazi, K.; Iannelli, F.; Cuppone, A.M.; Desjardins, D.; Caldwell, A.; Dereuddre-Bosquet, N.; Scala, C.; Smith, K.A.; Mukhopadya, I.; Frank, B.; et al. In Vivo Modulation of Cervicovaginal Drug Transporters and Tissue Distribution by Film-Released Tenofovir and Darunavir for Topical Prevention of HIV-1. Mol. Pharm. 2020, 17, 852–864. [Google Scholar] [CrossRef] [PubMed]
- Cautela, M.P.; Moshe, H.; Sosnik, A.; Sarmento, B.; das Neves, J. Composite Films for Vaginal Delivery of Tenofovir Disoproxil Fumarate and Emtricitabine. Eur. J. Pharm. Biopharm. 2019, 138, 3–10. [Google Scholar] [CrossRef] [PubMed]
- Nematpour, N.; Moradipour, P.; Zangeneh, M.M.; Arkan, E.; Abdoli, M.; Behbood, L. The Application of Nanomaterial Science in the Formulation a Novel Antibiotic: Assessment of the Antifungal Properties of Mucoadhesive Clotrimazole Loaded Nanofiber versus Vaginal Films. Mater. Sci. Eng. C 2020, 110, 110635. [Google Scholar] [CrossRef] [PubMed]
- Calvo, N.L.; Svetaz, L.A.; Alvarez, V.A.; Quiroga, A.D.; Lamas, M.C.; Leonardi, D. Chitosan-Hydroxypropyl Methylcellulose Tioconazole Films: A Promising Alternative Dosage Form for the Treatment of Vaginal Candidiasis. Int. J. Pharm. 2019, 556, 181–191. [Google Scholar] [CrossRef]
- Humelnicu, A.C.; Samoilă, P.; Cojocaru, C.; Dumitriu, R.; Bostănaru, A.C.; Mareș, M.; Harabagiu, V.; Simionescu, B.C. Chitosan-Based Therapeutic Systems for Superficial Candidiasis Treatment. Synergetic Activity of Nystatin and Propolis. Polymers 2022, 14, 689. [Google Scholar] [CrossRef]
- Jalil, A.; Asim, M.H.; Le, N.M.N.; Laffleur, F.; Matuszczak, B.; Tribus, M.; Bernkop-Schnürch, A. S-Protected Gellan Gum: Decisive Approach towards Mucoadhesive Antimicrobial Vaginal Films. Int. J. Biol. Macromol. 2019, 130, 148–157. [Google Scholar] [CrossRef]
- Gerton, M.L.; Mann, B.K. Mucoadhesive Hyaluronic Acid-Based Films for Vaginal Delivery of Metronidazole. J. Biomed. Mater. Res. B Appl. Biomater. 2021, 109, 1706–1712. [Google Scholar] [CrossRef]
- Ilomuanya, M.O.; Bassey, P.O.; Ogundemuren, D.A.; Ubani-Ukoma, U.N.; Tsamis, A.; Fan, Y.; Michalakis, K.; Angsantikul, P.; Usman, A.; Amenaghawon, A.N. Development of Mucoadhesive Electrospun Scaffolds for Intravaginal Delivery of Lactobacilli Spp., a Tenside, and Metronidazole for the Management of Bacterial Vaginosis. Pharmaceutics 2023, 15, 1263. [Google Scholar] [CrossRef]
- Almotairy, A.; Alyahya, M.; Althobaiti, A.; Almutairi, M.; Bandari, S.; Ashour, E.A.; Repka, M.A. Disulfiram 3D Printed Film Produced via Hot-Melt Extrusion Techniques as a Potential Anticervical Cancer Candidate. Int. J. Pharm. 2023, 635, 122709. [Google Scholar] [CrossRef]
- Pacheco-Quito, E.M.; Bedoya, L.M.; Rubio, J.; Tamayo, A.; Ruiz-Caro, R.; Veiga, M.D. Layer-by-Layer Vaginal Films for Acyclovir Controlled Release to Prevent Genital Herpes. Int. J. Pharm. 2022, 627, 122239. [Google Scholar] [CrossRef]
- Li, J.; Regev, G.; Patel, S.K.; Patton, D.; Sweeney, Y.; Graebing, P.; Grab, S.; Wang, L.; Sant, V.; Rohan, L.C. Rational Design of a Multipurpose Bioadhesive Vaginal Film for Co-Delivery of Dapivirine and Levonorgestrel. Pharmaceutics 2020, 12, 1. [Google Scholar] [CrossRef]
- Mašková, E.; Kubová, K.; Raimi-Abraham, B.T.; Vllasaliu, D.; Vohlídalová, E.; Turánek, J.; Mašek, J. Hypromellose—A Traditional Pharmaceutical Excipient with Modern Applications in Oral and Oromucosal Drug Delivery. J. Control. Release 2020, 324, 695–727. [Google Scholar] [CrossRef]
- Sakpal, D.; Gharat, S.; Momin, M. Recent Advancements in Polymeric Nanofibers for Ophthalmic Drug Delivery and Ophthalmic Tissue Engineering. Biomater. Adv. 2022, 141, 213124. [Google Scholar] [CrossRef]
- Machado, R.M.; Palmeira-De-Oliveira, A.; Martinez-De-Oliveira, J.; Palmeira-De-Oliveira, R. Vaginal Films for Drug Delivery. J. Pharm. Sci. 2013, 102, 2069–2081. [Google Scholar] [CrossRef]
- Menegatou, I.M.; Papakyriakopoulou, P.; Rekkas, D.M.; Dallas, P.; Valsami, G. Design of a Personalized Nasal Device (Matrix-Piston Nasal Device, MPD) for Drug Delivery: A 3D-Printing Application. AAPS PharmSciTech 2022, 23, 205. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Drug Delivery System | Production Method | Polymer | Administration Site | Results |
|---|---|---|---|---|
| Nanoparticulate, oral, fast-dissolving film dosage form of nitrendipine [58] | Solvent casting | HPMC E6 and PVA | Buccal | Increase solubility and dissolution of the drug |
| Polymeric and electrospun patches for drug delivery [66] | Solvent casting | PVA, sodium alginate, and sodium carboxymethyl cellulose | Buccal | Excellent mucoadhesive strength; buccal patch had optimum pH for buccal compatibility and prolonged release up to 5 h |
| Hydrobromide immediate-release buccal films using a central composite rotatable design [73] | Solvent casting | HPMC E5 | Buccal | Immediate-release drug delivery, rapidly improved migraine conditions, and enhanced patient compliance |
| Insulin fast-dissolving film [98] | Solvent casting | HPMC and PVA | Nasal | Significant elevation of the olfactory detection scores and olfactory discrimination values in the intervention group after intranasal administration |
| Timolol-loaded composite [103] | Solvent casting | Hyaluronic acid and HPMC | Ocular | Prolonged drug release profiles |
| Buccal films of propranolol hydrochloride [60] | 3D Printing | PVP and PVA | Buccal | Good mechanical and mucoadhesive pro-perties and prolonged drug release |
| Solid, dispersed, multilayered core-sheath, raloxifene-loaded, nanofibrous [84] | Electrospinning | PVA, HPMC, and chitosan | Buccal | Ongoing studies with expected therapeutic potential for use in preventing and treating osteoporosis and decreasing the risk of developing invasive breast cancer in postmenopausal women. |
| Nanofibrous fluocinolone acetonide [109] | Electrospinning | Poly(caprolactone) | Ocular | Higher drug permeation, higher systemic availability of drug, and higher retention of the drug carrier at the absorption site |
| Midazolam (2-dimensionally printed) [90] | Inkjet printing | Kollidon® 12 PF (polyvinyl pyrrolidone) | Buccal | Increased absorption and residence time of midazolam in the oral cavity |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
de Carvalho, A.C.W.; Paiva, N.F.; Demonari, I.K.; Duarte, M.P.F.; do Couto, R.O.; de Freitas, O.; Vicentini, F.T.M.d.C. The Potential of Films as Transmucosal Drug Delivery Systems. Pharmaceutics 2023, 15, 2583. https://doi.org/10.3390/pharmaceutics15112583
de Carvalho ACW, Paiva NF, Demonari IK, Duarte MPF, do Couto RO, de Freitas O, Vicentini FTMdC. The Potential of Films as Transmucosal Drug Delivery Systems. Pharmaceutics. 2023; 15(11):2583. https://doi.org/10.3390/pharmaceutics15112583
Chicago/Turabian Stylede Carvalho, Ana Clara Wada, Natália Floriano Paiva, Isabella Kriunas Demonari, Maíra Peres Ferreira Duarte, Renê Oliveira do Couto, Osvaldo de Freitas, and Fabiana Testa Moura de Carvalho Vicentini. 2023. "The Potential of Films as Transmucosal Drug Delivery Systems" Pharmaceutics 15, no. 11: 2583. https://doi.org/10.3390/pharmaceutics15112583