
The Effect of CYP2D6 Phenotypes on the Pharmacokinetics of Propafenone: A Systematic Review and Meta-Analysis

 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
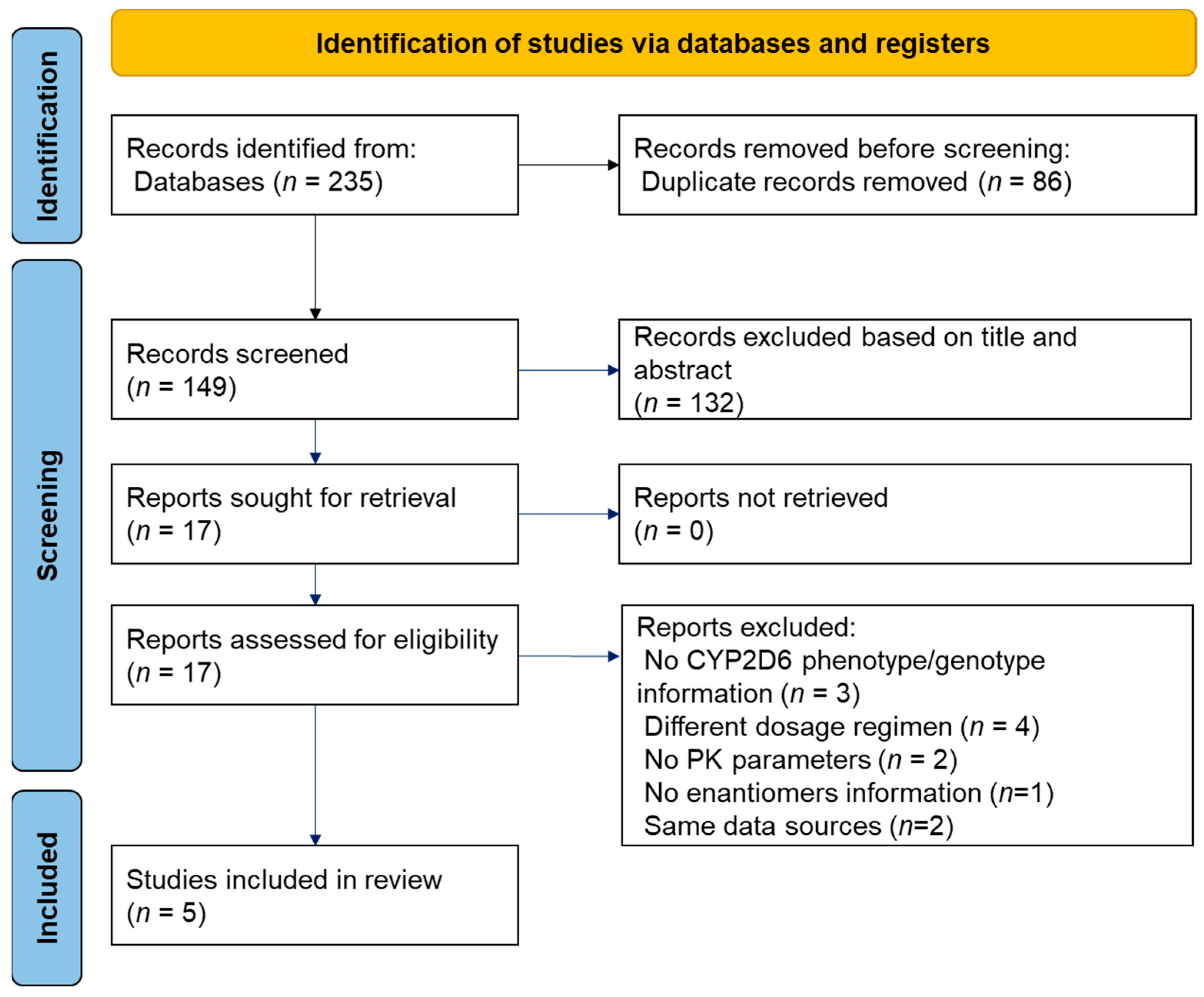
2.1. Data Sources and Study Selection Criteria
Search Strategy
2.2. Data Extraction
2.3. Statistical Analysis
3. Results
3.1. Study Characteristics
3.2. Meta-Analysis Results
3.2.1. Comparison of PMs and EMs at the 300 mg Dose
3.2.2. Comparison of S-Form and R-Form of PPF in EMs at the 400 mg Dose
3.2.3. Comparisons of the Quotient between CYP2D6 Phenotype and Enantiomers According to Dose
3.3. Risk of Bias across Studies
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ingelman-Sundberg, M. Genetic polymorphisms of cytochrome P450 2D6 (CYP2D6): Clinical consequences, evolutionary aspects and functional diversity. Pharm. J. 2005, 5, 6–13. [Google Scholar] [CrossRef]
- Kirchheiner, J.; Brøsen, K.; Dahl, M.L.; Gram, L.F.; Kasper, S.; Roots, I.; Sjöqvist, F.; Spina, E.; Brockmöller, J. CYP2D6 and CYP2C19 genotype base-dose recommendations for antidepressants: A first step towards subpopulation-specific dosages. ACTA Psychiatr. Scand. 2001, 104, 173–192. [Google Scholar] [CrossRef]
- Swen, J.J.; Nijenhuis, M.; de Boer, A.; Grandia, L.; Maitland-Van Der Zee, A.H.; Mulder, H.; Rongen, G.A.P.J.M.; van Schaik, R.H.N.; Schalekamp, T.; Touw, D.J.; et al. Pharmacogenetics: From bench to byte an update of guidelines. Clin. Pharmacol. Ther. 2011, 89, 662–673. [Google Scholar] [CrossRef]
- Kirchheiner, J.; Nickchen, K.; Bauer, M.; Wong, M.L.; Licinio, J.; Roots, I.; Brockmöller, J. Pharmacogenetics of antidepressants and antipsychotics: The contribution of allelic variations to the phenotype of drug response. Mol. Psychiatry 2004, 9, 442–473. [Google Scholar] [CrossRef]
- Zhou, S.-F. Polymorphism of human cytochrome P450 2D6 and its clinical significance: Part I. Clin. Pharmacokinet. 2009, 48, 689–723. [Google Scholar] [CrossRef]
- Thuerauf, N.; Lunkenheimer, J. The impact of the CYP2D6-polymorphism on dose recommendations for current antidepressants. Eur. Arch. Psychiatry Clin. Neurosci. 2006, 256, 287–293. [Google Scholar] [CrossRef]
- US Food and Drug Administration. Label for Propafenone. Available online: https://www.accessdata.fda.gov/drugsatfda_docs/label/2013/019151s012lbl.pdf (accessed on 12 January 2021).
- Hii, J.T.Y.; Duff, H.J.; Burgess, E.D. Clinical Pharmacokinetics of Propafenone. Clin. Pharmacokinet. 1991, 21, 1–10. [Google Scholar] [CrossRef]
- Dean, L. Propafenone Therapy and CYP2D6 Genotype. In Medical Genetics Summaries; Pratt, V.M., Scott, S.A., Pirmohamed, M., Esquivel, B., Kane, M.S., Kattman, B.L., Malheiro, A.J., Eds.; 2017; pp. 1–7. Available online: https://www.ncbi.nlm.nih.gov/books/NBK425391/ (accessed on 30 March 2021).
- Rouini, M.R.; Afshar, M. Effect of CYP2D6 polymorphisms on the pharmacokinetics of propafenone and its two main metabolites. Therapie 2017, 72, 373–382. [Google Scholar] [CrossRef]
- Zhou, S.F. Polymorphism of human cytochrome P450 2D6 and its clinical significance: Part II. Clin. Pharmacokinet. 2009, 48, 761–804. [Google Scholar] [CrossRef]
- Bing, C.; Wei-Min, C. Influence of CYP2D6 * 10B genotype on pharmacokinetics of propafenone enantiomers in Chinese subjects. Acta Pharmacol. Sin. 2003, 24, 1277–1280. [Google Scholar]
- Zhang, X.; Xiang, Q.; Zhao, X.; Ma, L.; Cui, Y. Association between aripiprazole pharmacokinetics and CYP2D6 phenotypes: A systematic review and meta-analysis. J. Clin. Pharm. Ther. 2019, 44, 163–173. [Google Scholar] [CrossRef] [Green Version]
- Wei-Min, C.; Chen, B.; Liu, Y.X.; Chu, X. Dextromethorphan metabolic phenotyping in a Chinese population. Acta Pharmacol. Sin. 1997, 18, 441–444. [Google Scholar]
- Crews, K.R.; Gaedigk, A.; Dunnenberger, H.M.; Klein, T.E.; Shen, D.D.; Callaghan, J.T.; Kharasch, E.D.; Skaar, T.C.; Consortium, C.P.I. Clinical Pharmacogenetics Implementation Consortium (CPIC) guidelines for codeine therapy in the context of cytochrome P450 2D6 (CYP2D6) genotype. Clin. Pharmacol. Ther. 2012, 91, 321–326. [Google Scholar] [CrossRef]
- Dilger, K.; Greiner, B.; Fromm, M.F.; Hofnmann, U.; Kroemer, H.K.; Elchelbaum, M. Consequence of rifanpicin treatment on propafenone disposition in extensive and poor metabolizers of CYP2D6. Pharmacogenomics 1999, 9, 551–559. [Google Scholar] [CrossRef]
- Li, G.; Gong, P.L.; Qiu, J.; Zeng, F.D.; Klotz, U. Stereoselective steady state disposition and action of propafenone in Chinese subjects. Br. J. Clin. Pharmacol. 1998, 46, 441–445. [Google Scholar] [CrossRef] [Green Version]
- Kroemer, H.K.; Funck-Brentano, C.; Silberstein, D.J.; Wood, A.J.J.; Eichelbaum, M.; Woosley, R.L.; Roden, D.M. Stereoselective disposition and pharmacologic activity of propafenone enantiomers. Circulation 1989, 79, 1068–1076. [Google Scholar] [CrossRef] [Green Version]
- Chen, X.; Zhong, D.; Blume, H. Stereoselective pharmacokinetics of propafenone and its major metabolites in healthy Chinese volunteers. Eur. J. Pharm. Sci. 2000, 10, 11–16. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Blake, C.; Kharasch, E.; Schwab, M.; Nagele, P. A Meta-Analysis of CYP2D6 Metabolizer Phenotype and Metoprolol Pharmacokinetics. Clin. Pharmacol. Ther. 2013, 94, 394–399. [Google Scholar] [CrossRef] [Green Version]
- Kroemer, H.K.; Fromm, M.F.; Bühl, K.; Terefe, H.; Blaschke, G.; Eichelbaum, M. An enantiomer-enantiomer interaction of (S)- and (R)-propafenone modifies the effect of racemic drug therapy. Circulation 1994, 89, 2396–2400. [Google Scholar] [CrossRef] [Green Version]
- LABBE, L. Pharmacokinetic and pharmacodynamic interaction between mexiletine and propafenone in human beings*1. Clin. Pharmacol. Ther. 2000, 68, 44–57. [Google Scholar] [CrossRef]
- Ujhelyi, M.R.; Rangers, E.A.O.; Fan, C.; Kluger, J.; Pharand, C.; Chow, M.S.S. The pharmacokinetic and pharmacodynamic interaction between propafenone and lidocaine. Clin. Pharmacol. Ther. 1993, 53, 38–48. [Google Scholar] [CrossRef]
- Doki, K.; Shirayama, Y.; Sekiguchi, Y.; Aonuma, K.; Kohda, Y.; Ieda, M.; Homma, M. Effect of CYP2D6 genetic polymorphism on peak propafenone concentration: No significant effect of CYP2D6*10. Pharmacogenomics 2020, 21, 1279–1288. [Google Scholar] [CrossRef]
- Wei-Min, C.; Xu, J.; Chen, B.; Zhang, F.-M.; Huang, Y.-Z.; Zhang, Y.-D. Effect of CYP2D6*10 genotype on propafenone pharmacodynamics in Chinese patients with ventricular arrhythmia. Acta Pharmacol. Sin. 2002, 23, 1040–1044. [Google Scholar]
- Lee, J.T.; Kroemer, H.K.; Silberstein, D.J.; Funck-Brentano, C.; Lineberry, M.D.; Wood, A.J.J.; Roden, D.M.; Woosley, R.L. The Role of Genetically Determined Polymorphic Drug Metabolism in the Beta-Blockade Produced by Propafenone. N. Engl. J. Med. 1990, 322, 1764–1768. [Google Scholar] [CrossRef]
- Wei-Min, C.; Yin-Di, Z.; Bing, C.; Minh-Hong, C.; Jian-Ping, L.; Shu-Sen, L. Simultaneous modeling of pharmacokinetics and pharmacodynamics of propafenone in healthy subjects. Acta Pharmacol. Sin. 2001, 22, 956–960. [Google Scholar]
- Wei-Min, C.; Bing, C.; Ming-Hong, C.; Yin-Di, Z. CYP2D6 phenotype determines pharmacokinetic variability of propafenone enantiomers in 16 HAN chinese subjects. Acta Pharmacol. Sin. 1999, 20, 720–724. [Google Scholar]
- Wei-Min, C.; Bing, C.; Ming-Hong, C.; Chen, Y.; Yin-Di, Z. The influence of CYP2D6 activity on the kinetics of propafenone enantiomers in Chinese subjects. Br. J. Clin. Pharmacol. 1999, 47, 553–556. [Google Scholar] [CrossRef] [Green Version]
- Wei-Min, C.; Bing, C.; Yan, Z.; Yin-DI, Z. Fluoxetine impairs the CYP2D6-mediated metabolism of propafenone enantiomers in healthy Chinese volunteers. Clin. Pharmacol. Ther. 1999, 66, 516–521. [Google Scholar] [CrossRef]
- Dilger, K.; Hofmann, U.; Klotz, U. Enzyme induction in the elderly: Effect of rifampin on the pharmacokinetics and pharmacodynamics of propafenone. Clin. Pharmacol. Ther. 2000, 67, 512–520. [Google Scholar] [CrossRef]
- Higgins, J.; Green, S. Addressing reporting biases. In Cochrane Handbook for Systematic Reviews of Interventions; Version 5.1.0. The Cochrane Collaboration; 2011; Available online: www.handbook.cochrane.org (accessed on 18 May 2021).
- Ovaska, H.; Ludman, A.; Spencer, E.P.; Wood, D.M.; Jones, A.L.; Dargan, P.I. Propafenone poisoning-A case report with plasma propafenone concentrations. J. Med. Toxicol. 2010, 6, 37–40. [Google Scholar] [CrossRef] [PubMed]
- Alsaad, A.A.; Ortiz Gonzalez, Y.; Austin, C.O.; Kusumoto, F. Revisiting propafenone toxicity. BMJ Case Rep. 2017, 2017, bcr2017219270. [Google Scholar] [CrossRef] [PubMed]
- Kroemer, H.K.; Fischer, C.; Meese, C.O.; Eichelbaum, M. Enantiomer/enantiomer interaction of (S)- and (R)-propafenone for cytochrome P450IID6-catalyzed 5-hydroxylation: In vitro evaluation of the mechanism. Mol. Pharmacol. 1991, 40, 135–142. [Google Scholar] [PubMed]
- Komura, H.; Iwaki, M. Nonlinear pharmacokinetics of propafenone in rats and humans: Application of a substrate depletion assay using hetatocytes for assessment of nonlinearity. Drug Metab. Dispos. 2005, 33, 726–732. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- US Food and Drug Administration RYTHMOL SR Labeling. Available online: https://www.accessdata.fda.gov/drugsatfda_docs/label/2003/21416_rythmol_lbl.pdf (accessed on 12 January 2021).


{kind=link}
| Reasons for Exclusion | References |
|---|---|
| No information on CYP2D6 phenotype/genotype was reported | [17,19,22] |
Studies with dosage regimens were different from the other studies
Due to the non-linear pharmacokinetics of PPF, combining studies according to normalized dose is inappropriate; thus, the four above studies were excluded. | [23,24,25,26] |
Two studies with a dosage of 150 mg three times per day but no identical PK parameters were reported:
| [18,27] |
| No information on PPF enantiomers was reported (400 mg dose) There were four more studies with a 400 mg dose; however, PPF was clarified as R- and S-enantiomer in those studies. Therefore, study [28] was excluded. | [28] |
| Three studies had used the same data, thus two of them were excluded. | [12,29] |
| Dose | Subgroup | Sample Size | Outcome | p-Value | Mean Difference (95% Prediction Interval) | Heterogeneity | References | |
|---|---|---|---|---|---|---|---|---|
| I2 | Model | |||||||
| 300 mg | PM vs. EM | 24 | Cmax | <0.001 | 0.51 [0.25, 0.76] | 0% | Fixed model | [10,16] |
| AUC | <0.001 | 13.83 [8.48, 19.19] | 60% | Random model | ||||
| t1/2 | <0.001 | 9.65 [8.26, 11.05] | 0% | Fixed model | ||||
| 400 mg | S-form and R-form in EM group | 25 | Cmax | <0.001 | 0.13 [0.06, 0.20] | 0% | Fixed model | [30,31] |
| AUC | <0.001 | 0.61 [0.23, 0.99] | 0% | Fixed model | ||||
| CL/F | <0.001 | −35.00 [−56.53, −13.46] | 0% | Fixed model | ||||
| n | Cmax (µg/mL) | AUC (µg·h/mL) | t1/2 (h) | |
|---|---|---|---|---|
| PM | 10 | 1.10 (0.796–1.40) | 15.9 (12.5–19.2) | 12.8 (11.3–14.3) |
| EM | 21 | 0.453 (0.294–0.612) | 1.41 (0.894–1.93) | 2.73 (2.2–3.27) |
| Ratio PM/EM | 2.42 (1.53–4.07) | 11.23 (7.45–18.88) | 4.68 (3.73–6.05) |
| n | Cmax (µg/mL) | AUC (µg·h/mL) | CL/F (L/h) | |
|---|---|---|---|---|
| S-form | 25 | 0.42 (0.365–0.475) | 2.22 (1.93–2.51) | 88.4 (75–102) |
| R-form | 25 | 0.30 (0.257–0.343) | 1.62 (1.39–1.85) | 127 (101–153) |
| Ratio S-/R-form | 1.40 (1.15–1.72) | 1.37 (1.22–1.68) | 0.70 (0.540–0.917) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tran, Q.T.; Baek, I.-h.; Han, N.-y.; Yun, H.-y.; Chae, J.-w. The Effect of CYP2D6 Phenotypes on the Pharmacokinetics of Propafenone: A Systematic Review and Meta-Analysis. Pharmaceutics 2022, 14, 1446. https://doi.org/10.3390/pharmaceutics14071446
Tran QT, Baek I-h, Han N-y, Yun H-y, Chae J-w. The Effect of CYP2D6 Phenotypes on the Pharmacokinetics of Propafenone: A Systematic Review and Meta-Analysis. Pharmaceutics. 2022; 14(7):1446. https://doi.org/10.3390/pharmaceutics14071446
Chicago/Turabian StyleTran, Quyen Thi, In-hwan Baek, Na-young Han, Hwi-yeol Yun, and Jung-woo Chae. 2022. "The Effect of CYP2D6 Phenotypes on the Pharmacokinetics of Propafenone: A Systematic Review and Meta-Analysis" Pharmaceutics 14, no. 7: 1446. https://doi.org/10.3390/pharmaceutics14071446