
Biomaterial-Based Therapeutic Strategies for Obesity and Its Comorbidities


Abstract
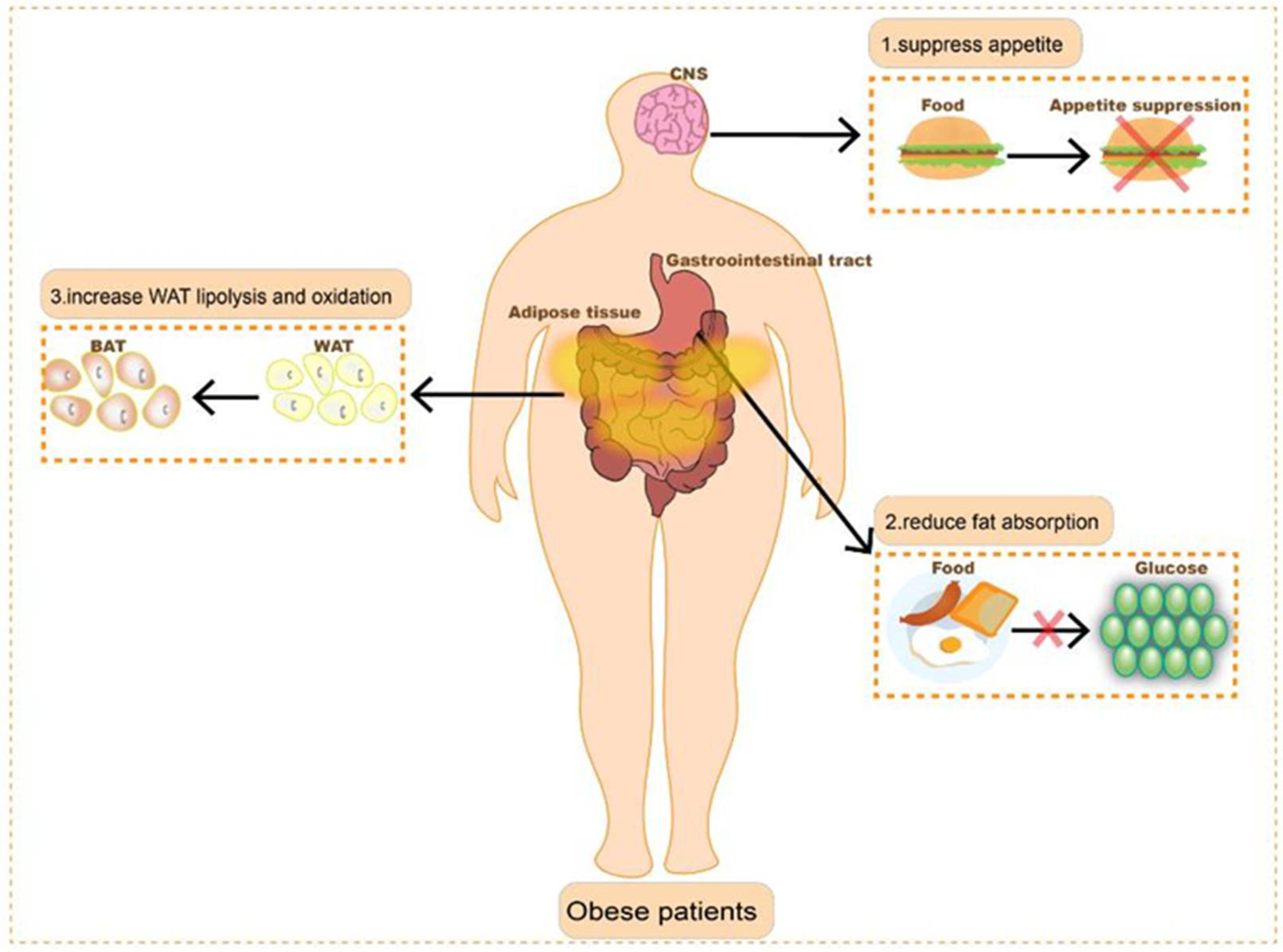
:1. Introduction
2. Pharmacological Treatment of Obesity
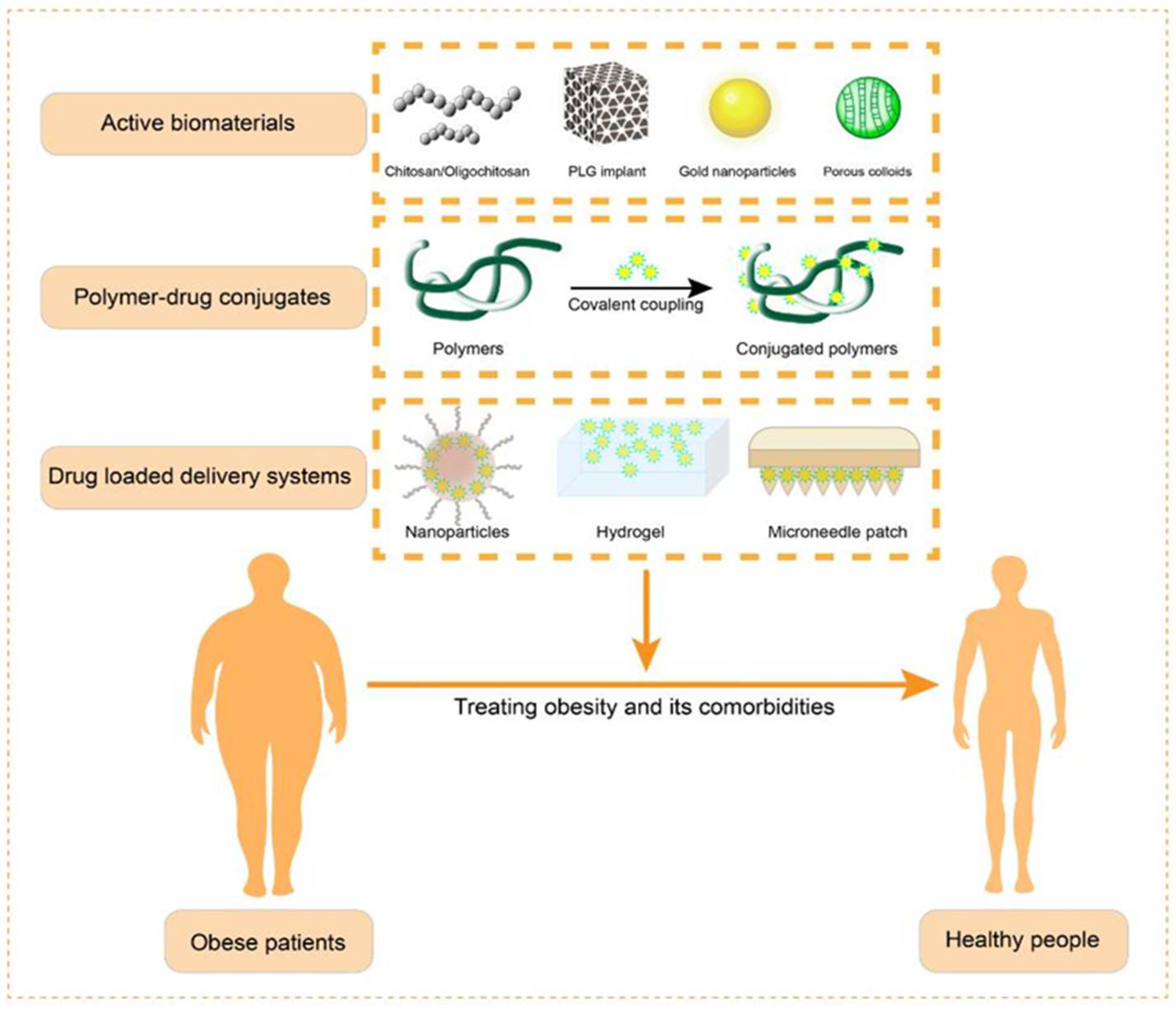
3. Biomaterial-Assisted Anti-Obesity Therapy
3.1. Biomaterials with Inherent Anti-Obesity Activity

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Materials | Mechanism of Action | Characteristics | Main Outcomes | Reference |
|---|---|---|---|---|
| Chitosan and chitosan oligosaccharide | Upregulates the expression of serum leptin and CRP to inhibit adipogenesis and activates PPARγ expression to ameliorate glucose and lipid metabolism disorders | Biodegradable and low toxicity, with easily modifiable amino groups | Attenuates obesity and modulates glucose and lipid metabolism | [74,75,76] |
| PLG implants | Increases the expression of glucose transporter 1 and insulin-like growth factor 1 and increases glucose uptake | Synthetic, degradable, and good biocompatibility | Attenuates obesity and alleviates glucose intolerance | [106] |
| Au NPs | Reduces inflammation, regulates lipid metabolism, and ablates fatty tissue with near-infrared light | Cell regulation, good biocompatibility, and photothermal conversion capacity | Attenuates obesity and alleviates glucose intolerance | [107,108,109,110,111] |
| Smectite clays and mesoporous silica | Adsorbs digestive enzymes to limit lipid digestion and adsorbs fats and carbohydrates to promote their excretion | Porous colloidal structure | Attenuates obesity | [112] |
3.2. Biomaterial-Encapsulated Phytochemicals for Anti-Obesity Treatment
3.2.1. Resveratrol
3.2.2. Capsaicin
| Drugs | Materials | Mechanism of Action | Characteristics | Main Outcomes | Reference |
|---|---|---|---|---|---|
| Resveratrol | Lipid nanoparticles modified with ASC-targeting peptides; nanocapsules prepared from starch particles | Induces browning of white adipocytes | Increases drug bioavailability and decreases toxicity | Attenuates obesity and reduces inflammatory response | [117,118,119] |
| Capsaicin | Liposomes; microneedle patches | Induces browning of white adipocytes and increases mitochondrial biogenesis to activate energy metabolism | Reduces drug irritation to the gastrointestinal tract and increases drug enrichment in local adipose tissue | Attenuates obesity and reduces inflammatory response | [122,123] |
| Caffeine | Microneedle patches | Reduces the levels of triglyceride, total cholesterol, and low-density lipoprotein and stimulates lipolysis | Avoids gastrointestinal absorption of the drug | Attenuates obesity | [124] |
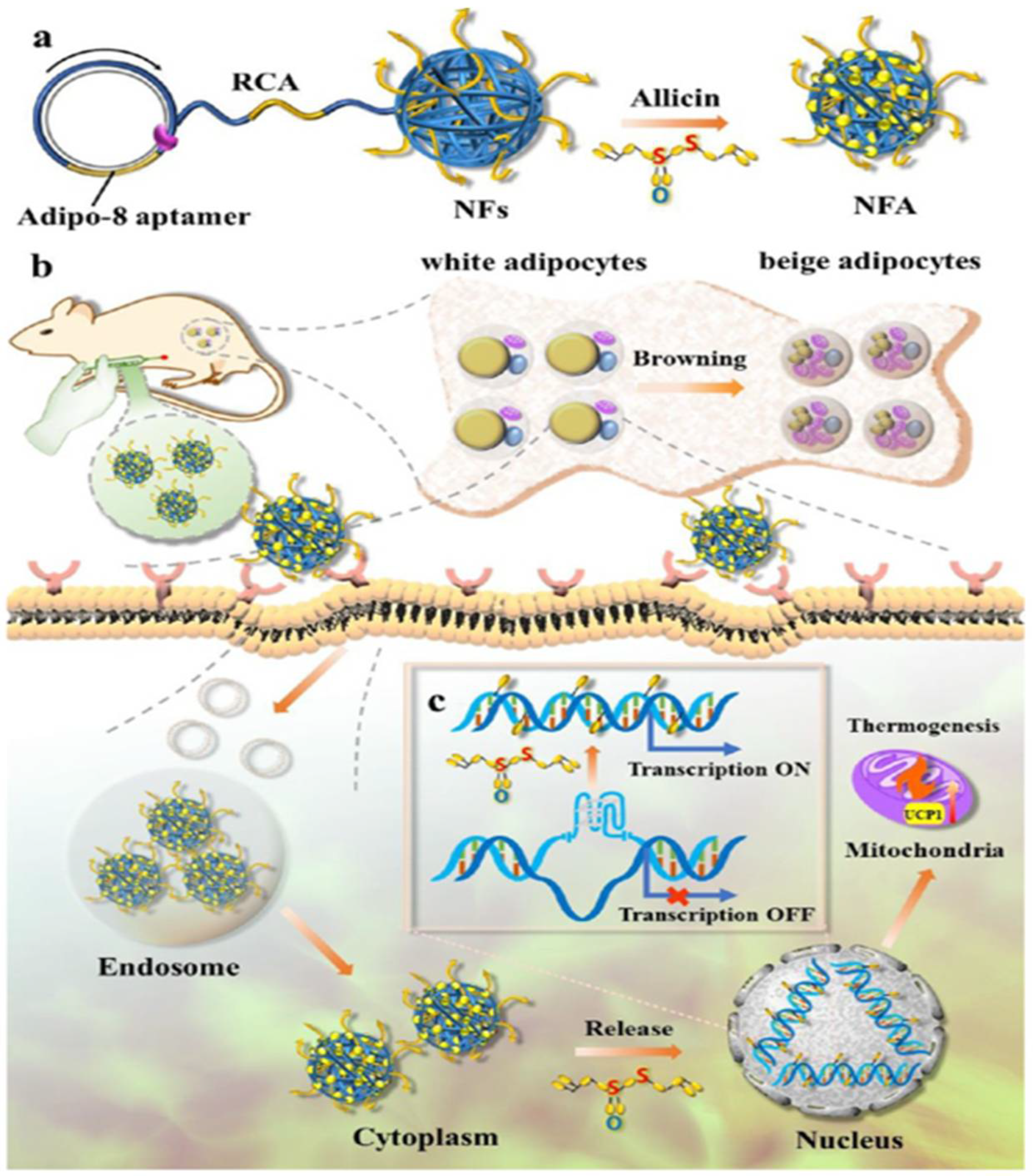
| Allicin | DNA nanoflowers modified with adipo-8 aptamer | Induces browning of white adipocytes | Enhance the biological activity and stability of the drug | Attenuates obesity | [125] |
3.2.3. Caffeine and Allicin
3.3. Biomaterial-Encapsulated Synthetic Drugs for Anti-Obesity Treatment
3.3.1. Rosiglitazone
3.3.2. Orlistat
3.3.3. Thiopental Sodium
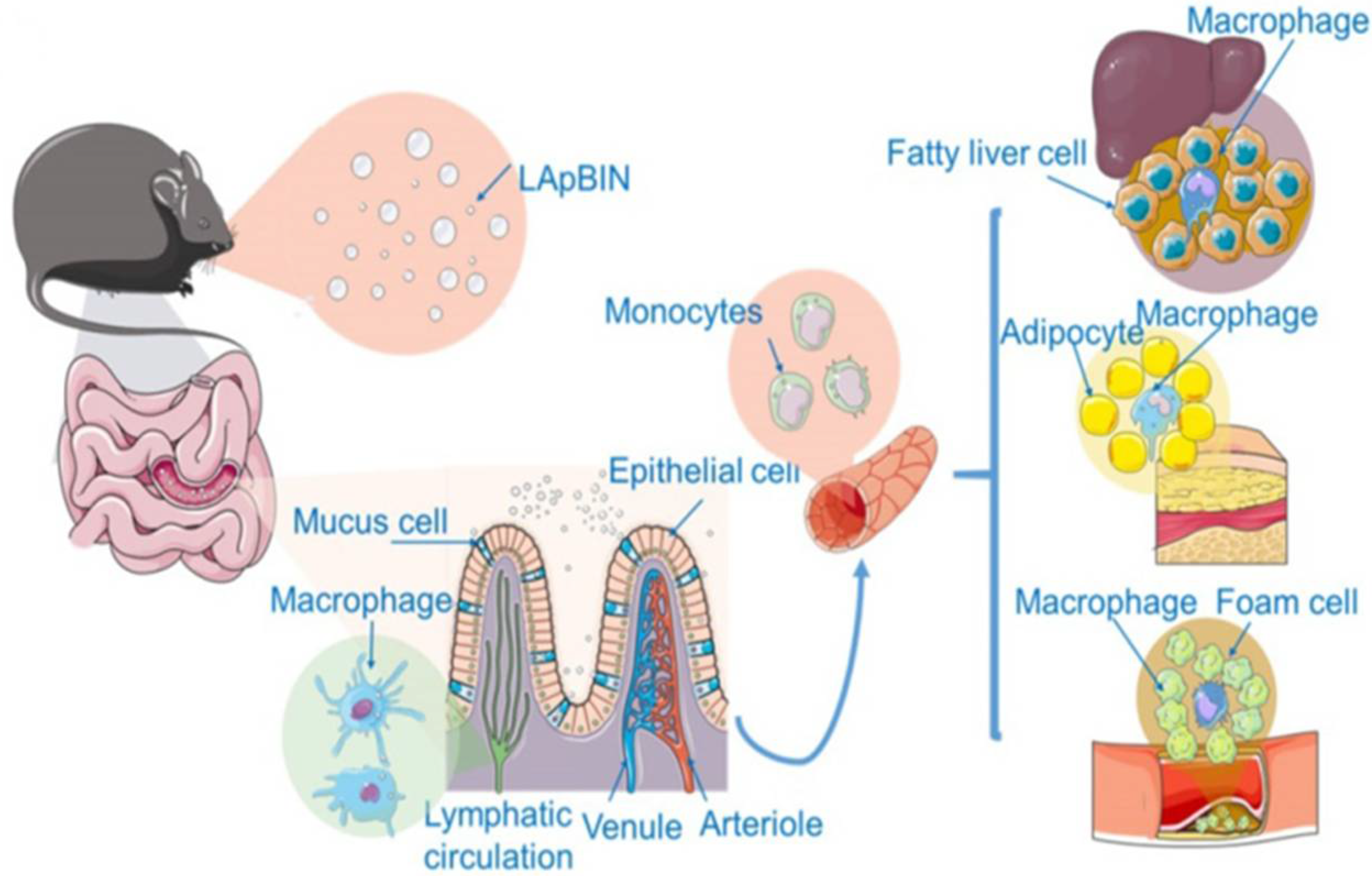
3.3.4. Bindarit
| Drugs | Materials | Mechanism of Action | Characteristics | Main Outcomes | Reference |
|---|---|---|---|---|---|
| Rosiglitazone | PLGA nanoparticles, virus-like particles (VLPs) modified with the ATP motif, PLGA/NaCl micro-lances, and PELA electrospun fibers | Induces browning of white adipocytes and reduces inflammatory responses mediated by macrophages | Targeted drug delivery to adipocytes, reducing drug toxicity and side effects | Attenuates obesity and reduces inflammatory response | [128,130,131,132] |
| Orlistat | Nanostructured clay particles | Inhibits lipase activity and hinders fat absorption | Reduces toxic side effects such as gastrointestinal irritation | Attenuates obesity | [134] |
| Thiopental sodium | Lipid nanoparticles | Reduces inflammatory responses | Improves drug bioavailability | Ameliorates obesity-induced cardiac dysfunction and cardiac hypertrophy | [135] |
| Bindarit | Laminarin-modified nanoparticles | Reduces inflammatory responses | Specifically identifies monocytes and macrophages and improves drug bioavailability | Prevents obesity, insulin resistance, fatty liver, and atherosclerosis | [140] |
3.4. Biologic Drugs for Anti-Obesity Treatment
3.4.1. Targeting Adipose Tissue Macrophages
3.4.2. Inhibition of WAT Angiogenesis
3.4.3. Regulation of Signaling Pathways
3.4.4. Regulation of Hormone Levels
3.4.5. Genetically Engineered Drug Delivery
| Strategies | Drugs | Materials | Mechanism of Action | Characteristics | Main Outcomes | Reference |
|---|---|---|---|---|---|---|
| Targeting adipose tissue macrophages | HIL-4 | PLG implants | Induces an anti-inflammatory phenotype in macrophages, increase the proportion of helper T cells | Acts locally and long-lastingly on WAT | Attenuates obesity and reduces inflammatory response | [145] |
| IL-10 | Liposomes with surface modified by phosphatidylserine | Inhibits the secretion of pro-inflammatory factors such as IL-6 and TNF-α | High affinity for macrophages | Attenuates obesity and reduces inflammatory response | [148] | |
| Sea cucumber saponins | Liposomes | Inhibits secretion of pro-inflammatory cytokines, reduces macrophage infiltration, and increases glucose uptake | Improves drug bioavailability | Attenuates obesity, reduces inflammatory response, and alleviates glucose intolerance | [150] | |
| Inhibition of WAT angiogenesis | Pro-apoptotic peptide KLA | Adipose homing peptide; liposomes modified by fat homing peptide | Inhibits angiogenesis | Targeting the WAT vascular system | Attenuates obesity | [153,154,155] |
| Regulation of signaling pathways | Bioactive peptide PDBSN | Liposomes modified with visceral tissue-targeting peptide | Activates AMPK pathway to inhibit adipocyte differentiation | Targeting white adipocytes | Attenuates obesity and modulates glucose and lipid metabolism | [157] |
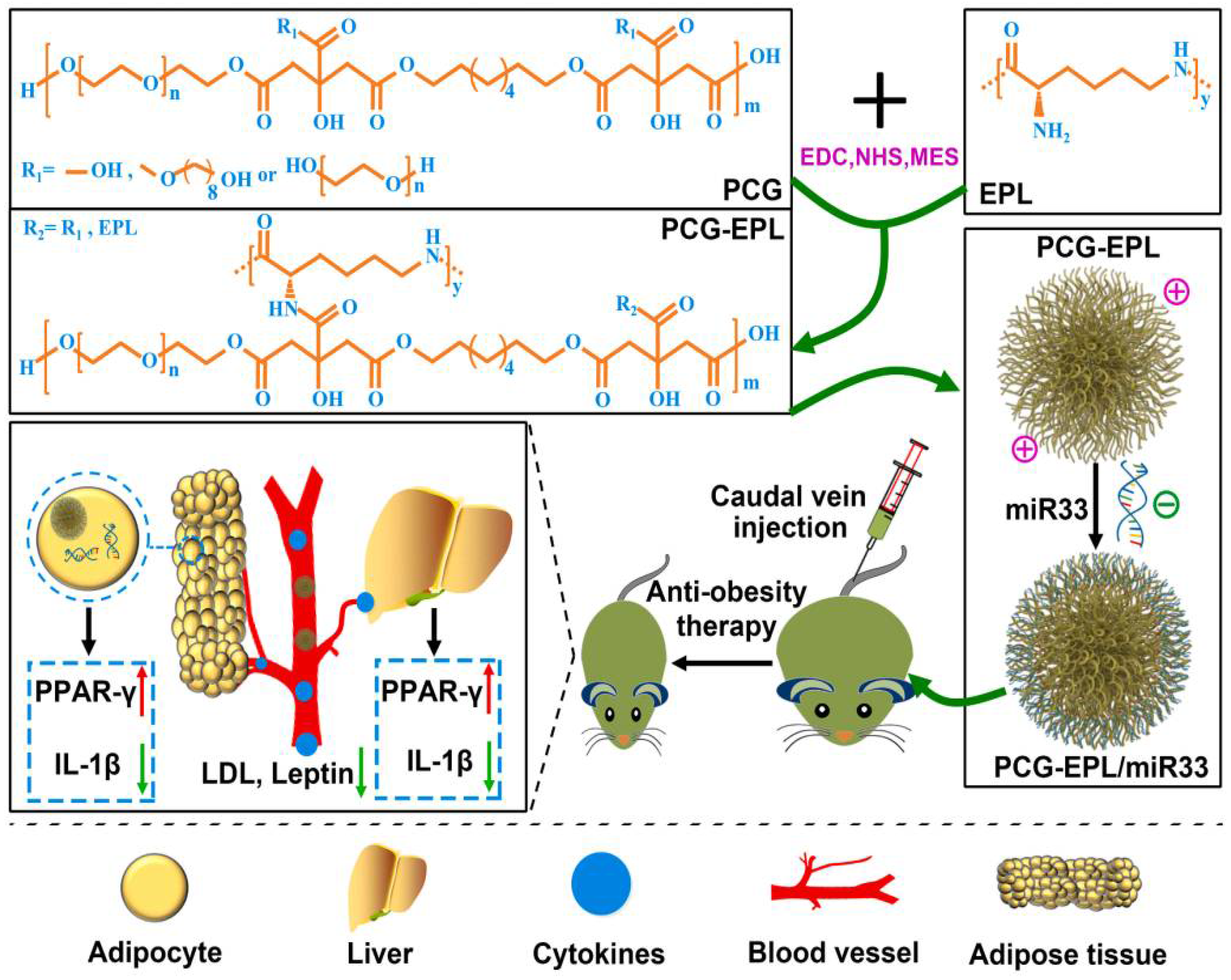
| Regulation of signaling pathways | miR33 | PCG-EPL micelles | Regulates leptin, insulin, and lipoprotein expression and controls metabolism | Delivers miRNA to adipocytes | Attenuates obesity and alleviates glucose intolerance | [158] |
| miR-130b | Cellular microvesicles | Regulates lipid metabolism | Delivers miRNA to epididymal adipose tissue | Attenuates obesity, alleviates glucose intolerance | [159] | |
| Regulation of hormone levels | Leptin | Pluronic P85 | Acts on the hypothalamus to regulate appetite and energy metabolism | Polymer modification to extend the half-life of the drug | Attenuates obesity | [160] |
| Oxyntomodulin analog | PEG | Regulates glucose metabolism and insulin secretion | Polymer modification to extend the half-life of the drug | Attenuates obesity, reduces blood glucose level, and reverses liver steatosis | [164] | |
| Genetically engineered drug delivery | Plasmids containing both IAPP and iridoid gene structure | Linear polyethyleneimine | Induces browning of white adipocytes and triggers thermogenic procedures | Synergistic effects of combination gene therapy | Attenuates obesity | [167] |
| FGF21 | PsTag polypeptide | Regulates glucose metabolism, lipid metabolism, and insulin resistance | Preparation of E. coli fusion expression proteins of cytokines and polypeptides to extend the half-life of protein drugs | Attenuates obesity, reduces blood glucose level, and reverses liver steatosis | [169] | |
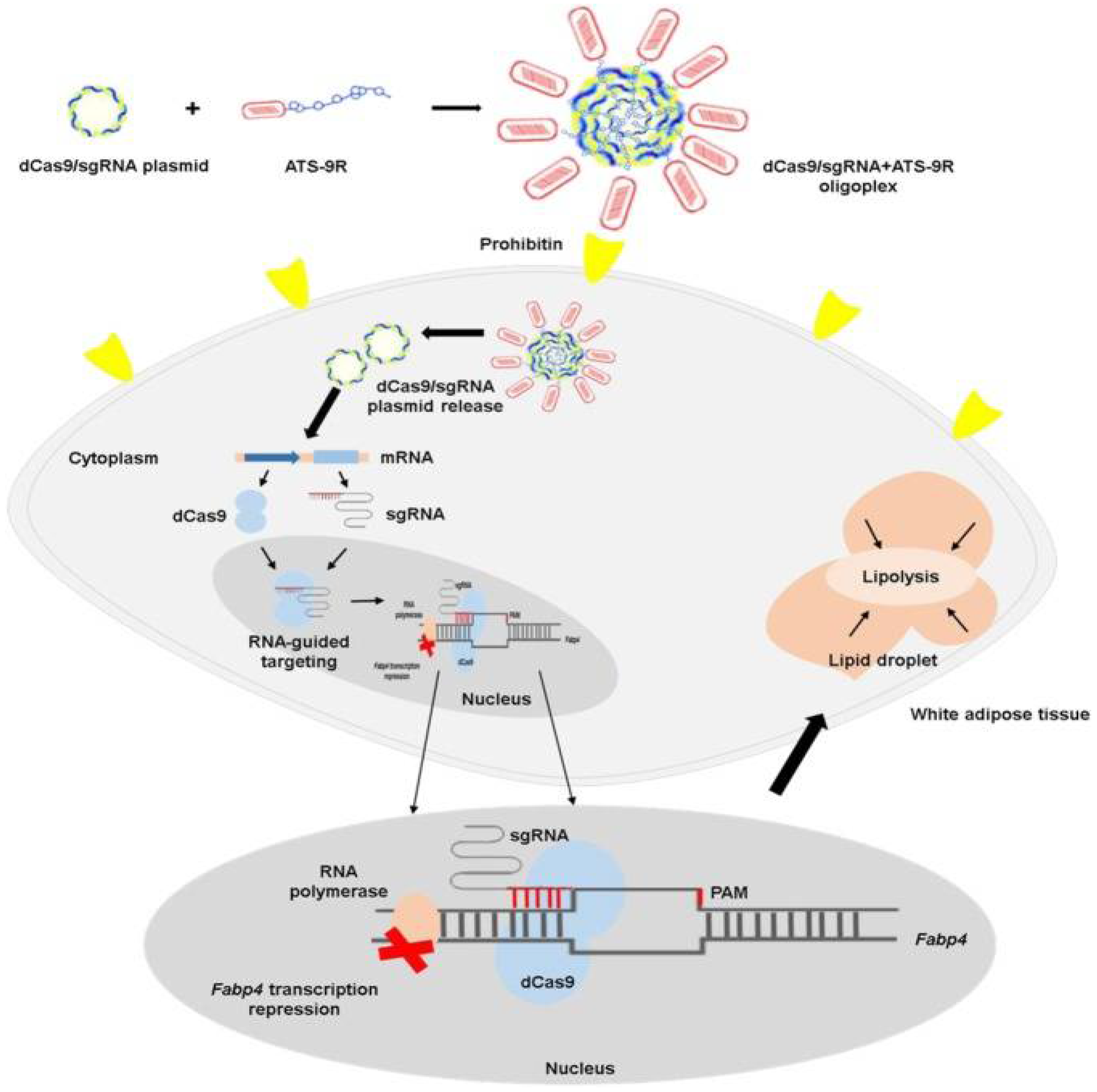
| fabp4 | dCas9/sgFabp4 CRISPRi interference system | Silencing the gene of Fabp4 | CRISPRi interference technology for selective regulation of metabolism-related genes | Attenuates obesity and reverses liver steatosis | [171] |
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Afshin, A.; Forouzanfar, M.H.; Reitsma, M.B.; Sur, P.; Estep, K. Health effects of overweight and obesity in 195 countries over 25 years. N. Engl. J. Med. 2017, 377, 13–27. [Google Scholar] [PubMed]
- Burki, T. European Commission classifies obesity as a chronic disease. Lancet Diabetes Endocrinol. 2021, 9, 418. [Google Scholar] [CrossRef]
- Soltani, G.; Poursheikhani, A.; Yassi, M.; Hayatbakhsh, A.; Kerachian, M.; Kerachian, M.A. Obesity, diabetes and the risk of colorectal adenoma and cancer. BMC Endocr. Disord. 2019, 19, 113–122. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hales, C.M.; Carroll, M.D.; Fryar, C.D.; Ogden, C.L. Prevalence of Obesity among Adults and Youth: United States, 2015–2016; NCHS Data Brief No. 288; National Center for Health Statistics: Hyattsville, MD, USA, 2017.
- Pan, X.F.; Wang, L.; Pan, A. Epidemiology and determinants of obesity in China. Lancet Diabetes Endocrinol. 2021, 9, 373–392. [Google Scholar] [CrossRef]
- Guo, Y.; Yin, X.; Wu, H.; Chai, X.; Yang, X. Trends in overweight and obesity among children and adolescents in China from 1991 to 2015: A meta-analysis. Int. J. Environ. Res. Public Health 2019, 16, 4656. [Google Scholar] [CrossRef] [Green Version]
- Damsgaard, C.T.; Michaelsen, K.F.; Molbo, D.; Mortensen, E.L.; Sørensen, T.I.A. Trends in adult body-mass index in 200 countries from 1975 to 2014: A pooled analysis of 1698 population-based measurement studies with 19.2 million participants. Lancet 2016, 387, 1377–1396. [Google Scholar]
- Kumar, S.; Kelly, A.S. Review of childhood obesity: From epidemiology, etiology, and comorbidities to clinical assessment and treatment. Mayo Clin. Proc. 2017, 92, 251–265. [Google Scholar] [CrossRef] [Green Version]
- Reilly, J.J.; Kelly, J. Long-term impact of overweight and obesity in childhood and adolescence on morbidity and premature mortality in adulthood: Systematic review. Int. J. Obes. 2011, 35, 891–898. [Google Scholar] [CrossRef] [Green Version]
- Franks, P.W.; McCarthy, M.I. Exposing the exposures responsible for type 2 diabetes and obesity. Science 2016, 354, 69–73. [Google Scholar] [CrossRef] [Green Version]
- Twig, G.; Yaniv, G.; Levine, H.; Leiba, A.; Goldberger, N.; Derazne, E.; Shor, D.B.-A.; Tzur, D.; Afek, A.; Shamiss, A.; et al. Body-mass index in 2.3 million adolescents and cardiovascular death in adulthood. N. Engl. J. Med. 2016, 374, 2430–2440. [Google Scholar] [CrossRef]
- Mandelbaum, R.S.; Bainvoll, L.; Violette, C.J.; Smith, M.B.; Matsuzaki, S.; Klar, M.; Ho, J.R.; Bendikson, K.A.; Paulson, R.J.; Matsuo, K. The influence of obesity on incidence of complications in patients hospitalized with ovarian hyperstimulation syndrome. Arch. Gynecol. Obstet. 2022, 305, 483–493. [Google Scholar] [CrossRef] [PubMed]
- Li, J.J.; Cha, R.T.; Luo, H.Z.; Hao, W.S.; Zhang, Y.; Jiang, X.Y. Nanomaterials for the theranostics of obesity. Biomaterials 2019, 223, 119474–119488. [Google Scholar] [CrossRef] [PubMed]
- Goodarzi, M.O. Genetics of obesity: What genetic association studies have taught us about the biology of obesity and its complications. Lancet Diabetes Endocrinol. 2018, 6, 223–236. [Google Scholar] [CrossRef]
- Fjalldal, S.; Follin, C.; Gabery, S.; Sundgren, P.C.; Björkman-Burtscher, I.M.; Lätt, J.; Mannfolk, P.; Nordström, C.H.; Rylander, L.; Ekman, B.; et al. Detailed assessment of hypothalamic damage in craniopharyngioma patients with obesity. Int. J. Obes. 2019, 4, 533–544. [Google Scholar] [CrossRef] [PubMed]
- Zhuo, C.J.; Xu, Y.; Liu, S.; Li, J.; Zheng, Q.S.; Gao, X.Y.; Li, S.; Jing, R.X.; Song, X.Q.; Yue, W.H.; et al. Topiramate and Metformin Are Effective Add-On Treatments in Controlling Antipsychotic-Induced Weight Gain: A Systematic Review and Network Meta-Analysis. Front. Pharmacol. 2018, 9, 1393–1402. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Magni, P.; Dozio, E.; Galliera, E.; Ruscica, M.; Corsi, M.M. Molecular aspects of adipokine-bone interactions. Curr. Mol. Med. 2010, 10, 522–532. [Google Scholar]
- Pories, W.J. Bariatric surgery: Risks and rewards. J. Clin. Endocrinol. Metab. 2008, 93, S89–S96. [Google Scholar] [CrossRef] [Green Version]
- Suter, M.; Calmes, J.M.; Paroz, A.; Romy, S.; Giusti, V. Results of Roux-en-Y gastric bypass in morbidly obese vs superobese patients: Similar body weight loss, correction of comorbidities, and improvement of quality of life. Arch. Surg. 2009, 144, 312–318. [Google Scholar] [CrossRef]
- Cooper, T.C.; Simmons, E.B.; Webb, K.; Burns, J.L.; Kushner, R.F. Trends in weight regain following roux-en-Y gastric bypass (RYGB) bariatric surgery. Obes. Surg. 2015, 25, 1474–1481. [Google Scholar] [CrossRef]
- Nudel, J.; Sanchez, V.M. Surgical management of obesity. Metabolism 2019, 92, 206–216. [Google Scholar] [CrossRef]
- Johansson, K.; Svensson, P.A.; Sderling, J.; Peltonen, M.; Sjholm, K. Long-term risk of anaemia after bariatric surgery: Results from the Swedish Obese Subjects study. Lancet Diabetes Endocrinol. 2021, 9, 515–524. [Google Scholar] [CrossRef]
- Jackson, V.M.; Price, D.A.; Carpino, P.A. Investigational drugs in Phase II clinical trials for the treatment of obesity: Implications for future development of novel therapies. Expert Opin. Investig. Drugs 2014, 23, 1055–1066. [Google Scholar] [CrossRef] [PubMed]
- Fasipe, O. Recent advances and current trend in the pharmacotherapy of obesity. Arch. Med. Health Sci. 2018, 6, 99. [Google Scholar] [CrossRef]
- Kennett, G.A.; Clifton, P.G. New approaches to the pharmacological treatment of obesity: Can they break through the efficacy barrier? Pharmacol. Biochem. Behav. 2010, 97, 63–83. [Google Scholar] [CrossRef] [PubMed]
- Derosa, G.; Mafoli, P. Anti-obesity drugs: A review about their effects and their safety. Expert Opin. Drug Saf. 2012, 11, 459–471. [Google Scholar] [CrossRef]
- Bray, G.A.; Greenway, F.L. Pharmacological treatment of the overweight patient. Pharmacol. Rev. 2007, 59, 151–184. [Google Scholar] [CrossRef] [Green Version]
- Kang, J.G.; Park, C.Y. Anti-obesity drugs: A review about their effects and safety. Diabetes Metab. J. 2012, 36, 13–25. [Google Scholar] [CrossRef] [Green Version]
- Krentz, A.J.; Fujioka, K.; Hompesch, M. Evolution of pharmacological obesity treatments: Focus on adverse side-effect profiles. Diabetes Obes. Metab. 2016, 18, 558–570. [Google Scholar] [CrossRef]
- Huang, D.; Deng, M.; Kuang, S.H. Polymeric carriers for controlled drug delivery in obesity treatment. Trends Endocrinol. Metab. 2019, 30, 974–989. [Google Scholar] [CrossRef]
- Srivastava, G.; Apovian, C.M. Current pharmacotherapy for obesity. Nat. Rev. Endocrinol. 2018, 14, 12–24. [Google Scholar] [CrossRef]
- Harp, J.B. Orlistat for the long-term treatment of obesity. Drugs Today (Barc) 1999, 35, 139–145. [Google Scholar] [CrossRef] [PubMed]
- Yanovski, S.Z.; Yanovski, J.A. Long-term drug treatment for obesity: A systematic and clinical review. J. Amer. Med. Assoc. 2014, 311, 74–86. [Google Scholar] [CrossRef] [PubMed]
- Filippatos, T.D.; Derdemezis, C.S.; Gazi, I.F.; Nakou, E.S.; Mikhailidis, D.P.; Elisaf, M.S. Orlistat-associated adverse effects and drug interactions: A critical review. Drug Saf. 2008, 31, 53–65. [Google Scholar] [CrossRef]
- Kim, K.O.; Lee, J.A.; Suh, H.W.; Kim, Y.S.; Kim, B.S.; Ahn, E.S.; Roh, Y.J.; Jung, S.G.; Kim, J.M.; Kang, M.K.; et al. Postmarketing surveillance study of the efficacy and safety of phentermine in patients with obesity. Korean J. Fam. Med. 2013, 34, 298–306. [Google Scholar] [CrossRef]
- Elhag, W.; Ansari, W.E.; Abdulrazzaq, S.; Elsherif, M.; Mustafa, I. Lorcaserin vs. Phentermine among non-surgical and surgical obese patients: Anthropometric, glycemic, lipid, safety and cost outcomes. Ann. Med. Surg. 2019, 45, 75–81. [Google Scholar] [CrossRef] [PubMed]
- Gustafson, A.; King, C.; Rey, J.A. Lorcaserin (Belviq): A selective serotonin 5-HT2C agonist in the treatment of obesity. Pharm. Ther. 2013, 38, 525–534. [Google Scholar]
- Greenway, F.L.; Fujioka, K.; Plodkowski, R.A.; Mudaliar, S.; Guttadauria, M.; Erickson, J.; Kim, D.D. Effect of naltrexone plus bupropion on weight loss in overweight and obese adults (COR-I): A multicentre, randomised, double-blind, placebo-controlled, phase 3 trial. Lancet 2010, 376, 595–605. [Google Scholar] [CrossRef]
- Apovian, C.M.; Aronne, L.; Rubino, D.; Still, C.; Wyatt, H.; Colleen, B. A randomized, phase 3 trial of naltrexone SR/bupropion SR on weight and obesity-related risk factors (COR-II). Obesity 2013, 21, 935–943. [Google Scholar] [CrossRef] [Green Version]
- Lonneman, D.J.; Rey, J.A.; Makee, B.D. Phentermine/topiramate extended-release capsules (Qsymia) for weight loss. Pharm. Ther. 2013, 38, 446–452. [Google Scholar]
- Bessesen, D.H.; van Gaal, L.F. Progress and challenges in anti-obesity pharmacotherapy. Lancet Diabetes Endocrinol. 2018, 6, 237–248. [Google Scholar] [CrossRef]
- Mehta, A.; Marso, S.P.; Neeland, I.J. Liraglutide for weight management: A critical review of the evidence. Obes. Sci. Pract. 2017, 3, 3–14. [Google Scholar] [CrossRef] [PubMed]
- Pi-Sunyer, X.; Astrup, A.; Fujioka, K.; Greenway, F.; Halpern, A.; Krempf, M.; Lau, D.C.W.; Roux, C.W.L.; Violante-Ortiz, R.; Jensen, C.B.; et al. A randomized, controlled trial of 3.0 mg of liraglutide in weight management. N. Engl. J. Med. 2015, 373, 11–22. [Google Scholar] [CrossRef] [PubMed]
- Wilding, J.P.H.; Jacob, S. Cardiovascular outcome trials in obesity: A review. Obes. Rev. 2021, 22, e13112–e13122. [Google Scholar] [CrossRef] [PubMed]
- Blundell, J.; Finlayson, G.; Axelsen, M.B.; Flint, A.; Gibbons, C.; Kvist, T.; Hjerpsted, J. Effects of once-weekly semaglutide on appetite, energy intake, control of eating, food preference and body weight in subjects with obesity. Diabetes Obes. Metab. 2017, 19, 1242–1251. [Google Scholar] [CrossRef]
- O’Neil, P.M.; Birkenfeld, A.L.; McGowan, B.; Mosenzon, O.; Pedersen, S.D.; Wharton, S.; Carson, C.G.; Jepsen, C.H.; Kabisch, M.; Wilding, J.P.H. Efficacy and safety of semaglutide compared with liraglutide and placebo for weight loss in patients with obesity: A randomised, double-blind, placebo and active controlled, dose-ranging, phase 2 trial. Lancet 2018, 392, 637–649. [Google Scholar] [CrossRef]
- Jackson, V.M.; Breen, D.M.; Fortin, J.P.; Liou, A.; Kuzmiski, J.B.; Loomis, A.K.; Rives, M.L.; Shah, B.; Carpino, P.A. Latest approaches for the treatment of obesity. Expert Opin. Drug Discov. 2015, 10, 825–839. [Google Scholar] [CrossRef]
- Tamrakar, A.K.; Maurya, C.K.; Rai, A.K. PTP1B inhibitors for type 2 diabetes treatment: A patent review. Expert Opin. Ther. Pat. 2014, 24, 1101–1115. [Google Scholar] [CrossRef]
- Panzhinskiy, E.; Ren, J.; Nair, S. Pharmacological inhibition of protein tyrosine phosphatase 1B: A promising strategy for the treatment of obesity and type 2 diabetes mellitus. Curr. Med. Chem. 2013, 20, 2609–2625. [Google Scholar] [CrossRef]
- Sohn, J.W.; Harris, L.E.; Berglund, E.D.; Liu, T.; Vong, L.; Lowell, B.B.; Balthasar, N.; Williams, K.W.; Elmquist, J.K. Melanocortin 4 receptors reciprocally regulate sympathetic and parasympathetic preganglionic neurons. Cell 2013, 152, 612–619. [Google Scholar] [CrossRef] [Green Version]
- Morgan, D.A.; Mcdaniel, L.N.; Yin, T.; Khan, M.; Jiang, J.W.; Acevedo, M.R.; Walsh, S.A.; Ponto, L.L.B.; Norris, A.W.; Lutter, M.; et al. Regulation of glucose tolerance and sympathetic activity by MC4R signaling in the lateral hypothalamus. Diabetes 2015, 64, 1976–1987. [Google Scholar] [CrossRef] [Green Version]
- Clément, K.; Biebermann, H.; Farooqi, I.S.; Ploeg, L.V.; Wolters, B.; Poitou, C.; Puder, L.; Fiedorek, F.; Gottesdiener, K.; Kleinau, G.; et al. MC4R agonism promotes durable weight loss in patients with leptin receptor deficiency. Nat. Med. 2018, 24, 551–555. [Google Scholar] [CrossRef] [PubMed]
- Haghighi, A.; Melka, M.G.; Bernard, M.; Abrahamowicz, M.; Leonard, G.T.; Richer, L.; Perron, M.; Veillette, S.; Xu, C.J.; Greenwood, C.M.T.; et al. Opioid receptor mu 1 gene, fat intake and obesity in adolescence. Mol. Psychiatry 2014, 19, 63–68. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Greenway, F.L.; Whitehouse, M.J.; Guttadauria, M.; Anderson, J.W.; Atkinson, R.L.; Fujioka, K.; Gadde, K.M.; Gupta, A.K.; O’Neil, P.; Schumacher, D.; et al. Rational design of a combination medication for the treatment of obesity. Obesity 2009, 17, 30–39. [Google Scholar] [CrossRef] [PubMed]
- Ignar, D.M.; Goetz, A.S.; Noble, K.N.; Carballo, L.H.; Stroup, A.E.; Fisher, J.C.; Boucheron, J.A.; Brainard, T.A.; Larkin, A.L.; Epperly, A.H.; et al. Regulation of ingestive behaviors in the rat by GSK1521498, a novel microopioid receptor-selective inverse agonist. J. Pharmacol. Exp. Ther. 2011, 339, 24–34. [Google Scholar] [CrossRef]
- Sarruf, D.A.; Thaler, J.P.; Morton, G.J.; German, J.; Fischer, J.D.; Ogimoto, K.; Schwartz, M.W. Fibroblast growth factor 21 action in the brain increases energy expenditure and insulin sensitivity in obese rats. Diabetes 2010, 59, 1817–1824. [Google Scholar] [CrossRef] [Green Version]
- Kurosu, H.; Choi, M.; Ogawa, Y.; Dickson, A.S.; Goetz, R.; Eliseenkova, A.V.; Mohammadi, M.; Rosenblatt, K.P.; Kliewer, S.A.; Kuro-O, M. Tissue-specific expression of beta Klotho and fibroblast growth factor (FGF) receptor isoforms determines metabolic activity of FGF19 and FGF21. J. Biol. Chem. 2007, 282, 26687–26695. [Google Scholar] [CrossRef] [Green Version]
- Coskun, T.; Bina, H.A.; Schneider, M.A.; Dunbar, J.D.; Hu, C.C.; Chen, Y.Y.; Moller, D.E.; Kharitonenkov, A. Fibroblast growth factor 21 corrects obesity in mice. Endocrinology 2008, 149, 6018–6027. [Google Scholar] [CrossRef]
- Xu, J.; Stanislaus, S.; Chinookoswong, N.; Lau, Y.Y.; Hager, T.; Patel, J.; Ge, H.F.; Weiszmann, J.; Lu, S.C.; Graham, M.; et al. Acute glucose-lowering and insulin sensitizing action of FGF21 in insulin resistant mouse models-association with liver and adipose tissue effects. Am. J. Physiol. Endocrinol. Metab. 2009, 297, 1105–1114. [Google Scholar] [CrossRef] [Green Version]
- Adams, A.C.; Halstead, C.A.; Hansen, B.C.; Irizarry, A.R.; Martin, J.A.; Myers, S.R.; Reynolds, V.L.; Smith, H.W.; Wroblewski, V.J.; Kharitonenkov, A. LY2405319, an engineered FGF21 variant, improves the metabolic status of diabetic monkeys. PLoS ONE 2013, 8, e65763. [Google Scholar] [CrossRef] [Green Version]
- Veniant, M.M.; Komorowski, R.; Chen, P.; Stanislaus, S.; Winters, K.; Hager, T.; Zhou, L.; Wada, R.; Hecht, R.; Xu, J. Long-acting FGF21 has enhanced efficacy in diet-induced obese mice and in obese rhesus monkeys. Endocrinology 2012, 153, 4192–4203. [Google Scholar] [CrossRef] [Green Version]
- Gaich, G.; Chien, J.Y.; Fu, H.; Glass, L.C.; Deeg, M.A.; Holland, W.L.; Kharitonenkov, A.; Bumol, T.; Schilske, H.K.; Moller, D.E. The effects of LY2405319, an FGF21 analog, in obese human subjects with type 2 diabetes. Cell Metab. 2013, 18, 333–340. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, S.; Moustaid-Moussa, N.; Chen, L.; Mo, H.; Shastri, A.; Su, R.; Bapat, P.; Kwun, I.; Shen, C.L. Novel insights of dietary polyphenols and obesity. J. Nutr. Biochem. 2014, 25, 1–18. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Howes, M.J.; Simmonds, M.S. The role of phytochemicals as micronutrients in health and disease. Curr. Opin. Clin. Nutr. Metab. Care 2014, 17, 558–566. [Google Scholar] [CrossRef] [PubMed]
- Holst, B.; Williamson, G. Nutrients and phytochemicals: From bioavailability to bioefficacy beyond antioxidants. Curr. Opin. Biotechnol. 2008, 19, 73–82. [Google Scholar] [CrossRef] [PubMed]
- Riley, R.S.; June, C.H.; Langer, R.; Mitchell, M.J. Delivery technologies for cancer immunotherapy. Nat. Rev. Drug Discov. 2019, 18, 175–196. [Google Scholar] [CrossRef]
- Zhang, Y.; Hsu, B.Y.W.; Ren, C.L.; Li, X.; Wang, J. Silica-based nanocapsules: Synthesis, structure control and biomedical applications. Chem. Soc. Rev. 2015, 44, 315–335. [Google Scholar] [CrossRef]
- Pitek, A.S.; Hu, H.; Shukla, S.; Steinmetz, N.F. Cancer theranostic applications of albumin-coated tobacco mosaic virus nanoparticles. ACS Appl. Mater. Interfaces 2018, 10, 39468–39477. [Google Scholar] [CrossRef]
- VanWijk, M.J.; VanBavel, E.; Sturk, A.; Nieuwland, R. Microparticles in cardiovascular diseases. Cardiovasc. Res. 2003, 59, 277–287. [Google Scholar] [CrossRef]
- Popovic, N.; Brundin, P. Therapeutic potential of controlled drug delivery systems in neurodegenerative diseases. Int. J. Pharm. 2006, 314, 120–126. [Google Scholar] [CrossRef]
- Rak, J. Microparticles in cancer. Semin. Thromb. Hemost. 2010, 36, 888–906. [Google Scholar] [CrossRef] [Green Version]
- Allen, R.; Chizari, S.; Ma, J.A.; Raychaudhuri, S.; Lewis, J.S. Combinatorial, microparticle-based delivery of immune modulators reprograms the dendritic cell phenotype and promotes remission of collagen-induced arthritis in mice. ACS Appl. Bio. Mater. 2019, 2, 2388–2404. [Google Scholar] [CrossRef] [PubMed]
- Lewis, J.S.; Allen, R.P. An introduction to biomaterial based strategies for curbing autoimmunity. Exp. Biol. Med. 2016, 241, 1107–1115. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Walsh, A.M.; Sweeney, T.; Bahar, B.; O’Doherty, J.V. Multi-functional roles of chitosan as a potential protective agent against obesity. PLoS ONE 2013, 8, e53828–e53834. [Google Scholar] [CrossRef]
- Pan, H.T.; Fu, C.H.; Huang, H.L.; Jiang, Y.; Deng, X.Y.; Guo, J.; Su, Z.Q. Anti-obesity effect of chitosan oligosaccharide capsules (COSCs) in obese rats by ameliorating leptin resistance and adipogenesis. Mar. Drugs 2018, 16, 198. [Google Scholar] [CrossRef] [Green Version]
- Bai, Y.B.; Zheng, J.P.; Yuan, X.B.; Jiao, S.M.; Feng, C.; Du, Y.G.; Liu, H.T.; Zheng, L.Y. Chitosan oligosaccharides improve glucolipid metabolism disorder in liver by suppression of obesity-related inflammation and restoration of peroxisome proliferator-activated receptor gamma (PPARγ). Mar. Drugs 2018, 16, 455. [Google Scholar] [CrossRef] [Green Version]
- Ash, G.I.; Kim, D.; Choudhury, M. Promises of nanotherapeutics in obesity. Trends Endocrinol. 2019, 30, 369–383. [Google Scholar] [CrossRef]
- Zhang, Y.Q.; Yu, J.C.; Qiang, L.; Gu, Z. Nanomedicine for obesity treatment. Nanomedicine for obesity treatment. Sci. China Life Sci. 2018, 61, 373–379. [Google Scholar] [CrossRef] [PubMed]
- Salah, E.; Abouelfetouh, M.M.; Pan, Y.H.; Chen, D.M.; Xie, S.Y. Solid lipid nanoparticles for enhanced oral absorption: A review. Colloid. Surf. B 2020, 196, 111305–111322. [Google Scholar] [CrossRef]
- Sharma, M.; Sharma, R.; Jain, D.K. Nanotechnology based approaches for enhancing oral bioavailability of poorly water soluble antihypertensive drugs. Scientifica 2016, 2016, 8525679. [Google Scholar] [CrossRef] [Green Version]
- Jiang, C.H.; Cano-Vega, M.A.; Yue, F.; Kuang, L.J.; Narayanan, N.; Uzunalli, G.; Merkel, M.P.; Kuang, S.H.; Deng, M. Dibenzazepine-loaded nanoparticles induce local browning of white adipose tissue to counteract obesity. Mol. Ther. 2017, 25, 1718–1729. [Google Scholar] [CrossRef] [Green Version]
- Zhang, Y.Q.; Liu, Q.G.; Yu, J.C.; Yu, S.G.; Wang, J.Q.; Qiang, L.; Gu, Z. Locally induced adipose tissue browning by microneedle patch for obesity treatment. ACS Nano 2017, 11, 9223–9230. [Google Scholar] [CrossRef] [PubMed]
- Miyano, T.; Tobinaga, Y.; Kanno, T.; Matsuzaki, Y.; Takeda, H.; Wakui, M.; Hanada, K. Sugar micro needles as transdermic drug delivery system. Biomed. Microdevices 2005, 7, 185–188. [Google Scholar] [CrossRef] [PubMed]
- Maaden, K.V.D.; Jiskoot, W.; Bouwstra, J. Microneedle technologies for (trans)dermal drug and vaccine delivery. J. Control. Release 2012, 161, 645–655. [Google Scholar] [CrossRef]
- Han, L.K.; Kimura, Y.; Okuda, H. Reduction in fat storage during chitin-chitosan treatment in mice fed a high-fat diet. Int. J. Obes. Relat. Metab. Disord. 1999, 23, 174–179. [Google Scholar] [CrossRef] [Green Version]
- Sumiyoshi, M.; Kimura, Y. Low molecular weight chitosan inhibits obesity induced by feeding a high-fat diet long-term in mice. J. Pharm. Pharmacol. 2006, 58, 201–207. [Google Scholar] [CrossRef]
- Chandy, T.; Sharma, C.P. Chitosan-as a biomaterial. Artif. Cells Blood Substit. Biotechnol. 1990, 18, 1–24. [Google Scholar] [CrossRef] [PubMed]
- Thanou, M.; Verhoef, J.C.; Junginger, H.E. Oral drug absorption enhancement by chitosan and its derivatives. Adv. Drug. Del. Rev. 2001, 52, 117–126. [Google Scholar] [CrossRef]
- Deuchi, K.; Kanauchi, O.; Imasato, Y.; Kobayashi, E. Effect of the viscosity or deacetylation degree of chitosan on fecal fat excreted from rats fed on a high-fat diet. Biosci. Biotechnol. Biochem. 1995, 59, 781–785. [Google Scholar] [CrossRef]
- Zhang, J.; Liu, J.; Li, L.; Xia, W. Dietary chitosan improves hypercholesterolemia in rats fed high-fat diets. Nutr. Res. 2008, 28, 383–390. [Google Scholar] [CrossRef]
- Jr, M.G.M.; Leibel, R.L.; Seeley, R.J.; Schwartz, M.W. Obesity and leptin resistance: Distinguishing cause from effect. Trends Endocrinol. Metab. 2010, 21, 643–651. [Google Scholar]
- Yang, X.; Zhang, J.; Chen, L.; Wu, Q.; Yu, C. Chitosan oligosaccharides enhance lipid droplets via down-regulation of PCSK9 gene expression in HepG2 cells. Exp. Cell Res. 2018, 366, 152–160. [Google Scholar] [CrossRef] [PubMed]
- Kunanusornchai, W.; Witoonpanich, B.; Tawonsawatruk, T.; Pichyangkura, R.; Chatsudthipong, V.; Muanprasat, C. Chitosan oligosaccharide suppresses synovial inflammation via AMPK activation: An in vitro and in vivo study. Pharmacol. Res. 2016, 113 Pt A, 458–467. [Google Scholar] [CrossRef]
- Zhao, D.; Wang, J.; Tan, L.; Sun, C.; Dong, J. Synthesis of N-furoyl chitosan and chito-oligosaccharides and evaluation of their antioxidant activity in vitro. Int. J. Biol. Macromol. 2013, 59, 391–395. [Google Scholar] [CrossRef] [PubMed]
- Azuma, K.; Osaki, T.; Minami, S.; Okamoto, Y. Anticancer and anti-inflammatory properties of chitin and chitosan oligosaccharides. J. Funct. Biomater. 2015, 6, 33–49. [Google Scholar] [CrossRef]
- Pan, H.T.; Yang, Q.Y.; Huang, G.D.; Ding, C.; Cao, P.Q.; Huang, L.L.; Xiao, T.C.; Guo, J.; Su, Z.Q. Hypolipidemic effects of chitosan and its derivatives in hyperlipidemic rats induced by a high-fat diet. Food Nutr. Res. 2016, 60, 31137. [Google Scholar] [CrossRef] [Green Version]
- Fu, C.H.; Jiang, Y.; Guo, J.; Su, Z.Q. Natural products with anti-obesity effects and different mechanisms of action. J. Agric. Food Chem. 2016, 64, 9571–9585. [Google Scholar] [CrossRef]
- Chiu, C.Y.; Feng, S.A.; Liu, S.H.; Chiang, M.T. Functional comparison for lipid metabolism and intestinal and fecal microflora enzyme activities between low molecular weight chitosan and chitosan oligosaccharide in high-fat-diet-fed rats. Mar. Drugs 2017, 15, 234. [Google Scholar] [CrossRef] [PubMed]
- Lehrke, M.; Lazar, M.A. The many faces of PPARγ. Cell 2005, 123, 993–999. [Google Scholar] [CrossRef] [Green Version]
- Virtue, S.; Masoodi, M.; Velagapudi, V.; Tan, C.Y.; Dale, M.; Suorti, T.; Slawik, M.; Blount, M.; Burling, K.; Campbell, M.; et al. Lipocalin prostaglandin D synthase and PPARγ2 coordinate to regulate carbohydrate and lipid metabolism in vivo. PLoS ONE 2012, 7, e39512. [Google Scholar]
- Arya, N.; Katti, D.S. Poly(d,l-lactide-co-glycolide)-chitosan composite particles for the treatment of lung cancer. Int. J. Nanomed. 2015, 10, 2997–3011. [Google Scholar]
- Koerner, J.; Horvath, D.; Herrmann, V.L.; MacKerracher, A.; Gander, B.; Yagita, H.; Rohayem, J.; Groettrup, M. PLGA-particle vaccine carrying TLR3/RIG-I ligand Riboxxim synergizes with immune checkpoint blockade for effective anti-cancer immunotherapy. Nat. Commun. 2021, 12, 2935–2950. [Google Scholar] [CrossRef] [PubMed]
- Gao, Y.; Ji, H.; Peng, L.; Gao, X.G.; Jiang, S.X. Development of PLGA-PEG-PLGA hydrogel delivery system for enhanced immunoreaction and efficacy of newcastle disease virus DNA Vaccine. Molecules 2020, 25, 2505. [Google Scholar] [CrossRef] [PubMed]
- Żywicka, B.; Krucińska, I.; Garcarek, J.; Szymonowicz, M.; Komisarczyk, A.; Rybak, Z. Biological properties of low-toxic PLGA and PLGA/PHB fibrous nanocomposite scaffolds for osseous tissue regeneration. Evaluation of potential bioactivity. Molecules 2017, 22, 1852. [Google Scholar] [CrossRef] [Green Version]
- Gower, R.M.; Boehler, R.M.; Azarin, S.M.; Ricci, C.F.; Leonard, J.N.; Shea, L.D. Modulation of leukocyte infiltration and phenotype in microporous tissue engineering scaffolds via vector induced IL-10 expression. Biomaterials 2014, 35, 2024–2031. [Google Scholar] [CrossRef] [Green Version]
- Hendley, M.A.; Murphy, K.P.; Isely, C.; Struckman, H.L.; Annamalai, P.; Gower, R.M. The host response to poly(lactide-co-glycolide) scaffolds protects mice from diet induced obesity and glucose intolerance. Biomaterials 2019, 217, 119281–119292. [Google Scholar] [CrossRef]
- Chen, H.; Ng, J.P.M.; Tan, Y.; McGrath, K.; Bishop, D.P.; Oliver, B.; Chan, Y.L.; Cortie, M.B.; Milthorpe, B.K.; Valenzuela, S.M. Gold nanoparticles improve metabolic profile of mice fed a high-fat diet. J. Nanobiotechnol. 2018, 16, 11–22. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, H.; Ng, J.P.M.; Bishop, B.P.; Milthorpe, B.K.; Valenzuela, S.M. Gold nanoparticles as cell regulators: Beneficial effects of gold nanoparticles on the metabolic profile of mice with pre-existing obesity. J. Nanobiotechnol. 2018, 16, 88–100. [Google Scholar] [CrossRef] [Green Version]
- Ansari, S.A.; Baria, A.; Ullah, R.; Mathanmohun, M.; Veeraraghavan, V.P.; Sun, Z.W. Gold nanoparticles synthesized with Smilax glabra rhizome modulates the anti-obesity parameters in high-fat diet and streptozotocin induced obese diabetes rat model. J. Photoch. Photobiol. B 2019, 201, 111643–111652. [Google Scholar] [CrossRef]
- Han, S.; Kim, Y.H. Polypyrrole-coated hollow gold nanoshell exerts anti-obesity effects via photothermal lipolysis. Colloid Surf. A 2019, 570, 414–419. [Google Scholar] [CrossRef]
- Lee, J.H.; Jeong, H.S.; Lee, D.H.; Beack, S.; Kim, T.; Lee, G.H.; Park, W.C.; Kim, C.; Kim, K.S.; Hahn, S.K. Targeted hyaluronate-hollow gold nanosphere conjugate for anti-obesity photothermal lipolysis. ACS Biomater. Sci. Eng. 2017, 3, 3646–3653. [Google Scholar] [CrossRef]
- Joyce, P.; Dening, T.J.; Meola, T.R.; Wignall, A.; Ulmefors, H.; Kovalainen, M.; Prestidge, C.A. Contrasting anti-obesity effects of smectite clays and mesoporous silica in Sprague-Dawley rats. ACS Appl. Bio. Mater. 2020, 3, 7779–7788. [Google Scholar] [CrossRef] [PubMed]
- Ma, P.; He, P.; Xu, C.Y.; Hou, B.Y.; Qiang, G.F.; Du, G.H. Recent developments in natural products for white adipose tissue browning. Chin. J. Nat. Medicines 2020, 18, 803–817. [Google Scholar] [CrossRef]
- Zhang, W.T.; Sheng, T.; Gu, Z.; Zhang, Y.Q. Strategies for browning agent delivery. Pharm. Res. 2021, 38, 1327–1334. [Google Scholar] [CrossRef] [PubMed]
- McClements, D.J. Advances in nanoparticle and microparticle delivery systems for increasing the dispersibility, stability, and bioactivity of phytochemicals. Biotechnol. Adv. 2020, 38, 107287. [Google Scholar] [CrossRef] [PubMed]
- Wang, P.; Li, D.T.; Ke, W.X.; Liang, D.; Hu, X.S.; Chen, F. Resveratrol-induced gut microbiota reduces obesity in high-fat diet-fed mice. Int. J. Obes. 2020, 44, 213–225. [Google Scholar] [CrossRef]
- Zu, Y.J.; Zhao, L.; Hao, L.; Mechref, Y.; Zabet-Moghaddam, M.; Keyel, P.A.; Abbasi, M.; Wu, D.Y.; Dawson, J.A.; Zhang, R.W.; et al. Browning white adipose tissue using adipose stromal cell-targeted resveratrol-loaded nanoparticles for combating obesity. J. Control. Release 2021, 333, 339–351. [Google Scholar] [CrossRef]
- Zu, Y.J.; Overby, H.; Ren, G.Y.; Fan, Z.Y.; Zhao, L.; Wang, S. Resveratrol liposomes and lipid nanocarriers: Comparison of characteristics and inducing browning of white adipocytes. Colloid. Surf. B 2018, 164, 414–423. [Google Scholar] [CrossRef] [Green Version]
- Ahmad, M.; Gani, A. Development of novel functional snacks containing nano-encapsulated resveratrol with anti-diabetic, anti-obesity and antioxidant properties. Food Chem. 2021, 352, 129323–129330. [Google Scholar] [CrossRef]
- Rondanelli, M.; Opizzi, A.; Perna, S.; Faliva, M.; Solerte, S.B.; Fioravanti, M.; Klersy, C.; Cava, E.; Paolini, M.; Scavone, L.; et al. Improvement in insulin resistance and favourable changes in plasma inflammatory adipokines after weight loss associated with two months’ consumption of a combination of bioactive food ingredients in overweight subjects. Endocrine 2013, 44, 391–401. [Google Scholar] [CrossRef] [Green Version]
- Joo, J.I.; Kim, D.H.; Choi, J.W.; Yun, J.W. Proteomic analysis for antiobesity potential of capsaicin on white adipose tissue in rats fed with a high fat diet. J. Proteome Res. 2010, 9, 2977–2987. [Google Scholar] [CrossRef]
- Lacatusu, I.; Badea, N.; Udeanu, D.; Coc, L.; Pop, A.; Negut, C.C.; Tanase, C.; Stan, R.; Meghea, A. Improved anti-obesity effect of herbal active and endogenous lipids coloaded lipid nanocarriers: Preparation, in vitro and in vivo evaluation. Mat. Sci. Eng. C-Mater. 2019, 99, 12–24. [Google Scholar] [CrossRef] [PubMed]
- Bao, C.; Li, Z.K.; Liang, S.; Hu, Y.L.; Wang, X.Y.; Fang, B.; Wang, P.J.; Chen, S.N.; Li, Y. Microneedle patch delivery of capsaicin-containing α-lactalbumin nanomicelles to adipocytes achieves potent anti-obesity effects. Adv. Funct. Mater. 2021, 31, 2011130. [Google Scholar] [CrossRef]
- Dangol, M.; Kim, S.; Li, C.G.; Lahiji, S.F.; Jang, M.Y.; Ma, Y.H.; Huh, I.; Jung, H. Anti-obesity effect of a novel caffeine-loaded dissolving microneedle patch in high-fat diet-induced obese C57BL/6J mice. J. Control. Release 2017, 265, 41–47. [Google Scholar] [CrossRef]
- Chen, X.; He, X.Y.; Gao, R.X.; Lan, X.Y.; Zhu, L.J.; Chen, K.; Hu, Y.Z.; Huang, K.L.; Xu, W.T. Aptamer-functionalized binary-drug delivery system for synergetic obesity therapy. ACS Nano 2022, 16, 1036–1050. [Google Scholar] [CrossRef] [PubMed]
- Gao, M.; Ma, Y.; Alsaggar, M.; Liu, D. Dual outcomes of rosiglitazone treatment on fatty liver. AAPS J. 2016, 18, 1023–1031. [Google Scholar] [CrossRef] [PubMed]
- Ahmadian, M.; Suh, J.M.; Hah, N.; Liddle, C.; Atkins, A.R.; Downes, M.; Evans, R.M. PPARγ signaling and metabolism: The good, the bad and the future. Nat. Med. 2013, 19, 557–566. [Google Scholar] [CrossRef] [Green Version]
- Mascolo, D.D.; Lyon, C.J.; Aryal, S.; Ramirez, M.R.; Wang, J.; Candeloro, P.; Guindani, M.; Hsueh, W.A.; Decuzzi, P. Rosiglitazone-loaded nanospheres for modulating macrophage-specific inflammation in obesity. J. Control. Release 2013, 170, 460–468. [Google Scholar] [CrossRef] [Green Version]
- Wanner, M.; Mihn, C.M.; Farinelli, A.W.; Doukas, A.; Zurakowski, D. Use of photodynamic therapy and sterile water to target adipose tissue. Dermatol. Surg. 2015, 41, 803–811. [Google Scholar] [CrossRef]
- Chen, R.H.; Huang, S.S.; Lin, T.T.; Ma, H.S.; Shan, W.J.; Duan, F.; Lv, J.; Zhang, J.D.; Ren, L.; Nie, L.M. Photoacoustic molecular imaging-escorted adipose photodynamic-browning synergy for fighting obesity with viruslike complexes. Nat. Nanotechnol. 2021, 16, 455–465. [Google Scholar] [CrossRef]
- Than, A.; Duong, P.K.; Zan, P.; Liu, J.J.; Leow, M.K.S.; Chen, P. Lancing drug reservoirs into subcutaneous fat to combat obesity and associated metabolic diseases. Small 2020, 16, 2002872. [Google Scholar] [CrossRef]
- Ding, Z.H.; Chen, M.H.; Tao, X.Y.; Liu, Y.; He, J.; Wang, T.; Li, X.H. Synergistic treatment of obesity via locally promoting beige adipogenesis and antioxidative defense in adipose tissues. ACS Biomater. Sci. Eng. 2021, 7, 727–738. [Google Scholar] [CrossRef] [PubMed]
- Dening, T.J.; Joyce, P.; Kovalainen, M.; Gustafsson, H.; Prestidge, C.A. Spray dried Smectite clay particles as a novel treatment against obesity. Pharm. Res. 2018, 36, 2–15. [Google Scholar] [CrossRef] [PubMed]
- Joyce, P.; Dening, T.J.; Meola, T.R.; Gustafsson, H.; Kovalainen, M.; Prestidge, C.A. Nanostructured clay particles supplement orlistat action in inhibiting lipid digestion: An in vitro evaluation for the treatment of obesity. Eur. J. Pharm. Sci. 2019, 135, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Zhu, C.Z.; Li, W.J.; Wang, X.H.; Xue, J.H.; Zhao, L.; Song, Y.F.; Zhou, T.; Zhang, M.J. Thiopental sodium loaded solid lipid nanoparticles attenuates obesity-induced cardiac dysfunction and cardiac hypertrophy via inactivation of inflammatory pathway. Drug Deliv. 2020, 27, 1188–1200. [Google Scholar] [CrossRef]
- Rocha, V.Z.; Libby, P. Obesity, inflammation, and atherosclerosis. Nat. Rev. Cardiol. 2009, 6, 399–409. [Google Scholar] [CrossRef]
- Saltiel, A.R.; Olefsky, J.M. Inflammatory mechanisms linking obesity and metabolic disease. J. Clin. Investig. 2017, 127, 1–4. [Google Scholar] [CrossRef] [Green Version]
- Ellulu, M.S.; Patimah, I.; Khaza’ai, H.; Rahmat, A.; Abed, Y. Obesity and inflammation: The linking mechanism and the complications. Arch. Med. Sci. 2017, 13, 851–863. [Google Scholar] [CrossRef]
- Castegna, A.; Gissi, R.; Menga, A.; Montopoli, M.; Favia, M.; Viola, A.; Canton, M. Pharmacological targets of metabolism in disease: Opportunities from macrophages. Pharmacol. Ther. 2020, 210, 107521. [Google Scholar] [CrossRef]
- Xu, C.M.; Yin, L.Q.; Teng, Z.P.; Zhou, X.M.; Li, W.J.; Lai, Q.; Peng, C.P.; Zhang, C.Y.; Lou, J.; Zhou, X. Prevention of obesity related diseases through laminarin-induced targeted delivery of bindarit. Theranostics 2020, 10, 9544–9560. [Google Scholar] [CrossRef]
- Chen, L.W.; Chen, P.H.; Yen, J.H. Inhibiting adipose tissue M1 cytokine expression decreases DPP4 activity and insulin resistance in a type 2 diabetes mellitus mouse model. PLoS ONE 2021, 16, e0252153. [Google Scholar] [CrossRef]
- Flynn, M.C.; Pernes, G.; Lee, M.K.S.; Nagareddy, P.R.; Murphy, A.J. Monocytes, macrophages, and metabolic disease in atherosclerosis. Front. Pharmacol. 2019, 10, 666–678. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Geginat, J.; Paroni, M.; Maglie, S.; Alfen, J.S.; Kastirr, I.; Gruarin, P.; Simone, M.D.; Pagani, M.; Abrignani, S. Plasticity of human CD4 T cell subsets. Front. Immunol. 2014, 5, 630. [Google Scholar] [CrossRef] [PubMed]
- Mills, C.D. M1 and M2 macrophages: Oracles of health and disease. Crit. Rev. Immunol. 2012, 32, 463–488. [Google Scholar] [CrossRef] [Green Version]
- Youngblood, R.; Flesher, C.G.; Delproposto, J.; Baker, N.A.; Neeley, C.K.; Li, F.H.; Lumeng, C.N.; Shea, L.D.; O’Rourke, R.W. Regulation of adipose tissue inflammation and systemic metabolism in murine obesity by polymer implants loaded with lentiviral vectors encoding human interleukin-4. Biotechnol. Bioeng. 2020, 117, 3891–3901. [Google Scholar] [CrossRef] [PubMed]
- Asadullah, K.; Sterry, W.; Volk, H.D. Interleukin-10 therapy-review of a new approach. Pharmacol. Rev. 2003, 55, 241–269. [Google Scholar] [CrossRef] [PubMed]
- Ouyang, W.; Rutz, S.; Crellin, N.K.; Valdez, P.A.; Hymowitz, S.G. Regulation and functions of the IL-10 family of cytokines in inflammation and disease. Annu. Rev. Immunol. 2011, 29, 71–109. [Google Scholar] [CrossRef] [PubMed]
- Toita, R.; Kawano, T.; Murata, M.; Kang, J.H. Anti-obesity and anti-inflammatory effects of macrophage-targeted interleukin-10-conjugated liposomes in obese mice. Biomaterials 2016, 110, 81–88. [Google Scholar] [CrossRef]
- Hu, X.; Li, Z.; Xue, Y.; Xu, J.; Xue, C.; Wang, J.; Wang, Y. Dietary saponins of sea cucumber ameliorate obesity, hepatic steatosis, and glucose intolerance in high-fat diet-fed mice. J. Med. Food 2012, 15, 909–916. [Google Scholar] [CrossRef]
- Chen, C.; Han, X.Q.; Dong, P.; Li, Z.J.; Yanagita, T.; Xue, C.H.; Zhang, T.T.; Wang, Y.M. Sea cucumber saponin liposomes ameliorate obesity-induced inflammation and insulin resistance in high-fat-diet-fed mice. Food Funct. 2018, 9, 861–870. [Google Scholar] [CrossRef]
- Sibuyi, N.R.S.; Moabelo, K.L.; Meyer, M.; Onani, M.O.; Dube, A.; Madiehe, A.M. Nanotechnology advances towards development of targeted-treatment for obesity. J. Nanobiotechnol. 2019, 17, 122–142. [Google Scholar] [CrossRef]
- Tong, Y.; Zhang, Y.; Shan, Z.Z.; Xu, Y.M.; Gao, X.D.; Yao, W.B. Improving high-fat diet-induced obesity and fatty liver by adipose tissue targeted delivery of vascular endothelial growth factor-B. Life Sci. 2020, 253, 117677–117685. [Google Scholar] [CrossRef] [PubMed]
- Kolonin, M.G.; Saha, P.K.; Chan, L.; Pasqualini, R.; Arap, W. Reversal of obesity by targeted ablation of adipose tissue. Nat. Med. 2004, 10, 625–632. [Google Scholar] [CrossRef] [PubMed]
- Barnhart, K.F.; Christianson, D.R.; Hanley, P.W.; Driessen, W.H.P.; Bernacky, B.J.; Baze, W.B.; Wen, S.J.; Tian, M.; Ma, J.F.; Kolonin, M.G.; et al. A peptidomimetic targeting white fat causes weight loss and improved insulin resistance in obese monkeys. Sci. Transl. Med. 2011, 3, 108–112. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hossen, M.N.; Kajimoto, K.; Akita, H.; Hyodo, M.; Harashima, H. A comparative study between nanoparticle-targeted therapeutics and bioconjugates as obesity medication. J. Control. Release 2013, 171, 104–112. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shen, D.; Gao, J.F.; Xia, J.; Wang, X.Y.; Zhou, Y.H.; Chen, L.; Xu, L.L.; Guo, X.R. Liposome-encapsulated peptide PDBSN ameliorates high-fat-diet induced obesity and improves metabolism homeostasis. Biochem. Bioph. Res. Commun. 2020, 533, 181–187. [Google Scholar] [CrossRef]
- Dagon, Y.; Avraham, Y.; Berry, E.M. AMPK activation regulates apoptosis, adipogenesis, and lipolysis by eIF2a in adipocytes. Biochem. Biophys. Res. Commun. 2006, 340, 43–47. [Google Scholar] [CrossRef]
- Zhang, L.; Wang, M.; Chen, M.; Niu, W.; Liu, W.G.; Leng, T.T.; Ji, W.C.; Lei, B. A safe and efficient bioactive citrate-lysine/miRNA33 agonist nanosystem for high fat diet-induced obesity therapy. Chem. Eng. J. 2021, 408, 127304–127316. [Google Scholar] [CrossRef]
- Pan, S.F.; Yang, X.J.; Jia, Y.M.; Li, Y.; Chen, R.R.; Wang, M.; Cai, D.M.; Zhao, R.Q. Intravenous injection of microvesicle delivery miR-130b alleviates high-fat diet induced obesity in C57BL/6 mice through translational repression of PPAR-γ. J. Biomed. Sci. 2015, 22, 86–97. [Google Scholar] [CrossRef] [Green Version]
- Yuan, D.F.; Yi, X.; Zhao, Y.L.; Poon, C.D.; Bullock, K.M.; Hansen, K.M.; Salameh, T.S.; Farr, S.A.; Banks, W.A.; Kabanov, A.V. Intranasal delivery of N-terminal modified leptin-pluronic conjugate for treatment of obesity. J. Control Release 2017, 263, 172–184. [Google Scholar] [CrossRef]
- Tunnemann, G.; Martin, R.M.; Haupt, S.; Patsch, C.; Edenhofer, F.; Cardoso, M.C. Cargo-dependent mode of uptake and bioavailability of TAT-containing proteins and peptides in living cells. FASEB J. 2006, 20, 1775–1784. [Google Scholar] [CrossRef] [Green Version]
- Khafagy, E.S.; Kamei, N.; Fujiwara, Y.; Okumura, H.; Yuasa, T.; Kato, M.; Arime, K.; Nonomura, A.; Ogino, H.; Hirano, S.; et al. Systemic and brain delivery of leptin via intranasal coadministration with cell-penetrating peptides and its therapeutic potential for obesity. J. Control Release 2020, 319, 397–406. [Google Scholar] [CrossRef] [PubMed]
- Behary, P.; Tharakan, G.; Alexiadou, K.; Johnson, N.; Albrechtsen, N.J.W.; Kenkre, J.; Cuenco, J.; Hope, D.; Anyiam, O.; Choudhury, S.; et al. Combined GLP-1, oxyntomodulin, and peptide YY improves body weight and glycemia in obesity and prediabetes/type 2 diabetes: A randomized single-blinded placebo controlled study. Diabetes Care 2019, 42, 1446–1453. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ma, T.; Huo, S.; Xu, B.; Li, F.F.; Wang, P.L.; Liu, Y.G.; Lei, H.M. A novel long-acting oxyntomodulin analogue eliminates diabetes and obesity in mice. Eur. J. Med. Chem. 2020, 203, 112496–112507. [Google Scholar] [CrossRef]
- Zhang, Z.M.; Liu, X.B.; Morgan, D.A.; Kuburas, A.; Thedens, D.R.; Russo, A.F.; Rahmouni, K. Neuronal receptor activity-modifying protein 1 promotes energy expenditure in mice. Diabetes 2011, 60, 1063–1071. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Boström, P.; Wu, J.; Jedrychowski, M.P.; Korde, A.; Ye, L.; Lo, J.C.; Rasbach, K.A.; Boström, E.A.; Choi, J.H.; Long, J.Z.; et al. A PGC1-α-dependent myokine that drives brown-fat-like development of white fat and thermogenesis. Nature 2012, 481, 463–468. [Google Scholar] [CrossRef] [PubMed]
- Park, H.; Cho, S.; Janat-Amsbury, M.M.; Bae, Y.H. Enhanced thermogenic program by non-viral delivery of combinatory browning genes to treat diet-induced obesity in mice. Biomaterials 2015, 73, 32–41. [Google Scholar] [CrossRef]
- Smith, R.; Duguay, A.; Weiszmann, J.; Stanislaus, S.; Belouski, E.; Cai, L.; Yie, J.M.; Xu, J.; Gupte, J.; Wu, X.L.; et al. A novel approach to improve the function of FGF21. BioDrugs 2013, 27, 159–166. [Google Scholar] [CrossRef] [PubMed]
- Yin, J.; Bao, L.C.; Tian, H.; Wang, Q.; Gao, X.D.; Yao, W.B. Genetic fusion of human FGF21 to a synthetic polypeptide improves pharmacokinetics and pharmacodynamics in a mouse model of obesity. Br. J. Pharmacol. 2016, 173, 2208–2223. [Google Scholar] [CrossRef] [Green Version]
- Won, Y.W.; Adhikary, P.P.; Lim, K.S.; Kim, H.J.; Kim, J.K.; Kim, Y.H. Oligopeptide complex for targeted non-viral gene delivery to adipocytes. Nat. Mater. 2014, 13, 1157–1164. [Google Scholar] [CrossRef]
- Chung, J.Y.; Ain, Q.U.; Song, Y.; Yong, S.B.; Kim, Y.H. Targeted delivery of CRISPR interference system against Fabp4 to white adipocytes ameliorates obesity, inflammation, hepatic steatosis, and insulin resistance. Genome Res. 2019, 29, 1442–1452. [Google Scholar] [CrossRef] [Green Version]






| Drug | Mechanism of Action | Delivery Mode | Side Effects | Reference |
|---|---|---|---|---|
| Orlistat | Increase intestinal lipid excretion and block the absorption of fat | Oral administration | Diarrhea, flatulence | [34] |
| Phentermine | Work through central nervous system pathways to reduce appetite | Insomnia, constipation, palpitation, dry mouth | [35,36] | |
| Lorcaserin | Headache, dizziness, fatigue, nausea, dry mouth | [37] | ||
| Naltrexone/bupropion sustained-release | Nausea, headache, constipation, dizziness, vomiting, dry mouth | [38,39] | ||
| Phentermine/topiramate extended release | Insomnia, constipation, dizziness, taste disorders | [40] | ||
| Liraglutide | Induce satiety by delaying gastric emptying | Hypodermic injection | Nausea, vomiting, diarrhea, constipation, dyspepsia | [43] |
| Semaglutide | Nausea, bloating, diarrhea, and vomiting | [45,46] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Li, J.; Duan, H.; Liu, Y.; Wang, L.; Zhou, X. Biomaterial-Based Therapeutic Strategies for Obesity and Its Comorbidities. Pharmaceutics 2022, 14, 1445. https://doi.org/10.3390/pharmaceutics14071445
Li J, Duan H, Liu Y, Wang L, Zhou X. Biomaterial-Based Therapeutic Strategies for Obesity and Its Comorbidities. Pharmaceutics. 2022; 14(7):1445. https://doi.org/10.3390/pharmaceutics14071445
Chicago/Turabian StyleLi, Jing, Hongli Duan, Yan Liu, Lu Wang, and Xing Zhou. 2022. "Biomaterial-Based Therapeutic Strategies for Obesity and Its Comorbidities" Pharmaceutics 14, no. 7: 1445. https://doi.org/10.3390/pharmaceutics14071445