
The Association between ABCG2 421C>A (rs2231142) Polymorphism and Rosuvastatin Pharmacokinetics: A Systematic Review and Meta-Analysis


Abstract
:1. Introduction
2. Materials and Methods
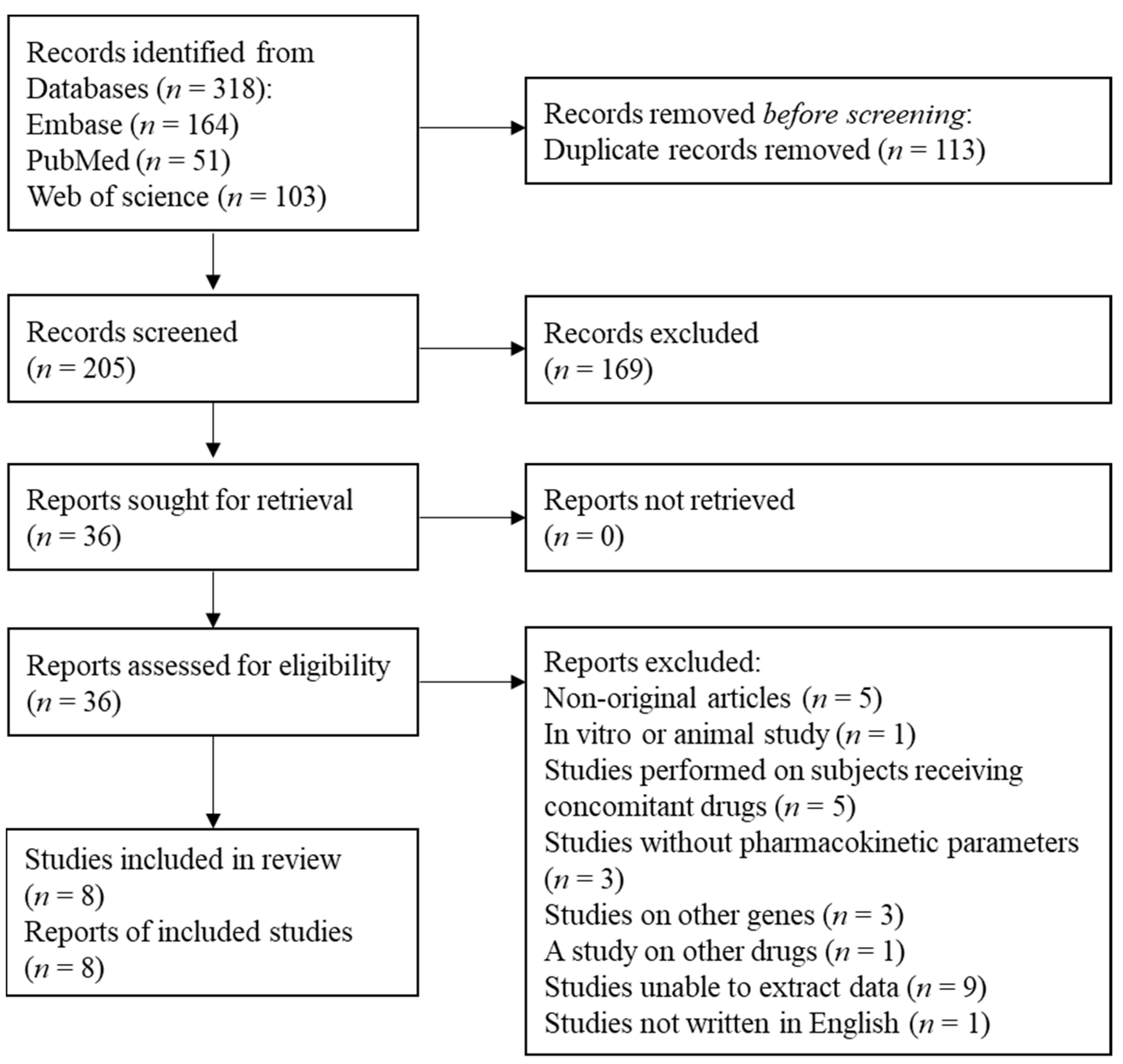
2.1. Search Strategy and Study Selection
2.2. Data Extraction and Study Quality Assessment
2.3. Statistical Analysis
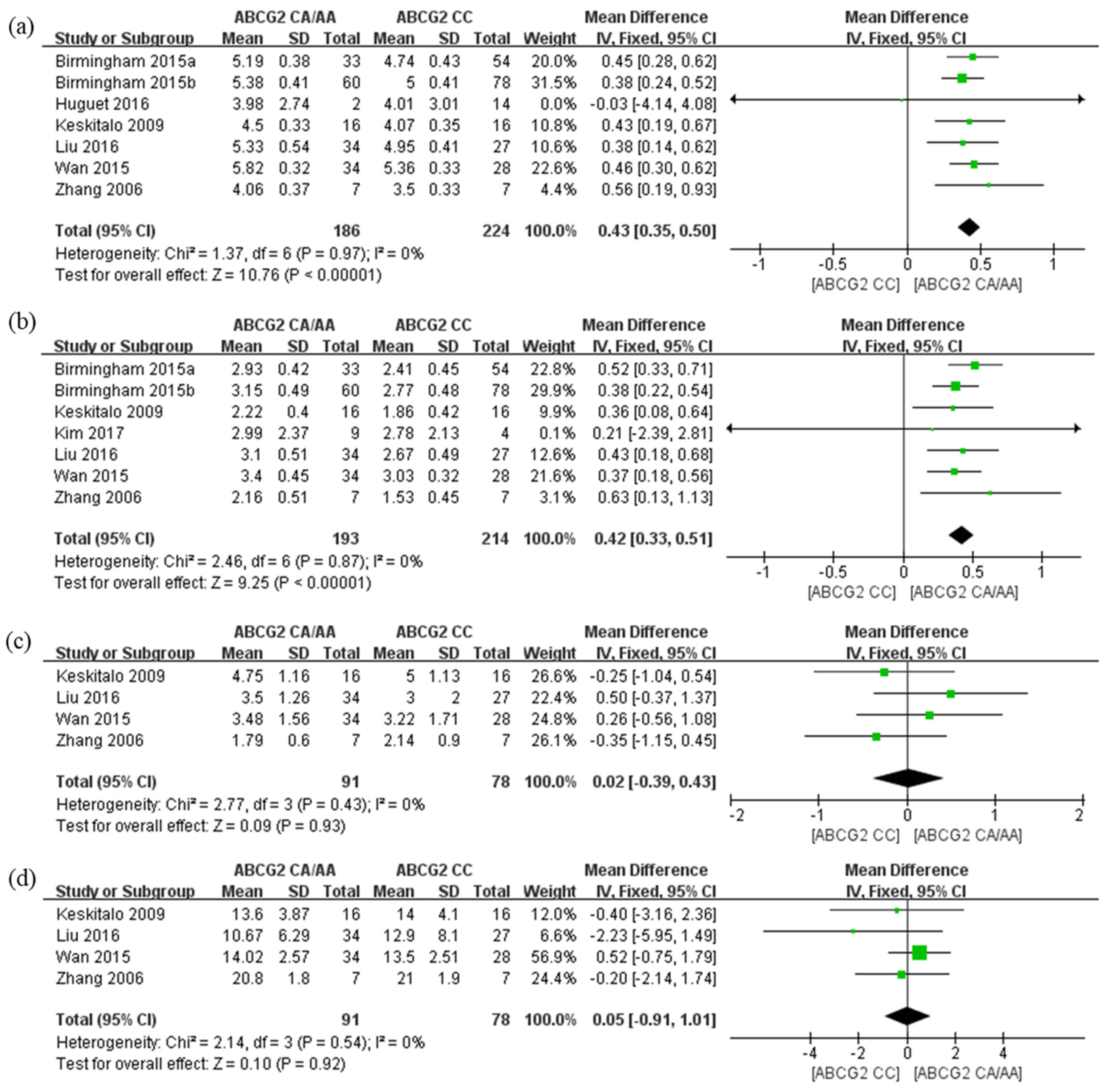
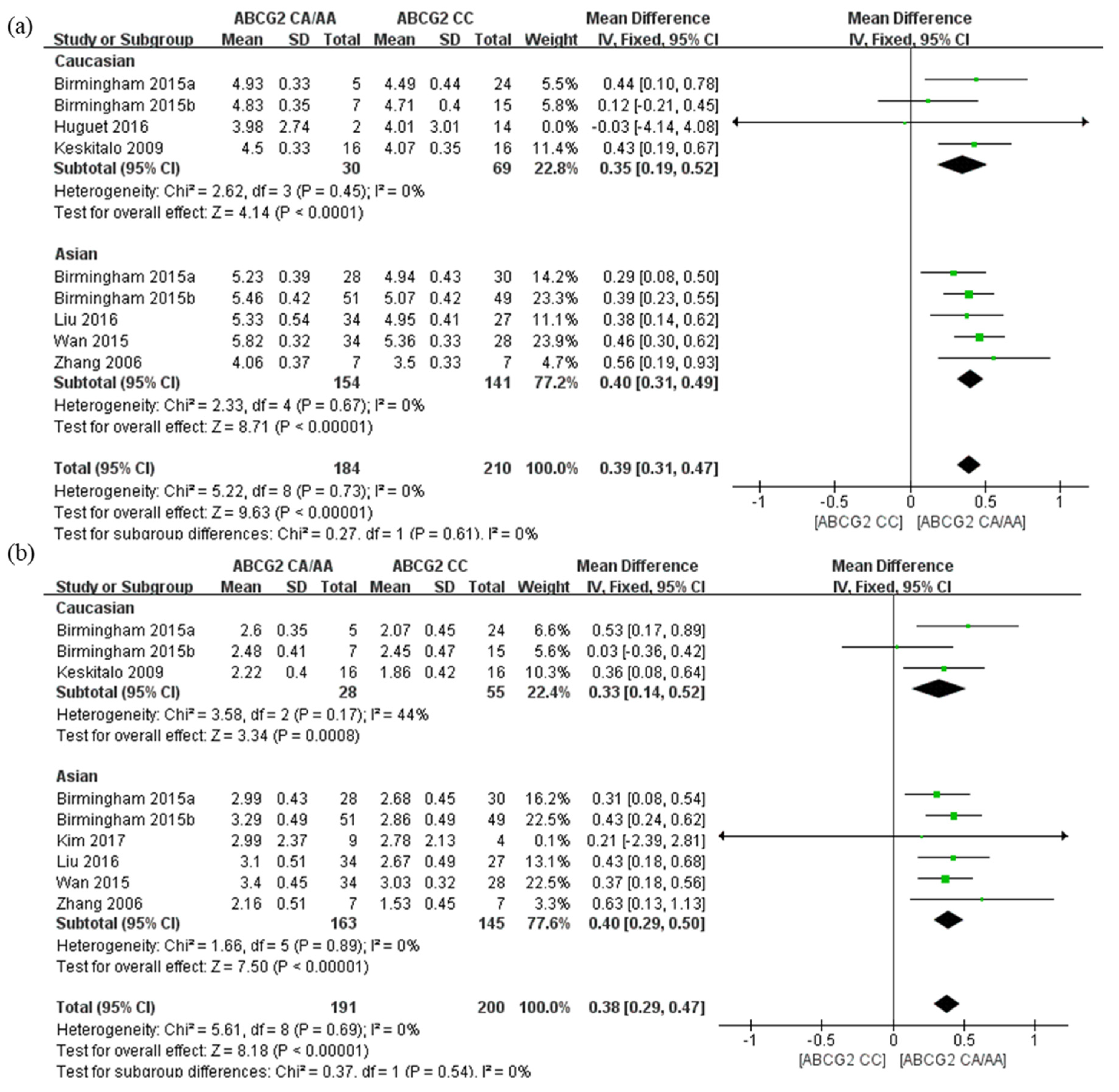
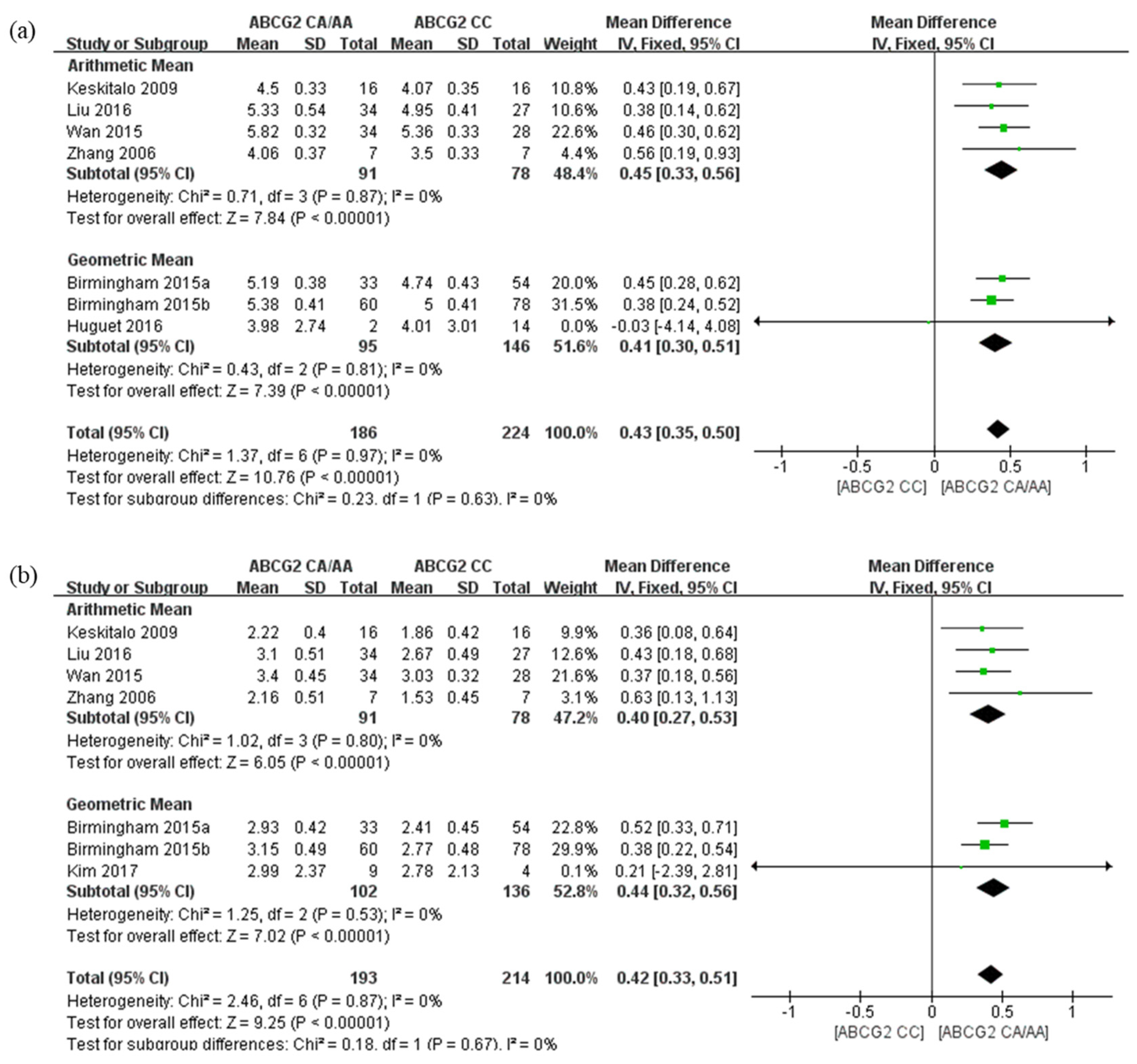
3. Results
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Nezasa, K.; Takao, A.; Kimura, K.; Takaichi, M.; Inazawa, K.; Koike, M. Pharmacokinetics and disposition of rosuvastatin, a new 3-hydroxy-3-methylglutaryl coenzyme A reductase inhibitor, in rat. Xenobiotica 2002, 32, 715–727. [Google Scholar] [CrossRef] [PubMed]
- Brewer, H.B., Jr. Benefit-risk assessment of Rosuvastatin 10 to 40 milligrams. Am. J. Cardiol. 2003, 92, 23K–29K. [Google Scholar] [CrossRef]
- Huguet, J.; Lu, J.; Gaudette, F.; Chiasson, J.L.; Hamet, P.; Michaud, V.; Turgeon, J. No effects of pantoprazole on the pharmacokinetics of rosuvastatin in healthy subjects. Eur. J. Clin. Pharmacol. 2016, 72, 925–931. [Google Scholar] [CrossRef] [PubMed]
- Kitamura, S.; Maeda, K.; Wang, Y.; Sugiyama, Y. Involvement of multiple transporters in the hepatobiliary transport of rosuvastatin. Drug Metab. Dispos. 2008, 36, 2014–2023. [Google Scholar] [CrossRef] [Green Version]
- Ho, R.H.; Tirona, R.G.; Leake, B.F.; Glaeser, H.; Lee, W.; Lemke, C.J.; Wang, Y.; Kim, R.B. Drug and bile acid transporters in rosuvastatin hepatic uptake: Function, expression, and pharmacogenetics. Gastroenterology 2006, 130, 1793–1806. [Google Scholar] [CrossRef]
- Hardwick, L.J.; Velamakanni, S.; van Veen, H.W. The emerging pharmacotherapeutic significance of the breast cancer resistance protein (ABCG2). Br. J. Pharmacol. 2007, 151, 163–174. [Google Scholar] [CrossRef] [Green Version]
- Willis, B.A.; Andersen, S.W.; Ayan-Oshodi, M.; James, D.E.; Liffick, E.; Hillgren, K.; Guo, Y.; Monk, S.A. Assessment of Transporter Polymorphisms as a Factor in a BCRP Drug Interaction Study With Lanabecestat. J. Clin. Pharmacol. 2020, 60, 107–116. [Google Scholar] [CrossRef]
- Keskitalo, J.E.; Zolk, O.; Fromm, M.F.; Kurkinen, K.J.; Neuvonen, P.J.; Niemi, M. ABCG2 polymorphism markedly affects the pharmacokinetics of atorvastatin and rosuvastatin. Clin. Pharmacol. Ther. 2009, 86, 197–203. [Google Scholar] [CrossRef]
- Morisaki, K.; Robey, R.W.; Ozvegy-Laczka, C.; Honjo, Y.; Polgar, O.; Steadman, K.; Sarkadi, B.; Bates, S.E. Single nucleotide polymorphisms modify the transporter activity of ABCG2. Cancer Chemother. Pharmacol. 2005, 56, 161–172. [Google Scholar] [CrossRef] [Green Version]
- Zhang, W.; Yu, B.N.; He, Y.J.; Fan, L.; Li, Q.; Liu, Z.Q.; Wang, A.; Liu, Y.L.; Tan, Z.R.; Fen-Jiang Huang, Y.F.; et al. Role of BCRP 421C>A polymorphism on rosuvastatin pharmacokinetics in healthy Chinese males. Clin. Chim. Acta 2006, 373, 99–103. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. Ann. Intern. Med. 2009, 6, 264–269. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wells, G.A.; Shea, B.; O’Connell, D.; Peterson, J.; Welch, V.; Losos, M.; Tugwell, P. The Newcastle-Ottawa Scale (NOS) for Assessing the Quality of Nonrandomised Studies in Meta-Analyses. 2020. Available online: http://www.ohri.ca/programs/clinical_epidemiology/oxford.asp (accessed on 18 January 2022).
- Rosenson, R.S. Rosuvastatin: A new inhibitor of HMG-coA reductase for the treatment of dyslipidemia. Expert. Rev. Cardiovasc. Ther. 2003, 1, 495–505. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.P.; White, I.R.; Anzures-Cabrera, J. Meta-analysis of skewed data: Combining results reported on log-transformed or raw scales. Stat. Med. 2008, 27, 6072–6092. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Higgins, J.P.; Thompson, S.G. Quantifying heterogeneity in a meta-analysis. Stat. Med. 2002, 21, 1539–1558. [Google Scholar] [CrossRef]
- DerSimonian, R.; Laird, N. Meta-analysis in clinical trials. Control. Clin. Trials 1986, 7, 177–188. [Google Scholar] [CrossRef]
- Egger, M.; Davey Smith, G.; Schneider, M.; Minder, C. Bias in meta-analysis detected by a simple, graphical test. BMJ 1997, 315, 629–634. [Google Scholar] [CrossRef] [Green Version]
- Begg, C.B.; Mazumdar, M. Operating characteristics of a rank correlation test for publication bias. Biometrics 1994, 50, 1088–1101. [Google Scholar] [CrossRef]
- Birmingham, B.K.; Bujac, S.R.; Elsby, R.; Azumaya, C.T.; Wei, C.; Chen, Y.; Mosqueda-Garcia, R.; Ambrose, H.J. Impact of ABCG2 and SLCO1B1 polymorphisms on pharmacokinetics of rosuvastatin, atorvastatin and simvastatin acid in Caucasian and Asian subjects: A class effect? Eur. J. Clin. Pharmacol. 2015, 71, 341–355. [Google Scholar] [CrossRef]
- Birmingham, B.K.; Bujac, S.R.; Elsby, R.; Azumaya, C.T.; Zalikowski, J.; Chen, Y.; Kim, K.; Ambrose, H.J. Rosuvastatin pharmacokinetics and pharmacogenetics in Caucasian and Asian subjects residing in the United States. Eur. J. Clin. Pharmacol. 2015, 71, 329–340. [Google Scholar] [CrossRef]
- Kim, T.E.; Ha, N.; Kim, Y.; Kim, H.; Lee, J.W.; Jeon, J.Y.; Kim, M.G. Effect of epigallocatechin-3-gallate, major ingredient of green tea, on the pharmacokinetics of rosuvastatin in healthy volunteers. Drug Des. Dev. Ther. 2017, 11, 1409–1416. [Google Scholar] [CrossRef] [Green Version]
- Liu, M.; Wu, X.J.; Zhao, G.L.; Zhang, T.; Xu, S.S.; Sun, Y.X.; Qiu, F.; Zhao, L.M. Effects of Polymorphisms in NR1H4, NR1I2, SLCO1B1, and ABCG2 on the Pharmacokinetics of Rosuvastatin in Healthy Chinese Volunteers. J. Cardiovasc. Pharmacol. 2016, 68, 383–390. [Google Scholar] [CrossRef] [PubMed]
- Wan, Z.; Wang, G.; Li, T.; Xu, B.; Pei, Q.; Peng, Y.; Sun, H.; Cheng, L.; Zeng, Y.; Yang, G.; et al. Marked Alteration of Rosuvastatin Pharmacokinetics in Healthy Chinese with ABCG2 34G>A and 421C>A Homozygote or Compound Heterozygote. J. Pharmacol. Exp. Ther. 2015, 354, 310–315. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, H.K.; Hu, M.; Lui, S.S.; Ho, C.S.; Wong, C.K.; Tomlinson, B. Effects of polymorphisms in ABCG2, SLCO1B1, SLC10A1 and CYP2C9/19 on plasma concentrations of rosuvastatin and lipid response in Chinese patients. Pharmacogenomics 2013, 14, 1283–1294. [Google Scholar] [CrossRef] [PubMed]
- DeGorter, M.K.; Tirona, R.G.; Schwarz, U.I.; Choi, Y.H.; Dresser, G.K.; Suskin, N.; Myers, K.; Zou, G.; Iwuchukwu, O.; Wei, W.Q.; et al. Clinical and pharmacogenetic predictors of circulating atorvastatin and rosuvastatin concentrations in routine clinical care. Circ. Cardiovasc. Genet. 2013, 6, 400–408. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tomlinson, B.; Hu, M.; Lee, V.W.; Lui, S.S.; Chu, T.T.; Poon, E.W.; Ko, G.T.; Baum, L.; Tam, L.S.; Li, E.K. ABCG2 polymorphism is associated with the low-density lipoprotein cholesterol response to rosuvastatin. Clin. Pharmacol. Ther. 2010, 87, 558–562. [Google Scholar] [CrossRef] [PubMed]
- Kozhakhmetov, S.S.; Kushugulova, A.R.; Kakimova, A.B.; Saduakhassova, S.A.; Urazova, M.S. Frequency of ABCG2 421C> A Genetic Variant and The Efficiency of Treatment with Rosuvastatin in Kazakh Male Patients. J. Mol. Genet. Med. 2016, 10, 1000225. [Google Scholar]
- Merćep, I.; Radman, I.; Trkulja, V.; Božina, T.; Šimičević, L.; Budimir, E.; Ganoci, L.; Božina, N. Loss of function polymorphisms in SLCO1B1 (c.521T>C, rs4149056) and ABCG2 (c.421C>A, rs2231142) genes are associated with adverse events of rosuvastatin: A case-control study. Eur. J. Clin. Pharmacol. 2022, 78, 227–236. [Google Scholar] [CrossRef]
- Cooper-DeHoff, R.M.; Niemi, M.; Ramsey, L.B.; Luzum, J.A.; Tarkiainen, E.K.; Straka, R.J.; Gong, L.; Tuteja, S.; Wilke, R.A.; Wadelius, M.; et al. The Clinical Pharmacogenetics Implementation Consortium (CPIC) guideline for SLCO1B1, ABCG2, and CYP2C9 and statin-associated musculoskeletal symptoms. Clin. Pharmacol. Ther. 2022. Print. [Google Scholar] [CrossRef]
- Imai, Y.; Nakane, M.; Kage, K.; Tsukahara, S.; Ishikawa, E.; Tsuruo, T.; Miki, Y.; Sugimoto, Y. C421A polymorphism in the human breast cancer resistance protein gene is associated with low expression of Q141K protein and low-level drug resistance. Mol. Cancer Ther. 2002, 1, 611–616. [Google Scholar]
- Mizuarai, S.; Aozasa, N.; Kotani, H. Single nucleotide polymorphisms result in impaired membrane localization and reduced atpase activity in multidrug transporter ABCG2. Int. J. Cancer 2004, 109, 238–246. [Google Scholar] [CrossRef]
- Kondo, C.; Suzuki, H.; Itoda, M.; Ozawa, S.; Sawada, J.; Kobayashi, D.; Ieiri, I.; Mine, K.; Ohtsubo, K.; Sugiyama, Y. Functional analysis of SNPs variants of BCRP/ABCG2. Pharm. Res. 2004, 21, 1895–1903. [Google Scholar] [CrossRef] [PubMed]
- Jiang, Z.P.; Zhao, X.L.; Takahashi, N.; Angelini, S.; Dubashi, B.; Sun, L.; Xu, P. Trough concentration and ABCG2 polymorphism are better to predict imatinib response in chronic myeloid leukemia: A meta-analysis. Pharmacogenomics 2017, 18, 35–56. [Google Scholar] [CrossRef] [PubMed]
- Ghafouri, H.; Ghaderi, B.; Amini, S.; Nikkhoo, B.; Abdi, M.; Hoseini, A. Association of ABCB1 and ABCG2 single nucleotide polymorphisms with clinical findings and response to chemotherapy treatments in Kurdish patients with breast cancer. Tumour Biol. 2016, 37, 7901–7906. [Google Scholar] [CrossRef] [PubMed]
- Ward, L.D.; Kellis, M. HaploReg: A resource for exploring chromatin states, conservation, and regulatory motif alterations within sets of genetically linked variants. Nucleic. Acids Res. 2012, 40, D930–D934. [Google Scholar] [CrossRef] [Green Version]
- Lee, E.; Ryan, S.; Birmingham, B.; Zalikowski, J.; March, R.; Ambrose, H.; Moore, R.; Lee, C.; Chen, Y.; Schneck, D. Rosuvastatin pharmacokinetics and pharmacogenetics in white and Asian subjects residing in the same environment. Clin. Pharmacol. Ther. 2005, 78, 330–341. [Google Scholar] [CrossRef]
- U.S. Food and Drug Administration. Crestor (Rosuvastatin calicum) Prescribing Information. Available online: https://www.accessdata.fda.gov/drugsatfda_docs/label/2005/21366slr005lbl.pdf (accessed on 18 January 2022).





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| First Author, Year | Nation | Race | N (Male Percent) | Age, Year (SD) | BMI, kg/m2 (SD) | Rosuvastatin Dose (mg) | PK Outcomes | Type of Mean Value | Genotyping Methods | Quantitative Methods | NOS |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Birmingham et al., 2015 [19] | U.S.A. | Caucasian, Chinese, Japanese | 93 (65.6) | 36.2 (14.3) | 23.8 (2.9) | 20 | AUC, Cmax | Geometric | TaqMan assay | LC-MS/MS | 7 |
| Birmingham et al., 2015 [20] | U.S.A. | Asian-Indian, Caucasian, Pooled-Asian a | 184 (66.3) | 23.0 (10.8) | 23.7 (3.0) | 20 | AUC, Cmax | Geometric | TaqMan assay | HPLC-MS/MS | 7 |
| Huguet et al., 2016 [3] | Canada | Caucasian | 16 (100.0) | 28.0 (8.0) | 24.1 (2.2) | 10 | AUC | Geometric | TaqMan assay | HPLC-HESI-MS/MS | 7 |
| Keskitalo et al., 2009 [8] | Finland | Caucasian | 32 (50.0) | 22.3 (2.6) | N/A | 20 | AUC, Cmax, tmax c, half-life | Arithmetic | TaqMan assay | LC-MS/MS | 7 |
| Kim et al., 2017 [21] | Korea | Korean | 13 (15.4) | 26.8 (4.0) | N/A | 20 | Cmax | Geometric | Pyrosequencing assay | LC-MS/MS | 6 |
| Liu et al., 2016 [22] | China | Chinese | 61 (100.0) | 20–32 b | 18–24 b | 20 | AUC, Cmax, tmax, half-life | Arithmetic | MALDI-TOF | LC-MS/MS | 7 |
| Wan et al., 2015 [23] | China | Chinese | 62 (100.0) | 18–24 b | 18–24 b | 10 | AUC, Cmax, tmax, half-life | Arithmetic | Pyrosequencing assay | HPLC-MS/MS | 6 |
| Zhang et al., 2006 [10] | China | Chinese | 14 (100.0) | N/A | N/A | 20 | AUC, Cmax, tmax, half-life | Arithmetic | Direct sequencing | LC-MS/MS | 7 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Song, Y.; Lim, H.-H.; Yee, J.; Yoon, H.-Y.; Gwak, H.-S. The Association between ABCG2 421C>A (rs2231142) Polymorphism and Rosuvastatin Pharmacokinetics: A Systematic Review and Meta-Analysis. Pharmaceutics 2022, 14, 501. https://doi.org/10.3390/pharmaceutics14030501
Song Y, Lim H-H, Yee J, Yoon H-Y, Gwak H-S. The Association between ABCG2 421C>A (rs2231142) Polymorphism and Rosuvastatin Pharmacokinetics: A Systematic Review and Meta-Analysis. Pharmaceutics. 2022; 14(3):501. https://doi.org/10.3390/pharmaceutics14030501
Chicago/Turabian StyleSong, Yubin, Hee-Hyun Lim, Jeong Yee, Ha-Young Yoon, and Hye-Sun Gwak. 2022. "The Association between ABCG2 421C>A (rs2231142) Polymorphism and Rosuvastatin Pharmacokinetics: A Systematic Review and Meta-Analysis" Pharmaceutics 14, no. 3: 501. https://doi.org/10.3390/pharmaceutics14030501