
Effect of GSTA1 Variants on Busulfan-Based Conditioning Regimen Prior to Allogenic Hematopoietic Stem-Cell Transplantation in Pediatric Asians

 ,
,  ,
,  , , , and
, , , and
Abstract
:1. Introduction
2. Patients and Methods
2.1. Patients and Conditioning Regimens
2.2. Conditioning-Related Regimen and Prophylaxis of Infection
2.3. DNA Extraction and GST Genotyping
2.4. Pharmacokinetic Analysis
2.5. Statistical Analysis
3. Results
3.1. Patient Characteristics
3.2. Frequencies of GSTA1, GSTM1 and GSTP1 Genotypes
3.3. Overview of Genetic Influences on PK of Busulfan
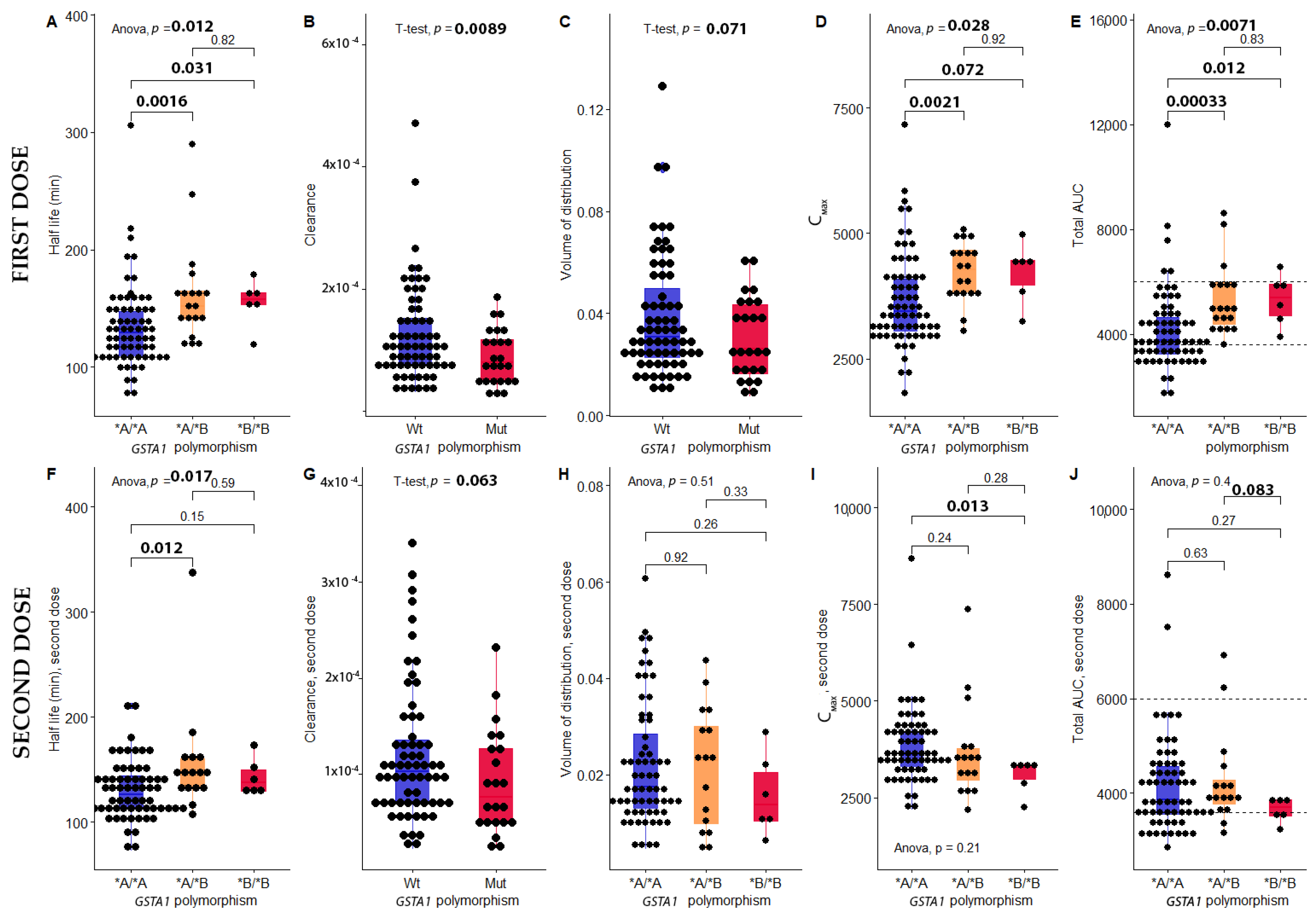
3.4. The Impact of GSTA1 Polymorphism on PK of Busulfan
3.5. Multivariate Regression Analysis between PK of Bu and Three Independent Variables: BSA, GSTA1 and Gender
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Hatzimichael, E.; Tuthill, M. Hematopoietic stem cell transplantation. Stem Cells Cloning 2010, 3, 105–117. [Google Scholar] [CrossRef] [Green Version]
- Kebriaei, P.; Anasetti, C.; Zhang, M.-J.; Wang, H.-L.; Aldoss, I.; de Lima, M.; Khoury, H.J.; Sandmaier, B.M.; Horowitz, M.M.; Artz, A.; et al. Intravenous Busulfan Compared with Total Body Irradiation Pretransplant Conditioning for Adults with Acute Lymphoblastic Leukemia. Biol. Blood Marrow Transplant. 2018, 24, 726–733. [Google Scholar] [CrossRef] [Green Version]
- Champlin, R.E. Busulfan or TBI: Answer to an age-old question. Blood 2013, 122, 3856–3857. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bredeson, C.; LeRademacher, J.; Kato, K.; Dipersio, J.F.; Agura, E.; Devine, S.M.; Appelbaum, F.R.; Tomblyn, M.R.; Laport, G.G.; Zhu, X.; et al. Prospective cohort study comparing intravenous busulfan to total body irradiation in hematopoietic cell transplantation. Blood 2013, 122, 3871–3878. [Google Scholar] [CrossRef] [Green Version]
- Bartelink, I.H.; Bredius, R.G.; Belitser, S.V.; Suttorp, M.M.; Bierings, M.; Knibbe, C.A.; Egeler, M.; Lankester, A.C.; Egberts, A.C.; Zwaveling, J. Association between busulfan exposure and outcome in children receiving intravenous busulfan before hematologic stem cell transplantation. Biol. Blood Marrow Transplant. 2009, 15, 231–241. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Geddes, M.; Kangarloo, S.B.; Naveed, F.; Quinlan, D.; Chaudhry, M.A.; Stewart, D.; Savoie, M.L.; Bahlis, N.J.; Brown, C.; Storek, J. High busulfan exposure is associated with worse outcomes in a daily iv busulfan and fludarabine allogeneic transplant regimen. Biol. Blood Marrow Transplant. 2008, 14, 220–228. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Feng, X.; Wu, Y.; Zhang, J.; Li, J.; Zhu, G.; Fan, D.; Yang, C.; Zhao, L. Busulfan systemic exposure and its relationship with efficacy and safety in hematopoietic stem cell transplantation in children: A meta-analysis. BMC Pediatrics 2020, 20, 176. [Google Scholar] [CrossRef]
- Corbacioglu, S.; Carreras, E.; Ansari, M.; Balduzzi, A.; Cesaro, S.; Dalle, J.-H.; Dignan, F.; Gibson, B.; Guengoer, T.; Gruhn, B. Diagnosis and severity criteria for sinusoidal obstruction syndrome/veno-occlusive disease in pediatric patients: A new classification from the European society for blood and marrow transplantation. Bone Marrow Transplant. 2018, 53, 138–145. [Google Scholar] [CrossRef] [PubMed]
- Bonifazi, F.; Barbato, F.; Ravaioli, F.; Sessa, M.; Defrancesco, I.; Arpinati, M.; Cavo, M.; Colecchia, A. Diagnosis and treatment of VOD/SOS after allogeneic hematopoietic stem cell transplantation. Front. Immunol. 2020, 11, 489. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sun, Y.; Huang, J.; Hao, C.; Li, Z.; Liang, W.; Zhang, W.; Chen, B.; Yang, W.; Hu, J. Population pharmacokinetic analysis of intravenous busulfan: GSTA1 genotype is not a predictive factor of initial dose in Chinese adult patients undergoing hematopoietic stem cell transplantation. Cancer Chemother. Pharmacol. 2020, 85, 293–308. [Google Scholar] [CrossRef] [PubMed]
- Wongpratate, M.; Phuthong, S.; Natphopsuk, S.; Ishida, T. Genetic polymorphism of glutathione S-transferase and cervical cancer susceptibility in Northeastern Thailand. Asian Pac. J. Cancer Biol. 2020, 5, 35–41. [Google Scholar]
- Myers, A.L.; Kawedia, J.D.; Champlin, R.E.; Kramer, M.A.; Nieto, Y.; Ghose, R.; Andersson, B.S. Clarifying busulfan metabolism and drug interactions to support new therapeutic drug monitoring strategies: A comprehensive review. Expert Opin. Drug Metab. Toxicol. 2017, 13, 901–923. [Google Scholar] [CrossRef] [PubMed]
- Uppugunduri, C.R.S.; Rezgui, M.A.; Diaz, P.H.; Tyagi, A.K.; Rousseau, J.; Daali, Y.; Duval, M.; Bittencourt, H.; Krajinovic, M.; Ansari, M. The association of cytochrome P450 genetic polymorphisms with sulfolane formation and the efficacy of a busulfan-based conditioning regimen in pediatric patients undergoing hematopoietic stem cell transplantation. Pharm. J. 2014, 14, 263–271. [Google Scholar] [CrossRef] [PubMed]
- Terakura, S.; Onizuka, M.; Fukumoto, M.; Kuwatsuka, Y.; Kohno, A.; Ozawa, Y.; Miyamura, K.; Inagaki, Y.; Sawa, M.; Atsuta, Y. Analysis of glutathione S-transferase and cytochrome P450 gene polymorphism in recipients of dose-adjusted busulfan-cyclophosphamide conditioning. Int. J. Hematol. 2020, 111, 84–92. [Google Scholar] [CrossRef]
- Ten Brink, M.H.; Van Bavel, T.; Swen, J.J.; Straaten, T.v.d.; Bredius, R.G.; Lankester, A.C.; Zwaveling, J.; Guchelaar, H.-J. Effect of genetic variants GSTA1 and CYP39A1 and age on busulfan clearance in pediatric patients undergoing hematopoietic stem cell transplantation. Pharmacogenomics 2013, 14, 1683–1690. [Google Scholar] [CrossRef] [Green Version]
- Strange, R.C.; Spiteri, M.A.; Ramachandran, S.; Fryer, A.A. Glutathione-S-transferase family of enzymes. Mutat. Res. /Fundam. Mol. Mech. Mutagenesis 2001, 482, 21–26. [Google Scholar] [CrossRef]
- Czerwinski, M.; Gibbs, J.P.; Slattery, J.T. Busulfan conjugation by glutathione S-transferases alpha, mu, and pi. Drug Metab. Dispos. 1996, 24, 1015–1019. [Google Scholar]
- Morel, F.; Rauch, C.; Coles, B.; Le Ferrec, E.; Guillouzo, A. The human glutathione transferase alpha locus: Genomic organization of the gene cluster and functional characterization of the genetic polymorphism in the hGSTA1 promoter. Pharm. Genom. 2002, 12, 277–286. [Google Scholar]
- Ansari, M.; Curtis, P.H.-D.; Uppugunduri, C.R.S.; Rezgui, M.A.; Nava, T.; Mlakar, V.; Lesne, L.; Théoret, Y.; Chalandon, Y.; Dupuis, L.L. GSTA1 diplotypes affect busulfan clearance and toxicity in children undergoing allogeneic hematopoietic stem cell transplantation: A multicenter study. Oncotarget 2017, 8, 90852–90867. [Google Scholar] [CrossRef] [Green Version]
- Johnson, L.A.; Orchard, P.J.; Baker, K.S.; Brundage, R.; Cao, Q.; Wang, X.; Langer, E.; Maasah, S.F.E.; Ross, J.A.; Remmel, R. Glutathione S-transferase A1 genetic variants reduce busulfan clearance in children undergoing hematopoietic cell transplantation. J. Clin. Pharmacol. 2008, 48, 1052–1062. [Google Scholar] [CrossRef] [Green Version]
- Yin, J.; Xiao, Y.; Zheng, H.; Zhang, Y. Once-daily iv BU-based conditioning regimen before allogeneic hematopoietic SCT: A study of influence of GST gene polymorphisms on BU pharmacokinetics and clinical outcomes in Chinese patients. Bone Marrow Transplant. 2015, 50, 696–705. [Google Scholar] [CrossRef] [Green Version]
- Nishikawa, T.; Yamaguchi, H.; Ikawa, K.; Nakayama, K.; Higashi, E.; Miyahara, E.; Abematsu, T.; Nakagawa, S.; Kodama, Y.; Tanabe, T. Influence of GST polymorphisms on busulfan pharmacokinetics in Japanese children. Pediatrics Int. 2019, 61, 558–565. [Google Scholar] [CrossRef]
- Elhasid, R.; Krivoy, N.; Rowe, J.M.; Sprecher, E.; Adler, L.; Elkin, H.; Efrati, E. Influence of glutathione S-transferase A1, P1, M1, T1 polymorphisms on oral busulfan pharmacokinetics in children with congenital hemoglobinopathies undergoing hematopoietic stem cell transplantation. Pediatric Blood Cancer 2010, 55, 1172–1179. [Google Scholar] [CrossRef]
- Ansari, M.; Lauzon-Joset, J.; Vachon, M.; Duval, M.; Theoret, Y.; Champagne, M.; Krajinovic, M. Influence of GST gene polymorphisms on busulfan pharmacokinetics in children. Bone Marrow Transplant. 2010, 45, 261–267. [Google Scholar] [CrossRef] [Green Version]
- Jahed, F.S.; Hamidi, S.; Ghaffary, S.; Nejati, B. Dispersive micro solid phase extraction of busulfan from plasma samples using novel mesoporous sorbent prior to determination by HPLC-MS/MS. J. Chromatogr. B 2020, 1145, 122091. [Google Scholar] [CrossRef]
- Xu, S.-j.; Wang, Y.-p.; Roe, B.; Pearson, W.R. Characterization of the Human Class Mu Glutathione S-Transferase Gene Cluster and the GSTM1Deletion. J. Biol. Chem. 1998, 273, 3517–3527. [Google Scholar] [CrossRef] [Green Version]
- Chen, B.; Cole, J.W.; Grond-Ginsbach, C. Departure from Hardy Weinberg equilibrium and genotyping error. Front. Genet. 2017, 8, 167. [Google Scholar] [CrossRef]
- Hassan, M.; Öberg, G.; Björkholm, M.; Wallin, I.; Lindgren, M. Influence of prophylactic anticonvulsant therapy on high-dose busulphan kinetics. Cancer Chemother. Pharmacol. 1993, 33, 181–186. [Google Scholar] [CrossRef]
- Nguyen, L.; Leger, F.; Lennon, S.; Puozzo, C. Intravenous busulfan in adults prior to haematopoietic stem cell transplantation: A population pharmacokinetic study. Cancer Chemother. Pharmacol. 2006, 57, 191–198. [Google Scholar] [CrossRef]
- Kim, S.-D.; Lee, J.-H.; Hur, E.-H.; Lee, J.-H.; Kim, D.-Y.; Lim, S.-N.; Choi, Y.; Lim, H.-S.; Bae, K.-S.; Noh, G.-J. Influence of GST gene polymorphisms on the clearance of intravenous busulfan in adult patients undergoing hematopoietic cell transplantation. Biol. Blood Marrow Transplant. 2011, 17, 1222–1230. [Google Scholar] [CrossRef] [Green Version]
- Gaziev, J.; Nguyen, L.; Puozzo, C.; Mozzi, A.F.; Casella, M.; Perrone Donnorso, M.; Gravina, P.; Sodani, P.; Marziali, M.; Isgro, A. Novel pharmacokinetic behavior of intravenous busulfan in children with thalassemia undergoing hematopoietic stem cell transplantation: A prospective evaluation of pharmacokinetic and pharmacodynamic profile with therapeutic drug monitoring. Blood J. Am. Soc. Hematol. 2010, 115, 4597–4604. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Córdoba, E.E.; Abba, M.C.; Lacunza, E.; Fernánde, E.; Güerci, A.M. Polymorphic variants in oxidative stress genes and acute toxicity in breast cancer patients receiving radiotherapy. Cancer Res. Treat. Off. J. Korean Cancer Assoc. 2016, 48, 948–954. [Google Scholar] [CrossRef] [PubMed]
- Bremer, S.; Fløisand, Y.; Brinch, L.; Gedde-Dahl, T.; Bergan, S. Glutathione transferase gene variants influence busulfan pharmacokinetics and outcome after myeloablative conditioning. Ther. Drug Monit. 2015, 37, 493–500. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abbasi, N.; Vadnais, B.; Knutson, J.A.; Blough, D.K.; Kelly, E.J.; O’Donnell, P.V.; Deeg, H.J.; Pawlikowski, M.A.; Ho, R.J.Y.; McCune, J.S. Pharmacogenetics of intravenous and oral busulfan in hematopoietic cell transplant recipients. J. Clin. Pharmacol. 2011, 51, 1429–1438. [Google Scholar] [CrossRef] [Green Version]
- Zong, C.; Sha, Y.; Xiang, H.; Wang, J.; Chen, D.; Liu, J.; Wang, B.; Cao, Y. Glutathione S-transferase A1 polymorphism and the risk of recurrent spontaneous abortion in Chinese Han population. J. Assist. Reprod. Genet. 2014, 31, 379–382. [Google Scholar] [CrossRef] [Green Version]
- Ping, J.; Wang, H.; Huang, M.; Liu, Z.-s. Genetic analysis of glutathione S-transferase A1 polymorphism in the Chinese population and the influence of genotype on enzymatic properties. Toxicol. Sci. 2006, 89, 438–443. [Google Scholar] [CrossRef] [Green Version]
- Choi, B.; Kim, M.G.; Han, N.; Kim, T.; Ji, E.; Park, S.; Kim, I.-W.; Oh, J.M. Population pharmacokinetics and pharmacodynamics of busulfan with GSTA1 polymorphisms in patients undergoing allogeneic hematopoietic stem cell transplantation. Pharmacogenomics 2015, 16, 1585–1594. [Google Scholar] [CrossRef]
- Matsuno, K.; Kubota, T.; Matsukura, Y.; Ishikawa, H.; Iga, T. Genetic analysis of glutathione S-transferase A1 and T1 polymorphisms in a Japanese population. Clin. Chem. Lab. Med. 2004, 42, 560–562. [Google Scholar] [CrossRef]
- Nava, T.; Kassir, N.; Rezgui, M.A.; Uppugunduri, C.R.S.; Huezo-Diaz Curtis, P.; Duval, M.; Théoret, Y.; Daudt, L.E.; Litalien, C.; Ansari, M. Incorporation of GSTA1 genetic variations into a population pharmacokinetic model for IV busulfan in paediatric hematopoietic stem cell transplantation. Br. J. Clin. Pharmacol. 2018, 84, 1494–1504. [Google Scholar] [CrossRef] [Green Version]
- Michaud, V.; Tran, M.; Pronovost, B.; Bouchard, P.; Bilodeau, S.; Alain, K.; Vadnais, B.; Franco, M.; Bélanger, F.; Turgeon, J. Impact of GSTA1 polymorphisms on busulfan oral clearance in adult patients undergoing hematopoietic stem cell transplantation. Pharmaceutics 2019, 11, 440. [Google Scholar] [CrossRef] [Green Version]
- Preedy, V.R. Handbook of Anthropometry: Physical Measures of Human form in Health and Disease; Springer Science & Business Media: Berlin, Germany, 2012. [Google Scholar]
- Mitchell, A.E.; Burns, S.A.; Rudolf, J.L. Isozyme-and gender-specific induction of glutathione S-transferases by flavonoids. Arch. Toxicol. 2007, 81, 777–784. [Google Scholar] [CrossRef] [PubMed]
- Miyagi, S.J.; Brown, I.W.; Chock, J.M.; Collier, A.C. Developmental changes in hepatic antioxidant capacity are age-and sex-dependent. J. Pharmacol. Sci. 2009, 111, 440–445. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hatayama, I.; Satoh, K.; Sato, K. Developmental and hormonal regulation of the major form of hepatic glutathione S-transferase in male mice. Biochem. Biophys. Res. Commun. 1986, 140, 581–588. [Google Scholar] [CrossRef]
- Staffas, L.; Ellis, E.M.; Hayes, J.D.; Lundgren, B.; Depierre, J.W.; Mankowitz, L. Growth hormone-and testosterone-dependent regulation of glutathione transferase subunit A5 in rat liver. Biochem. J. 1998, 332, 763–768. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ansell, P.; Espinosa-Nicholas, C.; Curran, E.; Judy, B.; Philips, B.; Hannink, M.; Lubahn, D. In vitro and in vivo regulation of antioxidant response element-dependent gene expression by estrogens. Endocrinology 2004, 145, 311–317. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- de Castro, F.A.; Lanchote, V.L.; Voltarelli, J.C.; Colturato, V.A.R.; Simões, B.P. Influence of fludarabine on the pharmacokinetics of oral busulfan during pretransplant conditioning for hematopoietic stem cell transplantation. J. Clin. Pharmacol. 2013, 53, 1205–1211. [Google Scholar] [CrossRef]
- Yeh, R.F.; Pawlikowski, M.A.; Blough, D.K.; McDonald, G.B.; O’Donnell, P.V.; Rezvani, A.; Deeg, H.J.; McCune, J.S. Accurate targeting of daily intravenous busulfan with 8-hour blood sampling in hospitalized adult hematopoietic cell transplant recipients. Biol. Blood Marrow Transplant. 2012, 18, 265–272. [Google Scholar] [CrossRef] [Green Version]
- Rezvani, A.R.; McCune, J.S.; Storer, B.E.; Batchelder, A.; Kida, A.; Deeg, H.J.; McDonald, G.B. Cyclophosphamide followed by intravenous targeted busulfan for allogeneic hematopoietic cell transplantation: Pharmacokinetics and clinical outcomes. Biol. Blood Marrow Transplant. 2013, 19, 1033–1039. [Google Scholar] [CrossRef] [Green Version]
- McCune, J.S.; Batchelder, A.; Deeg, H.J.; Gooley, T.; Cole, S.; Phillips, B.; Schoch, H.G.; McDonald, G.B. Cyclophosphamide following targeted oral busulfan as conditioning for hematopoietic cell transplantation: Pharmacokinetics, liver toxicity, and mortality. Biol. Blood Marrow Transplant. 2007, 13, 853–862. [Google Scholar] [CrossRef] [Green Version]
- Bensinger, W.I.; Buckner, C.D.; Lilleby, K.; Holmberg, L.; Storb, R.; Slattery, J.T. Dose escalation of busulfan with pentoxifylline and ciprofloxacin in patients with breast cancer undergoing autologous transplants. Oncology 2004, 67, 368–375. [Google Scholar] [CrossRef]
- Nava, T.; Rezgui, M.A.; Uppugunduri, C.R.; Curtis, P.H.-D.; Théoret, Y.; Duval, M.; Daudt, L.E.; Ansari, M.; Krajinovic, M.; Bittencourt, H. GSTA1 genetic variants and conditioning regimen: Missing key factors in dosing guidelines of busulfan in pediatric hematopoietic stem cell transplantation. Biol. Blood Marrow Transplant. 2017, 23, 1918–1924. [Google Scholar] [CrossRef] [PubMed]
- Kusama, M.; Kubota, T.; Matsukura, Y.; Matsuno, K.; Ogawa, S.; Kanda, Y.; Iga, T. Influence of glutathione S-transferase A1 polymorphism on the pharmacokinetics of busulfan. Clin. Chim. Acta 2006, 368, 93–98. [Google Scholar] [CrossRef] [PubMed]
- Marloes, H.; Swen, J.J.; Böhringer, S.; Wessels, J.A.; van der Straaten, T.; Marijt, E.W.; Peter, A.; Zwaveling, J.; Guchelaar, H.-J. Exploratory analysis of 1936 SNPs in ADME genes for association with busulfan clearance in adult hematopoietic stem cell recipients. Pharm. Genom. 2013, 23, 675–683. [Google Scholar]
- Ten Brink, M.; Wessels, J.; Den Hartigh, J.; Van Der Straaten, T.; Von Dem Borne, P.; Guchelaar, H.; Zwaveling, J. Effect of genetic polymorphisms in genes encoding GST isoenzymes on BU pharmacokinetics in adult patients undergoing hematopoietic SCT. Bone Marrow Transplant. 2012, 47, 190–195. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| Characteristics | Number of Patients | Percentage | |
|---|---|---|---|
| Gender | Male | 48 | 53% |
| Female | 44 | 47% | |
| Diagnosis | Thalassemia | 40 | 43.5% |
| Non-thalassemia | 52 | 56.5% | |
| Neuroblastoma | 9 | 9.9% | |
| AML | 7 | 7.6% | |
| ALL | 8 | 8.6% | |
| CML | 1 | 1.1% | |
| JMML | 1 | 1.1% | |
| Metabolic diseases | 3 | 3.3% | |
| Immunodeficiencies | 14 | 15% | |
| AIHA | 1 | 1.1% | |
| MDS | 2 | 2.2% | |
| SAA | 3 | 3.3% | |
| Osteopetrosis | 1 | 1.1% | |
| Undifferenciated round-cell tumor | 1 | 1.1% | |
| Other | 1 | 1.1% | |
| Conditioning regimen | BuCyMesna | 7 | 7.6% |
| BuCyATGMesna | 1 | 1.1% | |
| BuMel | 4 | 4.3% | |
| BuMelATG | 4 | 4.3% | |
| BuFluATG | 46 | 49.9% | |
| BuFluThio | 19 | 20.7% | |
| BuFluCyATGMesna | 1 | 1.1% | |
| BuFluMelATG | 3 | 3.3% | |
| BuFluATGRit | 3 | 3.3% | |
| BuFluThioRit | 2 | 2.2% | |
| Bu and BuCyATG | 2 | 2.2% | |
| Age | 0–2 years old | 8 | 8.7% |
| 2–6 years old | 27 | 29.3% | |
| 6–21 years old | 57 | 62% | |
| Age (year) | Min | 0.42 | |
| Mean | 8.41 | ||
| Max | 21.59 | ||
| BSA (square meters) | Min | 0.27 | |
| Mean | 0.935 | ||
| Max | 1.83 | ||
| Height (centimeter) | Min | 53.40 | |
| Mean | 121.91 | ||
| Max | 175.0 | ||
| Weight (kilograms) | Min | 4.10 | |
| Mean | 26.52 | ||
| Max | 72.20 |
| Gene | Variants | N (%) | HWE | |
|---|---|---|---|---|
| GSTA1 | Diplotype | *A/*A | 67 (72.8%) | 0.2542 |
| *A/*B | 19 (20.7%) | |||
| *B/*B | 6 (6.5%) | |||
| Haplotype | *A | 83.1% | ||
| *B | 16.9% | |||
| GSTP1 | Diplotype | A/A | 55 (59.8%) | 0.5896 |
| A/G | 35 (38.0%) | |||
| G/G | 2 (2.2%) | |||
| Haplotype | *A | 78.8% | ||
| *G | 21.2% | |||
| GSTM1 | Deletion | 63 (68.4%) | NA | |
| CNV:1 | 26 (28.3%) | |||
| CNV:2 | 2 (2.2%) | |||
| CNV:3 | 1 (1.1%) | |||
| First Dose | |||||
|---|---|---|---|---|---|
| Polymorphism | t1/2 | CL | Vd | Cmax | AUC0–inf |
| GSTA1 | |||||
| *A/*A (n = 67) | 134.34 ± 35.71 Ŧ | 124.23 ± 78.33 * | 23,434.0 ± 14,292.0 | 3675.5 ± 949.4 Ŧ | 4177.1 ± 1557.9 Ŧ |
| *A/*B (n = 19) | 161.86 ± 42.61 Ŧ | 94.01 ± 47.40 * | 21,896.3 ± 11,570.5 | 4232.6 ± 581.9 Ŧ | 5310.6 ± 1347.1 Ŧ |
| *B/*B (n = 6) | 154.99 ± 19.96 Ŧ | 72.05 ± 37.36 * | 16,266.7 ± 9879.6 | 4231.7 ± 605.9 Ŧ | 5296.4 ± 968.6 Ŧ |
| GSTM1 | |||||
| Deletion (n = 63) | 142.13 ± 42.09 | 119.75 ± 65.23 | 23,703.8 ± 12,622.1 | 3787.1 ± 849.8 | 4476.1 ± 1698.7 |
| 1 CNV (n = 26) | 141.27 ± 27.75 | 105.37 ± 90.54 | 20,971.9 ± 16,022.6 | 3896.9 ± 1048.9 | 4471.6 ± 1250.5 |
| 2 or 3 CNV (n = 3) | 126.16 ± 26.63 | 85.90 ± 34.80 | 15,033.3 ± 5533.8 | 4053.3 ± 447.7 | 4743.6 ± 1146.0 |
| GSTP1 | |||||
| A/A (n = 55) | 142.92 ± 36.82 | 115.71 ± 77.39 | 23,020.2 ± 14,464 | 3848.5 ± 956.7 | 4504.8 ± 1654.8 |
| A/G (n = 35) | 139.91 ± 41.03 | 114.48 ± 65.27 | 22,491.7 ± 12,157.1 | 3793.4 ± 832.6 | 4460.9 ± 1463.5 |
| G/G (n = 2) | 124.21 ± 0.93 | 85.20 ± 85.98 | 15,195 ± 15,280.6 | 3815 ± 49.5 | 4324.5 ± 201.9 |
| Second Dose | |||||
| Polymorphism | t1/2 | CL | Vd | Cmax | AUC0–inf |
| GSTA1 | |||||
| *A/*A (n = 64) | 129.81 ± 27.29 Ŧ | 119.31 ± 70.74 | 22,007.0 ± 12,898.1 | 3825.5 ± 968.6 | 4165.1 ± 1005.7 |
| *A/*B (n = 16) | 156.09 ± 52.20 Ŧ | 97.29 ± 59.73 | 21,496.3 ± 12,524.5 | 3679.4 ± 1290.5 | 4265.8 ± 998.4 |
| *B/*B (n = 6) | 142.65 ± 17.61 Ŧ | 75.85 ± 38.68 | 15,775 ± 8377.1 | 3070 ± 446.1 | 3646.5 ± 257.7 |
| GSTM1 | |||||
| Deletion (n = 60) | 137.17 ± 38.34 | 117.83 ± 66.28 | 22,707.5 ± 12,469.3 | 3781 ± 1090.0 | 4186.4 ± 1003.3 |
| 1 CNV (n = 23) | 129.50 ± 20.51 | 101.40 ± 74.80 | 18,743.0 ± 13,203.6 | 3715.2 ± 883.8 | 4088.3 ± 966.9 |
| 2 or 3 CNV (n = 3) | 150.70 ± 20.11 | 81.83 ± 25.72 | 17,833.3 ± 6560.7 | 3270 ± 350 | 3827.8 ± 392.1 |
| GSTP1 | |||||
| A/A (n = 52) | 134.27 ± 25.37 | 116.27 ± 73.34 | 21,873.6 ± 12,824.2 | 3643.3 ± 751.2 | 4053.0 ± 808.3 |
| A/G (n = 32) | 138.65 ± 45.70 | 106.94 ± 58.18 | 21,238.8 ± 12,294.6 | 3807.8 ± 1213.3 | 4260.7 ± 1158.8 |
| G/G (n = 2) | 121.12 ± 10.97 | 89.95 ± 94.82 | 14,980 ± 15,160.3 | 5410 ± 2771.9 | 4800.1 ± 2017.4 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nguyen, A.-H.; Biswas, M.; Puangpetch, A.; Prommas, S.; Pakakasama, S.; Anurathapan, U.; Rachanakul, J.; Sukprasong, R.; Nuntharadtanaphong, N.; Jongjitsook, N.; et al. Effect of GSTA1 Variants on Busulfan-Based Conditioning Regimen Prior to Allogenic Hematopoietic Stem-Cell Transplantation in Pediatric Asians. Pharmaceutics 2022, 14, 401. https://doi.org/10.3390/pharmaceutics14020401
Nguyen A-H, Biswas M, Puangpetch A, Prommas S, Pakakasama S, Anurathapan U, Rachanakul J, Sukprasong R, Nuntharadtanaphong N, Jongjitsook N, et al. Effect of GSTA1 Variants on Busulfan-Based Conditioning Regimen Prior to Allogenic Hematopoietic Stem-Cell Transplantation in Pediatric Asians. Pharmaceutics. 2022; 14(2):401. https://doi.org/10.3390/pharmaceutics14020401
Chicago/Turabian StyleNguyen, Ai-Hoc, Mohitosh Biswas, Apichaya Puangpetch, Santirhat Prommas, Samart Pakakasama, Usanarat Anurathapan, Jiratha Rachanakul, Rattanaporn Sukprasong, Nutthan Nuntharadtanaphong, Nutcha Jongjitsook, and et al. 2022. "Effect of GSTA1 Variants on Busulfan-Based Conditioning Regimen Prior to Allogenic Hematopoietic Stem-Cell Transplantation in Pediatric Asians" Pharmaceutics 14, no. 2: 401. https://doi.org/10.3390/pharmaceutics14020401