
Pharmacogene Variants Associated with Liver Transplant in a Twelve-Year Clinical Follow-Up

 , , , and
, , , and
Abstract
:1. Introduction
2. Methods
2.1. Patients
2.2. Immunosuppressive Therapy
2.3. Clinical Outcomes
2.4. Single Nucleotide Polymorphism Identification
2.5. SNPs Panel
2.6. Statistical Analyses
3. Results
3.1. Patients’ Genotypes
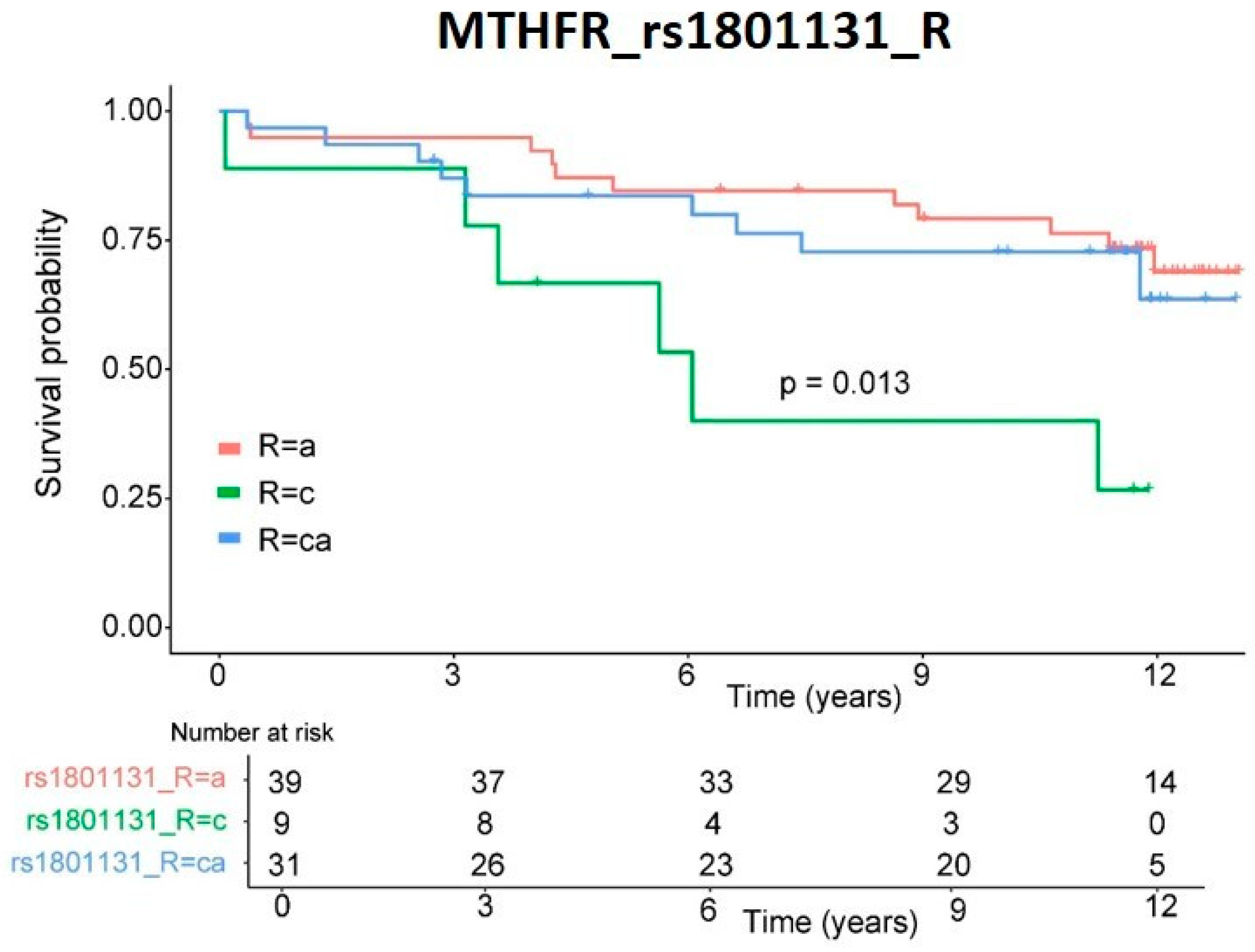
3.2. Survival
3.3. Tumor
3.4. Other Clinical Variables
3.5. Other Clinical Variables: Transporter Genes
3.6. Other Clinical Variables: Metabolizer and Signaling Pathway Genes
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| A | Adenine |
| ABC | ATP-binding cassette |
| C | Cytosine |
| CI | Confidence Interval |
| CYP | Cytochrome P450 |
| DHF | Dihydrofolate |
| DHFR | Dihydrofolate reductase |
| DM | Diabetes mellitus |
| DNA | Deoxyribonucleic acid |
| dTMP | Deoxythymidine monophosphate |
| dUMP | Deoxyuridine monophosphate |
| EDTA | Ethylenediaminetetraacetic acid |
| FDA | Food and Drug Administration |
| FDR | False Discovery Rate |
| G | Guanine |
| HCV | Hepatitis C virus |
| MAF | Minor Allele Frequency |
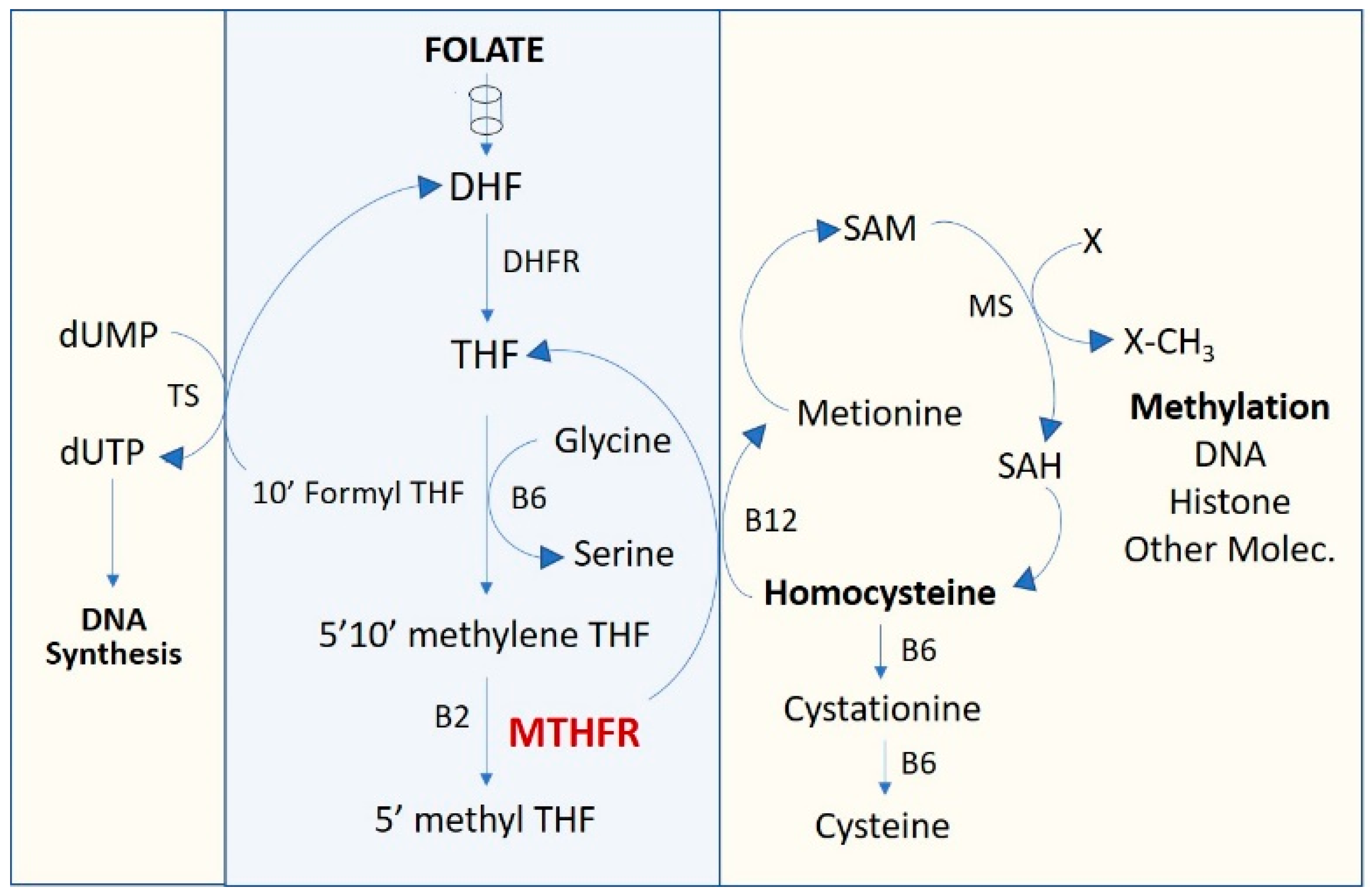
| MTHFR | Methylenetetrahydrofolate reductase |
| NOD | Nucleotide-binding oligomerization domain |
| OR | Odds Ratio |
| SAM | S-Adenosyl methionine |
| SLCO | Solute Carrier |
| SNP | Single nucleotide polymorphism |
| T | Thymine |
| THF | Tetrahydrofolate |
| TPMT | Thiopurine methyltransferase |
| UGT | Uridine diphosphate glucuronyltransferase |
References
- Home—GODT. Available online: http://www.transplant-observatory.org/ (accessed on 15 July 2021).
- Adam, R.; Karam, V.; Cailliez, V.; Grady, J.G.O.; Mirza, D.; Cherqui, D.; Klempnauer, J.; Salizzoni, M.; Pratschke, J.; Jamieson, N.; et al. 2018 Annual Report of the European Liver Transplant Registry (ELTR)-50-year evolution of liver transplantation. Transpl. Int. 2018, 31, 1293–1317. [Google Scholar] [CrossRef] [Green Version]
- Rub, A.; Anchez-Montes, C.S.; Aguilera, V.; Juan, F.S.; Ferrer, I.; Moya, A.; Montalva, E.; Pareja, E.; López-Andujar, R.; Prieto, M.; et al. Long-term outcome of “long-term liver transplant survivors”. Transpl. Int. 2013, 26, 740–750. [Google Scholar]
- Kisor, D.F.; Bodzin, A.S. Pharmacogenomics in liver transplantation: Testing the recipient and the ex-vivo donor liver. Pharmacogenomics 2018, 19, 753–756. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Caputo, V.; Strafella, C.; Cosio, T.; Lanna, C.; Campione, E.; Novelli, G.; Giardina, E.; Cascella, R. Pharmacogenomics: An Update on Biologics and Small-Molecule Drugs in the Treatment of Psoriasis. Genes 2021, 12, 1398. [Google Scholar] [CrossRef] [PubMed]
- Membrive Jiménez, C.; Pérez Ramírez, C.; Sánchez Martín, A.; Vieira Maroun, S.; Arias Santiago, S.; Ramírez Tortosa, M.C.; Jiménez Morales, A. Clinical Application of Pharmacogenetic Markers in the Treatment of Dermatologic Pathologies. Pharmaceuticals 2021, 14, 905. [Google Scholar] [CrossRef] [PubMed]
- Cargnin, S.; Sances, G.; Shin, J.I.; Tassorelli, C.; Terrazzino, S. Gene polymorphism association studies in cluster headache: A field synopsis and systematic meta-analyses. Headache J. Head Face Pain 2021, 61, 1060–1076. [Google Scholar] [CrossRef] [PubMed]
- Katara, P.; Yadav, A. Pharmacogenes (PGx-genes): Current understanding and future directions. Gene 2019, 718, 144050. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Li, K.; Zhang, X.; Teng, D.; Ju, M.; Jing, Y.; Zhao, Y.; Li, G. The correlation between the expression of genes involved in drug metabolism and the blood level of tacrolimus in liver transplant receipts. Sci. Rep. 2017, 7, 3429. [Google Scholar] [CrossRef] [Green Version]
- Hendijani, F.; Azarpira, N.; Kaviani, M. Effect of CYP3A5*1 expression on tacrolimus required dose after liver transplantation: A systematic review and meta-analysis. Clin. Transplant. 2018, 32, e13306. [Google Scholar] [CrossRef]
- Birdwell, K.; Decker, B.; Barbarino, J.M.; Peterson, J.F.; Stein, C.M.; Sadee, W.; Wang, D.; Vinks, A.; He, Y.; Swen, J.; et al. Clinical Pharmacogenetics Implementation Consortium (CPIC) Guidelines forCYP3A5Genotype and Tacrolimus Dosing. Clin. Pharmacol. Ther. 2015, 98, 19–24. [Google Scholar] [CrossRef] [Green Version]
- Calvo, P.L.; Serpe, L.; Brunati, A.; Nonnato, A.; Bongioanni, D.; Olio, D.D.; Pinon, M.; Ferretti, C.; Tandoi, F.; Carbonaro, G.; et al. Donor CYP3A5 genotype influences tacrolimus disposition on the first day after paediatric liver transplantation. Br. J. Clin. Pharmacol. 2017, 83, 1252–1262. [Google Scholar] [CrossRef] [PubMed]
- Lloberas, N.; Hesselink, D.A.; Van Schaik, R.H.; Grinyó, J.M.; Colom, H.; Van Gelder, T.; Elens, L. Detection of a rare CYP3A4 variant in a transplant patient characterized by a tacrolimus poor metabolizer phenotype. Pharmacogenomics 2018, 19, 305–310. [Google Scholar] [CrossRef] [PubMed]
- Berger, F.A.; Mulder, M.B.; ten Bosch-Dijksman, W.; van Schaik, R.H.N.; Coenen, S.; de Winter, B.C.M. Differences in CYP3A genotypes of a liver transplant recipient and the donor liver graft and adjustment of tacrolimus dose. Br. J. Clin. Pharmacol. 2019, 85, 1852. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- PharmGKB. Stanford University. 2020. Available online: https://www.pharmgkb.org (accessed on 25 October 2021).
- Tron, C.; Woillard, J.-B.; Houssel-Debry, P.; David, V.; Jezequel, C.; Rayar, M.; Balakirouchenane, D.; Blanchet, B.; Debord, J.; Petitcollin, A.; et al. Pharmacogenetic—Whole blood and intracellular pharmacokinetic—Pharmacodynamic (PG-PK2-PD) relationship of tacrolimus in liver transplant recipients. PLoS ONE 2020, 15, e0230195. [Google Scholar] [CrossRef]
- Gong, J.-M.; Shen, Y.; Shan, W.-W.; He, Y.-X. The association between MTHFR polymorphism and cervical cancer. Sci. Rep. 2018, 8, 7244. [Google Scholar] [CrossRef]
- Liew, S.-C.; Das Gupta, E. Methylenetetrahydrofolate reductase (MTHFR) C677T polymorphism: Epidemiology, metabolism and the associated diseases. Eur. J. Med. Genet. 2015, 58, 1–10. [Google Scholar] [CrossRef]
- Levey, A.S.; Coresh, J.; Greene, T.; Marsh, J.; Stevens, L.A.; Kusek, J.W.; Van Lente, F.; Chronic Kidney Disease Epidemiology Collaboration. Expressing the Modification of Diet in Renal Disease Study Equation for Estimating Glomerular Filtration Rate with Standardized Serum Creatinine Values. Clin. Chem. 2007, 53, 766–772. [Google Scholar] [CrossRef] [Green Version]
- Huang, A.; Xu, S.; Cai, X. Empirical Bayesian elastic net for multiple quantitative trait locus mapping. Heredity 2014, 114, 107–115. [Google Scholar] [CrossRef] [Green Version]
- Zou, H.; Hastie, T. Regularization and variable selection via the elastic net. J. R. Stat. Soc. Ser. B 2005, 67, 301–320. [Google Scholar] [CrossRef] [Green Version]
- Kang, S.S.; Wong, P.W.; Susmano, A.; Sora, J.; Norusis, M.; Ruggie, N. Thermolabile methylenetetrahydrofolate reductase: An inherited risk factor for coronary artery disease. Am. J. Hum. Genet. 1991, 48, 536–545. [Google Scholar]
- Ghodke-Puranik, Y.; Puranik, A.S.; Shintre, P.; Joshi, K.; Patwardhan, B.; Lamba, J.; Niewold, T.B.; Chopra, A. Folate metabolic pathway single nucleotide polymorphisms: A predictive pharmacogenetic marker of methotrexate response in Indian (Asian) patients with rheumatoid arthritis. Pharmacogenomics 2015, 16, 2019–2034. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Olivera, G.G.; Yáñez, Y.; Gargallo, P.; Sendra, L.; Aliño, S.F.; Segura, V.; Sanz, M.Á.; Cañete, A.; Castel, V.; De Mora, J.F.; et al. MTHFR and VDR Polymorphisms Improve the Prognostic Value of MYCN Status on Overall Survival in Neuroblastoma Patients. Int. J. Mol. Sci. 2020, 21, 2714. [Google Scholar] [CrossRef] [PubMed]
- Gao, X.; Sanderson, S.M.; Dai, Z.; Reid, M.A.; Cooper, D.E.; Lu, M.; Richie, J.P., Jr.; Ciccarella, A.; Calcagnotto, A.; Mikhael, P.G.; et al. Dietary methionine influences therapy in mouse cancer models and alters human metabolism. Nature 2019, 572, 397–401. [Google Scholar] [CrossRef] [PubMed]
- Jiang, Z.; Hu, N. Effect of UGT polymorphisms on pharmacokinetics and adverse reactions of mycophenolic acid in kidney transplant patients. Pharmacogenomics 2021, 22, 1019–1040. [Google Scholar] [CrossRef] [PubMed]
- Vanhove, T.; Annaert, P.; Lambrechts, D.; Kuypers, D.R.J. Effect of ABCB1 diplotype on tacrolimus disposition in renal recipients depends on CYP3A5 and CYP3A4 genotype. Pharm. J. 2016, 17, 556–562. [Google Scholar] [CrossRef] [PubMed]
- Tron, C.; Lemaitre, F.; Verstuyft, C.; Petitcollin, A.; Verdier, M.-C.; Bellissant, E. Pharmacogenetics of Membrane Transporters of Tacrolimus in Solid Organ Transplantation. Clin. Pharmacokinet. 2018, 58, 593–613. [Google Scholar] [CrossRef] [PubMed]
- Genvigir, F.D.V.; Nishikawa, A.M.; Felipe, C.R.; Helio, T.-S., Jr.; Oliveira, N.; Salazar, A.B.C.; Pestana, J.M.; Doi, S.Q.; Hirata, M.H.; Hirata, R.D.C. Influence ofABCC2, CYP2C8, andCYP2J2Polymorphisms on Tacrolimus and Mycophenolate Sodium-Based Treatment in Brazilian Kidney Transplant Recipients. Pharmacother. J. Hum. Pharmacol. Drug Ther. 2017, 37, 535–545. [Google Scholar] [CrossRef]
- Božina, N.; Lalić, Z.; Nađ-Škegro, S.; Borić-Bilušić, A.; Kaštelan, Ž.; Trkulja, V. Steady-state pharmacokinetics of mycophenolic acid in renal transplant patients: Exploratory analysis of the effects of cyclosporine, recipients’ and donors’ ABCC2 gene variants, and their interactions. Eur. J. Clin. Pharmacol. 2017, 73, 1129–1140. [Google Scholar] [CrossRef]
- Thishya, K.; Sreenu, B.; Raju, S.B.; Kutala, V.K. Impact of Pharmacogenetic Determinants of Tacrolimus and Mycophenolate on Adverse Events in Renal Transplant Patients. Curr. Drug Metab. 2021, 22, 342–352. [Google Scholar] [CrossRef]
- Ivanyuk, A.; Livio, F.; Biollaz, J.; Buclin, T. Renal Drug Transporters and Drug Interactions. Clin. Pharmacokinet. 2017, 56, 825–892. [Google Scholar] [CrossRef]
- Lu, X.; Chan, T.; Cheng, Z.; Shams, T.; Zhu, L.; Murray, M.; Zhou, F. The 5′-AMP-Activated Protein Kinase Regulates the Function and Expression of Human Organic Anion Transporting Polypeptide 1A2. Mol. Pharmacol. 2018, 94, 1412–1420. [Google Scholar] [CrossRef] [PubMed]
- Nwogu, J.N.; Gandhi, M.; Owen, A.; Khoo, S.H.; Taiwo, B.; Olagunju, A.; Berzins, B.; Okochi, H.; Tallerico, R.; Robertson, K.; et al. Associations between efavirenz concentrations, pharmacogenetics and neurocognitive performance in people living with HIV in Nigeria. AIDS 2021, 35, 1919–1927. [Google Scholar] [CrossRef] [PubMed]
- Langmia, I.M.; Just, K.S.; Yamoune, S.; Brockmöller, J.; Masimirembwa, C.; Stingl, J.C. CYP2B6 Functional Variability in Drug Metabolism and Exposure Across Populations—Implication for Drug Safety, Dosing, and Individualized Therapy. Front. Genet. 2021, 12, 692234. [Google Scholar] [CrossRef] [PubMed]
- Lv, C.; Huang, L. Xenobiotic receptors in mediating the effect of sepsis on drug metabolism. Acta Pharm. Sin. B 2019, 10, 33–41. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Gender (n) | Average ± SD | % |
|---|---|---|
| Male (m) | 55 | 69.62 |
| Female (f) | 24 | 30.38 |
| Weight (kg) | 74.90 ± 13.10 | |
| Age at Tx (years) | 54.65 ± 10.24 | |
| Diagnosis at Tx (n) | ||
| Cirrhosis | 70 | 88.61 |
| Hepatitis C virus (HCV) | 37 | 46.84 |
| Hepatocellular carcinoma (HCC) | 31 | 39.24 |
| Tacrolimus dose (mg/kg/day) | 0.09 ± 0.02 | |
| Hospital stay (days) | 24.14 ± 43.07 | |
| Retransplantation required (n) | 5 | 6.33 |
| Exitus during follow-up | ||
| n | 26 | 32.91 |
| Time (years) | 9.22 ± 3.97 | |
| De novo cancer during follow-up | ||
| n | 15 | 18.99 |
| Time (years) | 6.21 ± 2.40 | |
| Clinical events during follow-up (n) | ||
| De novo DM2 | 27 | 34.18 |
| De novo arterial hypertension | 29 | 36.71 |
| Graft rejection | 36 | 45.57 |
| Infections | 46 | 58.23 |
| Acute nephrotoxicity | 28 | 35.44 |
| Chronic nephrotoxicity | 24 | 30.38 |
| Patients with emergencies | 58 | 73.42 |
| Average emergencies | 7.17 ± 9.49 | |
| Patients requiring hospitalizations | 68 | 86.08 |
| Average hospitalizations | 4.81 ± 4.15 | |
| Pharmacological treatment | ||
| Tacrolimus | 79 | 100.00 |
| Micophenolic acid | 36 | 45.57 |
| Corticosteroids | 75 | 94.94 |
| Time (months) | 11.00 ± 9.30 | |
| Azatioprin | 12 | 15.19 |
| Induction therapy | 4 | 5.06 |
| Nephrotoxic drugs | 11 | 13.92 |
| CYP3A5 modifier drugs | 5 | 6.33 |
| Gene | Function | SNP | |
|---|---|---|---|
| ABCB1 | Transporter | rs1045642 | rs2235013 |
| rs1128503 | rs2235033 | ||
| rs2032582 | rs3213619 | ||
| rs229109 | rs9282564 | ||
| ABCC2 | Transporter | rs3740066 | rs717620 |
| rs2273697 | |||
| ABCG2 | Transporter | rs2231137 | rs2231142 |
| CYP2B6 | Metabolizer | rs2279343 | rs3745274 |
| CYP2C19 | Metabolizer | rs4244285 | |
| CYP2C9 | Metabolizer | rs1799853 | rs1057910 |
| CYP3A4 | Metabolizer | rs2740574 | |
| CYP3A5 | Metabolizer | rs41303343 | rs776746 |
| rs10264272 | |||
| MTHFR | Metabolizer | rs1801131 | rs1801133 |
| NOD2 | Signaling pathway | rs2066844 | rs2066845 |
| SLCO1A2 | Transporter | rs11568564 | rs72559749 |
| rs11568563 | |||
| SLCO1B1 | Transporter | rs2306283 | rs4149056 |
| TPMT | Signaling pathway | rs1142345 | rs1800462 |
| rs1800460 | |||
| UGT1A9 | Metabolizer | rs17868320 | rs72551330 |
| rs6714486 | |||
| Model Data | |||||||||
|---|---|---|---|---|---|---|---|---|---|
| Logistic Regression | CI (95%) | ||||||||
| Gene | SNP | D/R | Genotype | R2 Cox Snell | R2 Nagelkerke | p-Value | OR | Lower | Upper |
| MTHFR | rs1801131 | R | CC | 0.294 | 0.409 | 0.036 | 7.34 | 1.39 | 38.70 |
| MTHFR | rs1801133 | D | TT | 0.032 | 7.90 | 1.67 | 37.43 | ||
| Model Data | |||||||||
|---|---|---|---|---|---|---|---|---|---|
| Logistic Regression | CI (95%) | ||||||||
| Gene | SNP | D/R | Genotype | R2 Cox Snell | R2 Nagelkerke | p-Value | OR | Lower | Upper |
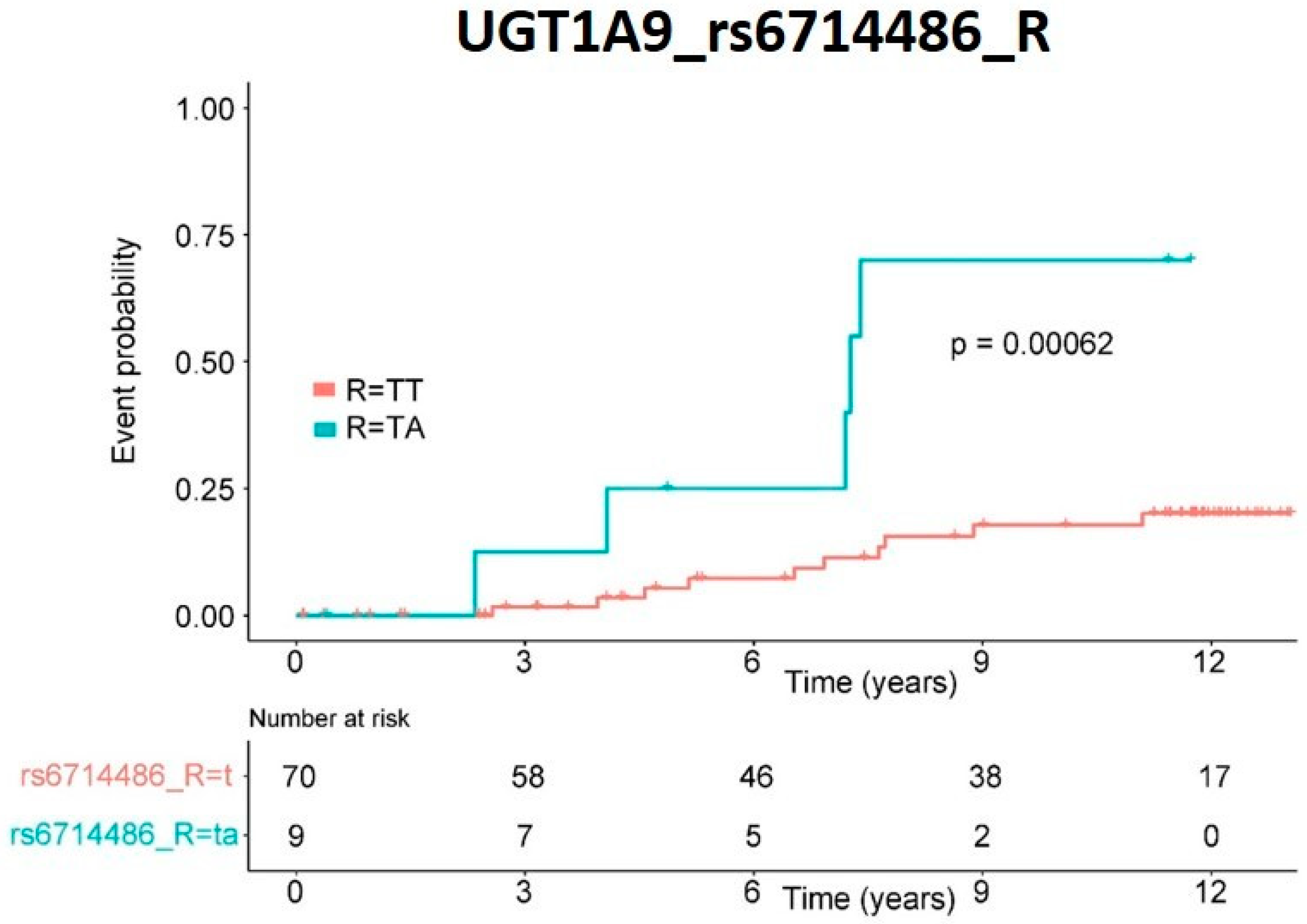
| UGT1A9 | rs6714486 | R | TA | 0.248 | 0.399 | 0.032 | 0.13 | 0.030 | 0.583 |
| All SNPs | |||||||
|---|---|---|---|---|---|---|---|
| Clinical Variables | Gene | SNP | D/R | Genotype | n | % | OR |
| Diabetes mellitus | SLCO1A2 | rs11568563 | R | CA † | 15 | 18.99 | 0.705 |
| Infections | CYP2B6 | rs2279343 | R | GA | 35 | 44.30 | 1.116 |
| Chronic nephrotoxicity | ABCC2 | rs3740066 | R | CT † | 39 | 49.37 | 0.920 |
| rs717620 | R | TC † | 29 | 36.71 | 0.878 | ||
| Transporter Genes SNPs | De Novo Disease (n) | ||||||
|---|---|---|---|---|---|---|---|
| Clinical Variables | Gene | SNP | D/R | Genotype | Absence | Presence | OR |
| Diabetes mellitus | SLCO1A2 | rs11568563 | R | A | 37 | 27 | - |
| CA † | 15 | 0 | 0.550 | ||||
| ABCG2 | rs2231142 | R | C | 48 | 21 | - | |
| CA | 4 | 6 | 1.008 | ||||
| ABCB1 | rs1128503 | D | C | 15 | 12 | - | |
| CT | 28 | 8 | 0.922 | ||||
| TT | 9 | 7 | - | ||||
| rs2032582 | D | GT | 28 | 10 | - | ||
| G | 20 | 11 | - | ||||
| TT | 4 | 6 | 1.063 | ||||
| Arterial hypertension | ABCB1 | rs1045642 | R | TC | 27 | 15 | - |
| CC | 7 | 11 | - | ||||
| TT † | 16 | 3 | 0.976 | ||||
| rs1128503 | R | CT | 29 | 20 | - | ||
| CC | 9 | 8 | - | ||||
| TT † | 12 | 1 | 0.859 | ||||
| rs229109 | R | GA | 1 | 4 | - | ||
| AA | 2 | 3 | - | ||||
| GG † | 47 | 22 | 0.857 | ||||
| ABCC2 | rs2273697 | R | GG | 29 | 23 | - | |
| AA | 3 | 2 | - | ||||
| GA | 18 | 4 | 0.942 | ||||
| Acute nephrotoxicity | ABCB1 | rs1045642 | D | CC | 11 | 10 | - |
| TC | 27 | 17 | - | ||||
| TT † | 13 | 1 | 0.916 | ||||
| Chronic nephrotoxicity | ABCC2 | rs3740066 | R | CC | 15 | 12 | - |
| CT † | 33 | 6 | 0.831 | ||||
| TT | 7 | 6 | - | ||||
| rs717620 | R | CC | 27 | 20 | - | ||
| TC † | 26 | 3 | 0.784 | ||||
| TT | 2 | 1 | - | ||||
| Metabolizer and Target Genes SNPs | De Novo Disease (n) | ||||||
|---|---|---|---|---|---|---|---|
| Clinical Variables | Gene | SNP | D/R | Genotype | Absence | Presence | OR |
| Infections | CYP2B6 | rs2279343 | R | AA | 18 | 18 | - |
| GA | 8 | 27 | 1.240 | ||||
| GG | 6 | 2 | - | ||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sendra, L.; Olivera, G.G.; López-Andújar, R.; Serrano, C.; Rojas, L.E.; Montalvá, E.M.; Herrero, M.J.; Aliño, S.F. Pharmacogene Variants Associated with Liver Transplant in a Twelve-Year Clinical Follow-Up. Pharmaceutics 2022, 14, 354. https://doi.org/10.3390/pharmaceutics14020354
Sendra L, Olivera GG, López-Andújar R, Serrano C, Rojas LE, Montalvá EM, Herrero MJ, Aliño SF. Pharmacogene Variants Associated with Liver Transplant in a Twelve-Year Clinical Follow-Up. Pharmaceutics. 2022; 14(2):354. https://doi.org/10.3390/pharmaceutics14020354
Chicago/Turabian StyleSendra, Luis, Gladys G. Olivera, Rafael López-Andújar, Cristina Serrano, Luis E. Rojas, Eva María Montalvá, María José Herrero, and Salvador F. Aliño. 2022. "Pharmacogene Variants Associated with Liver Transplant in a Twelve-Year Clinical Follow-Up" Pharmaceutics 14, no. 2: 354. https://doi.org/10.3390/pharmaceutics14020354