
Safety and Immunogenicity of Inactivated Whole Virion COVID-19 Vaccine CoviVac in Clinical Trials in 18–60 and 60+ Age Cohorts
 ,
,  , , , , , ,
, , , , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Ethical Approval
2.2. Study Design and Participants
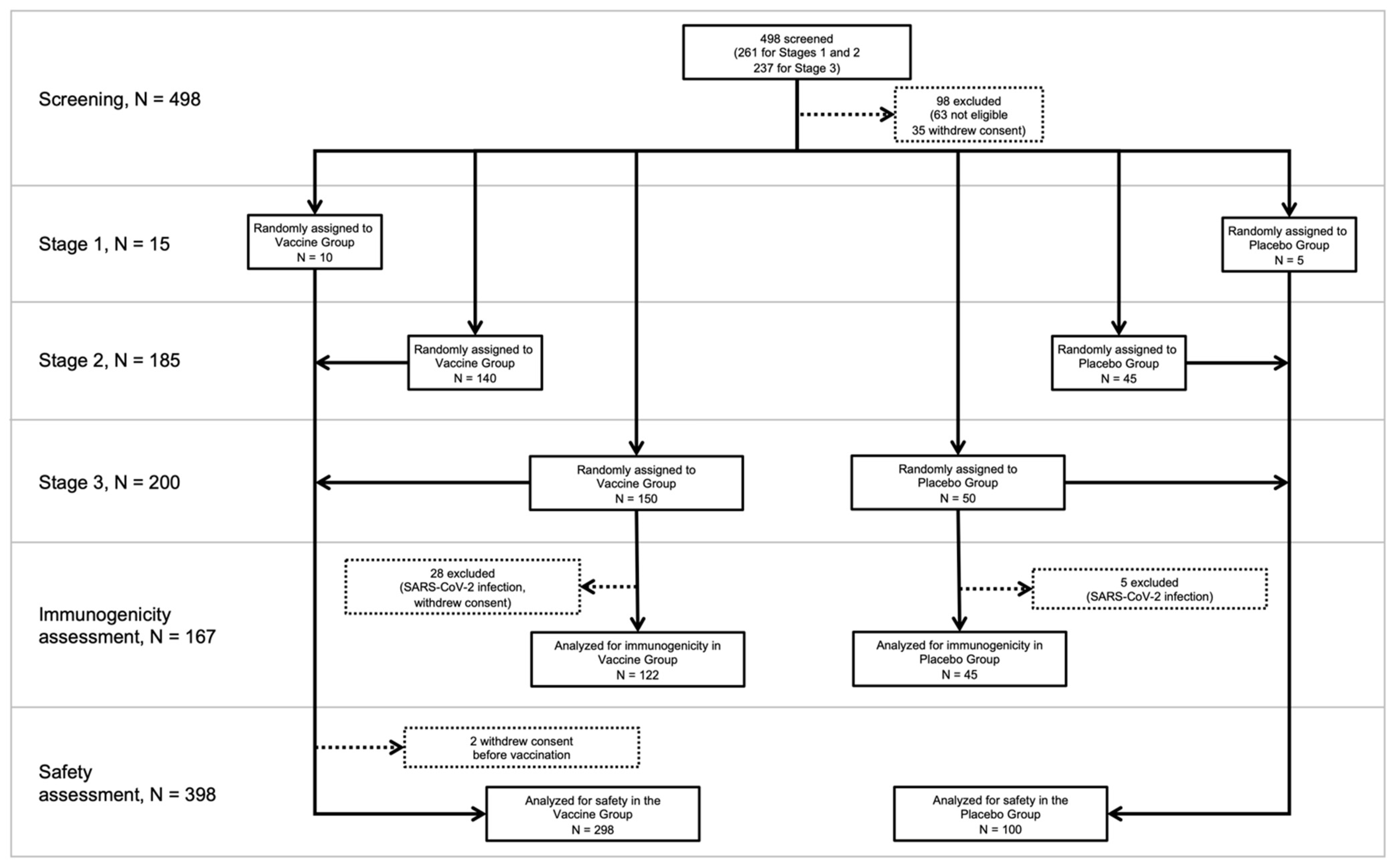
2.2.1. Design and Participants in 18–60 Age Cohort
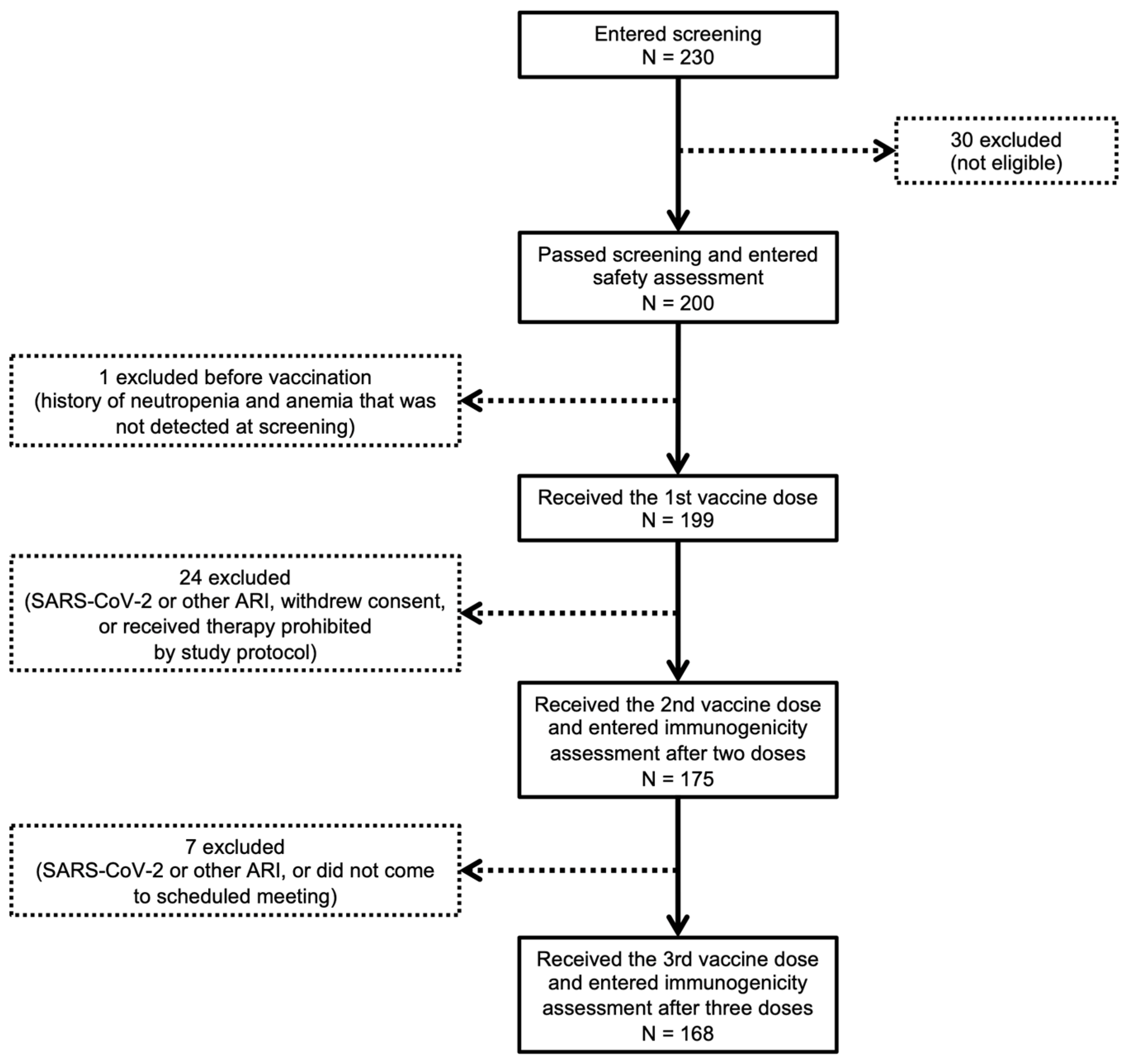
2.2.2. Design and Participants in 60+ Age Cohort
2.3. Randomization and Blinding
2.4. Procedures
2.5. Safety Assessment
2.6. Immunogenicity Assessment
2.7. Study Outcomes
2.8. Statistical Analysis
3. Results
3.1. Demographic and Anthropometric Data
3.1.1. 18–60 Age Cohort
3.1.2. 60+ Age Cohort
3.2. Tolerance, Reactogenicity and Safety
3.3. CoviVac Humoral Immunogenicity Assessment
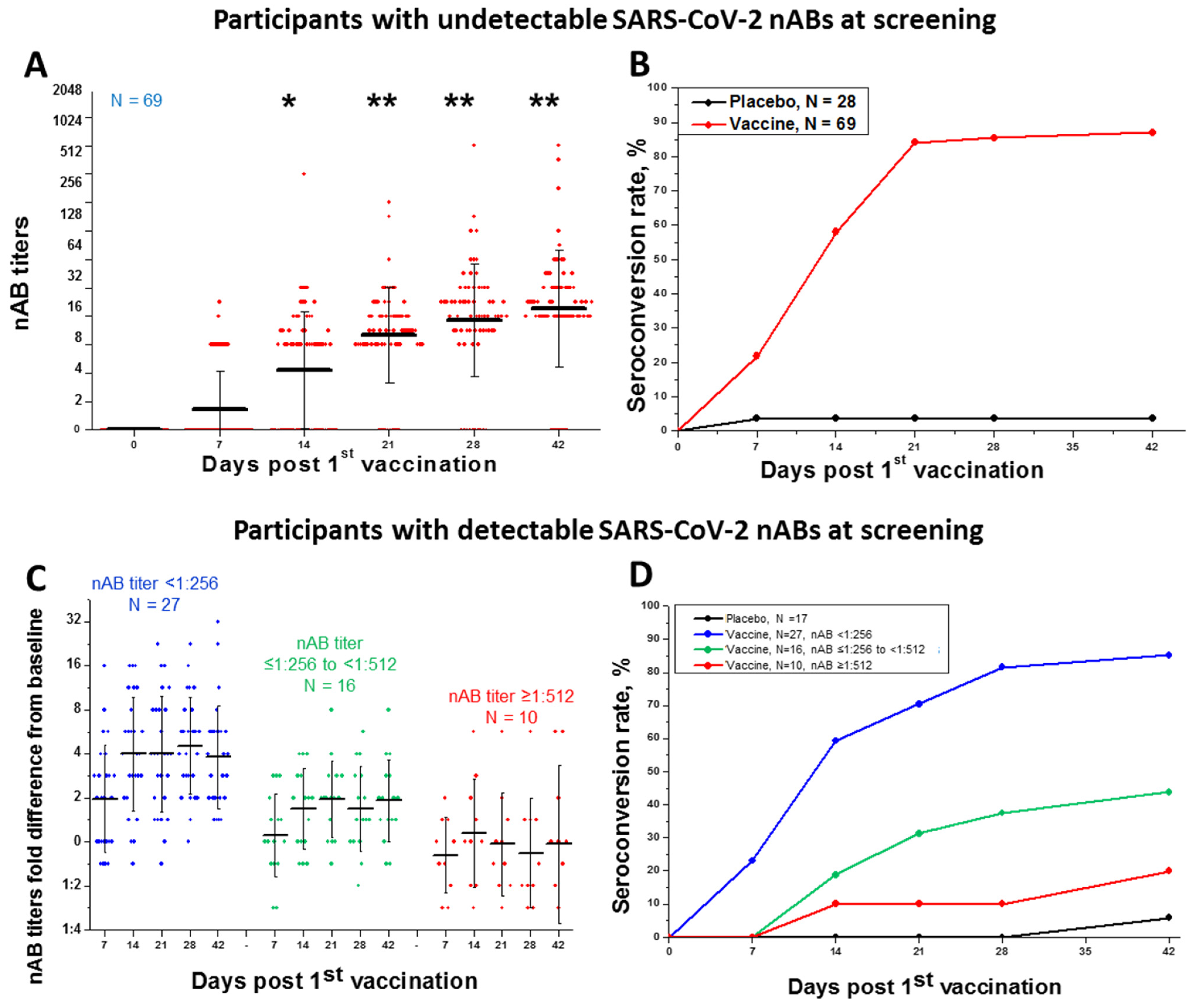
3.3.1. 18–60 Age Cohort
3.3.2. 60+ Age Cohort
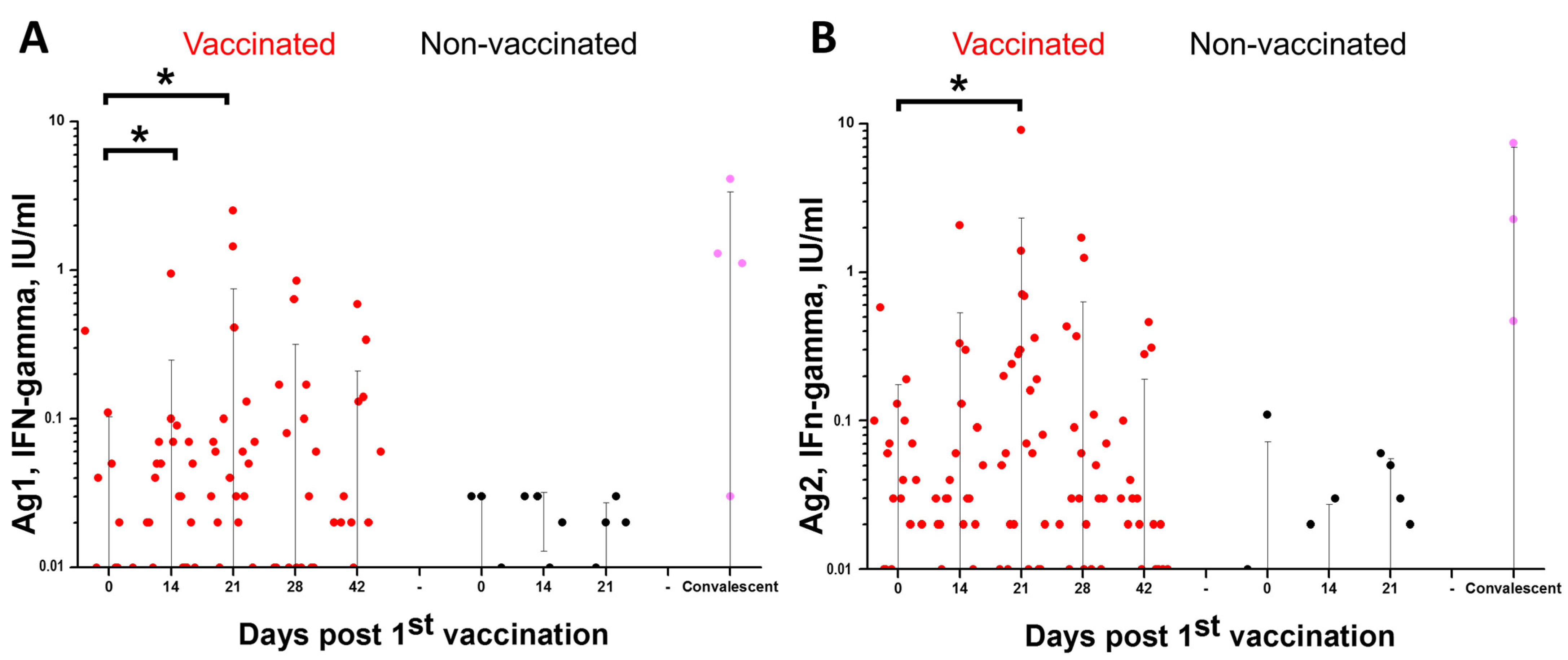
3.4. Cellular Immunity Assessment
4. Discussion
4.1. CoviVac Safety in Phases I/II and IIb
4.2. CoviVac Immunogenicity in Phases II (18–60 Years) and IIb (60+ Years)
4.3. Prospects for Further Development
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- WHO. WHO Coronavirus (COVID-19) Dashboard. WHO Coronavirus (COVID-19) Dashboard with Vaccination Data. 2023. Available online: https://covid19.who.int/ (accessed on 30 May 2023).
- Polack, F.P.; Thomas, S.J.; Kitchin, N.; Absalon, J.; Gurtman, A.; Lockhart, S.; Perez, J.L.; Pérez Marc, G.; Moreira, E.D.; Zerbini, C.; et al. Safety and Efficacy of the BNT162b2 mRNA Covid-19 Vaccine. N. Engl. J. Med. 2020, 383, 2603–2615. [Google Scholar] [CrossRef] [PubMed]
- Baden, L.R.; El Sahly, H.M.; Essink, B.; Kotloff, K.; Frey, S.; Novak, R.; Diemert, D.; Spector, S.A.; Rouphael, N.; Creech, C.B.; et al. Efficacy and Safety of the mRNA-1273 SARS-CoV-2 Vaccine. N. Engl. J. Med. 2021, 384, 403–416. [Google Scholar] [CrossRef] [PubMed]
- Logunov, D.Y.; Dolzhikova, I.V.; Shcheblyakov, D.V.; Tukhvatulin, A.I.; Zubkova, O.V.; Dzharullaeva, A.S.; Kovyrshina, A.V.; Lubenets, N.L.; Grousova, D.M.; Erokhova, A.S.; et al. Safety and efficacy of an rAd26 and rAd5 vector-based heterologous prime-boost COVID-19 vaccine: An interim analysis of a randomised controlled phase 3 trial in Russia. Lancet 2021, 397, 671–681. [Google Scholar] [CrossRef] [PubMed]
- Falsey, A.R.; Sobieszczyk, M.E.; Hirsch, I.; Sproule, S.; Robb, M.L.; Corey, L.; Neuzil, K.M.; Hahn, W.; Hunt, J.; Mulligan, M.J.; et al. Phase 3 Safety and Efficacy of AZD1222 (ChAdOx1 nCoV-19) Covid-19 Vaccine. N. Engl. J. Med. 2021, 25, 2348–2360. [Google Scholar] [CrossRef]
- Heath, P.T.; Galiza, E.P.; Baxter, D.N.; Boffito, M.; Browne, D.; Burns, F.; Chadwick, D.R.; Clark, R.; Cosgrove, C.; Galloway, J.; et al. Safety and Efficacy of NVX-CoV2373 Covid-19 Vaccine. N. Engl. J. Med. 2021, 385, 1172–1183. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Zeng, G.; Pan, H.; Li, C.; Hu, Y.; Chu, K.; Han, W.; Chen, Z.; Tang, R.; Yin, W.; et al. Safety, tolerability, and immunogenicity of an inactivated SARS-CoV-2 vaccine in healthy adults aged 18–59 years: A randomised, double-blind, placebo-controlled, phase 1/2 clinical trial. Lancet Infect. Dis. 2021, 21, 181–192. [Google Scholar] [CrossRef]
- Ella, R.; Reddy, S.; Blackwelder, W.; Potdar, V.; Yadav, P.; Sarangi, V.; Aileni, V.K.; Kanungo, S.; Rai, S.; Reddy, P.; et al. Efficacy, safety, and lot-to-lot immunogenicity of an inactivated SARS-CoV-2 vaccine (BBV152): Interim results of a randomised, double-blind, controlled, phase 3 trial. Lancet 2021, 398, 2173–2184. [Google Scholar] [CrossRef]
- Al Kaabi, N.; Zhang, Y.; Xia, S.; Yang, Y.; Al Qahtani, M.M.; Abdulrazzaq, N.; Al Nusair, M.; Hassany, M.; Jawad, J.S.; Abdalla, J.; et al. Effect of 2 Inactivated SARS-CoV-2 Vaccines on Symptomatic COVID-19 Infection in Adults: A Randomized Clinical Trial. JAMA 2021, 326, 35–45. [Google Scholar] [CrossRef]
- Zakarya, K.; Kutumbetov, L.; Orynbayev, M.; Abduraimov, Y.; Sultankulova, K.; Kassenov, M.; Sarsenbayeva, G.; Kulmagambetov, I.; Davlyatshin, T.; Sergeeva, M.; et al. Safety and immunogenicity of a QazCovid-in® inactivated whole-virion vaccine against COVID-19 in healthy adults: A single-centre, randomised, single-blind, placebo-controlled phase 1 and an open-label phase 2 clinical trials with a 6 months follow-up in K. EclinicalMedicine 2021, 39, 101078. [Google Scholar] [CrossRef]
- COVID-19 Treatment Guidelines. What’s New in the Guidelines. Available online: https://www.covid19treatmentguidelines.nih.gov/about-the-guidelines/whats-new/ (accessed on 3 August 2023).
- Levin, E.G.; Lustig, Y.; Cohen, C.; Fluss, R.; Indenbaum, V.; Amit, S.; Doolman, R.; Asraf, K.; Mendelson, E.; Ziv, A.; et al. Waning Immune Humoral Response to BNT162b2 Covid-19 Vaccine over 6 Months. N. Engl. J. Med. 2021, 385, e84. [Google Scholar] [CrossRef]
- Crawford, K.H.D.; Dingens, A.S.; Eguia, R.; Wolf, C.R.; Wilcox, N.; Logue, J.K.; Shuey, K.; Casto, A.M.; Fiala, B.; Wrenn, S.; et al. Dynamics of Neutralizing Antibody Titers in the Months After Severe Acute Respiratory Syndrome Coronavirus 2 Infection. J. Infect. Dis. 2021, 223, 197–205. [Google Scholar] [CrossRef] [PubMed]
- Fadlyana, E.; Rusmil, K.; Tarigan, R.; Rahmadi, A.R.; Prodjosoewojo, S.; Sofiatin, Y.; Khrisna, C.V.; Sari, R.M.; Setyaningsih, L.; Surachman, F.; et al. A phase III, observer-blind, randomized, placebo-controlled study of the efficacy, safety, and immunogenicity of SARS-CoV-2 inactivated vaccine in healthy adults aged 18–59 years: An interim analysis in Indonesia. Vaccine 2021, 39, 6520–6528. [Google Scholar] [CrossRef]
- Trougakos, I.P.; Terpos, E.; Alexopoulos, H.; Politou, M.; Paraskevis, D.; Scorilas, A.; Kastritis, E.; Andreakos, E.; Dimopoulos, M.A. Adverse effects of COVID-19 mRNA vaccines: The spike hypothesis. Trends Mol. Med. 2022, 28, 542–554. [Google Scholar] [CrossRef] [PubMed]
- Kozlovskaya, L.I.; Piniaeva, A.N.; Ignatyev, G.M.; Gordeychuk, I.V.; Volok, V.P.; Rogova, Y.V.; Shishova, A.A.; Kovpak, A.A.; Ivin, Y.Y.; Antonova, L.P.; et al. Long-term humoral immunogenicity, safety and protective efficacy of inactivated vaccine against COVID-19 (CoviVac) in preclinical studies. Emerg. Microbes Infect. 2021, 10, 1790–1806. [Google Scholar] [CrossRef] [PubMed]
- Рoсстат—Всерoссийская Перепись Населения 2020 Гoда. Available online: https://rosstat.gov.ru/vpn/2020 (accessed on 4 August 2023).
- Vorovitch, M.F.; Grishina, K.G.; Volok, V.P.; Chernokhaeva, L.L.; Grishin, K.V.; Karganova, G.G.; Ishmukhametov, A.A. Evervac: Phase I/II study of immunogenicity and safety of a new adjuvant-free TBE vaccine cultivated in Vero cell culture. Hum. Vaccines Immunother. 2020, 16, 2123–2130. [Google Scholar] [CrossRef]
- Piniaeva, A.; Ignatyev, G.; Kozlovskaya, L.; Ivin, Y.; Kovpak, A.; Ivanov, A.; Shishova, A.; Antonova, L.; Khapchaev, Y.; Feldblium, I.; et al. Immunogenicity and Safety of Inactivated Sabin-Strain Polio Vaccine “PoliovacSin”: Clinical Trials Phase I and II. Vaccines 2021, 9, 565. [Google Scholar] [CrossRef] [PubMed]
- COVID-19 incidence. Available online: https://www.rospotrebnadzor.ru (accessed on 27 July 2023).
- Prévost, J.; Gasser, R.; Beaudoin-Bussières, G.; Richard, J.; Duerr, R.; Laumaea, A.; Anand, S.P.; Goyette, G.; Benlarbi, M.; Ding, S.; et al. Cross-Sectional Evaluation of Humoral Responses against SARS-CoV-2 Spike. Cell Rep. Med. 2020, 1, 100126. [Google Scholar] [CrossRef]
- Wang, X.; Guo, X.; Xin, Q.; Pan, Y.; Hu, Y.; Li, J.; Chu, Y.; Feng, Y.; Wang, Q. Neutralizing Antibody Responses to Severe Acute Respiratory Syndrome Coronavirus 2 in Coronavirus Disease 2019 Inpatients and Convalescent Patients. Clin. Infect. Dis. 2020, 71, 2688–2694. [Google Scholar] [CrossRef]
- Cho, A.; Muecksch, F.; Schaefer-Babajew, D.; Wang, Z.; Finkin, S.; Gaebler, C.; Ramos, V.; Cipolla, M.; Mendoza, P.; Agudelo, M.; et al. Anti-SARS-CoV-2 receptor-binding domain antibody evolution after mRNA vaccination. Nature 2021, 600, 517–522. [Google Scholar] [CrossRef]
- Khoury, D.S.; Cromer, D.; Reynaldi, A.; Schlub, T.E.; Wheatley, A.K.; Juno, J.A.; Subbarao, K.; Kent, S.J.; Triccas, J.A.; Davenport, M.P. Neutralizing antibody levels are highly predictive of immune protection from symptomatic SARS-CoV-2 infection. Nat. Med. 2021, 27, 1205–1211. [Google Scholar] [CrossRef]
- Lazarus, R.; Taucher, C.; Brown, C.; Čorbic Ramljak, I.; Danon, L.; Dubischar, K.; Duncan, C.J.A.; Eder-Lingelbach, S.; Faust, S.N.; Green, C.; et al. Safety and immunogenicity of the inactivated whole-virus adjuvanted COVID-19 vaccine VLA2001: A randomized, dose escalation, double-blind phase 1/2 clinical trial in healthy adults. J. Infect. 2022, 85, 306–317. [Google Scholar] [CrossRef] [PubMed]
- Kozlovskaya, L.; Gordeychuk, I.; Piniaeva, A.; Kovpak, A.; Shishova, A.; Lunin, A.; Shustova, E.; Apolokhov, V.; Fominykh, K.; Ivin, Y.; et al. CoviVac vaccination induces production of neutralizing antibodies against Delta and Omicron variants of SARS-CoV-2. MedRxiv 2022. [Google Scholar] [CrossRef]
- Bagrov, D.V.; Glukhov, G.S.; Moiseenko, A.V.; Karlova, M.G.; Litvinov, D.S.; Zaitsev, P.А.; Kozlovskaya, L.I.; Shishova, A.A.; Kovpak, A.A.; Ivin, Y.Y.; et al. Structural characterization of β-propiolactone inactivated severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) particles. Microsc. Res. Tech. 2022, 85, 562–569. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Demographic and Anthropometric Parameters | Total Participants | Vaccine | Placebo | |
|---|---|---|---|---|
| n (%) | ||||
| Safety assessment (Stages 1–3) | ||||
| No. of participants | 398 | 298 | 100 | |
| Age, years | Mean ± SD | 33.2 ± 11.8 | 33.1 ± 11.8 | 33.5 ± 12.1 |
| Sex | F | 144 (36.2) | 110 (36.9) | 34 (34) |
| M | 254 (63.8) | 188 (63.1) | 66 (66) | |
| BMI, kg/m2 | Mean ± SD | 23.9 ± 2.8 | 23.8 ± 2.8 | 24.0 ± 2.7 |
| Immunogenicity assessment (Stage 3) | ||||
| No. of participants | 167 | 122 | 45 | |
| Age, years | Mean ± SD | 34.4 ± 12.9 | 34.6 ± 12.9 | 33.6 ± 13.3 |
| Sex | F | 61 (36.5) | 46 (37.7) | 15 (33.3) |
| M | 106 (63.5) | 76 (63.3) | 30 (66.7) | |
| BMI, kg/m2 | Mean ± SD | 24.1 ± 2.7 | 24.1 ± 3.2 | 24.1 ± 2.7 |
| Demographic and Anthropometric Parameters | Total Participants | |
|---|---|---|
| n (%) | ||
| No. of participants | 200 | |
| Age, years | Mean ± SD | 67.26 ± 6.29 |
| Sex | F | 130 (65) |
| M | 70 (35) | |
| BMI, kg/m2 | Mean ± SD | 27.09 ± 4.83 |
| Adverse Event | Score | Vaccine Number of Participants with AEs (%, 95% CI)/Total Number of AEs | Placebo Number of Participants with AEs (%, 95% CI)/Total Number of AEs | ||||
|---|---|---|---|---|---|---|---|
| Total Participants N = 298 | Within 28 Days After | Total Participants N = 100 | Within 28 Days After | ||||
| First Dose | Second Dose | First Dose | Second Dose | ||||
| Local and systemic reactions | Mild | 57 (19.1%. 15.1–24.0%)/80 | 33 (11.1%. 8.0–15.1%)/37 | 34 (11.4%. 8.3–15.5%)/43 | 16 (16%. 10.1–24.4%)/23 | 7 (7%. 3.4–13.7%)/8 | 10 (10%. 5.5–17.4%)/15 |
| Moderate | 3 (1%. 0.3–2.9%)/3 | 2 (0.7%. 0.2–2.4%)/2 | 1 (0.3%. 0.1–1.9%)/1 | ||||
| Severe | 1 (0.3%. 0.1–1.9%)/1 | - | 1 (0.3%. 0.1–1.9%)/1 | ||||
| Pain at the injection site | Mild | 47 (15.8%. 12.1–20.3%)/55 * | 30 (10.1%. 7.1–14.0%)/30 | 25 (8.4%. 5.7–12.1%)/25 | 11 (11%. 6.3–18.6%)/12 * | 5 (5%. 2.2–11.2%)/5 | 7 (7%. 3.4–13.7%)/7 |
| Moderate | 1 (0.3%. 0.1–1.9%)/1 | 1 (0.3%. 0.1–1.9%)/1 | |||||
| Induration at the injection site | Mild | 3 (1%. 0.3–2.9%)/3 | 1 (0.3%. 0.1–1.9%)/1 | 2 (0.7%. 0.2–2.4%)/2 | 3 (3%. 1.0–8.5%)/3 | - | 3 (3%. 1.0–8.5%)/3 |
| Hematoma at the injection site | Mild | - | - | - | 1 (1%. 0.2–5.4%)/1 | 1 (1%. 0.2–5.4%)/1 | - |
| Swelling at the injection site | Mild | 1 (1%. 0.2–5.4%)/1 | 1 (1%. 0.2–5.4%)/1 | ||||
| Itching at the injection site | Mild | 1 (1%. 0.2–5.4%)/1 | 1 (1%. 0.2–5.4%)/1 | ||||
| Fever | Mild | 11 (3.7%. 2.1–6.5%)/12 | 5 (1.7%. 0.7–3.9%)/5 | 6 (2%. 0.9–4.3%)/7 | 2 (2%. 0.6–7.0%)/2 | 2 (2%. 0.6–7.0%)/2 | - |
| Moderate | 2 (0.7%. 0.2–2.4%)/2 | 1 (0.3%. 0.1–1.9%)/1 | 1 (0.3%. 0.1–1.9%)/1 | - | - | - | |
| Malaise | Mild | 4 (1.3%. 0.5–3.4%)/10 | 1 (0.3%. 0.1–1.9%)/1 | 3 (1%. 0.3–2.9%)/9 | 2 (2%. 0.6–7.0%)/3 | - | 2 (2%. 0.6–7.0%)/3 |
| Severe | 1 (0.3%. 0.1–1.9%)/1 | - | 1 (0.3%. 0.1–1.9%)/1 | - | - | - | |
| Laboratory methods | Mild | 19 (6.4%. 4.1–9.7%)/22 | 7 (2.3%. 1.1–4.8%)/7 | 12 (4%)/15 | 7 (7%. 3.4–13.7%)/7 | 2 (2%. 0.6–7.0%)/2 | 5 (5%. 2.2–11.2%)/5 |
| Moderate | 3 (1%. 0.3–2.9%)/3 | 1 (0.3%. 0.1–1.9%)/1 | 2 (0.7%. 0.2–2.4%)/2 | ||||
| Increased leukocyte count | Moderate | 1 (0.3%. 0.1–1.9%)/1 | 1 (0.3%. 0.1–1.9%)/1 | - | - | - | - |
| Positive SARS-CoV-2 PCR test | Mild | 17 (5.7%. 3.6–8.9%)/17 | 7 (2.3%. 1.1–4.8%)/7 | 10 (3.4%. 1.8–6.1%)/10 | 6 (6%. 2.8–12.5%)/6 | 2 (2%. 0.6–7.0%)/2 | 4 (4%. 1.6–9.8%)/4 |
| Moderate | 2 (0.7%. 0.2–2.4%)/2 | 2 (0.7%. 0.2–2.4%)/2 | |||||
| Increased creatine phosphokinase level | Mild | 1 (0.3%. 0.1–1.9%)/1 | - | 1 (0.3%. 0.1–1.9%)/1 | |||
| Moderate | 2 (0.7%. 0.2–2.4%)/2 | 2 (0.7%. 0.2–2.4%)/2 | 1 (1%. 0.2–5.4%)/1 | - | 1 (1%. 0.2–5.4%)/1 | ||
| Increased ALT level | Mild | 1 (0.3%. 0.1–1.9%)/1 | - | 1 (0.3%. 0.1–1.9%)/1 | - | - | - |
| Increased AST level | Mild | 1 (0.3%. 0.1–1.9%)/1 | - | 1 (0.3%. 0.1–1.9%)/1 | - | - | - |
| Increased CRP level | Mild | 1 (0.3%. 0.1–1.9%)/1 | - | 1 (0.3%. 0.1–1.9%)/1 | - | - | - |
| Blood and lymphatic system disorders | Mild | 1 (0.3%. 0.1–1.9%)/1 | 1 (0.3%. 0.1–1.9%)/1 | - | |||
| Inguinal lymphadenitis | Mild | 1 (0.3%. 0.1–1.9%)/1 | 1 (0.3%. 0.1–1.9%)/1 | - | - | - | - |
| Blood vessel disorders | 1 (1%. 0.2–5.4%)/1 | 1 (1%. 0.2–5.4%)/1 | - | ||||
| Deep venous leg thrombosis | Moderate | - | - | - | 1 (1%. 0.2–5.4%)/1 | 1 (1%. 0.2–5.4%)/1 | - |
| Infections and parasitic invasions | Mild | 22 (7.4%. 4.9–10.9%)/22 | 15 (5%. 2.2–11.2%)/15 | 7 (2.3%. 1.1–4.8%)/7 | 3 (3%. 1.0–8.5%)/3 | 2 (2%. 0.6–7.0%)/2 | 1 (1%. 0.2–5.4%)/1 |
| Moderate | 7 (2.3%. 1.1–4.8%)/7 | 3 (1%. 0.3–2.9%)/3 | 4 (1.3%. 0.5–3.4%)/4 | ||||
| Severe | 1 (1%. 0.2–5.4%)/1 | - | 1 (1%. 0.2–5.4%)/1 | ||||
| SARS-CoV-2 infection | Mild | 20 (6.7%. 4.4–10.1%)/20 | 14 (4.7%. 2.8–7.7%)/14 | 6 (2%. 0.9–4.3%)/6 | 3 (3%. 1.0–8.5%)/3 | 2 (2%. 0.6–7.0%)/2 | 1 (1%. 0.2–5.4%)/1 |
| Moderate | 5 (1.7%. 0.7–3.9%)/5 | 2 (0.7%. 0.2–2.4%)/2 | 3 (1%. 0.3–2.9%)/3 | - | - | - | |
| Severe | - | - | - | 1 (1%. 0.2–5.4%)/1 | - | 1 (1%. 0.2–5.4%)/1 | |
| Candidiasis | Mild | 1 (0.3%. 0.1–1.9%)/1 | - | 1 (0.3%. 0.1–1.9%)/1 | - | - | - |
| Other upper respiratory tract infections | Mild | 1 (0.3%. 0.1–1.9%)/1 | 1 (0.3%. 0.1–1.9%)/1 | - | - | - | - |
| Moderate | 2 (0.7%. 0.2–2.4%)/2 | 1 (0.3%. 0.1–1.9%)/1 | 1 (0.3%. 0.1–1.9%)/1 | - | - | - | |
| Nervous system disorders | Mild | 11 (3.7%. 2.1–6.5%)/20 | 4 (1.3%. 0.5–3.4%)/4 | 9 (3%. 1.6–5.6%)/16 | 6 (6%. 2.8–12.5%)/12 | 3 (3%. 1.0–8.5%)/3 | 3 (3%. 1.0–8.5%)/9 |
| Headache | Mild | 11 (3.7%. 2.1–6.5%)/19 | 4 (1.3%. 0.5–3.4%)/4 | 8 (2.7%. 1.4–5.2%)/15 | 6 (6%. 2.8–12.5%)/12 | 3 (3%. 1.0–8.5%)/3 | 3 (3%. 1.0–8.5%)/9 |
| Dizziness | Mild | 1 (0.3%. 0.1–1.9%)/1 | - | 1 (0.3%. 0.1–1.9%)/1 | - | - | - |
| Musculoskeletal and connective tissue disorders | Mild | 4 (1.3%. 0.5–3.4%)/6 | 2 (0.7%. 0.2–2.4%)/3 | 2 (0.7%. 0.2–2.4%)/3 | |||
| Moderate | 1 (0.3%. 0.1–1.9%)/1 | 1 (0.3%. 0.1–1.9%)/2 | 1 (1%. 0.2–5.4%)/1 | 1 (1%. 0.2–5.4%)/1 | - | ||
| Arthralgia | Mild | 2 (0.7%. 0.2–2.4%)/2 | 1 (0.3%. 0.1–1.9%)/1 | 1 (0.3%. 0.1–1.9%)/1 | - | - | - |
| Moderate | 1 (0.3%. 0.1–1.9%)/1 | - | 1 (0.3%. 0.1–1.9%)/1 | - | - | - | |
| Lumbar pain | Moderate | - | - | - | 1 (1%. 0.2–5.4%)/1 | 1 (1%. 0.2–5.4%)/1 | - |
| Myalgia | Mild | 4 (1.3%. 0.5–3.4%)/4 | 2 (0.7%. 0.2–2.4%)/2 | 2 (0.7%. 0.2–2.4%)/2 | - | - | - |
| Moderate | 1 (0.3%. 0.1–1.9%)/1 | - | 1 (0.3%. 0.1–1.9%)/1 | - | - | - | |
| Gastrointestinal tract disorders | Mild | 3 (1%. 0.3–2.9%)/3 | 1 (0.3%. 0.1–1.9%)/1 | 2 (0.7%. 0.2–2.4%)/2 | 1 (1%. 0.2–5.4%)/1 | - | 1 (1%. 0.2–5.4%)/1 |
| Moderate | 1 (0.3%. 0.1–1.9%)/1 | - | 1 (0.3%. 0.1–1.9%)/1 | ||||
| Diarrhea | Mild | 1 (0.3%. 0.1–1.9%)/1 | - | 1 (0.3%. 0.1–1.9%)/1 | 1 (1%. 0.2–5.4%)/1 | - | 1 (1%. 0.2–5.4%)/1 |
| Pyrosis | Mild | 1 (0.3%. 0.1–1.9%)/1 | 1 (0.3%. 0.1–1.9%)/1 | - | - | - | - |
| Nausea | Mild | 1 (0.3%. 0.1–1.9%)/1 | - | 1 (0.3%. 0.1–1.9%)/1 | - | - | - |
| Moderate | 1 (0.3%. 0.1–1.9%)/1 | - | 1 (0.3%. 0.1–1.9%)/1 | - | - | - | |
| Hearing disorders | Mild | 1 (0.3%. 0.1–1.9%)/1 | 1 (0.3%. 0.1–1.9%)/1 | - | |||
| Ear congestion | Mild | 1 (0.3%. 0.1–1.9%)/1 | 1 (0.3%. 0.1–1.9%)/1 | - | - | - | - |
| Disorders of respiratory system and mediastinal organs | Mild | 6 (2%. 0.9–4.3%)/6 | 2 (0.7%. 0.2–2.4%)/2 | 4 (1.3%. 0.5–3.4%)/4 | 3 (3%. 1.0–8.5%)/5 | 1 (1%. 0.2–5.4%)/1 | 2 (2%. 0.6–7.0%)/4 |
| Moderate | 1 (0.3%. 0.1–1.9%)/1 | 1 (0.3%. 0.1–1.9%)/1 | |||||
| Throat pain | Mild | 1 (0.3%. 0.1–1.9%)/1 | - | 1 (0.3%. 0.1–1.9%)/1 | 1 (1%. 0.2–5.4%)/2 | - | 1 (1%. 0.2–5.4%)/2 |
| Moderate | 1 (0.3%. 0.1–1.9%)/1 | 1 (0.3%. 0.1–1.9%)/1 | |||||
| Pain in the oropharynx | Mild | 1 (0.3%. 0.1–1.9%)/1 | - | 1 (0.3%. 0.1–1.9%)/1 | 1 (1%. 0.2–5.4%)/1 | - | 1 (1%. 0.2–5.4%)/1 |
| Cough | Mild | 1 (0.3%. 0.1–1.9%)/1 | - | 1 (0.3%. 0.1–1.9%)/1 | 1 (1%. 0.2–5.4%)/1 | - | 1 (1%. 0.2–5.4%)/1 |
| Impaired sense of smell | Mild | 1 (0.3%. 0.1–1.9%)/1 | 1 (0.3%. 0.1–1.9%)/1 | - | - | - | - |
| Dyspnea | Mild | 1 (0.3%. 0.1–1.9%)/1 | - | 1 (0.3%. 0.1–1.9%)/1 | - | - | - |
| Sore throat | Mild | 1 (0.3%. 0.1–1.9%)/1 | 1 (0.3%. 0.1–1.9%)/1 | - | 1 (1%. 0.2–5.4%)/1 | 1 (1%. 0.2–5.4%)/1 | - |
| Metabolic disorders | Mild | 2 (0.7%. 0.2–2.4%)/8 | - | 2 (0.7%. 0.2–2.4%)/8 | 1 (1%. 0.2–5.4%)/1 | - | 1 (1%. 0.2–5.4%)/1 |
| Moderate | 1 (0.3%. 0.1–1.9%)/1 | - | 1 (0.3%. 0.1–1.9%)/1 | ||||
| Impaired appetite | Mild | 2 (0.7%. 0.2–2.4%) /8 | - | 2 (0.7%. 0.2–2.4%)/8 | 1 (1%. 0.2–5.4%)/1 | - | 1 (1%. 0.2–5.4%)/1 |
| Moderate | 1 (0.3%. 0.1–1.9%)/1 | - | 1 (0.3%. 0.1–1.9%)/1 | - | - | - | |
| Other | Severe | 1 (0.3%. 0.1–1.9%)/1 | - | 1 (0.3%. 0.1–1.9%)/1 | |||
| Death from acute circulatory disorder ** | Severe | 1 (0.3%. 0.1–1.9%)/1 | - | 1 (0.3%. 0.1–1,9%)/1 | |||
| Adverse Event | Score | Number of Participants with AEs (%)/Number of AEs | |||
|---|---|---|---|---|---|
| Within 21 Days After | Total Participants, N = 199 | ||||
| First Dose | Second Dose | Third Dose | |||
| Local and systemic reactions | Mild | 56 (28%)/85 | 45 (22.5%)/74 | 32 (16%)/55 | 79 (39.5%)/214 |
| Moderate | 19 (9.5%)/26 | 8 (4%)/8 | 11 (5.5%)/13 | 23 (11.5%)/47 | |
| Severe | 3 (1.5%)/4 | 2 (1%)/2 | – | 5 (2.5%)/6 | |
| Asthenia | Mild | 4 (2%)/4 | 1 (0.5%)/1 | – | 5 (2.5%)/5 |
| Pain | Mild | – | 1 (0.5%)/1 | 2 (1%)/2 | 3 (1.5%)/3 |
| Pain at the injection site | Mild | 43 (21.5%)/43 | 35 (17.5%)/36 | 17 (8.5%)/17 | 62 (31%)/96 |
| Moderate | 10 (5%)/10 | 5 (2.5%)/5 | 7 (3.5%)/7 | 16 (8%)/22 | |
| Severe | 3 (1.5%)/3 | 2 (1%)/2 | – | 5 (2.5%)/5 | |
| Itching at the injection site | Mild | 4 (2%)/4 | 3 (1.5%)/3 | 7 (3.5%)/7 | 11 (5.5%)/14 |
| Moderate | – | 1 (0.5%)/1 | – | 1 (0.5%)/1 | |
| Chills | Mild | 4 (2%)/5 | 3 (1.5%)/3 | 1 (0.5%)/1 | 7 (3.5%)/9 |
| Moderate | 2 (1%)/2 | – | – | 2 (1%)/2 | |
| Swelling at the injection site | Mild | 1 (0.5%)/1 | 2 (1%)/3 | 3 (1.5%)/3 | 5 (2.5%)/7 |
| Foreign body sensation | Mild | 1 (0.5%)/1 | – | – | 1 (0.5%)/1 |
| Fever | Mild | 3 (1.5%)/3 | 1 (0.5%)/1 | 3 (1.5%)/3 | 7 (3.5%)/7 |
| Moderate | 1 (0.5%)/1 | – | – | 1 (0.5%)/1 | |
| Malaise | Mild | – | 1 (0.5%)/1 | – | 1 (0.5%)/1 |
| Induration at the injection site | Mild | 3 (1.5%)/3 | 7 (3.5%)/8 | 6 (3%)/6 | 11 (5.5%)/17 |
| Moderate | 1 (0.5%)/1 | – | – | 1 (0.5%)/1 | |
| Fatigue | Mild | 15 (7.5%)/17 | 12 (6%)/15 | 10 (5%)/11 | 27 (13.5%)/43 |
| Moderate | 10 (5%)/12 | 2 (1%)/2 | 5 (2.5%)/6 | 15 (12.5%)/20 | |
| Severe | 1 (0.5%)/1 | – | – | 1 (0.5%)/1 | |
| Discomfort at the injection site | Mild | 1 (0.5%)/1 | – | – | 1 (0.5%)/1 |
| Erythema at the injection site | Mild | 3 (1.5%)/3 | 2 (1%)/2 | 5 (2.5%)/5 | 9 (4.5%)/10 |
| Laboratory methods | Mild | 68 (34%)/88 | 45 (22.5%)/57 | 72 (36%)/109 | 133 (66.5%)/254 |
| Moderate | 9 (4.5%)/11 | 12 (6%)/13 | 19 (9.5%)/22 | 36 (18%)/46 | |
| Severe | – | 7 (3.5%)/7 | 9 (4.5%)/11 | 15 (12.5%)/18 | |
| Proteinuria | Mild | 2 (1%)/2 | – | 3 (1.5%)/3 | 5 (2.5%)/5 |
| Moderate | 1 (0.5%)/1 | – | – | 1 (0.5%)/1 | |
| Glycosuria | Severe | – | – | 1 (0.5%)/1 | 1 (0.5%)/1 |
| Leukocytes in urine | Mild | 2 (1%)/2 | 3 (1.5%)/3 | 5 (2.5%)/5 | 9 (4.5%)/10 |
| Abnormal ALT level | Moderate | 3 (1.5%)/3 | – | – | 3 (1.5%)/3 |
| Abnormal glucose level | Severe | – | – | 1 (0.5%)/1 | 1 (0.5%)/1 |
| Abnormal urea level | Moderate | – | 1 (0.5%)/1 | 1 (0.5%)/1 | 2 (1%)/2 |
| Severe | – | – | 1 (0.5%)/1 | 1 (0.5%)/1 | |
| Abnormal CRP level | Mild | 1 (0.5%)/1 | 1 (0.5%)/1 | 1 (0.5%)/2 | 3 (1.5%)/4 |
| Moderate | – | – | 3 (1.5%)/3 | 3 (1.5%)/3 | |
| Abnormal cholesterol level | Mild | – | – | 1 (0.5%)/1 | 1 (0.5%)/1 |
| Moderate | – | – | 2 (1%)/2 | 2 (1%)/2 | |
| Abnormal blood ALP level | Mild | – | – | 2 (1%)/3 | 2 (1%)/3 |
| Moderate | – | 3 (1.5%)/3 | – | 3 (1.5%)/3 | |
| Increased arterial blood pressure | Mild | 4 (2%)/5 | 2 (1%)/2 | 1 (0.5%)/2 | 4 (2%)/9 |
| Severe | – | 1 (0.5%)/1 | 1 (0.5%)/1 | 2 (1%)/2 | |
| Increased diastolic blood pressure | Mild | 5 (2.5%)/5 | 4 (2%)/4 | 1 (0.5%)/1 | 10 (5%)/10 |
| Increased relative density of urine | Mild | – | – | 1 (0.5%)/1 | 1 (0.5%)/1 |
| Increased systolic blood pressure | Mild | 5 (2.5%)/5 | 3 (1.5%)/3 | 1 (0.5%)/1 | 9 (4.5%)/9 |
| Increased erythrocyte sedimentation rate | Mild | 2 (1%)/2 | 1 (0.5%)/1 | 1 (0.5%)/1 | 4 (2%)/4 |
| Increased ALT level | Mild | 4 (2%)/4 | 1 (0.5%)/1 | 6 (3%)/7 | 11 (5.5%)/12 |
| Increased AST level | Mild | 5 (2.5%)/5 | 2 (1%)/2 | 6 (3%)/8 | 12 (6%)/15 |
| Moderate | – | – | 1 (0.5%)/1 | 1 (0.5%)/1 | |
| Increased bilirubin level | Mild | 2 (1%)/2 | 2 (1%)/2 | 3 (1.5%)/3 | 6 (3%)/7 |
| Moderate | 1 (0.5%)/1 | 2 (1%)/2 | 2 (1%)/2 | 5 (2.5%)/5 | |
| Increased glucose level | Mild | 2 (1%)/2 | 2 (1%)/2 | 3 (1.5%)/3 | 7 (3.5%)/7 |
| Moderate | 2 (1%)/2 | 1 (0.5%)/1 | 4 (2%)/4 | 6 (3%)/7 | |
| Severe | – | 1 (0.5%)/1 | – | 1 (0.5%)/1 | |
| Increased creatinine level | Mild | 1 (0.5%)/1 | 1 (0.5%)/1 | 1 (0.5%)/1 | 3 (1.5%)/3 |
| Increased creatine phosphokinase level | Mild | 3 (1.5%)/3 | 5 (2.5%)/5 | 7 (3.5%)/7 | 15 (7.5%)/16 |
| Moderate | 2 (1%)/2 | – | 1 (0.5%)/1 | 3 (1.5%)/3 | |
| Severe | – | 1 (0.5%)/1 | – | 1 (0.5%)/1 | |
| Increased urea phosphokinase level | Mild | 2 (1%)/2 | 3 (1.5%)/3 | 7 (3.5%)/7 | 11 (5.5%)/12 |
| Moderate | – | – | 1 (0.5%)/1 | 1 (0.5%)/1 | |
| Increased CRP level | Mild | 1 (0.5%)/1 | 2 (1%)/2 | 1 (0.5%)/1 | 4 (2%)/4 |
| Moderate | 1 (0.5%)/1 | 1 (0.5%)/1 | – | 2 (1%)/2 | |
| Increased transaminase levels | Mild | – | 1 (0.5%)/1 | – | 1 (0.5%)/1 |
| Increased cholesterol level | Mild | 4 (2%)/4 | 4 (2%)/4 | 10 (5%)/10 | 17 (8.5%)/18 |
| Moderate | – | 4 (2%)/4 | 5 (2.5%)/5 | 9 (4.5%)/9 | |
| Severe | – | 4 (2%)/4 | 5 (2.5%)/5 | 9 (4.5%)/9 | |
| Increased ALP level | Mild | 2 (1%)/2 | 1 (0.5%)/1 | 3 (1.5%)/3 | 5 (2.5%)/6 |
| Increased basophil count | Mild | 1 (0.5%)/1 | – | 1 (0.5%)/1 | 1 (0.5%)/2 |
| Increased leukocyte count | Mild | 6 (3%)/6 | 1 (0.5%)/1 | – | 7 (3.5%)/7 |
| Moderate | 1 (0.5%)/1 | – | – | 1 (0.5%)/1 | |
| Increased eosinophil count | Mild | 1 (0.5%)/1 | 2 (1%)/2 | 1 (0.5%)/1 | 4 (2%)/4 |
| SARS-CoV-2 infection | Moderate | – | 1 (0.5%)/1 | – | 1 (0.5%)/1 |
| Severe | – | – | 1 (0.5%)/1 | 1 (0.5%)/1 | |
| Decreased hemoglobin level | Mild | – | – | 4 (2%)/4 | 4 (2%)/4 |
| Decreased glucose level | Mild | – | – | 3 (1.5%)/3 | 3 (1.5%)/3 |
| Moderate | – | – | 1 (0.5%)/1 | 1 (0.5%)/1 | |
| Severe | – | – | 1 (0.5%)/1 | 1 (0.5%)/1 | |
| Decreased creatine phosphokinase level | Mild | – | – | 1 (0.5%)/1 | 1 (0.5%)/1 |
| Decreased total protein level | Mild | – | – | 2 (1%)/2 | 2 (1%)/2 |
| Decreased lymphocyte count | Mild | 2 (1%)/2 | 1 (0.5%)/1 | – | 3 (1.5%)/3 |
| Decreased neutrophil count | Mild | 8 (4%)/8 | 1 (0.5%)/1 | 2 (1%)/2 | 10 (5%)/11 |
| Decreased platelet count | Mild | 1 (0.5%)/1 | 1 (0.5%)/1 | – | 2 (1%)/2 |
| Increased lymphocyte count | Mild | 2 (1%)/2 | – | – | 2 (1%)/2 |
| Cylindruria | Mild | – | 1 (0.5%)/1 | – | 1 (0.5%)/1 |
| Erythrocytes in urine | Mild | 19 (9.5%)/19 | 12 (6%)/12 | 25 (12.5%)/25 | 52 (26%)/56 |
| Moderate | – | – | 1 (0.5%)/1 | 1 (0.5%)/1 | |
| Gastrointestinal tract disorders | Mild | 11 (5.5%)/11 | 3 (1.5%)/3 | 2 (1%)/3 | 14 (7%)/17 |
| Moderate | 2 (1%)/2 | – | 1 (0.5%)/1 | 3 (1.5%)/3 | |
| Abdominal discomfort | Mild | 1 (0.5%)/1 | – | – | 1 (0.5%)/1 |
| Abdominal pain | Mild | 1 (0.5%)/1 | – | – | 1 (0.5%)/1 |
| Lip pain | Mild | 1 (0.5%)/1 | – | – | 1 (0.5%)/1 |
| Diarrhea | Mild | 3 (1.5%)/3 | 2 (1%)/2 | 2 (1%)/2 | 6 (3%)/7 |
| Moderate | 1 (0.5%)/1 | – | 1 (0.5%)/1 | 2 (1%)/2 | |
| Dyspepsia | Mild | 2 (1%)/2 | – | – | 2 (1%)/2 |
| Toothache | Mild | – | 1 (0.5%)/1 | – | 1 (0.5%)/1 |
| Nausea | Mild | 3 (1.5%)/3 | – | 1 (0.5%)/1 | 4 (2%)/4 |
| Moderate | 1 (0.5%)/1 | – | – | 1 (0.5%)/1 | |
| Infections and parasitic invasions | Mild | 5 (2.5%)/5 | 6 (3%)/6 | 6 (3%)/6 | 17 (8.5%)/17 |
| Moderate | 3 (1.5%)/3 | 2 (1%)/2 | 4 (2%)/4 | 9 (4.5%)/9 | |
| Severe | 1 (0.5%)/1 | 1 (0.5%)/1 | 3 (1.5%)/3 | 5 (2.5%)/5 | |
| Upper respiratory tract infections | Mild | 1 (0.5%)/1 | 4 (2%)/4 | 2 (1%)/2 | 10 (5%)/10 |
| Moderate | – | 2 (1%)/2 | 1 (0.5%)/1 | 3 (1.5%)/3 | |
| SARS-CoV-2 infection | Mild | 2 (1%)/2 | 2 (1%)/2 | 4 (2%)/4 | 8 (4%)/8 |
| Moderate | 3 (1.5%)/3 | – | 2 (1%)/2 | 5 (2.5%)/5 | |
| Severe | 1 (0.5%)/1 | 1 (0.5%)/1 | 3 (1.5%)/3 | 5 (2.5%)/5 | |
| Nasal herpes simplex lesions | Mild | 1 (0.5%)/1 | – | – | 1 (0.5%)/1 |
| Herpes zoster | Moderate | – | – | 1 (0.5%)/1 | 1 (0.5%)/1 |
| Labial herpes simplex lesions | Mild | 1 (0.5%)/1 | – | – | 1 (0.5%)/1 |
| Metabolic and nutrition disorders | Mild | 6 (3%)/6 | 1 (0.5%)/1 | 9 (4.5%)/10 | 14 (7%)/17 |
| Moderate | – | 1 (0.5%)/1 | 2 (1%)/2 | 3 (1.5%)/3 | |
| Hyperglycemia | Mild | 1 (0.5%)/1 | 1 (0.5%)/1 | – | 2 (1%)/2 |
| Hypoglycemia | Mild | 1 (0.5%)/1 | – | 7 (3.5%)/7 | 8 (4%)/8 |
| Moderate | – | 1 (0.5%)/1 | 2 (1%)/2 | 3 (1.5%)/3 | |
| Hypoproteinemia | Mild | 4 (2%)/4 | – | 3 (1.5%)/3 | 5 (2.5%)/7 |
| Disorders of respiratory system and mediastinal organs | Mild | 7 (3.5%)/7 | 9 (4.5%)/13 | 8 (4%)/10 | 21 (10.5%)/31 |
| Moderate | 1 (0.5%)/1 | – | 1 (0.5%)/1 | 2 (1%)/2 | |
| Pain in the oropharynx | Mild | 1 (0.5%)/1 | 2 (1%)/2 | 1 (0.5%)/1 | 4 (2%)/4 |
| Moderate | – | – | 1 (0.5%)/1 | 1 (0.5%)/1 | |
| Nasal congestion | Mild | 1 (0.5%)/1 | 2 (1%)/2 | 1 (0.5%)/1 | 4 (2%)/4 |
| Cough | Mild | 3 (1.5%)/3 | 1 (0.5%)/1 | 2 (1%)/2 | 6 (3%)/6 |
| Dyspnea | Mild | – | 1 (0.5%)/1 | – | 1 (0.5%)/1 |
| Swelling of the pharynx | Mild | – | – | 2 (1%)/2 | 2 (1%)/2 |
| Sore throat | Mild | 2 (1%)/2 | 1 (0.5%)/1 | 1 (0.5%)/1 | 4 (2%)/4 |
| Rhinorrhea | Mild | 1 (0.5%)/1 | 5 (2.5%)/5 | 3 (1.5%)/3 | 8 (4%)/9 |
| Moderate | 1 (0.5%)/1 | – | – | 1 (0.5%)/1 | |
| Sneezing | Mild | – | 1 (0.5%)/1 | – | 1 (0.5%)/1 |
| Skin and subcutaneous tissue disorders | Mild | 3 (1.5%)/3 | 1 (0.5%)/1 | – | 4 (2%)/4 |
| Hyperhidrosis | Mild | 1 (0.5%)/1 | – | – | 1 (0.5%)/1 |
| Itching | Mild | 2 (1%)/2 | – | – | 2 (1%)/2 |
| Rash | Mild | – | 1 (0.5%)/1 | – | 1 (0.5%)/1 |
| Muscular. skeletal and connective tissue disorders | Mild | 14 (7%)/15 | 8 (4%)/9 | 7 (3.5%)/8 | 23 (11.5%)/32 |
| Moderate | 4 (2%)/4 | – | 2 (1%)/2 | 6 (3%)/6 | |
| Arthralgia | Mild | 2 (1%)/2 | 2 (1%)/2 | 1 (0.5%)/2 | 5 (2.5%)/6 |
| Pain in the limb | Mild | 1 (0.5%)/1 | – | 1 (0.5%)/1 | 2 (1%)/2 |
| Back pain | Mild | 1 (0.5%)/1 | – | – | 1 (0.5%)/1 |
| Moderate | – | – | 1 (0.5%)/1 | 1 (0.5%)/1 | |
| Myalgia | Mild | 10 (5%)/10 | 7 (3.5%)/7 | 5 (2.5%)/5 | 19 (9.5%)/22 |
| Moderate | 4 (2%)/4 | – | 1 (0.5%)/1 | 5 (2.5%)/5 | |
| Musculoskeletal discomfort | Mild | 1 (0.5%)/1 | – | – | 1 (0.5%)/1 |
| Nervous system disorders | Mild | 20 (10%)/26 | 18 (9%)/22 | 9 (4.5%)/11 | 37 (18.5%)/59 |
| Moderate | 1 (0.5%)/1 | 1 (0.5%)/1 | 3 (1.5%)/4 | 5 (2.5%)/6 | |
| Severe | – | – | 1 (0.5%)/1 | 1 (0.5%)/1 | |
| Insomnia | Mild | 1 (0.5%)/1 | 2 (1%)/2 | – | 3 (1.5%)/3 |
| Headache | Mild | 15 (7.5%)/20 | 15 (7.5%)/18 | 8 (4%)/9 | 32 (16%)/47 |
| Moderate | 1 (0.5%)/1 | 1 (0.5%)/1 | 3 (1.5%)/4 | 1 (0.5%)/1 | |
| Severe | – | – | 1 (0.5%)/1 | 1 (0.5%)/1 | |
| Dizziness | Mild | 2 (1%)/2 | 1 (0.5%)/1 | 1 (0.5%)/1 | 4 (2%)/4 |
| Discomfort in the head | Mild | – | 1 (0.5%)/1 | – | 1 (0.5%)/1 |
| Syncope | Mild | – | – | 1 (0.5%)/1 | 1 (0.5%)/1 |
| Somnolence | Mild | 2 (1%)/3 | – | – | 2 (1%)/3 |
| Eye disorders | Mild | 1 (0.5%)/1 | – | 1 (0.5%)/1 | 1 (0.5%)/2 |
| Hypersecretory lacrimation | Mild | 1 (0.5%)/1 | – | – | 1 (0.5%)/1 |
| Photopsy | Mild | – | – | 1 (0.5%)/1 | 1 (0.5%)/1 |
| Hearing disorders | Mild | 1 (0.5%)/1 | – | 1 (0.5%)/1 | 2 (1%)/2 |
| Ear congestion | Mild | 1 (0.5%)/1 | – | – | 1 (0.5%)/1 |
| tinnitus | Mild | – | – | 1 (0.5%)/1 | 1 (0.5%)/1 |
| Renal and urinary tract disorders | Mild | 6 (3%)/6 | – | 3 (1.5%)/3 | 9 (5.5%)/9 |
| Moderate | – | 1 (0.5%)/1 | – | 1 (0.5%)/1 | |
| Severe | 1 (0.5%)/1 | – | – | 1 (0.5%)/1 | |
| Hematuria | Mild | 1 (0.5%)/1 | – | – | 1 (0.5%)/1 |
| Moderate | – | 1 (0.5%)/1 | – | 1 (0.5%)/1 | |
| Glycosuria | Severe | 1 (0.5%)/1 | – | – | 1 (0.5%)/1 |
| Leukocyturia | Mild | 4 (2%)/4 | – | – | 4 (2%)/4 |
| Proteinuria | Mild | 1 (0.5%)/1 | – | 3 (1.5%)/3 | 4 (2%)/4 |
| Heart disorders | Mild | 5 (2.5%)/5 | – | 3 (1.5%)/4 | 8 (4%)/9 |
| Moderate | 1 (0.5%)/1 | – | – | 1 (0.5%)/1 | |
| Arrhythmia | Mild | – | – | 1 (0.5%)/1 | 1 (0.5%)/2 |
| Moderate | 1 (0.5%)/1 | – | – | 1 (0.5%)/1 | |
| Chest pain | Mild | 1 (0.5%)/1 | – | – | 1 (0.5%)/1 |
| Bradycardia | Mild | 2 (1%)/2 | – | – | 2 (1%)/2 |
| Discomfort in the heart | Mild | – | – | 1 (0.5%)/2 | 1 (0.5%)/2 |
| Stenocardia | Mild | 1 (0.5%)/1 | – | 1 (0.5%)/1 | 2 (1%)/2 |
| Tachycardia | Mild | 1 (0.5%)/1 | – | – | 1 (0.5%)/1 |
| Vascular disorders | Mild | 1 (0.5%)/1 | – | 2 (1%)/2 | 3 (1.5%)/3 |
| Hypertensive crisis | Mild | 1 (0.5%)/1 | – | – | 1 (0.5%)/1 |
| Blood vessel rupture | Mild | – | – | 1 (0.5%)/1 | 1 (0.5%)/1 |
| Nosebleed | Mild | – | – | 1 (0.5%)/1 | 1 (0.5%)/1 |
| Injuries. intoxications and complications of procedures | Moderate | 1 (0.5%)/1 | 1 (0.5%)/1 | – | 2 (1%)/2 |
| Fracture of the upper limb | Moderate | 1 (0.5%)/1 | – | – | 1 (0.5%)/1 |
| Meniscus injury | Moderate | – | 1 (0.5%)/1 | – | 1 (0.5%)/1 |
| Group | N | Positive, n (%, 95% CI) | |||||
|---|---|---|---|---|---|---|---|
| Screening | Day 7 | Day 14 | Day 21 (7 Days after the 2nd Vaccination) | Day 28 (14 Days after the 2nd Vaccination) | Day 42 (28 Days after the 2nd Vaccination) | ||
| Vaccine | 122 | 53 (43.4, 35.0–52.3) | 68 (55.7, 46.9–64.2) | 92 (75.4, 67.1–82.2) | 112 (91.8, 85.6–95.5) | 112 (91.8, 85.6–95.5) | 113 (92.6, 86.6–96.1) |
| Placebo | 45 | 17 (37.8, 25.1–52.4) | 18 (40.0, 27.0–54.6) | 19 (42.2, 29.0–56.7) | 17 (38.6, 25.7–53.4) 1 | 17 (37.8, 25.1–52.4) | 18 (40.9, 27.7–55.6) 1 |
| Immunogenicity Parameters | Seroconversion Rate | ||
|---|---|---|---|
| At Screening | 21 Days after 2nd Vaccination | 21 Days after 3rd Vaccination | |
| Total participants | |||
| Number of participants, N | 199 | 175 | 168 |
| Seroconversion rate (%, 95% CI) | – | 80 (45.7%, 38.5–53.1%) | 122 (72.6%, 65.4–78.8%) |
| GMT (95% CI) | 15.97 (11.52–22.14) | 86.60 (65.03–115.33) | 145.76 (114.10–186.21) |
| GMT fold increase relative to screening | – | 4.76 | 7.88 |
| Seropositive at screening | |||
| Number of participants, N | 131 | 120 | 116 |
| Seroconversion rate (%, 95% CI) | – | 35 (29.2%, 21.8–37.8%) | 76 (65.5%, 56.5–73.5%) |
| GMT (95% CI) | 68.72 (53.22–88.74) | 197.15 (152.26–255.27) | 291.22 (239.58–353.98) |
| GMT fold increase relative to screening | – | 2.87 | 4.26 |
| Seronegative at screening | |||
| Number of participants, N | 68 | 55 | 52 |
| Seroconversion rate (%, 95% CI) | 45 (81.8%, 69.7–89.8%) | 46 (88.5%, 77–94.6%) | |
| GMT | 31.13 (20.21–47.94) | 14.39 (9.31–22.24) | |
| Group | Positive (%, 95% CI) | ||
|---|---|---|---|
| II (18–60 years) | IIb (Age 60+ years) | ||
| 28 d Post 2nd Vaccination | 21 d Post 2nd Vaccination | 21 d Post 3rd Vaccination | |
| All participants | |||
| Vaccine | N = 122 | N = 175 | N = 168 |
| 79 (64.8%, 55.9–72.7%) | 80 (45.7%, 38.5–53.1%) | 122 (72.6%, 65.4–78.8%) | |
| Placebo | N = 45 | – | – |
| 2 (4.5%, 1.3–15.1) | |||
| Participants Seronegative at Screening | |||
| Vaccine | N = 69 | N = 55 | N = 52 |
| 60 (86.9%, 77.0–93%) | 45 (81.8%, 69.7–89.8%) | 46 (88.5%, 77.0–94.6%) | |
| Placebo | N = 27 | – | – |
| 1 (3.7%, 0.7–18.3%) | |||
| Participants seropositive at screening | |||
| Vaccine | N = 53 | N = 120 | N = 116 |
| 19 (35.8%, 24.3–49.3%) | 35 (29.2%, 21.8–37.8%) | 76 (65.5%, 56.5–73.5%) | |
| Placebo | N = 17 | – | – |
| 1 (5.9%, 1.0–27.0%) | |||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gordeychuk, I.V.; Kozlovskaya, L.I.; Siniugina, A.A.; Yagovkina, N.V.; Kuzubov, V.I.; Zakharov, K.A.; Volok, V.P.; Dodina, M.S.; Gmyl, L.V.; Korotina, N.A.; et al. Safety and Immunogenicity of Inactivated Whole Virion COVID-19 Vaccine CoviVac in Clinical Trials in 18–60 and 60+ Age Cohorts. Viruses 2023, 15, 1828. https://doi.org/10.3390/v15091828
Gordeychuk IV, Kozlovskaya LI, Siniugina AA, Yagovkina NV, Kuzubov VI, Zakharov KA, Volok VP, Dodina MS, Gmyl LV, Korotina NA, et al. Safety and Immunogenicity of Inactivated Whole Virion COVID-19 Vaccine CoviVac in Clinical Trials in 18–60 and 60+ Age Cohorts. Viruses. 2023; 15(9):1828. https://doi.org/10.3390/v15091828
Chicago/Turabian StyleGordeychuk, Ilya V., Liubov I. Kozlovskaya, Aleksandra A. Siniugina, Nadezhda V. Yagovkina, Vladimir I. Kuzubov, Konstantin A. Zakharov, Viktor P. Volok, Maria S. Dodina, Larissa V. Gmyl, Natalya A. Korotina, and et al. 2023. "Safety and Immunogenicity of Inactivated Whole Virion COVID-19 Vaccine CoviVac in Clinical Trials in 18–60 and 60+ Age Cohorts" Viruses 15, no. 9: 1828. https://doi.org/10.3390/v15091828