
CSF Inflammation Markers Associated with Asymptomatic Viral Escape in Cerebrospinal Fluid of HIV-Positive Individuals on Antiretroviral Therapy
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Participants
2.2. Neurocognitive Testing and HAND Diagnoses
2.3. Meso Scale Discovery Assays
2.4. Measurement of CSF/Plasma Albumin Ratio
2.5. Statistical Analysis
3. Results
3.1. Characteristics of the Study Cohort
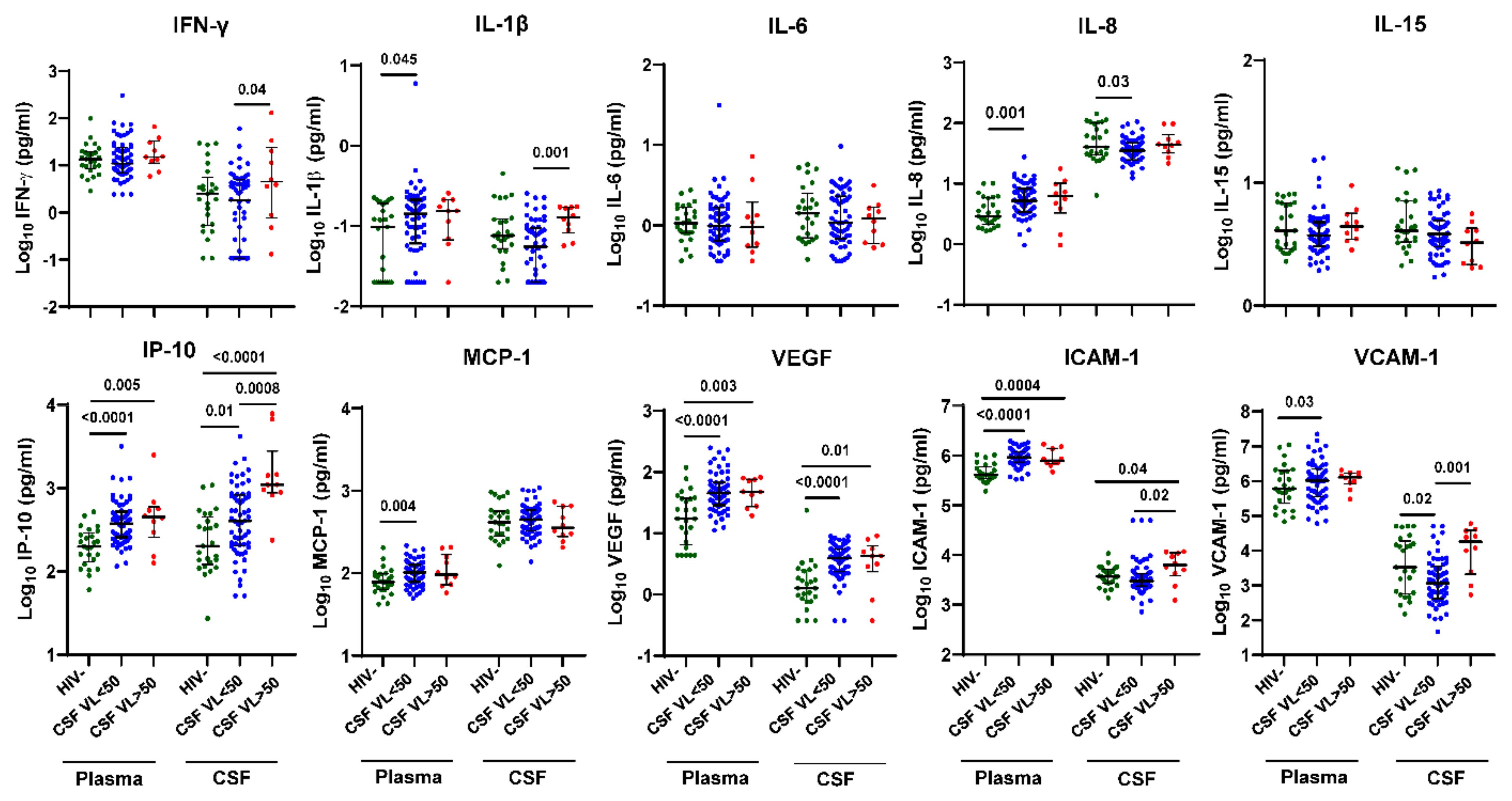
3.2. Increased Inflammation Biomarkers and Cell Adhesion Molecules in CSF But Not Plasma of HIV+ Individuals on ART with CSF VL > 50 Copies/mL vs. <50 Copies/mL
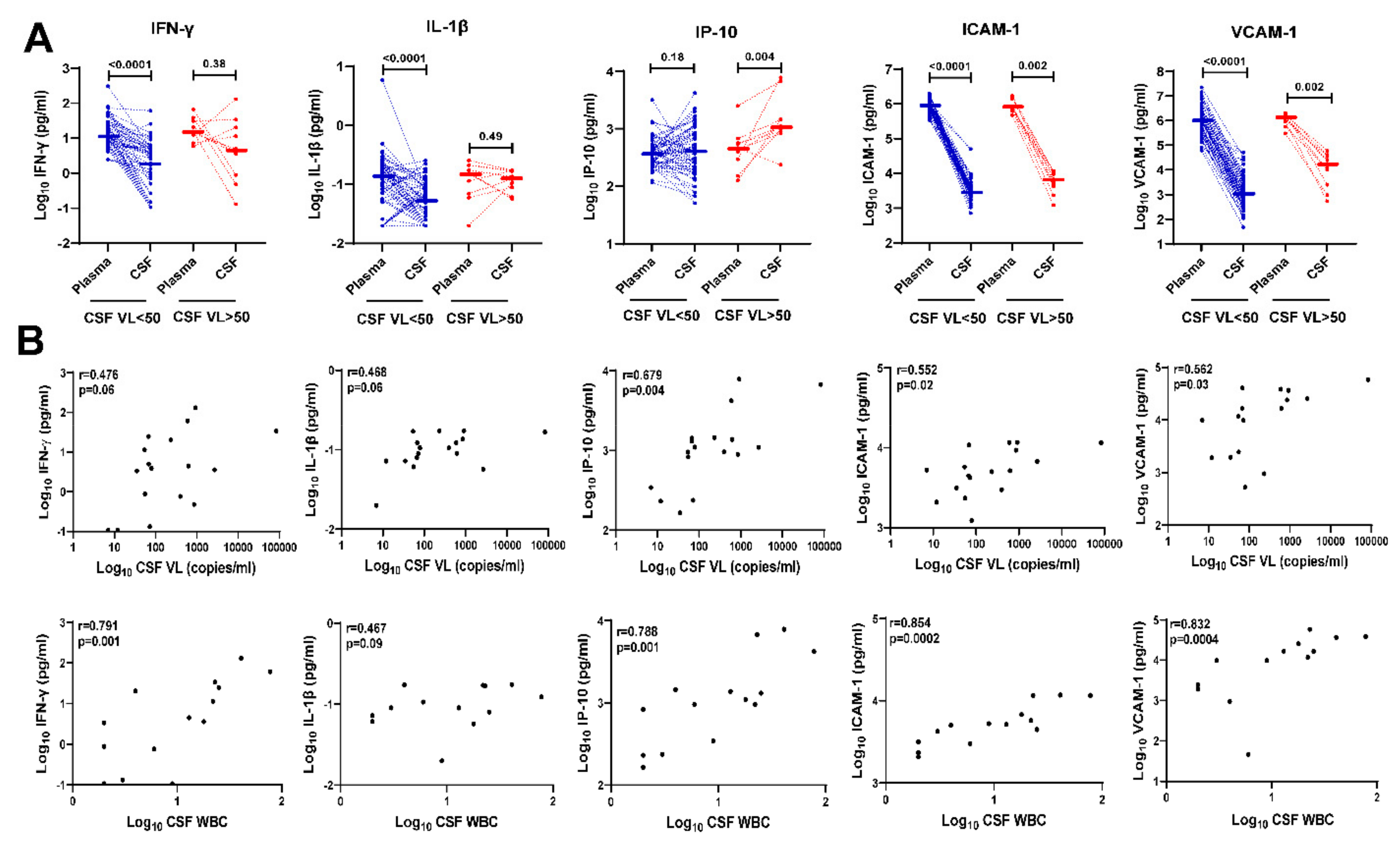
3.3. Inflammation Biomarkers in CSF of HIV+ Individuals on ART with Detectable CSF HIV RNA Correlate with CSF HIV RNA Levels and CSF WBC
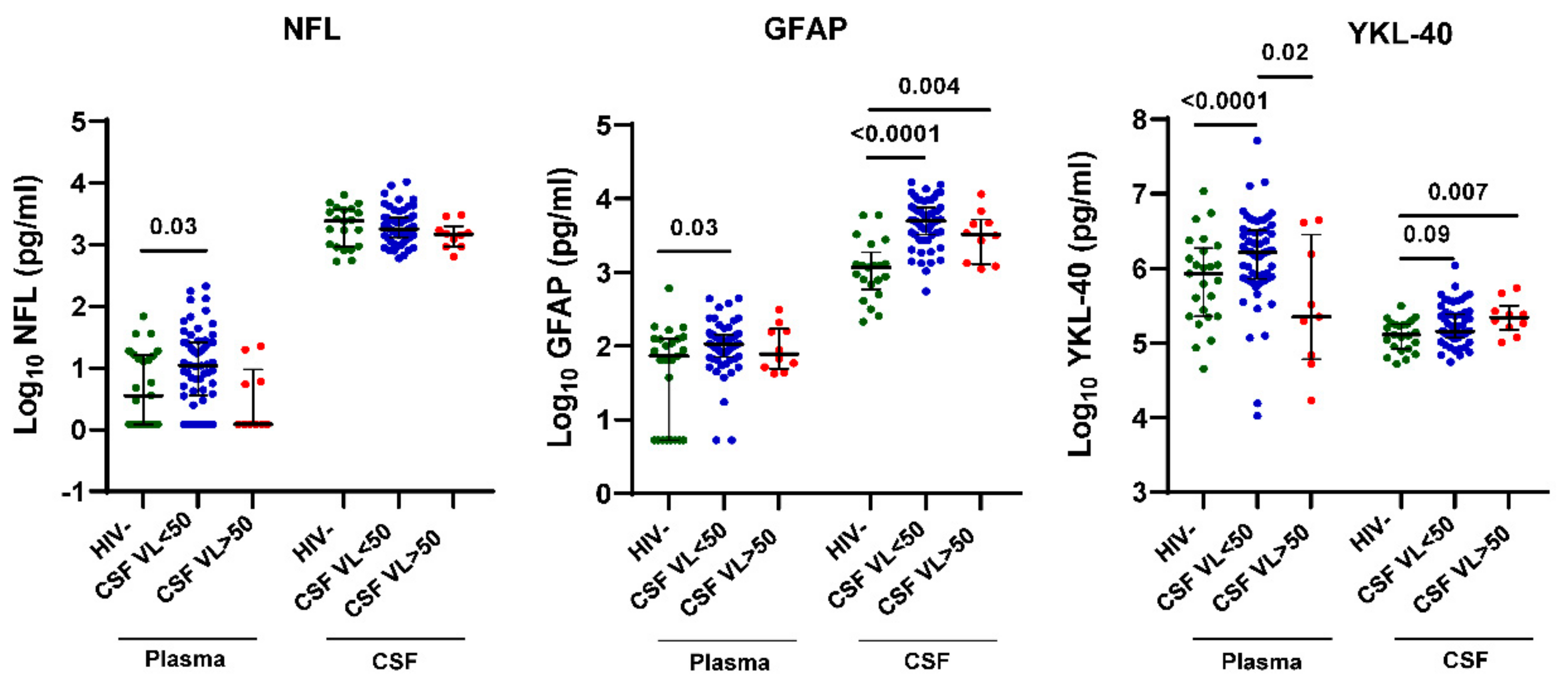
3.4. CSF VL > 50 Copies/mL Is Associated with Increased YKL-40 But Not NFL and GFAP in CSF of HIV+ Individuals on ART
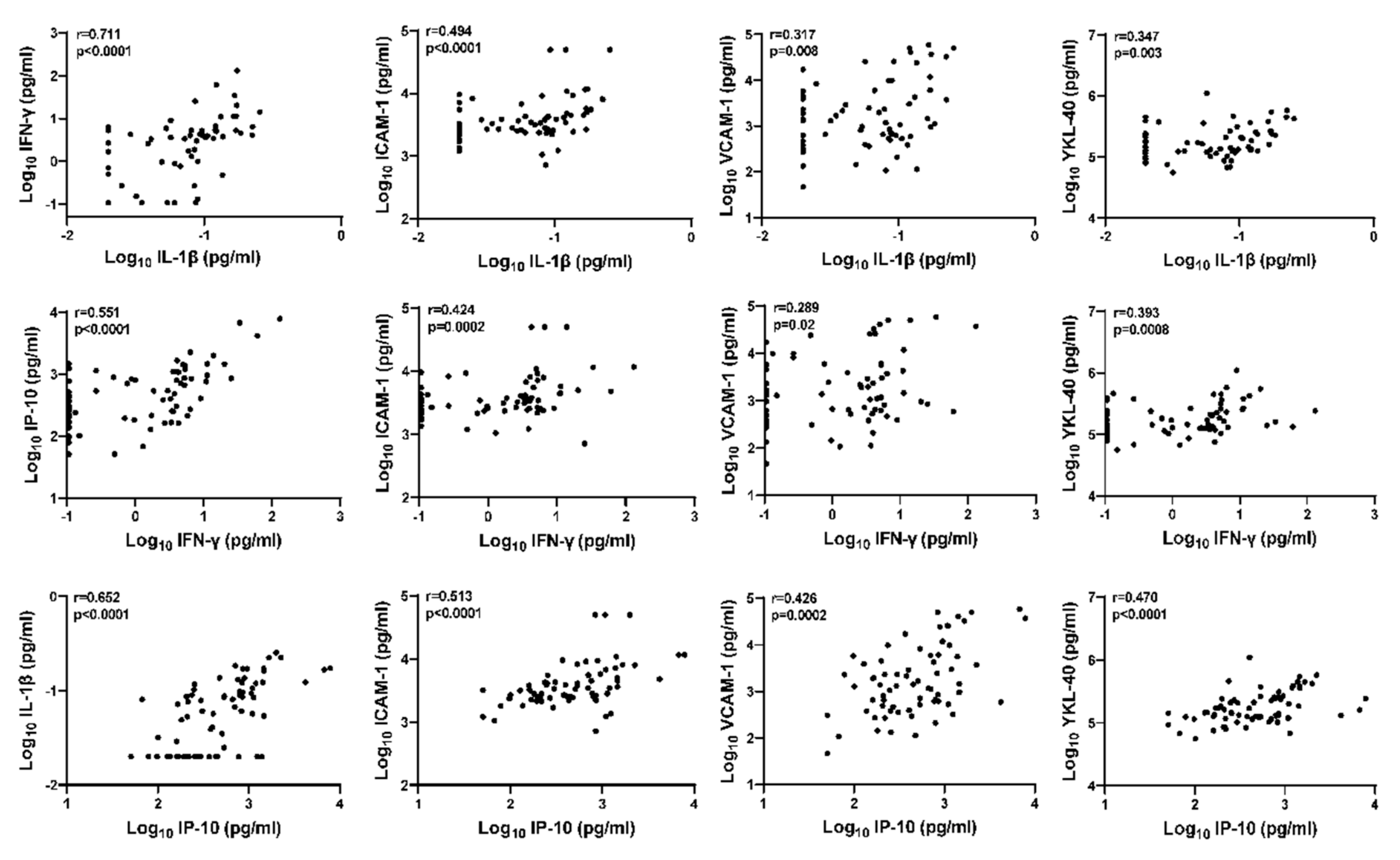
3.5. Inter-Relationship between CSF Inflammation Markers, Cell Adhesion Molecules, and Glial Activation Marker YKL-40 in HIV+ Individuals on ART
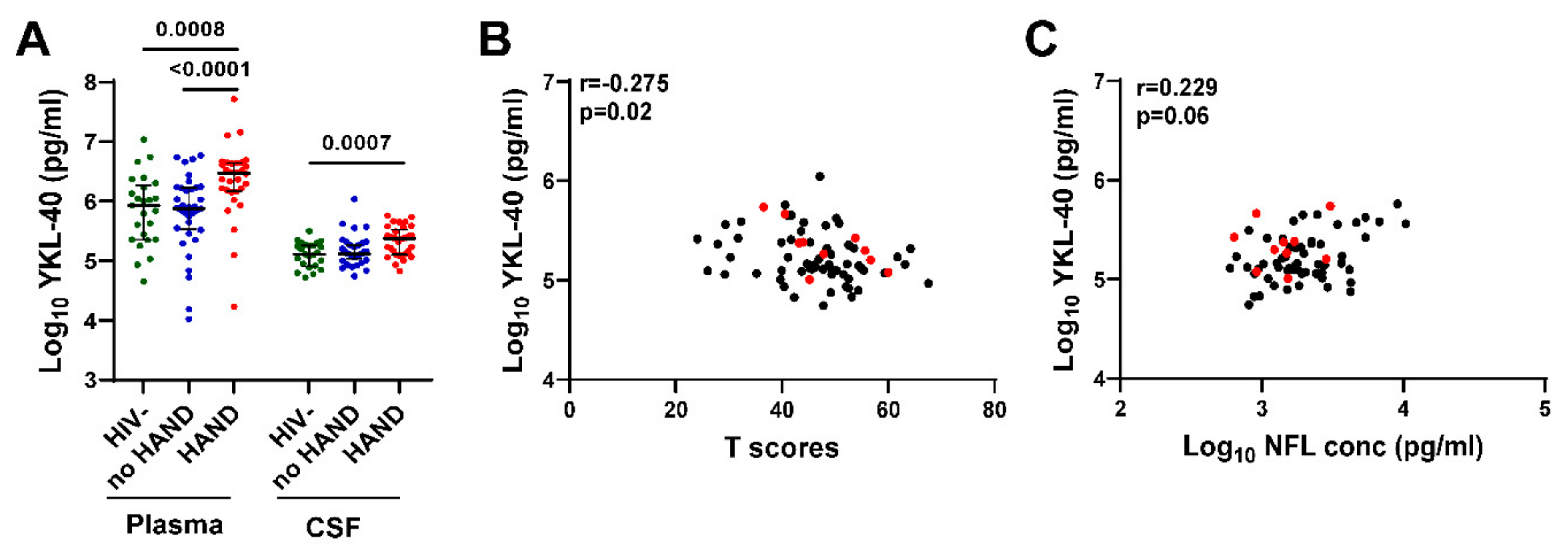
3.6. Plasma and CSF YKL-40 Levels Are Elevated in HIV+ Individuals on ART with HAND Compared with No HAND or HIV- Controls and Correlate with Lower Global Neurocognitive T Scores and Higher NFL Levels
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Brew, B.J.; Barnes, S.L. The impact of HIV central nervous system persistence on pathogenesis. AIDS 2019, 33 (Suppl. 2), S113–S121. [Google Scholar] [CrossRef] [PubMed]
- Spudich, S.; Peterson, J.; Fuchs, D.; Price, R.W.; Gisslen, M. Potential for early antiretroviral therapy to reduce central nervous system HIV-1 persistence. AIDS 2019, 33 (Suppl. 2), S135–S144. [Google Scholar] [CrossRef] [PubMed]
- Joseph, S.B.; Gianella, S.; Burdo, T.H.; Cinque, P.; Gisslen, M.; Letendre, S.; Nath, A.; Morgello, S.; Ndhlovu, L.C.; Spudich, S. Biotypes of Central Nervous System Complications in People with Human Immunodeficiency Virus: Virology, Immunology, and Neuropathology. J. Infect. Dis. 2023, 227, S3–S15. [Google Scholar] [CrossRef] [PubMed]
- Farhadian, S.F.; Lindenbaum, O.; Zhao, J.; Corley, M.J.; Im, Y.; Walsh, H.; Vecchio, A.; Garcia-Milian, R.; Chiarella, J.; Chintanaphol, M.; et al. HIV viral transcription and immune perturbations in the CNS of people with HIV despite ART. JCI Insight 2022, 7, e160267. [Google Scholar] [CrossRef] [PubMed]
- Lustig, G.; Cele, S.; Karim, F.; Derache, A.; Ngoepe, A.; Khan, K.; Gosnell, B.I.; Moosa, M.-Y.S.; Ntshuba, N.; Marais, S. T cell derived HIV-1 is present in the CSF in the face of suppressive antiretroviral therapy. PLoS Pathog. 2021, 17, e1009871. [Google Scholar] [CrossRef] [PubMed]
- Suzuki, K.; Zaunders, J.; Gates, T.M.; Levert, A.; Butterly, S.; Liu, Z.; Ishida, T.; Palmer, S.; Rae, C.D.; Juge, L.; et al. Elevation of cell-associated HIV-1 transcripts in CSF CD4+ T cells, despite effective antiretroviral therapy, is linked to brain injury. Proc. Natl. Acad. Sci. USA 2022, 119, e2210584119. [Google Scholar] [CrossRef] [PubMed]
- Saylor, D.; Dickens, A.M.; Sacktor, N.; Haughey, N.; Slusher, B.; Pletnikov, M.; Mankowski, J.L.; Brown, A.; Volsky, D.J.; McArthur, J.C. HIV-associated neurocognitive disorder—Pathogenesis and prospects for treatment. Nat. Rev. Neurol. 2016, 12, 234–248. [Google Scholar] [CrossRef]
- Winston, A.; Spudich, S. Cognitive disorders in people living with HIV. Lancet HIV 2020, 7, e504–e513. [Google Scholar] [CrossRef]
- Aung, H.L.; Alagaratnam, J.; Chan, P.; Chow, F.C.; Joska, J.; Falutz, J.; Letendre, S.L.; Lin, W.; Munoz-Moreno, J.A.; Cinque, P.; et al. Cognitive Health in Persons with Human Immunodeficiency Virus: The Impact of Early Treatment, Comorbidities, and Aging. J. Infect. Dis. 2023, 227, S38–S47. [Google Scholar] [CrossRef]
- Gabuzda, D.; Yin, J.; Misra, V.; Chettimada, S.; Gelman, B.B. Intact Proviral DNA Analysis of the Brain Viral Reservoir and Relationship to Neuroinflammation in People with HIV on Suppressive Antiretroviral Therapy. Viruses 2023, 15, 1009. [Google Scholar] [CrossRef]
- Kamat, A.; Lyons, J.L.; Misra, V.; Uno, H.; Morgello, S.; Singer, E.J.; Gabuzda, D. Monocyte activation markers in cerebrospinal fluid associated with impaired neurocognitive testing in advanced HIV infection. J. Acquir. Immune Defic. Syndr. 2012, 60, 234–243. [Google Scholar] [CrossRef] [PubMed]
- Dahl, V.; Peterson, J.; Fuchs, D.; Gisslen, M.; Palmer, S.; Price, R.W. Low levels of HIV-1 RNA detected in the cerebrospinal fluid after up to 10 years of suppressive therapy are associated with local immune activation. AIDS 2014, 28, 2251–2258. [Google Scholar] [CrossRef] [PubMed]
- Cinque, P.; Bestetti, A.; Marenzi, R.; Sala, S.; Gisslen, M.; Hagberg, L.; Price, R.W. Cerebrospinal fluid interferon-gamma-inducible protein 10 (IP-10, CXCL10) in HIV-1 infection. J. Neuroimmunol. 2005, 168, 154–163. [Google Scholar] [CrossRef] [PubMed]
- Perez-Valero, I.; Ellis, R.; Heaton, R.; Deutsch, R.; Franklin, D.; Clifford, D.B.; Collier, A.; Gelman, B.; Marra, C.; McCutchan, J.A.; et al. Cerebrospinal fluid viral escape in aviremic HIV-infected patients receiving antiretroviral therapy: Prevalence, risk factors and neurocognitive effects. AIDS 2019, 33, 475–481. [Google Scholar] [CrossRef] [PubMed]
- Williams, M.E.; Stein, D.J.; Joska, J.A.; Naude, P.J.W. Cerebrospinal fluid immune markers and HIV-associated neurocognitive impairments: A systematic review. J. Neuroimmunol. 2021, 358, 577649. [Google Scholar] [CrossRef] [PubMed]
- Anderson, A.M.; Kundu, S.; Tang, B.; Vaida, F.; Okwuegbuna, O.; McClernon, D.; Cherner, M.; Deutsch, R.; Cookson, D.; Crescini, M.; et al. Cerebrospinal fluid CXCL10 is associated with the presence of low level CSF HIV during suppressive antiretroviral therapy. J. Neuroimmunol. 2021, 353, 577493. [Google Scholar] [CrossRef] [PubMed]
- Bandera, A.; Taramasso, L.; Bozzi, G.; Muscatello, A.; Robinson, J.A.; Burdo, T.H.; Gori, A. HIV-Associated Neurocognitive Impairment in the Modern ART Era: Are We Close to Discovering Reliable Biomarkers in the Setting of Virological Suppression? Front. Aging Neurosci. 2019, 11, 187. [Google Scholar] [CrossRef]
- Gisslen, M.; Keating, S.M.; Spudich, S.; Arechiga, V.; Stephenson, S.; Zetterberg, H.; Di Germanio, C.; Blennow, K.; Fuchs, D.; Hagberg, L.; et al. Compartmentalization of cerebrospinal fluid inflammation across the spectrum of untreated HIV-1 infection, central nervous system injury and viral suppression. PLoS ONE 2021, 16, e0250987. [Google Scholar] [CrossRef]
- Hermansson, L.; Yilmaz, A.; Axelsson, M.; Blennow, K.; Fuchs, D.; Hagberg, L.; Lycke, J.; Zetterberg, H.; Gisslen, M. Cerebrospinal fluid levels of glial marker YKL-40 strongly associated with axonal injury in HIV infection. J. Neuroinflamm. 2019, 16, 16. [Google Scholar] [CrossRef]
- Cassol, E.; Misra, V.; Morgello, S.; Gabuzda, D. Applications and limitations of inflammatory biomarkers for studies on neurocognitive impairment in HIV infection. J. Neuroimmune Pharmacol. 2013, 8, 1087–1097. [Google Scholar] [CrossRef]
- Peluso, M.J.; Valcour, V.; Phanuphak, N.; Ananworanich, J.; Fletcher, J.L.; Chalermchai, T.; Krebs, S.J.; Robb, M.L.; Hellmuth, J.; Gisslen, M.; et al. Immediate initiation of cART is associated with lower levels of cerebrospinal fluid YKL-40, a marker of microglial activation, in HIV-1 infection. AIDS 2017, 31, 247–252. [Google Scholar] [CrossRef] [PubMed]
- Guha, D.; Lorenz, D.R.; Misra, V.; Chettimada, S.; Morgello, S.; Gabuzda, D. Proteomic analysis of cerebrospinal fluid extracellular vesicles reveals synaptic injury, inflammation, and stress response markers in HIV patients with cognitive impairment. J. Neuroinflamm. 2019, 16, 254. [Google Scholar] [CrossRef] [PubMed]
- Guha, D.; Mukerji, S.S.; Chettimada, S.; Misra, V.; Lorenz, D.R.; Morgello, S.; Gabuzda, D. Cerebrospinal fluid extracellular vesicles and neurofilament light protein as biomarkers of central nervous system injury in HIV-infected patients on antiretroviral therapy. AIDS 2019, 33, 615–625. [Google Scholar] [CrossRef] [PubMed]
- Gabuzda, D.; McArthur, J.C.; Letendre, S.L. Efficacy and safety of two-drug regimens for treatment of HIV in the central nervous system. AIDS 2020, 34, 1975–1977. [Google Scholar] [CrossRef] [PubMed]
- Mukerji, S.S.; Petersen, K.J.; Pohl, K.M.; Dastgheyb, R.M.; Fox, H.S.; Bilder, R.M.; Brouillette, M.J.; Gross, A.L.; Scott-Sheldon, L.A.J.; Paul, R.H.; et al. Machine Learning Approaches to Understand Cognitive Phenotypes in People with HIV. J. Infect. Dis. 2023, 227, S48–S57. [Google Scholar] [CrossRef]
- Anderson, A.M.; Munoz-Moreno, J.A.; McClernon, D.R.; Ellis, R.J.; Cookson, D.; Clifford, D.B.; Collier, A.C.; Gelman, B.B.; Marra, C.M.; McArthur, J.C.; et al. Prevalence and Correlates of Persistent HIV-1 RNA in Cerebrospinal Fluid during Antiretroviral Therapy. J. Infect. Dis. 2017, 215, 105–113. [Google Scholar] [CrossRef] [PubMed]
- Livelli, A.; Vaida, F.; Ellis, R.J.; Ma, Q.; Ferrara, M.; Clifford, D.B.; Collier, A.C.; Gelman, B.B.; Marra, C.M.; McArthur, J.C.; et al. Correlates of HIV RNA concentrations in cerebrospinal fluid during antiretroviral therapy: A longitudinal cohort study. Lancet HIV 2019, 6, e456–e462. [Google Scholar] [CrossRef] [PubMed]
- Anderson, A.M.; Tang, B.; Vaida, F.; McClernon, D.; Deutsch, R.; Cherner, M.; Cookson, D.; Crescini, M.; Grant, I.; Ellis, R.J.; et al. Low-Level HIV RNA in Cerebrospinal Fluid and Neurocognitive Performance: A Longitudinal Cohort Study. J. Acquir. Immune Defic. Syndr. 2021, 87, 1196–1204. [Google Scholar] [CrossRef]
- Eden, A.; Nilsson, S.; Hagberg, L.; Fuchs, D.; Zetterberg, H.; Svennerholm, B.; Gisslen, M. Asymptomatic Cerebrospinal Fluid HIV-1 Viral Blips and Viral Escape during Antiretroviral Therapy: A Longitudinal Study. J. Infect. Dis. 2016, 214, 1822–1825. [Google Scholar] [CrossRef]
- Joseph, J.; Cinque, P.; Colosi, D.; Dravid, A.; Ene, L.; Fox, H.; Gabuzda, D.; Gisslen, M.; Beth Joseph, S.; Letendre, S.; et al. Highlights of the Global HIV-1 CSF Escape Consortium Meeting, 9 June 2016, Bethesda, MD, USA. J. Virus Erad. 2016, 2, 243–250. [Google Scholar] [CrossRef]
- Mastrangelo, A.; Turrini, F.; de Zan, V.; Caccia, R.; Gerevini, S.; Cinque, P. Symptomatic cerebrospinal fluid escape. AIDS 2019, 33 (Suppl. 2), S159–S169. [Google Scholar] [CrossRef] [PubMed]
- Joseph, S.B.; Trunfio, M.; Kincer, L.P.; Calcagno, A.; Price, R.W. What can characterization of cerebrospinal fluid escape populations teach us about viral reservoirs in the central nervous system? AIDS 2019, 33 (Suppl. 2), S171–S179. [Google Scholar] [CrossRef] [PubMed]
- Winston, A.; Antinori, A.; Cinque, P.; Fox, H.S.; Gisslen, M.; Henrich, T.J.; Letendre, S.; Persaud, D.; Price, R.W.; Spudich, S. Defining cerebrospinal fluid HIV RNA escape: Editorial review AIDS. AIDS 2019, 33 (Suppl. 2), S107–S111. [Google Scholar] [CrossRef] [PubMed]
- Canestri, A.; Lescure, F.X.; Jaureguiberry, S.; Moulignier, A.; Amiel, C.; Marcelin, A.G.; Peytavin, G.; Tubiana, R.; Pialoux, G.; Katlama, C. Discordance between cerebral spinal fluid and plasma HIV replication in patients with neurological symptoms who are receiving suppressive antiretroviral therapy. Clin. Infect. Dis. 2010, 50, 773–778. [Google Scholar] [CrossRef] [PubMed]
- Mukerji, S.S.; Misra, V.; Lorenz, D.; Cervantes-Arslanian, A.M.; Lyons, J.; Chalkias, S.; Wurcel, A.; Burke, D.; Venna, N.; Morgello, S.; et al. Temporal Patterns and Drug Resistance in CSF Viral Escape Among ART-Experienced HIV-1 Infected Adults. J. Acquir. Immune Defic. Syndr. 2017, 75, 246–255. [Google Scholar] [CrossRef] [PubMed]
- Mukerji, S.S.; Misra, V.; Lorenz, D.R.; Uno, H.; Morgello, S.; Franklin, D.; Ellis, R.J.; Letendre, S.; Gabuzda, D. Impact of Antiretroviral Regimens on Cerebrospinal Fluid Viral Escape in a Prospective Multicohort Study of Antiretroviral Therapy-Experienced Human Immunodeficiency Virus-1-Infected Adults in the United States. Clin. Infect. Dis. 2018, 67, 1182–1190. [Google Scholar] [CrossRef] [PubMed]
- Nightingale, S.; Michael, B.D.; Fisher, M.; Winston, A.; Nelson, M.; Taylor, S.; Ustianowski, A.; Ainsworth, J.; Gilson, R.; Haddow, L.; et al. CSF/plasma HIV-1 RNA discordance even at low levels is associated with up-regulation of host inflammatory mediators in CSF. Cytokine 2016, 83, 139–146. [Google Scholar] [CrossRef]
- Peluso, M.J.; Ferretti, F.; Peterson, J.; Lee, E.; Fuchs, D.; Boschini, A.; Gisslen, M.; Angoff, N.; Price, R.W.; Cinque, P.; et al. Cerebrospinal fluid HIV escape associated with progressive neurologic dysfunction in patients on antiretroviral therapy with well controlled plasma viral load. AIDS 2012, 26, 1765–1774. [Google Scholar] [CrossRef]
- Eden, A.; Fuchs, D.; Hagberg, L.; Nilsson, S.; Spudich, S.; Svennerholm, B.; Price, R.W.; Gisslen, M. HIV-1 viral escape in cerebrospinal fluid of subjects on suppressive antiretroviral treatment. J. Infect. Dis. 2010, 202, 1819–1825. [Google Scholar] [CrossRef]
- Chan, T.Y.; De Zan, V.; Gregg, A.; Alagaratnam, J.; Gerevini, S.; Antinori, A.; D’Arminio Monforte, A.; Saracino, A.; Trunfio, M.; Everitt, A.; et al. The symptomatology of cerebrospinal fluid HIV RNA escape: A large case-series. AIDS 2021, 35, 2341–2346. [Google Scholar] [CrossRef]
- Filippidis, P.; Damas, J.; Viala, B.; Assal, F.; Nawej Tshikung, O.; Tarr, P.; Derfuss, T.; Oberholzer, M.; Jelcic, I.; Hundsberger, T.; et al. Cerebrospinal Fluid HIV-1 Escape in Patients with Neurocognitive Symptoms: Pooled Data from a Neuro-HIV Platform and the NAMACO Study. J. Acquir. Immune Defic. Syndr. 2023, 93, 219–228. [Google Scholar] [CrossRef] [PubMed]
- De Almeida, S.M.; Rotta, I.; de Pereira, A.P.; Tang, B.; Umlauf, A.; Ribeiro, C.E.L.; Letendre, S.; Ellis, R.J.; The HIV Neurobehavioral Research Center (HNRC) Group. Cerebrospinal fluid pleocytosis as a predictive factor for CSF and plasma HIV RNA discordance and escape. J. Neurovirol. 2020, 26, 241–251. [Google Scholar] [CrossRef] [PubMed]
- Narvid, J.; Callen, A.; Talbott, J.; Uzelac, A.; Dupont, S.M.; Chow, F.; Price, R.W.; Rehani, B. Brain MRI Features of CSF Human Immunodeficiency Virus Escape. J. Neuroimaging 2018, 28, 601–607. [Google Scholar] [CrossRef] [PubMed]
- Morgello, S.; Gelman, B.; Kozlowski, P.; Vinters, H.; Masliah, E.; Cornford, M.; Cavert, W.; Marra, C.; Grant, I.; Singer, E. The National NeuroAIDS Tissue Consortium: A new paradigm in brain banking with an emphasis on infectious disease. Neuropathol. Appl. Neurobiol. 2001, 27, 326–335. [Google Scholar] [CrossRef] [PubMed]
- Heaton, R.K.; Clifford, D.B.; Franklin, D.R., Jr.; Woods, S.P.; Ake, C.; Vaida, F.; Ellis, R.J.; Letendre, S.L.; Marcotte, T.D.; Atkinson, J.H.; et al. HIV-associated neurocognitive disorders persist in the era of potent antiretroviral therapy: CHARTER Study. Neurology 2010, 75, 2087–2096. [Google Scholar] [CrossRef] [PubMed]
- Woods, S.P.; Rippeth, J.D.; Frol, A.B.; Levy, J.K.; Ryan, E.; Soukup, V.M.; Hinkin, C.H.; Lazzaretto, D.; Cherner, M.; Marcotte, T.D.; et al. Interrater reliability of clinical ratings and neurocognitive diagnoses in HIV. J. Clin. Exp. Neuropsychol. 2004, 26, 759–778. [Google Scholar] [CrossRef] [PubMed]
- Antinori, A.; Arendt, G.; Becker, J.T.; Brew, B.J.; Byrd, D.A.; Cherner, M.; Clifford, D.B.; Cinque, P.; Epstein, L.G.; Goodkin, K.; et al. Updated research nosology for HIV-associated neurocognitive disorders. Neurology 2007, 69, 1789–1799. [Google Scholar] [CrossRef]
- Guha, D.; Misra, V.; Yin, J.; Horiguchi, M.; Uno, H.; Gabuzda, D. Vascular injury markers associated with cognitive impairment in people with HIV on suppressive antiretroviral therapy. AIDS 2023. [Google Scholar] [CrossRef]
- Schrier, R.D.; Hong, S.; Crescini, M.; Ellis, R.; Perez-Santiago, J.; Spina, C.; Letendre, S.; Group, H. Cerebrospinal fluid (CSF) CD8+ T-cells that express interferon-gamma contribute to HIV associated neurocognitive disorders (HAND). PLoS ONE 2015, 10, e0116526. [Google Scholar] [CrossRef]
- Spudich, S.; Robertson, K.R.; Bosch, R.J.; Gandhi, R.T.; Cyktor, J.C.; Mar, H.; Macatangay, B.J.; Lalama, C.M.; Rinaldo, C.; Collier, A.C.; et al. Persistent HIV-infected cells in cerebrospinal fluid are associated with poorer neurocognitive performance. J. Clin. Investig. 2019, 129, 3339–3346. [Google Scholar] [CrossRef]
- Bissel, S.J.; Kofler, J.; Nyaundi, J.; Murphey-Corb, M.; Wisniewski, S.R.; Wiley, C.A. Cerebrospinal Fluid Biomarkers of Simian Immunodeficiency Virus Encephalitis: CSF Biomarkers of SIV Encephalitis. J. Neuroimmune Pharmacol. 2016, 11, 332–347. [Google Scholar] [CrossRef]
- Bonneh-Barkay, D.; Bissel, S.J.; Wang, G.; Fish, K.N.; Nicholl, G.C.; Darko, S.W.; Medina-Flores, R.; Murphey-Corb, M.; Rajakumar, P.A.; Nyaundi, J.; et al. YKL-40, a marker of simian immunodeficiency virus encephalitis, modulates the biological activity of basic fibroblast growth factor. Am. J. Pathol. 2008, 173, 130–143. [Google Scholar] [CrossRef]
- Olsson, B.; Lautner, R.; Andreasson, U.; Ohrfelt, A.; Portelius, E.; Bjerke, M.; Holtta, M.; Rosen, C.; Olsson, C.; Strobel, G.; et al. CSF and blood biomarkers for the diagnosis of Alzheimer’s disease: A systematic review and meta-analysis. Lancet Neurol. 2016, 15, 673–684. [Google Scholar] [CrossRef]
- Deng, Y.; Li, G.; Chang, D.; Su, X. YKL-40 as a novel biomarker in cardio-metabolic disorders and inflammatory diseases. Clin. Chim. Acta 2020, 511, 40–46. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| HIV- Controls (n = 50) | HIV+ CSF VL < 50 Copies/mL (n = 60) | HIV+ CSF VL > 50 Copies/mL (n = 10) | p-Value | |
|---|---|---|---|---|
| Age (years) | 54 (50–60) | 50 (46–55) | 49 (44–61) | 0.90 |
| Male gender (n, %) | 39 (78) | 54 (90) | 6 (60) | 0.03 |
| Race (n, %) | 0.49 | |||
| Black | 12 (24) | 20 (33) | 2 (20) | |
| White | 37 (74) | 37 (62) | 8 (80) | |
| Other | 1 (2) | 3 (5) | 0 (0) | |
| Duration of HIV infection (years) | 16 (11–22) | 14 (8–23) | 0.66 | |
| Plasma viral load > 50 copies/mL (n, %) | 0 (0) | 4 (40) | <0.0001 | |
| CD4 count (cells/μL) | 512 (354–756) | 318 (200–532) | 0.045 | |
| Nadir CD4 count (cells/μL) | 65 (13–192) | 80 (14–147) | 0.82 | |
| Hepatitis C seropositivity (n, %) | 20 (33) | 3 (30) | 0.84 | |
| ART use (n, %) | 0.38 | |||
| Protease inhibitors (n, %) | 34 (57) | 5 (50) | ||
| Integrase inhibitors (n, %) | 11 (18) | 1 (10) | ||
| NNRTI (n, %) | 25 (42) | 3 (30) | ||
| Duration of ART (years) | 10 (7–13) | 8 (7–11) | 0.27 | |
| HAND diagnosis (n, %) Ϯ | 28 (47) | 5 (50) | 0.85 | |
| CPE score | 8 (7–9) | 8 (7–8) | 0.35 | |
| CSF viral load (copies/mL) | 40 (40–40) | 156 (65–1364) | <0.0001 | |
| CSF white blood cells (cells/μL) | 2 (0–4) | 4 (0–22) | 0.15 | |
| CSF protein (mg/dL) | 37 (32–46) | 29 (23–56) | 0.47 | |
| CSF/plasma albumin ratio | 4 (2–19) | 6 (2–23) | 0.91 | |
| BDI score | 7 (1–18) | 6 (3–10) | 0.46 | |
| Global neurocognitive T score | 47 (41–52) | 47 (43–56) | 0.57 | |
| Global clinical rating | 4 (3–5) | 4 (2–4) | 0.40 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Guha, D.; Misra, V.; Yin, J.; Gabuzda, D. CSF Inflammation Markers Associated with Asymptomatic Viral Escape in Cerebrospinal Fluid of HIV-Positive Individuals on Antiretroviral Therapy. Viruses 2023, 15, 1829. https://doi.org/10.3390/v15091829
Guha D, Misra V, Yin J, Gabuzda D. CSF Inflammation Markers Associated with Asymptomatic Viral Escape in Cerebrospinal Fluid of HIV-Positive Individuals on Antiretroviral Therapy. Viruses. 2023; 15(9):1829. https://doi.org/10.3390/v15091829
Chicago/Turabian StyleGuha, Debjani, Vikas Misra, Jun Yin, and Dana Gabuzda. 2023. "CSF Inflammation Markers Associated with Asymptomatic Viral Escape in Cerebrospinal Fluid of HIV-Positive Individuals on Antiretroviral Therapy" Viruses 15, no. 9: 1829. https://doi.org/10.3390/v15091829