
An Extensive Examination of the Warning Signs, Symptoms, Diagnosis, Available Therapies, and Prognosis for Lumpy Skin Disease
 , , , , and
, , , , and
Abstract
:1. Introduction
2. Clinical Signs and Symptoms
3. Diagnosis and Outbreaks of LSD
Differential Diagnosis
4. Control Measures
4.1. Control of Cattle Movement
4.2. Vector Management
4.3. Vaccination
4.4. Awareness
5. Conclusions and Future Perspectives
Author Contributions
Funding
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Woods, J.A. Lumpy Skin Disease-A Review. Trop. Anim. Health Prod. 1988, 20, 11–17. [Google Scholar] [CrossRef]
- Tuppurainen, E.S.M.; Oura, C.A.L. Review: Lumpy Skin Disease: An Emerging Threat to Europe, the Middle East and Asia. Transbound. Emerg. Dis. 2012, 59, 40–48. [Google Scholar] [CrossRef]
- Yeruham, I.; Nir, O.; Braverman, Y.; Davidson, M.; Grinstein, H.; Haymovitch, M.; Zamir, O. Spread of lumpy skin disease in Israeli dairy herds. Vet. Rec. 1995, 137, 91–93. [Google Scholar] [CrossRef]
- Sudhakar, S.B.; Mishra, N.; Kalaiyarasu, S.; Jhade, S.K.; Hemadri, D.; Sood, R.; Bal, G.C.; Nayak, M.K.; Pradhan, S.K.; Singh, V.P. Lumpy skin disease (LSD) outbreaks in cattle in Odisha state, India in August 2019: Epidemiological features and molecular studies. Transbound. Emerg. Dis. 2020, 67, 2408–2422. [Google Scholar] [CrossRef]
- Fauquet, C.M.; Mayo, M.A.; Maniloff, J.; Desselberger, U.; Ball, L.A. Virus Taxonomy: Eighth Report of the International Committee on Taxonomy of Viruses; Elsevier Academic Press: Amsterdam, The Netherlands, 2005; ISBN 978-0-12-249951-7. [Google Scholar]
- Carn, V.M.; Kitching, R.P. An investigation of possible routes of transmission of lumpy skin disease virus (Neethling). Epidemiol. Infect. 1995, 114, 219–226. [Google Scholar] [CrossRef] [Green Version]
- Gari, G.; Waret-Szkuta, A.; Grosbois, V.; Jacquiet, P.; Roger, F. Risk factors associated with observed clinical lumpy skin disease in Ethiopia. Epidemiol. Infect. 2010, 138, 1657–1666. [Google Scholar] [CrossRef] [Green Version]
- Sprygin, A.; Pestova, Y.; Wallace, D.; Tuppurainen, E.; Kononov, A. Transmission of lumpy skin disease virus: A short review. Virus Res. 2019, 269, 197637. [Google Scholar] [CrossRef]
- Shimshony, A.; Economides, P. Disease prevention and preparedness for animal health emergencies in the Middle East. Rev. Sci. Tech. Int. Off. Epizoot. 2006, 25, 253–269. [Google Scholar] [CrossRef] [Green Version]
- Kumar, N.; Tripathi, B.N. A serious skin virus epidemic sweeping through the Indian subcontinent is a threat to the livelihood of farmers. Virulence 2022, 13, 1943–1944. [Google Scholar] [CrossRef]
- Rinchen, S. Descriptive epidemiology of the first lumpy skin disease outbreak in Bhutan. Bhutan J. Anim. Sci. 2022, 6, 46–51. [Google Scholar]
- Acharya, K.P.; Subedi, D. First outbreak of lumpy skin disease in Nepal. Transbound. Emerg. Dis. 2020, 67, 2280–2281. [Google Scholar] [CrossRef]
- Kayesh, M.E.H.; Hussan, M.T.; Hashem, A.; Eliyas, M.; Anower, A.M. Lumpy Skin Disease Virus Infection: An Emerging Threat to Cattle Health in Bangladesh. Hosts Viruses 2020, 7, 97. [Google Scholar] [CrossRef]
- Babiuk, S.; Bowden, T.R.; Parkyn, G.; Dalman, B.; Hoa, D.M.; Long, N.T.; Vu, P.P.; Bieu, D.X.; Copps, J.; Boyle, D.B. Yemen and Vietnam capripoxviruses demonstrate a distinct host preference for goats compared with sheep. J. Gen. Virol. 2009, 90, 105–114. [Google Scholar] [CrossRef]
- Lu, G.; Xie, J.; Luo, J.; Shao, R.; Jia, K.; Li, S. Lumpy skin disease outbreaks in China, since 3 August 2019. Transbound. Emerg. Dis. 2021, 68, 216–219. [Google Scholar] [CrossRef]
- Tsai, K.-J.; Tu, Y.-C.; Wu, C.-H.; Huang, C.-W.; Ting, L.-J.; Huang, Y.-L.; Pan, C.-H.; Chang, C.-Y.; Deng, M.-C.; Lee, F. First detection and phylogenetic analysis of lumpy skin disease virus from Kinmen Island, Taiwan in 2020. J. Vet. Med. Sci. 2022, 84, 1093–1100. [Google Scholar] [CrossRef]
- Abutarbush, S.M.; Ababneh, M.M.; Al Zoubi, I.G.; Al Sheyab, O.M.; Al Zoubi, M.G.; Alekish, M.O.; Al Gharabat, R.J. Lumpy Skin Disease in Jordan: Disease Emergence, Clinical Signs, Complications and Preliminary-associated Economic Losses. Transbound. Emerg. Dis. 2015, 62, 549–554. [Google Scholar] [CrossRef]
- Babiuk, S.; Bowden, T.R.; Boyle, D.B.; Wallace, D.B.; Kitching, R.P. Capripoxviruses: An Emerging Worldwide Threat to Sheep, Goats and Cattle. Transbound. Emerg. Dis. 2008, 55, 263–272. [Google Scholar] [CrossRef] [Green Version]
- Constable, P.D.; Hinchcliff, K.W.; Done, S.H.; Grünberg, W.; Colwell, D.D.; Connelly, S.; Dirikolu, L.; Gasser, R.; Hovda, L.; Ikede, B.; et al. Dedication, 11th ed.; Constable, P.D., Hinchcliff, K.W., Done, S.H., Grünberg, W.B.T.-V.M.E., Eds.; W.B. Saunders: Philadelphia, PA, USA, 2017; pp. x–xi. ISBN 978-0-7020-5246-0. [Google Scholar]
- Babiuk, S.; Bowden, T.R.; Parkyn, G.; Dalman, B.; Manning, L.; Neufeld, J.; Embury-Hyatt, C.; Copps, J.; Boyle, D.B. Quantification of Lumpy Skin Disease Virus Following Experimental Infection in Cattle. Transbound. Emerg. Dis. 2008, 55, 299–307. [Google Scholar] [CrossRef]
- Wolff, J.; Krstevski, K.; Beer, M.; Hoffmann, B. Minimum Infective Dose of a Lumpy Skin Disease Virus Field Strain from North Macedonia. Viruses 2020, 12, 768. [Google Scholar] [CrossRef]
- Carn, V.M.; Kitching, R.P. The clinical response of cattle experimentally infected with lumpy skin disease (Neethling) virus. Arch. Virol. 1995, 140, 503–513. [Google Scholar] [CrossRef]
- Beard, P.M. Lumpy skin disease: A direct threat to Europe. Vet. Rec. 2016, 178, 557–558. [Google Scholar] [CrossRef] [Green Version]
- Al-Salihi, K. Lumpy Skin Disease: Review of Literature. Mirror Res. Vet. Sci. Anim. 2014, 3, 6–23. [Google Scholar]
- Tageldin, M.H.; Wallace, D.B.; Gerdes, G.H.; Putterill, J.F.; Greyling, R.R.; Phosiwa, M.N.; Al Busaidy, R.M.; Al Ismaaily, S.I. Lumpy skin disease of cattle: An emerging problem in the Sultanate of Oman. Trop. Anim. Health Prod. 2014, 46, 241–246. [Google Scholar] [CrossRef] [Green Version]
- Kawther, S.Z. Observations on Lumpy Skin Disease in Local Egyptian Cows with Emphasis on Its Impact on Ovarian Function. Afr. J. Microbiol. Res. 2008, 2, 252–257. [Google Scholar]
- Alemayehu, G.; Zewde, G.; Admassu, B. Risk assessments of lumpy skin diseases in Borena bull market chain and its implication for livelihoods and international trade. Trop. Anim. Health Prod. 2013, 45, 1153–1159. [Google Scholar] [CrossRef] [Green Version]
- El-Ansary, R.E.; El-Dabae, W.H.; Bream, A.S.; El Wakil, A. Isolation and molecular characterization of lumpy skin disease virus from hard ticks, Rhipicephalus (Boophilus) annulatus in Egypt. BMC Vet. Res. 2022, 18, 302. [Google Scholar] [CrossRef]
- Greiner, M.; Gardner, I. Application of diagnostic tests in veterinary epidemiologic studies. Prev. Vet. Med. 2000, 45, 43–59. [Google Scholar] [CrossRef]
- Current situation of Lumpy Skin Disease Virus in some areas in El-Wady El-Gedid Governorate During 2020. Egypt. J. Anim. Health 2021, 1, 9–20. [CrossRef]
- Otranto, D.; Paradies, P.; Sasanelli, M.; Spinelli, R.; Brandonisio, O. Rapid Immunochromatographic Test for Serodiagnosis of Canine Leishmaniasis. J. Clin. Microbiol. 2004, 42, 2769–2770. [Google Scholar] [CrossRef] [Green Version]
- Chala, G. Epidemiology and diagnostic methods of lumpy skin disease: A Short Review. Int. J. Vet. Sci. Res. 2022, 8, 64–70. [Google Scholar] [CrossRef]
- Belák, S. Molecular diagnosis of viral diseases, present trends and future aspects: A view from the OIE Collaborating Centre for the Application of Polymerase Chain Reaction Methods for Diagnosis of Viral Diseases in Veterinary Medicine. Vaccine 2007, 25, 5444–5452. [Google Scholar] [CrossRef]
- Tuppurainen, E.S.; Venter, E.H.; Coetzer, J.A. The detection of lumpy skin disease virus in samples of experimentally infected cattle using different diagnostic techniques. Onderstepoort J. Veter. Res. 2005, 72, 153–164. [Google Scholar] [CrossRef] [Green Version]
- Balinsky, C.A.; Delhon, G.; Smoliga, G.; Prarat, M.; French, R.A.; Geary, S.J.; Rock, D.L.; Rodriguez, L.L. Rapid Preclinical Detection of Sheeppox Virus by a Real-Time PCR Assay. J. Clin. Microbiol. 2008, 46, 438–442. [Google Scholar] [CrossRef] [Green Version]
- Zeynalova, S.; Asadov, K.; Guliyev, F.; Vatani, M.; Aliyev, V. Epizootology and Molecular Diagnosis of Lumpy Skin Disease among Livestock in Azerbaijan. Front. Microbiol. 2016, 7, 1022. [Google Scholar] [CrossRef] [Green Version]
- Kasem, S.; Saleh, M.; Qasim, I.; Hashim, O.; Alkarar, A.; Abu-Obeida, A.; Gaafer, A.; Hussien, R.; Al-Sahaf, A.; Al-Doweriej, A.; et al. Outbreak investigation and molecular diagnosis of Lumpy skin disease among livestock in Saudi Arabia 2016. Transbound. Emerg. Dis. 2017, 65, e494–e500. [Google Scholar] [CrossRef]
- Ochwo, S.; VanderWaal, K.; Ndekezi, C.; Nkamwesiga, J.; Munsey, A.; Witto, S.G.; Nantima, N.; Mayanja, F.; Okurut, A.R.A.; Atuhaire, D.K.; et al. Molecular detection and phylogenetic analysis of lumpy skin disease virus from outbreaks in Uganda 2017–2018. BMC Vet. Res. 2020, 16, 66. [Google Scholar] [CrossRef] [Green Version]
- Azeem, S.; Sharma, B.; Shabir, S.; Akbar, H.; Venter, E. Lumpy skin disease is expanding its geographic range: A challenge for Asian livestock management and food security. Vet. J. 2022, 279, 105785. [Google Scholar] [CrossRef]
- Kumar, N.; Chander, Y.; Kumar, R.; Khandelwal, N.; Riyesh, T.; Chaudhary, K.; Shanmugasundaram, K.; Kumar, S.; Kumar, A.; Gupta, M.K.; et al. Isolation and characterization of lumpy skin disease virus from cattle in India. PLoS ONE 2021, 16, e0241022. [Google Scholar] [CrossRef]
- Kumar, N.; Barua, S.; Kumar, R.; Khandelwal, N.; Kumar, A.; Verma, A.; Singh, L.; Godara, B.; Chander, Y.; Riyesh, T.; et al. Evaluation of the safety, immunogenicity and efficacy of a new live-attenuated lumpy skin disease vaccine in India. bioRxiv 2022, 2022, 2022-12. [Google Scholar] [CrossRef]
- Salib, F.A.; Osman, A.H. Incidence of Lumpy Skin Disease among Egyptian Cattle in Giza Governorate, Egypt. Vet. World 2011, 4, 162–167. [Google Scholar]
- Evik, M.; Doğan, M. Epidemiological and Molecular Studies on Lumpy Skin Disease Outbreaks in Turkey during 2014–2015. Transbound. Emerg. Dis. 2017, 64, 1268–1279. [Google Scholar]
- Norian, R.; Ahangran, N.A.; Varshovi, H.R.; Azadmehr, A. Comparative efficacy of two heterologous capripox vaccines to control lumpy skin disease in cattle. Bulg. J. Vet. Med. 2019, 22, 171–179. [Google Scholar] [CrossRef]
- Amin, D.M.; Shehab, G.; Emran, R.; Hassanien, R.T.; Alagmy, G.N.; Hagag, N.M.; Abd-El-Moniem, M.I.I.; Habashi, A.R.; Ibraheem, E.M.; Shahein, M.A. Diagnosis of naturally occurring lumpy skin disease virus infection in cattle using virological, molecular, and immunohistopathological assays. Vet. World 2021, 14, 2230–2237. [Google Scholar] [CrossRef]
- Gari, G.; Bonnet, P.; Roger, F.; Waret-Szkuta, A. Epidemiological aspects and financial impact of lumpy skin disease in Ethiopia. Prev. Vet. Med. 2011, 102, 274–283. [Google Scholar] [CrossRef]
- Tuppurainen, E.S.M.; Antoniou, S.E.; Tsiamadis, E.; Topkaridou, M.; Labus, T.; Debeljak, Z.; Plavšić, B.; Miteva, A.; Alexandrov, T.; Pite, L. Field Observations and Experiences Gained from the Implementation of Control Measures against Lumpy Skin Disease in South-East Europe between 2015 and 2017. Prev. Vet. Med. 2020, 181, 104600. [Google Scholar] [CrossRef]
- Bedeković, T.; Šimić, I.; Krešić, N.; Lojkić, I. Detection of lumpy skin disease virus in skin lesions, blood, nasal swabs and milk following preventive vaccination. Transbound. Emerg. Dis. 2017, 65, 491–496. [Google Scholar] [CrossRef]
- Zewdiem, G.; Deresem, G.; Getachew, B.; Belay, H.; Akalu, M. Review of sheep and goat pox disease: Current updates on ep-idemiology, diagnosis, prevention and control measures in Ethiopia. Anim. Dis. 2021, 1, 28. [Google Scholar] [CrossRef]
- Gari, G.; Abie, G.; Gizaw, D.; Wubete, A.; Kidane, M.; Asgedom, H.; Bayissa, B.; Ayelet, G.; Oura, C.A.; Roger, F.; et al. Evaluation of the safety, immunogenicity and efficacy of three capripoxvirus vaccine strains against lumpy skin disease virus. Vaccine 2015, 33, 3256–3261. [Google Scholar] [CrossRef]
- Hunter, P.; Wallace, D. Lumpy skin disease in southern Africa: A review of the disease and aspects of control. J. S. Afr. Vet. Assoc. 2001, 72, 68–71. [Google Scholar] [CrossRef] [Green Version]
- Ayelet, G.; Abate, Y.; Sisay, T.; Nigussie, H.; Gelaye, E.; Jemberie, S.; Asmare, K. Lumpy skin disease: Preliminary vaccine efficacy assessment and overview on outbreak impact in dairy cattle at Debre Zeit, central Ethiopia. Antivir. Res. 2013, 98, 261–265. [Google Scholar] [CrossRef]
- Hamdi, J.; Boumart, Z.; Daouam, S.; El Arkam, A.; Bamouh, Z.; Jazouli, M.; Tadlaoui, K.O.; Fihri, O.F.; Gavrilov, B.; El Harrak, M. Development and Evaluation of an Inactivated Lumpy Skin Disease Vaccine for Cattle. Vet. Microbiol. 2020, 245, 108689. [Google Scholar] [CrossRef]
- Tuppurainen, E.; Venter, E.; Coetzer, J.; Bell-Sakyi, L. Lumpy skin disease: Attempted propagation in tick cell lines and presence of viral DNA in field ticks collected from naturally-infected cattle. Ticks Tick-Borne Dis. 2015, 6, 134–140. [Google Scholar] [CrossRef] [Green Version]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| S. No. | Country/Region | Date of Outbreak | References |
|---|---|---|---|
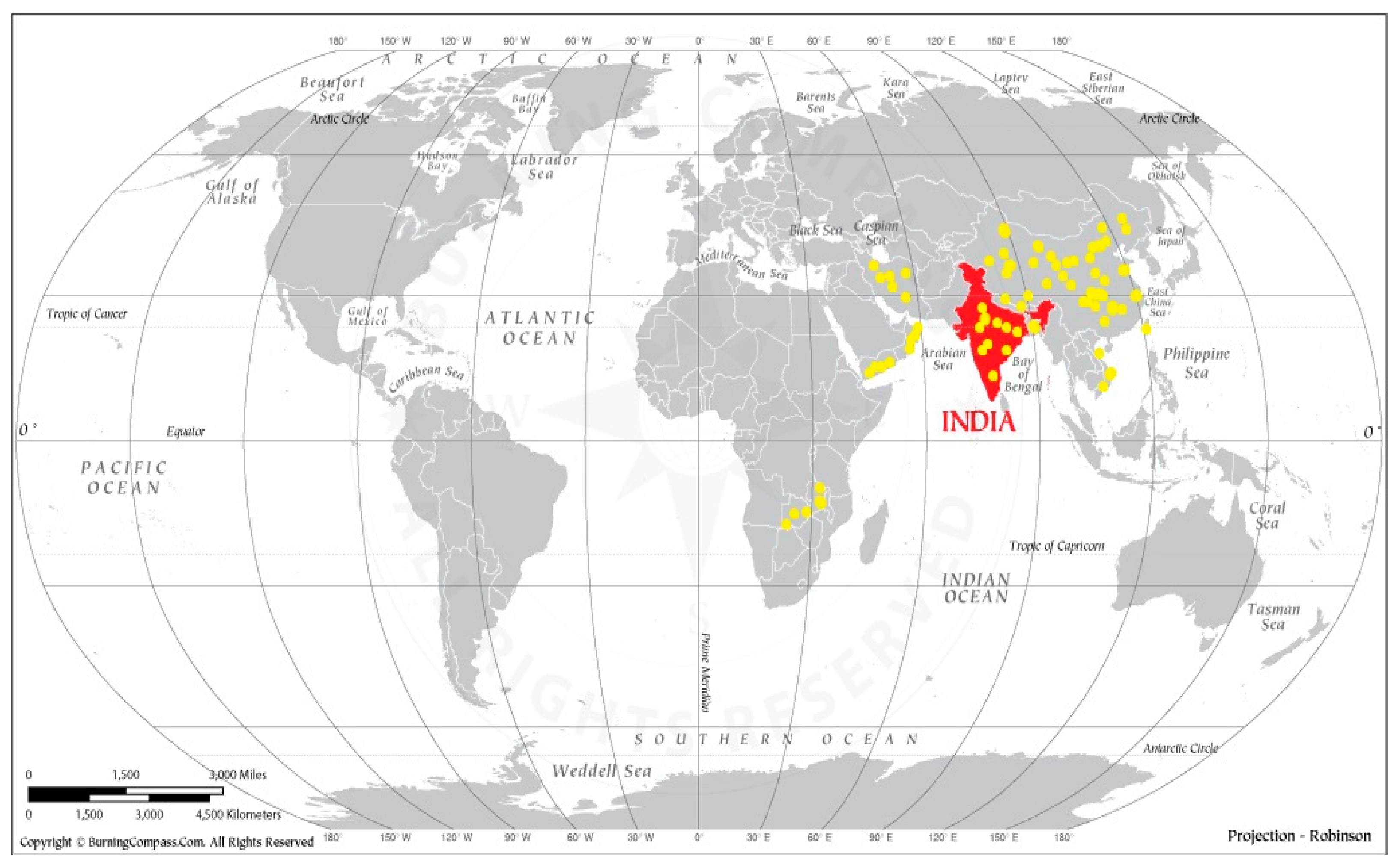
| 1. | India | 2019 | [10] |
| 2. | Bhutan | 2020 | [11] |
| 3. | Nepal | 2020 | [12] |
| 4. | Bangladesh | 2019 | [13] |
| 5. | Yemen | 1995 | [14] |
| 6. | Vietnam | 2020 | [4] |
| 7. | Oman | 2010 | [4] |
| 8. | China | 2019 | [15] |
| 9. | Zambia | 1929 | [2] |
| 10. | Taiwan | 2021 | [16] |
| 11. | Kuwait | 1991 | [4] |
| Sr. No. | Diagnostic Techniques Used for the Identification of LSD | Impacts on LSD | Pros | Cons | Reference |
|---|---|---|---|---|---|
| 1. | Viral isolation and identification through indirect fluorescent antibody test (IFAT) | It is one of the most accurate techniques for finding LSDV in a skin sample. | It is a quantitative as well as qualitative approach. | This method’s accuracy is based on the operator’s skill. | [30] |
| 2. | Detection using conventional PCR | It is the quickest and most reliable method for LSDV detection. | It is a substitute for the gold standard that allows for quick clinical confirmation and isolation in the absence of a live agent. | It is time-consuming, less sensitive, and involves post-PCR processing that introduces carryover contamination. | [30,31] |
| 3. | Histopathological examination | This technique is used to characterize LSDV and acts as a confirmatory test for its identification. | It is typically a very precise diagnostic method that provides greater details about a tissue and focuses on its architecture. | Its accuracy depends on the skill of the operator. | [30,31] |
| 4. | Immunohistochemistry test (IHC) | It is utilized to validate the presence of LSDV. | Tissue samples may be fresh or frozen, and IHC is well established and widely available. IHC provides a speedy turnaround and is reasonably priced. Because there are no live viral infections present, there is very little risk to human life. | It is extremely inexpensive, but IHC equipment is very pricey. Data quantification is especially difficult, and IHC is prone to human mistakes. It is essential that employees have the right training. | [30] |
| 5. | Indirect enzyme-linked immunosorbent Assay (iELISA) | This method is employed to identify antibodies in cows with LSDV infections. | This method is straightforward, has a high antigen–antibody response specificity and sensitivity, is accurate because multiple examinations can be performed simultaneously without time-consuming sample preparation, and is typically safe and environmentally friendly because radioactive materials and significant amounts of organic solvents are not required. Cost-effective chemicals are used in the test. | Making antibodies is labor-intensive and expensive due to the complex technology and pricey cell culture media required to manufacture a specific antibody. Erroneous positive or negative results pose a serious concern due to insufficient blocking at the bottom of the microtiter plate immobilized with the antigen. Since an antibody is a protein, it needs to be transported and refrigerated. | [31] |
| 6. | Transmission electron microscopy (TEM) | This method is used to evaluate skin biopsies to detect LSDV infection. | TEM can be applied in a wide range of unique research, academic, and industrial fields. Enhancements of one million times or more are seen in TEM, which provides information about element and compound structures. TEM images are crisp and detailed, and with the right training, they are easy to use. The topography, form, size, and structure of the surface can all be described in depth. | Large, expensive, labor-intensive samples that may contain artefacts during preparation must be electron-transparent, tolerant of the vacuum environment, and tiny enough to fit inside the vacuum chamber for TEM to be used. Analysis and operation also require specific abilities, appropriate housing, and management. It displays black-and-white images. | [32] |
| 7. | Virus neutralization test (VNT) | LSD employs this technique. Neutralizing antibodies take 3–4 days to manifest after the onset of pathogenic alterations. | It is a straightforward technology with a high performance, good accuracy, and sensitivity due to an antigen–antibody interaction. | High probability of false-positive or -negative results as a result of inadequate blocking of the antigen-coated microtiter plate surfaces. Since the production of antibodies requires technical expertise and an expensive cell growth medium, they are expensive to produce. | [33] |
| 8. | Agar gel immune diffusion test (AGID) | The procedure’s cross-reactivity with antibodies of all other poxviruses make it less precise than VNT. | It is an easy, group-specific test. | It takes time, is group-specific, has a semi-quantitative nature, and is moderately sensitive. | [33] |
| 9. | Immunological blotting (Western blotting) | Western blotting is difficult and expensive to perform, but it is exceedingly precise. | It tests denatured proteins to find changes in their functional states; is a delicate assay; provides excellent, clear information that is easy to interpret; and there are thousands of widely available commercial antibodies. | The tissue needs to be homogenized, which takes some time. | [33] |
| 10. | Real-time PCR (qPCR) | Real-time PCR tests offer quick and innovative ways to detect viruses in diagnostic laboratories. | Real-time PCR techniques enable quantitative estimation in addition to “positive” or “negative” results. | The considerable nucleotide sequence diversity (mismatches) in the genomes of the numerous strains of the targeted virus makes the PCR-based diagnostic techniques vulnerable, despite their many benefits. | [34] |
| Sr. No. | Different Control Measures for LSD | Impacts of Control Measures on LSD | Reference |
|---|---|---|---|
| 1. | Control of animal movement | LSD prevention and reducing the economic tolls of the outbreaks. | [46] |
| 2. | Restrictions for persons dealing with affected animals | People should not be allowed to leave the affected region if possible. | [47] |
| 3. | Immediate isolation | The isolation of symptomatic affected animals may be carried out with all precautions and bio-security measures. | [47] |
| 4. | Clinical surveillance | Clinical surveillance against LSD in affected areas should be intensified. | [47] |
| 5. | Separating other animals | By separating other animals from affected animals, the spread of LSD can be controlled. | [47] |
| 6. | Visiting by veterinarians | Regular visiting by veterinarians until all cases are recovered and taking all precautions to avoid further spread of the disease to other farms should be performed. | [47] |
| 7. | Vaccination | The vaccination of buffalo with the available goat pox vaccine prevents LSD. Currently, we only give immunizations against the sheep and goat pox viruses. Due to the fact that all three viruses belong to the same capripoxvirus genus, these heterologous vaccinations only provide cross-protection (up to 60–70%) for cattle against LSD. | [32] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Datten, B.; Chaudhary, A.A.; Sharma, S.; Singh, L.; Rawat, K.D.; Ashraf, M.S.; Alneghery, L.M.; Aladwani, M.O.; Rudayni, H.A.; Dayal, D.; et al. An Extensive Examination of the Warning Signs, Symptoms, Diagnosis, Available Therapies, and Prognosis for Lumpy Skin Disease. Viruses 2023, 15, 604. https://doi.org/10.3390/v15030604
Datten B, Chaudhary AA, Sharma S, Singh L, Rawat KD, Ashraf MS, Alneghery LM, Aladwani MO, Rudayni HA, Dayal D, et al. An Extensive Examination of the Warning Signs, Symptoms, Diagnosis, Available Therapies, and Prognosis for Lumpy Skin Disease. Viruses. 2023; 15(3):604. https://doi.org/10.3390/v15030604
Chicago/Turabian StyleDatten, Bharti, Anis Ahmad Chaudhary, Shalini Sharma, Lokender Singh, Krishna Dutta Rawat, Mohammad Saquib Ashraf, Lina M. Alneghery, Malak O. Aladwani, Hassan Ahmad Rudayni, Deen Dayal, and et al. 2023. "An Extensive Examination of the Warning Signs, Symptoms, Diagnosis, Available Therapies, and Prognosis for Lumpy Skin Disease" Viruses 15, no. 3: 604. https://doi.org/10.3390/v15030604