
Detection of Platelet-Activating Antibodies Associated with Vaccine-Induced Thrombotic Thrombocytopenia by Flow Cytometry: An Italian Experience

 , , , and
, , , and
Abstract
:1. Introduction
2. Methods
2.1. Study Population
2.2. Blood Collection
2.3. Immunological Assays
2.4. Functional Assays
3. Results
3.1. Immunological Assays
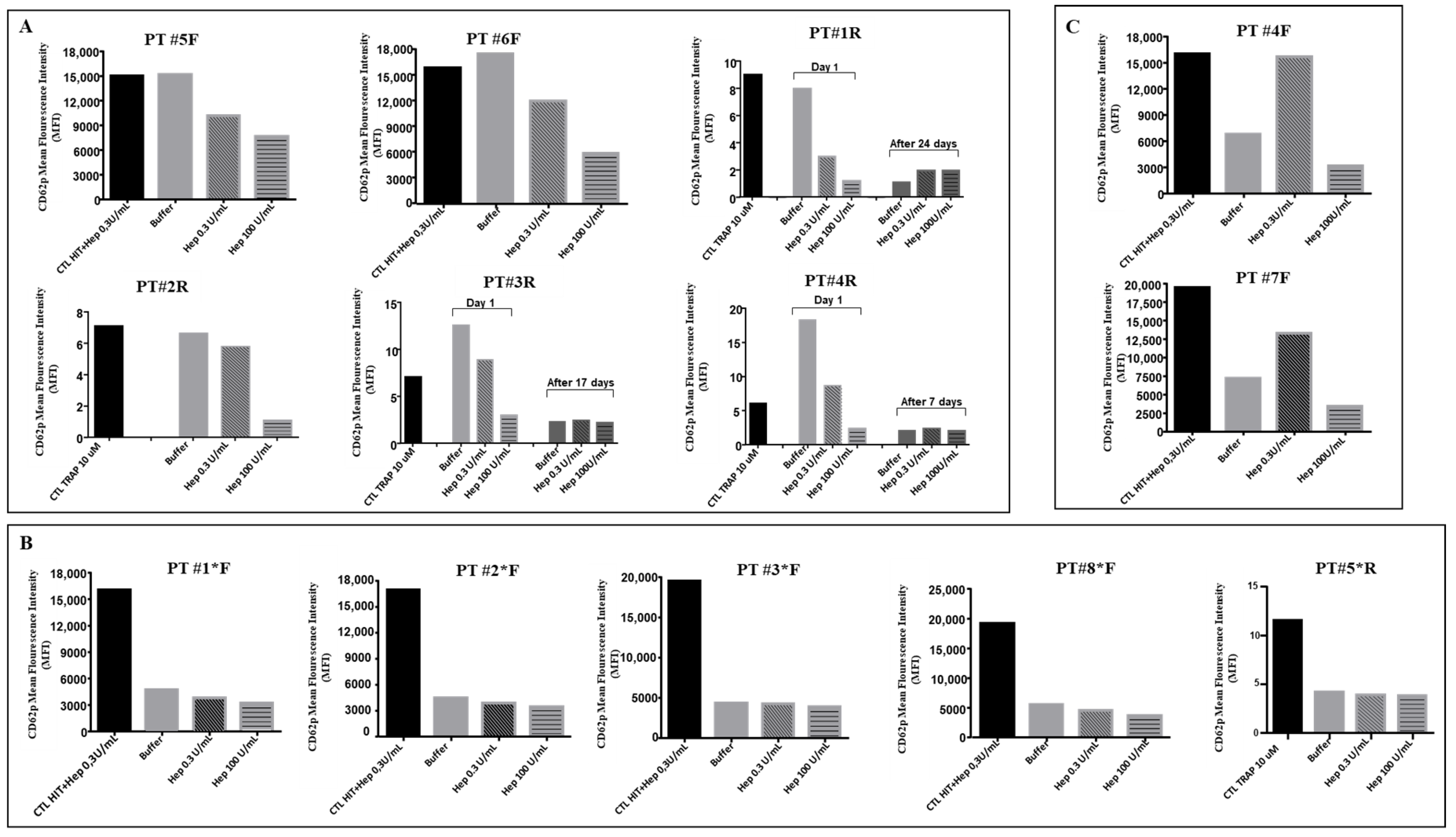
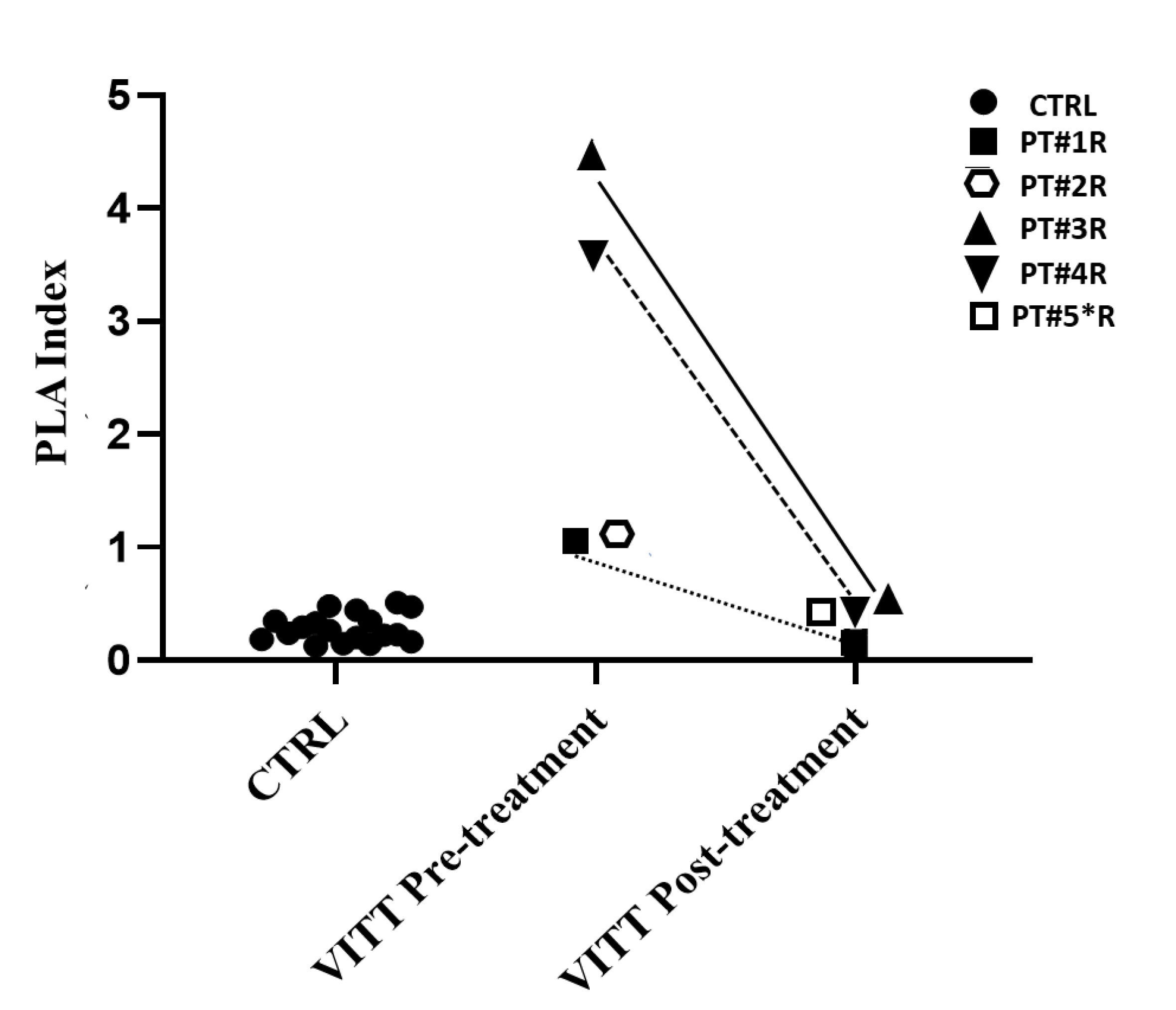
3.2. Functional Assays
4. Discussion
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- Anand, U.; Jakhmola, S.; Indari, O.; Jha, H.C.; Chen, Z.S.; Tripathi, V.; de la Lastra, J.M.P. Potential Therapeutic Targets and Vaccine Development for SARS-CoV-2/COVID-19 Pandemic Management: A Review on the Recent Update. Front. Immunol. 2021, 12, 658519. [Google Scholar] [CrossRef] [PubMed]
- Ling, Y.; Zhong, J.; Luo, J. Safety and effectiveness of SARS-CoV-2 vaccines: A systematic review and meta-analysis. J. Med. Virol. 2021, 93, 6486–6495. [Google Scholar] [CrossRef] [PubMed]
- Mendonça, S.A.; Lorincz, R.; Boucher, P.; Curiel, D.T. Adenoviral vector vaccine platforms in the SARS-CoV-2 pandemic. NPJ Vaccines 2021, 6, 97. [Google Scholar] [CrossRef] [PubMed]
- Greinacher, A.; Thiele, T.; Warkentin, T.E.; Weisser, K.; Kyrle, P.A.; Eichinger, S. Thrombotic Thrombocytopenia after ChAdOx1 nCov-19 Vaccination. N. Engl. J. Med. 2021, 384, 2092–2101. [Google Scholar] [CrossRef] [PubMed]
- Schultz, N.H.; Sørvoll, I.H.; Michelsen, A.E.; Munthe, L.A.; Lund-Johansen, F.; Ahlen, M.T.; Wiedmann, M.; Aamodt, A.H.; Skattør, T.H.; Tjønnfjord, G.E.; et al. Thrombosis and Thrombocytopenia after ChAdOx1 nCoV-19 Vaccination. N. Engl. J. Med. 2021, 384, 2124–2130. [Google Scholar] [CrossRef] [PubMed]
- Scully, M.; Singh, D.; Lown, R.; Poles, A.; Solomon, T.; Levi, M.; Goldblatt, D.; Kotoucek, P.; Thomas, W.; Lester, W. Pathologic Antibodies to Platelet Factor 4 after ChAdOx1 nCoV-19 Vaccination. N. Engl. J. Med. 2021, 384, 2202–2211. [Google Scholar] [CrossRef] [PubMed]
- Pavord, S.; Scully, M.; Hunt, B.J.; Lester, W.; Bagot, C.; Craven, B.; Rampotas, A.; Ambler, G.; Makris, M. Clinical Features of Vaccine-Induced Immune Thrombocytopenia and Thrombosis. N. Engl. J. Med. 2021, 385, 1680–1689. [Google Scholar] [CrossRef] [PubMed]
- Huynh, A.; Kelton, J.G.; Arnold, D.M.; Daka, M.; Nazy, I. Antibody epitopes in vaccine-induced immune thrombotic thrombocytopaenia. Nature 2021, 596, 565–569. [Google Scholar] [CrossRef] [PubMed]
- Greinacher, A.; Selleng, K.; Palankar, R.; Wesche, J.; Handtke, S.; Wolff, M.; Aurich, K.; Lalk, M.; Methling, K.; Völker, U.; et al. Insights in ChAdOx1 nCoV-19 vaccine-induced immune thrombotic thrombocytopenia. Blood 2021, 138, 2256–2268. [Google Scholar] [CrossRef] [PubMed]
- Greinacher, A.; Selleng, K.; Warkentin, T.E. Autoimmune heparin-induced thrombocytopenia. J. Thromb. Haemost. 2017, 15, 2099–2114. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Platton, S.; Bartlett, A.; MacCallum, P.; Makris, M.; McDonald, V.; Singh, D.; Scully, M.; Pavord, S. Evaluation of laboratory assays for anti-platelet factor 4 antibodies after ChAdOx1 nCOV-19 vaccination. J. Thromb. Haemost. JTH 2021, 19, 2007–2013. [Google Scholar] [CrossRef] [PubMed]
- Sørvoll, I.H.; Horvei, K.D.; Ernstsen, S.L.; Laegreid, I.J.; Lund, S.; Grønli, R.H.; Olsen, M.K.; Jacobsen, H.K.; Eriksson, A.; Halstensen, A.M.; et al. An observational study to identify the prevalence of thrombocytopenia and anti-PF4/polyanion antibodies in Norwegian health care workers after COVID-19 vaccination. J. Thromb. Haemost. 2021, 19, 1813–1818. [Google Scholar] [CrossRef] [PubMed]
- Warkentin, T.E. Laboratory diagnosis of heparin-induced thrombocytopenia. Int. J. Lab. Hematol. 2019, 41, 15–25. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Handtke, S.; Wolff, M.; Zaninetti, C.; Wesche, J.; Schönborn, L.; Aurich, K.; Ulm, L.; Hübner, N.O.; Becker, K.; Thiele, T.; et al. A flow cytometric assay to detect platelet-activating antibodies in VITT after ChAdOx1 nCov-19 vaccination. Blood 2021, 137, 3656–3659. [Google Scholar] [CrossRef] [PubMed]
- Runser, A.; Schaning, C.; Allemand, F.; Amiral, J. An Optimized and Standardized Rapid Flow Cytometry Functional Method for Heparin-Induced Thrombocytopenia. Biomedicines 2021, 9, 296. [Google Scholar] [CrossRef] [PubMed]
- Denys, B.; Stove, V.; Philippé, J.; Devreese, K. A clinical-laboratory approach contributing to a rapid and reliable diagnosis of heparin-induced thrombocytopenia. Thromb. Res. 2008, 123, 137–145. [Google Scholar] [CrossRef] [PubMed]
- Tardy-Poncet, B.; Montmartin, A.; Piot, M.; Alhenc-Gelas, M.; Nguyen, P.; Elalamy, I.; Greinacher, A.; Maistre, E.; Lasne, D.; Horellou, M.H.; et al. Functional Flow Cytometric Assay for Reliable and Convenient Heparin-Induced Thrombocytopenia Diagnosis in Daily Practice. Biomedicines 2021, 9, 332. [Google Scholar] [CrossRef] [PubMed]
- Greinacher, A.; Michels, I.; Kiefel, V.; Mueller-Eckhardt, C. A rapid and sensitive test for diagnosing heparin-associated thrombocytopenia. Thromb. Haemost. 1991, 66, 734–736. [Google Scholar] [CrossRef] [PubMed]
- Eichler, P.; Budde, U.; Haas, S.; Kroll, H.; Loreth, R.M.; Meyer, O.; Pachmann, U.; Pötzsch, B.; Schabel, A.; Albrecht, D.; et al. First workshop for detection of heparin induced antibodies: Validation of the heparin-induced platelet-activation test (HIPA) in comparison with a PF4/heparin ELISA. Thromb. Haemost. 1999, 81, 625–629. [Google Scholar] [CrossRef] [PubMed]
- Hursting, M.J.; Pai, P.J.; McCracken, J.E.; Hwang, F.; Suvarna, S.; Lokhnygina, Y.; Bandarenko, N.; Arepally, G.M. Platelet factor 4/heparin antibodies in blood bank donors. Am. J. Clin. Pathol. 2010, 134, 774–780. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
| VITT Cases | Age | Sex | Vaccine Type | Onset after Administration (Days) | Platelet Count | Thrombosis |
|---|---|---|---|---|---|---|
| Pt #1*F | 57 | F | AZ | 6 | 10.000/µL | Portal vein; pulmonary embolism; splenic vein |
| Pt #2*F | 73 | F | AZ | 6 | 10.000/µL | Pulmonary embolism; cerebral vein |
| Pt #3*F | 75 | F | AZ | 7 | 23.000/µL | Cerebral vein; portal vein |
| Pt #4F | 71 | M | AZ | 6 | <10.000/µL | Pulmonary embolism |
| Pt #5F | 78 | F | JJ | 10 | 24.000/µL | Multiple lower limb vein |
| Pt #6F | 41 | F | AZ | 9 | 49.000/µL | Cerebral vein |
| Pt #7F | 61 | M | AZ | 7 | 20.000/µL | Multiple lower limb vein |
| Pt #8F | 59 | F | AZ | 9 | 69.000/µL | Multiple lower limb vein; pulmonary embolism |
| Pt #1R | 35 | F | AZ | 6 | 20.000/µL | Right superior sinus; right transverse sinus; intrahepatic portal vessels |
| Pt #2R | 67 | M | AZ | 11 | 25.000/µL | Portal vein; mesenteric veins; splenic veins |
| Pt #3R | 42 | M | AZ | 7 | 33.000/µL | Superior sagittal sinus (partial); right sigmoid and transverse sinuses |
| Pt #4R | 33 | M | AZ | 7 | 25.000/µL | Superior sagittal sinus; straight sinus; right transverse sinus; right jugular vein; left carotid bifurcation; pulmonary embolism; abdominal aorta |
| Pt #5*R | 34 | M | JJ | 11 | 66.000/µL | Right sigmoid and transverse sinuses; right jugular vein |
| VITT Case | Vaccine Type | Hemosil AcuStar HIT-IgG (n.v. ≤ 1 U/mL) | Lifecode PF4 IgG Test (O.D./Cut Off 0.4) | Asserachrom HPIA IgG ELISA Pre-Treatment (O.D./Cut Off) | Asserachrom HPIA IgG ELISA Post-Treatment (O.D./Cut Off) | Flow Cytometry (MFI) | PLA Index Pre-Treatment (Cut Off 0.534) | PLA Index Post-Treatment (Cut Off 0.534) | Hipa Test |
|---|---|---|---|---|---|---|---|---|---|
| Pt #1*F | AZ | 0.04 | Positive (2.472) | / | / | Weakly Positive | / | / | Positive |
| Pt #2*F | AZ | 0.15 | Positive (1.912) | / | / | Weakly Positive | / | / | Negative |
| Pt #3*F | AZ | 0.06 | Positive (3.128) | / | / | Weakly Positive | / | / | Weakly Positive |
| Pt #4F | AZ | 0.04 | Positive (2.942) | / | / | HIT pattern | / | / | HIT Pattern |
| Pt #5F | JJ | 0.01 | Positive (3.339) | / | / | Positive | / | / | Positive |
| Pt #6F | AZ | 0.02 | Positive (1.473) | / | / | Positive | / | / | Positive |
| Pt #7F | AZ | 0.51 | Positive (3.257) | / | / | HIT pattern | / | / | HIT Pattern |
| Pt #8*F | AZ | 0.19 | Positive (3.026) | / | / | Weakly Positive | / | / | Positive |
| Pt #1R | AZ | 0.06 | / | Positive (1.230/1.135) | Negative (0.344/0.988) | Positive | 1.031 | 0.125 | Positive |
| Pt #2R | AZ | / | / | Positive (1.330/1.135) | / | Positive | 1.075 | / | Weakly Positive |
| Pt #3R | AZ | 0.04 | / | Positive (2.723/1.135) | Negative (0.464/1.809) | Positive | 4.286 | 0.441 | Positive |
| Pt #4R | AZ | 0.38 | / | Positive (2.973/1.123) | Negative (0.696/1.092) | Positive | 3.552 | 0.326 | Weakly Positive |
| Pt #5*R | JJ | 0.16 | / | / | Negative (0.790/1.344) | Weakly Positive | / | 0.373 | / |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cesari, F.; Sorrentino, S.; Gori, A.M.; Rogolino, A.; De Cristofaro, R.; Giusti, B.; Sticchi, E.; De Candia, E.; Marcucci, R. Detection of Platelet-Activating Antibodies Associated with Vaccine-Induced Thrombotic Thrombocytopenia by Flow Cytometry: An Italian Experience. Viruses 2022, 14, 1133. https://doi.org/10.3390/v14061133
Cesari F, Sorrentino S, Gori AM, Rogolino A, De Cristofaro R, Giusti B, Sticchi E, De Candia E, Marcucci R. Detection of Platelet-Activating Antibodies Associated with Vaccine-Induced Thrombotic Thrombocytopenia by Flow Cytometry: An Italian Experience. Viruses. 2022; 14(6):1133. https://doi.org/10.3390/v14061133
Chicago/Turabian StyleCesari, Francesca, Silvia Sorrentino, Anna Maria Gori, Angela Rogolino, Raimondo De Cristofaro, Betti Giusti, Elena Sticchi, Erica De Candia, and Rossella Marcucci. 2022. "Detection of Platelet-Activating Antibodies Associated with Vaccine-Induced Thrombotic Thrombocytopenia by Flow Cytometry: An Italian Experience" Viruses 14, no. 6: 1133. https://doi.org/10.3390/v14061133