
Simplified Acute Physiology Score 3 Performance in Austrian COVID-19 Patients Admitted to Intensive Care Units with and without Diabetes

 , , , , and
, , , , and
Abstract
:1. Introduction
2. Methods
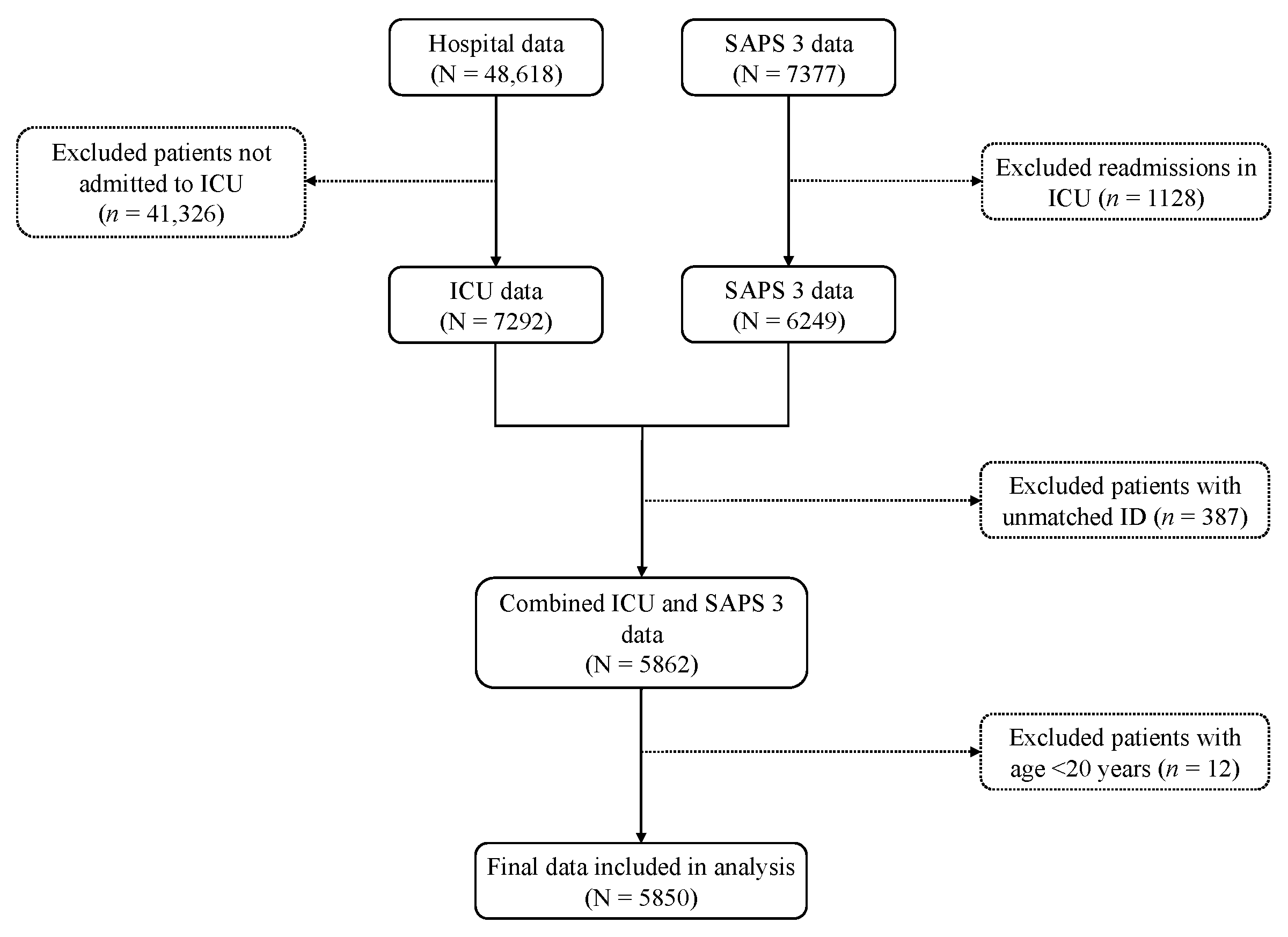
2.1. Study Design and Data Source
2.2. Data Extraction
2.3. Study Variables
2.4. Statistical Analysis
2.4.1. Summary Statistics
2.4.2. Calculation of SAPS 3 Score and Predicted in-Hospital Mortality
2.4.3. Assessment of Predictive Performance of SAPS 3
2.5. Ethical Considerations
3. Results
3.1. Characteristics of Patients
3.2. Observed In-Hospital Mortality and Its Comparison with Variables
3.3. Predicted In-Hospital Mortality and Standardized Mortality Ratio
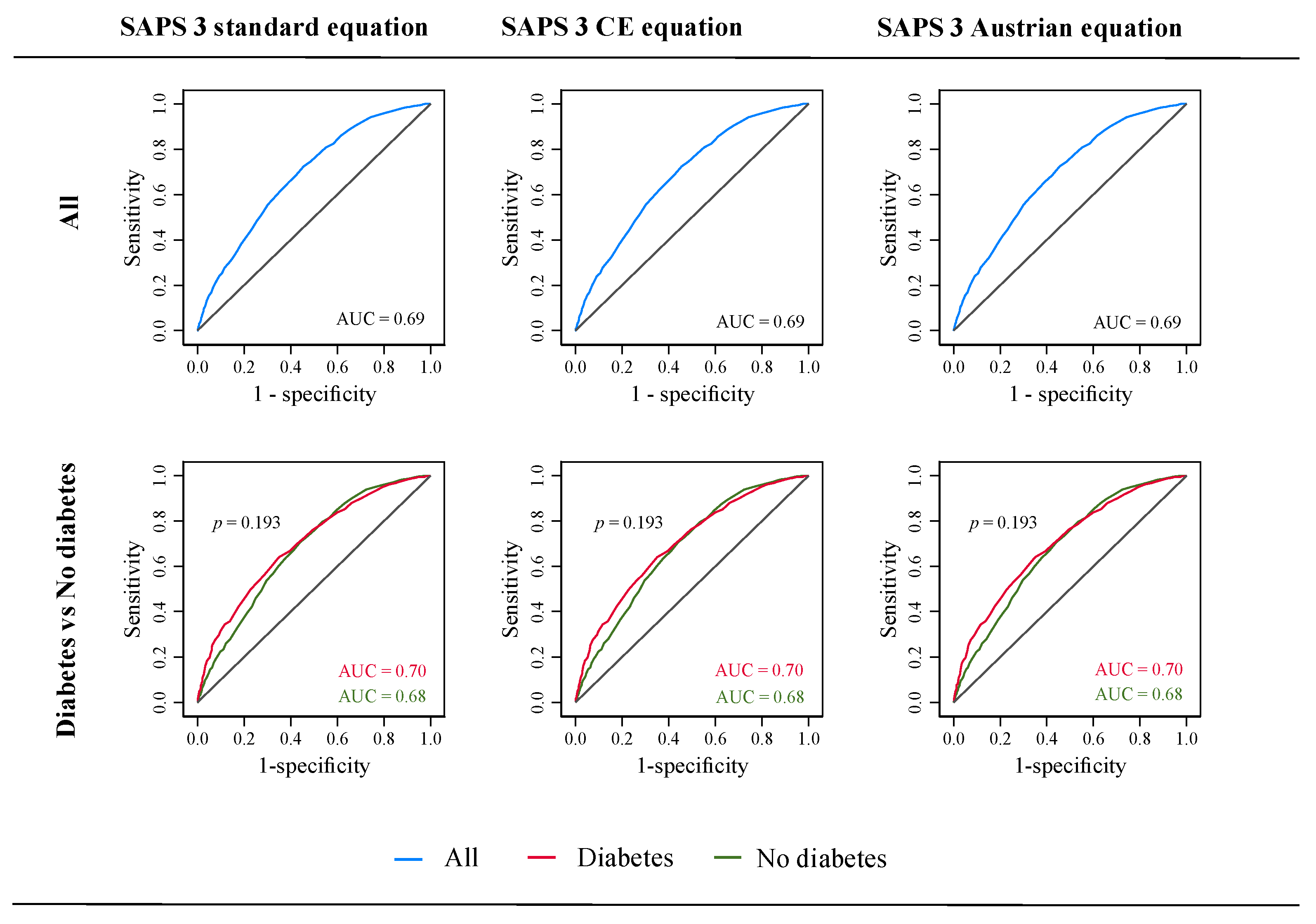
3.4. Discrimination and Accuracy of SAPS 3
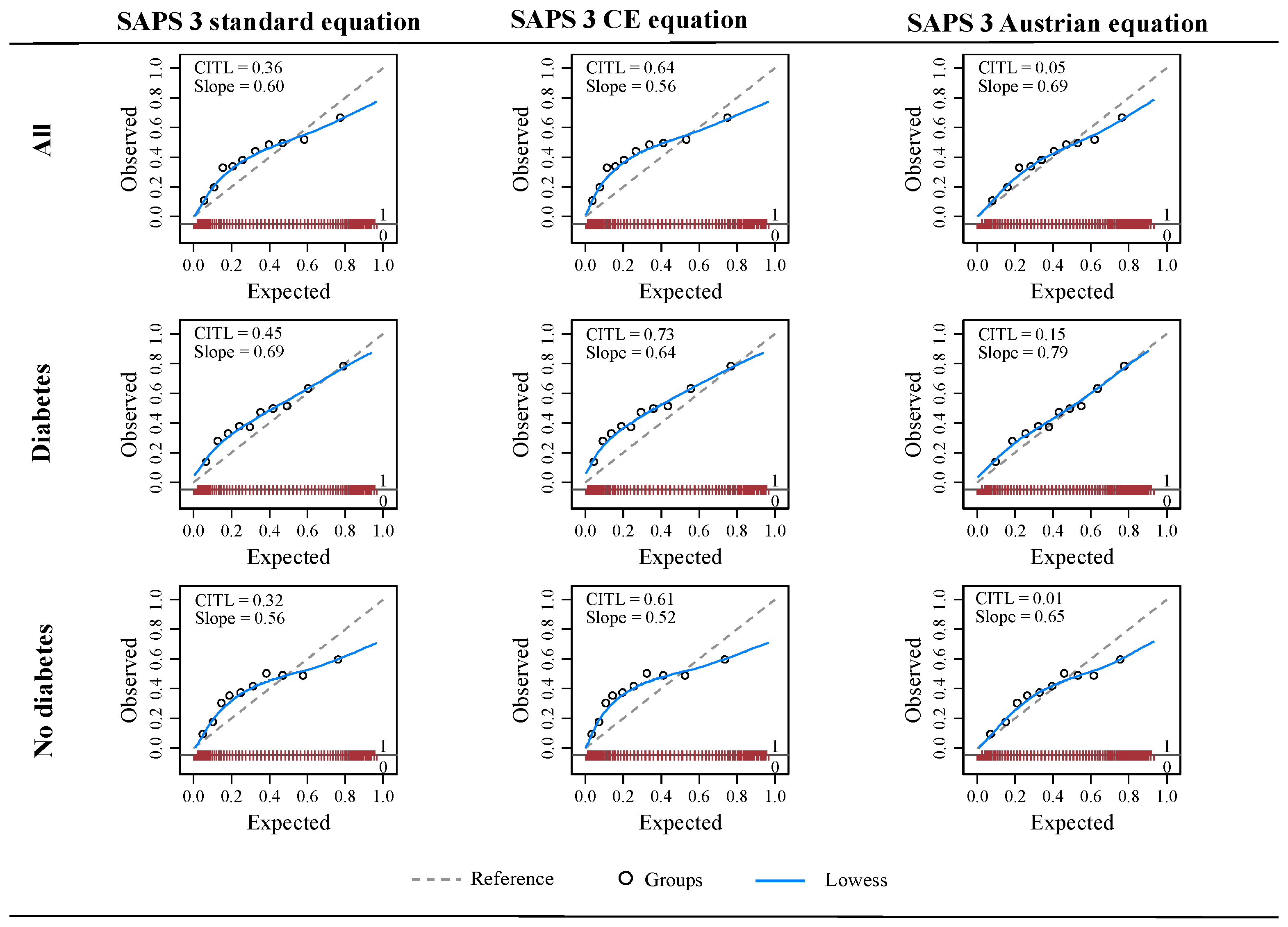
3.5. Calibration of SAPS 3
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- WHO. WHO Coronavirus (COVID-19) Dashboard. Available online: https://covid19.who.int (accessed on 22 October 2021).
- Emanuel, E.J.; Persad, G.; Upshur, R.; Thome, B.; Parker, M.; Glickman, A.; Zhang, C.; Boyle, C.; Smith, M.; Phillips, J.P. Fair Allocation of Scarce Medical Resources in the Time of Covid-19. N. Engl. J. Med. 2020, 382, 2049–2055. [Google Scholar] [CrossRef] [PubMed]
- Salluh, J.I.F.; Soares, M. ICU Severity of Illness Scores: APACHE, SAPS and MPM. Curr. Opin. Crit. Care 2014, 20, 557–565. [Google Scholar] [CrossRef] [PubMed]
- Moreno, R.P.; Metnitz, P.G.H.; Almeida, E.; Jordan, B.; Bauer, P.; Campos, R.A.; Iapichino, G.; Edbrooke, D.; Capuzzo, M.; Le Gall, J.-R.; et al. SAPS 3—From Evaluation of the Patient to Evaluation of the Intensive Care Unit. Part 2: Development of a Prognostic Model for Hospital Mortality at ICU Admission. Intensive Care Med. 2005, 31, 1345–1355. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kurtz, P.; Bastos, L.S.L.; Salluh, J.I.F.; Bozza, F.A.; Soares, M. SAPS-3 Performance for Hospital Mortality Prediction in 30,571 Patients with COVID-19 Admitted to ICUs in Brazil. Intensive Care Med. 2021, 47, 1047–1049. [Google Scholar] [CrossRef] [PubMed]
- Metnitz, P.G.H.; Moreno, R.P.; Fellinger, T.; Posch, M.; Zajic, P. Evaluation and Calibration of SAPS 3 in Patients with COVID-19 Admitted to Intensive Care Units. Intensive Care Med. 2021, 47, 910–912. [Google Scholar] [CrossRef] [PubMed]
- Collins, G.S.; Reitsma, J.B.; Altman, D.G.; Moons, K.G.M. Transparent Reporting of a Multivariable Prediction Model for Individual Prognosis or Diagnosis (TRIPOD): The TRIPOD Statement. Ann. Intern. Med. 2015, 162, 55–63. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pencina, M.J.; D’Agostino, R.B. Evaluating Discrimination of Risk Prediction Models: The C Statistic. JAMA 2015, 314, 1063–1064. [Google Scholar] [CrossRef] [PubMed]
- Steyerberg, E.W. Evaluation of Performance. In Clinical Prediction Models: A Practical Approach to Development, Validation, and Updating; Steyerberg, E.W., Ed.; Statistics for Biology and Health; Springer International Publishing: Cham, Switzerland, 2019; pp. 277–308. ISBN 978-3-030-16399-0. [Google Scholar]
- Covino, M.; De Matteis, G.; Polla, D.A.D.; Santoro, M.; Burzo, M.L.; Torelli, E.; Simeoni, B.; Russo, A.; Sandroni, C.; Gasbarrini, A.; et al. Predictors of In-Hospital Mortality AND Death RISK STRATIFICATION among COVID-19 PATIENTS Aged ≥ 80 YEARs OLD. Arch. Gerontol. Geriatr. 2021, 95, 104383. [Google Scholar] [CrossRef]
- Poncet, A.; Perneger, T.V.; Merlani, P.; Capuzzo, M.; Combescure, C. Determinants of the Calibration of SAPS II and SAPS 3 Mortality Scores in Intensive Care: A European Multicenter Study. Crit. Care 2017, 21, 85. [Google Scholar] [CrossRef] [Green Version]
- Mokhtari, T.; Hassani, F.; Ghaffari, N.; Ebrahimi, B.; Yarahmadi, A.; Hassanzadeh, G. COVID-19 and Multiorgan Failure: A Narrative Review on Potential Mechanisms. J. Mol. Histol. 2020, 51, 613–628. [Google Scholar] [CrossRef] [PubMed]
- Sourij, H.; Aziz, F.; Bräuer, A.; Ciardi, C.; Clodi, M.; Fasching, P.; Karolyi, M.; Kautzky-Willer, A.; Klammer, C.; Malle, O.; et al. COVID-19 Fatality Prediction in People with Diabetes and Prediabetes Using a Simple Score upon Hospital Admission. Diabetes Obes. Metab. 2021, 23, 589–598. [Google Scholar] [CrossRef] [PubMed]
- Knight, S.R.; Ho, A.; Pius, R.; Buchan, I.; Carson, G.; Drake, T.M.; Dunning, J.; Fairfield, C.J.; Gamble, C.; Green, C.A.; et al. Risk Stratification of Patients Admitted to Hospital with Covid-19 Using the ISARIC WHO Clinical Characterisation Protocol: Development and Validation of the 4C Mortality Score. BMJ 2020, 370, m3339. [Google Scholar] [CrossRef] [PubMed]
- Falcão, A.L.E.; Barros, A.G.d.A.; Bezerra, A.A.M.; Ferreira, N.L.; Logato, C.M.; Silva, F.P.; do Monte, A.B.F.O.; Tonella, R.M.; de Figueiredo, L.C.; Moreno, R.; et al. The Prognostic Accuracy Evaluation of SAPS 3, SOFA and APACHE II Scores for Mortality Prediction in the Surgical ICU: An External Validation Study and Decision-Making Analysis. Ann. Intensive Care 2019, 9, 18. [Google Scholar] [CrossRef] [PubMed]
- Moralez, G.M.; Rabello, L.S.C.F.; Lisboa, T.C.; Lima, M.d.F.A.; Hatum, R.M.; De Marco, F.V.C.; Alves, A.; Pinto, J.E.d.S.S.; de Araújo, H.B.N.; Ramos, G.V.; et al. External Validation of SAPS 3 and MPM0-III Scores in 48,816 Patients from 72 Brazilian ICUs. Ann. Intensive Care 2017, 7, 53. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aziz, F.; Aberer, F.; Bräuer, A.; Ciardi, C.; Clodi, M.; Fasching, P.; Karolyi, M.; Kautzky-Willer, A.; Klammer, C.; Malle, O.; et al. COVID-19 In-Hospital Mortality in People with Diabetes Is Driven by Comorbidities and Age—Propensity Score-Matched Analysis of Austrian National Public Health Institute Data. Viruses 2021, 13, 2401. [Google Scholar] [CrossRef] [PubMed]
- Lim, S.; Bae, J.H.; Kwon, H.-S.; Nauck, M.A. COVID-19 and Diabetes Mellitus: From Pathophysiology to Clinical Management. Nat. Rev. Endocrinol. 2021, 17, 11–30. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Variable | All | Diabetes | p-Value | |
|---|---|---|---|---|
| Yes | No | |||
| All, n (%) | 5850 | 1667 (28.50) | 4183 (71.50) | -- |
| Sex, n (%) | ||||
| Female | 1985 (33.93) | 541 (32.45) | 1444 (34.52) | 0.132 |
| Male | 3865 (66.07) | 1126 (67.55) | 2739 (65.48) | |
| Age, years, n (%) | ||||
| <40 | 215 (3.68) | 22 (1.32) | 193 (4.61) | <0.001 |
| 40–59 | 1258 (21.50) | 330 (19.80) | 928 (22.19) | |
| 60–69 | 1471 (25.15) | 457 (27.41) | 1014 (24.24) | |
| 70–74 | 906 (15.49) | 312 (18.72) | 594 (14.20) | |
| 75–79 | 895 (15.30) | 259 (15.54) | 636 (15.20) | |
| ≥80 | 1105 (18.89) | 287 (17.22) | 818 (19.56) | |
| Stay in hospital before ICU admission, days, n (%) | ||||
| <14 | 4437 (75.85) | 1254 (75.22) | 3183 (76.09) | 0.781 |
| 14–27 | 912 (15.59) | 267 (16.02) | 645 (15.42) | |
| ≥28 | 501 (8.56) | 146 (8.76) | 355 (8.49) | |
| Intra-hospital location before ICU admission, n (%) | ||||
| Operative room | 334 (5.71) | 70 (4.20) | 264 (6.31) | 0.017 |
| Emergency room | 920 (15.73) | 265 (15.90) | 655 (15.66) | |
| Other ICU | 1160 (19.83) | 344 (20.64) | 816 (19.51) | |
| Hospital wards | 3436 (58.74) | 988 (59.27) | 2448 (58.52) | |
| Comorbidities | ||||
| Cancer therapy, n (%) | 480 (8.21) | 154 (9.24) | 326 (7.79) | 0.069 |
| Congestive heart failure, NYHA IV, n (%) | 131 (2.24) | 49 (2.94) | 82 (1.96) | 0.022 |
| Hematological cancer, n (%) | 148 (2.53) | 29 (1.74) | 119 (2.84) | 0.015 |
| Cirrhosis, n (%) | 86 (1.47) | 25 (1.50) | 61 (1.46) | 0.905 |
| AIDS, n (%) | 3 (0.05) | 3 (0.18) | 0 (0.00) | 0.023 |
| Cancer with metastasis, n (%) | 114 (1.95) | 16 (0.96) | 98 (2.34) | 0.001 |
| Vasoactive drugs before ICU admission, n (%) | 916 (15.66) | 246 (14.76) | 670 (16.02) | 0.231 |
| Reasons for ICU admission | ||||
| Cardiovascular, n (%) | ||||
| Arrhythmia | 112 (1.91) | 20 (1.20) | 92 (2.20) | 0.043 |
| All others | 5576 (95.32) | 1601 (96.04) | 3975 (95.03) | |
| Hypovolemic shock | 32 (0.55) | 6 (0.36) | 26 (0.62) | |
| Septic, anaphylactic, undefined, and mixed shock | 130 (2.22) | 40 (2.40) | 90 (2.15) | |
| Hepatic, n (%) | ||||
| All other | 5831 (99.68) | 1660 (99.58) | 4171 (99.71) | 0.420 |
| Liver failure | 19 (0.32) | 7 (0.42) | 12 (0.29) | |
| Digestive, n (%) | ||||
| All others | 5783 (98.85) | 1653 (99.16) | 4130 (98.73) | 0.260 |
| Acute abdomen, other | 54 (0.92) | 10 (0.60) | 44 (1.05) | |
| Severe pancreatitis | 13 (0.22) | 4 (0.24) | 9 (0.22) | |
| Neurologic, n (%) | ||||
| Seizures | 19 (0.32) | 1 (0.06) | 18 (0.43) | 0.007 |
| All others | 5482 (93.71) | 1562 (93.70) | 3920 (93.71) | |
| Coma, stupor, obtund patient, agitation, vigilance disturbances, confusion, delirium | 248 (5.24) | 85 (5.10) | 163 (3.90) | |
| Focal neurological deficit | 71 (1.21) | 12 (0.72) | 59 (1.41) | |
| Intracranial mass effect | 30 (0.51) | 7 (0.42) | 23 (0.55) | |
| Surgical status at ICU admission, n (%) | ||||
| No surgery | 5251 (89.76) | 1552 (93.10) | 3699 (88.43) | <0.001 |
| Scheduled surgery | 294 (5.03) | 64 (3.84) | 230 (5.50) | |
| Emergency surgery | 305 (5.21) | 51 (3.06) | 254 (6.07) | |
| Anatomical site of surgery, n (%) | ||||
| Transplant surgery | 1 (0.02) | 0 (0.00) | 1 (0.02) | 0.169 |
| Trauma | 51 (0.87) | 11 (0.66) | 40 (0.96) | |
| Cardiac surgery | 23 (0.39) | 6 (0.36) | 17 (0.41) | |
| All others | 5746 (98.22) | 1647 (98.80) | 4099 (97.99) | |
| Neurosurgery | 29 (0.50) | 3 (0.18) | 26 (0.62) | |
| GCS score, median (IQR) | 15 (1) | 15 (1) | 15 (1) | 0.016 |
| Mean ± SD | 13.40 ± 3.51 | 13.34 ± 3.50 | 13.43 ± 3.51 | |
| Total bilirubin, mg/dL, median (IQR) | 0.60 (0.50) | 0.50 (0.40) | 0.60 (0.50) | <0.001 |
| Body temperature, °C, mean ± SD | 37.27 ± 1.30 | 37.31 ± 1.29 | 37.26 ± 1.21 | 0.192 |
| Creatinine, mg/dL, median (IQR) | 1.00 (0.60) | 1.10 (0.90) | 1.00 (0.60) | <0.001 |
| Heart rate, bpm, mean ± SD | 90 ± 30 | 93 ± 30 | 90 ± 29 | <0.001 |
| Leukocytes, G/L, median (IQR) | 9.40 (6.40) | 9.40 (6.20) | 9.40 (6.50) | 0.775 |
| Hydrogen ion, pH, median (IQR) | 7.42 (0.12) | 7.41 (0.13) | 7.42 (0.11) | <0.001 |
| Platelets, G/L, median (IQR) | 218.00 (122.00) | 224.00 (123.50) | 215.50 (123.00) | 0.043 |
| Systolic blood pressure, mmHg, mean ± SD | 116.12 ± 31.27 | 116.68 ± 32.35 | 115.89 ± 30.81 | 0.417 |
| PaO2, mmHg, median (IQR) | 69 (27) | 68 (26) | 69 (28) | 0.052 |
| FiO2, %, median (IQR) | 60 (40) | 65 (30) | 60 (40) | <0.001 |
| SAPS 3 score, mean ± SD | 57.39 ± 13.18 | 58.78 ± 12.92 | 56.84 ± 13.23 | <0.001 |
| Characteristic | In-Hospital Mortality | p-Value | |
|---|---|---|---|
| Yes | No | ||
| All, n (%) | 2276 (38.91) | 3574 (61.09) | -- |
| Diabetes, n (%) | |||
| No | 1560 (37.29) | 2623 (62.71) | <0.001 |
| Yes | 716 (42.95) | 951 (57.05) | |
| Sex, n (%) | |||
| Female | 742 (37.38) | 1243 (62.62) | 0.086 |
| Male | 1534 (39.69) | 2331 (60.31) | |
| Age, years, n (%) | |||
| <40 | 22 (10.23) | 193 (89.77) | <0.001 |
| 40–59 | 219 (17.41) | 1039 (82.59) | |
| 60–69 | 496 (33.72) | 975 (66.28) | |
| 70–74 | 401 (44.26) | 505 (55.74) | |
| 75–79 | 467 (52.18) | 428 (47.82) | |
| ≥80 | 671 (60.72) | 434 (39.28) | |
| Stay in hospital before ICU admission, days, n (%) | |||
| <14 | 2009 (45.28) | 2428 (54.72) | <0.001 |
| 14–27 | 197 (21.60) | 715 (78.40) | |
| ≥28 | 70 (13.97) | 431 (86.03) | |
| Intra-hospital location before ICU admission, n (%) | |||
| Operative room | 64 (19.16) | 270 (80.84) | <0.001 |
| Emergency room | 326 (35.43) | 594 (64.57) | |
| Other ICU | 479 (41.29) | 681 (58.71) | |
| Hospital wards | 1407 (40.95) | 2029 (59.05) | |
| Comorbidities | |||
| Cancer therapy, n (%) | 247 (51.46) | 233 (48.54) | <0.001 |
| Congestive heart failure, NYHA IV, n (%) | 84 (64.12) | 47 (35.88) | <0.001 |
| Hematological cancer, n (%) | 72 (48.65) | 76 (51.35) | 0.003 |
| Cirrhosis, n (%) | 52 (60.47) | 34 (39.53) | 0.001 |
| AIDS, n (%) | 0 (0.00) | 3 (100.00) | 0.167 |
| Cancer with metastasis, n (%) | 60 (52.63) | 54 (47.37) | 0.002 |
| Vasoactive drugs before ICU admission, n (%) | 429 (46.83) | 487 (53.17) | <0.001 |
| Reasons for ICU admission | |||
| Cardiovascular, n (%) | |||
| Arrhythmia | 35 (31.25) | 77 (78.75) | <0.001 |
| All others | 2155 (38.35) | 3421 (61.35) | |
| Hypovolemic shock | 15 (46.88) | 17 (53.12) | |
| Septic, anaphylactic, undefined, and mixed shock | 71 (54.62) | 59 (45.38) | |
| Hepatic, n (%) | |||
| All other | 1970 (33.78) | 3861 (66.22) | <0.001 |
| Liver failure | 15 (78.95) | 4 (21.05) | |
| Digestive, n (%) | |||
| All others | 2262 (39.11) | 3521 (60.89) | 0.003 |
| Acute abdomen, other | 9 (16.67) | 45 (83.33) | |
| Severe pancreatitis | 5 (38.46) | 8 (61.54) | |
| Neurologic, n (%) | 0.045 | ||
| Seizures | 6 (31.58) | 13 (68.62) | |
| All others | 2115 (38.58) | 3367 (61.42) | |
| Coma, stupor, obtunded patient, agitation, vigilance disturbances, confusion, delirium | 119 (47.98) | 129 (52.02) | |
| Focal neurological deficit | 25 (35.21) | 46 (64.79) | |
| Intracranial mass effect | 11 (36.67) | 19 (63.33) | |
| Surgical status at ICU admission, n (%) | <0.001 | ||
| No surgery | 2155 (41.04) | 3096 (58.96) | |
| Scheduled surgery | 47 (15.99) | 247 (84.01) | |
| Emergency surgery | 74 (24.26) | 231 (75.74) | |
| Anatomical site of surgery, n (%) | |||
| Transplant surgery | 1 (100.00) | 0 (0.00) | <0.001 |
| Trauma | 14 (27.45) | 37 (72.55) | |
| Cardiac surgery | 0 (0.00) | 23 (100.00) | |
| All others | 2255 (39.24) | 3491 (60.76) | |
| Neurosurgery | 6 (20.69) | 23 (79.31) | |
| GCS score, median (IQR) | 15 (2) | 15 (0) | <0.001 |
| Mean ± SD | 12.72 ± 3.99 | 13.83 ± 3.08 | |
| Total bilirubin, mg/dL, median (IQR) | 0.60 (0.50) | 0.60 (0.40) | 0.001 |
| Body temperature, °C, mean ± SD | 37.26 ± 1.29 | 37.29 ± 1.20 | 0.471 |
| Creatinine, mg/dL, median (IQR) | 1.19 (0.80) | 0.90 (0.50) | <0.001 |
| Heart rate, bpm, mean ± SD | 97 ± 26 | 93 ± 23 | <0.001 |
| Leukocytes, G/L, median (IQR) | 9.87 (7.10) | 9.00 (5.80) | <0.001 |
| Hydrogen ion, pH, median (IQR) | 7.40 (0.14) | 7.43 (0.09) | <0.001 |
| Platelets, G/L, median (IQR) | 202.00 (117.00) | 229.00 (123.00) | <0.001 |
| Systolic blood pressure, mmHg, mean ± SD | 112.57 ± 31.93 | 118.43 ± 30.62 | <0.001 |
| PaO2, mmHg, median (IQR) | 66 (24) | 70 (29) | <0.001 |
| FiO2, %, median (IQR) | 70 (40) | 55 (40) | <0.001 |
| SAPS 3 score | |||
| All patients, mean ± SD | 62.57 ± 12.86 | 54.10 ± 12.29 | <0.001 |
| Diabetes, mean ± SD | 63.96 ± 13.15 | 54.87 ± 11.28 | <0.001 |
| No diabetes, mean ± SD | 61.92 ± 12.68 | 53.82 ± 12.62 | <0.001 |
| SAPS 3 Equations | Mortality | Discrimination | Calibration | ||
|---|---|---|---|---|---|
| Predicted Mortality Mean ± SD | SMR (95%CI) | AUROC (95%CI) | H-L X2, p-Value | Brier Score | |
| Standard equation | |||||
| All | 32.47 ± 21.69 | 1.20 (1.16–1.24) | 68.67 (67.31–70.02) | 100.03, <0.001 | 0.22 |
| Diabetes | 34.56 ± 21.62 | 1.24 (1.18–1.31) | 70.03 (67.53–72.53) | 12.21, 0.142 | 0.22 |
| No diabetes | 31.63 ± 21.66 | 1.18 (1.13–1.22) | 68.05 (66.44–69.67) | 101.64, <0.001 | 0.22 |
| Central Europe equation | |||||
| All | 28.05 ± 21.43 | 1.39 (1.34–1.43) | 68.67 (67.31–70.02) | 120.95, <0.001 | 0.23 |
| Diabetes | 30.02 ± 21.56 | 1.43 (1.35–1.51) | 70.03 (67.53–72.53) | 15.08, 0.058 | 0.23 |
| No diabetes | 27.28 ± 21.33 | 1.37 (1.31–1.42) | 68.05 (66.44–69.67) | 119.99, <0.001 | 0.23 |
| Austrian equation | |||||
| All | 37.86 ± 20.56 | 1.03 (0.99–1.06) | 68.67 (67.31–70.02) | 65.10, <0.001 | 0.22 |
| Diabetes | 40.03 ± 20.16 | 1.07 (1.02–1.13) | 70.03 (67.53–72.53) | 9.04, 0.339 | 0.22 |
| No diabetes | 37.00 ± 20.66 | 1.01 (0.98–1.05) | 68.05 (66.44–69.67) | 69.55, <0.001 | 0.22 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Aziz, F.; Reisinger, A.C.; Aberer, F.; Sourij, C.; Tripolt, N.; Siller-Matula, J.M.; von-Lewinski, D.; Eller, P.; Kaser, S.; Sourij, H.; et al. Simplified Acute Physiology Score 3 Performance in Austrian COVID-19 Patients Admitted to Intensive Care Units with and without Diabetes. Viruses 2022, 14, 777. https://doi.org/10.3390/v14040777
Aziz F, Reisinger AC, Aberer F, Sourij C, Tripolt N, Siller-Matula JM, von-Lewinski D, Eller P, Kaser S, Sourij H, et al. Simplified Acute Physiology Score 3 Performance in Austrian COVID-19 Patients Admitted to Intensive Care Units with and without Diabetes. Viruses. 2022; 14(4):777. https://doi.org/10.3390/v14040777
Chicago/Turabian StyleAziz, Faisal, Alexander Christian Reisinger, Felix Aberer, Caren Sourij, Norbert Tripolt, Jolanta M. Siller-Matula, Dirk von-Lewinski, Philipp Eller, Susanne Kaser, Harald Sourij, and et al. 2022. "Simplified Acute Physiology Score 3 Performance in Austrian COVID-19 Patients Admitted to Intensive Care Units with and without Diabetes" Viruses 14, no. 4: 777. https://doi.org/10.3390/v14040777