
Epidemiological and Clinical Characteristics of Acute Dengue Virus Infections Detected through Acute Febrile Illness Surveillance, Belize 2020

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Data Collection and Laboratory Testing
2.3. Data Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Centers for Disease Control and Prevention. Neglected Tropical Diseases-Diseases. Available online: https://www.cdc.gov/globalhealth/ntd/diseases/index.html (accessed on 23 January 2021).
- Centers for Disease Control and Prevention, Dengue. Available online: https://www.cdc.gov/dengue/index.html (accessed on 16 August 2020).
- Hotez, P.J.; Bottazzi, M.E.; Franco-Paredes, C.; Ault, S.K.; Periago, M.R. The Neglected Tropical Diseases of Latin America and the Caribbean: A Review of Disease Burden and Distribution and a Roadmap for Control and Elimination. PLoS Negl. Trop. Dis. 2008, 2, e300. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organization. Dengue and Severe Dengue. Available online: https://www.who.int/news-room/fact-sheets/detail/dengue-and-severe-dengue (accessed on 16 August 2020).
- Torres, J.R.; Castro, J. The Health and Economic Impact of Dengue in Latin America. Cad. Saúde Pública 2007, 23, S23–S31. [Google Scholar] [CrossRef] [Green Version]
- Statistical Institute of Belize. Postcensal Estimates by Age Group and Sex, 2010–2020. Available online: http://sib.org.bz/statistics/population/ (accessed on 6 March 2020).
- Central Intelligence Agency. The World Factbook: Belize. Available online: https://www.cia.gov/the-world-factbook/countries/belize/ (accessed on 24 January 2021).
- National Meteorological Service of Belize. Climate Summary: The Climate of Belize. Available online: http://nms.gov.bz/climate-services/climate-summary/ (accessed on 4 October 2021).
- The World Bank. World Bank Country and Lending Groups. Available online: https://datahelpdesk.worldbank.org/knowledgebase/articles/906519-world-bank-country-and-lending-groups (accessed on 9 October 2020).
- Belize Ministry of Health. Belize Health Sector Strategic Plan 2014–2024. Available online: http://health.gov.bz/www/attachments/article/801/Belize%20Health%20Sector%20Strategic%20Plan%202014-2024-April%202014.pdf (accessed on 26 October 2020).
- Dillon, L.; Drebot, M.A.; Robertson, L.; Wood, H.; Loftis, A.; Grolla, A.; Lee, E.; Forde, M.; Dewailly, E.; Krecek, R.C.; et al. Seroprevalence of Seven Zoonotic Pathogens in Pregnant Women from the Caribbean. Am. J. Trop. Med. Hyg. 2014, 91, 642–644. [Google Scholar] [CrossRef]
- Belize Ministry of Health. Vector Control. Available online: https://health.gov.bz/www/organogram/214-vector-control (accessed on 2 September 2020).
- World Health Organization; Special Programme for Research; Training in Tropical Diseases. Dengue: Guidelines for Diagnosis, Treatment, Prevention, and Control; World Health Organization: Geneva, Switzerland, 2009. [Google Scholar]
- Gorchakov, R.; Berry, R.M.; Patel, S.M.; El Sahly, H.M.; Ronca, S.E.; Murray, K.O. Optimizing PCR Detection of Zika Virus from Various Body Fluids. Am. J. Trop. Med. Hyg. 2019, 100, 427–433. [Google Scholar] [CrossRef] [PubMed]
- Lanciotti, R.S.; Kosoy, O.L.; Laven, J.J.; Velez, J.O.; Lambert, A.J.; Johnson, A.J.; Stanfield, S.M.; Duffy, M.R. Genetic and Serologic Properties of Zika Virus Associated with an Epidemic, Yap State, Micronesia, 2007. Emerg. Infect. Dis. 2008, 14, 1232–1239. [Google Scholar] [CrossRef] [PubMed]
- Gorchakov, R.; Gulas-Wroblewski, B.E.; Ronca, S.E.; Ruff, J.C.; Nolan, M.S.; Berry, R.; Alvarado, R.E.; Gunter, S.M.; Murray, K.O. Optimizing PCR Detection of West Nile Virus from Body Fluid Specimens to Delineate Natural History in an Infected Human Cohort. Int. J. Mol. Sci. 2019, 20, 1934. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lanciotti, R.S.; Kosoy, O.L.; Laven, J.J.; Panella, A.J.; Velez, J.O.; Lambert, A.J.; Campbell, G.L. Chikungunya Virus in US Travelers Returning from India, 2006. Emerg. Infect. Dis. 2007, 13, 764–767. [Google Scholar] [CrossRef] [PubMed]
- Gurukumar, K.; Priyadarshini, D.; Patil, J.; Bhagat, A.; Singh, A.; Shah, P.; Cecilia, D. Development of Real Time PCR for Detection and Quantitation of Dengue Viruses. Virol. J. 2009, 6, 10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mun, M.-J.; Bae, J.-Y.; Kim, J.H.; Kim, S.B.; Lee, I.; Kim, J.I.; Park, M.S.; Park, M.-S.; Nam, Y.S. One-Step Multiplex Real-Time RT-PCR for Detection and Typing of Dengue Virus. Mol. Cell. Probes 2019, 43, 86–91. [Google Scholar] [CrossRef] [PubMed]
- Stata; StataCorp LLC: College Station, TX, USA, 2020.
- ArcGIS Desktop; Esri Inc.: Redlands, CA, USA, 2020.
- Meerman, J.; Clabaugh, J. Biodiversity and Environmental Resource Data System of Belize. Available online: http://www.biodiversity.bz/ (accessed on 28 February 2021).
- Statistical Institute of Belize. Postcensal Estimates by Administrative Area and Sex, 2010–2020. Available online: http://sib.org.bz/statistics/population/ (accessed on 18 February 2021).
- Pan American Health Organization; World Health Organization. Dengue serotypes by Year for Countries and Territories of the Americas. Available online: https://www.paho.org/data/index.php/en/mnu-topics/indicadores-dengue-en/dengue-nacional-en/517-dengue-serotypes-en.html?start=1 (accessed on 24 January 2021).
- Guo, C.; Zhou, Z.; Wen, Z.; Liu, Y.; Zeng, C.; Xiao, D.; Ou, M.; Han, Y.; Huang, S.; Liu, D.; et al. Global Epidemiology of Dengue Outbreaks in 1990–2015: A Systematic Review and Meta-Analysis. Front. Cell. Infect. Microbiol. 2017, 7, 317. [Google Scholar] [CrossRef]
- Pan American Health Organization; World Health Organization. PAHO Warns of the Complex Situation of Dengue in Latin America and the Caribbean. Available online: https://www.paho.org/hq/index.php?option=com_content&view=article&id=15365:paho-warns-of-the-complex-situation-of-dengue-in-latin-america-and-the-caribbean&Itemid=135&lang=en (accessed on 6 March 2021).
- Dhanoa, A.; Hassan, S.S.; Ngim, C.F.; Lau, C.F.; Chan, T.S.; Adnan, N.A.A.; Eng, W.W.H.; Gan, H.M.; Rajasekaram, G. Impact of Dengue Virus (DENV) Co-Infection on Clinical Manifestations, Disease Severity and Laboratory Parameters. BMC Infect. Dis. 2016, 16, 406. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Senaratne, U.T.N.; Murugananthan, K.; Sirisena, P.D.N.N.; Carr, J.M.; Noordeen, F. Dengue Virus Co-Infections with Multiple Serotypes Do Not Result in a Different Clinical Outcome Compared to Mono-Infections. Epidemiol. Infect. 2020, 148, e119. [Google Scholar] [CrossRef] [PubMed]
- Afreen, N.; Naqvi, I.H.; Broor, S.; Ahmed, A.; Parveen, S. Phylogenetic and Molecular Clock Analysis of Dengue Serotype 1 and 3 from New Delhi, India. PLoS ONE 2015, 10, e0141628. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Beaty, B.J.; Farfán, J.A.; Rosado-Paredes, E.P.; Loroño-Pino, M.A.; Flores-Flores, L.F.; Vorndam, A.V.; Gubler, D.J.; Cropp, C.B.; Rodríguez-Angulo, E.M. Common Occurrence of Concurrent Infections by Multiple Dengue Virus Serotypes. Am. J. Trop. Med. Hyg. 1999, 61, 725–730. [Google Scholar] [CrossRef] [Green Version]
- Savargaonkar, D.; Sinha, S.; Srivastava, B.; Nagpal, B.N.; Sinha, A.; Shamim, A.; Das, R.; Pande, V.; Anvikar, A.R.; Valecha, N. An Epidemiological Study of Dengue and Its Coinfections in Delhi. Int. J. Infect. Dis. 2018, 74, 41–46. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- VinodKumar, C.S.; Kalapannavar, N.K.; Basavarajappa, K.G.; Sanjay, D.; Gowli, C.; Nadig, N.G.; Prasad, B.S. Episode of Coexisting Infections with Multiple Dengue Virus Serotypes in Central Karnataka, India. J. Infect. Public Health 2013, 6, 302–306. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Centers for Disease Control and Prevention. Dengue and Dengue Hemorrhagic Fever. Available online: https://www.cdc.gov/dengue/resources/denguedhf-information-for-health-care-practitioners_2009.pdf (accessed on 7 March 2021).
- Belize Tourism Board. Travel & Tourism Statistics Digest. Available online: https://infogram.com/overnight-tourist-arrivals-1hdw2j7kjq1x2l0 (accessed on 24 January 2021).
- Wilke, A.B.B.; Chase, C.; Vasquez, C.; Carvajal, A.; Medina, J.; Petrie, W.D.; Beier, J.C. Urbanization Creates Diverse Aquatic Habitats for Immature Mosquitoes in Urban Areas. Sci. Rep 2019, 9, 15335. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, Y.; Kamara, F.; Zhou, G.; Puthiyakunnon, S.; Li, C.; Liu, Y.; Zhou, Y.; Yao, L.; Yan, G.; Chen, X.-G. Urbanization Increases Aedes Albopictus Larval Habitats and Accelerates Mosquito Development and Survivorship. PLoS Negl. Trop. Dis. 2014, 8, e3301. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- San Martín, J.L.; Brathwaite, O.; Zambrano, B.; Solórzano, J.O.; Bouckenooghe, A.; Dayan, G.H.; Guzmán, M.G. The Epidemiology of Dengue in the Americas Over the Last Three Decades: A Worrisome Reality. Am. J. Trop. Med. Hyg. 2010, 82, 128–135. [Google Scholar] [CrossRef] [PubMed]
- Pan American Health Organization; World Health Organization. Suspected Dengue Cases. Available online: https://www.paho.org/data/index.php/en/mnu-topics/indicadores-dengue-en/dengue-nacional-en/252-dengue-pais-ano-en.html?start=2 (accessed on 24 February 2021).
- UN Resident Coordinator’s Office for Belize; UN Emergency Technical Team; UN Office for the Coordination of Humanitarian Affairs. Belize: Hurricane Nana Flash Update No. 01, As of 03 September 2020-Belize. Available online: https://reliefweb.int/report/belize/belize-hurricane-nana-flash-update-no-01-03-september-2020 (accessed on 24 February 2021).
- UN Resident Coordinator’s Office for Belize; UN Emergency Technical Team; UN Office for the Coordination of Humanitarian Affairs. Belize: Hurricane Iota Flash Update No. 01, As of 24 November 2020-Belize. Available online: https://reliefweb.int/report/belize/belize-hurricane-iota-flash-update-no-01-24-november-2020 (accessed on 24 February 2021).
- UN Resident Coordinator’s Office for Belize; UN Emergency Technical Team; UN Office for the Coordination of Humanitarian Affairs. Belize: Hurricane Eta Flash Update No. 01, As of 10 November 2020-Belize. Available online: https://reliefweb.int/report/belize/belize-hurricane-eta-flash-update-no-01-10-november-2020 (accessed on 24 February 2021).
- Government of Belize. Ministry of Health Announces First Case of COVID-19. Available online: https://www.pressoffice.gov.bz/ministry-of-health-announces-first-case-of-covid-19/ (accessed on 24 February 2021).
- Overseas Security Advisory Council. Health Alert: Belize, State of Emergency for Next 30 Days. Available online: https://www.osac.gov/Content/Report/d7e46f05-2bae-4b28-acf1-1854f537c53e (accessed on 24 February 2021).



{kind=link}
{kind=link}
| Variable | Total | DENV-Positive | DENV-Negative |
|---|---|---|---|
| n = 894 | n = 44 | n = 850 | |
| n (%) | n (%) | n (%) | |
| Age | |||
| Median age, year (IQR) | 27 (33) | 21 (22) | 27 (34) |
| Under 15 years | 277 (31) | 15 (34) | 262 (31) |
| 15–29 | 224 (25) | 13 (30) | 211 (25) |
| 30–44 | 196 (22) | 10 (23) | 186 (22) |
| 45–59 | 118 (13) | 4 (9) | 114 (13) |
| 60 or older | 74 (8) | 2 (5) | 72 (8) |
| Sex | |||
| Male | 421 (47) | 22 (50) | 399 (47) |
| Female | 473 (53) | 22 (50) | 451 (53) |
| Indoor Occupations | |||
| Professional, technical, managerial | 166 (19) | 5 (11) | 161 (19) |
| Clerical support | 6 (1) | 0 (0) | 6 (1) |
| Domestic services | 51 (6) | 6 (14) | 45 (5) |
| Sales and services | 74 (8) | 4 (9) | 70 (8) |
| Student | 163 (18) | 17 (39) | 146 (17) |
| Unemployed | 107 (12) | 3 (7) | 104 (12) |
| Under school-age children | 156 (17) | 3 (7) | 153 (18) |
| Outdoor Occupations | |||
| Agriculture, forestry, fishery | 26 (3) | 0 (0) | 26 (3) |
| Armed forces | 21 (2) | 0 (0) | 21 (2) |
| Skilled manual | 29 (3) | 1 (2) | 28 (3) |
| Unskilled manual | 28 (3) | 3 (7) | 25 (3) |
| Race | |||
| Black | 215 (24) | 10 (23) | 205 (24) |
| American Indian/Ketchi/Mopan/Mayan | 130 (15) | 1 (2) | 129 (15) |
| White | 92 (10) | 2 (5) | 90 (11) |
| Asian | 36 (4) | 0 (0) | 36 (4) |
| More than one race | 253 (28) | 12 (27) | 241 (28) |
| Unknown | 168 (19) | 19 (43) | 149 (18) |
| Ethnicity | |||
| Not Hispanic or Latino | 389 (44) | 11 (25) | 378 (44) |
| Hispanic or Latino | 338 (38) | 14 (32) | 324 (38) |
| Unknown | 167 (19) | 19 (43) | 148 (17) |
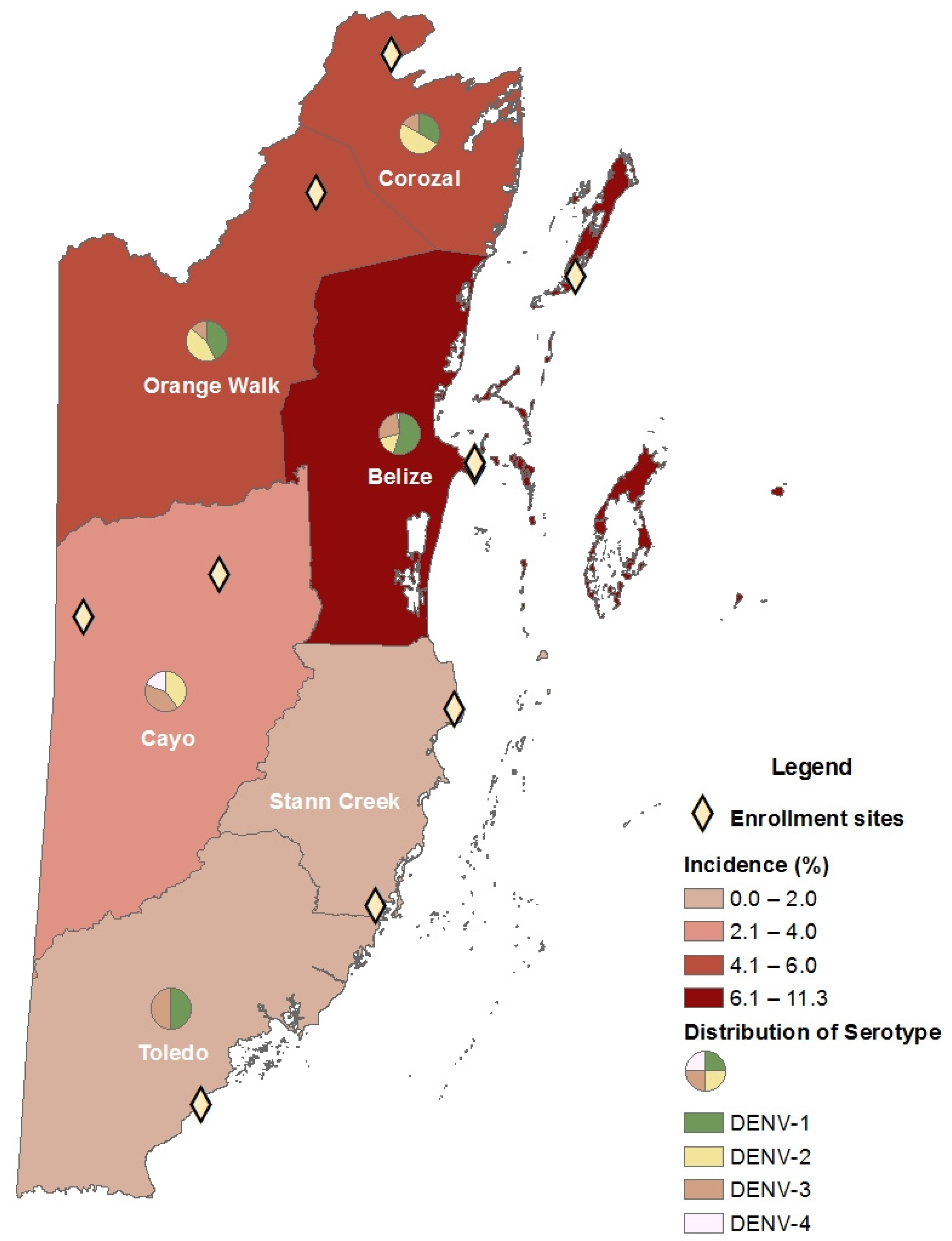
| Clinical Site in North Belize | |||
| Belize | 257 (29) | 29 (66) | 228 (27) |
| Corozal | 67 (7) | 4 (9) | 63 (7) |
| Orange Walk | 107 (12) | 6 (14) | 101(12) |
| Clinical Site in South Belize | |||
| Cayo | 134 (15) | 4 (9) | 130 (15) |
| Stann Creek | 134 (15) | 0 (0) | 134 (16) |
| Toledo | 195 (22) | 1 (2) | 194 (23) |
| DENV mono-infection | |||
| DENV-1 | - | 13 (30) | - |
| DENV-2 | - | 13 (30) | - |
| DENV-3 | - | 1 (2) | - |
| DENV-4 | - | 0 (0) | - |
| DENV co-infections | |||
| DENV-1/ DENV-2 | - | 2 (5) | - |
| DENV-1/DENV-3 | - | 13 (30) | - |
| DENV-1/DENV-3/DENV-4 | - | 1 (2) | - |
| DENV-3/DENV-4 | - | 1 (2) | - |
| Variable | DENV-Positive n = 44 n (%) | DENV-Negative n = 850 n (%) | Odds Ratio (95% CI) | p-Value * |
|---|---|---|---|---|
| Contact with mosquito 1 | 34 (77) | 442 (52) | 3.1 (1.5, 6.4) | 0.002 |
| Contact with sick individuals 1 | 10 (23) | 119 (14) | 1.9 (0.9, 3.9) | 0.10 |
| Travel history 2 | 6 (14) | 95 (11) | 1.2 (0.5, 3.0) | 0.64 |
| Outdoor occupation † | 4 (9) | 99 (12) | 0.7 (0.2, 2.1) | 0.81 |
| Student | 17 (39) | 146 (17) | 3.0 (1.6, 5.7) | 0.001 |
| Twenty years or older | 22 (50) | 533 (63) | 0.6 (0.3, 1.1) | 0.08 |
| Female sex | 22 (50) | 451 (53) | 0.9 (0.5, 1.6) | 0.70 |
| Black race | 10 (23) | 205 (24) | 1.6 (0.7, 3.6) | 0.25 |
| Hispanic or Latino | 14 (32) | 324 (38) | 1.5 (0.7, 3.3) | 0.34 |
| Clinical site in northern region † | 39 (89) | 392 (46) | 9.1 (3.5, 29.9) | <0.001 |
| Variable | Odds Ratio (95% CI) | p-Value |
|---|---|---|
| Contact with mosquito 1 | 2.8 (1.3, 5.7) | 0.007 |
| Clinical site in northern region | 8.3 (3.2, 21.5) | <0.001 |
| Student | 2.3 (1.2, 4.4) | 0.015 |
| District | Total Enrolled | Total DENV Positive | Cohort Incidence (%) | Belize Population 2020 [23] | Population Incidence (per 100,000) |
|---|---|---|---|---|---|
| Corozal | 67 | 4 | 6.0 | 50,490 | 7.9 |
| Orange Walk | 107 | 6 | 5.6 | 53,373 | 11.2 |
| Belize | 257 | 29 | 11.3 | 127,683 | 22.7 |
| Cayo | 134 | 4 | 3.0 | 102,115 | 3.9 |
| Stann Creek | 134 | 0 | 0 | 46,015 | 0 |
| Toledo | 195 | 1 | 0.5 | 39,525 | 2.5 |
| Sign/Symptom | DENV- Positive n = 44 n (%) | DENV-Negative n = 850 n (%) | OR (95% CI) | p Value * | DENV-1 n = 29 n (%) | DENV-2 n = 15 n (%) | DENV-3 n = 16 n (%) | DENV-4 n = 2 n (%) |
|---|---|---|---|---|---|---|---|---|
| General | ||||||||
| Fever † | 43 (98) | 718 (84) | 7.9 (1.3, 321.7) | 0.01 | 29 (100) | 14 (93) | 16 (100) | 2 (100) |
| Rash † | 3 (7) | 27 (3) | 2.2 (0.4, 7.7) | 0.18 | 2 (7) | 1 (7) | 1 (6) | 0 (0) |
| Conjunctivitis † | 2 (5) | 9 (1) | 4.4 (0.5, 22.4) | 0.10 | 1 (3) | 1 (7) | 0 (0) | 0 (0) |
| Arthralgia | 14 (32) | 119 (14) | 2.9 (1.5, 5.6) | 0.002 | 7 (24) | 8 (53) | 4 (25) | 1 (50) |
| Headache | 26 (59) | 339 (40) | 2.2 (1.2, 4.0) | 0.01 | 15 (52) | 12 (80) | 7 (44) | 2 (100) |
| Retroorbital pain | 15 (34) | 64 (8) | 6.4 (3.2, 12.5) | <0.001 | 11 (38) | 6 (40) | 5 (31) | 1 (50) |
| Muscle pain/aches | 16 (36) | 141 (17) | 2.9 (1.5, 5.5) | 0.001 | 8 (28) | 7 (47) | 6 (38) | 2 (100) |
| Chills | 19 (43) | 139 (16) | 3.9 (2.1, 7.3) | <0.001 | 11 (38) | 8 (53) | 7 (44) | 2 (100) |
| Jaundice † | 1 (2) | 4 (0.5) | 4.9 (0.1, 50.9) | 0.22 | 1 (3) | 0 (0) | 0 (0) | 0 (0) |
| Night or unusual sweats † | 4 (9) | 26 (3) | 3.2 (0.8, 9.8) | 0.05 | 4 (14) | 2 (13) | 0 (0) | 0 (0) |
| Dysuria † | 3 (7) | 8 (1) | 7.7 (1.3, 33.5) | 0.01 | 3 (10) | 0 (0) | 0 (0) | 0 (0) |
| Loss of appetite † | 3 (7) | 4 (0.5) | 15.5 (2.2, 93.9) | 0.003 | 2 (7) | 1 (7) | 0 (0) | 0 (0) |
| Fatigue † | 2 (5) | 10 (1) | 4.0 (0.4, 19.6) | 0.11 | 2 (7) | 0 (0) | 0 (0) | 0 (0) |
| Respiratory | ||||||||
| Cough | 17 (39) | 472 (56) | 0.5 (0.3, 0.9) | 0.03 | 9 (31) | 6 (40) | 6 (38) | 2 (100) |
| Sore throat | 11 (25) | 279 (33) | 0.7 (0.3, 1.4) | 0.28 | 6 (21) | 4 (27) | 4 (25) | 1 (50) |
| Wheezing † | 1 (2) | 42 (5) | 0.4 (0, 2.8) | 0.72 | 1 (3) | 0 (0) | 0 (0) | 0 (0) |
| Chest pain † | 2 (5) | 95 (11) | 0.4 (0, 1.5) | 0.22 | 2 (7) | 0 (0) | 1 (6) | 1 (50) |
| Sneezing † | 2 (5) | 150 (18) | 0.2 (0, 0.9) | 0.02 | 2 (7) | 0 (0) | 1 (6) | 0 (0) |
| Difficulty breathing | 7 (16) | 174 (20) | 0.7 (0.3, 1.7) | 0.46 | 4 (14) | 1 (7) | 2 (13) | 1 (50) |
| Coryza/congestion/rhinorrhea | 10 (23) | 309 (36) | 0.5 (0.3, 1.1) | 0.07 | 8 (28) | 1 (7) | 6 (38) | 2 (100) |
| Gastrointestinal | ||||||||
| Diarrhea | 8 (18) | 164 (19) | 0.9 (0.4, 2.0) | 0.86 | 6 (21) | 2 (13) | 3 (19) | 1 (50) |
| Nausea | 8 (18) | 117 (14) | 1.4 (0.6, 3.1) | 0.41 | 6 (21) | 2 (13) | 2 (13) | 1 (50) |
| Vomiting | 10 (23) | 156 (18) | 1.3 (0.6, 2.7) | 0.47 | 8 (28) | 2 (13) | 4 (25) | 1 (50) |
| Abdominal/stomach pain | 7 (16) | 126 (15) | 1.1 (0.5, 2.5) | 0.84 | 6 (21) | 1 (7) | 2 (13) | 1 (50) |
| Upset stomach † | 5 (11) | 40 (5) | 2.6 (0.8, 7.1) | 0.06 | 3 (10) | 2 (13) | 1 (6) | 1 (50) |
| Clinical Outcome | DENV Positive n = 44 n (%) | DENV-1 n = 29 n (%) | DENV-2 n = 15 n (%) | DENV-3 n = 15 n (%) | DENV-4 n = 2 n (%) | Monoinfection n = 27 n (%) | Coinfection n = 17 n (%) |
|---|---|---|---|---|---|---|---|
| Elevated hematocrit (male > 54%, female > 48%) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) |
| Thrombocytopenia (platelets < 150 × 103/μL) | 10 (23) | 5 (17) | 5 (33) | 2 (13) | 0 (0) | 8 (30) | 2 (12) |
| Leukopenia (<5000/μL) | 10 (23) | 5 (17) | 5 (33) | 2 (13) | 0 (0) | 8 (30) | 2 (12) |
| Leukocytosis (>10,000/μL) | 1 (2) | 1 (4) | 0 (0) | 1 (6) | 1 (50) | 0 (0) | 1 (6) |
| Elevated AST (>40 U/L) | 4 (9) | 1 (4) | 3 (20) | 0 (0) | 0 (0) | 4 (15) | 0 (0) |
| Elevated ALT (>40 U/L) | 3 (7) | 1 (4) | 2 (13) | 0 (0) | 0 (0) | 3 (11) | 0 (0) |
| Hospital admission | 2 (5) | 0 (0) | 2 (13) | 0 (0) | 0 (0) | 2 (7) | 0 (0) |
| Death Met WHO suggested case definition † | 0 (0) 25 (57) | 0 (0) 15 (52) | 0 (0) 11 (73) | 0 (0) 8 (53) | 0 (0) 2 (100) | 0 (0) 15 (56) | 0 (0) 10 (59) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ly, A.N.; Manzanero, R.; Maliga, A.; Gunter, S.M.; Ronca, S.E.; Zielinski-Gutierrez, E.; Morey, F.; Bautista, K.; Espinosa-Bode, A.; López, B.; et al. Epidemiological and Clinical Characteristics of Acute Dengue Virus Infections Detected through Acute Febrile Illness Surveillance, Belize 2020. Viruses 2022, 14, 768. https://doi.org/10.3390/v14040768
Ly AN, Manzanero R, Maliga A, Gunter SM, Ronca SE, Zielinski-Gutierrez E, Morey F, Bautista K, Espinosa-Bode A, López B, et al. Epidemiological and Clinical Characteristics of Acute Dengue Virus Infections Detected through Acute Febrile Illness Surveillance, Belize 2020. Viruses. 2022; 14(4):768. https://doi.org/10.3390/v14040768
Chicago/Turabian StyleLy, Anh N., Russell Manzanero, Adrianna Maliga, Sarah M. Gunter, Shannon E. Ronca, Emily Zielinski-Gutierrez, Francis Morey, Kim Bautista, Andres Espinosa-Bode, Beatriz López, and et al. 2022. "Epidemiological and Clinical Characteristics of Acute Dengue Virus Infections Detected through Acute Febrile Illness Surveillance, Belize 2020" Viruses 14, no. 4: 768. https://doi.org/10.3390/v14040768