
Early Childhood Growth Parameters in South African Children with Exposure to Maternal HIV Infection and Placental Insufficiency

 , ,
, ,  , ,
, , 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Settings and Participants
2.2. Study Design
2.3. Sample Size Determination
2.4. Data Collection Methods
2.5. Data Processing and Statistical Analysis
2.6. Ethical Considerations
3. Results
3.1. The Socio-Demographic and Medical Characteristics of the Mothers of the Study Children
3.2. The Characteristics of the Study Children
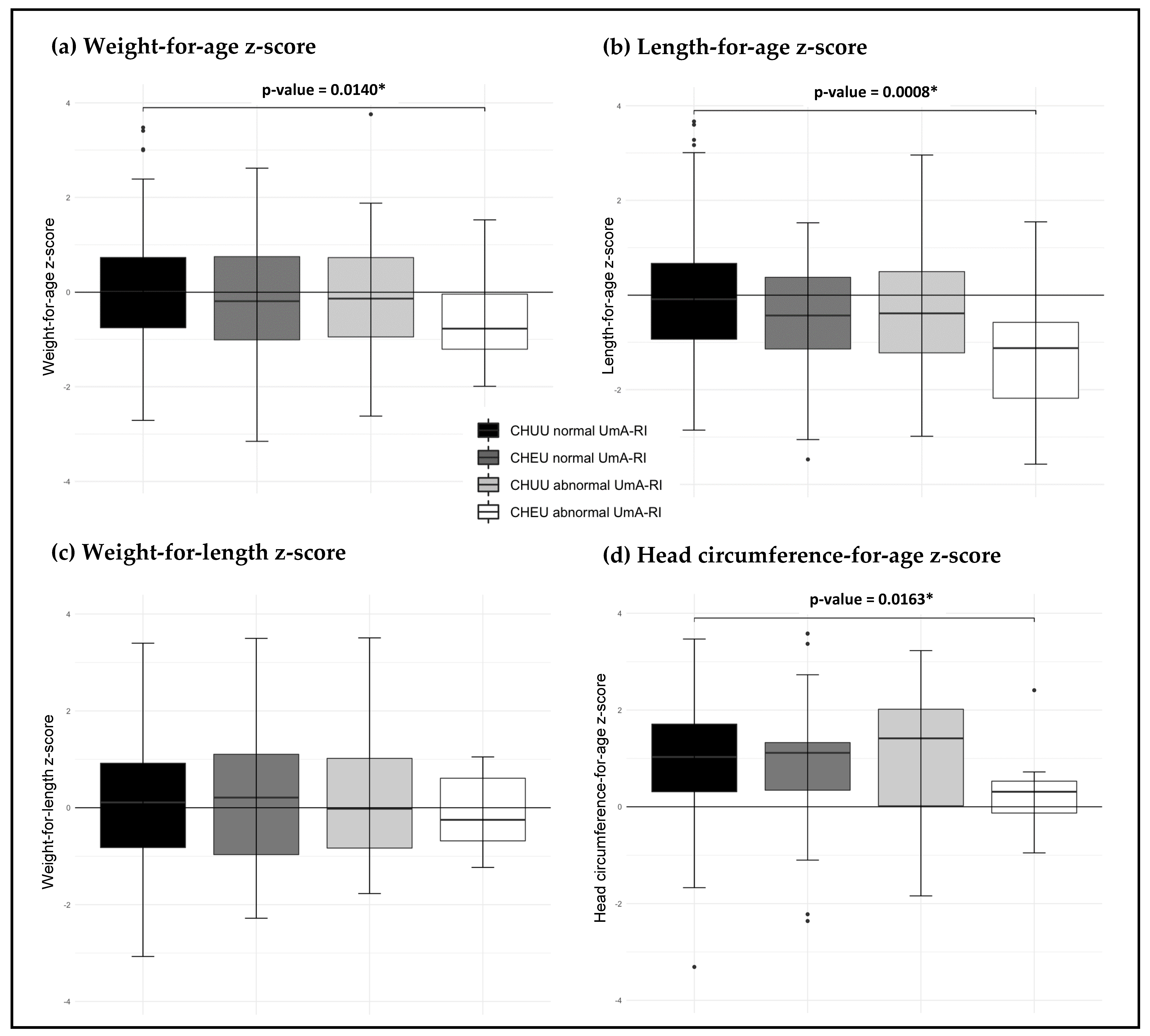
3.3. Growth Parameters of Study Children
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Clouse, K.; Malope-Kgokong, B.; Bor, J.; Nattey, C.; Mudau, M.; Maskew, M. The South African National HIV Pregnancy Cohort: Evaluating continuity of care among women living with HIV. BMC Public Health 2020, 20, 1–11. [Google Scholar] [CrossRef] [PubMed]
- South African National AIDS Council (SANAC). Let our actions count: National Strategic Plan on HIV, TB and STIs (2017–2022) 2018. Available online: https://sanac.org.za/wpcontent/uploads/2018/09/NSP_FullDocument_FINAL.pdf (accessed on 14 May 2021).
- Conroy, A.; McDonald, C.R.; Gamble, J.L.; Olwoch, P.; Natureeba, P.; Cohan, D.; Kamya, M.R.; Havlir, D.V.; Dorsey, G.; Kain, K.C. Altered angiogenesis as a common mechanism underlying preterm birth, small for gestational age, and stillbirth in women living with HIV. Am. J. Obstet. Gynecol. 2017, 217, 684.e1–684.e17. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Canlorbe, G.; Matheron, S.; Mandelbrot, L.; Oudet, B.; Luton, D.; Azria, E. Vasculoplacental complications in pregnant women with HIV infection: A case-control study. Am. J. Obstet. Gynecol. 2015, 213, 241.e1–241.e9. [Google Scholar] [CrossRef] [PubMed]
- Ndirangu, J.; Newell, M.-L.; Bland, R.M.; Thorne, C. Maternal HIV infection associated with small-for-gestational age infants but not preterm births: Evidence from rural South Africa. Hum. Reprod. 2012, 27, 1846–1856. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Weckman, A.M.; Ngai, M.; Wright, J.; McDonald, C.R.; Kain, K.C. The Impact of Infection in Pregnancy on Placental Vascular Development and Adverse Birth Outcomes. Front. Microbiol. 2019, 10, 1924. [Google Scholar] [CrossRef] [Green Version]
- Flores-Guillén, E.; Ochoa-Díaz-López, H.; Castro-Quezada, I.; Irecta-Nájera, C.A.; Cruz, M.; Meneses, M.E.; Gurri, F.D.; Solís-Hernández, R.; García-Miranda, R. Intrauterine growth restriction and overweight, obesity, and stunting in adolescents of indigenous communities of Chiapas, Mexico. Eur. J. Clin. Nutr. 2019, 74, 149–157. [Google Scholar] [CrossRef]
- Burton, G.J.; Jauniaux, E. Pathophysiology of placental-derived fetal growth restriction. Am. J. Obstet. Gynecol. 2018, 218, S745–S761. [Google Scholar] [CrossRef] [Green Version]
- Ramokolo, V.; Lombard, C.; Fadnes, L.T.; Doherty, T.; Jackson, D.J.; Goga, A.E.; Chhagan, M.; Broeck, J.V.D. HIV Infection, Viral Load, Low Birth Weight, and Nevirapine Are Independent Influences on Growth Velocity in HIV-Exposed South African Infants. J. Nutr. 2013, 144, 42–48. [Google Scholar] [CrossRef] [Green Version]
- Slogrove, A.; Cotton, M.F.; Esser, M.M. Severe Infections in HIV-Exposed Uninfected Infants: Clinical Evidence of Immunodeficiency. J. Trop. Pediatr. 2009, 56, 75–81. [Google Scholar] [CrossRef] [Green Version]
- Evans, C.; Jones, C.E.; Prendergast, A.J. HIV-exposed, uninfected infants: New global challenges in the era of paediatric HIV elimination. Lancet Infect. Dis. 2016, 16, e92–e107. [Google Scholar] [CrossRef]
- Wedderburn, C.J.; Evans, C.; Yeung, S.; Gibb, D.M.; Donald, K.A.; Prendergast, A.J. Growth and Neurodevelopment of HIV-Exposed Uninfected Children: A Conceptual Framework. Curr. HIV/AIDS Rep. 2019, 16, 501–513. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jumare, J.; Datong, P.; Osawe, S.; Okolo, F.; Mohammed, S.; Inyang, B.; Abimiku, A. Compromised Growth Among HIV-exposed Uninfected Compared with Unexposed Children in Nigeria. Pediatr. Infect. Dis. J. 2019, 38, 280–286. [Google Scholar] [CrossRef] [PubMed]
- Neary, J.; Langat, A.; Singa, B.; Kinuthia, J.; Itindi, J.; Nyaboe, E.; Ng’Anga’, L.W.; Katana, A.; John-Stewart, G.C.; McGrath, C.J. Higher prevalence of stunting and poor growth outcomes in HIV-exposed uninfected than HIV-unexposed infants in Kenya. AIDS 2021, 36, 605–610. [Google Scholar] [CrossRef]
- Black, R.; Victora, C.; Walker, S.P.; Bhutta, Z.A.; Christian, P.; de Onis, M.; Ezzati, M.; Grantham-McGregor, S.; Katz, J.; Martorell, R.; et al. Maternal and child undernutrition and overweight in low-income and middle-income countries. Lancet 2013, 382, 427–451. [Google Scholar] [CrossRef] [PubMed]
- Wardinger, J.E.; Ambati, S. Placental Insufficiency. StatPearls [Internet]. 2021. Available online: https://www.ncbi.nlm.nih.gov/books/NBK563171/ (accessed on 21 February 2022).
- Audette, M.C.; Kingdom, J.C. Screening for fetal growth restriction and placental insufficiency. Semin. Fetal Neonatal Med. 2018, 23, 119–125. [Google Scholar] [CrossRef] [PubMed]
- Flenady, V.; Wojcieszek, A.; Ellwood, D.; Leisher, S.H.; Erwich, J.J.H.; Draper, E.; McClure, E.M.; Reinebrant, H.; Oats, J.; McCowan, L.; et al. Classification of causes and associated conditions for stillbirths and neonatal deaths. Semin. Fetal Neonatal Med. 2017, 22, 176–185. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Saleem, T.; Sajjad, N.; Fatima, S.; Habib, N.; Ali, S.R.; Qadir, M. Intrauterine growth retardation - small events, big consequences. Ital. J. Pediatr. 2011, 37, 41–44. [Google Scholar] [CrossRef] [Green Version]
- Lawn, J.E.; Blencowe, H.M.; Waiswa, P.; Amouzou, A.; Mathers, C.; Hogan, D.; Flenady, V.; Frøen, J.F.; Qureshi, Z.U.; Calderwood, C.; et al. Stillbirths: Rates, risk factors, and acceleration towards 2030. Lancet 2016, 387, 587–603. [Google Scholar] [CrossRef] [Green Version]
- Sania, A.; Spiegelman, D.; Rich-Edwards, J.; Okuma, J.; Kisenge, R.; Msamanga, G.; Urassa, W.; Fawzi, W.W. The Contribution of Preterm Birth and Intrauterine Growth Restriction to Infant Mortality in Tanzania. Paediatr. Périnat. Epidemiol. 2013, 28, 23–31. [Google Scholar] [CrossRef]
- Kesavan, K.; Devaskar, S.U. Intrauterine Growth Restriction: Postnatal Monitoring and Outcomes. Pediatr. Clin. N. Am. 2019, 66, 403–423. [Google Scholar] [CrossRef]
- Theron, G.B.; Theron, A.M.; Odendaal, H.J.; Bunn, A.E. Comparison between a newly developed PC-based Doppler umbilical artery waveform analyser and a commercial unit. S. Afr. Med. J. 2005, 95, 62–64. [Google Scholar]
- Nkosi, S.; Makin, J.; Hlongwane, T.; Pattinson, R.C. Screening and managing a low-risk pregnant population using continu-ous-wave Doppler ultrasound in a low-income population: A cohort analytical study. S. Afr. Med. J. 2019, 109, 347–352. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hlongwane, T.; Cronje, T.; Nkosi, B.; Pattinson, R. The prevalence of abnormal Doppler’s of the umbilical artery in a low-risk pregnant population in South Africa. eClinicalMedicine 2021, 34, 100792. [Google Scholar] [CrossRef] [PubMed]
- Vannevel, V.; Vogel, J.P.; Pattinson, R.C.; Adanu, R.; Charantimath, U.; Goudar, S.S.; Gwako, G.; Kavi, A.; Maya, E.; Osoti, A.; et al. Antenatal Doppler screening for fetuses at risk of adverse outcomes: A multicountry cohort study of the prevalence of abnormal resistance index in low-risk pregnant women. BMJ Open 2022, 12, e053622. [Google Scholar] [CrossRef]
- Prado, E.L.; Dewey, K.G. Nutrition and brain development in early life. Nutr. Rev. 2014, 72, 267–284. [Google Scholar] [CrossRef] [Green Version]
- Pattinson, R.C.; Theron, G.B.; Thompson, M.L.; Tung, M.L. Doppler ultrasonography of the fetoplacental circulation—Normal reference values. S. Afr. Med. J. 1989, 76, 623–625. [Google Scholar]
- Stomfai, S.; Ahrens, W.; Bammann, K.; Kovacs, E.; Mårild, S.; Michels, N.; Moreno, L.A.; Pohlabeln, H.; Siani, A.; Tornaritis, M.; et al. Intra- and inter-observer reliability in anthropometric measurements in children. Int. J. Obes. 2011, 35, S45–S51. [Google Scholar] [CrossRef] [Green Version]
- Nieman, C.D. Nutritional Assessment, 7th ed.; 2 Penn Plaza, McGraw-Hill: New Your, NY, USA, 2019. [Google Scholar]
- Patridge, E.F.; Bardyn, T.P. Research Electronic Data Capture (REDCap). J. Med. Libr. Assoc. 2018, 106, 142–144. [Google Scholar] [CrossRef] [Green Version]
- le Roux, S.M.; Abrams, E.J.; Donald, K.A.; Brittain, K.; Phillips, T.K.; Nguyen, K.K.; Zerbe, A.; Kroon, M.; Myer, L. Growth trajectories of breastfed HIV-exposed uninfected and HIV-unexposed children under conditions of universal maternal antiretroviral therapy: A prospective study. Lancet Child Adolesc. Health 2019, 3, 234–244. [Google Scholar] [CrossRef]
- Nyemba, D.C.; Kalk, E.; Vinikoor, M.J.; Madlala, H.P.; Mubiana-Mbewe, M.; Mzumara, M.; Moore, C.B.; Slogrove, A.L.; Boulle, A.; Davies, M.-A.; et al. Growth patterns of infants with in- utero HIV and ARV exposure in Cape Town, South Africa and Lusaka, Zambia. BMC Public Health 2022, 22, 1–14. [Google Scholar] [CrossRef]
- Fowler, M.G.; Aizire, J.; Sikorskii, A.; Atuhaire, P.; Ogwang, L.W.; Mutebe, A.; Katumbi, C.; Maliwichi, L.; Familiar, I.; Taha, T.; et al. Growth deficits in antiretroviral and HIV-exposed uninfected versus unexposed children in Malawi and Uganda persist through 60 months of age. AIDS 2021, 36, 573–582. [Google Scholar] [CrossRef] [PubMed]
- Aizire, J.; Sikorskii, A.; Ogwang, L.W.; Kawalazira, R.; Mutebe, A.; Familiar-Lopez, I.; Mallewa, M.; Taha, T.; Boivin, M.J.; Fowler, M.G. Decreased growth among antiretroviral drug and HIV-exposed uninfected versus unexposed children in Malawi and Uganda. AIDS 2020, 34, 215–225. [Google Scholar] [CrossRef]
- Sirajee, R.; Conroy, A.L.; Namasopo, S.; Opoka, R.O.; Lavoie, S.; Forgie, S.; Salami, B.O.; Hawkes, M.T. Growth Faltering and Developmental Delay in HIV-Exposed Uninfected Ugandan Infants: A Prospective Cohort Study. J. Acquir. Immune Defic. Syndr. 2021, 87, 730–740. [Google Scholar] [CrossRef] [PubMed]
- Gagnon, R. Placental insufficiency and its consequences. Eur. J. Obstet. Gynecol. Reprod. Biol. 2003, 110, S99–S107. [Google Scholar] [CrossRef] [PubMed]
- Pintican, D.; Poienar, A.A.; Strilciuc, S.; Mihu, D. Effects of maternal smoking on human placental vascularization: A systematic review. Taiwan. J. Obstet. Gynecol. 2019, 58, 454–459. [Google Scholar] [CrossRef] [PubMed]
- Govender, I.; Steyn, C.; Maphasha, O.; Abdulrazak, A. A profile of Caesarean sections performed at a district hospital in Tshwane, South Africa. S. Afr. Fam. Pract. 2019, 61, 246–251. [Google Scholar] [CrossRef] [Green Version]
- Rossouw, M.E.; Cornell, M.; Cotton, M.F.; Esser, M.M. Feeding practices and nutritional status of HIV-exposed and HIV-unexposed infants in the Western Cape. S. Afr. J. HIV Med. 2016, 17, 9. [Google Scholar] [CrossRef] [Green Version]
- Simbayi, L.; Zuma, K.; Zungu, N.; Moyo, S.; Marinda, E.; Jooste, S.; Mabaso, M.; Ramlagan, S.; North, A.; Van Zyl, J.; et al. South African National HIV Prevalence, Incidence, Behaviour and Communication Survey, 2017: Towards Achieving the UNAIDS 90-90-90 Targets. 2019. Available online: http://hdl.handle.net/20.500.11910/15052 (accessed on 2 May 2021).
- Chandna, J.; Ntozini, R.; Evans, C.; Kandawasvika, G.; Chasekwa, B.; Majo, F.D.; Mutasa, K.; Tavengwa, N.V.; Mutasa, B.; Mbuya, M.N.; et al. Effects of improved complementary feeding and improved water, sanitation and hygiene on early child development among HIV-exposed children: Substudy of a cluster randomised trial in rural Zimbabwe. BMJ Glob. Health 2020, 5, e001718. [Google Scholar] [CrossRef] [Green Version]
- WHO; UNICEF. Guideline: Updates on HIV and Infant Feeding; the Duration of Breastfeeding and Support from Health Services to Improve Feeding Practices among Mothers Living with HIV; World Health Organization: Geneva, Switzerland, 2016. [Google Scholar]
- Lassi, Z.S.; Rind, F.; Irfan, O.; Hadi, R.; Das, J.K.; Bhutta, Z.A. Impact of Infant and Young Child Feeding (IYCF) Nutrition Interventions on Breastfeeding Practices, Growth and Mortality in Low- and Middle-Income Countries: Systematic Review. Nutrients 2020, 12, 722. [Google Scholar] [CrossRef] [Green Version]
- Wallenborn, J.T.; Levine, G.A.; dos Santos, A.C.; Grisi, S.; Brentani, A.; Fink, G. Breastfeeding, Physical Growth, and Cognitive Development. Pediatrics 2021, 147, e2020008029. [Google Scholar] [CrossRef]
- Szanyi, J.; Walles, J.K.; Tesfaye, F.; Gudeta, A.N.; Björkman, P. Intrauterine HIV exposure is associated with linear growth restriction among Ethiopian children in the first 18 months of life. Trop. Med. Int. Health 2022, 27, 823–830. [Google Scholar] [CrossRef] [PubMed]
- Kapito-Tembo, A.P.; Bauleni, A.; Wesevich, A.; Ongubo, D.; Hosseinipour, M.C.; Dube, Q.; Mwale, P.; Corbett, A.; Mwapasa, V.; Phiri, S. Growth and Neurodevelopment Outcomes in HIV-, Tenofovir-, and Efavirenz-Exposed Breastfed Infants in the PMTCT Option B+ Program in Malawi. J. Acquir. Immune Defic. Syndr. 2020, 86, 81–90. [Google Scholar] [CrossRef] [PubMed]
- Blake, R.A.; Park, S.; Baltazar, P.; Ayaso, E.B.; Monterde, D.B.S.; Acosta, L.P.; Olveda, R.M.; Tallo, V.; Friedman, J.F. LBW and SGA Impact Longitudinal Growth and Nutritional Status of Filipino Infants. PLoS ONE 2016, 11, e0159461. [Google Scholar] [CrossRef] [Green Version]
- von Beckerath, A.-K.; Kollmann, M.; Rotky-Fast, C.; Karpf, E.; Lang, U.; Klaritsch, P. Perinatal complications and long-term neurodevelopmental outcome of infants with intrauterine growth restriction. Am. J. Obstet. Gynecol. 2012, 208, 130.e1–130.e6. [Google Scholar] [CrossRef]
- Stranix-Chibanda, L.; Tierney, C.; Pinilla, M.; George, K.; Aizire, J.; Chipoka, G.; Mallewa, M.; Naidoo, M.; Nematadzira, T.; Kusakara, B.; et al. Effect on growth of exposure to maternal antiretroviral therapy in breastmilk versus extended infant nevirapine prophylaxis among HIV-exposed perinatally uninfected infants in the PROMISE randomized trial. PLoS ONE 2021, 16, e0255250. [Google Scholar] [CrossRef] [PubMed]
- Zhang, P.; Wu, J.; Xun, N. Role of Maternal Nutrition in the Health Outcomes of Mothers and Their Children: A Retrospective Analysis. J. Pharmacol. Exp. Ther. 2019, 25, 4430–4437. [Google Scholar] [CrossRef]
- Fall, C.H.D.; Sachdev, H.S.; Osmond, C.; Restrepo-Mendez, M.C.; Victora, C.; Martorell, R.; Stein, A.D.; Sinha, S.; Tandon, N.; Adair, L.; et al. Association between maternal age at childbirth and child and adult outcomes in the offspring: A prospective study in five low-income and middle-income countries (COHORTS collaboration). Lancet Glob. Health 2015, 3, e366–e377. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Variables | CHUU with Normal UmA-RI | CHEU with Normal UmA-RI | CHUU with Abnormal UmA-RI | CHEU with Abnormal UmA-RI | p-Value a | |
|---|---|---|---|---|---|---|
| Sample size (n) (%) | 186 (68.6%) | 50 (18.5%) | 20 (7.4%) | 15 (5.5%) | ||
| Mean age (years) | 30.1 ± 5.1 | 31.3 ± 5.5 | 28.5 ± 4.5 | 36.6 ± 6.1 | <0.001 | |
| Marital status | Single | 79 (42.5%) | 21 (42.0%) | 6 (30.0%) | 4 (26.7%) | n/a |
| Married | 69 (37.1%) | 17 (34.0%) | 10 (50.0%) | 8 (53.3%) | ||
| Co-habiting | 38 (20.4%) | 12 (24.0%) | 4 (20.0%) | 3 (20.0%) | ||
| Educational level | Any primary schooling | 13 (7.0%) | 4 (8.0%) | 3 (15.0%) | 2 (13.3%) | n/a |
| Any secondary schooling | 127 (68.3%) | 40 (80.0%) | 13 (65.0%) | 12 (80.0%) | ||
| Post-school education | 46 (24.7%) | 6 (12.0%) | 4 (20.0%) | 1 (6.7%) | ||
| Employment status | Unemployed | 112 (60.2%) | 29 (58.0%) | 11 (55.0%) | 10 (66.7%) | 0.118 |
| Employed | 74 (39.8%) | 21 (42.0%) | 9 (45.0%) | 5 (33.3%) | ||
| Monthly household income b | R 0–R 2000 | 37 (20.1%) | 7 (14.0%) | 0 (0%) | 4 (26.7%) | n/a |
| R 2001–R 4000 | 43 (23.4%) | 15 (30.0%) | 8 (40.0%) | 0 (0%) | ||
| R 4001–R 6000 | 39 (21.2%) | 13 (26.0%) | 5 (25.0%) | 6 (40.0%) | ||
| R 6001–R 8000 | 11 (6.0%) | 5 (10.0%) | 1 (5.0%) | 2 (13.3%) | ||
| R 8000+ | 45 (24.5%) | 9 (18.0%) | 6 (30.0%) | 1 (6.7%) | ||
| Don’t know | 9 (4.9%) | 1 (2.0%) | 0 (0%) | 2 (13.3%) | ||
| Access to running water | Inside house | 68 (36.6%) | 10 (20.0%) | 7 (35.0%) | 4 (26.7%) | n/a |
| Inside yard | 89 (47.8%) | 27 (54.0%) | 10 (50.0%) | 8 (53.3%) | ||
| Communal tap | 21 (11.3%) | 9 (18.0%) | 3 (15.0%) | 3 (20.0%) | ||
| Water tank | 8 (4.3%) | 4 (8.0%) | 0 (0%) | 0 (0%) | ||
| Access to toilet c | Flushing toilet | 131 (70.4%) | 30 (61.2%) | 16 (80.0%) | 9 (64.3%) | n/a |
| Pit latrine/bucket | 55 (29.6%) | 19 (38.8%) | 4 (20.0%) | 5 (35.7%) | ||
| Drinks alcohol d | Yes | 54 (29.2%) | 11 (22.0%) | 2 (11.1%) | 1 (7.1%) | n/a |
| Smokes cigarettes | Yes | 3 (1.6%) | 2 (4.0%) | 0 (0%) | 1 (6.7%) | n/a |
| Latest CD4 count | Cells/mm3 e | N/A | 463 ± 310 | N/A | 416 ± 295 | 0.147 |
| Latest HIV viral load | Copies/mL (log) f,g | N/A | 0.0 [0.0, 4.0] | N/A | 0.0 [0.0, 0.0] | 0.277 |
| Current ART | TDF/FTC/EFV | N/A | 31 (62.0%) | N/A | 8 (53.3%) | n/a |
| Other ART h | N/A | 10 (20.0%) | N/A | 6 (40.0%) | ||
| Not recorded | N/A | 9 (18.0%) | N/A | 1 (6.7%) | ||
| Obstetric history | Parity f | 2 [1, 3] | 2 [1, 3] | 2 [0, 2] | 3 [3, 3] | 0.006 |
| Gravidity f | 2 [1, 3] | 3 [2, 3] | 2 [2, 3] | 3 [3, 4] | 0.018 | |
| Previous pregnancy losses f | 0 [0, 0] | 0 [0, 1] | 0 [0, 0] | 0 [0, 1] | 0.372 | |
| Preeclampsia/eclampsia | 2 (13.3%) | 0 (0%) | 0 (0%) | 0 (0%) | n/a | |
| Umbilical artery Doppler | UmA-RI value at 28–34 weeks’ gestation g | 0.64 ± 0.05 | 0.63 ± 0.04 | 0.74 ± 0.06 | 0.76 ± 0.04 | <0.001 |
| Mode of delivery | Vaginal delivery | 127 (68.3%) | 31 (62.0%) | 10 (50.0%) | 6 (40.0%) | n/a |
| Assisted delivery | 3 (1.6%) | 0 (0%) | 0 (0%) | 0 (0%) | ||
| Caesarean section | 56 (30.1%) | 19 (38.0%) | 10 (50.0%) | 9 (60.0%) | ||
| Body measurements and indices g,i | Weight (kg) | 77.6 ± 19.6 | 77.5 ± 25.0 | 69.7 ± 20.2 | 63.1 ± 15.4 | 0.016 |
| Height (cm) | 160.2 ± 6.2 | 161.3 ± 8.9 | 157.8 ± 5.3 | 158.3 ± 5.3 | 0.402 | |
| BMI (kg/m2) | 30.3 ± 7.7 | 29.5 ± 8.4 | 27.9 ± 7.4 | 25.1 ± 5.2 | 0.043 | |
| MUAC (cm) | 32.1 ± 5.0 | 31.8 ± 5.7 | 30.7 ± 5.0 | 28.0 ± 4.0 | 0.025 | |
| TSF (mm) | 19.9 ± 5.1 | 21.4 ± 7.4 | 20.0 ± 5.3 | 18.5 ± 3.6 | 0.243 |
| Variables | CHUU with Normal UmA-RI | CHEU with Normal UmA-RI | CHUU with Abnormal UmA-RI | CHEU with Abnormal UmA-RI | p-Value a | |
|---|---|---|---|---|---|---|
| Sample size (n) (%) | 186 (68.6%) | 50 (18.5%) | 20 (7.4%) | 15 (5.5%) | ||
| Mean age (months) | 18.6 ± 0.9 | 18.5 ± 0.8 | 18.2 ± 0.2 | 18.8 ± 0.9 | ||
| Sex | Male | 91 (48.9%) | 28 (56.0%) | 8 (40.0%) | 4 (26.7%) | n/a |
| Female | 95 (51.1%) | 22 (44.0%) | 12 (60.0%) | 11 (73.3%) | ||
| Mean GA at birth (weeks) | 39.3 ± 1.9 | 39.4 ± 1.3 | 36.8 ± 2.5 | 38.3 ± 1.0 | <0.001 | |
| Born premature | 15 (8.1%) | 2 (4.0%) | 7 (35.0%) | 1 (6.7%) | n/a | |
| APGAR score (5 min) b | 10 [9, 10] | 9 [9, 10] | 9 [9, 10] | 9 [9, 9] | 0.069 | |
| Neonatal hospitalization | 35 (18.9%) | 6 (12.0%) | 7 (35.0%) | 1 (7.1%) | n/a | |
| Neonatal diagnosis c | Respiratory distress | 7 (3.8%) | 3 (6.0%) | 3 (15.0%) | 0 (0%) | n/a |
| Jaundice | 18 (9.7%) | 2 (4.0%) | 2 (10.0%) | 0 (0%) | ||
| Other | 10 (5.4%) | 1 (2.0%) | 1 (5.0%) | 1 (7.1%) | ||
| Prevention of vertical HIV transmission | Single drug (NVP) | N/A | 41 (82.0%) | N/A | 7 (46.7%) | n/a |
| Dual drug (NVP and AZT) | N/A | 3 (6.0%) | N/A | 6 (40.0%) | ||
| History of childhood illnesses | Malnutrition | 11 (6.0%) | 6 (12.0%) | 0 (0%) | 0 (0%) | n/a |
| Diarrhea | 57 (30.6%) | 13 (26.0%) | 4 (20.0%) | 2 (13.3%) | ||
| Hospital admission (post-neonatal) | Any illness | 18 (9.7%) | 5 (10.0%) | 0 (0%) | 1 (6.7%) | n/a |
| Breastfeeding | Ever breastfeed | 178 (95.7%) | 47 (94.0%) | 20 (100.0%) | 15 (100.0%) | |
| Early initiation of breastfeeding d | Within 1 h after birth | 124 (78.5%) | 21 (48.8%) | 9 (52.9%) | 8 (61.5%) | <0.001 |
| After 1 h of birth | 34 (21.5%) | 22 (51.2%) | 8 (47.1%) | 5 (38.5%) | ||
| Infant feeding from birth until 6 months e,f | Exclusive breastfeeding | 122 (65.9%) | 32 (64.0%) | 14 (70.0%) | 8 (53.4%) | 0.750 |
| Formula feeding | 11 (5.9%) | 3 (6.0%) | 0 (0%) | 0 (0%) | ||
| Mixed feeding | 45 (24.3%) | 8 (16.0%) | 4 (20.0%) | 2 (13.3%) | ||
| Formula feeding only at 6 months, but previous exclusive breastfeeding | 7 (3.8%) | 7 (14.0%) | 2 (10.0%) | 5 (33.3%) | ||
| Current breastfeeding | 50 (27.0%) | 3 (6.1%) | 4 (22.2%) | 2 (14.3%) | n/a |
| Growth Indicators a | CHUU | CHEU | p-Value | Normal UmA-RI | Abnormal UmA-RI | p-Value |
|---|---|---|---|---|---|---|
| n = 206 (76.0%) | n = 65 (24.0%) | n = 236 (87.1%) | n = 35 (12.9%) | |||
| WAZ | 0.04 ± 1.19 | −0.24 ± 1.26 | 0.122 | 0.01 ± 1.19 | −0.29 ± 1.32 | 0.122 |
| LAZ | −0.05 ± 1.32 | −0.73 ± 1.23 | 0.003 | −0.14 ± 1.29 | −0.68 ± 1.53 | <0.001 |
| WLZ | 0.08 ± 1.21 | 0.14 ± 1.33 | 0.710 | 0.10 ± 1.26 | 0.04 ± 1.10 | 0.710 |
| HCZ | 0.93 ± 1.18 | 0.71 ± 1.15 | 0.198 | 0.88 ± 1.16 | 0.85 ± 1.27 | 0.141 |
| Variables | CHUU with Normal UmA-RI | CHEU with Normal UmA-RI | CHUU with Abnormal UmA-RI | CHEU with Abnormal UmA-RI | p-Value a | |
|---|---|---|---|---|---|---|
| Sample size (n) (%) | 186 (68.6%) | 50 (18.5%) | 20 (7.4%) | 15 (5.5%) | ||
| At birth | ||||||
| Anthropometry (mean ± SD) | Weight (g) | 3187 ± 483 | 3108 ± 433 | 2649 ± 566 | 2704 ± 408 | <0.001 b |
| Length (cm) | 50.7 ± 3.0 | 49.9 ± 2.3 | 48.8 ± 2.9 | 49.1 ± 2.6 | 0.005 b | |
| HC (cm) | 34.5 ± 1.7 | 34.5 ± 1.5 | 33.0 ± 1.9 | 33.9 ± 1.5 | 0.003 b | |
| Indicators (mean ± SD) d | WAZ | −0.30 ± 1.16 | −0.54 ± 0.96 | −0.48 ± 1.07 | −1.04 ± 0.76 | 0.003 |
| LAZ | 0.68 ± 1.66 | 0.15 ± 1.32 | 0.64 ± 1.24 | 0.36 ± 1.28 | 0.023 c | |
| HCZ | 0.40 ± 1.34 | 0.35 ± 1.24 | 0.20 ± 0.95 | 0.48 ± 1.07 | 0.778 | |
| At age 18 months | ||||||
| Anthropometry (mean ± SD) | Weight (kg) | 10.9 ± 1.5 | 10.7 ± 1.8 | 10.8 ± 1.9 | 9.9 ± 1.0 | 0.079 |
| Length (cm) | 81.9 ± 3.8 | 80.6 ± 3.3 | 81.1 ± 4.1 | 78.2 ± 3.5 | <0.001 | |
| HC (cm) | 48.1 ± 1.6 | 48.1 ± 1.9 | 48.5 ± 1.9 | 47.1 ± 1.2 | 0.011 | |
| MUAC (cm) | 16.0 ± 1.4 | 16.2 ± 1.7 | 16.4 ± 1.7 | 16.0 ± 1.4 | 0.825 | |
| TSF (mm) | 8.7 ± 2.0 | 8.4 ± 2.2 | 8.7 ± 2.7 | 8.6 ± 1.3 | 0.869 | |
| Indicators (mean ± SD) e | WAZ | 0.05 ± 1.15 | −0.11 ± 1.32 | −0.02 ± 1.52 | −0.64 ± 0.92 | 0.014 |
| LAZ | −0.03 ± 1.30 | −0.56 ± 1.16 | −0.21 ± 1.53 | −1.30 ± 1.32 | <0.001 | |
| WLZ | 0.07 ± 1.20 | 0.19 ± 1.46 | 0.09 ± 1.32 | −0.02 ± 0.76 | 0.662 | |
| HCZ | 0.89 ± 1.15 | 0.83 ± 1.23 | 1.26 ± 1.47 | 0.33 ± 0.73 | 0.016 | |
| Nutritional classifications (n; %) | Underweight | 4 (2.2%) | 3 (6.0%) | 1 (5.0%) | 0 (0.0%) | n/a |
| Stunting f | 9 (4.8%) | 8 (16.0%) | 2 (10.0%) | 6 (40.0%) | <0.001 | |
| Wasting | 6 (3.2%) | 4 (8.0%) | 0 (0.0%) | 0 (0.0%) | n/a |
| Feeding Practices during the First Six Months of Life | Continued Breastfeeding at Age 18 Months | |||||||
|---|---|---|---|---|---|---|---|---|
| Exclusive Breastfeeding | Formula Feeding | Mixed Feeding | Formula Feeding Only, but Previously Exclusive Breastfeeding | p-Value a | Supplementary Breastfeeding | No Supplementary Breastfeeding | p-Value a | |
| Sample size b | 176 (65.2%) | 14 (5.2%) | 59 (21.9%) | 21 (7.8%) | 59 (21.8%) | 212 (78.2%) | ||
| WAZ c | −0.13 ± 1.18 | 0.03 ± 1.23 | 0.31 ± 1.25 | −0.14 ± 1.24 | 0.105 | 0.03 ± 1.25 | −0.04 ± 1.20 | 0.672 |
| LAZ c | −0.34 ± 1.25 | 0.28 ± 1.33 | 0.10 ± 1.46 | −0.32 ± 1.55 | 0.067 | −0.01 ± 1.46 | −0.27 ± 1.29 | 0.225 |
| WLZ c | 0.04 ± 1.19 | −0.18 ± 1.78 | 0.34 ± 1.29 | 0.01 ± 1.13 | 0.335 | 0.05 ± 1.21 | 0.10 ± 1.25 | 0.768 |
| HCZ c | 0.86 ± 1.17 | 0.83 ± 1.12 | 1.07 ± 1.07 | 0.60 ± 1.39 | 0.506 | 1.04 ± 1.10 | 0.83 ± 1.19 | 0.220 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nyofane, M.; Hoffman, M.; Mulol, H.; Botha, T.; Vannevel, V.; Pattinson, R.; Feucht, U. Early Childhood Growth Parameters in South African Children with Exposure to Maternal HIV Infection and Placental Insufficiency. Viruses 2022, 14, 2745. https://doi.org/10.3390/v14122745
Nyofane M, Hoffman M, Mulol H, Botha T, Vannevel V, Pattinson R, Feucht U. Early Childhood Growth Parameters in South African Children with Exposure to Maternal HIV Infection and Placental Insufficiency. Viruses. 2022; 14(12):2745. https://doi.org/10.3390/v14122745
Chicago/Turabian StyleNyofane, Mothusi, Marinel Hoffman, Helen Mulol, Tanita Botha, Valerie Vannevel, Robert Pattinson, and Ute Feucht. 2022. "Early Childhood Growth Parameters in South African Children with Exposure to Maternal HIV Infection and Placental Insufficiency" Viruses 14, no. 12: 2745. https://doi.org/10.3390/v14122745