
Symptomatic Chikungunya Virus Infection and Pregnancy Outcomes: A Nested Case-Control Study in French Guiana
 ,
,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
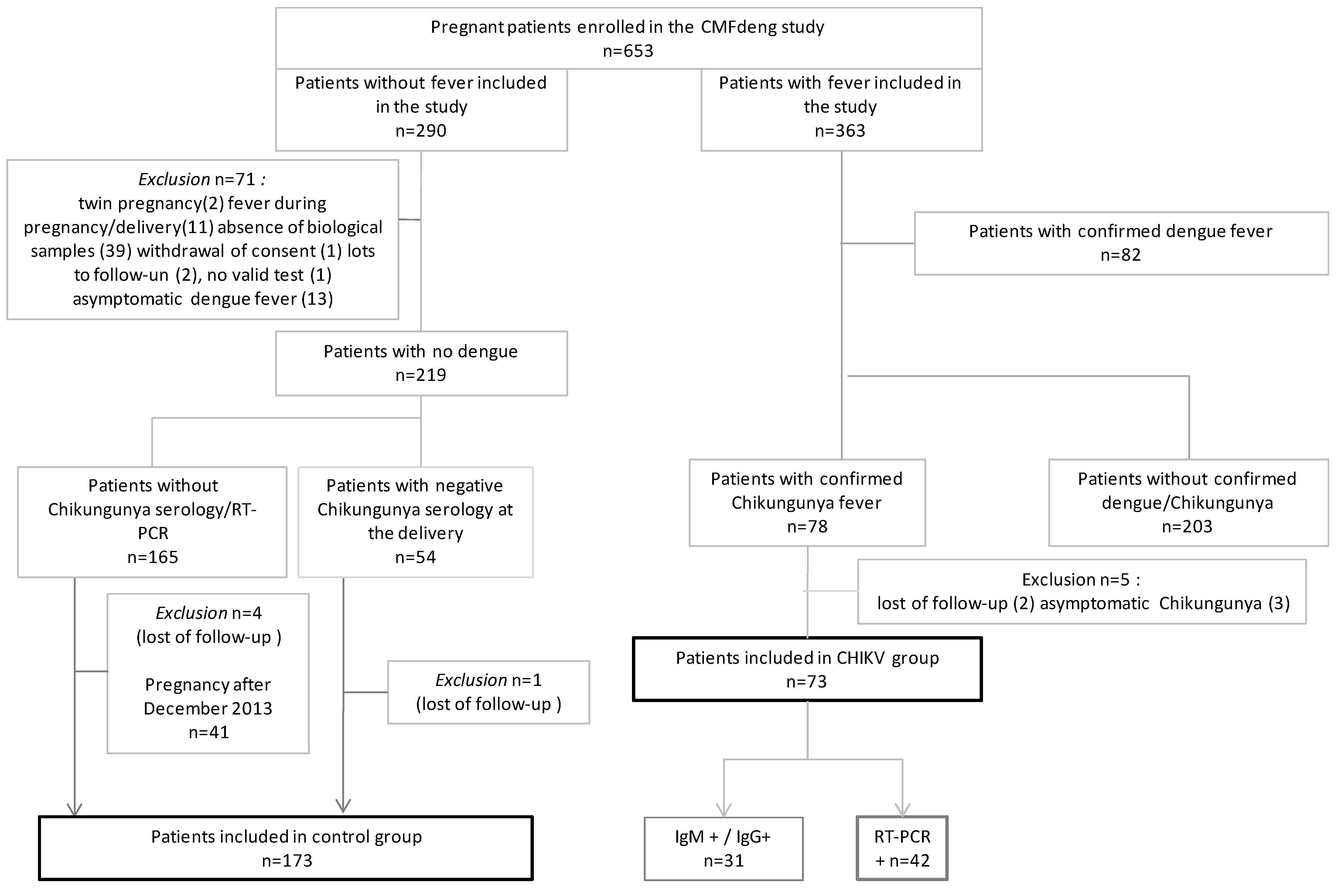
2.1. Study Overview
2.2. Definition of Groups
2.3. Biological Analysis
2.4. Data Collection and Outcome
2.5. Statistical Analysis
2.6. Ethics Statement
3. Results
3.1. Participant Characteristics
3.2. Description of Maternal CHIKV
3.3. Pregnancy Outcomes
3.4. Neonatal Outcomes
4. Discussion
5. Conclusions
CMFdengStudy Group
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Robinson, M.C. An epidemic of virus disease in Southern Province, Tanganyika territory, in 1952–1953. Trans. R. Soc. Trop. Med. Hyg. 1955, 49, 28–32. [Google Scholar] [CrossRef] [PubMed]
- Pialoux, G.; Gaüzère, B.-A.; Jauréguiberry, S.; Strobel, M. Chikungunya, an epidemic arbovirosis. Lancet Infect. Dis. 2007, 7, 319–327. [Google Scholar] [CrossRef] [PubMed]
- Weaver, S.C.; Lecuit, M. Chikungunya Virus and the Global Spread of a Mosquito-Borne Disease. N. Engl. J. Med. 2015, 372, 1231–1239. [Google Scholar] [CrossRef] [Green Version]
- Cassadou, S.; Boucau, S.; Petit-Sinturel, M.; Huc, P.; Leparc-Goffart, I.; Ledrans, M. Emergence of chikungunya fever on the French side of Saint Martin island, October to December 2013. Eurosurveillance 2014, 19, 20752. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dorléans, F.; Hoen, B.; Najioullah, F.; Herrmann-Storck, C.; Schepers, K.M.; Abel, S.; Lamaury, I.; Fagour, L.; Césaire, R.; Guyomard, S.; et al. Outbreak of Chikungunya in the French Caribbean Islands of Martinique and Guadeloupe: Findings from a Hospital-Based Surveillance System (2013–2015). Am. J. Trop. Med. Hyg. 2018, 98, 1819–1825. [Google Scholar] [CrossRef] [Green Version]
- Interregional Epidemiology Unit (CIRE) of the Indian Ocean. [Dengue, Chikungunya: Risks for the Overseas Territories]. BVS. 2015, 26. [French]. Available online: https://www.ocean-indien.ars.sante.fr/sites/default/files/2017-01/2015_26_BVS_thematique_Arbos_1.pdf (accessed on 31 March 2015).
- Bonifay, T.; Prince, C.; Neyra, C.; Demar, M.P.; Rousset, D.; Kallel, H.; Nacher, M.; Djossou, F.; Epelboin, L.; the Char Chik Working group. Atypical and severe manifestations of chikungunya virus infection in French Guiana: A hospital-based study. PLoS ONE 2018, 13, e0207406. [Google Scholar] [CrossRef] [Green Version]
- Vouga, M.; Chiu, Y.-C.; Pomar, L.; de Meyer, S.V.; Masmejan, S.; Genton, B.; Musso, D.; Baud, D.; Stojanov, M. Dengue, Zika and chikungunya during pregnancy: Pre- and post-travel advice and clinical management. J. Travel Med. 2019, 26, taz077. [Google Scholar] [CrossRef]
- Escobar, M.; Nieto, A.J.; Loaiza-Osorio, S.; Barona, J.S.; Rosso, F. Pregnant Women Hospitalized with Chikungunya Virus Infection, Colombia, 2015. Emerg. Infect. Dis. 2017, 23, 1777–1783. [Google Scholar] [CrossRef]
- Foeller, M.E.; Nosrat, C.; Krystosik, A.; Noel, T.; Gérardin, P.; Cudjoe, N.; Mapp-Alexander, V.; Mitchell, G.; Macpherson, C.; Waechter, R.; et al. Chikungunya infection in pregnancy—Reassuring maternal and perinatal outcomes: A retrospective observational study. BJOG Int. J. Obstet. Gynaecol. 2021, 128, 1077–1086. [Google Scholar] [CrossRef]
- Oliveira, R.D.M.A.B.; Barreto, F.K.D.A.; Maia, A.M.P.C.; Gomes, I.P.; Simião, A.R.; Barbosa, R.B.; Rodrigues, A.S.R.; Lopes, K.W.; Araújo, F.M.D.C.; Vale, R.L.S.D.; et al. Maternal and infant death after probable vertical transmission of chikungunya virus in Brazil—Case report. BMC Infect. Dis. 2018, 18, 333. [Google Scholar] [CrossRef]
- Gupta, N.; Gupta, S. Short-term pregnancy outcomes in patients chikungunya infection: An observational study. J. Fam. Med. Prim. Care 2019, 8, 985–987. [Google Scholar] [CrossRef]
- Ramful, D.; Carbonnier, M.; Pasquet, M.; Bouhmani, B.; Ghazouani, J.; Noormahomed, T.; Beullier, G.; Attali, T.; Samperiz, S.; Fourmaintraux, A.; et al. Mother-to-Child Transmission of Chikungunya Virus Infection. Pediatr. Infect. Dis. J. 2007, 26, 811–815. [Google Scholar] [CrossRef] [PubMed]
- Gérardin, P.; Barau, G.; Michault, A.; Bintner, M.; Randrianaivo, H.; Choker, G.; Lenglet, Y.; Touret, Y.; Bouveret, A.; Grivard, P.; et al. Multidisciplinary Prospective Study of Mother-to-Child Chikungunya Virus Infections on the Island of La Réunion. PLoS Med. 2008, 5, e60. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marinho, P.S.; Cunha, A.J.; Junior, J.A.; Prata-Barbosa, A. A review of selected Arboviruses during pregnancy. Matern. Health Neonatol. Perinatol. 2017, 3, 17. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Basurko, C.; Everhard, S.; Matheus, S.; Restrepo, M.; Hildéral, H.; Lambert, V.; Boukhari, R.; Duvernois, J.-P.; Favre, A.; Valmy, L.; et al. A prospective matched study on symptomatic dengue in pregnancy. PLoS ONE 2018, 13, e0202005. [Google Scholar] [CrossRef] [Green Version]
- Talarmin, A.; Labeau, B.; Lelarge, J.; Sarthou, J.-L. Immunoglobulin A-Specific Capture Enzyme-Linked Immunosorbent Assay for Diagnosis of Dengue Fever. J. Clin. Microbiol. 1998, 36, 1189–1192. [Google Scholar] [CrossRef] [Green Version]
- Panning, M.; Grywna, K.; Van Esbroeck, M.; Emmerich, P.; Drosten, C. Chikungunya Fever in Travelers Returning to Europe from the Indian Ocean Region, 2006. Emerg. Infect. Dis. 2008, 14, 416–422. [Google Scholar] [CrossRef]
- Grivard, P.; Le Roux, K.; Laurent, P.; Fianu, A.; Perrau, J.; Gigan, J.; Hoarau, G.; Grondin, N.; Staikowsky, F.; Favier, F.; et al. Molecular and serological diagnosis of Chikungunya virus infection. Pathol. Biol. 2007, 55, 490–494. [Google Scholar] [CrossRef]
- Economopoulou, A.; Dominguez, M.; Helynck, B.; Sissoko, D.; Wichmann, O.; Quenel, P.; Germonneau, P.; Quatresous, I. Atypical chikungunya virus infections: Clinical manifestations, mortality and risk factors for severe disease during the 2005–2006 outbreak on Réunion. Epidemiol. Infect. 2009, 137, 534–541. [Google Scholar] [CrossRef] [Green Version]
- Fritel, X.; Rollot, O.; Gérardin, P.; Gaüzère, B.-A.; Bideault, J.; Lagarde, L.; Dhuime, B.; Orvain, E.; Cuillier, F.; Ramful, D.; et al. Chikungunya Virus Infection during Pregnancy, Réunion, France, 2006. Emerg. Infect. Dis. 2010, 16, 418–425. [Google Scholar] [CrossRef]
- Bernard, M.; Lastère, S.; Kuo, P.; Pawlotsky, F.; Darteyre, S.; Guyot, D.; Elie, V.; Jacqz-Aigrain, E.; Lévy, M.; Papouin-Rauzy, M. [Maternal-Fetal Chikungunya Infection in French Polynesia, 2014–2015], BVS, 2015, 8-9, Page 3 [French]. Available online: https://www.ors-martinique.org/images/PDF/pathologies/bvs_ag_2015_08-09_JRVS.pdf (accessed on 31 October 2015).
- Torres, J.R.; Falleiros-Arlant, L.H.; Dueñas, L.; Navarrete, J.P.; Salgado, D.M.; Castillo, J.B.-D. Congenital and perinatal complications of chikungunya fever: A Latin American experience. Int. J. Infect. Dis. 2016, 51, 85–88. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Villamil-Gómez, W.; Alba-Silvera, L.; Menco-Ramos, A.; Gonzalez-Vergara, A.; Molinares-Palacios, T.; Barrios-Corrales, M.; Rodríguez-Morales, A.J. Congenital Chikungunya Virus Infection in Sincelejo, Colombia: A Case Series. J. Trop. Pediatr. 2015, 61, 386–392. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gavotto, A.; Muanza, B.; Delion, F.; Dusacre, J.-A.; Amedro, P. Chikungunya disease among infants in French West Indies during the 2014 outbreak. Arch. Pédiatr. 2019, 26, 259–262. [Google Scholar] [CrossRef] [PubMed]
- Teo, T.H.; Her, Z.; Tan, J.J.; Lum, F.M.; Lee, W.W.; Chan, Y.H.; Ong, R.Y.; Kam, Y.W.; Leparc-Goffart, I.; Gallian, P.; et al. Caribbean and La Réunion Chikungunya Virus Isolates Differ in Their Capacity To Induce Pro inflammatory Th1 and NK Cell Responses and Acute Joint Pathology. J. Virol. 2015, 89, 7955–7969. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Girod, R.; Guidez, A.; Carinci, R.; Issaly, J.; Gaborit, P.; Ferrero, E.; Ardillon, V.; Fontaine, A.; Dusfour, I.; Briolant, S. Detection of Chikungunya Virus Circulation Using Sugar-BaitedTraps during a Major Outbreak in French Guiana. PLoS Negl. Trop. Dis. 2016, 10, e0004876. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Socio-Demographic Characteristics | |||
|---|---|---|---|
| Control Group N (%) | CHIKV Group N (%) | p-Value | |
| Age at inclusion (n = 246) | |||
| ≤25 | 59 (34.1) | 25 (34.2) | 0.383 |
| 26–35 | 90 (52.0) | 33 (45.2) | |
| ≥36 | 24 (13.9) | 15 (20.5) | |
| Has a complementary health insurance (n = 200) | 119 (86.9) | 57 (90.5) | 0.465 |
| Married couples (n = 200) | 95 (69.3) | 40 (63.5) | 0.412 |
| Homeowner (n = 200) | 33 (24.1) | 18 (28.6) | 0.499 |
| Had contact with family in the past 6 months (n = 199) | 115 (84.6) | 51 (80.9) | 0.525 |
| Medical History | |||
| Hypertension (n = 245) | 4 (2.3) | 3 (4.2) | 0.422 |
| Diabetes (n = 245) | 0 (0) | 1 (1.4) | 0.294 |
| Habits | |||
| Active smoking during pregnancy (n = 246) | 6 (3.5) | 4 (5.5) | 0.489 |
| Known alcoholism (n = 246) | 1 (0.6) | 3 (4.1) | 0.080 |
| Gravidity upon Inclusion | |||
| Primigravida (n = 245) | 37 (21.5) | 9 (12.3) | 0.092 |
| Obstetrical History (Exclusion of Primigravida Women) | |||
| Preterm delivery (n = 198) | 20 (14.8) | 11 (17.5) | 0.633 |
| Fetal growth restriction (n = 198) | 7 (5.2) | 3 (4.8) | 1 |
| Hypertensive disorders (n = 198) | 17 (12.6) | 11 (17.5) | 0.360 |
| Post-partum hemorrhage (n = 198) | 8 (5.9) | 3 (4.8) | 1 |
| Gestational diabetes (n = 198) | 5 (3.7) | 4 (6.3) | 0.469 |
| Induced abortions (n = 198) | 44 (32.6) | 22 (34.9) | 0.746 |
| Medical termination of pregnancy (n = 199) | 6 (4.4) | 3 (4.8) | 1 |
| Congenital anomalies(n = 198) | 4 (2.9) | 3 (4.8) | 0.680 |
| Miscarriage (<22WG) (n = 199) | 44 (32.3) | 19 (30.2) | 0.757 |
| Intra-uterine fetal death (n = 198) | 6 (4.4) | 1 (1.6) | 0.434 |
| Cesarean section (n = 199) | 25 (18.4) | 15 (23.8) | 0.374 |
| Quality of Pregnancy Follow-Up | |||
| First ultrasound before 14 WG (n = 218) | 127 (77.0) | 37 (69.8) | 0.294 |
| At least 7 prenatal visits (n = 232) | 122 (74.4) | 51 (75.0) | 0.923 |
| Trimester of CHIKV Maternal Symptoms | |||
|---|---|---|---|
| Maternal Symptoms | 1st [n = 3] N (%) | 2nd [n = 24] N (%) | 3rd [n = 46] N (%) |
| Fever | 3 (100) | 24 (100) | 46 (100) |
| Joint pain | 2 (66.7) | 20 (83.3) | 24 (52.2) |
| Headache, retro-orbital pain | 1 (33.3) | 10 (41.7) | 15 (32.6) |
| Muscle pain | 0 (0) | 8 (33.3) | 11 (23.9) |
| Digestive symptoms (nausea, vomiting, pain) | 1 (33.3) | 7 (29.2) | 5 (10.9) |
| Altered general condition, asthenia | 0 (0) | 2 (8.3) | 6 (13.0) |
| General body pain | 1 (33.3) | 1 (4.2) | 5 (10.9) |
| Chills | 0 (0) | 3 (12.5) | 2 (4.3) |
| Skin rash, pruritus | 1 (33.3) | 2 (8.3) | 2 (4.3) |
| Occurrence of | Control Group N (%) | CHIKV Group N (%) | p-Value * |
|---|---|---|---|
| Pregnancy adverse outcomes (composite) (n = 246) | 53 (30.6) | 27 (37.0) | 0.331 |
| Preterm labor (n = 246) | 17 (9.8) | 6 (8.2) | 0.692 |
| Preterm delivery under 37 WG (n = 246) | 19 (11.0) | 7 (9.6) | 0.745 |
| Fetal growth restriction (n = 246) | 11 (6.4) | 4 (5.5) | 0.792 |
| Stillbirth (n = 246) | 0 (0) | 0 (0) | / |
| Postpartum hemorrhage (n = 246) | 11 (6.4) | 10 (13.7) | 0.060 |
| Caesarean section for abnormal fetal heart rate (n = 246) | 14 (8.1) | 7 (9.6) | 0.701 |
| Control Group N (%) | CHIKV Group N (%) | p-Value * | |
|---|---|---|---|
| Macrosomia (n = 246) | 9 (5.2) | 2 (2.7) | 0.514 |
| Small for gestational age infants (n = 246) | 16 (9.2) | 7 (9.6) | 0.933 |
| Length of hospital stay (newborn) > 3 days (n = 244) | 63 (36.8) | 29 (39.7) | 0.670 |
| Neonatal adverse outcomes (composite) (n = 246) | 31 (17.9) | 15 (20.5) | 0.629 |
| Congenital anomalies (n = 246) | 11/173 (4.6) | 5/73 (5.5) | 0.542 |
| Five-minutes APGAR score < 7 (n = 244) | 2/171 (1.2) | 1/73 (1.4) | 1 |
| Respiratory distress (n = 244) | 10/173 (5.8) | 7/71 (9.9) | 0.274 |
| Seizures (n = 246) | 1/173 (0.6) | 0/73 | 1 |
| NICU admission (n = 246) | 21/173 (12.1) | 10/73 (13.7) | 0.736 |
| Hyperthermia at birth (≥38 °C) (n = 183) | 2/128 (1.6) | 1/55 (1.8) | 1 |
| Delay between CHIKV Maternal Symptoms and Delivery | p-Value | ||
|---|---|---|---|
| Outcomes | >7 Days N (%) | ≤7 Days N (%) | |
| Preterm delivery under 37 WG (n = 73) | 5 (7.6) | 2 (28.6) | 0.132 |
| Preterm delivery under 34 WG (n = 73) | 1 (1.5) | 1 (14.3) | 0.184 |
| Caesarean section for abnormal fetal heart rate (n = 73) | 6 (9.1) | 1 (14.3) | 0.522 |
| Post-partum hemorrhage (n = 73) | 9 (13.6) | 1 (14.3) | 1 |
| Length of hospital stay (newborn) > 3 d. (n = 73) | 25 (37.9) | 4 (57.1) | 0.425 |
| Five-minute APGAR score < 7 (n = 73) | 1 (1.5) | 0 (0) | 1 |
| Respiratory distress (n = 71) | 5 (7.8) | 2 (28.6) | 0.138 |
| Neonatal ICU admission (n = 73) | 7 (10.6) | 3 (42.9) | 0.049 |
| Hyperthermia at birth (n = 55) | 0 (0) | 1 (20.0) | 0.091 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Basurko, C.; Hcini, N.; Demar, M.; Abboud, P.; the CMFdeng study group; Nacher, M.; Carles, G.; Lambert, V.; Matheus, S. Symptomatic Chikungunya Virus Infection and Pregnancy Outcomes: A Nested Case-Control Study in French Guiana. Viruses 2022, 14, 2705. https://doi.org/10.3390/v14122705
Basurko C, Hcini N, Demar M, Abboud P, the CMFdeng study group, Nacher M, Carles G, Lambert V, Matheus S. Symptomatic Chikungunya Virus Infection and Pregnancy Outcomes: A Nested Case-Control Study in French Guiana. Viruses. 2022; 14(12):2705. https://doi.org/10.3390/v14122705
Chicago/Turabian StyleBasurko, Célia, Najeh Hcini, Magalie Demar, Philippe Abboud, the CMFdeng study group, Mathieu Nacher, Gabriel Carles, Véronique Lambert, and Séverine Matheus. 2022. "Symptomatic Chikungunya Virus Infection and Pregnancy Outcomes: A Nested Case-Control Study in French Guiana" Viruses 14, no. 12: 2705. https://doi.org/10.3390/v14122705