Adjuvant Sorafenib for Postoperative Patients with Hepatocellular Carcinoma and Macrovascular Invasion

 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Diagnosis and Treatment of HCC
2.3. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA A Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef]
- Lu, J.; Zhang, X.P.; Zhong, B.Y.; Lau, W.Y.; Madoff, D.C.; Davidson, J.C.; Qi, X.; Cheng, S.Q.; Teng, G.J. Management of patients with hepatocellular carcinoma and portal vein tumour thrombosis: Comparing east and west. Lancet Gastroenterol. Hepatol. 2019, 4, 721–730. [Google Scholar] [CrossRef]
- Costentin, C.E.; Decaens, T.; Laurent, A.; Nault, J.C.; Paule, B.; Letoublon, C.; Luciani, A.; Calderaro, J.; Adam, R.; Bricault, I.; et al. Sorafenib vs. surgical resection for hepatocellular carcinoma with macrovascular invasion: A propensity score analysis. Liver Int. Off. J. Int. Assoc. Study Liver 2017, 37, 1869–1876. [Google Scholar] [CrossRef]
- European Association for the Study of the Liver. EASL Clinical Practice Guidelines: Management of hepatocellular carcinoma. J. Hepatol. 2018, 69, 182–236. [Google Scholar] [CrossRef]
- Singal, A.G.; Llovet, J.M.; Yarchoan, M.; Mehta, N.; Heimbach, J.K.; Dawson, L.A.; Jou, J.H.; Kulik, L.M.; Agopian, V.G.; Marrero, J.A.; et al. AASLD Practice Guidance on prevention, diagnosis, and treatment of hepatocellular carcinoma. Hepatology 2023, 78, 1922–1965. [Google Scholar] [CrossRef]
- Llovet, J.M.; Ricci, S.; Mazzaferro, V.; Hilgard, P.; Gane, E.; Blanc, J.F.; de Oliveira, A.C.; Santoro, A.; Raoul, J.L.; Forner, A.; et al. Sorafenib in advanced hepatocellular carcinoma. N. Engl. J. Med. 2008, 359, 378–390. [Google Scholar] [CrossRef]
- Cheng, A.L.; Kang, Y.K.; Chen, Z.; Tsao, C.J.; Qin, S.; Kim, J.S.; Luo, R.; Feng, J.; Ye, S.; Yang, T.S.; et al. Efficacy and safety of sorafenib in patients in the Asia-Pacific region with advanced hepatocellular carcinoma: A phase III randomised, double-blind, placebo-controlled trial. Lancet Oncol. 2009, 10, 25–34. [Google Scholar] [CrossRef]
- Finn, R.S.; Qin, S.; Ikeda, M.; Galle, P.R.; Ducreux, M.; Kim, T.Y.; Kudo, M.; Breder, V.; Merle, P.; Kaseb, A.O.; et al. Atezolizumab plus Bevacizumab in Unresectable Hepatocellular Carcinoma. N. Engl. J. Med. 2020, 382, 1894–1905. [Google Scholar] [CrossRef]
- Huang, S.; Li, D.; Zhuang, L.; Sun, L.; Wu, J. A meta-analysis of the efficacy and safety of adjuvant sorafenib for hepatocellular carcinoma after resection. World J. Surg. Oncol. 2021, 19, 168. [Google Scholar] [CrossRef]
- Xia, F.; Wu, L.L.; Lau, W.Y.; Huan, H.B.; Wen, X.D.; Ma, K.S.; Li, X.W.; Bie, P. Adjuvant sorafenib after heptectomy for Barcelona Clinic Liver Cancer-stage C hepatocellular carcinoma patients. World J. Gastroenterol. WJG 2016, 22, 5384–5392. [Google Scholar] [CrossRef] [PubMed]
- Bruix, J.; Takayama, T.; Mazzaferro, V.; Chau, G.Y.; Yang, J.; Kudo, M.; Cai, J.; Poon, R.T.; Han, K.H.; Tak, W.Y.; et al. Adjuvant sorafenib for hepatocellular carcinoma after resection or ablation (STORM): A phase 3, randomised, double-blind, placebo-controlled trial. Lancet Oncol. 2015, 16, 1344–1354. [Google Scholar] [CrossRef]
- Sun, Y.; Zhang, W.; Bi, X.; Yang, Z.; Tang, Y.; Jiang, L.; Bi, F.; Chen, M.; Cheng, S.; Chi, Y.; et al. Systemic Therapy for Hepatocellular Carcinoma: Chinese Consensus-Based Interdisciplinary Expert Statements. Liver Cancer 2022, 11, 192–208. [Google Scholar] [CrossRef]
- Wang, S.N.; Chuang, S.C.; Lee, K.T. Efficacy of sorafenib as adjuvant therapy to prevent early recurrence of hepatocellular carcinoma after curative surgery: A pilot study. Hepatol. Res. Off. J. Jpn. Soc. Hepatol. 2014, 44, 523–531. [Google Scholar] [CrossRef]
- Rinella, M.E.; Lazarus, J.V.; Ratziu, V.; Francque, S.M.; Sanyal, A.J.; Kanwal, F.; Romero, D.; Abdelmalek, M.F.; Anstee, Q.M.; Arab, J.P.; et al. A multi-society Delphi consensus statement on new fatty liver disease nomenclature. Hepatology 2023, 29, 101133. [Google Scholar] [CrossRef]
- Johnson, P.J.; Berhane, S.; Kagebayashi, C.; Satomura, S.; Teng, M.; Reeves, H.L.; O’Beirne, J.; Fox, R.; Skowronska, A.; Palmer, D.; et al. Assessment of liver function in patients with hepatocellular carcinoma: A new evidence-based approach-the ALBI grade. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2015, 33, 550–558. [Google Scholar] [CrossRef]
- Marrero, J.A.; Kulik, L.M.; Sirlin, C.B.; Zhu, A.X.; Finn, R.S.; Abecassis, M.M.; Roberts, L.R.; Heimbach, J.K. Diagnosis, Staging, and Management of Hepatocellular Carcinoma: 2018 Practice Guidance by the American Association for the Study of Liver Diseases. Hepatology 2018, 68, 723–750. [Google Scholar] [CrossRef]
- Ikai, I.; Yamamoto, Y.; Yamamoto, N.; Terajima, H.; Hatano, E.; Shimahara, Y.; Yamaoka, Y. Results of hepatic resection for hepatocellular carcinoma invading major portal and/or hepatic veins. Surg. Oncol. Clin. N. Am. 2003, 12, 65–75. [Google Scholar] [CrossRef]
- Hsu, W.F.; Wang, H.W.; Chen, C.K.; Lai, H.C.; Chuang, P.H.; Tsai, M.H.; Su, W.P.; Chen, H.Y.; Chu, C.S.; Chou, J.W.; et al. Alpha-fetoprotein response predicts treatment outcomes in patients with unresectable hepatocellular carcinoma receiving immune checkpoint inhibitors with or without tyrosine kinase inhibitors or locoregional therapies. Am. J. Cancer Res. 2021, 11, 6173–6187. [Google Scholar]
- Liao, S.H.; Chen, C.L.; Hsu, C.Y.; Chien, K.L.; Kao, J.H.; Chen, P.J.; Chen, T.H.; Chen, C.H. Long-term effectiveness of population-wide multifaceted interventions for hepatocellular carcinoma in Taiwan. J. Hepatol. 2021, 75, 132–141. [Google Scholar] [CrossRef]
- Reig, M.; Forner, A.; Rimola, J.; Ferrer-Fabrega, J.; Burrel, M.; Garcia-Criado, A.; Kelley, R.K.; Galle, P.R.; Mazzaferro, V.; Salem, R.; et al. BCLC strategy for prognosis prediction and treatment recommendation: The 2022 update. J. Hepatol. 2022, 76, 681–693. [Google Scholar] [CrossRef] [PubMed]
- Kudo, M.; Finn, R.S.; Qin, S.; Han, K.H.; Ikeda, K.; Piscaglia, F.; Baron, A.; Park, J.W.; Han, G.; Jassem, J.; et al. Lenvatinib versus sorafenib in first-line treatment of patients with unresectable hepatocellular carcinoma: A randomised phase 3 non-inferiority trial. Lancet 2018, 391, 1163–1173. [Google Scholar] [CrossRef]
- Brown, T.J.; Gupta, A.; Sedhom, R.; Beg, M.S.; Karasic, T.B.; Yarchoan, M. Trends of Clinical Outcomes of Patients with Advanced Hepatocellular Carcinoma Treated with First-Line Sorafenib in Randomized Controlled Trials. Gastrointest. Tumors 2022, 9, 19–26. [Google Scholar] [CrossRef]
- Yau, T.; Tang, V.Y.; Yao, T.J.; Fan, S.T.; Lo, C.M.; Poon, R.T. Development of Hong Kong Liver Cancer staging system with treatment stratification for patients with hepatocellular carcinoma. Gastroenterology 2014, 146, 1691–1700.e1693. [Google Scholar] [CrossRef]
- Ho, M.C.; Hasegawa, K.; Chen, X.P.; Nagano, H.; Lee, Y.J.; Chau, G.Y.; Zhou, J.; Wang, C.C.; Choi, Y.R.; Poon, R.T.; et al. Surgery for Intermediate and Advanced Hepatocellular Carcinoma: A Consensus Report from the 5th Asia-Pacific Primary Liver Cancer Expert Meeting (APPLE 2014). Liver Cancer 2016, 5, 245–256. [Google Scholar] [CrossRef]


{kind=link}
| Character | All (n = 43) | Adjuvant Sorafenib (n = 10) | Control (n = 33) | p-Value |
|---|---|---|---|---|
| Age (years) | 58 (52–65) | 66 (62–72) | 57 (50–63) | 0.007 |
| Sex (male), n (%) | 31 (72.1) | 5 (50) | 26 (78.8) | 0.175 |
| Body mass index (kg/m2) | 23.57 (21.28–26.39) | 25.44 (21.50–27.05) | 23.46 (21.06–25.90) | 0.232 |
| Platelet count (109/L) | 198 (162–253) | 210 (148–399) | 197 (166–249) | 0.380 |
| AST (U/L) | 41 (29–66) | 34 (28–74) | 41 (32–62) | 0.645 |
| ALT (U/L) | 35 (24–59) | 29 (21–41) | 38 (28–63) | 0.079 |
| Total bilirubin (mg/dL) | 0.80 (0.6–1.00) | 0.76 (0.45–1.27) | 0.8 (0.62–0.98) | 0.729 |
| Albumin (g/dL) | 4.3 (4.1–4.6) | 4.2 (3.7–4.4) | 4.4 (4.1–4.6) | 0.074 |
| Creatinine (mg/dL) | 0.89 (0.79–0.98) | 0.89 (0.74–0.98) | 0.89 (0.81–0.99) | 0.774 |
| Etiology | ||||
| Alcohol | 10 (23.3) | 1 (10) | 9 (27.3) | 0.419 |
| HBV | 27 (62.8) | 3 (30) | 24 (72.7) | 0.041 |
| HCV | 11 (26.2) | 4 (40) | 7 (21.9) | 0.406 |
| Diabetes mellitus | 12 (27.9) | 1 (10) | 11 (33.3) | 0.273 |
| Liver cirrhosis | 18 (41.9) | 6 (60) | 12 (36.4) | 0.273 |
| ALBI grade | 0.154 | |||
| 1 | 35 (83.3) | 6 (60) | 29 (90.6) | |
| 2 | 7 (16.7) | 4 (40) | 3 (9.4) | |
| AFP (ng/mL) | 98.96 (10.93–2786.89) | 24.02 (8.74–545.98) | 249.88 (11.15–5591.50) | 0.202 |
| AFP > 400 ng/mL | 15 (35.7) | 2 (20) | 13 (40.6) | 0.343 |
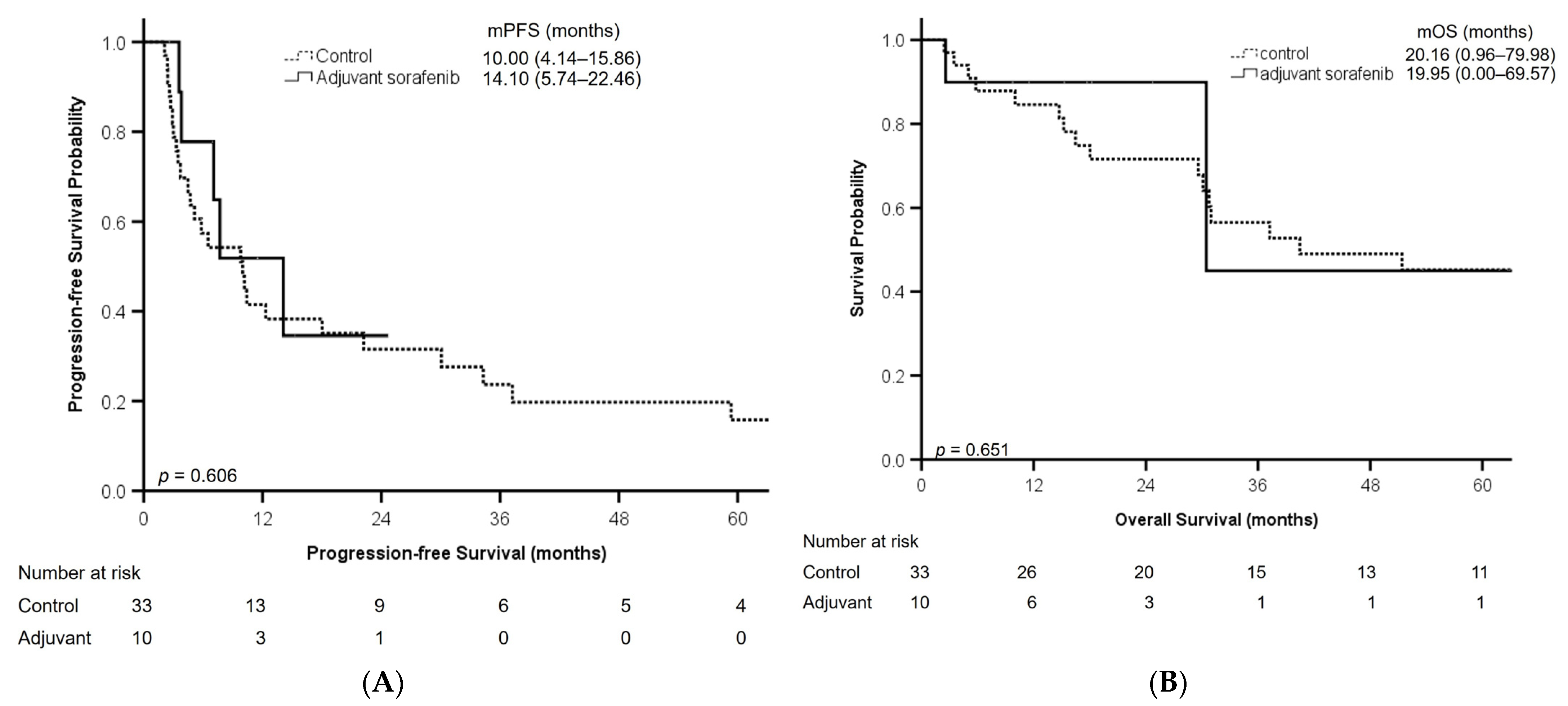
| PFS (months) * | 10.00 (6.04–13.96) | 14.10 (5.74–22.46) | 10.00 (4.14–15.86) | 0.268 |
| OS (months) * | 19.77 (1.71–79.23) | 19.95 (0.00–69.57) | 20.16 (0.96–79.98) | 0.204 |
| Characteristic | Univariate Analysis | Multivariate Analysis | |||
|---|---|---|---|---|---|
| HR (95% CI) | p Value | HR (95% CI) | p Value | ||
| Age (year) | 1.005 (0.974–1.037) | 0.757 | |||
| Sex | M vs. F | 1.066 (0.476–2.387) | 0.877 | ||
| Alcohol | Yes vs. no | 1.240 (0.578–2.660) | 0.580 | ||
| HBV | Yes vs. no | 1.119 (0.522–2.400) | 0.773 | ||
| HCV | Yes vs. no | 1.583 (0.709–3.537) | 0.263 | ||
| DM | Yes vs. no | 0.936 (0.432–2.027) | 0.866 | ||
| AFP (ng/mL) | <400 vs. ≥400 | 1.210 (0.564–2.599) | 0.625 | ||
| AST (U/L) | >40 vs. ≤40 | 0.529 (0.242–1.158) | 0.111 | ||
| ALT (U/L) | >40 vs. ≤40 | 0.799 (0.382–1.669) | 0.550 | ||
| ALBI grade | 2 vs. 1 | 0.602 (0.208–1.739) | 0.349 | ||
| Adjuvant sorafenib | Yes vs. no | 0.773 (0.291–2.052) | 0.606 | ||
| Characteristic | Univariate Analysis | Multivariate Analysis | |||
|---|---|---|---|---|---|
| HR (95% CI) | p Value | HR (95% CI) | p Value | ||
| Age (year) | 0.977 (0.942–1.013) | 0.202 | |||
| Sex | M vs. F | 2.025 (0.675–6.077) | 0.208 | ||
| Alcohol | Yes vs. no | 2.351 (0.956–5.783) | 0.063 | 2.930 (1.150–7.467) | 0.024 |
| HBV | Yes vs. no | 1.571 (0.566–4.357) | 0.386 | ||
| HCV | Yes vs. no | 0.710 (0.233–2.167) | 0.548 | ||
| DM | Yes vs. no | 1.221 (0.494–3.019) | 0.665 | ||
| AFP (ng/mL) | <400 vs. ≥400 | 2.244 (0.903–5.575) | 0.082 | 2.614 (1.033–6.614) | 0.043 |
| AST (U/L) | >40 vs. ≤40 | 1.234 (0.485–3.139) | 0.659 | ||
| ALT (U/L) | >40 vs. ≤40 | 0.903 (0.368–2.212) | 0.823 | ||
| ALBI grade | 2 vs 1 | 1.442 (0.475–4.375) | 0.518 | ||
| Adjuvant sorafenib | Yes vs no | 0.710 (0.160–3.155) | 0.653 | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chang, C.-J.; Hsu, W.-F.; Jeng, L.-B.; Lai, H.-C.; Hsu, S.-C.; Chen, T.-H.; Wang, H.-W.; Peng, C.-Y. Adjuvant Sorafenib for Postoperative Patients with Hepatocellular Carcinoma and Macrovascular Invasion. Curr. Oncol. 2023, 30, 10134-10141. https://doi.org/10.3390/curroncol30120737
Chang C-J, Hsu W-F, Jeng L-B, Lai H-C, Hsu S-C, Chen T-H, Wang H-W, Peng C-Y. Adjuvant Sorafenib for Postoperative Patients with Hepatocellular Carcinoma and Macrovascular Invasion. Current Oncology. 2023; 30(12):10134-10141. https://doi.org/10.3390/curroncol30120737
Chicago/Turabian StyleChang, Che-Jui, Wei-Fan Hsu, Long-Bin Jeng, Hsueh-Chou Lai, Shih-Chao Hsu, Te-Hung Chen, Hung-Wei Wang, and Cheng-Yuan Peng. 2023. "Adjuvant Sorafenib for Postoperative Patients with Hepatocellular Carcinoma and Macrovascular Invasion" Current Oncology 30, no. 12: 10134-10141. https://doi.org/10.3390/curroncol30120737