Comparative Analysis of Subclassification Systems in Patients with Intermediate-Stage Hepatocellular Carcinoma (Barcelona Clinic Liver Classification B) Receiving Systemic Therapy

 , , , , , , and
, , , , , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Design of the Study
2.2. Baseline, Subclassification, and Re-Evaluation
2.3. Management of Sorafenib
2.4. Statistical Analysis
3. Results
3.1. Study Population
3.2. Survival Analysis and Stratification According to Subclassification Systems
3.3. Postestimation Analysis of Subclassification Systems
3.4. Evaluation of Subclassification Systems According to Alpha-Fetoprotein
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Reig, M.; Forner, A.; Rimola, J.; Ferrer-Fàbrega, J.; Burrel, M.; Garcia-Criado, Á.; Kelley, R.K.; Galle, P.R.; Mazzaferro, V.; Salem, R.; et al. BCLC strategy for prognosis prediction and treatment recommendation: The 2022 update. J. Hepatol. 2022, 76, 681–693. [Google Scholar] [CrossRef] [PubMed]
- Mazzaferro, V.; Llovet, J.M.; Miceli, R.; Bhoori, S.; Schiavo, M.; Mariani, L.; Camerini, T.; Roayaie, S.; Schwartz, M.E.; Grazi, G.L.; et al. Predicting survival after liver transplantation in patients with hepatocellular carcinoma beyond the Milan criteria: A retrospective, exploratory analysis. Lancet Oncol. 2009, 10, 35–43. [Google Scholar] [CrossRef] [PubMed]
- Yi, P.-S.; Wang, H.; Li, J.-S. Evolution and current status of the subclassification of intermediate hepatocellular carcinoma. World J. Gastrointest. Surg. 2020, 12, 85–92. [Google Scholar] [CrossRef] [PubMed]
- Bolondi, L.; Burroughs, A.; Dufour, J.F.; Galle, P.; Mazzaferro, V.; Piscaglia, F.; Raoul, J.L.; Sangro, B. Heterogeneity of Patients with Intermediate (BCLC B) Hepatocellular Carcinoma: Proposal for a Subclassification to Facilitate Treatment Decisions. Semin. Liver Dis. 2013, 32, 348–359. [Google Scholar]
- Ciria, R.; López-Cillero, P.; Gallardo, A.B.; Cabrera, J.; Pleguezuelo, M.; Ayllón, M.D.; Luque, A.; Zurera, L.; Espejo, J.J.; Rodríguez-Perálvarez, M.; et al. Optimizing the management of patients with BCLC stage-B hepatocellular carcinoma: Modern surgical resection as a feasible alternative to transarterial chemoemolization. Eur. J. Surg. Oncol. EJSO 2015, 4, 1153–1161. [Google Scholar] [CrossRef]
- Giannini, E.G.; Moscatelli, A.; Pellegatta, G.; Vitale, A.; Farinati, F.; Ciccarese, F.; Piscaglia, F.; Rapaccini, G.L.; Di Marco, M.; Caturelli, E.; et al. Application of the Intermediate-Stage Subclassification to Patients With Untreated Hepatocellular Carcinoma. Am. J. Gastroenterol. 2016, 111, 70–77. [Google Scholar] [CrossRef]
- Yamakado, K.; Miyayama, S.; Hirota, S.; Mizunuma, K.; Nakamura, K.; Inaba, Y.; Maeda, H.; Matsuo, K.; Nishida, N.; Aramaki, T.; et al. Subgrouping of intermediate-stage (BCLC stage B) hepatocellular carcinoma based on tumor number and size and Child–Pugh grade correlated with prognosis after transarterial chemoembolization. Jpn. J. Radiol. 2014, 32, 260–265. [Google Scholar] [CrossRef]
- Kudo, M.; Arizumi, T.; Ueshima, K.; Sakurai, T.; Kitano, M.; Nishida, N. Subclassification of BCLC B Stage Hepatocellular Carcinoma and Treatment Strategies: Proposal of Modified Bolondi’s Subclassification (Kinki Criteria). Dig. Dis. 2015, 33, 751–758. [Google Scholar] [CrossRef]
- Arizumi, T.; Ueshima, K.; Iwanishi, M.; Minami, T.; Chishina, H.; Kono, M.; Takita, M.; Kitai, S.; Inoue, T.; Yada, N.; et al. Validation of Kinki Criteria, a Modified Substaging System, in Patients with Intermediate Stage Hepatocellular Carcinoma. Dig. Dis. 2016, 34, 671–678. [Google Scholar] [CrossRef]
- Wang, J.-H.; Kee, K.-M.; Lin, C.-Y.; Hung, C.-H.; Chen, C.-H.; Lee, C.-M.; Lu, S.-N. Validation and modification of a proposed substaging system for patients with intermediate hepatocellular carcinoma: Substaging of intermediate hepatocellular carcinoma. J. Gastroenterol. Hepatol. 2015, 30, 358–363. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.; Kim, B.K.; Song, K.; Park, J.Y.; Ahn, S.H.; Kim, S.U.; Han, K.H.; Kim, D.Y.; Korea Central Cancer Registry. Subclassification of Barcelona Clinic Liver Cancer B and C hepatocellular carcinoma: A cohort study of the multicenter registry database: Subclassification of BCLC stages. J. Gastroenterol. Hepatol. 2016, 31, 842–847. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.H.; Shim, J.H.; Lee, H.C.; Sung, K.-B.; Ko, H.-K.; Ko, G.-Y.; Gwon, D.I.; Kim, J.W.; Lim, Y.-S.; Park, S.H. New intermediate-stage subclassification for patients with hepatocellular carcinoma treated with transarterial chemoembolization. Liver Int. 2017, 37, 1861–1868. [Google Scholar] [CrossRef] [PubMed]
- Kimura, H.; Ohkawa, K.; Miyazaki, M.; Sakakibara, M.; Imanaka, K.; Tamura, T.; Sueyoshi, H.; Takada, R.; Fukutake, N.; Uehara, H.; et al. Subclassification of patients with intermediate-stage (Barcelona Clinic Liver Cancer stage-B) hepatocellular carcinoma using the up-to-seven criteria and serum tumor markers. Hepatol. Int. 2017, 11, 105–114. [Google Scholar] [CrossRef] [PubMed]
- Eisenhauer, E.A.; Therasse, P.; Bogaerts, J.; Schwartz, L.H.; Sargent, D.; Ford, R.; Dancey, J.; Arbuck, S.; Gwyther, S.; Mooney, M.; et al. New response evaluation criteria in solid tumours: Revised RECIST guideline (version 1.1). Eur. J. Cancer Oxf. Engl. 2009, 45, 228–247. [Google Scholar] [CrossRef] [PubMed]
- Ogasawara, S.; Chiba, T.; Ooka, Y.; Kanogawa, N.; Motoyama, T.; Suzuki, E.; Tawada, A.; Kanai, F.; Yoshikawa, M.; Yokosuka, O. Efficacy of sorafenib in intermediate-stage hepatocellular carcinoma patients refractory to transarterial chemoembolization. Oncology 2014, 87, 330–341. [Google Scholar] [CrossRef] [PubMed]
- Sansone, V.; Tovoli, F.; Casadei-Gardini, A.; Di Costanzo, G.G.; Magini, G.; Sacco, R.; Pressiani, T.; Trevisani, F.; Rimini, M.; Tortora, R.; et al. Comparison of Prognostic Scores in Patients with Hepatocellular Carcinoma Treated With Sorafenib. Clin. Transl. Gastroenterol. 2021, 12, e00286. [Google Scholar] [CrossRef]
- Kudo, M.; Finn, R.S.; Qin, S.; Han, K.-H.; Ikeda, K.; Piscaglia, F.; Baron, A.; Park, J.-W.; Han, G.; Jassem, J.; et al. Lenvatinib versus sorafenib in first-line treatment of patients with unresectable hepatocellular carcinoma: A randomised phase 3 non-inferiority trial. Lancet Lond. Engl. 2018, 391, 1163–1173. [Google Scholar] [CrossRef]
- Bruix, J.; Qin, S.; Merle, P.; Granito, A.; Huang, Y.-H.; Bodoky, G.; Pracht, M.; Yokosuka, O.; Rosmorduc, O.; Breder, V.; et al. Regorafenib for patients with hepatocellular carcinoma who progressed on sorafenib treatment (RESORCE): A randomised, double-blind, placebo-controlled, phase 3 trial. Lancet Lond. Engl. 2017, 389, 56–66. [Google Scholar] [CrossRef]
- Abou-Alfa, G.K.; Meyer, T.; Cheng, A.-L.; El-Khoueiry, A.B.; Rimassa, L.; Ryoo, B.-Y.; Cicin, I.; Merle, P.; Chen, Y.; Park, J.-W.; et al. Cabozantinib in Patients with Advanced and Progressing Hepatocellular Carcinoma. N. Engl. J. Med. 2018, 379, 54–63. [Google Scholar] [CrossRef]
- Ielasi, L.; Sansone, V.; Granito, A.; Benevento, F.; De Lorenzo, S.; Tovoli, F. An update of treatments of hepatocellular carcinoma in patients refractory to sorafenib. Drugs Today Barc. Spain 1998 2018, 54, 615–627. [Google Scholar] [CrossRef] [PubMed]
- Finn, R.S.; Qin, S.; Ikeda, M.; Galle, P.R.; Ducreux, M.; Kim, T.Y.; Kudo, M.; Breder, V.; Merle, P.; Kaseb, A.O.; et al. Atezolizumab plus Bevacizumab in Unresectable Hepatocellular Carcinoma. N. Engl. J. Med. 2020, 382, 1894–1905. [Google Scholar] [CrossRef] [PubMed]
- Kudo, M.; Matsui, O.; Izumi, N.; Kadoya, M.; Okusaka, T.; Miyayama, S.; Yamakado, K.; Tsuchiya, K.; Ueshima, K.; Hiraoka, A.; et al. Transarterial chemoembolization failure/refractoriness: JSH-LCSGJ criteria 2014 update. Oncology 2014, 87, 22–31. [Google Scholar] [CrossRef] [PubMed]
- Kudo, M.; Han, K.-H.; Ye, S.-L.; Zhou, J.; Huang, Y.-H.; Lin, S.-M.; Wang, C.-K.; Ikeda, M.; Chan, S.L.; Choo, S.P.; et al. A Changing Paradigm for the Treatment of Intermediate-Stage Hepatocellular Carcinoma: Asia-Pacific Primary Liver Cancer Expert Consensus Statements. Liver Cancer. 2020, 9, 245–260. [Google Scholar] [CrossRef] [PubMed]
- Kudo, M. New treatment paradigm with systemic therapy in intermediate-stage hepatocellular carcinoma. Int. J. Clin. Oncol. 2022, 27, 1110–1119. [Google Scholar] [CrossRef] [PubMed]
- Rimassa, L.; Finn, R.S.; Sangro, B. Combination immunotherapy for hepatocellular carcinoma. J. Hepatol. 2023, 79, 506–515. [Google Scholar] [CrossRef] [PubMed]
- Hatanaka, T.; Yata, Y.; Naganuma, A.; Kakizaki, S. Treatment Strategy for Intermediate-Stage Hepatocellular Carcinoma: Transarterial Chemoembolization, Systemic Therapy, and Conversion Therapy. Cancers 2023, 15, 1798. [Google Scholar] [CrossRef]
- Li, X.; Wang, X.; Bai, T.; Chen, J.; Lu, S.; Wei, T.; Tang, Z.; Zhao, G.; Lu, H.; Li, L.; et al. Conversion surgery for initially unresectable hepatocellular carcinoma using lenvatinib combined with TACE plus PD-1 inhibitor: A real-world observational study. Dig. Liver Dis. 2023. Online ahead of print. [Google Scholar] [CrossRef]
- Long, Y.; Huang, J.; Liao, J.; Zhang, D.; Huang, Z.; He, X.; Zhang, L. Safety and Survival Outcomes of Liver Resection following Triple Combination Conversion Therapy for Initially Unresectable Hepatocellular Carcinoma. Cancers 2023, 15, 5878. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| BCLC B Subclassification | Function | Tumor Burden | Others | |
|---|---|---|---|---|
| Bolondi criteria | B1 | CP 5–7 | Up-to-7 In | PS 0 |
| B2 | CP 5–6 | Up-to-7 Out | PS 0 | |
| B3 | CP 7 | Up-to-7 Out | PS 0 | |
| B4 | CP 8–9 | Up-to-7 any | PS 0–1 | |
| Yamakado criteria | B1 | CP A | N 4–7 cm In | |
| B2 | CP A | N 4–7 cm Out | ||
| B3 | CP B | N 4–7 cm In | ||
| B4 | CP B | N 4–7 cm Out | ||
| Kinki criteria | B1 | CP 5–7 | Up-to-7 In | |
| B2 | CP 5–7 | Up-to-7 Out | ||
| B3 | CP 8–9 | Up-to-7 any | ||
| Wang criteria | B1 | CP 5–7 | Up-to-7 In | AFP < 200 |
| B2 | CP 5–7 | Up-to-7 In | AFP > 200 | |
| CP 5–6 | Up-to-7 Out | AFP < 200 | ||
| B3 | CP 5–6 | Up-to-7 Out | AFP > 200 | |
| CP 7 | Up-to-7 Out | AFP any | ||
| Lee criteria | B1 | CP any | 5 cm In | |
| B2 | CP A | 5 cm Out | ||
| B3 | CP B | 5 cm Out | ||
| Kim criteria | B1 | CP A | Up-to 11 In | |
| B2 | CP A | Up-to 11 Out | ||
| CP B | Up-to 11 In | |||
| B3 | CP B | Up-to 11 Out | ||
| Kimura criteria | B1 | Up-to-7 In | DCP < 150–AFP any | |
| B2 | Other than those included in B1 and B3 | |||
| B3 | Up-to-7 Out | DCP any–AFP > 100 | ||
| Variable | Variable | ||
|---|---|---|---|
| Male sex | 137 (80.1%) | N° nodules | 5.8 ± 3.4 |
| Age (years) | 69.0 ± 9.1 | Largest nodule size (cm) | 5.0 ± 3.7 |
| Viral etiology | 121 (70.8%) | Largest nodule < 5 cm | 5.0 ± 3.7 |
| Child–Pugh B | 13 (7.6%) | N4-S7 In | 59 (34.5%) |
| AFP (ng/mL) | 1561 ± 5531 | Up-to-7 In | 46 (26.9%) |
| AFP < 200 (ng/mL) | 116 (67.8%) | Up to-11 In | 87 (50.9%) |
| Variable | OS, mo (95% CI) | Hazard Ratio (95% CI) | p |
|---|---|---|---|
| Male sex | 13.5 (10.6–16.3) vs. 11.9 (4.2–19.6) | 0.833 (0.558–1.245) | 0.373 |
| Viral etiology | 13.5 (9.7–17.2) vs. 12.6 (7.7–17.4) | 0.847 (0.604–1.189) | 0.338 |
| Child–Pugh B | 6.8 (4.8–8.8) vs. 13.5 (9.8–17.1) | 1.673 (0.926–3.024) | 0.088 |
| AFP > 200 | 8.6 (5.1–12.0) vs. 16.1 (10.2–22.0) | 1.405 (1.000–1.974) | 0.050 |
| Largest nodule > 5 cm | 10.0 (6.9–13.2) vs. 16.7 (10.5–22.8) | 1.526–1.099–2.118) | 0.012 |
| N4-S7 Out | 11.4 (9.7–13.1) vs. 20.1 (12.4–27.9) | 1.465 (1.051–2.042) | 0.024 |
| Up-to-7 Out | 11.3 (9.7–13.0) vs. 22.5 (17.9–27.1) | 2.069 (1.418–3.018) | <0.001 |
| Up to-11 Out | 11.3 (9.3–13.4) vs. (16.7 (10.1–23.3) | 1.422 (1.038–1.947) | 0.028 |
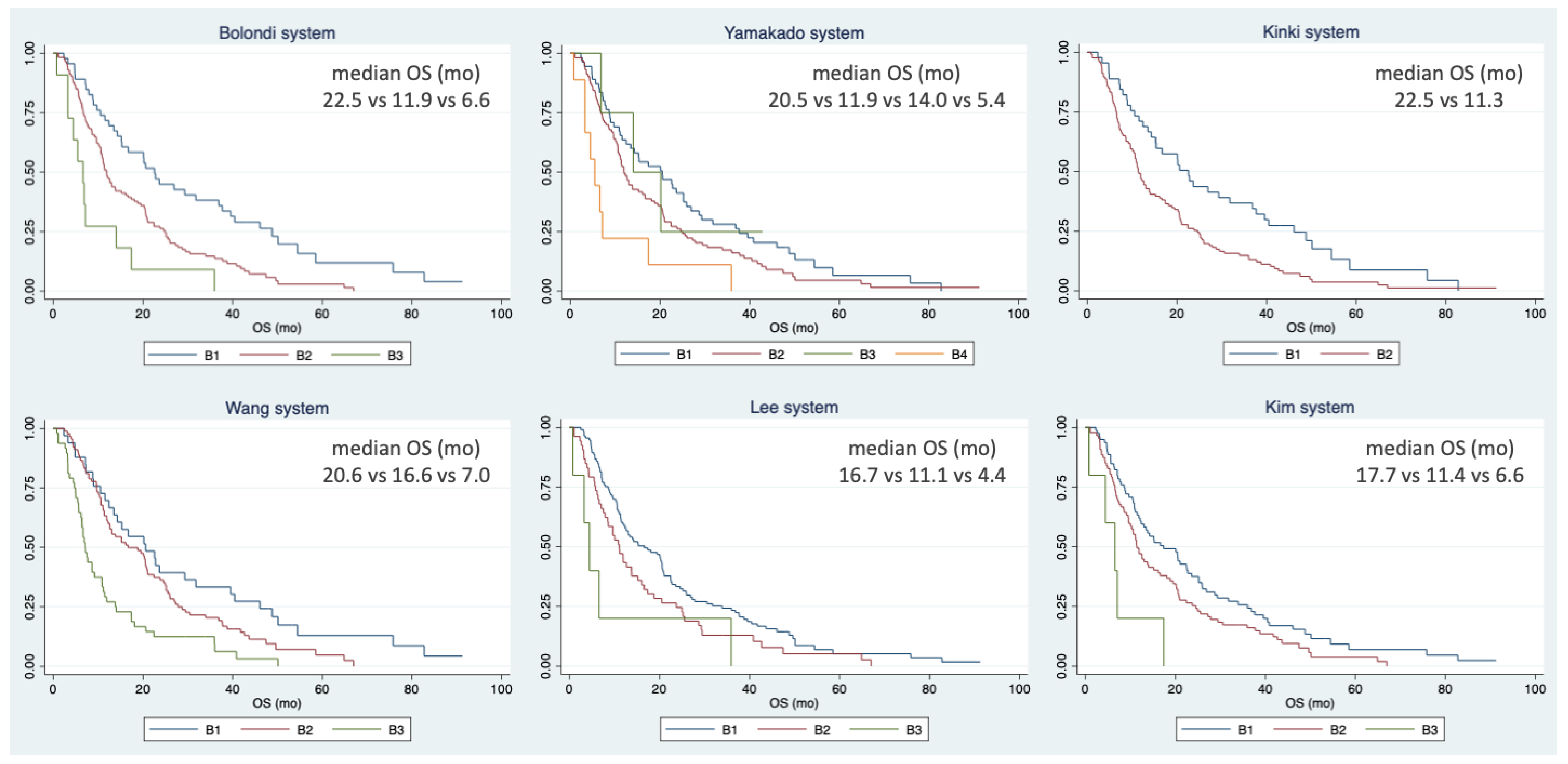
| BCLC B Subclassification | n | OS, mo (95% CI) | HR (95% CI) | p | |
|---|---|---|---|---|---|
| Bolondi criteria | B1 | 46 (26.9%) | 22.5 (17.9–27.1) | Ref. | |
| B2 | 114 (66.7%) | 11.9 (10.2–13.6) | 1.981 (1.352–2.901) | <0.001 | |
| B3 | 11 (6.4%) | 6.6 (4.0–9.1) | 4.248 (2.132–8.461) | <0.001 | |
| Yamakado criteria | B1 | 55 (32.2%) | 20.5 (11.8–29.2) | Ref. | |
| B2 | 103 (60.2%) | 11.9 (10.2–13.6) | 1.394 (0.988–1.966) | 0.058 | |
| B3 | 4 (2.3%) | 14.0 (0.9–27.0) | 0.970 (0.302–3.118) | 0.959 | |
| B4 | 9 (5.3%) | 5.4 (2.5–8.3) | 3.342 (1.628–6.861) | 0.001 | |
| Kinki criteria | B1 | 45 (26.3%) | 22.5 (18.0–27.1) | Ref. | |
| B2 | 126 (73.7%) | 11.3 (9.7–12.9) | 1.784 (1.236–2.575) | 0.002 | |
| Wang criteria | B1 | 33 (19.3%) | 20.6 (12.2–29.0) | Ref. | |
| B2 | 90 (52.6%) | 16.6 (9.8–23.3) | 1.484 (0.959–2.297) | 0.077 | |
| B3 | 48 (28.1%) | 7.0 (5.8–8.3) | 2.983 (1.834–4.854) | <0.001 | |
| Lee criteria | B1 | 113 (66.1%) | 16.7 (10.5–22.8) | Ref. | |
| B2 | 53 (31.0%) | 11.1 (8.1–14.0) | 1.461 (1.042–2.049) | 0.028 | |
| B3 | 5 (2.9%) | 4.4 (1.9–6.9) | 2.788 (1.130–6.878) | 0.026 | |
| Kim criteria | B1 | 79 (46.2%) | 17.3 (10.9–23.7) | Ref. | |
| B2 | 87 (50.9%) | 11.4 (9.4–13.4) | 1.414 (1.026–1.950) | 0.034 | |
| B3 | 5 (2.9%) | 6.6 (2.0–11.2) | 4.023 (1.600–10.116) | 0.003 | |
| BCLC B Subclassification | Harrel C-Index | AIC | BIC |
|---|---|---|---|
| Bolondi criteria | 0.586 | 1338 | 1344 |
| Yamakado criteria | 0.566 | 1350 | 1360 |
| Kinki criteria | 0.563 | 1346 | 1349 |
| Wang criteria | 0.607 | 1337 | 1344 |
| Lee criteria | 0.563 | 1351 | 1357 |
| Kim criteria | 0.560 | 1349 | 1356 |
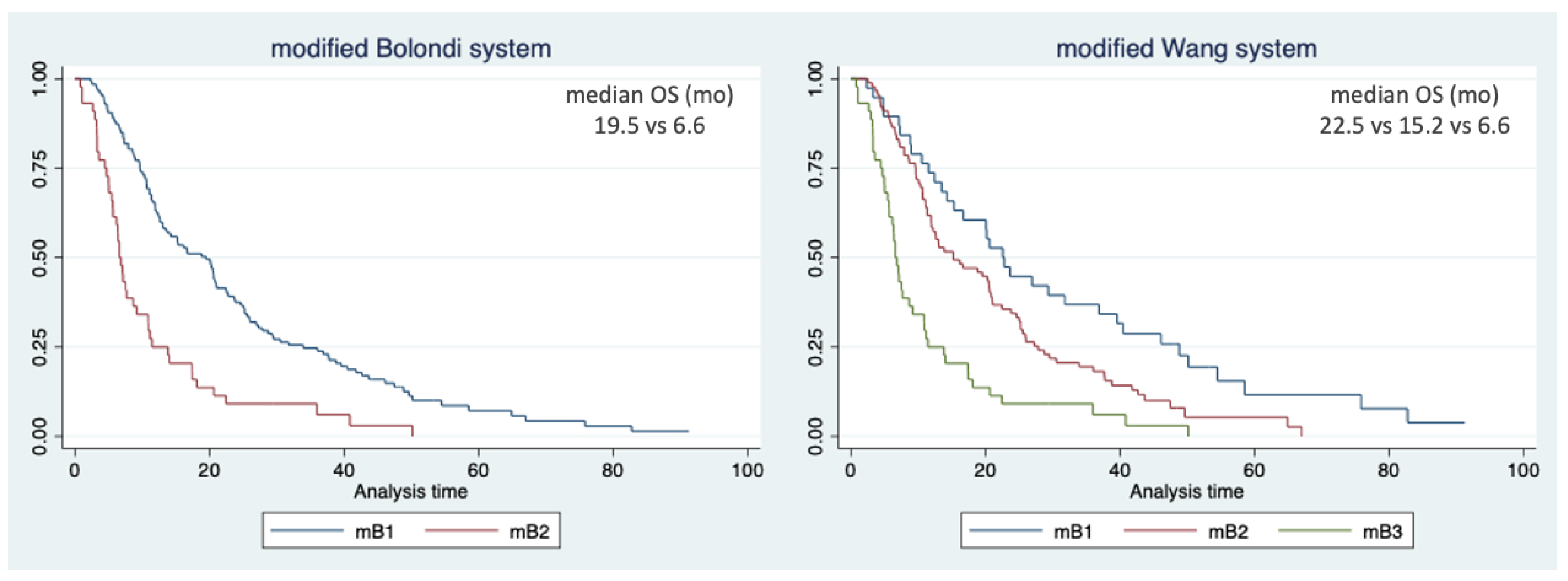
| BCLC B Subclassification | n | OS, mo (95% CI) | HR (95% CI) | p | |
|---|---|---|---|---|---|
| Modified Bolondi criteria | mB1 | 127 (74.3%) | 19.5 (14.9–24.0) | Ref. | |
| mB2 | 44 (25.7%) | 6.6 (5.7–7.4) | 2.530 (1.765–3.626) | <0.001 | |
| Modified Wang criteria | mB1 | 38 (22.2%) | 22.5 (17.3–27.8) | Ref. | |
| mB2 | 89 (52.0%) | 15.2 (8.2–22.1) | 1.635 (1.077–2.483) | 0.021 | |
| mB3 | 44 (25.7%) | 6.6 (5.7–7.4) | 3.564 (2.216–5.732) | <0.001 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ielasi, L.; Stefanini, B.; Conti, F.; Tonnini, M.; Tortora, R.; Magini, G.; Sacco, R.; Pressiani, T.; Trevisani, F.; Foschi, F.G.; et al. Comparative Analysis of Subclassification Systems in Patients with Intermediate-Stage Hepatocellular Carcinoma (Barcelona Clinic Liver Classification B) Receiving Systemic Therapy. Curr. Oncol. 2024, 31, 547-557. https://doi.org/10.3390/curroncol31010038
Ielasi L, Stefanini B, Conti F, Tonnini M, Tortora R, Magini G, Sacco R, Pressiani T, Trevisani F, Foschi FG, et al. Comparative Analysis of Subclassification Systems in Patients with Intermediate-Stage Hepatocellular Carcinoma (Barcelona Clinic Liver Classification B) Receiving Systemic Therapy. Current Oncology. 2024; 31(1):547-557. https://doi.org/10.3390/curroncol31010038
Chicago/Turabian StyleIelasi, Luca, Bernardo Stefanini, Fabio Conti, Matteo Tonnini, Raffaella Tortora, Giulia Magini, Rodolfo Sacco, Tiziana Pressiani, Franco Trevisani, Francesco Giuseppe Foschi, and et al. 2024. "Comparative Analysis of Subclassification Systems in Patients with Intermediate-Stage Hepatocellular Carcinoma (Barcelona Clinic Liver Classification B) Receiving Systemic Therapy" Current Oncology 31, no. 1: 547-557. https://doi.org/10.3390/curroncol31010038