
Non-Pharmacological Interventions for Type 2 Diabetes in People Living with Severe Mental Illness: Results of a Systematic Review and Meta-Analysis
 ,
, 
Abstract
:1. Introduction
1.1. Description of the Intervention
1.2. How the Interventions Might Work
1.3. Why This Review Is Important
2. Methods
2.1. Search Strategy
- Studies Included
- Studies Excluded
- Participants/Population
- Intervention(s) and Exposure(s) Include:
- Comparator(s)/Control:
- Context:
- Outcomes of Interest:
- Primary outcomes were:
- Glycaemic control: glycated haemoglobin, fasting blood glucose;
- Psychiatric symptoms: reduction in self-harm, anxiety, and depression;
- Quality of life (QoL).
- Secondary outcomes included:
- Lipid profile—low-density lipoprotein (LDL) cholesterol, high-density lipoprotein (HDL) cholesterol, triglycerides, and total cholesterol;
- Body mass index (BMI).
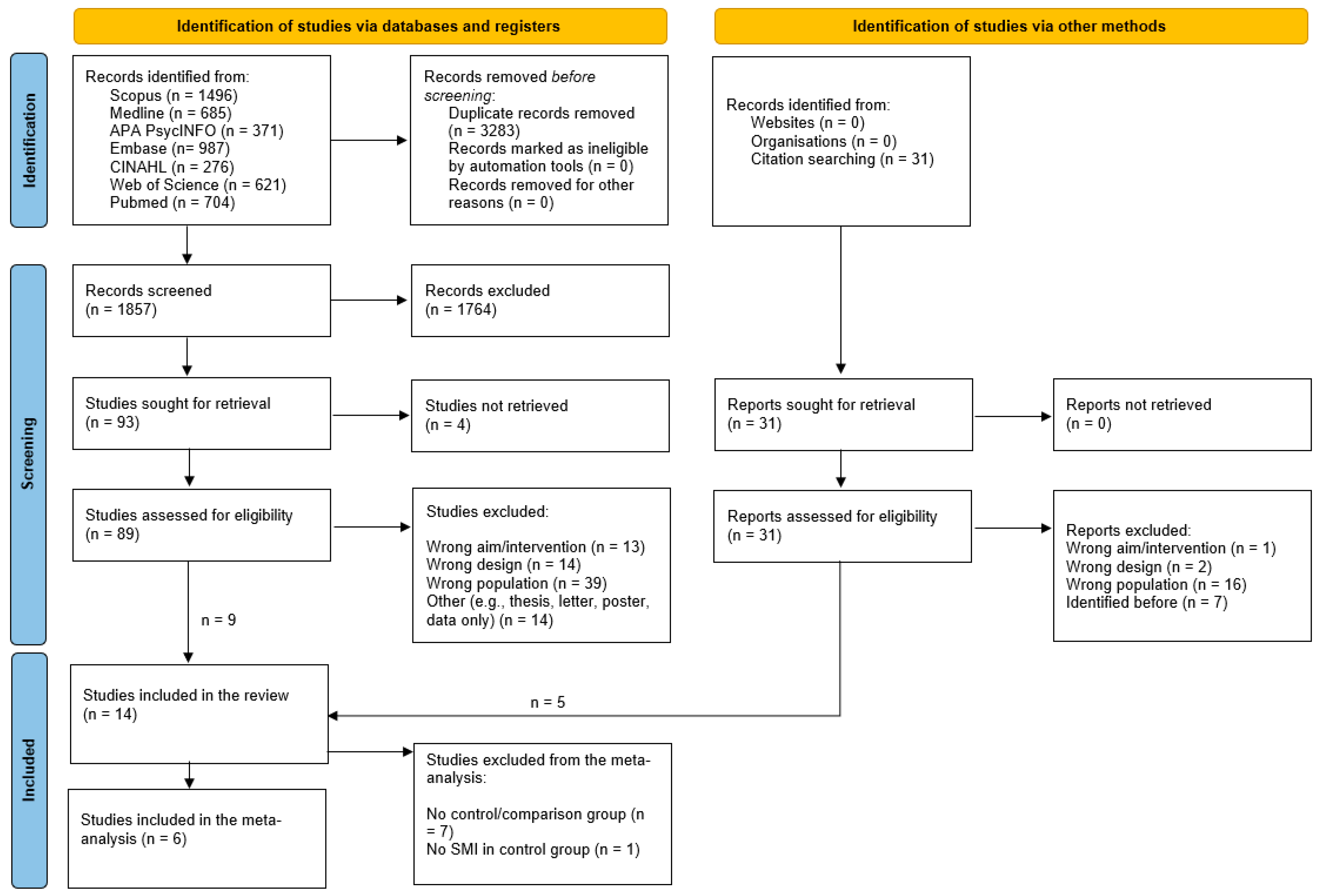
2.2. Study Selection Process
2.3. Data Extraction, Quality Appraisal, and Risk of Bias Assessment
2.4. Meta-Analysis
3. Results
3.1. Descriptive Results and Results of the Systematic Review
3.2. Qualitative Synthesis and Meta-Analysis Results
- Glycaemic control;
- Psychiatric symptoms;
- Health-related quality of life;
- Lipid profile;
- Body mass index.
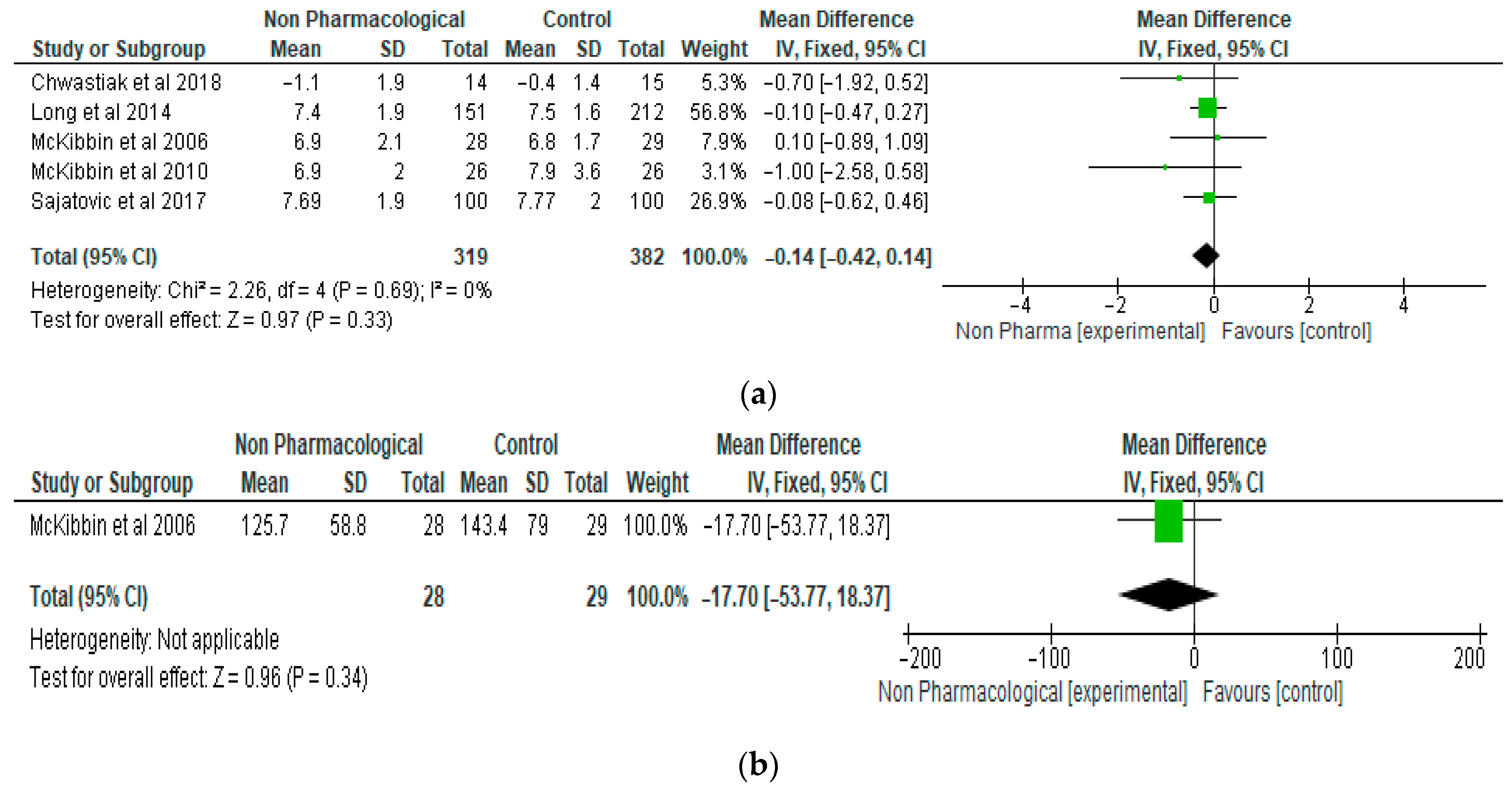
3.3. Glycaemic Control
3.4. Psychiatric Symptoms
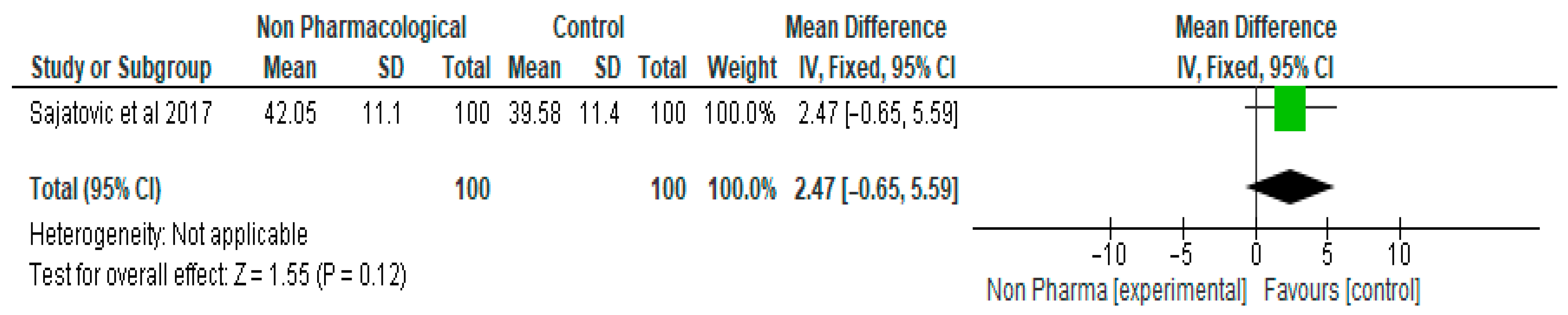
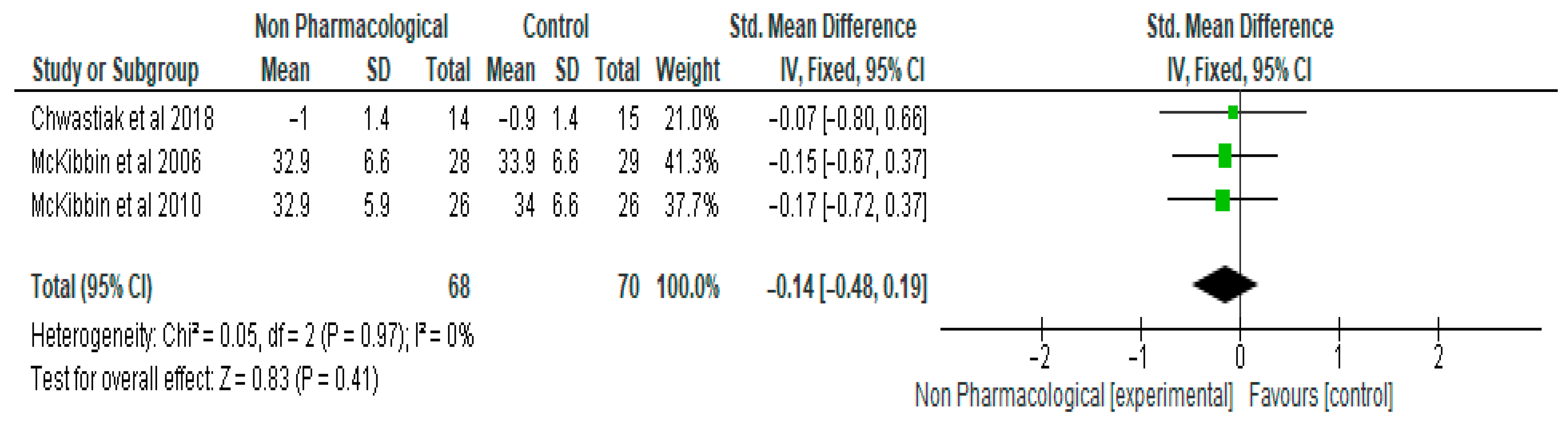
3.5. Health-Related Quality of Life (HRQL)
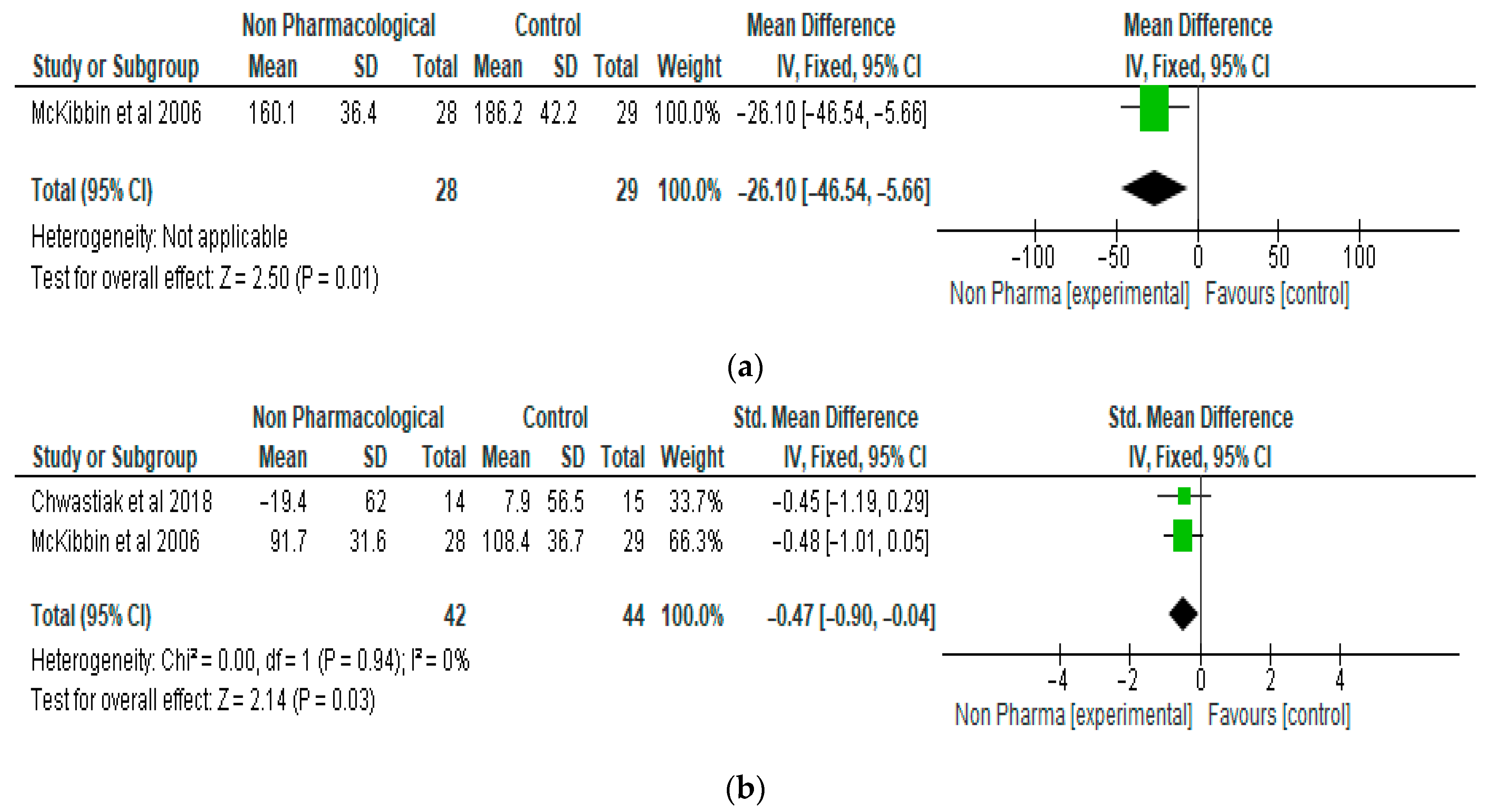
3.6. Lipid Profile
3.7. Body Mass Index (BMI)
4. Discussion
4.1. Association between SMI and Obesity
4.2. The Effects of Psychotropic Medications on Obesity, Type 2 Diabetes, and Other Metabolic Abnormalities
4.3. Limitations of the Review
4.4. Implications for Clinical Practice
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sun, H.; Saeedi, P.; Karuranga, S.; Pinkepank, M.; Ogurtsova, K.; Duncan, B.B.; Stein, C.; Basit, A.; Chan, J.C.; Mbanya, J.C.; et al. IDF Diabetes Atlas: Global, regional and country-level diabetes prevalence estimates for 2021 and projections for 2045. Diabetes Res. Clin. Pract. 2022, 183, 109119. [Google Scholar] [CrossRef]
- Ong, K.L.; Stafford, L.K.; McLaughlin, S.A.; Boyko, E.J.; Vollset, S.E.; Smith, A.E.; Dalton, B.E.; Duprey, J.; Cruz, J.A.; Hagins, H.; et al. Global, regional, and national burden of diabetes from 1990 to 2021, with projections of prevalence to 2050: A systematic analysis for the Global Burden of Disease Study 2021. Lancet 2023, 402, 203–234. [Google Scholar] [CrossRef]
- Nanda, M.; Sharma, R.; Mubarik, S.; Aashima, A.; Zhang, K. Type-2 Diabetes Mellitus (T2DM): Spatial-temporal Patterns of Incidence, Mortality and Attributable Risk Factors from 1990 to 2019 among 21 World Regions. Endocrine 2022, 77, 444–454. [Google Scholar] [CrossRef]
- Safiri, S.; Karamzad, N.; Kaufman, J.S.; Bell, A.W.; Nejadghaderi, S.A.; Sullman, M.J.M.; Moradi-Lakeh, M.; Collins, G.; Kolahi, A.-A. Prevalence, Deaths and Disability-Adjusted-Life-Years (DALYs) Due to Type 2 Diabetes and Its Attributable Risk Factors in 204 Countries and Territories, 1990-2019: Results from the Global Burden of Disease Study 2019. Front. Endocrinol. 2022, 13, 838027. [Google Scholar] [CrossRef]
- Mazereel, V.; Detraux, J.; Vancampfort, D.; van Winkel, R.; De Hert, M. Impact of Psychotropic Medication Effects on Obesity and the Metabolic Syndrome in People with Serious Mental Illness. Front. Endocrinol. 2020, 11, 573479. [Google Scholar] [CrossRef]
- DE Hert, M.; Correll, C.U.; Bobes, J.; Cetkovich-Bakmas, M.; Cohen, D.; Asai, I.; Detraux, J.; Gautam, S.; Möller, H.; Ndetei, D.M.; et al. Physical illness in patients with severe mental disorders. I. Prevalence, impact of medications and disparities in health care. World Psychiatry 2011, 10, 52–77. [Google Scholar] [CrossRef]
- Cimo, A.; Stergiopoulos, E.; Cheng, C.; Bonato, S.; Dewa, C.S. Effective lifestyle interventions to improve type II diabetes self-management for those with schizophrenia or schizoaffective disorder: A systematic review. BMC Psychiatry 2012, 12, 24. [Google Scholar] [CrossRef]
- Tuudah, E.; Foye, U.; Donetto, S.; Simpson, A. Non-Pharmacological Integrated Interventions for Adults Targeting Type 2 Diabetes and Mental Health Comorbidity: A Mixed-Methods Systematic Review. Int. J. Integr. Care 2022, 22, 27. [Google Scholar] [CrossRef]
- Grøn, A.; Dalsgaard, E.-M.; Ribe, A.; Seidu, S.; Mora, G.; Cebrián-Cuenca, A.; Charles, M. Improving diabetes care among patients with severe mental illness: A systematic review of the effect of interventions. Prim. Care Diabetes 2018, 12, 289–304. [Google Scholar] [CrossRef] [PubMed]
- Cimo, A.; Dewa, C.S. Symptoms of Mental Illness and Their Impact on Managing Type 2 Diabetes in Adults. Can. J. Diabetes 2018, 42, 372–381. [Google Scholar] [CrossRef] [PubMed]
- Wykes, T.L.; Lee, A.A.; Bourassa, K.; Kitchen, K.A.; McKibbin, C.L. Diabetes Knowledge Among Adults with Serious Mental Illness and Comorbid Diabetes Mellitus. Arch. Psychiatr. Nurs. 2017, 31, 190–196. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Moher, D. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews Systematic reviews and Meta-Analyses. BMJ 2021, 372, 71. [Google Scholar] [CrossRef]
- Ouzzani, M.; Hammady, H.; Fedorowicz, Z.; Elmagarmid, A. Rayyan—A web and mobile app for systematic reviews. Syst. Rev. 2016, 5, 210. [Google Scholar] [CrossRef]
- Public Health England. Severe Mental Illness (SMI) and Physical Health Inequalities: Briefing. 2018. Available online: https://www.gov.uk/government/publications/severe-mental-illness-smi-physical-health-inequalities/severe-mental-illness-and-physical-health-inequalities-briefing#:~:text=The%20phrase%20severe%20mental%20illness,an%20SMI%20%5Bfootnote%201%5D (accessed on 12 December 2022).
- Guyatt, G.H.; Oxman, A.D.; Vist, G.E.; Kunz, R.; Falck-Ytter, Y.; Alonso-Coello, P.; Schünemann, H.J. GRADE: An emerging consensus on rating quality of evidence and strength of recommendations. BMJ 2008, 336, 924–926. [Google Scholar] [CrossRef]
- Higgins, J.P.T.; Green, S. Cochrane Handbook for Systematic Reviews of Interventions; Wiley-Blackwell: Hoboken, NJ, USA, 2009; p. 31. [Google Scholar]
- The Nordic Cochrane Centre. Review Manager, Version 5.3; The Cochrane Collaboration: Copenhagen, Denmark, 2014. [Google Scholar]
- Aftab, A.; Bhat, C.; Gunzler, D.; Cassidy, K.; Thomas, C.; McCormick, R.; Dawson, N.V.; Sajatovic, M. Associations among comorbid anxiety, psychiatric symptomatology, and diabetic control in a population with serious mental illness and diabetes: Findings from an interventional randomized controlled trial. Int. J. Psychiatry Med. 2018, 53, 126–140. [Google Scholar] [CrossRef]
- Chwastiak, L.A.; Luongo, M.; Russo, J.; Johnson, L.; Lowe, J.M.; Hoffman, G.; McDonell, M.G.; Wisse, B. Use of a Mental Health Center Collaborative Care Team to Improve Diabetes Care and Outcomes for Patients with Psychosis. Psychiatr. Serv. 2018, 69, 349–352. [Google Scholar] [CrossRef]
- Cimo, A.; Loong, D.; Dewa, C.S. Exploring the Outcomes of a Pilot Education Program Tailored for Adults with Type 2 Diabetes and Mental Illness in a Community Mental Health Care Setting. Can. J. Diabetes 2020, 44, 461–472.e1. [Google Scholar] [CrossRef]
- Lindenmayer, J.-P.; Khan, A.; Wance, D.; Maccabee, N.; Kaushik, S.; Kaushik, S. Outcome evaluation of a structured educational wellness program in patients with severe mental illness. J. Clin. Psychiatry 2009, 70, 13562. [Google Scholar] [CrossRef]
- Long, J.A.; Wang, A.; Medvedeva, E.L.; Eisen, S.V.; Gordon, A.J.; Kreyenbuhl, J.; Marcus, S.C. Glucose Control and Medication Adherence Among Veterans with Diabetes and Serious Mental Illness: Does Collocation of Primary Care and Mental Health Care Matter? Diabetes Care 2014, 37, 2261–2267. [Google Scholar] [CrossRef] [PubMed]
- McKibbin, C.L.; Patterson, T.L.; Norman, G.; Patrick, K.; Jin, H.; Roesch, S.; Mudaliar, S.; Barrio, C.; O’Hanlon, K.; Griver, K.; et al. A lifestyle intervention for older schizophrenia patients with diabetes mellitus: A randomized controlled trial. Schizophr. Res. 2006, 86, 36–44. [Google Scholar] [CrossRef] [PubMed]
- McKibbin, C.L.; Golshan, S.; Griver, K.; Kitchen, K.; Wykes, T.L. A healthy lifestyle intervention for middle-aged and older schizophrenia patients with diabetes mellitus: A 6-month follow-up analysis. Schizophr. Res. 2010, 121, 203–206. [Google Scholar] [CrossRef]
- Morello, C.M.; Nguyen, T.; Tao, L.; Hirsch, J.D. Improved Glycemic Control Outcomes Regardless of Mental Health Disorders in a Pharmacist-Endocrinologist Diabetes Intense Medical Management (DIMM) “Tune Up” Clinic. Ann. Pharmacother. 2020, 54, 858–865. [Google Scholar] [CrossRef]
- Pratt, S.I.; Bartels, S.J.; Mueser, K.T.; Naslund, J.A.; Wolfe, R.; Pixley, H.S.; Josephson, L. Feasibility and effectiveness of an automated telehealth intervention to improve illness self-management in people with serious psychiatric and medical disorders. Psychiatr. Rehabil. J. 2013, 36, 297–305. [Google Scholar] [CrossRef]
- Sajatovic, M.; Dawson, N.V.; Perzynski, A.T.; Blixen, C.E.; Bialko, C.S.; McKibbin, C.L.; Bauer, M.S.; Seeholzer, E.L.; Kaiser, D.; Fuentes-Casiano, E. Best Practices: Optimizing Care for People with Serious Mental Illness and Comorbid Diabetes. Psychiatr. Serv. 2011, 62, 1001–1003. [Google Scholar] [CrossRef]
- Sajatovic, M.; Gunzler, D.D.; Kanuch, S.W.; Cassidy, K.A.; Tatsuoka, C.; McCormick, R.; Blixen, C.E.; Perzynski, A.T.; Einstadter, D.; Thomas, C.L.; et al. A 60-Week Prospective RCT of a Self-Management Intervention for Individuals with Serious Mental Illness and Diabetes Mellitus. Psychiatr. Serv. 2017, 68, 883–890. [Google Scholar] [CrossRef]
- Teachout, A.; Kaiser, S.M.; Wilkniss, S.M.; Moore, H. Paxton House: Integrating mental health and diabetes care for people with serious mental illnesses in a residential setting. Psychiatr. Rehabil. J. 2011, 34, 324–327. [Google Scholar] [CrossRef]
- Chiverton, P.; Lindley, P.; Tortoretti, D.M.; Plum, K.C. Well Balanced: 8 Steps to Wellness for Adults with Mental Illness and Diabetes. J. Psychosoc. Nurs. Ment. Health Serv. 2007, 45, 46–55. [Google Scholar] [CrossRef]
- Tseng, E.; Dalcin, A.T.; Jerome, G.J.; Gennusa, J.V.; Goldsholl, S.; Cook, C.; Appel, L.J.; Maruthur, N.M.; Daumit, G.L.; Wang, N.-Y. Effect of a Behavioral Weight Loss Intervention in People with Serious Mental Illness and Diabetes. Diabetes Care 2019, 42, 804–809. [Google Scholar] [CrossRef]
- Pendlebury, J.; Holt, R. Supporting the lifestyle modification and treatment of type 2 diabetes for people with severe mental illness. Eur. Diabetes Nurs. 2008, 5, 58–63. [Google Scholar] [CrossRef]
- Atyabi, V.C.; Kreider, K.E. Screening for Diabetes and Self-Care in Patients with Severe Mental Illness. J. Nurse Pract. 2020, 16, e5–e8. [Google Scholar] [CrossRef]
- Wang, H.-I.; Han, L.; Jacobs, R.; Doran, T.; Holt, R.I.G.; Prady, S.L.; Gilbody, S.; Shiers, D.; Alderson, S.; Hewitt, C.; et al. Healthcare resource use and costs for people with type 2 diabetes mellitus with and without severe mental illness in England: Longitudinal matched-cohort study using the Clinical Practice Research Datalink. Br. J. Psychiatry 2022, 221, 402–409. [Google Scholar] [CrossRef] [PubMed]
- Toender, A.; Vestergaard, M.; Munk-Olsen, T.; Larsen, J.T.; Kristensen, J.K.; Laursen, T.M. Risk of diabetic complications and subsequent mortality among individuals with schizophrenia and diabetes—A population-based register study. Schizophr. Res. 2020, 218, 99–106. [Google Scholar] [CrossRef] [PubMed]
- Sánchez-Ortí, J.V.; Balanzá-Martínez, V.; Correa-Ghisays, P.; Selva-Vera, G.; Vila-Francés, J.; Magdalena-Benedito, R.; San-Martin, C.; Victor, V.M.; Escribano-Lopez, I.; Hernández-Mijares, A.; et al. Specific metabolic syndrome components predict cognition and social functioning in people with type 2 diabetes mellitus and severe mental disorders. Acta Psychiatr. Scand. 2022, 146, 215–226. [Google Scholar] [CrossRef] [PubMed]
- Holt, R.I.G.; Peveler, R.C.; Byrne, C.D. Schizophrenia, the metabolic syndrome and diabetes. Diabet. Med. 2004, 21, 515–523. [Google Scholar] [CrossRef] [PubMed]
- de Bartolomeis, A.; De Simone, G.; De Prisco, M.; Barone, A.; Napoli, R.; Beguinot, F.; Billeci, M.; Fornaro, M. Insulin effects on core neurotransmitter pathways involved in schizophrenia neurobiology: A meta-analysis of preclinical studies. Implications for the treatment. Mol. Psychiatry 2023, 28, 2811–2825. [Google Scholar] [CrossRef] [PubMed]
- Kızılay, D.; Sapmaz, Y.; Şen, S.; Özkan, Y.; Ersoy, B. Insulin Resistance is Related to Psychiatric Disorders Among Obese Children. J. Clin. Res. Pediatr. Endocrinol. 2018, 10, 364–372. [Google Scholar] [CrossRef]
- Rønne, S.T.; Joensen, L.E.; Zabell, V.; Arnfred, S.M.; Brown, J.V.E.; Jørgensen, R. Schizophrenia and type 2 diabetes: Perceptions and understandings of illness management in everyday life. Int. J. Ment. Health Nurs. 2023, 32, 893–903. [Google Scholar] [CrossRef]
- Knyahnytska, Y.; Williams, C.; Dale, C.; Webster, F. Changing the Conversation: Diabetes Management in Adults with Severe Mental Illnesses and Type 2 Diabetes. Can. J. Diabetes 2018, 42, 595–602. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Citation/Country of Study | Study Design and Duration | Aim | Population/Participant Details | Sample Size | Intervention | Comparator | Results | Grade Rating (Overall) |
|---|---|---|---|---|---|---|---|---|
| Aftab et al. [18], 2018 USA | Secondary analysis of data from a prospective, 60-week RCT. | Examines the impact of comorbid anxiety on baseline psychiatric symptomatology and diabetic control, and on longitudinal treatment outcomes. | Individuals with SMI and T2D; 47% of the participants also had one or more anxiety disorders with GAD being the most common in the study population. No demographic information provided. | n = 200 | Targeted Training in Illness Management (TTIM), group-based self-management training approach to target SMI and T2D concurrently. Includes 12 weekly, in-person group sessions co-delivered by a nurse educator and peer educator plus short telephone maintenance sessions over 48 weeks. | Treatment as usual (TAU). | At baseline, those with an anxiety diagnosis had higher illness severity, as well as depressive and other psychiatric symptomatology. Diabetic control (HbA1c) was not significantly different at baseline. In the longitudinal analyses, those with anxiety disorders in the TTIM group had significantly greater improvement in mental health functioning; in the same group, those with anxiety comorbidity demonstrated significantly lower HbA1c levels compared to no anxiety comorbidity and also demonstrated a greater improvement in HbA1c over the first 30 weeks compared to those without anxiety comorbidity. | Moderate |
| Chwastiak et al. [19], 2018 USA | 3-month RCT pilot study. | Evaluates the feasibility, acceptability, and preliminary effectiveness of a collaborative care model compared with usual care in CMHC. | Community mental health centre (CMHC) people with psychosis and poorly controlled T2D. MH diagnoses: Schizophrenia or schizoaffective disorder (40%); other diagnoses included bipolar disorder and major depressive disorder with psychosis. Mean age: 51 (18–64). | n = 35 (18 intervention group, 17 usual care) | Collaborative care provided by a CMHC-based team that included a nurse care manager, psychiatrist, advanced practice registered nurse, and an endocrinologist consultant. Participants had a comprehensive health assessment, individualised health plan, and 30-min visits to support illness self-management every other week for 12 weeks. | Usual care: Usual mental health treatment through CMHC and usual medical care for diabetes. | People in the intervention group had a statistically significant mean decrease in HbA1c of 1.1% (p = 0.049) after 3 months. There was no significant change in HbA1c in the usual-care group. The pilot also demonstrated the feasibility and acceptability of the intervention. | Low: Selection bias, effect estimate comes from a small sample; implementation modified based on MH diagnosis; results may not be transferable to a different healthcare setting; funding information not disclosed. |
| Cimo et al. [20], 2020 Canada | Pilot study: interviews combined with quantitative data analysis. Intervention was delivered over a year. | Explores the outcomes of a diabetes education intervention tailored to the learning needs of people with SMI. | Individuals with T2D (71%) or pre-diabetes (29%) and one or more mental illness diagnoses (defined as schizophrenia, schizoaffective disorder, bipolar disorder, or major depressive disorder). Mean age: 63 (11). 57% male; 71% Caucasian. | n = 7 | 12-session diabetes education programme provided by a registered dietitian, certified diabetes educator, and a mental health registered nurse. Focus on understanding diabetes, nutrition, exercise, and behaviours contributing to healthy lifestyle. | No comparator. | Blood sugar control and physical activity level improved for some participants and worsened for others. Weight remained stable; dietary intake patterns seemed to improve overall. Participants also reported an improved understanding about diabetes and gained self-management knowledge. | Very low: Observational; very small sample with a variety of MH diagnoses. |
| Lindenmayer et.al. [21], 2009 USA | Randomised, single-blind, uncontrolled study that used medical and laboratory results and data generated by two structured education programmes with people tested on knowledge assessment questions and metabolic markers recorded at baseline, midpoint, and endpoint over 36 weeks. | Evaluates the effectiveness of the Solutions for Wellness and Team Solutions programmes on obesity and other metabolic markers in a large, naturalistic inpatient sample. | Patients at a tertiary care psychiatric facility. Psychiatric diagnoses: Schizophrenia (62%), schizoaffective disorder (17%), bipolar disorder (14%), other (7%). Mean age: 42.94 (18.63–64.41). Male: 83%, Female: 17%. Ethnicity: Hispanic (22%), Asian (3%), White (8%), African American (65%), Other (2%). | n = 275 | Structured education programmes with mandatory group sessions for all inpatients. 1. Team Solutions: focus on symptoms of mental illness, recovery, and relapse prevention. 2. Solutions for Wellness: information on nutrition, fitness, and practicing exercise. | No comparator. | Knowledge assessment: Significant increases in scores were observed for 7 of the 11 modules. Weight: There was a significant mean weight loss of 4.88 lb (p = 0.035) together with a significant decrease in mean BMI (p = 0.045). People with diabetes showed a reduction in mean weight of 5.98 lb. Glucose and triglyceride levels: Significant reductions were observed (p = 0.000); 69 participants met the criteria for metabolic syndrome at the baseline, and this number was reduced to 53 participants at the endpoint. | Moderate |
| Long et.al. [22], 2014 USA | Cross-sectional, observational cohort study. | Evaluates and compares glucose control and diabetes medication adherence among people receiving collocated care vs. usual care. | Veterans with T2D and SMI receiving care from 3 Veteran Affairs medical facilities. 88% on psychiatric medication, 70% on antipsychotics, 53% on mood stabilising medication, 36% on both. Mean age: 59 (7). Male: 95%. Ethnicity: white (46%), Black (40%), and other (14%). Mean duration of diabetes: 10 (8). 59% on oral diabetes medication alone. | n = 363 (151 from collocated care, and 212 from usual care) | Collocated care Site 1: Integrates primary care professionals into MH clinics. Site 2: Collocates primary care healthcare professionals in a specialised site caring for veterans with mental illness. | Usual care. | No differences were observed in glucose control and medication adherence by collocation of care. People seen in collocated care tended to have better HbA1c levels (b = 20.149; p = 0.393) and MPR values (b = 0.34; p = 0.132) and worse self-reported medication adherence (odds ratio 0.71; p = 0.143), but these were not statistically significant. | Low: Observational; selection bias (veteran population); care delivery at different VA clinics—not sufficient information to assess consistency of care. |
| McKibbin et al. [23], 2006 USA | Randomised pre-test, post-test control group design to evaluate a 24-week lifestyle intervention; participants were evaluated at baseline and at 6 months. | Tests the feasibility and preliminary efficacy of a group-based lifestyle intervention for middle-aged and older people with schizophrenia and T2D. | People aged 40 or older with physician-confirmed diagnoses of schizophrenia and T2D. MH diagnosis: Schizophrenia (75%), schizoaffective disorder (25%). Age: 40–81 years. Male: 58%, female: 42%. Ethnicity: Caucasian 55%, other 45%. Diabetes duration: less than 10 years. | n = 64 (32 intervention group, 32 UCI group) | Diabetes Awareness and Rehabilitation Training (DART): 24 weekly, 90 min sessions with groups of 6–8 addressing diabetes education, nutrition, and lifestyle and exercise. | Usual care plus information (UCI). | A significant group × time interaction was observed for body weight, with people in the intervention group losing a mean of 5 lb, and those in the UCI gaining a mean 6 lb. Significant group × time interactions were also found for triglycerides, diabetes knowledge, diabetes self-efficacy, and self-reported physical activity, but not for fasting plasma glucose or glycosylated haemoglobin. | Moderate |
| McKibbin et al. [24], 2010 USA | Randomised pre-test, post-test control group design to evaluate a 24-week lifestyle intervention; participants were evaluated at baseline, at 6 months, and 12 months. Baseline and 12-month assessments were used for this follow-up analysis. | Evaluates the duration of treatment gains from the DART programme 6 months after intervention completion. | Participants who returned for assessments 6 months after completion of the intervention programme reported in McKibbin et al. (2006). For the sample characteristics—see above. | n = 52 (of the 64 original subjects) | Diabetes Awareness and Rehabilitation Training (DART): 24 weekly, 90 min sessions with groups of 6–8 addressing diabetes education, nutrition, and lifestyle and exercise. | Usual Care plus information (UCI). | The intervention group experienced significantly greater improvement in BMI and waist circumference from baseline to the 12-month follow up assessment than the control group. There were no changes in antipsychotic treatment type between 6 months and 12 months post-baseline. Likewise, few changes in diabetes treatment type occurred from baseline to 6 months and 12 months for either the DART or UCI groups. Significant group × time interactions were found for diabetes knowledge, with greater improvements observed for the DART group from baseline to 12 months. No group × time interactions were observed for A1C or energy expenditure. | Moderate |
| Morello et al. [25], 2020 USA | Retrospective cohort study in people with T2D divided into subgroups of those with ≥1 mental health (MH) diagnoses and without MH diagnoses in a 6-month Diabetes Intense Medical Management (DIMM) clinic programme. | Compares mean change in A1C after 6 months in the DIMM clinic in people with and without MH disorders. | People diagnosed with T2D who received care at the DIMM clinic. Diagnoses within the MH group: Depression (71%), GAD (20%), bipolar disorder (15%), schizophrenia (6%), PTSD (38%). Mean age = 61. Baseline demographics between the MH and non-MH groups were similar, except for race with a greater percentage being white people in the MH group (70%) compared with the non-MH group (52%). | n = 155 (66 MH group, 89 non-MH group) | People with at least 1 MH disorder (MH group). Both groups were treated at the DIMM clinic, which is a collaborative pharmacist-endocrinologist practice, to manage complex cases of T2D. The clinic used a tune-up model, coupling personalised clinical care with real-time, patient-specific diabetes and self-care education during an average of three 60 min visits. | People without MH diagnosis (non-MH group). | Mean A1C, fasting blood glucose (FBG), and triglycerides (TGs) change did not differ significantly between MH and non-MH groups at 6 months. Percentage at A1C goal did not differ significantly between the two groups; however, a higher percentage of the non-MH group achieved FBG and TG goals compared to the MH group. | Low: Non-randomised, exploratory, retrospective, single-clinic, veteran population; baseline imbalances; no information on how consistently the intervention was applied through the sample. |
| Pratt et al. [26], 2013 USA | Single-arm pilot trial of telehealth intervention delivered over 6 months. | Examines the feasibility and effectiveness of an automated telehealth intervention supported by a nurse care manager. | Adult participants at a community mental health centre. Psychiatric diagnoses: Schizophrenia (16%), bipolar disorder (17%), PTSD (26%), major depression (41%). Subgroup with T2D: 66%. Mean age: 52.7 (10.6). Male (23%), female (77%). Ethnicity: white. (99%), non-white (1%). | n = 70 | Automated telehealth intervention with daily, 5-to-10 min sessions with tailored questions regarding medical and psychiatric symptoms, vital signs, disease-specific health indicators, self-management knowledge, and health behaviours. Participant responses were arranged hierarchically based on risks and reviewed by a nurse, who contacted high- or moderate-risk participants by phone/sms to follow up. | No comparator. | The results demonstrated the feasibility and acceptability of the intervention, and its potential effectiveness in improving self-management of psychiatric symptoms and chronic health conditions. Among a subgroup of individuals with T2D, decreases in fasting blood glucose were achieved, and among those with T2D and major depression or bipolar disorder there were reductions in urgent care and primary care visits. | Moderate |
| Sajatovic et al. [27], 2011 USA | Prospective, uncontrolled, case-series pilot trial of a group-based psychosocial treatment delivered over 16 weeks. | Pilots the Targeted Training in Illness Management (TTIM) intervention. | Individuals with SMI and T2D. Baseline symptom scores suggested moderate degrees of psychopathology; almost 50% had poorly controlled diabetes (HbA1C > 8). Median age: 49.5 (33–62). 75% participants from racial-ethnic minority groups. | n = 12 | TTIM is a group-based psychosocial treatment that blends psychoeducation, problem identification, goal setting, behavioural modelling, and care linkage. The first phase consists of 12 weekly, 60-to-90 min group sessions co-led by a nurse educator and a peer educator with SMI and T2D; the second phase consists of telephone maintenance sessions. | No comparator. | The overall trend across most measures was toward clinically relevant improvement: a 15% mean reduction in BPRS and 48% mean reduction in MADRS scores, and a 7% improvement in SF-12 MCS and 15% improvement in SF-12 PCS scores. Weight and HbA1c did not show a statistically significant improvement over the 16 weeks, but the results for HbA1c were overall promising (improvement for 67% of participants). | Low: Uncontrolled study; effect estimate comes from small sample; selection bias; no sufficient data on implementation to judge consistency. |
| Sajatovic et al. [28], 2017 USA | A 60-week prospective RCT. | Assess the effects of the Targeted Training in Illness Management (TTIM) intervention versus usual care. | Individuals with SMI and T2D identified by clinicians and self-referral. MH diagnoses: Schizophrenia (25%), bipolar disorder (28%), major depressive disorder (48%). Duration of SMI: 18.5 years (12.6). Duration of diabetes: 10.1 years (7.8). Mean age: 52.7 (9.5). Female (64%). Race: Caucasian (37%), African American (54%), other (10%). | n = 200 (100 in the intervention group, 100 TAU) | See above Sajatovic et al. (2011) for the details of the intervention. | Treatment as usual (TAU). | At 60 weeks, there was greater improvement among the intervention group versus TAU recipients on the CGI (p<0.001), the MADRS (p = 0.016), and the GAF (p = 0.003). Diabetes knowledge was also significantly improved among TTIM participants but not in the TAU group. Among participants whose HbA1c levels at baseline suggested high comorbidity (53%), TTIM participants had minimal change in HbA1c over the 60-week follow-up, whereas HbA1c levels worsened in the TAU group. | Moderate |
| Teachout et al. [29], 2011 USA | Retrospective evaluation of a supported housing residence based on health outcome (weight, blood glucose levels) and satisfaction survey data. | Provides a programme description of a supported housing residence for individuals with co-occurring T2D and SMI. | Residents of supported housing (Paxton House) with co-occurring T2D and SMI. MH diagnoses: Schizophrenia (46%), schizoaffective disorder (31%), depression (15%), psychotic disorder (8%). Mean age: 45 (6.9). Male (77%). Ethnicity: Black/African American (69%), white/Caucasian (31%). | n = 13 | Supported housing providing comprehensive MH support, residential care, regular on-site diabetes education classes (weekly), nutrition counselling, and exercise instructions for residents. | No comparator. | Overall, the participants were satisfied with the diabetes education and monitoring provided. In the first 6 months of participation, they lost weight, and their fasting glucose readings fell into the ADA recommended range. | Very low: Observational; small sample; no control group; participants from one research site; no CI; not an independent evaluation (authors employed by the research sites); information on care accessible, but it is not clear in which activities each participant took part. |
| Tortoretti [30], 2007 USA | Evaluation of health outcome and client satisfaction questionnaire data (approximate duration of the intervention: 16 weeks). | Evaluates the effects of a novel nursing model (Well Balanced programme) on health risk status, diabetes self-management, and satisfaction with care. | Adults with diabetes and SMI who were regular clients in three local health care sites. MH diagnoses: Schizophrenia (46%), episodic mood disorder (49%), substance abuse (66%), personality disorder. 85% had T2D, and 15% T1D. Mean age = 46 (22–64). Female (68%), male (32%). Race: white (58%), Black (34%), other (8%). | n = 74 | 16 nursing intervention visits addressing client assessment, education, and support in major areas of wellness and diabetes self-management. | No comparator. | Overall, participants’ A1C levels declined significantly after the program (t = 2.61, df = 70, p < 0.05). Approximately 32% had A1C levels below 6% at the start of the program, compared with approximately 43% afterward. Mean health risk status also improved significantly from baseline to program completion (mean = 67, SD = 17) (t = –3.405, df = 73, p < 0.001). Overall, the participants were satisfied with the programme—mean satisfaction was 3.55 (SD = 0.44) on a 4-point scale, with scores ranging from 2 to 4. | Low: Observational; selection bias; recruitment from a few health centres; no CI intervals. |
| Tseng et al. [31], 2019 USA | Long-term RCT with data collected at baseline, and 6, 12, and 18 months. | Evaluates the effectiveness of a behavioural weight loss intervention for people with SMI separately, in those with T2D and without T2D, and explores potential heterogeneity of treatment effect between these two subgroups. | The trial recruited overweight/obese adults who attended a community outpatient psychiatric rehabilitation programme in Maryland. Of the 291 participants, 82 (28.2%) individuals had T2D. Psychiatric diagnoses: Schizophrenia (44%), schizoaffective disorder (26%), bipolar disorder (12%), major depression (14%), other (4%). Mean age: 48.4 (9.6). Race: white (55%), Black (40%), other (5%). | RCT n = 291 (144 in intervention group; 147 control group). Diabetes subgroup n = 82 (43 in intervention group; 48 in control). | ACHIEVE, a behavioural weight loss programme consisting of group weight management sessions, individual weight management sessions, and group exercise sessions. | Standard nutrition and physical activity information at baseline plus health classes offered quarterly. | At 18 months, participants in the control group with diabetes lost 1.2 lb (0.6%) of body weight compared with 0.8 lb (0.7%) among those without diabetes. In the intervention group, participants with diabetes lost 13.7 lb (6.6%) of their initial body weight compared with 5.4 lb (2.9%) for those without diabetes. Corresponding net effects were 4.6 lb (2.2%) and 12.5 lb (6.0%) net weight reduction over 18 months in the no diabetes and the diabetes subgroups, respectively; the between-group difference in intervention effects was not statistically significant. | Moderate |
| People with Type 2 Diabetes and SMI | ||||||
|---|---|---|---|---|---|---|
| Outcomes | Number of Studies | Number of Participants | Statistical Method | Weighted Difference (95% CI) | p-Value | I2% |
| Triglycerides | 2 | 86 | Standardised Mean Difference | −0.27 (−0.70, 0.15) | 0.21 | 0.0 |
| HDL cholesterol | 1 | 57 | Mean Difference | −03.90 (−9.23, 1.43) | 0.15 | 0.0 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ojo, O.; Kalocsányiová, E.; McCrone, P.; Elliott, H.; Milligan, W.; Gkaintatzi, E. Non-Pharmacological Interventions for Type 2 Diabetes in People Living with Severe Mental Illness: Results of a Systematic Review and Meta-Analysis. Int. J. Environ. Res. Public Health 2024, 21, 423. https://doi.org/10.3390/ijerph21040423
Ojo O, Kalocsányiová E, McCrone P, Elliott H, Milligan W, Gkaintatzi E. Non-Pharmacological Interventions for Type 2 Diabetes in People Living with Severe Mental Illness: Results of a Systematic Review and Meta-Analysis. International Journal of Environmental Research and Public Health. 2024; 21(4):423. https://doi.org/10.3390/ijerph21040423
Chicago/Turabian StyleOjo, Omorogieva, Erika Kalocsányiová, Paul McCrone, Helen Elliott, Wendy Milligan, and Evdoxia Gkaintatzi. 2024. "Non-Pharmacological Interventions for Type 2 Diabetes in People Living with Severe Mental Illness: Results of a Systematic Review and Meta-Analysis" International Journal of Environmental Research and Public Health 21, no. 4: 423. https://doi.org/10.3390/ijerph21040423