
Antidiabetic Drug Prescription Pattern in Hospitalized Older Patients with Diabetes
 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Setting
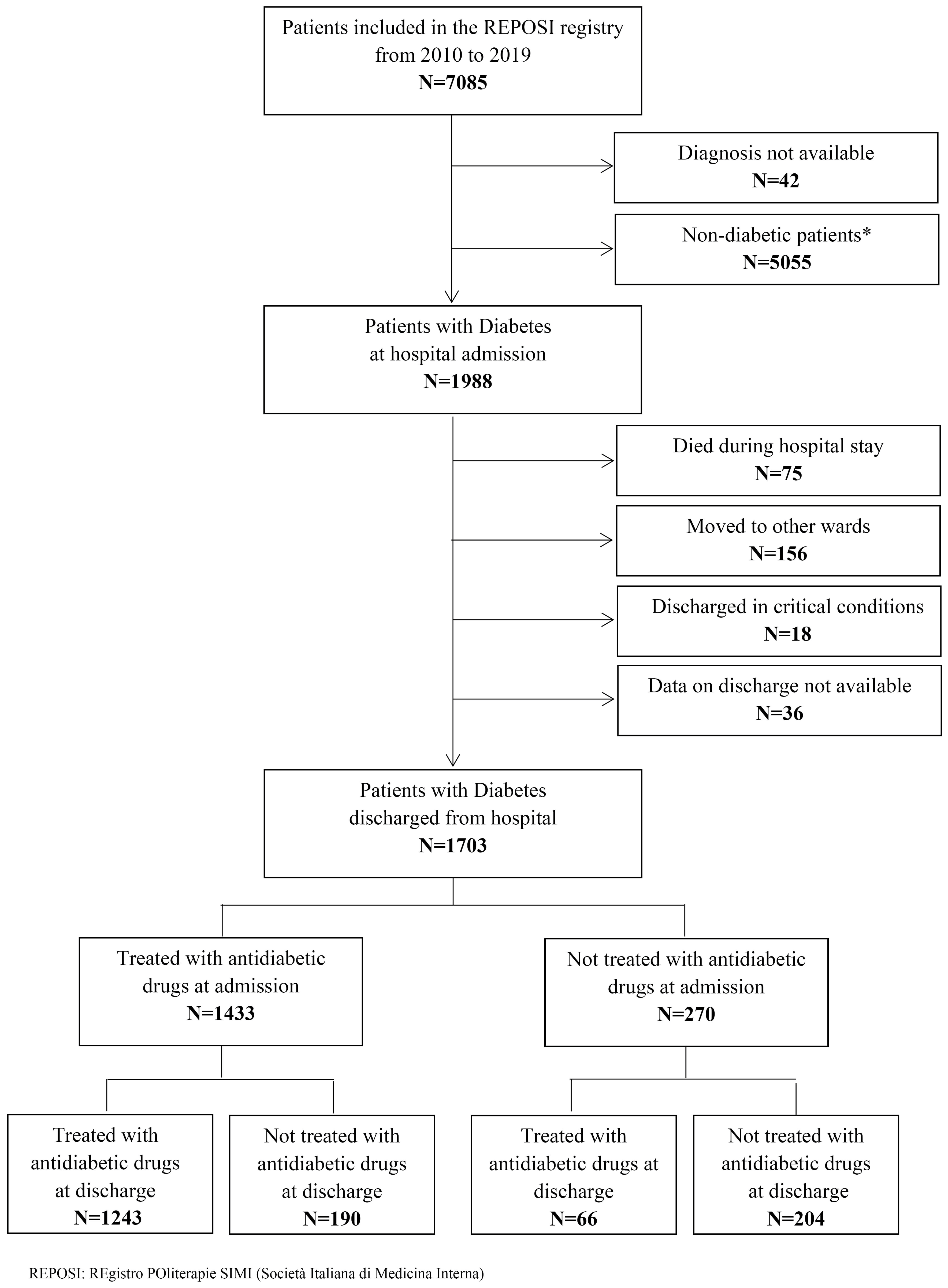
2.2. Study Population
2.3. Statistical Analysis
3. Results
3.1. Study Population
3.2. Antidiabetic Drugs
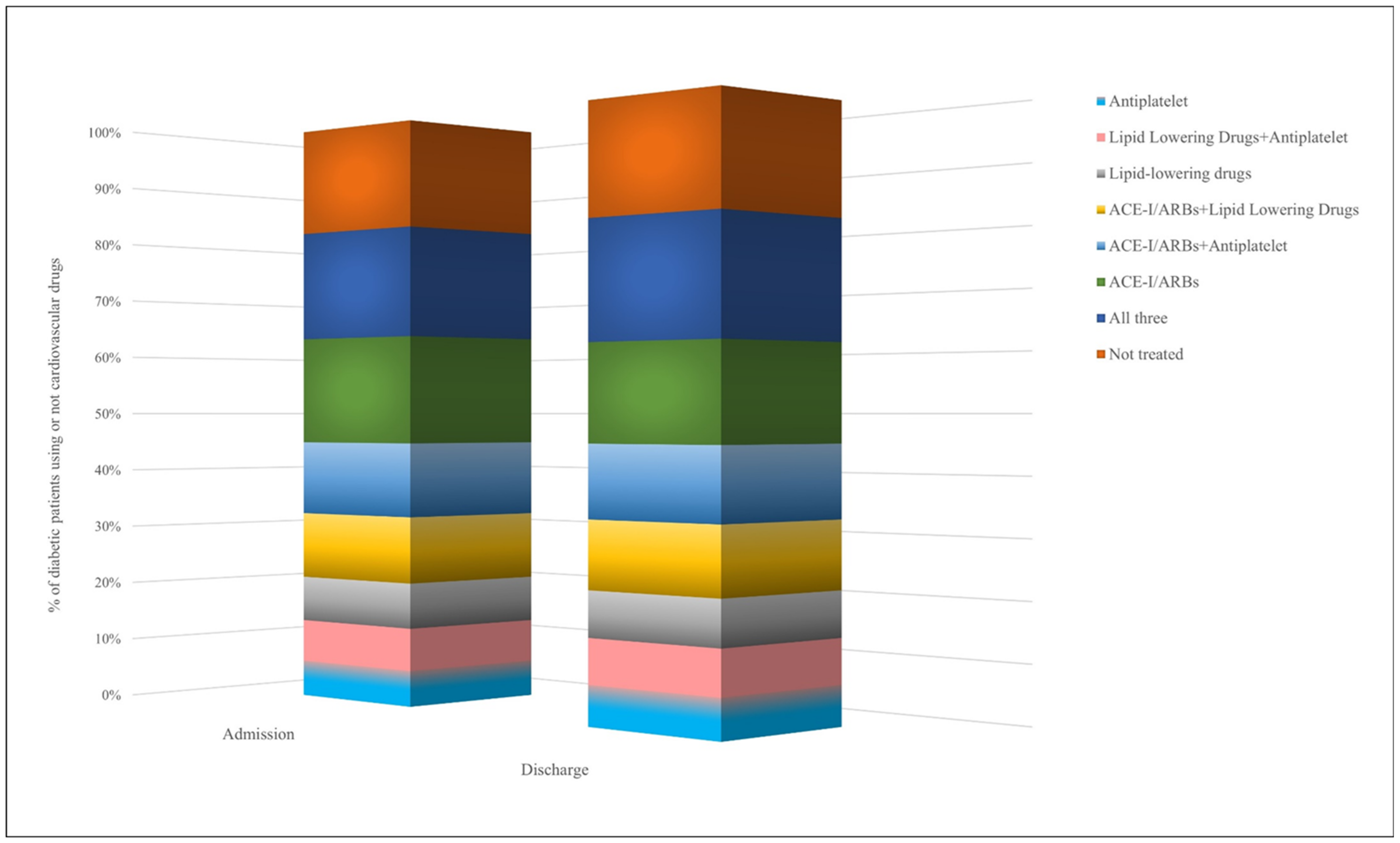
3.3. Concomitant Cardiovascular Therapies
4. Discussion
Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A
- Steering Committee: Pier Mannuccio Mannucci (Chair) (Fondazione IRCCS Cà Granda Ospedale Maggiore Policlinico, Milano), Alessandro Nobili (co-chair) (Istituto di Ricerche Farmacologiche Mario Negri IRCCS, Milano), Giorgio Sesti (Presidente SIMI), Antonello Pietrangelo (Direttore CRIS—SIMI), Francesco Perticone (Università Magna Grecia Policlinico Mater Domini, Catanzaro) Francesco Violi (Policlinico Umberto I, Roma), Gino Roberto Corazza, (IRCCS Policlinico San Matteo di Pavia, Pavia), Salvatore Corrao (ARNAS Civico, Di Cristina, Benfratelli, DiBiMIS, Università di Palermo, Palermo), Alessandra Marengoni (Spedali Civili di Brescia, Brescia), Francesco Salerno (IRCCS Policlinico San Donato Milanese, Milano), Matteo Cesari (Fondazione Maugeri, Milano), Mauro Tettamanti, Luca Pasina, Carlotta Franchi (Istituto di Ricerche Farmacologiche Mario Negri IRCCS, Milano).
- Clinical Data Monitoring and Revision: Carlotta Franchi, Alessio Novella, Mauro Tettamanti, Gabriella Miglio (Istituto di Ricerche Farmacologiche Mario Negri IRCCS, Milano).
- Database Management and Statistics: Mauro Tettamanti, Alessia Antonella Galbussera, Ilaria Ardoino, Alessio Novella (Istituto di Ricerche Farmacologiche Mario Negri IRCCS, Milano).
- -
- Domenico Prisco, Elena Silvestri, Giacomo Emmi, Alessandra Bettiol, Irene Mattioli (Azienda Ospedaliero Universitaria Careggi Firenze, SOD Medicina Interna Interdisciplinare);
- -
- Gianni Biolo, Michela Zanetti, Giacomo Bartelloni, Michele Zaccari, Massimiliano Chiuch (Azienda Sanitaria Universitaria Integrata di Trieste, Clinica Medica Generale e Terapia Medica);
- -
- Massimo Vanoli, Giulia Grignani, Edoardo Alessandro Pulixi (Azienda Ospedaliera della Provincia di Lecco, Ospedale di Merate, Lecco, Medicina Interna);
- -
- Matteo Pirro, Graziana Lupattelli, Vanessa Bianconi, Riccardo Alcidi, Alessia Giotta, Massimo R. Mannarino (Azienda Ospedaliera Santa Maria della Misericordia, Perugia, Medicina Interna, Angiologia Malattie da Arteriosclerosi);
- -
- Domenico Girelli, Fabiana Busti, Giacomo Marchi (Azienda Ospedaliera Universitaria Integrata di Verona, Verona, Medicina Generale e Malattie Aterotrombotiche e Degenerative);
- -
- Mario Barbagallo, Ligia Dominguez, Vincenza Beneduce, Federica Cacioppo (Azienda Ospedaliera Universitaria Policlinico Giaccone Policlinico di Palermo, Palermo, Unità Operativa di Geriatria e Lungodegenza);
- -
- Salvatore Corrao, Giuseppe Natoli, Salvatore Mularo, Massimo Raspanti, Christiano Argano, Federica Cavallaro (A.R.N.A.S. Civico, Di Cristina, Benfratelli, Palermo, UOC Medicina Interna ad Indirizzo Geriatrico-Riabilitativo);
- -
- Marco Zoli, Maria Laura Matacena, Giuseppe Orio, Eleonora Magnolfi, Giovanni Serafini, Angelo Simili, Mattia Brunori, Ilaria Lazzari, Angelo Simili (Azienda Ospedaliera Universitaria Policlinico S. Orsola-Malpighi, Bologna, Unità Operativa di Medicina Interna Zoli);
- -
- Maria Domenica Cappellini, Giovanna Fabio, Margherita Migone De Amicis, Giacomo De Luca, Natalia Scaramellini, Valeria Di Stefano, Simona Leoni, Sonia Seghezzi, Alessandra Danuto Di Mauro, Diletta Maira, Marta Mancarella (Fondazione IRCCS Cà Granda Ospedale Maggiore Policlinico, Milano, Unità Operativa Medicina Interna IA);
- -
- Tiziano Lucchi, Paolo Dionigi Rossi, Marta Clerici, Simona Leoni, Alessandra Danuta Di Mauro, Giulia Bonini, Federica Conti, Silvia Prolo, Maddalena Fabrizi, Miriana Martelengo, Giulia Vigani (Fondazione IRCCS Cà Granda Ospedale Maggiore Policlinico, Milano, Geriatria);
- -
- Antonio Di Sabatino, Emanuela Miceli, Marco Vincenzo Lenti, Martina Pisati, Costanza Caccia Dominioni, Lavinia Pitotti, Donatella Padula (IRCCS Policlinico San Matteo di Pavia, Pavia, Clinica Medica I, Reparto 11);
- -
- Roberto Pontremoli, Valentina Beccati, Giulia Nobili, Giovanna Leoncini, Jacopo Alberto, Federico Cattaneo (IRCCS Azienda Ospedaliera Universitaria San Martino-IST di Genova, Genova, Clinica di Medicina Interna 2);
- -
- Luigi Anastasio, Lucia Sofia, Maria Carbone (Ospedale Civile Jazzolino di Vibo Valentia, Vibo Valentia, Medicina Generale);
- -
- Francesco Cipollone, Maria Teresa Guagnano, Ilaria Rossi, Emanuele Valeriani, Damiani D’Ardes, Lucia Esposito, Simona Sestili, Ermanno Angelucci (Ospedale Clinicizzato SS. Annunziata, Chieti, Clinica Medica);
- -
- Gerardo Mancuso, Daniela Calipari, Mosè Bartone (Ospedale Giovanni Paolo II Lamezia Terme, Catanzaro, Unità Operativa Complessa Medicina Interna);
- -
- Giuseppe Delitala, Maria Berria, Alessandro Delitala (Azienda ospedaliera-universitaria di Sassari, Clinica Medica);
- -
- Maurizio Muscaritoli, Alessio Molfino, Enrico Petrillo, Antonella Giorgi, Christian Gracin, Giovanni Imbimbo (Policlinico Umberto I, Sapienza Università di Roma, Medicina Interna e Nutrizione Clinica Policlinico Umberto I);
- -
- Giuseppe Zuccalà, Gabriella D’Aurizio (Policlinico Universitario A. Gemelli, Roma, Roma, Unità Operativa Complessa Medicina d’Urgenza e Pronto Soccorso)
- -
- Giuseppe Romanelli, Alessandra Marengoni, Andrea Volpini, Daniela Lucente, Francesca Manzoni, Annalisa Pirozzi, Alberto Zucchelli (Unità Operativa Complessa di Medicina I a indirizzo geriatrico, Spedali Civili, Montichiari, Brescia);
- -
- Antonio Picardi, Umberto Vespasiani Gentilucci, Paolo Gallo, Chiara Dell’Unto (Università Campus Bio-Medico, Roma, Medicina Clinica-Epatologia);
- -
- Giuseppe Bellelli, Maurizio Corsi, Cesare Antonucci, Chiara Sidoli, Giulia Principato, Alessandra Bonfanti, Hajnalka Szabo, Paolo Mazzola, Andrea Piazzoli, Maurizio Corsi (Università degli studi di Milano-Bicocca Ospedale S. Gerardo, Monza, Unità Operativa di Geriatria);
- -
- Franco Arturi, Elena Succurro, Bruno Tassone, Federica Giofrè (Università degli Studi Magna Grecia, Policlinico Mater Domini, Catanzaro, Unità Operativa Complessa di Medicina Interna);
- -
- Maria Grazia Serra, Maria Antonietta Bleve (Azienda Ospedaliera “Cardinale Panico” Tricase, Lecce, Unità Operativa Complessa Medicina);
- -
- Antonio Brucato, Teresa De Falco, Enrica Negro, Martino Brenna, Lucia Trotta (ASST Fatebenefratelli—Sacco, Milano, Medicina Interna);
- -
- Maria Luisa Randi, Fabrizio Fabris, Irene Bertozzi, Giulia Bogoni, Maria Victoria Rabuini, Tancredi Prandini, Francesco Ratti, Chiara Zurlo, Lorenzo Cerruti, Elisabetta Cosi (Azienda Ospedaliera Università di Padova, Padova, Clinica Medica I);
- -
- Roberto Manfredini, Fabio Fabbian, Benedetta Boari, Alfredo De Giorgi, Ruana Tiseo (Azienda Ospedaliera—Universitaria Sant’Anna, Ferrara, Unità Operativa Clinica Medica);
- -
- Giuseppe Paolisso, Maria Rosaria Rizzo, Claudia Catalano, Irene Di Meo (Azienda Ospedaliera Universitaria della Seconda Università degli Studi di Napoli, Napoli, VI Divisione di Medicina Interna e Malattie Nutrizionali dell’Invecchiamento);
- -
- Claudio Borghi, Enrico Strocchi, Eugenia Ianniello, Mario Soldati, Silvia Schiavone, Alessio Bragagni, Francesca Giulia Leoni, Valeria De Sando, Sara Scarduelli, Michela Cammarosano, Ilenia Pareo (Azienda Ospedaliera Universitaria Policlinico S. Orsola-Malpighi, Bologna, Unità Operativa di Medicina Interna Borghi);
- -
- Carlo Sabbà, Francesco Saverio Vella, Patrizia Suppressa, Giovanni Michele De Vincenzo, Alessio Comitangelo, Emanuele Amoruso, Carlo Custodero, Giuseppe Re, Andrea Schilardi, Francesca Loparco (Azienda Ospedaliero-Universitaria Consorziale Policlinico di Bari, Bari, Medicina Interna Universitaria C. Frugoni);
- -
- Luigi Fenoglio, Andrea Falcetta, Alessia Valentina Giraudo, Salvatore D’Aniano (Azienda Sanitaria Ospedaliera Santa Croce e Carle di Cuneo, Cuneo, S. C. Medicina Interna);
- -
- Anna L. Fracanzani, Silvia Tiraboschi, Annalisa Cespiati, Giovanna Oberti, Giordano Sigon, Felice Cinque (Fondazione IRCCS Cà Granda Ospedale Maggiore Policlinico, Milano, UOC Medicina Generale ad Indirizzo Metabolico);
- -
- Flora Peyvandi, Raffaella Rossio, Giulia Colombo, Pasquale Agosti, Erica Pagliaro (Fondazione IRCCS Cà Granda Ospedale Maggiore Policlinico, Milano, Medicina Interna 2, Ematologia non tumorale e Coagulopatie);
- -
- Canetta Ciro, Valter Monzani, Valeria Savojardo, Giuliana Ceriani, Christian Folli (Fondazione IRCCS Cà Granda Ospedale Maggiore Policlinico, Milano, Medicina Interna Alta Intensità di Cure);
- -
- Francesco Salerno, Giada Pallini (IRCCS Policlinico San Donato e Università di Milano, San Donato Milanese, Medicina Interna);
- -
- Fabrizio Montecucco, Luciano Ottonello, Lara Caserza, Giulia Vischi, Salam Kassem, Luca Liberale (IRCCS Ospedale Policlinico San Martino e Università di Genova, Genova, Clinica Medica 1, Medicina Interna e Specialità Mediche);
- -
- Nicola Lucio Liberato, Tiziana Tognin (ASST di Pavia, UOSD Medicina Interna, Ospedale di Casorate Primo, Pavia);
- -
- Francesco Purrello, Antonino Di Pino, Salvatore Piro (Ospedale Garibaldi Nesima, Catania, Unità Operativa Complessa di Medicina Interna);
- -
- Renzo Rozzini, Lina Falanga, Maria Stella Pisciotta, Francesco Baffa Bellucci, Stefano Buffelli, Camillo Ferrandina, Francesca Mazzeo, Elena Spazzini, Giulia Cono, Giulia Cesaroni (Ospedale Poliambulanza, Brescia, Medicina Interna e Geriatria);
- -
- Giuseppe Montrucchio, Paolo Peasso, Edoardo Favale, Cesare Poletto, Carl Margaria, Maura Sanino (Dipartimento di Scienze Mediche, Università di Torino, Città della Scienza e della Salute, Torino, Medicina Interna 2 Unità Indirizzo d’Urgenza);
- -
- Francesco Violi, Ludovica Perri (Policlinico Umberto I, Roma, Prima Clinica Medica);
- -
- Luigina Guasti, Luana Castiglioni, Andrea Maresca, Alessandro Squizzato, Leonardo Campiotti, Alessandra Grossi, Roberto Davide Diprizio, Francesco Dentali (Università degli Studi dell’Insubria, Ospedale di Circolo e Fondazione Macchi, Varese, Medicina e Geriatria);
- -
- Marco Bertolotti, Chiara Mussi, Giulia Lancellotti, Maria Vittoria Libbra, Matteo Galassi, Yasmine Grassi, Alessio Greco, Elena Bigi, Elisa Pellegrini, Laura Orlandi, Giulia Dondi, Lucia Carulli (Università di Modena e Reggio Emilia, Azienda Ospedaliero-Universitaria di Modena; Ospedale Civile di Baggiovara, Unità Operativa di Geriatria);
- -
- Angela Sciacqua, Maria Perticone, Rosa Battaglia, Raffaele Maio, Aleandra Scozzafava, Valentino Condoleo, Tania Falbo, Lidia Colangelo; Marco Filice, Elvira Clausi (Università Magna Grecia Policlinico Mater Domini, Catanzaro, Unità Operativa Malattie Cardiovascolari Geriatriche);
- -
- Vincenzo Stanghellini, Eugenio Ruggeri, Sara del Vecchio, Ilaria Benzoni (Dipartimento di Scienze Mediche e Chirurgiche, Unità Operativa di Medicina Interna, Università degli Studi di Bologna/Azienda Ospedaliero-Universitaria S.Orsola-Malpighi, Bologna);
- -
- Andrea Salvi, Roberto Leonardi, Giampaolo Damiani (Spedali Civili di Brescia, U.O. 3a Medicina Generale);
- -
- Gianluca Moroncini, William Capeci, Massimo Mattioli, Giuseppe Pio Martino, Lorenzo Biondi, Pietro Pettinari, Monica Ormas, Emanuele Filippini, Devis Benfaremo, Roberto Romiti (Clinica Medica, Azienda Ospedaliera Universitaria-Ospedali Riuniti di Ancona);
- -
- Riccardo Ghio, Anna Dal Col (Azienda Ospedaliera Università San Martino, Genova, Medicina III);
- -
- Salvatore Minisola, Luciano Colangelo, Mirella Cilli, Giancarlo Labbadia (Policlinico Umberto I, Roma, SMSC03—Medicina Interna F e Malattie Metaboliche dell’osso);
- -
- Antonella Afeltra, Benedetta Marigliano, Maria Elena Pipita (Policlinico Campus Biomedico Roma, Roma, Medicina Clinica);
- -
- Pietro Castellino, Luca Zanoli, Alfio Gennaro, Agostino Gaudio, Samuele Pignataro (Azienda Ospedaliera Universitaria Policlinico—V. Emanuele, Catania, Dipartimento di Medicina);
- -
- Francesca Mete, Miriam Gino (Ospedale degli Infermi di Rivoli, Torino, Medicina Interna);
- -
- Guido Moreo, Silvia Prolo, Gloria Pina (Clinica San Carlo Casa di Cura Polispecialistica, Paderno Dugnano, Milano, Unità Operativa di Medicina Generale Emilio Bernardelli);
- -
- Alberto Ballestrero, Fabio Ferrando, Roberta Gonella, Domenico Cerminara, Paolo Setti, Chiara Traversa, Camilla Scarsi (Clinica Di Medicina Interna ad Indirizzo Oncologico, Azienda Ospedaliera Università San Martino di Genova);
- -
- Bruno Graziella, Stefano Baldassarre, Salvatore Fragapani, Gabriella Gruden (Medicina Interna III, Ospedale S. Giovanni Battista Molinette, Torino);
- -
- Franco Berti, Giuseppe Famularo, Patrizia Tarsitani (Azienda Ospedaliera San Camillo Forlanini, Roma, Medicina Interna II);
- -
- Roberto Castello, Michela Pasino (Ospedale Civile Maggiore Borgo Trento, Verona, Medicina Generale e Sezione di Decisione Clinica);
- -
- Marcello Giuseppe Maggio Gian Paolo Ceda, Simonetta Morganti, Andrea Artoni, Margherita Grossi (Azienda Ospedaliero Universitaria di Parma, U.O.C Clinica Geriatrica);
- -
- Stefano Del Giacco, Davide Firinu, Giulia Costanzo, Giacomo Argiolas, Giovanni Paoletti, Francesca Losa (Policlinico Universitario Duilio Casula, Azienda Ospedaliero-Universitaria di Cagliari, Cagliari, Medicina Interna, Allergologia ed Immunologia Clinica);
- -
- Giuseppe Montalto, Anna Licata, Filippo Alessandro Montalto (Azienda Ospedaliera Universitaria Policlinico Paolo Giaccone, Palermo, UOC di Medicina Interna);
- -
- Francesco Corica, Giorgio Basile, Antonino Catalano, Federica Bellone, Concetto Principato (Azienda Ospedaliera Universitaria Policlinico G. Martino, Messina, Unità Operativa di Geriatria);
- -
- Lorenzo Malatino, Benedetta Stancanelli, Valentina Terranova, Salvatore Di Marca, Rosario Di Quattro, Lara La Malfa, Rossella Caruso (Azienda Ospedaliera per l’Emergenza Cannizzaro, Catania, Clinica Medica Università di Catania);
- -
- Patrizia Mecocci, Carmelinda Ruggiero, Virginia Boccardi (Università degli Studi di Perugia-Azienda Ospedaliera S.M. della Misericordia, Perugia, Struttura Complessa di Geriatria);
- -
- Tiziana Meschi, Andrea Ticinesi, Antonio Nouvenne (Azienda Ospedaliera Universitaria di Parma, U.O Medicina Interna e Lungodegenza Critica);
- -
- Pietro Minuz, Luigi Fondrieschi, Giandomenico Nigro Imperiale, Sarah Morellini (Azienda Ospedaliera Universitaria Verona, Policlinico GB Rossi, Verona, Medicina Generale per lo Studio ed il Trattamento dell’Ipertensione Arteriosa);
- -
- Mario Pirisi, Gian Paolo Fra, Daniele Sola, Mattia Bellan (Azienda Ospedaliera Universitaria Maggiore della Carità, Medicina Interna 1);
- -
- Roberto Quadri, Erica Larovere, Marco Novelli (Ospedale di Ciriè, ASL TO4, Torino, S.C. Medicina Interna);
- -
- Emilio Simeone, Rosa Scurti, Fabio Tolloso (Ospedale Spirito Santo di Pescara, Geriatria);
- -
- Roberto Tarquini, Alice Valoriani, Silvia Dolenti, Giulia Vannini (Ospedale San Giuseppe, Empoli, USL Toscana Centro, Firenze, Medicina Interna I);
- -
- Riccardo Volpi, Pietro Bocchi, Alessandro Vignali (Azienda Ospedaliera Universitaria di Parma, Clinica e Terapia Medica);
- -
- Sergio Harari, Chiara Lonati, Federico Napoli, Italia Aiello (Ospedale San Giuseppe Multimedica Spa, U.O. Medicina Generale);
- -
- Francesco Purrello, Antonino Di Pino (Ospedale Garibaldi-Nesima–Catania, U.O.C Medicina Interna);
- -
- Teresa Salvatore, Lucio Monaco, Carmen Ricozzi (Policlinico Università della Campania L. Vanvitelli, UOC Medicina Interna);
- -
- Alberto Pilotto, Ilaria Indiano, Federica Gandolfo (Ente Ospedaliero Ospedali Galliera Genova, SC Geriatria Dipartimento Cure Geriatriche, Ortogeriatria e Riabilitazione)
- -
- Franco Laghi Pasini, Pier Leopoldo Capecchi (Azienda Ospedaliera Universitaria Senese, Siena, Unità Operativa Complessa Medicina 2);
- -
- Ranuccio Nuti, Roberto Valenti, Martina Ruvio, Silvia Cappelli, Alberto Palazzuoli (Azienda Ospedaliera Università Senese, Siena, Medicina Interna I);
- -
- Mauro Bernardi, Silvia Li Bassi, Luca Santi, Giacomo Zaccherini (Azienda Ospedaliera Policlinico Sant’Orsola-Malpighi, Bologna, Semeiotica Medica Bernardi);
- -
- Vittorio Durante, Daniela Tirotta, Giovanna Eusebi (Ospedale di Cattolica, Rimini, Medicina Interna);
- -
- Marco Cattaneo, Maria Valentina Amoruso, Paola Fracasso, Cristina Fasolino (Azienda ospedaliera San Paolo, Milano, Medicina III);
- -
- Moreno Tresoldi, Enrica Bozzolo, Sarah Damanti (IRCCS Ospedale San Raffaele–Milano, Medicina Generale e delle Cure Avanzate);
- -
- Massimo Porta, Miriam Gino (AOU Città della Salute e della Scienza di Torino–Torino, Medicina Interna 1U).
References
- World Health Organization. Diabetes. Available online: https://www.who.int/news-room/fact-sheets/detail/diabetes (accessed on 2 December 2022).
- International Diabetes Federation. Diabetes Atlas 2021, 10th ed.; International Diabetes Federation: Brussels, Belgium, 2021; Available online: https://diabetesatlas.org/ (accessed on 2 December 2022).
- International Diabetes Federation. Diabetes in Europe. Policy Puzzle. The State We Are in. Available online: https://www.idf.org/our-network/regions-members/europe/publications-and-resources/56-diabetes-in-europe-policy-puzzle.html (accessed on 2 December 2022).
- Huang, E.S. Management of diabetes mellitus in older people with comorbidities. BMJ 2016, 353, i2200. [Google Scholar] [CrossRef] [PubMed]
- Di Martino, G.; Di Giovanni, P.; Cedrone, F.; Meo, F.; Scampoli, P.; Romano, F.; Staniscia, T. Hospitalization for Short-Term Diabetes-Related Complications: Focus on Patients aged over 85 years. Healthcare 2021, 9, 460. [Google Scholar] [CrossRef] [PubMed]
- Comino, E.J.; Harris, M.F.; Islam, M.D.; Tran, D.T.; Jalaludin, B.; Jorm, L.; Flack, J.; Haas, M. Impact of diabetes on hospital admission and length of stay among a general population aged 45 year or more: A record linkage study. BMC Health Serv. Res. 2015, 15, 12. [Google Scholar] [CrossRef] [PubMed]
- American Diabetes Association. Standard in Medical Care in Diabetes—2022. Older Adults. Diabetes Care 2022, 45 (Suppl. 1), S195–S207. [Google Scholar] [CrossRef]
- American Diabetes Association. Standard in Medical Care in Diabetes—2022. Diabetes Care in the hospital. Diabetes Care 2022, 45 (Suppl. 1), S244–S253. Available online: https://diabetesjournals.org/care/article/45/Supplement_1/S244/138924/16-Diabetes-Care-in-the-Hospital-Standards-of (accessed on 2 December 2022). [CrossRef]
- Bogun, M.; Inzucchi, S.E. Inpatient management of diabetes and hyperglycemia. Clin. Ther. 2013, 35, 724–733. [Google Scholar] [CrossRef]
- Raghavan, S.; Vassy, J.L.; Ho, Y.L.; Song, R.J.; Gagnon, D.R.; Cho, K.; Wilson, P.W.S.; Phillips, L.S. Diabetes Mellitus-Related All-Cause and Cardiovascular Mortality in a National Cohort of Adults. J. Am. Heart Assoc. 2019, 8, e011295. [Google Scholar] [CrossRef] [Green Version]
- Rawshani, A.; Rawshani, A.; Franzen, S.; Sattar, N.; Eliasson, B.; Svensson, A.M.; Zethelius, B.; Miftaraj, M.; McGuire, D.K.; Rosengren, A.; et al. Mortality and Cardiovascular Disease in Type 1 and Type 2 Diabetes. N. Engl. J. Med. 2017, 376, 1407–1418. [Google Scholar] [CrossRef] [Green Version]
- Joseph, J.J.; Deedwania, P.; Acharya, T.; Aguilar, D.; Bhatt, D.L.; Chyun, D.A.; Di Palo, K.E.; Golden, S.H.; Sperling, L.S.; American Heart Association Diabetes Committee of the Council on Lifestyle and Cardiometabolic Health; et al. Comprehensive Management of Cardiovascular Risk Factors for Adults With Type 2 Diabetes: A Scientific Statement From the American Heart Association. Circulation 2022, 145, e722–e759. [Google Scholar] [CrossRef]
- Gaiţă, D.; Moşteoru, S.; Sperling, L. Diabetes Management—Lowering Cardiovascular Risk. Eur. Cardiol. 2014, 9, 7–9. [Google Scholar] [CrossRef]
- Rossio, R.; Mandelli, S.; Ardoino, I.; Nobili, A.; Peyvandi, F.; Mannucci, P.M.; Franchi, C.; REPOSI Collaborators. Prescription appropriateness of anticoagulant drugs for prophylaxis of venous thromboembolism in hospitalized multimorbid older patients. Intern. Emerg. Med. 2022, 18, 97–104. [Google Scholar] [CrossRef]
- Franchi, C.; Lancellotti, G.; Bertolotti, M.; Di Salvatore, S.; Nobili, A.; Mannucci, P.M.; Mussi, C.; Ardoino, I.; REPOSI Study Group. Use of Lipid-Lowering Drugs and Associated Outcomes According to Health State Profiles in Hospitalized Older Patients. Clin. Interv. Aging 2021, 2, 1251–1264. [Google Scholar] [CrossRef]
- Mahoney, F.I.; Barthel, D. Functional evaluation: The Barthel Index. Md. State Med. J. 1965, 14, 56–61. [Google Scholar]
- Miller, M.D.; Towers, A. Manual of Guidelines for Scoring the Cumulative Illness Rating Scale for Geriatrics (CIRS-G); University of Pittsburgh: Pittsburg, PA, USA, 1991. [Google Scholar]
- World Health Organization. Global Report on Diabetes. 2016. Available online: https://www.who.int/publications/i/item/9789241565257 (accessed on 2 December 2022).
- Wong, E.; Backholer, K.; Gearon, E.; Harding, J.; Freak-Poli, R.; Stevenson, C.; Peeters, A. Diabetes and risk of physical disability in adults: A systematic review and meta-analysis. Lancet Diabetes Endocrinol. 2013, 1, 106–114. [Google Scholar] [CrossRef] [Green Version]
- Marcucci, M.; Franchi, C.; Nobili, A.; Mannucci, P.M.; Ardoino, I.; REPOSI Investigators. Defining aging phenotypes and related outcomes: Clues to recognize frailty in hospitalized older patients. J Gerontol. A Biol. Sci. Med. Sci. 2017, 72, 395–402. [Google Scholar] [CrossRef] [Green Version]
- Yakaryilmaz, F.D.; Ozturk, A. Treatment of type 2 diabetes mellitus in the elderly. World J. Diabetes 2017, 8, 278–285. [Google Scholar] [CrossRef] [PubMed]
- Mata-Cases, M.; Franch-Nadal, J.; Real, J.; Vlacho, B.; Gomez-Garcia, A.; Mauricio, D. Evaluation of clinical and antidiabetic treatment characteristics of different sub-groups of patients with type 2 diabetes: Data from a Mediterranean population database. Prim. Care Diabetes 2021, 15, 588–595. [Google Scholar] [CrossRef] [PubMed]
- Gomes, M.B.; Rathmann, W.; Charbonnel, B.; Khunti, K.; Kosiborod, M.; Nicolucci, A.; Pocock, S.J.; Shestakova, M.V.; Shimoura, I.; Tang, F.; et al. DISCOVER investigators. Treatment of type 2 diabetes mellitus worldwide: Baseline patient characteristics in the global DISCOVER study. Diabetes Res. Clin. Pract. 2019, 151, 20–32. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nicolucci, A.; Charbonnel, B.; Gomes, M.B. Treatment patterns and associated factors in 14,668 people with type 2 diabetes initiating a second-line therapy: Results from the global DISCOVER study programme. Diabetes Obes. Metab. 2019, 21, 2474–2485. [Google Scholar] [CrossRef] [Green Version]
- Pantalone, K.M.; Hobbs, T.M.; Wells, B.J.; Kong, S.X.; Kattan, M.W.; Bouchard, J.; Yu, C.; Sakurada, B.; Milinovich, A.; Weng, W.; et al. Clinical characteristics, complications, comorbidities and treatment patterns among patients with type 2 diabetes mellitus in a large integrated health system. BMJ Open Diabetes Res. Care 2015, 3, e000093. [Google Scholar] [CrossRef] [Green Version]
- Wojszel, Z.B.; Kasiukiewicz, A. A retrospective cross-sectional study of type 2 diabetes overtreatment in patients admitted to the geriatric ward. BMC Geriatr. 2019, 19, 242. [Google Scholar] [CrossRef] [Green Version]
- Bongaerts, B.; Arnold, S.V.; Charbonnel, B.H.; Chen, H.; Cooper, A.; Fenici, P.; Gomes, M.; Ji, L.; Khunti, K.; Kosiborod, M.; et al. Inappropriate intensification of glucose lowering treatment in older patients with type 2 diabetes: The global DISCOVER study. BMJ Open Diabetes Res. Care 2021, 9, e001585. [Google Scholar] [CrossRef]
- Anderson, T.S.; Lee, S.; Jing, B.; Fung, K.; Ngo, S.; Silvestrini, M.; Steinman, M.A. Prevalence of Diabetes Medication Intensifications in Older Adults Discharged From US Veterans Health Administration Hospitals. JAMA Netw. Open 2020, 3, e201511. [Google Scholar] [CrossRef] [Green Version]
- Sesti, G.; Antonelli Incalzi, R.; Bonora, E.; Consoli, A.; Giaccari, A.; Maggi, S.; Paolisso, G.; Purrello, F.; Vendemiale, G.; Ferrara, N. Management of Diabetes in older adults. Nutr. Metab. Cardiovasc. Dis. 2018, 28, 206–2018. [Google Scholar] [CrossRef] [Green Version]
- Inzucchi, S.E. Management of Diabetes Mellitus in Hospitalized Patients. In Review. Available online: https://www.uptodate.com/contents/management-of-diabetes-mellitus-in-hospitalized-patients (accessed on 2 December 2022).
- Pasquel, F.J.; Lansang, M.C.; Dhatariya, K.; Umpierrez, G.E. Management of diabetes and hyperglycaemia in the hospital. Lancet Diabetes Endocrinol. 2021, 9, 174–188. [Google Scholar] [CrossRef]
- Malcom, J.; Halperin, I.; Miller, D.B.; Moore, S.; Nerenberg, K.A.; Woo, V.; Yu, C.H. In-Hospital Management of Diabetes. Can. J. Diabetes 2018, 42, S115–S123. [Google Scholar] [CrossRef] [Green Version]
- Gamble, J.M.; Chibrikov, E.; Twells, L.K. Association of insulin dosage with mortality or major adverse cardiovascular events: A retrospective cohort study. Lancet Diabetes Endocrinol. 2017, 5, 43–52. [Google Scholar] [CrossRef]
- Cosmi, F.; Shen, L.; Magnoli, M.; Abraham, W.T.; Anand, I.S.; Cleland, J.G.; Cohn, J.N.; Cosmi, D.; De Berardis, G.; Dickstein, K.; et al. Treatment with insulin is associated with worse outcome in patients with chronic heart failure and diabetes. Eur. J. Heart Fail. 2018, 20, 888–895. [Google Scholar] [CrossRef] [Green Version]
- Fixen, D.R. 2019 AGS Beers Criteria for Older Adults. Available online: https://www.pharmacytoday.org/article/S1042-0991(19)31235-6/pdf (accessed on 2 December 2022).
- Caughey, G.E.; Barratt, J.D.; Shakib, S.; Kemp-Casey, A.; Roughead, E.E. Medication use and potentially high-risk prescribing in older patients hospitalized for diabetes: A missed opportunity to improve care? Diabet. Med. 2017, 34, 432–439. [Google Scholar] [CrossRef]
- Franchi, C.; Ardoino, I.; Nobili, A.; Pasina, L.; Mannucci, P.M.; Marengoni, A.; Perticone, F.; REPOSI Investigators. Pattern of in-hospital changes in drug use in the older people from 2010 to 2016. Pharmacoepidemiol. Drug Saf. 2017, 26, 1534–1539. [Google Scholar] [CrossRef]
- Bonora, E.; Cataudella, S.; Marchesini, G. A view on the quality of diabetes care in Italy and the role of Diabetes Clinics from the 2018 ARNO Diabetes Observatory. Nutr. Metab. Cardiovasc. Dis. 2020, 30, 1945–1953. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Characteristics | Diabetic Patients N = 1703 | N Missing |
|---|---|---|
| Age, years, mean (SD) | 78.3 (7.0) | |
| Sex | ||
| Female | 793 (46.6) | |
| Male | 910 (53.4) | |
| Year of enrollment | ||
| 2010 | 324 (19.0) | |
| 2012 | 336 (19.7) | |
| 2014 | 269 (15.8) | |
| 2016 | 175 (10.3) | |
| 2017 | 224 (13.1) | |
| 2018 | 161 (9.5) | |
| 2019 | 214 (12.6) | |
| BMI | 215 | |
| Underweight (<18.5) | 23 (1.5) | |
| Normal weight (18.5–24.9) | 483 (32.5) | |
| Overweight (25–29.9) | 588 (39.5) | |
| Obesity (≥30) | 394 (26.5) | |
| Smoke | 59 | |
| Never | 837 (50.9) | |
| Ex-smoker | 662 (40.3) | |
| Smoker | 145 (8.8) | |
| Alcohol | 75 | |
| Never | 944 (58.0) | |
| Ex-drinker | 191 (11.7) | |
| Drinker | 493 (36.3) | |
| Social drinker | 274 (16.8) | |
| Barthel Index | 351 | |
| No or negligible dependence (91–100) | 635 (47.0) | |
| Mild dependence (75–90) | 302 (22.3) | |
| Moderate dependence (50–74) | 206 (15.2) | |
| Severe dependence (25–49) | 105 (7.8) | |
| Total dependence (0–24) | 104 (7.7) | |
| Glucose, mg/dL, mean (SD) | 161.7 (80.7) | 47 |
| Low (<100 mg/dL) | 293 (17.7) | |
| Medium (100–125 mg/dL) | 316 (19.1) | |
| High (≥126 mg/dL) | 1047 (63.2) | |
| Creatinine, mg/dL, mean (SD) | 1.36 (0.9) | 19 |
| GFR, mL/min/1.73 m2, mean (SD) 1 | 55.7 (24.4) | 19 |
| Total cholesterol, mg/dL, mean (SD) | 150.5 (43.0) | 462 |
| Number of drugs at admission 2, median (IQR) | 6 (4–8) | |
| 0–1 | 91 (5.4) | |
| 2–4 | 491 (28.8) | |
| 5+ | 1121 (65.8) | |
| CIRS—Comorbidity index, mean (SD) | 3.7 (1.9) | |
| CIRS—Severity index, mean (SD) | 1.8 (0.3) | |
| Co-morbidities 3 | ||
| Hypertension | 1274 (74.8) | |
| Ischemic heart disease | 582 (34.2) | |
| CKD | 513 (30.1) | |
| Atrial fibrillation | 489 (28.7) | |
| Heart Failure | 353 (20.7) | |
| Stroke/TIA | 340 (20.0) | |
| Peripheral arterial disease | 287 (16.8) | |
| Dyslipidemia | 215 (12.6) | |
| Dementia | 144 (8.5) |
| Admission N = 1703 | Discharge N = 1703 | ||
|---|---|---|---|
| Untreated | 270 (15.8) | 394 (23.1) | |
| Treated with monotherapy | |||
| Insulin monotherapy | 482 (28.3) | 589 (34.6) | |
| Metformin monotherapy | 328 (19.2) | 257 (15.1) | |
| Sulfonylureas monotherapy | 112 (6.6) | 69 (4.1) | |
| Repaglinides monotherapy | 107 (6.3) | 101 (5.9) | |
| Other antidiabetic drugs excl. insulin monotherapy 1 | 25 (1.5) | 23 (1.4) | |
| Treated with combinations | |||
| Fixed combination of antidiabetic drugs 2 | 80 (4.7) | 38 (2.2) | |
| Insulins + Metformin | 64 (3.8) | 63 (3.7) | |
| Metformin + Sulfonylureas | 64 (3.8) | 42 (2.5) | |
| Metformin + Repaglinide | 39 (2.3) | 26 (1.5) | |
| Insulins + Other antidiabetic drugs | 77 (4.5) | 71 (4.2) | |
| Other combinations of antidiabetic drugs excl. insulin | 55 (3.2) | 30 (1.7) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ardoino, I.; Mandelli, S.; Baviera, M.; Rossio, R.; Nobili, A.; Mannucci, P.M.; Franchi, C.; on behalf of REPOSI Investigator. Antidiabetic Drug Prescription Pattern in Hospitalized Older Patients with Diabetes. Int. J. Environ. Res. Public Health 2023, 20, 2607. https://doi.org/10.3390/ijerph20032607
Ardoino I, Mandelli S, Baviera M, Rossio R, Nobili A, Mannucci PM, Franchi C, on behalf of REPOSI Investigator. Antidiabetic Drug Prescription Pattern in Hospitalized Older Patients with Diabetes. International Journal of Environmental Research and Public Health. 2023; 20(3):2607. https://doi.org/10.3390/ijerph20032607
Chicago/Turabian StyleArdoino, Ilaria, Sara Mandelli, Marta Baviera, Raffaella Rossio, Alessandro Nobili, Pier Mannuccio Mannucci, Carlotta Franchi, and on behalf of REPOSI Investigator. 2023. "Antidiabetic Drug Prescription Pattern in Hospitalized Older Patients with Diabetes" International Journal of Environmental Research and Public Health 20, no. 3: 2607. https://doi.org/10.3390/ijerph20032607