

Association between Malnutrition Assessed by the Global Leadership Initiative on Malnutrition Criteria and Mortality in Older People: A Scoping Review
 , , ,
, , ,
Abstract
:1. Introduction
2. Methods
2.1. Population/Concept/Context (PCC)
2.2. Information Sources
2.3. Search Strategy
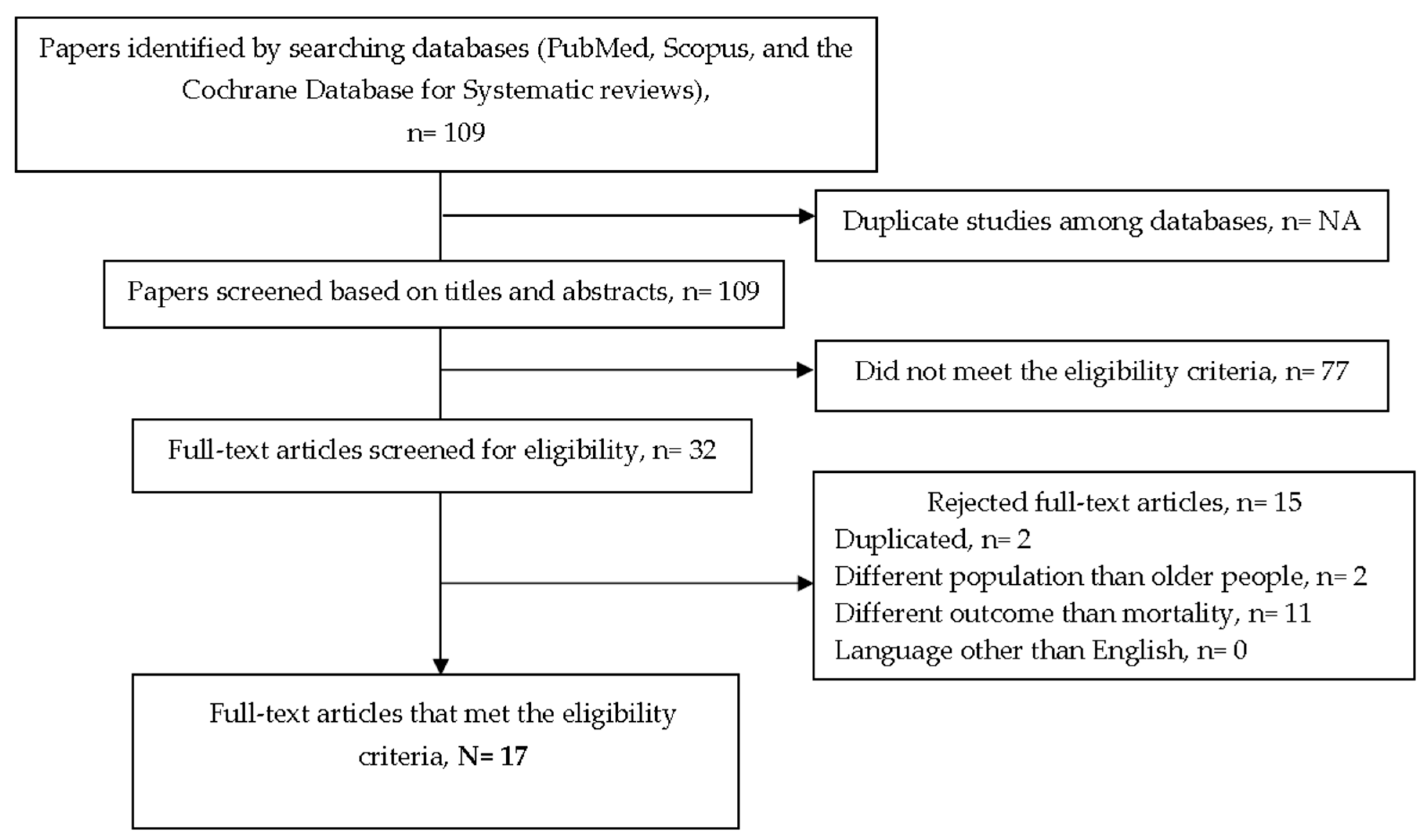
2.4. Selection Process
2.5. Data Collection Process
2.6. Data Items (Outcomes)
2.7. Synthetic Method
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
References
- Cederholm, T.; Barazzoni, R.; Austin, P.; Ballmer, P.; Biolo, G.; Bischoff, S.C.; Compher, C.; Correia, I.; Higashiguchi, T.; Holst, M.; et al. ESPEN guidelines on definitions and terminology of clinical nutrition. Clin. Nutr. 2017, 36, 49–64. [Google Scholar] [CrossRef]
- Cederholm, T.; Rothenberg, E.; Barazzoni, R. Editorial: A Clinically Relevant Diagnosis Code for “Malnutrition in Adults” Is Needed in ICD-11. J. Nutr. Health Aging 2022, 26, 314–315. [Google Scholar] [CrossRef] [PubMed]
- Beard, J.R.; Officer, A.; De Carvalho, I.A.; Sadana, R.; Pot, A.M.; Michel, J.P.; Lloyd-Sherlock, P.; Epping-Jordan, J.E.; Peeters, G.G.; Mahanani, W.R.; et al. The World report on ageing and health: A policy framework for healthy ageing. Lancet 2016, 387, 2145–2154. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organization. The Double Burden of Malnutrition: Policy Brief. 2017. Available online: https://www.who.int/publications/i/item/WHO-NMH-NHD-17.3 (accessed on 25 February 2023).
- Cederholm, T.; Jensen, G.L.; Correia, M.I.T.D.; Gonzalez, M.C.; Fukushima, R.; Higashiguchi, T.; Baptista, G.; Barazzoni, R.; Blaauw, R.; Coats, A.J.; et al. GLIM criteria for the diagnosis of malnutrition—A consensus report from the global clinical nutrition community. J. Cachexia Sarcopenia Muscle 2019, 10, 207–217. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cederholm, T.; Jensen, G.L. To create a consensus on malnutrition diagnostic criteria: A report from the Global Leadership Initiative on Malnutrition (GLIM) meeting at the ESPEN Congress 2016. Clin. Nutr. 2016, 36, 7–10. [Google Scholar] [CrossRef]
- Swan, L.; Martin, N.; Horgan, N.F.; Warters, A.; O’Sullivan, M. Assessing Sarcopenia, Frailty, and Malnutrition in Community-Dwelling Dependant Older Adults—An Exploratory Home-Based Study of an Underserved Group in Research. Int. J. Environ. Res. Public Health 2022, 19, 16133. [Google Scholar] [CrossRef]
- Beaudart, C.; Sanchez-Rodriguez, D.; Locquet, M.; Reginster, J.-Y.; Lengelé, L.; Bruyère, O. Malnutrition as a Strong Predictor of the Onset of Sarcopenia. Nutrients 2019, 11, 2883. [Google Scholar] [CrossRef] [Green Version]
- Leij-Halfwerk, S.; Verwijs, M.H.; van Houdt, S.; Borkent, J.W.; Guaitoli, P.R.; Pelgrim, T.; Heymans, M.W.; Power, L.; Visser, M.; Corish, C.A.; et al. Prevalence of protein-energy malnutrition risk in European older adults in community, residential and hospital settings, according to 22 malnutrition screening tools validated for use in adults ≥65 years: A systematic review and meta-analysis. Maturitas 2019, 126, 80–89. [Google Scholar] [CrossRef]
- Volkert, D.; Beck, A.M.; Cederholm, T.; Cruz-Jentoft, A.; Hooper, L.; Kiesswetter, E.; Maggio, M.; Raynaud-Simon, A.; Sieber, C.; Sobotka, L.; et al. ESPEN practical guideline: Clinical nutrition and hydration in geriatrics. Clin. Nutr. 2022, 41, 958–989. [Google Scholar] [CrossRef]
- Sanchez-Rodriguez, D.; Annweiler, C.; Marco, E.; Hope, S.; Piotrowicz, K.; Surquin, M.; Ranhoff, A.; Noortgate, N.V.D.; Andersen-Ranberg, K.; Bonin-Guillaume, S.; et al. European Academy for medicine of ageing session participants’ report on malnutrition assessment and diagnostic methods; an international survey. Clin. Nutr. ESPEN 2020, 35, 75–80. [Google Scholar] [CrossRef]
- Totland, T.H.; Krogh, H.W.; Smedshaug, G.B.; Tornes, R.A.; Bye, A.; Paur, I. Harmonization and standardization of malnutrition screening for all adults—A systematic review initiated by the Norwegian Directorate of Health. Clin. Nutr. ESPEN 2022, 52, 32–49. [Google Scholar] [CrossRef] [PubMed]
- Sanchez-Rodriguez, D.; Locquet, M.; Reginster, J.; Cavalier, E.; Bruyère, O.; Beaudart, C. Mortality in malnourished older adults diagnosed by ESPEN and GLIM criteria in the SarcoPhAge study. J. Cachex-Sarcopenia Muscle 2020, 11, 1200–1211. [Google Scholar] [CrossRef] [PubMed]
- Cárdenas, D.; Correia, M.I.T.D.; Hardy, G.; Ochoa, J.B.; Barrocas, A.; Hankard, R.; Hannequart, I.; Schneider, S.; Bermúdez, C.; Papapietro, K.; et al. Nutritional care is a human right: Translating principles to clinical practice. Clin. Nutr. 2022, 41, 1613–1618. [Google Scholar] [CrossRef] [PubMed]
- de van der Schueren, M.A.E.; Keller, H.; Consortium, G.L.I.M.; Cederholm, T.; Barazzoni, R.; Compher, C.; Correia, M.I.T.D.; Gonzalez, M.C.; Jager-Wittenaar, H.; Pirlich, M.; et al. Global Leadership Initiative on Malnutrition (GLIM): Guidance on validation of the operational criteria for the diagnosis of protein-energy malnutrition in adults. Clin. Nutr. 2020, 39, 2872–2880. [Google Scholar] [CrossRef]
- Barazzoni, R.; Jensen, G.L.; Correia, M.I.T.D.; Gonzalez, M.C.; Higashiguchi, T.; Shi, H.P.; Bischoff, S.C.; Boirie, Y.; Carrasco, F.; Cruz-Jentoft, A.; et al. Guidance for assessment of the muscle mass phenotypic criterion for the Global Leadership Initiative on Malnutrition (GLIM) diagnosis of malnutrition. Clin. Nutr. 2022, 41, 1425–1433. [Google Scholar] [CrossRef] [PubMed]
- Visser, M.; Mendonça, N.; Avgerinou, C.; Cederholm, T.; Cruz-Jentoft, A.J.; Goisser, S.; Kiesswetter, E.; Siebentritt, H.M.; Volkert, D.; Torbahn, G. Towards developing a Core Outcome Set for malnutrition intervention studies in older adults: A scoping review to identify frequently used research outcomes. Eur. Geriatr. Med. 2022, 13, 867–879. [Google Scholar] [CrossRef]
- Correia, M.I.T.; Tappenden, K.A.; Malone, A.; Prado, C.M.; Evans, D.C.; Sauer, A.C.; Hegazi, R.; Gramlich, L. Utilization and validation of the Global Leadership Initiative on Malnutrition (GLIM): A scoping review. Clin. Nutr. 2022, 41, 687–697. [Google Scholar] [CrossRef]
- Tricco, A.C.; Lillie, E.; Zarin, W.; O’Brien, K.K.; Colquhoun, H.; Levac, D.; Moher, D.; Peters, M.D.J.; Horsley, T.; Weeks, L.; et al. PRISMA Extension for Scoping Reviews (PRISMA-ScR): Checklist and Explanation. Ann. Intern. Med. 2018, 169, 467–473. [Google Scholar] [CrossRef] [Green Version]
- Sanchez-Rodriguez, D.; Locquet, M.; Bruyère, O.; Lengelé, L.; Cavalier, E.; Reginster, J.-Y.; Beaudart, C. Prediction of 5-year mortality risk by malnutrition according to the GLIM format using seven pragmatic approaches to define the criterion of loss of muscle mass. Clin. Nutr. 2020, 40, 2188–2199. [Google Scholar] [CrossRef]
- Sanchez-Rodriguez, D.; Bergmann, P.; Body, J.; Cavalier, E.; Gielen, E.; Goemaere, S.; Lapauw, B.; Laurent, M.R.; Rozenberg, S.; Honvo, G.; et al. The Belgian Bone Club 2020 guidelines for the management of osteoporosis in postmenopausal women. Maturitas 2020, 139, 69–89. [Google Scholar] [CrossRef]
- Zhang, X.; Tang, M.; Zhang, Q.; Zhang, K.-P.; Guo, Z.-Q.; Xu, H.-X.; Yuan, K.-T.; Yu, M.; Braga, M.; Cederholm, T.; et al. The GLIM criteria as an effective tool for nutrition assessment and survival prediction in older adult cancer patients. Clin. Nutr. 2020, 40, 1224–1232. [Google Scholar] [CrossRef] [PubMed]
- Contreras-Bolívar, V.; Sánchez-Torralvo, F.J.; Ruiz-Vico, M.; González-Almendros, I.; Barrios, M.; Padín, S.; Alba, E.; Olveira, G. GLIM Criteria Using Hand Grip Strength Adequately Predict Six-Month Mortality in Cancer Inpatients. Nutrients 2019, 11, 2043. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Huang, D.-D.; Yu, D.-Y.; Song, H.-N.; Wang, W.-B.; Luo, X.; Wu, G.-F.; Yu, Z.; Liu, N.-X.; Dong, Q.-T.; Chen, X.-L.; et al. The relationship between the GLIM-defined malnutrition, body composition and functional parameters, and clinical outcomes in elderly patients undergoing radical gastrectomy for gastric cancer. Eur. J. Surg. Oncol. 2021, 47, 2323–2331. [Google Scholar] [CrossRef] [PubMed]
- Yeung, S.S.Y.; Chan, J.H.Y.; Chan, R.S.M.; Sham, A.; Ho, S.C.; Woo, J. Predictive Value of the GLIM Criteria in Chinese Community-Dwelling and Institutionalized Older Adults Aged 70 Years and over. J. Nutr. Health Aging 2021, 25, 645–652. [Google Scholar] [CrossRef]
- Sanz-Paris, A.; Fernández, M.G.; Perez-Nogueras, J.; Serrano-Oliver, A.; Torres-Anoro, E.; Sanz-Arque, A.; Arbones-Mainar, J.M. Prevalence of Malnutrition and 1-Year All-Cause Mortality in Institutionalized Elderly Patients Comparing Different Combinations of the GLIM Criteria. J. Parenter. Enter. Nutr. 2020, 45, 1164–1171. [Google Scholar] [CrossRef]
- Rodríguez-Mañas, L.; Rodríguez-Sánchez, B.; Carnicero, J.; Rueda, R.; García-Garcia, F.; Pereira, S.; Sulo, S. Impact of nutritional status according to GLIM criteria on the risk of incident frailty and mortality in community-dwelling older adults. Clin. Nutr. 2020, 40, 1192–1198. [Google Scholar] [CrossRef] [PubMed]
- Yeung, S.S.; Chan, R.S.; Kwok, T.; Lee, J.S.; Woo, J. Malnutrition According to GLIM Criteria and Adverse Outcomes in Community-Dwelling Chinese Older Adults: A Prospective Analysis. J. Am. Med. Dir. Assoc. 2020, 22, 1953–1959.e4. [Google Scholar] [CrossRef] [PubMed]
- Hirose, S.; Matsue, Y.; Kamiya, K.; Kagiyama, N.; Hiki, M.; Dotare, T.; Sunayama, T.; Konishi, M.; Saito, H.; Saito, K.; et al. Prevalence and prognostic implications of malnutrition as defined by GLIM criteria in elderly patients with heart failure. Clin. Nutr. 2021, 40, 4334–4340. [Google Scholar] [CrossRef]
- Dávalos-Yerovi, V.; Marco, E.; Sánchez-Rodríguez, D.; Duran, X.; Meza-Valderrama, D.; Rodríguez, D.; Muñoz, E.; Tejero-Sánchez, M.; Muns, M.; Guillén-Solà, A.; et al. Malnutrition According to GLIM Criteria Is Associated with Mortality and Hospitalizations in Rehabilitation Patients with Stable Chronic Obstructive Pulmonary Disease. Nutrients 2021, 13, 369. [Google Scholar] [CrossRef]
- Allepaerts, S.; Buckinx, F.; Bruyère, O.; Reginster, J.Y.; Paquot, N.; Gillain, S. Clinical Impact of Nutritional Status and Energy Balance in Elderly Hospitalized Patients. J. Nutr. Health Aging 2020, 24, 1073–1079. [Google Scholar] [CrossRef]
- Muñoz Fernandez, S.S.; Garcez, F.B.; Alencar, J.C.G.; Cederholm, T.; Aprahamian, I.; Morley, J.E.; de Souza, H.P.; Avelino da Silva, T.J.; Ribeiro, S.M.L. Applicability of the GLIM criteria for the diagnosis of malnutrition in older adults in the emergency ward: A pilot validation study. Clin. Nutr. 2021, 40, 5447–5456. [Google Scholar] [CrossRef] [PubMed]
- Sanz-París, A.; Martín-Palmero, A.; Gomez-Candela, C.; García-Almeida, J.M.; Burgos-Pelaez, R.; Sanz-Arque, A.; Espina, S.; Arbones-Mainar, J.M.; Study VIDA Group. GLIM Criteria at Hospital Admission Predict 8-Year All-Cause Mortality in Elderly Patients with Type 2 Diabetes Mellitus: Results from VIDA Study. J. Parenter. Enter. Nutr. 2020, 44, 1492–1500. [Google Scholar] [CrossRef] [PubMed]
- Sobestiansky, S.; Åberg, A.C.; Cederholm, T. Sarcopenia and malnutrition in relation to mortality in hospitalised patients in geriatric care—Predictive validity of updated diagnoses. Clin. Nutr. ESPEN 2021, 45, 442–448. [Google Scholar] [CrossRef] [PubMed]
- Pereira, A.G.; Costa, N.A.; Vulcano, D.S.B.; de Moraes, M.B.; Dorna, M.D.S.; Polegato, B.F.; Zornoff, L.A.M.; Azevedo, P.S.; Minicucci, M.F.; Paiva, S.A.R. Association between GLIM criteria for diagnosis of malnutrition and hospital mortality in patients receiving parenteral nutrition. Nutrire 2021, 46, 9. [Google Scholar] [CrossRef]
- Xu, J.Y.; Zhu, M.W.; Zhang, H.; Li, L.; Tang, P.X.; Chen, W.; Wei, J.M. A Cross-Sectional Study of Glim-Defined Malnutrition Based on New Validated Calf Circumference Cut-Off Values and Different Screening Tools in Hospitalised Patients over 70 Years Old. J. Nutr. Health Aging 2020, 24, 832–838. [Google Scholar] [CrossRef]
- Meza-Valderrama, D.; Marco, E.; Muñoz-Redondo, E.; Morgado-Pérez, A.; Sánchez, M.T.; Peña, Y.C.; De Jaime, E.; Canchucaja, L.; Concepción, F.M.; Perkisas, S.; et al. Musculoskeletal Ultrasound Shows Muscle Mass Changes during Post-Acute Care Hospitalization in Older Men: A Prospective Cohort Study. Int. J. Environ. Res. Public Health 2022, 19, 15150. [Google Scholar] [CrossRef] [PubMed]
- Landi, F.; Camprubi-Robles, M.; Bear, D.; Cederholm, T.; Malafarina, V.; Welch, A.; Cruz-Jentoft, A. Muscle loss: The new malnutrition challenge in clinical practice. Clin. Nutr. 2018, 38, 2113–2120. [Google Scholar] [CrossRef] [Green Version]
- Perkisas, S.; Bastijns, S.; Baudry, S.; Bauer, J.; Beaudart, C.; Beckwée, D.; Cruz-Jentoft, A.; Gasowski, J.; Hobbelen, H.; Jager-Wittenaar, H.; et al. Application of ultrasound for muscle assessment in sarcopenia: 2020 SARCUS update. Eur. Geriatr. Med. 2021, 12, 45–59. [Google Scholar] [CrossRef]
- Grant, M.J.; Booth, A. A typology of reviews: An analysis of 14 review types and associated methodologies. Health Inf. Libr. J. 2009, 26, 91–108. [Google Scholar] [CrossRef]
- Peters, M.D.J.; Godfrey, C.M.; Khalil, H.; McInerney, P.; Parker, D.; Soares, C.B. Guidance for conducting systematic scoping reviews. JBI Evid. Implement. 2015, 13, 141–146. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| Population | Human patient population. Age ≥ 65-year-old. Any condition or disease state. Any healthcare geriatric setting (hospitalized, community-dwelling, and nursing home population). |
| Concept | Articles about the GLIM criteria Articles published from 3 September 2018 (date when the GLIM criteria were launched) to 1 January 2023 (date when the last bibliographic search for the review was consulted). All-cause mortality as primary or secondary outcome. |
| Context | Full-text, peer-reviewed publications in indexed journals. All type of study designs were included in the bibliographic search. Utilization of the GLIM criteria. Written in English. |
| First Author, Year of Publication, and Citation | Population | Sample Size (n) | Mean Age (Years) ± SD | Primary Outcome: Mortality. Other Secondary Outcomes | Design | Muscle Mass Assessment Method | Odds Ratio/Hazard Ratio (95%CI; p-Value) |
|---|---|---|---|---|---|---|---|
| Hirose, 2021 [29] | Hospitalized patients | 1332 | Aged 65 and older | Mortality | Cohort study | BIA | HR = 1.57 (95%CI 1.09–2.27; p = 0.016) |
| Gomes Pereira, 2021 [35] | Hospitalized patients | 90 | 68.0 (56.3–5.3) | Mortality | Cross-sectional study | Omission of muscle mass as phenotypic criterion | OR = 1.498 (95%CI 0.496–4.521; p = 0.473) |
| Davalos-Yerovi, 2021 [30] | Hospitalized patients with stable COPD | 200 | 66.5 ± 9 | Mortality Hospitalization, length of stay | Cohort study | BIA | HR = 2.8 (95%CI 0.9–8; p = 0.005) |
| Allepaerts, 2020 [31] | Hospitalized patients | 79 | 84.9 ± 5.3 | Mortality Institutionalization | Cohort study | BIA | OR = 7.29 (95%CI 1.87–28.4; p = 0.0043) |
| Xu, 2020 [36] | Hospitalized patients | 6519 | 78.4 ± 6 | Mortality Diagnostic performance indicators of several cut-off points of calf circumference | Cross-sectional study | Calf circumference | OR = 1.231 (95%CI 1.022–1.484; p = 0.029) |
| Munoz, 2021 [32] | Hospitalized patients in emergency wards | 165 | 73 (65–102) | Mortality Length of stay, transfer to intensive unit care, and the diagnostic performance indicators | Cohort study | Handgrip strength, calf circumference, subscapular skinfold thickness, triceps skinfold thickness, adductor pollicis thickness. | HR = 4.23 (95%CI 1.2–14.9; p = 0.02) |
| Sanz-Paris, 2020 [33] | Hospitalized patients with type 2 diabetes | 159 | 77.9 | Mortality Frailty | Cohort study | Calf and mid-arm circumference | HR = 2.09 (95%CI 1.29–3.38; p = 0.003) |
| Sobestiansky, 2021 [34] | Hospitalized | 56 | 84 ± 7.3 | Mortality Malnutrition and sarcopenia | Cohort study | DXA and calf circumference | HR = 4.83 (95%CI 1.04–22.39) |
| Zhang, 2021 [22] | Hospitalized patients with cancer | 1192 | Aged 65 and older | Mortality | Cohort study | Calf circumference | HR = 1.35 (95%CI 1.09–1.66; p = 0.006) |
| Contreras-Bolívar, 2019 [23] | Hospitalized patients with cancer | 282 | 60 ± 12.6 | Mortality | Cohort study | DXA, BIA, CT, handgrip strength, mid-arm circumference, and arm muscular circumference | If using handgrip strength, OR = 2.72 (95%CI 1.37–5.4; p = 0.004) If using FFMI, OR = 1.87 (95%CI 1.01–3.48; p = 0.047) |
| Huang, 2021 [24] | Hospitalized patient with cancer | 597 | 72 ± 8 | Mortality | Cohort study | CT | OR = 1.360 (95%CI 0.942–1.963; p = 0.101) |
| Rodríguez-Mañas, 2021 [27] | Community-dwelling | 1294 | 75 ± 6.29 | Mortality Incident frailty | Cohort study | Handgrip strength | OR = 1.758 (95%CI 1.073–2.849; p < 0.05 |
| Sanchez-Rodriguez, 2021 [20] | Community-dwelling | 534 | 73.07 ± 5.96 | Mortality | Cohort study | DXA, handgrip strength, calf circumference, mid-arm circumference, Goodman grid, Ishii score chart, Yu formula, and omission of muscle mass as phenotypic criterion | HR = 3.38 (95%CI 1.89–6.09) |
| Sanchez-Rodriguez, 2020 [13] | Community-dwelling | 534 | 73.2 ± 6.05 | Mortality Falls, fractures, and institutionalization | Cohort study | DXA | HR = 4.41 (95%CI 2.17–8.97) |
| Yeung, 2021 [28] | Community dwelling | 3702 | 72 ± 4 | Mortality Onset of sarcopenia, frailty, falls, mobility limitation, and hospitalization | Cohort study | DXA | HR = 1.62 (95%CI 1.39–1.89; p < 0.01) |
| Yeung, 2021 [25] | Community-dwelling and institutionalized patients | 2032 | CD: 78.1 ± 6.5 I: 85.5 ± 6.4 | Mortality | Cohort study | Corrected muscle mass arm circumference | HR = 1.37 (95%CI 1.12–1.66; p = 0.002) |
| Sanz-Paris, 2021 [26] | Institutionalized patients | 485 | 84.71 | Mortality | Cohort study | BIA, handgrip strength, and calf circumference | Min: HR = 0.81 (95%CI 0.46–1.42; p = 0.0456) Max: HR = 2.41 (95%CI 1.36–4.27; p < 0.01) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sánchez-Rodríguez, D.; De Meester, D.; Minon, L.; Claessens, M.; Gümüs, N.; Lieten, S.; Benoit, F.; Surquin, M.; Marco, E. Association between Malnutrition Assessed by the Global Leadership Initiative on Malnutrition Criteria and Mortality in Older People: A Scoping Review. Int. J. Environ. Res. Public Health 2023, 20, 5320. https://doi.org/10.3390/ijerph20075320
Sánchez-Rodríguez D, De Meester D, Minon L, Claessens M, Gümüs N, Lieten S, Benoit F, Surquin M, Marco E. Association between Malnutrition Assessed by the Global Leadership Initiative on Malnutrition Criteria and Mortality in Older People: A Scoping Review. International Journal of Environmental Research and Public Health. 2023; 20(7):5320. https://doi.org/10.3390/ijerph20075320
Chicago/Turabian StyleSánchez-Rodríguez, Dolores, Dorien De Meester, Léa Minon, Marie Claessens, Neslian Gümüs, Siddhartha Lieten, Florence Benoit, Murielle Surquin, and Ester Marco. 2023. "Association between Malnutrition Assessed by the Global Leadership Initiative on Malnutrition Criteria and Mortality in Older People: A Scoping Review" International Journal of Environmental Research and Public Health 20, no. 7: 5320. https://doi.org/10.3390/ijerph20075320