
Association between Muscle Fatigability, Self-Perceived Fatigue and C-Reactive Protein at Admission in Hospitalized Geriatric Patients


Abstract
:1. Introduction
2. Materials and Methods
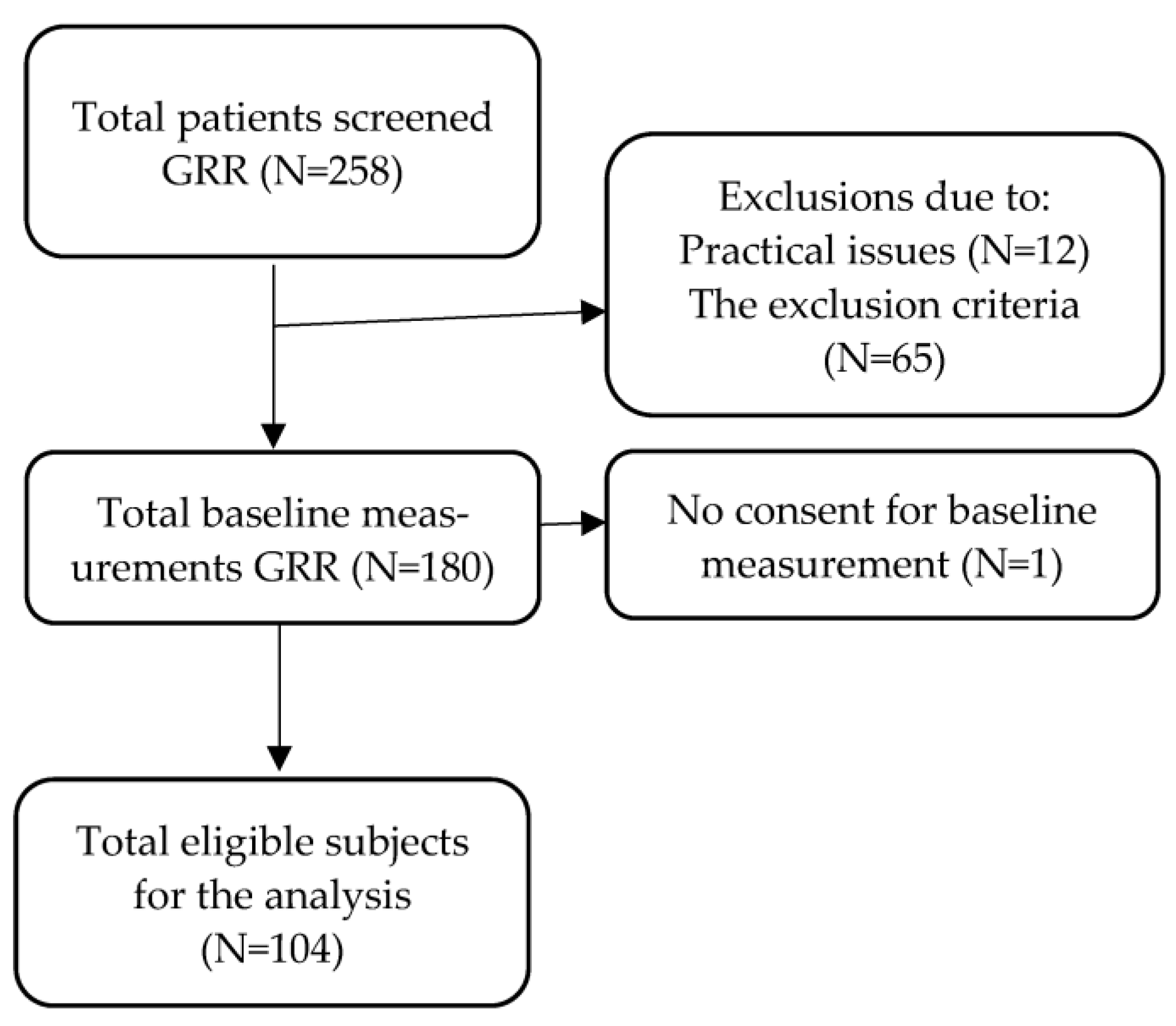
2.1. Study Sample
2.2. Data Collection
2.3. CPV Ratio
2.4. CRP
2.5. Statistical Analysis
3. Results
3.1. Cross-Sectional Association between CRP and CPV
3.2. Cross-Sectional Association between CRP and GW and SPF
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Woo, J. Combating frailty and sarcopenia in aging populations: Switching to a more positive paradigm. Aging Med. 2019, 2, 7–10. [Google Scholar] [CrossRef]
- Knoop, V.; Costenoble, A.; Debain, A.; Azzopardi, R.V.; Vermeiren, S.; van Laere, S.; Jansen, B.; Scafoglieri, A.; Bautmans, I.; Verté, D.; et al. The interrelationship between grip work, self-perceived fatigue and pre-frailty in community-dwelling octogenarians. Exp. Gerontol. 2021, 152, 111440. [Google Scholar] [CrossRef] [PubMed]
- Vermeiren, S.; Vella-Azzopardi, R.; Beckwée, D.; Habbig, A.-K.; Scafoglieri, A.; Jansen, B.; Bautmans, I.; Gerontopole Brussels Study Group. Frailty and the Prediction of Negative Health Outcomes: A Meta-Analysis. J. Am. Med. Dir. Assoc. 2016, 17, 1163.e1–1163.e17. [Google Scholar] [CrossRef] [PubMed]
- Hadley, E.C.; Kuchel, G.A.; Newman, A.B.; Allore, H.G.; Bartley, J.M.; Bergeman, C.S.; Blinov, M.L.; Colon-Emeric, C.S.; Dabhar, F.S.; Dugan, L.L.; et al. Report: NIA Workshop on Measures of Physiologic Resiliencies in Human Aging. J. Gerontol. Ser. A 2017, 72, 980–990. [Google Scholar] [CrossRef]
- Gijzel, S.M.W.; Van De Leemput, I.A.; Scheffer, M.; Roppolo, M.; Rikkert, M.G.M.O.; Melis, R.J.F. Dynamical Resilience Indicators in Time Series of Self-Rated Health Correspond to Frailty Levels in Older Adults. J. Gerontol. Ser. A 2017, 72, 991–996. [Google Scholar] [CrossRef] [PubMed]
- Cesari, M.; De Carvalho, I.A.; Thiyagarajan, J.A.; Cooper, C.; Martin, F.C.; Reginster, J.-Y.; Vellas, B.; Beard, J.R. Evidence for the Domains Supporting the Construct of Intrinsic Capacity. J. Gerontol. Ser. A Boil. Sci. Med. Sci. 2018, 73, 1653–1660. [Google Scholar] [CrossRef] [PubMed]
- Beard, J.R.; Officer, A.; de Carvalho, I.A.; Sadana, R.; Pot, A.M.; Michel, J.-P.; Lloyd-Sherlock, P.; Epping-Jordan, J.E.; Peeters, G.M.E.E.G.; Mahanani, W.R.; et al. The World report on ageing and health: A policy framework for healthy ageing. Lancet 2016, 387, 2145–2154. [Google Scholar] [CrossRef]
- Clegg, A.; Young, J.; Iliffe, S.; Rikkert, M.O.; Rockwood, K. Frailty in elderly people. Lancet 2013, 381, 752–762. [Google Scholar] [CrossRef]
- Pothier, K.; Gana, W.; Bailly, N.; Fougère, B. Associations between Frailty and Inflammation, Physical, and Psycho-Social Health in Older Adults: A Systematic Review. Front. Psychol. 2022, 13, 805501. [Google Scholar] [CrossRef]
- Koivunen, K.; Hoogendijk, E.O.; Schaap, L.A.; Huisman, M.; Heymans, M.W.; van Schoor, N.M. Development and validation of an intrinsic capacity composite score in the Longitudinal Aging Study Amsterdam: A formative approach. Aging Clin. Exp. Res. 2023, 35, 815–825. [Google Scholar] [CrossRef]
- Nagae, M.; Umegaki, H.; Komiya, H.; Nakashima, H.; Fujisawa, C.; Watanabe, K.; Yamada, Y.; Miyahara, S. Intrinsic capacity in acutely hospitalized older adults. Exp. Gerontol. 2023, 179, 112247. [Google Scholar] [CrossRef] [PubMed]
- Bautmans, I.; Njemini, R.; De Backer, J.; De Waele, E.; Mets, T. Surgery-Induced Inflammation in Relation to Age, Muscle Endurance, and Self-Perceived Fatigue. J. Gerontol. Ser. A 2009, 65A, 266–273. [Google Scholar] [CrossRef] [PubMed]
- Fried, L.P.; Tangen, C.M.; Walston, J.; Newman, A.B.; Hirsch, C.; Gottdiener, J.; Seeman, T.; Tracy, R.; Kop, W.J.; Burke, G.; et al. Frailty in Older adults: Evidence for a phenotype. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2001, 56, M146–M156. [Google Scholar] [CrossRef]
- Dent, E.; Martin, F.C.; Bergman, H.; Woo, J.; Romero-Ortuno, R.; Walston, J.D. Management of frailty: Opportunities, challenges, and future directions. Lancet 2019, 394, 1376–1386. [Google Scholar] [CrossRef] [PubMed]
- Norheim, K.L.; Bautmans, I.; Kjaer, M. Handgrip strength shows no improvements in geriatric patients with persistent inflammation during hospitalization. Exp. Gerontol. 2017, 99, 115–119. [Google Scholar] [CrossRef]
- Bautmans, I.; Onyema, O.; Van Puyvelde, K.; Pleck, S.; Mets, T. Grip work estimation during sustained maximal contraction: Validity and relationship with dependency and inflammation in elderly persons. J. Nutr. Health Aging 2011, 15, 731–736. [Google Scholar] [CrossRef]
- Sproston, N.R.; Ashworth, J.J. Role of C-Reactive Protein at Sites of Inflammation and Infection. Front. Immunol. 2018, 9, 754. [Google Scholar] [CrossRef]
- Lutomski, J.E.; Baars, M.A.E.; Schalk, B.W.M.; Boter, H.; Buurman, B.M.; Elzen, W.P.J.D.; Jansen, A.P.D.; Kempen, G.I.J.M.; Steunenberg, B.; Steyerberg, E.W.; et al. The Development of the Older Persons and Informal Caregivers Survey Minimum DataSet (TOPICS-MDS): A Large-Scale Data Sharing Initiative. PLoS ONE 2013, 8, e81673. [Google Scholar] [CrossRef]
- Smith, B.W.; Dalen, J.; Wiggins, K.; Tooley, E.; Christopher, P.; Bernard, J. The brief resilience scale: Assessing the ability to bounce back. Int. J. Behav. Med. 2008, 15, 194–200. [Google Scholar] [CrossRef]
- Church, S.; Rogers, E.; Rockwood, K.; Theou, O. A scoping review of the Clinical Frailty Scale. BMC Geriatr. 2020, 20, 1–18. [Google Scholar] [CrossRef]
- De Dobbeleer, L.; Swart, M.M.; Geerds, M.A.J.; Baggen, R.J.; Jansen, A.-J.S.; Tielemans, R.; Silva, H.; Lieten, S.; Barbé, K.; Peeters, G.; et al. Validity and reliability of Eforto®, a system to (self-)monitor grip strength and muscle fatigability in older persons. Aging Clin. Exp. Res. 2023, 35, 835–845. [Google Scholar] [CrossRef] [PubMed]
- Collard, R.M.; Boter, H.; Schoevers, R.A.; Voshaar, R.C.O. Prevalence of Frailty in Community-Dwelling Older Persons: A Systematic Review. J. Am. Geriatr. Soc. 2012, 60, 1487–1492. [Google Scholar] [CrossRef] [PubMed]
- Austin, P.C.; White, I.R.; Lee, D.S.; van Buuren, S. Missing Data in Clinical Research: A Tutorial on Multiple Imputation. Can. J. Cardiol. 2021, 37, 1322–1331. [Google Scholar] [CrossRef] [PubMed]
- Bautmans, I.; Gorus, E.; Njemini, R.; Mets, T. Handgrip performance in relation to self-perceived fatigue, physical functioning and circulating IL-6 in elderly persons without inflammation. BMC Geriatr. 2007, 7, 5. [Google Scholar] [CrossRef] [PubMed]
- Tuttle, C.S.; Thang, L.A.; Maier, A.B. Markers of inflammation and their association with muscle strength and mass: A systematic review and meta-analysis. Ageing Res. Rev. 2020, 64, 101185. [Google Scholar] [CrossRef] [PubMed]
- Louati, K.; Berenbaum, F. Fatigue in chronic inflammation—A link to pain pathways. Artritis Res. Ter. 2015, 17, 254. [Google Scholar] [CrossRef] [PubMed]
- Cooper, R.; Popham, M.; Santanasto, A.J.; Hardy, R.; Glynn, N.W.; Kuh, D. Are BMI and inflammatory markers independently associated with physical fatigability in old age? Int. J. Obes. 2019, 43, 832–841. [Google Scholar] [CrossRef]
- Valentine, R.J.; Woods, J.A.; McAuley, E.; Dantzer, R.; Evans, E.M. The associations of adiposity, physical activity and inflammation with fatigue in older adults. Brain Behav. Immun. 2011, 25, 1482–1490. [Google Scholar] [CrossRef]
- Ticinesi, A.; Lauretani, F.; Nouvenne, A.; Porro, E.; Fanelli, G.; Maggio, M.; Meschi, T. C-reactive protein (CRP) measurement in geriatric patients hospitalized for acute infection. Eur. J. Intern. Med. 2016, 37, 7–12. [Google Scholar] [CrossRef]
- Ablij, H.; Meinders, A. Creactive protein: History and revival. Eur. J. Intern. Med. 2002, 13, 412. [Google Scholar] [CrossRef]


{kind=link}
| Variables | Total Sample (n = 104) |
|---|---|
| Age (years, mean ± SD) | 83.3 ± 7.5 |
| Sex (% women) | 55.8 |
| Weight (kg) | 72.0 ± 15.9 |
| Clinical frailty scale (mean ± SD) | 5.5 ± 1.4 |
| Brief resilience scale (mean ± SD) | 3.2 ± 0.8 |
| No. of chronic conditions (median [IQR]) | 3 [2–5] |
| Length of stay (days, median [IQR]) | 7 [4–10] |
| Mortality during admission (% deceased) | 26.0 |
| Self-perceived fatigue (median [IQR]) | 6 [4–8] |
| Maximum grip strength (kPa, mean ± SD) | 40.4 ± 17.4 |
| Fatigue resistance (s, median [IQR]) | 24.5 [16–40] |
| Grip work (median [IQR]) | 675 [369–1193] |
| CPV ratio (median [IQR]) | 1.7 [0.9–4.2] |
| CRP (mg/L, median [IQR]) | 26.5 [4.8–60] |
| Time between CPV and CRP measurement (days, median [IQR]) | 1 [1, 2] |
| Reasons for admissions (n) | |
| Multiple admission reasons | 15 |
| General malaise | 6 |
| Musculoskeletal problems with a fracture | 18 |
| Musculoskeletal problems without a fracture | 7 |
| Cognitive problems | 5 |
| Cardio-vascular problems | 5 |
| Infections | 28 |
| Oncological reasons | 1 |
| Others | 19 |
| Sample Size | Regression Coefficient (95% Confidence Interval) | |
|---|---|---|
| Capacity to perceived vitality (CPV) | ||
| Unadjusted association | n = 86 | −1.69 (−4.48 to 1.10) |
| Adjusted for confounders * | n = 86 | −1.32 (−4.44 to 1.76) |
| Adjusted for confounders * and after imputation of missing data | n = 104 | −0.33 (−4.00 to 3.34) |
| Grip Work (GW) | ||
| Unadjusted association | n = 86 | −187.50 (−679.59 to 304.54) |
| Adjusted for confounders * | n = 86 | −116.71 (−676.73 to 433.30) |
| Adjusted for confounders * and after imputation of missing data | n = 104 | 25.53 (−478.23 to 529.30) |
| Self-perceived fatigue (SPF) | ||
| Unadjusted association | n = 86 | 0.45 (−0.73 to 1.62) |
| Adjusted for confounders * | n = 86 | 0.58 (−0.76 to 1.91) |
| Adjusted for confounders * and after imputation of missing data | n = 104 | 0.57 (−0.64 to 1.77) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hoekstra, C.; Swart, M.; Bautmans, I.; Melis, R.; Peeters, G. Association between Muscle Fatigability, Self-Perceived Fatigue and C-Reactive Protein at Admission in Hospitalized Geriatric Patients. Int. J. Environ. Res. Public Health 2023, 20, 6582. https://doi.org/10.3390/ijerph20166582
Hoekstra C, Swart M, Bautmans I, Melis R, Peeters G. Association between Muscle Fatigability, Self-Perceived Fatigue and C-Reactive Protein at Admission in Hospitalized Geriatric Patients. International Journal of Environmental Research and Public Health. 2023; 20(16):6582. https://doi.org/10.3390/ijerph20166582
Chicago/Turabian StyleHoekstra, Carmen, Myrthe Swart, Ivan Bautmans, René Melis, and Geeske Peeters. 2023. "Association between Muscle Fatigability, Self-Perceived Fatigue and C-Reactive Protein at Admission in Hospitalized Geriatric Patients" International Journal of Environmental Research and Public Health 20, no. 16: 6582. https://doi.org/10.3390/ijerph20166582