
The Prevalence of Nutritional Anaemia in Brazilian Pregnant Women: A Systematic Review and Meta-Analysis

 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Eligibility Criteria
2.2. Information Sources
2.3. Search Strategy
2.4. Studies Selection
2.5. Data Extraction
2.6. Appraisal of Methodological Quality
2.7. Summary Measures and Data Analysis
2.8. Assessment of Heterogeneity and Publication Bias
2.9. Quality of Meta-Evidence
3. Results
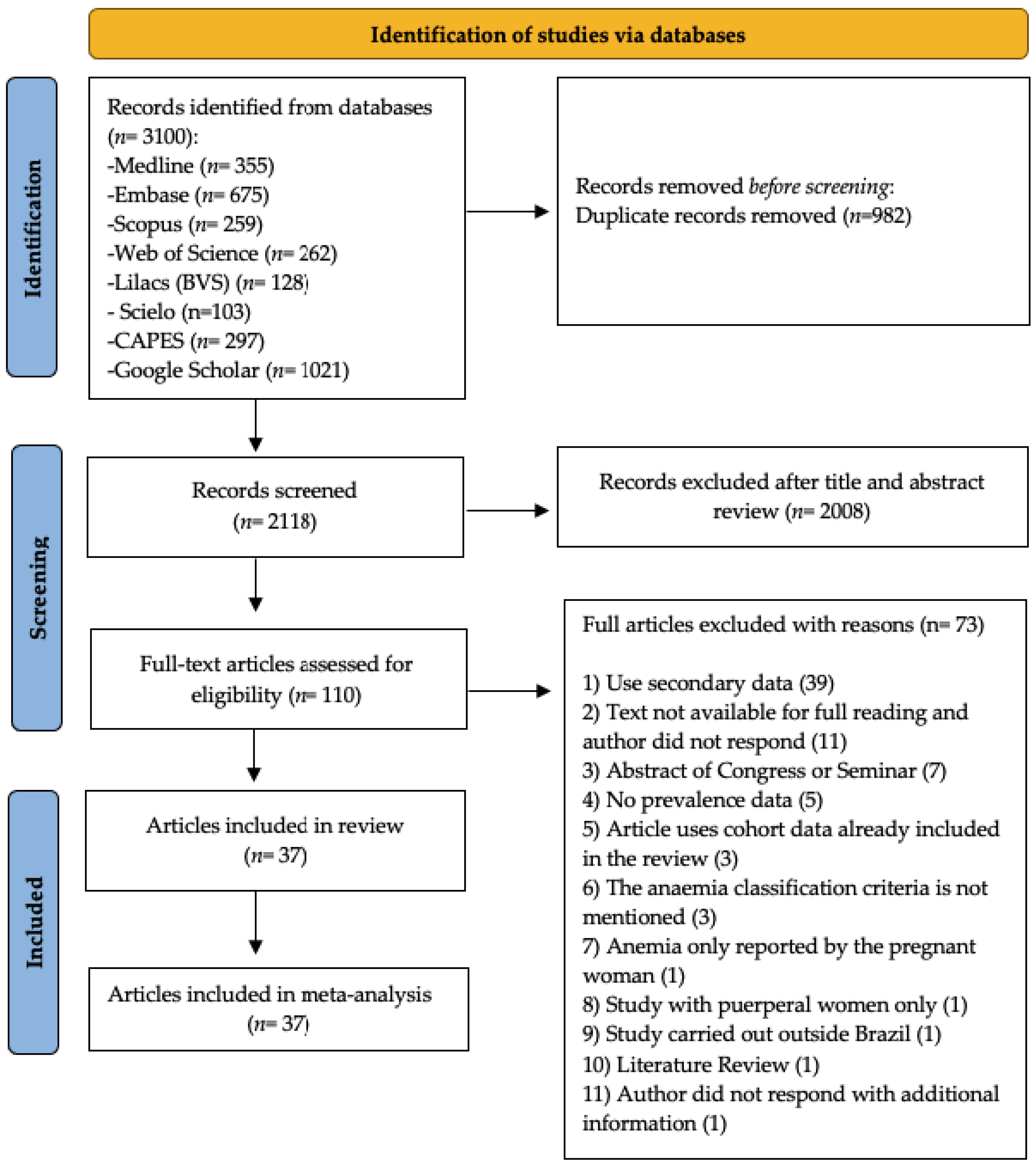
3.1. Selected Studies
3.2. Characteristics of the Studies
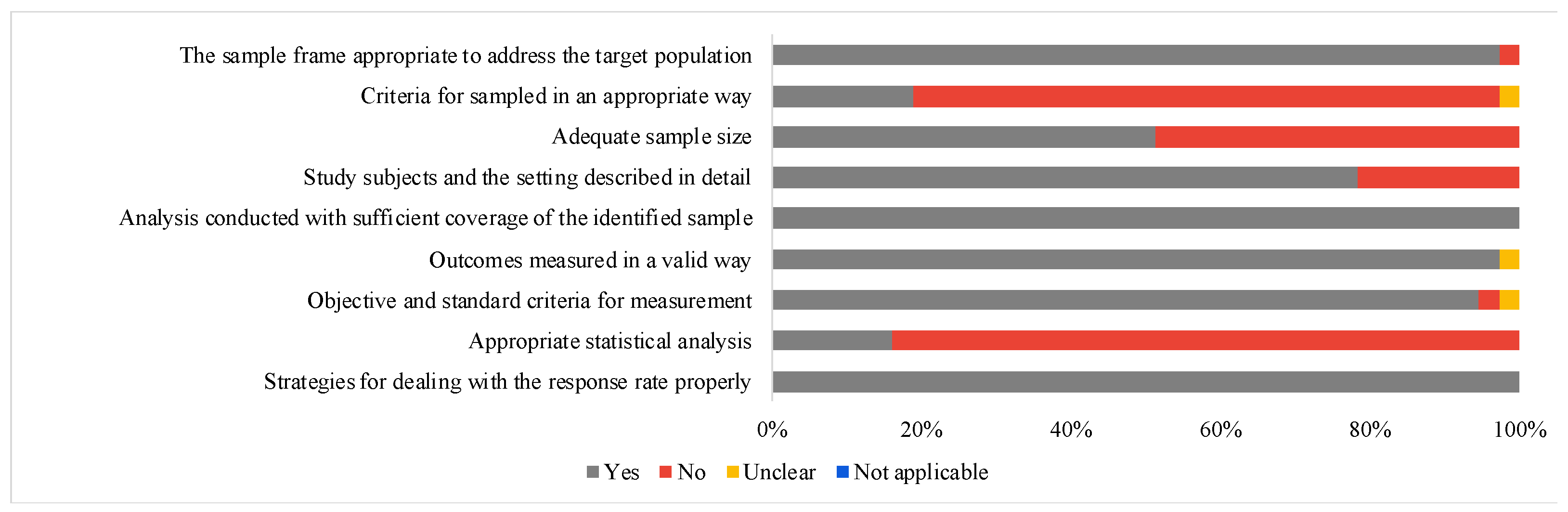
3.3. Methodological Quality of Individual Studies
3.4. Results of Individual Studies
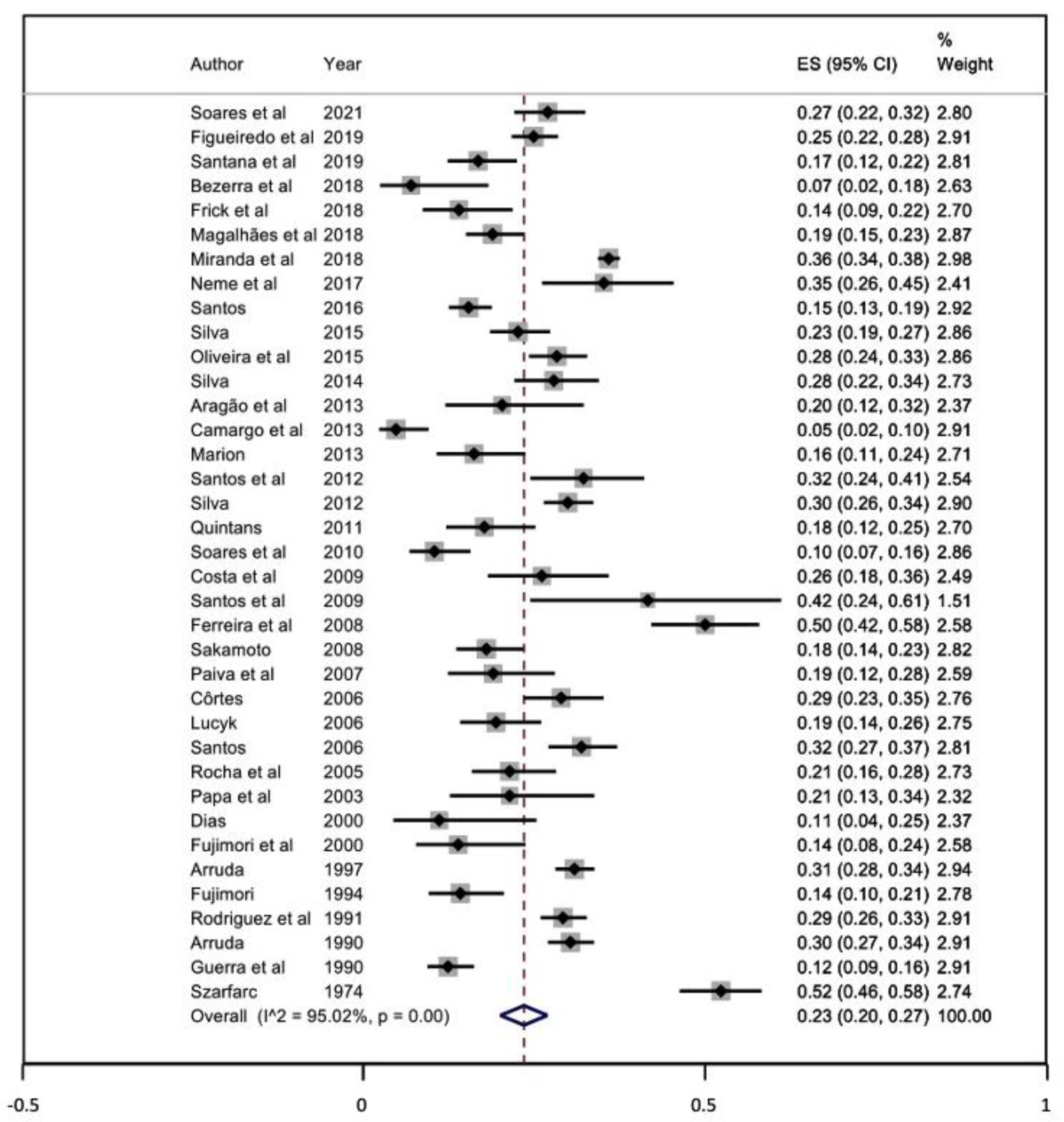
3.5. Meta-Analysis
3.6. Certainty of Evidence
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Means, R.T. Iron Deficiency and Iron Deficiency Anemia: Implications and Impact in Pregnancy, Fetal Development, and Early Childhood Parameters. Nutrients 2020, 12, 447. [Google Scholar] [CrossRef] [Green Version]
- Milman, N.; Byg, K.E.; Agger, A.O. Hemoglobin and Erythrocyte Indices during Normal Pregnancy and Postpartum in 206 Women with and without Iron Supplementation. Acta Obstet. Gynecol. Scand. 2000, 79, 89–98. [Google Scholar] [CrossRef] [PubMed]
- de Sá, S.A.; Willner, E.; Duraes Pereira, T.A.; de Souza, V.R.; Teles Boaventura, G.; Blondet de Azeredo, V. Anemia in pregnancy: Impact on weight and in the development of anemia in newborn. Nutr. Hosp. 2015, 32, 2071–2079. [Google Scholar] [CrossRef]
- Worls Health Organization (WHO). The Global Prevalence of Anaemia in 2011; WHO: Geneva, Switzerland, 2015; pp. 1–48. [Google Scholar]
- Mello, M.; Zancanaro, V.; Bellaver, H. Determination of the Iron Deficiency and Megaloblastic Anemic Profile in Pregnant Women Attended in the Maternal and Infant Public Service of a City in the Middle West of Santa Catarina. Rev. Bras. Análises Clín. 2016, 48, 331–336. [Google Scholar] [CrossRef]
- Zulfiqar, H.; Shah, I.U.; Sheas, M.N.; Ahmed, Z.; Ejaz, U.; Ullah, I.; Saleem, S.; Imran, M.; Hameed, M.; Akbar, B. Dietary Association of Iron Deficiency Anemia and Related Pregnancy Outcomes. Food Sci. Nutr. 2021, 9, 4127–4133. [Google Scholar] [CrossRef] [PubMed]
- Figueiredo, A.; Gomes-Filho, I.; Silva, R.; Pereira, P.; Mata, F.; Lyrio, A.; Souza, E.; Cruz, S.; Pereira, M. Maternal Anemia and Low Birth Weight: A Systematic Review and Meta-Analysis. Nutrients 2018, 10, 601. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Silveira, V.N.C.; Carvalho, C.A.; Viola, P.C.A.F.; Magalhães, E.I.S.; Padilha, L.L.; Conceição, S.I.O.; Frota, M.T.B.A.; Calado, I.L.; Cantanhede, N.A.C.; Franceschini, S.C.C.; et al. Prevalence of Iron-Deficiency Anaemia in Brazilian Children under 5 Years of Age: A Systematic Review and Meta-Analysis. Br. J. Nutr. 2020, 126, 1257–1269. [Google Scholar] [CrossRef]
- Geng, F.; Mai, X.; Zhan, J.; Xu, L.; Zhao, Z.; Georgieff, M.; Shao, J.; Lozoff, B. Impact of Fetal-Neonatal Iron Deficiency on Recognition Memoryat 2 Months of Age. J. Pediatr. 2015, 167, 1226–1232. [Google Scholar] [CrossRef] [Green Version]
- De-Regil, L.M.; Peña-Rosas, J.P.; Fernández-Gaxiola, A.C.; Rayco-Solon, P.J. Effects and Safety of Periconceptional Oral Folate Supplementationfor Preventing Birth Defects. Cochrane Database Syst. Rev. 2015, 12, CD007950. [Google Scholar]
- Achebe, M.M.; Gafter-Gvili, A. How I Treat Anemia in Pregnancy_Iron, Cobalamin, and Folate. Blood 2017, 129, 940–949. [Google Scholar] [CrossRef] [PubMed]
- Sayar, E.H. The Frequency of Vitamin B12, Iron, Folic Acid Deficiency in the Neonatal Period and Infancy and Relationship with Maternal Levels. Türk. Pediatr. Arşivi 2020, 55, 139–148. [Google Scholar] [CrossRef]
- BRASIL. Programa Nacional de Suplementação de Ferro-Manual de Condutas Gerais; Ministério da Saúde: Brasília, Brazil, 2013.
- Stevens, G.A.; Finucane, M.M.; De-Regil, L.M.; Paciorek, C.J.; Flaxman, S.R.; Branca, F.; Peña-Rosas, J.P.; Bhutta, Z.A.; Ezzati, M. Global, Regional, and National Trends in Haemoglobin Concentration and Prevalence of Total and Severe Anaemia in Children and Pregnant and Non-Pregnant Women for 1995–2011: A Systematic Analysis of Population-Representative Data. Lancet Glob. Health 2013, 1, e16–e25. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stevens, G.A.; Paciorek, C.J.; Flores-Urrutia, M.C.; Borghi, E.; Namaste, S.; Wirth, J.P.; Suchdev, P.S.; Ezzati, M.; Rohner, F.; Flaxman, S.R.; et al. National, Regional, and Global Estimates of Anaemia by Severity in Women and Children for 2000–19: A Pooled Analysis of Population-Representative Data. Lancet Glob. Health 2022, 10, e627–e639. [Google Scholar] [CrossRef]
- World Health Organization (WHO). Global Health Observatory–Anaemia in Pregnant Women. Available online: https://apps.who.int/gho/data/view.main.ANAEMIAWOMENCOUNTRYv?lang=en (accessed on 10 November 2022).
- Côrtes, M.H.; Vasconcelos, I.A.L.; Coitinho, D.C. Prevalência de Anemia Ferropriva em Gestantes Brasileiras: Uma Revisão dos Últimos 40 Anos. Rev. Nutr. 2009, 22, 409–418. [Google Scholar] [CrossRef]
- Conde, W.L.; Monteiro, C.A. Nutrition Transition and Double Burden of Undernutrition and Excess of Weight in Brazil. Am. J. Clin. Nutr. 2014, 100, 1617S–1622S. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 Statement: An Updated Guideline for Reporting Systematic Reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- World Health Organization. Nutrition in Adolescence-Issues and Challenges for the Health Sector Issues in Adolescent Health and Development; World Health Organization: Geneva, Switzerland, 2005. [Google Scholar]
- McGowan, J.; Sampson, M.; Salzwedel, D.M.; Cogo, E.; Foerster, V.; Lefebvre, C. PRESS Peer Review of Electronic Search Strategies: 2015 Guideline Statement. J. Clin. Epidemiol. 2016, 75, 40–46. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pizato, N.; Botelho, P.B.; Gonçalves, V.S.S.; Dutra, E.S.; Carvalho, K.M.B. Effect of Grazing Behavior on Weight Regain Post-Bariatric Surgery: A Systematic Review. Nutrients 2017, 9, 1322. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dean, A.G.; Sullivan, K.M.; Soe, M. OpenEpi: Open Source Epidemiologic Statistics for Public Health, Versão. Available online: www.OpenEpi.com (accessed on 16 May 2022).
- Munn, Z.; MClinSc, S.M.; Lisy, K.; Riitano, D.; Tufanaru, C. Methodological Guidance for Systematic Reviews of Observational Epidemiological Studies Reporting Prevalence and Cumulative Incidence Data. Int. J. Evid. Based. Healthc. 2015, 13, 147–153. [Google Scholar] [CrossRef]
- Higgins, J.P.T.; Thompson, S.G. Quantifying Heterogeneity in a Meta-Analysis. Stat. Med. 2002, 21, 1539–1558. [Google Scholar] [CrossRef]
- Deeks, J.J.; Altman, D.G.; Bradburn, M.J.; Egger, M.; Smith, G.D. Systematic Review in Health Care: Meta-Analysis in Context; BMJ: London, UK, 2001. [Google Scholar]
- Aragão, F.K.S.; de Almeida, A.L.; Nunes, S.F.L. Prevalência e Fatores Associados à Anemia Em Gestantes Atendidas Em Uma Maternidade Pública No Município de Imperatriz, Maranhão. JMPHC J. Manag. Prim. Health Care 2013, 4, 190. [Google Scholar] [CrossRef]
- Arruda, I.K.G. de Prevalência de Anemia Em Gestantes de Baixa Renda: Algumas Variáveis Associadas e Sua Repercussão No Recém-Nascido. Master’s Thesis, Universidade de Pernambuco-UFPE, Recife, Brazil, 1990. [Google Scholar]
- Frick, G.G.; Frizzo, M.N. Prevalência de Anemia e Seus Fatores Determinantes Em Gestantes de Município Do Noroeste Do Estado Do RS. Rev. Context. Saúde 2018, 18, 69. [Google Scholar] [CrossRef]
- Fujimori, E. Gravidez Na Adolescência: Estado Nutricional Referente Ao Ferro. Ph.D. Thesis, Universidade de São Paulo, Brazil, 1994; p. 87. [Google Scholar]
- Fujimori, E.; Laurenti, D.; Núñez DE Cassana, L.M.; de Oliveira, I.M.V.; Szarfarc, S.C. Anemia e Deficiência de Ferro Em Gestantes Adolescentes. Rev. Nutr. 2000, 13, 177–184. [Google Scholar] [CrossRef] [Green Version]
- Guerra, E.M.; de Barretto, O.C.O.; Vaz, A.J.; Silveira, M.B. Prevalência de Anemia Em Gestantes de Primeira Consulta Em Centros de Saúde de Área Metropolitana, Brasil. Rev. Saude Publica 1990, 24, 380–386. [Google Scholar] [CrossRef] [PubMed]
- Lucyk, J.M. Perfil Antropométrico, Consumo Alimentar e Concentração de Hemoglobina Em Gestantes Assistidas No Hospital Universitário de Brasília. Master’s Thesis, Universidade de Brasília—UnB, Brasília, Brazil, 2006. [Google Scholar]
- Magalhães, E.I.S.; Maia, D.S.; Pereira Netto, M.; Lamounier, J.A.; Rocha, D.D.S. Prevalência de Anemia e Determinantes Da Concentração de Hemoglobina Em Gestantes. Cad. Saúde Coletiva 2018, 26, 384–390. [Google Scholar] [CrossRef]
- Marion, M. Prevalência de Anemia e Hipotireoidismo Em Gestantes Atendidas No Pré-Natal Do Hospital Universitário de Santa Maria—RS (HUSM). Master’s Thesis, Universidade Federal de Santa Maria, Santa Maria, Brazil, 2013. [Google Scholar]
- Miranda, V.I.A.; Santos, I.S.; da Silveira, M.F.; Silveira, M.P.T.; da Pizzol, T.S.D.; Bertoldi, A.D. Validade Do Autorrelato de Anemia e Do Uso Terapêutico de Sais de Ferro Durante a Gestação: Coorte de Nascimentos de 2015 de Pelotas, Rio Grande Do Sul, Brasil. Cadernos Saúde Públ. 2018, 34, e00125517. [Google Scholar] [CrossRef] [PubMed]
- Neme, L.C.L.H.; Brognoli, A.F.; Szarfarc, S.; Cristina, A.; Oliveira, L.; Renata, C.; Silva, D.M. Estado Nutricional, Consumo de Ferro e Vitamina C e Níveis Sanguíneos de Hemoglobina de Gestantes. Cadernos Escola Saúde 2017, 1, 149–164. [Google Scholar]
- Oliveira, A.C.M.; Barros, A.M.R.; Ferreira, R.C. Fatores de Associados à Anemia Em Gestantes Da Rede Pública de Saúde de Uma Capital Do Nordeste Do Brasil. Rev. Bras. Ginecol. Obs. 2015, 37, 505–511. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- de Arruda, I.K.G. Deficiência de Ferro, de Folato e Anemia Em Gestantes Atendidas Do Instituto Materno-Infantil de Pernambuco Magnitude, Fatores de Risco e Algumas Implicações Nos Seus Conceptos. Master’s Thesis, Departamento de Nutrição, Universidade Federal de Pernambuco, Recife, Brazil, 1997. [Google Scholar]
- Paiva, A.d.A.; Rondó, P.H.C.; Pagliusi, R.A.; Latorre, M.d.R.D.O.; Cardoso, M.A.A.; Gondim, S.S.R. Relationship between the Iron Status of Pregnant Women and Their Newborns. Rev. Saúde Pública 2007, 41, 321–327. [Google Scholar] [CrossRef] [Green Version]
- Papa, A.C.E.; Furlan, J.P.; Pasquelle, M.; Guazzelli, C.A.F.; Figueiredo, M.S.; Camano, L.; Mattar, R. A Anemia Por Deficiência de Ferro Na Grávida Adolescente: Comparação Entre Métodos Laboratoriais. Rev. Bras. Ginecol. Obs. 2003, 25, 731–738. [Google Scholar] [CrossRef] [Green Version]
- Quintans, A.M. Anemia Em Gestantes: Avaliação Das Usuárias Das Unidades Básicas de Saúde Do Município de Cabedelo-Paraíba. Master’s Thesis, Universidade Federal da Paraíba, João Pessoa, Brazil, 2011. [Google Scholar]
- Rocha, D.S.; Netto, M.P.; Priore, S.E.; Lima, N.M.M.; Rosado, L.E.F.P.L.; Franceschini, S.C.C. Estado Nutricional e Anemia Ferropriva Em Gestantes: Relação Com o Peso Da Criança Ao Nascer. Rev. Nutr. 2005, 18, 481–489. [Google Scholar] [CrossRef] [Green Version]
- Sinisterra Rodriguez, O.; Szarfarc, S.C.; Benicio, M.H. d’Aquino Anemia e Desnutrição Maternas e Sua Relação Com o Peso Ao Nascer. Rev. Saúde Públ. 1991, 25, 193–197. [Google Scholar] [CrossRef]
- Sakamoto, T.M. Hemoglobinopatias e Anemias em Gestantes no Hospital Universitário de Campo Grande-MS. Master’s Thesis, Hospital Universitário Maria Aparecida Pedrossian, Campo Grande, Brazil, 2008; pp. 1–100. [Google Scholar]
- Santana, M.S.; Costa Filho, A.A.; Lisboa, C.S.; Viana, A.S.; Santos, D.B. Influência Da Anemia Em Gestantes Sobre O Peso Ao Nascer: Um Estudo Da Coorte NISAMI. Rev. Baiana Saúde Públ. 2019, 43, 581–598. [Google Scholar] [CrossRef]
- Santos, P.N.P. Prevalência de Anemia Nas Gestantes Atendidas em Unidades de Saúde da Família em Feira de Santana, Bahia, Entre Outubro de 2005 e Março de 2006. Master’s Thesis, Universidade Estadual de Feira de Santana Departamento de Saúde Programa de Pós-Graduação Em Saúde Coletiva, Feira de Santana, Brazil, 2006. [Google Scholar]
- Santos, A.C.B. Frequência de Consumo de Frutas, Hortaliças e Produtos Ultraprocessados e Estado Nutricional de Gestantes de Cruzeiro Do Sul, Acre. Master’s Thesis, Universidade de São Paulo, São Paulo, Brazil, 2016. [Google Scholar]
- Santos, A.M.C.; Azeredo, V.B.; Boaventura, G.T. Estado Nutricional de Gestantes Adolescentes de Um Serviço Público de Referência Para Assistência Pré-Natal de Alto Risco. Nutr. Bras. 2009, 8, 344. [Google Scholar]
- Bezerra, A.S.; Cardoso, V.V.B.P.; Barbosa, V.S.A. Estado Nutricional, Anemia e Parasitoses Intestinais Em Gestantes de Um Município Do Curimataú Paraibano. Rev. APS 2018, 21, 15910. [Google Scholar] [CrossRef] [Green Version]
- Santos, F.F.; Conceição, S.I.O.; Monteiro, S.G. Anemia Em Gestantes Atendidas Em Maternidades, Em São Luís (MA). Cad. Pesqui. 2012, 19, 54–61. [Google Scholar]
- Silva, D.F.S. Anemia Ferropriva e Fatores Associados Em Gestantes Assistidas Em Hospital de Referência Do Estado de Pernambuco. Master’s Thesis, Universidade Federal de Pernambuco, Recife, Brazil, 2012. [Google Scholar]
- Silva, S.A.M.D.S. Anemia Em Gestantes Usuárias Do Serviço Público de Saúde Em Santo Antônio de Jesus—BA. Master’s Thesis, Universidade Federal do Recôncavo da Bahia, Cruz das Almas, Bahia, Brazil, 2014. [Google Scholar]
- Silva, R.M. Determinantes Da Anemia Em Gestantes Usuárias Do Programa de Saúde Da Família No Município de Santo Antônio de Jesus—Bahia. Master’s Thesis, Universidad Estatal de Feira de Santana, Feira de Santana, Brazil, 2015. [Google Scholar]
- Soares, N.N.; Mattar, R.; Camano, L.; Torloni, M.R. Iron Deficiency Anemia and Iron Stores in Adult and Adolescent Women in Pregnancy. Acta Obstet. Gynecol. Scand. 2010, 89, 343–349. [Google Scholar] [CrossRef] [PubMed]
- Soares, F.M.M.; Nunes, R.d.S.; Henrique, I.d.S.N.; Simão, A.L.S. Incidência de Anemia Ferropriva Em Gestantes Em Um Município de Pequeno Porte. Revista Rede de Cuidados em Saúde 2021, 15, 74–83. [Google Scholar]
- Szarfarc, S.C. Anemia Ferropriva Em Parturientes e Recém-Nascidos. Rev. Saude Publica 1974, 8, 369–374. [Google Scholar] [CrossRef] [Green Version]
- Camargo, R.; Pereira, R. Fatores Associados à Deficiência de Ferro Em Gestantes Atendidas Em Serviço Público de Pré-Natal. Rev. Nutr. 2013, 26, 455–464. [Google Scholar] [CrossRef] [Green Version]
- Côrtes, M.H. Impacto Da Fortificação Das Farinhas de Trigo e de Milho Com Ferro Nos Níveis de Hemoglobina Das Gestantes Atendidas Pelo Pré-Natal Do Hospital Universitário de Brasília/DF. Master’s Thesis, Universidade de Brasília, Brasília, Brazil, 2006. [Google Scholar]
- Costa, C.M.; Brum, I.R.; Lima, E.S. Anemia e Marcadores Séricos Da Deficiência de Ferro Em Grávidas Atendidas Na Rede Pública Municipal de Manaus, Amazonas, Brasil. Acta Amaz. 2009, 39, 901–905. [Google Scholar] [CrossRef] [Green Version]
- Dias, A.C.P. Anemia Ferropriva Em Gestantes Adolescentes Atendidas Em Postos de Saúde de Araraquara-SP. Master’s Thesis, Universidade Estadual Paulista Júlio de Mesquita Filho, Araraquara, Brazil, 2000. [Google Scholar]
- Ferreira, H.S.; Moura, F.A.; Cabral Júnior, C.R. Prevalência e Fatores Associados à Anemia Em Gestantes Da Região Semi-Árida Do Estado de Alagoas. Rev. Bras. Ginecol. Obs. 2008, 30, 445–451. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Figueiredo, A.C.M.G.; Gomes-Filho, I.S.; Batista, J.E.T.; Orrico, G.S.; Porto, E.C.L.; Pimenta, R.M.C.; Conceição, S.D.S.; Brito, S.M.; de Santana Xavier Ramos, M.; Sena, M.C.F.; et al. Maternal Anemia and Birth Weight: A Prospective Cohort Study. PLoS ONE 2019, 14, e0212817. [Google Scholar] [CrossRef]
- World Health Organization (WHO). Haemoglobin Concentrations for the Diagnosis of Anaemia and Assessment of Severity; Chan, M., Ed.; World Health Organization: Geneva, Switzerland, 2011; pp. 1–6. [Google Scholar]
- Macena, M.; Praxedes, D.; Oliveira, A.D.; Paula, D.; Barros, M.; Júnior, A.S.; Araújo, W.; Pureza, I.; de Melo, I.S.; Bueno, N. Prevalence of Iron Deficiency Anemia in Brazilian Women of Childbearing Age: A Systematic Review with Meta-Analysis. PeerJ 2022, 10, e12959. [Google Scholar] [CrossRef] [PubMed]
- Annan, R.A.; Gyimah, L.A.; Apprey, C.; Edusei, A.K.; Asamoah-Boakye, O.; Aduku, L.N.E.; Azanu, W.; Lutterodt, H.E. Factors Associated with Iron Deficiency Anaemia among Pregnant Teenagers in Ashanti Region, Ghana: A Hospital-Based Prospective Cohort Study. PLoS ONE 2021, 16, e0250246. [Google Scholar] [CrossRef] [PubMed]
- Hruschka, D.J.; Williams, A.M.; Mei, Z.; Leidman, E.; Suchdev, P.S.; Young, M.F.; Namaste, S. Comparing Hemoglobin Distributions between Population-Based Surveys Matched by Country and Time. BMC Public Health 2020, 20, 422. [Google Scholar] [CrossRef] [PubMed]
- Leal, L.P.; Filho, M.B.; De Cabral Lira, P.I.; Figueiroa, J.N.; Osó Rio, M.M. Temporal Trends and Anaemia-Associated Factors in 6-to 59-Month-Old Children in Northeast Brazil. Public Health Nutr. 2012, 15, 1645–1652. [Google Scholar] [CrossRef] [Green Version]
- Brazil. Resolução de Diretoria Colegiada No 344, de 13 de Dezembro de 2002 (Collegiate Board Resolution 344, of December 13, 2002). Available online: https://bvsms.saude.gov.br/bvs/saudelegis/anvisa/2002/rdc0344_13_12_2002.html (accessed on 28 June 2022).
- da BRASIL, M.S. Regulamento Técnico Para a Fortificação Das Farinhas de Trigo e Das Farinhas de Milho Com Ferro e Ácido Fólico. Resolução RDC No 344, de 13 de Dezembro de 2002. 2002. Available online: http://antigo.anvisa.gov.br/documents/33880/2568070/RDC_344_2002.pdf/dd69b7d7-e5dc-41d1-a6fd-68af0c4bea63?version=1.0 (accessed on 28 June 2022).
- Sato, A.P.S.; Fujimori, E.; Szarfarc, S.C.; Sato, J.R.; Bonadio, I.C. Prevalência de Anemia Em Gestantes e a Fortificaçãoo de Farinhas Com Ferro. Texto Context. Enferm 2008, 17, 474–481. [Google Scholar] [CrossRef]
- Vellozo, E.P.; Fisberg, M. O Impacto Da Fortificação de Alimentos Na Prevenção Da Deficiência de Ferro. Rev. Bras. Hematol. Hemoter. 2010, 32, 134–139. [Google Scholar] [CrossRef] [Green Version]
- Cassimiro, G.N.; da Mata, J.A.L. Adesão Ao Uso de Sulfato Ferroso Por Gestantes Atendidas No Sistema Único de Saúde TT—Adhesion to the Use of Ferrous Sulphate by Pregnant Women Served in the Unified Health System. Rev. Enferm. UFPE Line 2017, 11, 2156–2167. [Google Scholar] [CrossRef]
- World Health Organization; United Nations. Children’s Fund the Extension of the 2025 Maternal, Infant and Young Child Nutrition Targets to 2030. Discussion Paper. 2019. Available online: https://data.unicef.org/resources/who-unicef-discussion-paper-nutrition-targets/ (accessed on 28 June 2022).
- Barros, D.D.M.; da Silva, A.P.F.; de Moura, D.F.; Barros, M.V.C.; Pereira, A.B.S.; Melo, M.A.; Silva, A.L.B.; Rocha, T.A.; Ferreira, S.A.O.; Siqueira, T.T.A.; et al. A Influência Da Transição Alimentar E Nutricional Sobre o Aumento da Prevalência de Doenças Crônicas Não Transmissíveis. Braz. J. Dev. 2021, 7, 74647–74664. [Google Scholar] [CrossRef]
- Batista Filho, M.; Souza, A.I.; Miglioli, T.C.; Santos, M.C. Anemia e Obesidade: Um Paradoxo da Transição Nutricional Brasileira. Cad. Saude Publica 2008, 24, 247–257. [Google Scholar] [CrossRef] [PubMed]
- IBGE. Brasil Pesquisa de Orçamentos Familiares 2017–2018: Primeiros Resultados; IBGE—Instituto Brasileiro de Geografia Estatística: Rio de Janeiro, Brazil, 2019; ISBN 9788524041389. [Google Scholar]




{kind=link}
{kind=link}
{kind=link}
| Author | Study Period | Geographic Region of Brazil | Study Design | Location of Data Collection | Age (Range or Mean) | Gestational Age (Range or Mean) | Sample Size n | Capillary or Venous | Criteria for Anemia Status | Prevalence of Anaemia (%) | 95% CI | Quality Grade (Risk) |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Soares et al. (2021) [56] | 2020 | Northeast | Cross-sectional | Primary health unit | 12–45 | NR | 278 | Venous | WHO (Hb < 11 g/dL) | 26.98 | 22.01; 32.43 | High |
| Figueiredo et al. (2019) [63] | 2013–2017 | Northeast | Cohort | Primary health unit | 13–46 | NR | 622 | Venous | WHO (Hb < 11 g/dL) | 24.9 | 21.64; 28.43 | High |
| Santana et al. (2019) [46] | 2012 | Northeast | Cross-sectional | Primary health unit | NR | NR | 208 | Venous | WHO (Hb < 11 g/dL) | 16.8 | 12.2; 22.37 | High |
| Bezerra et al. (2018) [50] | 2014 | Northeast | Cross-sectional | Community | 14–37 | 1st, 2nd and 3rd Trimester | 45 | Venous | WHO (Hb < 11 g/dL) | 7 | 1.72; 17.08 | High |
| Frick et al. (2018) [29] | 2009–2011 | South | Cross-sectional | Primary health unit | 10–49 | 1st Trimester | 107 | Venous | WHO (Hb < 11 g/dL) | 14.02 | 8.37; 21.59 | High |
| Magalhães et al. (2018) [34] | 2010–2011 | Northeast | Cross-sectional | Primary health unit | 20–35 | 1st, 2nd and 3rd Trimester | 328 | Capillary | WHO (Hb < 11 g/dL) | 18.9 | 14.94; 23.41 | High |
| Miranda et al. (2018) [36] | 2015 | South | Cohort | Community | 13–46 | NR | 3419 | Venous | WHO (Hb < 11 g/dL) | 35.9 | 34.29; 37.51 | High |
| Neme et al. (2017) [37] | 2008 | South | Cross-sectional | Primary health unit | NR | NR | 91 | Venous | WHO (Hb < 11 g/dL) | 35.16 | 25.88; 45.38 | High |
| Santos (2016) [48] | 2015–2016 | North | Cross-sectional | Primary health unit | 13–40 | 2nd Trimester | 506 | Venous | WHO (Hb < 11 g/dL) | 15.4 | 12.3; 18.9 | High |
| Silva (2015) [54] | 2013 | Northeast | Cross-sectional | Primary health unit | 13–41 | 1st, 2nd and 3rd Trimester | 349 | Venous | WHO (Hb < 11 g/dL) | 22.64 | 18.47; 27.25 | High |
| Oliveira et al. (2015) [38] | 2014 | Northeast | Cross-sectional | Primary health unit | 14–44 | NR | 428 | Capillary | WHO (Hb < 11 g/dL) | 28.30 | 24.16; 32.68 | Low |
| Silva (2014) [53] | 2013 | Northeast | Cross-sectional+E11 | Primary health unit | 14–40 | 1st, 2nd and 3rd Trimester | 201 | Venous | WHO (Hb < 11 g/dL) | 27.86 | 21.99; 34.36 | High |
| Aragão et al. (2013) [27] | 2011 | Northeast | Cross-sectional | Hospital | 15–40 | 1st, 2nd and 3rd Trimester | 59 | Venous | WHO (Hb < 11 g/dL) | 20.3 | 11.51; 32.02 | High |
| Camargo et al. (2013) [58] | 2008–2009 | Midwest | Cross-sectional | University Hospital | 19–49 | 2nd Trimester | 146 | Venous | WHO (Hb < 11 g/dL) | 5 | 2.121; 9.25 | High |
| Marion (2013) [35] | 2011 | South | Cross-sectional | University Hospital | 16–44 | 1st, 2nd and 3rd Trimester | 124 | Venous | WHO (Hb < 11 g/dL) | 16.2 | 10.43; 23.4 | High |
| Santos et al. (2012) [51] | 2008 | Northeast | Cross-sectional | Maternity | 16–40 | 1st, 2nd and 3rd Trimester | 118 | Venous | WHO (Hb < 11 g/dL) | 32.2 | 24.32; 41.03 | High |
| Silva (2012) [52] | 2011–2012 | Northeast | Cross-sectional | Hospital | 18–35 | NR | 611 | Venous | WHO (Hb < 11 g/dL) | 29.9 | 26.42; 33.67 | High |
| Quintans (2011) [42] | 2009 | Northeast | Cross-sectional | Primary health unit | 18–42 | 1st, 2nd and 3rd Trimester | 130 | Venous | WHO (Hb < 11 g/dL) | 17.7 | 11.84; 24.97 | High |
| Soares et al. (2010) [55] | 2004–2008 | Southeast | Cohort | Prenatal clinic | 15–37 | NR | 183 | Venous | WHO (Hb < 11 g/dL) | 10.4 | 6.55; 15.45 | High |
| Costa et al. (2009) [60] | 2006 | North | Cross-sectional | Primary health unit | NR | 1st, 2nd and 3rd Trimester | 92 | Venous | WHO (Hb < 11 g/dL) | 26.1 | 17.89; 35.77 | High |
| Santos et al. (2009) [49] | NR | Southeast | Cross-sectional | Prenatal clinic | 13–17 | 3rd Trimester | 24 | Venous | WHO (Hb < 11 g/dL) | 41.6 | 23.45; 61.79 | High |
| Ferreira et al. (2008) [62] | 2007 | Northeast | Cross-sectional | Community | 16–43 | 1st, 2nd and 3rd Trimester | 150 | Capillary | WHO (Hb < 11 g/dL) | 50 | 42.04; 57.96 | High |
| Sakamoto (2008) [45] | 2007 | Midwest | Cross-sectional | University Hospital | 14–42 | 1st, 2nd and 3rd Trimester | 233 | Venous | WHO (Hb < 11 g/dL) | 18 | 13.48; 23.36 | High |
| Paiva et al. (2007) [40] | 2000 | Southeast | Cross-sectional | Hospital | NR | NR | 95 | Venous | WHO (Hb < 11 g/dL) | 19 | 12; 27.76 | High |
| Côrtes (2006) [59] | 2004 | Midwest | Cross-sectional | University Hospital | <20, >35 | 1st, 2nd and 3rd Trimester | 228 | Capillary | WHO (Hb < 11 g/dL) | 28.94 | 23.34; 35.09 | Low |
| Lucyk (2006) [33] | 2005 | Midwest | Cross-sectional | University Hospital | NR | 1st, 2nd and 3rd Trimester | 170 | Capillary | WHO (Hb < 11 g/dL) | 19.40 | 13.98; 25.87 | High |
| Santos (2006) [47] | 2005–2006 | Northeast | Cross-sectional | Primary health unit | 12–44 | 1st, 2nd and 3rd Trimester | 326 | Venous | WHO (Hb < 11 g/dL) | 31.9 | 27.01; 37.11 | High |
| Rocha et al. (2005) [43] | 2002–2003 | Southeast | Cross-sectional | Primary health unit | 14–38 | 1st, 2nd and 3rd Trimester | 168 | Capillary | WHO (Hb < 11 g/dL) | 21.4 | 15.72; 28.12 | High |
| Papa et al. (2003) [41] | 2001–2002 | Southeast | Cross-sectional | University | >16 | 1st and 2nd Trimester | 56 | Venous | WHO (Hb < 11 g/dL) | 21.4 | 12.16; 33.59 | High |
| Dias (2000) [61] | NR | Southeast | Cross-sectional | Primary health unit | NR | NR | 36 | Venous | WHO (Hb < 11 g/dL) | 10 | 3.63; 24.66 | High |
| Fujimori et al. (2000) [31] | 2000 | Southeast | Cross-sectional | Primary health unit | NR | 1st, 2nd and 3rd Trimester | 72 | Venous | WHO (Hb < 11 g/dL) | 13.9 | 7.27; 23.36 | High |
| Arruda (1997) [39] | 1992 | Northeast | Cross-sectional | Maternity | NR | NR | 1007 | Venous | WHO (Hb < 11 g/dL) | 30.88 | 28.09; 33.79 | High |
| Fujimori (1994) [30] | 1993 | Southeast | Cross-sectional | Maternity | 13–19 | 1st, 2nd and 3rd Trimester | 155 | Venous | WHO (Hb < 11 g/dL) | 14.2 | 9.34; 20.37 | High |
| Rodriguez et al. (1991) [44] | NR | Southeast | Cross-sectional | Hospital | NR | NR | 691 | Venous | WHO (Hb < 11 g/dL) | 29.2 | 25.93; 32.71 | High |
| Arruda (1990) [28] | 1989 | Northeast | Cross-sectional | Maternity | 13–44 | 1st, 2nd and 3rd Trimester | 710 | Venous | WHO (Hb < 11 g/dL) | 30.3 | 26.98; 33.74 | High |
| Guerra et al. (1990) [32] | 1988 | Southeast | Cross-sectional | Primary health unit | 14–46 | 1st, 2nd and 3rd Trimester | 363 | Venous | HURTADO et al., 1945, FINCH, 1969 (<11.6 g/dL) | 12.4 | 9.29; 16.09 | High |
| Szarfarc (1974) [57] | NR | Southeast | Cross-sectional | Philanthropic Unit | NR | 3rd Trimester | 263 | Venous | Benjamin, Rauramo et al. e de Sanchez-Medal (<12 g/dL) | 52.3 | 46.43; 58.46 | High |
| Variables | Number of Studies | Number of Participants | Prevalence (%) | 95% CI | I2 (%) | p (Chi-Squared) | I2 between Groups (%) | p (Chi-Squared) between Groups |
|---|---|---|---|---|---|---|---|---|
| Sample size | 95.02 | 0.00 | ||||||
| ≤500 | 30.00 | 5226.00 | 22.00 | 18–26 | 92.50 | 0.00 | ||
| >500 | 7.00 | 7566.00 | 28.00 | 23–33 | 95.80 | 0.00 | ||
| Age | 95.02 | 0.00 | ||||||
| Adolescents | 4.00 | 271.00 | 19.00 | 10–28 | 65.62 | 0.03 | ||
| Adults and Adolescents | 26.00 | 11,009.00 | 23.00 | 19–27 | 95.76 | 0.00 | ||
| Not Reported | 7.00 | 1512.00 | 28.00 | 18–37 | 94.04 | 0.00 | ||
| Gestational Trimester | 95.02 | 0.00 | ||||||
| All | 21.00 | 5460.00 | 24.00 | 20–27 | 89.07 | 0.00 | ||
| Only one or two | 8.00 | 1269.00 | 22.00 | 11–33 | 96.27 | 0.00 | ||
| Not Reported | 8.00 | 6063.00 | 25.00 | 18–31 | 95.80 | 0.00 | ||
| Region | 95.02 | 0.00 | ||||||
| North | 2.00 | 598.00 | 17.00 | 14–20 | ||||
| Northeast | 16.00 | 5570.00 | 26.00 | 23–29 | 87.70 | 0.00 | ||
| Midwest | 4.00 | 777.00 | 18.00 | 07–28 | 94.79 | 0.00 | ||
| Southeast | 11.00 | 2106.00 | 22.00 | 14–30 | 94.72 | 0.00 | ||
| South | 4.00 | 3741.00 | 25.00 | 12–38 | 95.70 | 0.00 | ||
| Data collection period | 95.02 | 0.00 | ||||||
| Before 2004 | 11.00 | 3616.00 | 24.00 | 17–30 | 94.89 | 0.00 | ||
| After 2004 | 26.00 | 9176.00 | 23.00 | 19–28 | 95.26 | 0.00 | ||
| Data collection period | 95.02 | 0.00 | ||||||
| Before 2011 | 25.00 | 5942.00 | 24.00 | 19–28 | 94.53 | 0.00 | ||
| After 2011 | 12.00 | 6850.00 | 23.00 | 18–28 | 95.18 | 0.00 | ||
| Hb determination method | 95.02 | 0.00 | ||||||
| Capillary | 6.00 | 1472.00 | 27.00 | 20–35 | 90.74 | 0.00 | ||
| Venous | 31.00 | 11,320.00 | 23.00 | 19–27 | 95.52 | 0.00 | ||
| Methodological quality | 95.28 | 0.00 | 95.02 | 0.00 | ||||
| Low | 2.00 | 656.00 | 29.00 | 25–32 | ||||
| High | 35.00 | 12,136.00 | 23.00 | 20–27 |
| Outcomes | Risk of Bias a | Inconsistency b | Indirectness c | Imprecision d | Publication Bias e | Certainty |
|---|---|---|---|---|---|---|
| Prevalence of anaemia in Brazilian pregnant women | Very serious | Very Serious | Not serious | Serious | Not serious | ⊕◯◯◯ Very low |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Biete, A.; Gonçalves, V.S.S.; Franceschini, S.C.C.; Nilson, E.A.F.; Pizato, N. The Prevalence of Nutritional Anaemia in Brazilian Pregnant Women: A Systematic Review and Meta-Analysis. Int. J. Environ. Res. Public Health 2023, 20, 1519. https://doi.org/10.3390/ijerph20021519
Biete A, Gonçalves VSS, Franceschini SCC, Nilson EAF, Pizato N. The Prevalence of Nutritional Anaemia in Brazilian Pregnant Women: A Systematic Review and Meta-Analysis. International Journal of Environmental Research and Public Health. 2023; 20(2):1519. https://doi.org/10.3390/ijerph20021519
Chicago/Turabian StyleBiete, Amanda, Vivian S. S. Gonçalves, Sylvia C. C. Franceschini, Eduardo A. F. Nilson, and Nathalia Pizato. 2023. "The Prevalence of Nutritional Anaemia in Brazilian Pregnant Women: A Systematic Review and Meta-Analysis" International Journal of Environmental Research and Public Health 20, no. 2: 1519. https://doi.org/10.3390/ijerph20021519