
Past Traumatic Life Events, Postpartum PTSD, and the Role of Labor Support
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Ethical Considerations
2.3. Measures
2.3.1. Demographic and Obstetric Variables
2.3.2. Birth-Related Trauma and Past Traumatic Experience
2.3.3. Postpartum Depression (PPD)
2.3.4. Postpartum PTSD (PP-PTSD)
2.3.5. Covariates
2.3.6. Statistical Analyses
3. Results
3.1. Prevalence of Postpartum Depressive and PTSD Symptoms and Past Traumatic Experience
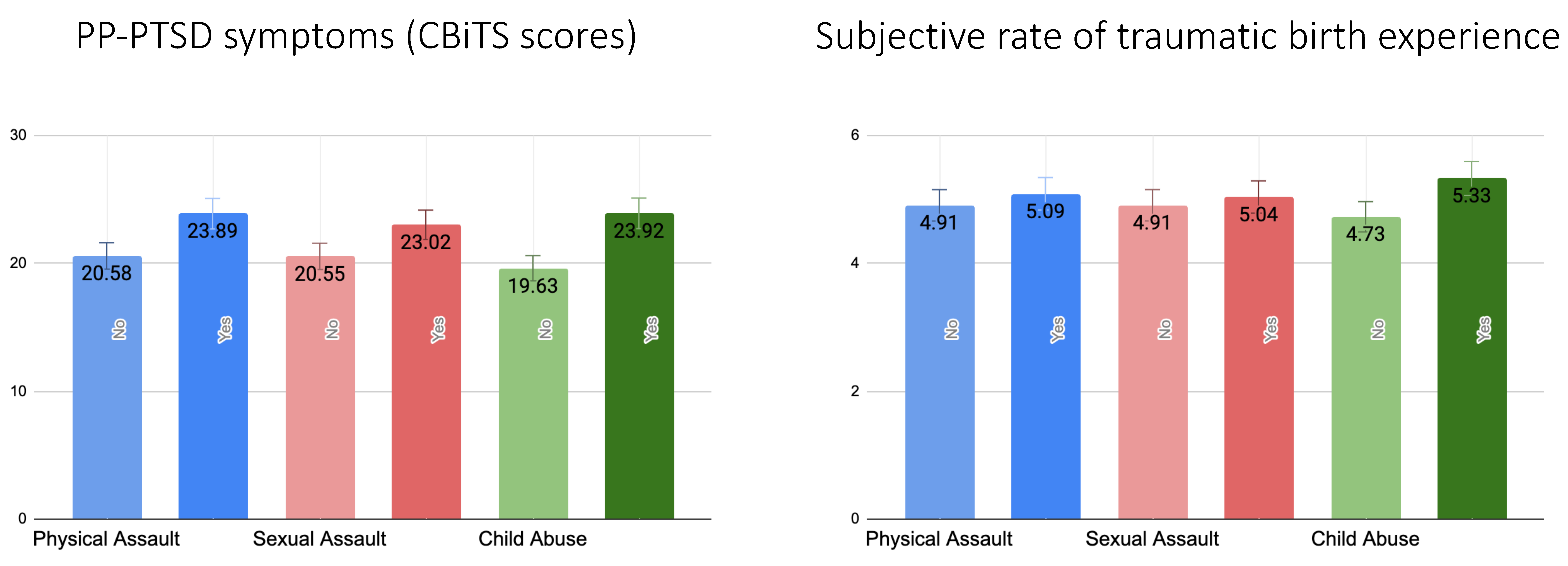
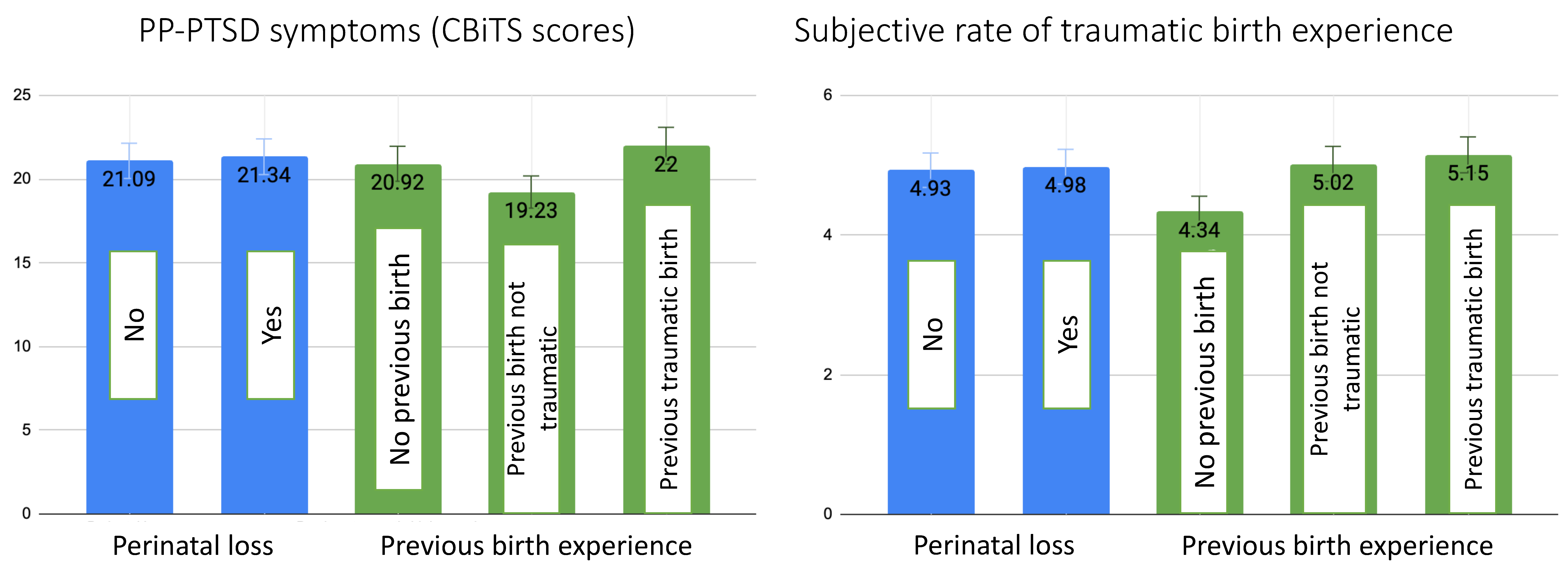
3.2. Postpartum PTSD and Past Traumatic Experiences
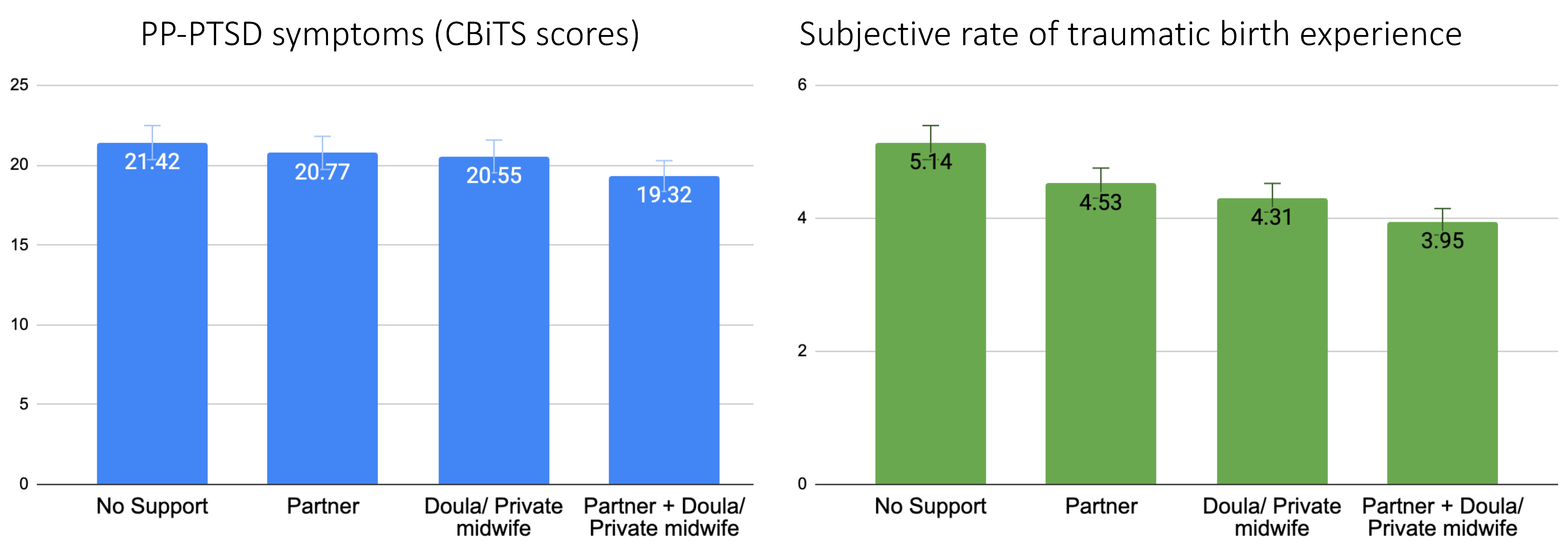
3.3. Postpartum PTSD and Support during Labour
3.4. Moderation Analysis
4. Discussion
5. Strengths and Limitations
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- O’Donovan, A.; Alcorn, K.L.; Patrick, J.C.; Creedy, D.K.; Dawe, S.; Devilly, G.J. Predicting Posttraumatic Stress Disorder after Childbirth. Midwifery 2014, 30, 935–941. [Google Scholar] [CrossRef] [Green Version]
- De Graaff, L.F.; Honig, A.; Van Pampus, M.G.; Stramrood, C.A.I. Preventing Post-Traumatic Stress Disorder Following Childbirth and Traumatic Birth Experiences: A Systematic Review. Acta Obstet. Gynecol. Scand. 2018, 97, 648–656. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stramrood, C.A.I.; Paarlberg, K.M.; Huis In’t Veld, E.M.J.; Berger, L.W.A.R.; Vingerhoets, A.J.J.M.; Schultz, W.C.M.W.; van Pampus, M.G. Posttraumatic Stress Following Childbirth in Homelike- and Hospital Settings. J. Psychosom. Obstet. Gynaecol. 2011, 32, 88–97. [Google Scholar] [CrossRef]
- Grekin, R.; O’Hara, M.W. Prevalence and Risk Factors of Postpartum Posttraumatic Stress Disorder: A Meta-Analysis. Clin. Psychol. Rev. 2014, 34, 389–401. [Google Scholar] [CrossRef] [PubMed]
- Dekel, S.; Stuebe, C.; Dishy, G. Childbirth Induced Posttraumatic Stress Syndrome: A Systematic Review of Prevalence and Risk Factors. Front. Psychol. 2017, 8, 560. [Google Scholar] [CrossRef] [Green Version]
- Yildiz, P.D.; Ayers, S.; Phillips, L. The Prevalence of Posttraumatic Stress Disorder in Pregnancy and after Birth: A Systematic Review and Meta-Analysis. J. Affect. Disord. 2017, 208, 634–645. [Google Scholar] [CrossRef] [PubMed]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders: DSM-5TM, 5th ed.; American Psychiatric Publishing, Inc.: Arlington, VA, USA, 2013. [Google Scholar] [CrossRef]
- Beck, C.T. Post-Traumatic Stress Disorder Due to Childbirth: The Aftermath. Nurs. Res. 2004, 53, 216–224. [Google Scholar] [CrossRef] [Green Version]
- Beck, C.T.; Casavant, S. Synthesis of Mixed Research on Posttraumatic Stress Related to Traumatic Birth. J. Obstet. Gynecol. Neonatal Nurs. JOGNN 2019, 48, 385–397. [Google Scholar] [CrossRef]
- Beck, C.T.; Gable, R.K.; Sakala, C.; Declercq, E.R. Posttraumatic Stress Disorder in New Mothers: Results from a Two-Stage U.S. National Survey. Birth 2011, 38, 216–227. [Google Scholar] [CrossRef]
- Ayers, S.; Eagle, A.; Waring, H. The Effects of Childbirth-Related Post-Traumatic Stress Disorder on Women and Their Relationships: A Qualitative Study. Psychol. Health Med. 2006, 11, 389–398. [Google Scholar] [CrossRef] [Green Version]
- Garthus-Niegel, S.; Horsch, A.; Ayers, S.; Junge-Hoffmeister, J.; Weidner, K.; Eberhard-Gran, M. The Influence of Postpartum PTSD on Breastfeeding: A Longitudinal Population-Based Study. Birth 2018, 45, 193–201. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Beck, C.T.; Watson, S. Impact of Birth Trauma on Breast-Feeding: A Tale of Two Pathways. Nurs. Res. 2008, 57, 228–236. [Google Scholar] [CrossRef] [PubMed]
- Cook, N.; Ayers, S.; Horsch, A. Maternal Posttraumatic Stress Disorder during the Perinatal Period and Child Outcomes: A Systematic Review. J. Affect. Disord. 2018, 225, 18–31. [Google Scholar] [CrossRef] [PubMed]
- Kjerulff, K.H.; Attanasio, L.B.; Sznajder, K.K.; Brubaker, L.H. A Prospective Cohort Study of Post-Traumatic Stress Disorder and Maternal-Infant Bonding after First Childbirth. J. Psychosom. Res. 2021, 144, 110424. [Google Scholar] [CrossRef] [PubMed]
- Dekel, S.; Thiel, F.; Dishy, G.; Ashenfarb, A.L. Is Childbirth-Induced PTSD Associated with Low Maternal Attachment? Arch. Womens Ment. Health 2019, 22, 119–122. [Google Scholar] [CrossRef]
- Delicate, A.; Ayers, S.; Easter, A.; McMullen, S. The Impact of Childbirth-Related Post-Traumatic Stress on a Couple’s Relationship: A Systematic Review and Meta-Synthesis. J. Reprod. Infant Psychol. 2018, 36, 102–115. [Google Scholar] [CrossRef]
- Vogel, T.M.; Homitsky, S. Antepartum and Intrapartum Risk Factors and the Impact of PTSD on Mother and Child. BJA Educ. 2020, 20, 89–95. [Google Scholar] [CrossRef]
- Ayers, S.; Bond, R.; Bertullies, S.; Wijma, K. The Aetiology of Post-Traumatic Stress Following Childbirth: A Meta-Analysis and Theoretical Framework. Psychol. Med. 2016, 46, 1121–1134. [Google Scholar] [CrossRef] [Green Version]
- Yakupova, V.; Suarez, A. Postpartum PTSD and Birth Experience in Russian-Speaking Women. Midwifery 2022, 112, 103385. [Google Scholar] [CrossRef]
- Anderson, C.; Cacola, P. Implications of Preterm Birth for Maternal Mental Health and Infant Development. MCN Am. J. Matern. Child Nurs. 2017, 42, 108–114. [Google Scholar] [CrossRef]
- Hollander, M.H.; van Hastenberg, E.; van Dillen, J.; van Pampus, M.G.; de Miranda, E.; Stramrood, C.A.I. Preventing Traumatic Childbirth Experiences: 2192 Women’s Perceptions and Views. Arch. Womens Ment. Health 2017, 20, 515–523. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Martínez-Vazquez, S.; Rodríguez-Almagro, J.; Hernández-Martínez, A.; Delgado-Rodríguez, M.; Martínez-Galiano, J.M. Long-Term High Risk of Postpartum Post-Traumatic Stress Disorder (PTSD) and Associated Factors. J. Clin. Med. 2021, 10, 488. [Google Scholar] [CrossRef] [PubMed]
- Yakupova, V.; Suarez, A.; Kharchenko, A. Birth Experience, Postpartum PTSD and Depression before and during the Pandemic of COVID-19 in Russia. Int. J. Environ. Res. Public Health 2021, 19, 335. [Google Scholar] [CrossRef] [PubMed]
- Martinez-Vázquez, S.; Rodríguez-Almagro, J.; Hernández-Martínez, A.; Martínez-Galiano, J.M. Factors Associated with Postpartum Post-Traumatic Stress Disorder (PTSD) Following Obstetric Violence: A Cross-Sectional Study. J. Pers. Med. 2021, 11, 338. [Google Scholar] [CrossRef] [PubMed]
- Andersen, L.B.; Melvaer, L.B.; Videbech, P.; Lamont, R.F.; Joergensen, J.S. Risk Factors for Developing Post-Traumatic Stress Disorder Following Childbirth: A Systematic Review. Acta Obstet. Gynecol. Scand. 2012, 91, 1261–1272. [Google Scholar] [CrossRef] [PubMed]
- Chabbert, M.; Panagiotou, D.; Wendland, J. Predictive Factors of Women’s Subjective Perception of Childbirth Experience: A Systematic Review of the Literature. J. Reprod. Infant Psychol. 2021, 39, 43–66. [Google Scholar] [CrossRef]
- Simpson, M.; Catling, C. Understanding Psychological Traumatic Birth Experiences: A Literature Review. Women Birth J. Aust. Coll. Midwives 2016, 29, 203–207. [Google Scholar] [CrossRef]
- De Oliveira, A.G.E.S.; Reichenheim, M.E.; Moraes, C.L.; Howard, L.M.; Lobato, G. Childhood Sexual Abuse, Intimate Partner Violence during Pregnancy, and Posttraumatic Stress Symptoms Following Childbirth: A Path Analysis. Arch. Womens Ment. Health 2017, 20, 297–309. [Google Scholar] [CrossRef]
- Seng, J.S.; Low, L.K.; Sperlich, M.; Ronis, D.L.; Liberzon, I. Prevalence, Trauma History, and Risk for Posttraumatic Stress Disorder among Nulliparous Women in Maternity Care. Obstet. Gynecol. 2009, 114, 839–847. [Google Scholar] [CrossRef] [Green Version]
- Wosu, A.C.; Gelaye, B.; Williams, M.A. Childhood Sexual Abuse and Posttraumatic Stress Disorder among Pregnant and Postpartum Women: Review of the Literature. Arch. Womens Ment. Health 2015, 18, 61–72. [Google Scholar] [CrossRef] [Green Version]
- Berman, Z.; Thiel, F.; Kaimal, A.J.; Dekel, S. Association of Sexual Assault History with Traumatic Childbirth and Subsequent PTSD. Arch. Womens Ment. Health 2021, 24, 767–771. [Google Scholar] [CrossRef] [PubMed]
- Global Status Report on Preventing Violence against Children 2020. Available online: https://www.who.int/publications-detail-redirect/9789240004191 (accessed on 5 February 2023).
- Sardinha, L.; Maheu-Giroux, M.; Stöckl, H.; Meyer, S.R.; García-Moreno, C. Global, Regional, and National Prevalence Estimates of Physical or Sexual, or Both, Intimate Partner Violence against Women in 2018. Lancet 2022, 399, 803–813. [Google Scholar] [CrossRef] [PubMed]
- Hutti, M.H.; Myers, J.; Hall, L.A.; Polivka, B.J.; White, S.; Hill, J.; Kloenne, E.; Hayden, J.; Grisanti, M.M. Predicting Grief Intensity after Recent Perinatal Loss. J. Psychosom. Res. 2017, 101, 128–134. [Google Scholar] [CrossRef] [PubMed]
- Krosch, D.J.; Shakespeare-Finch, J. Grief, Traumatic Stress, and Posttraumatic Growth in Women Who Have Experienced Pregnancy Loss. Psychol. Trauma Theory Res. Pract. Policy 2017, 9, 425–433. [Google Scholar] [CrossRef] [Green Version]
- Horesh, D.; Nukrian, M.; Bialik, Y. To Lose an Unborn Child: Post-Traumatic Stress Disorder and Major Depressive Disorder Following Pregnancy Loss among Israeli Women. Gen. Hosp. Psychiatry 2018, 53, 95–100. [Google Scholar] [CrossRef]
- Engelhard, I.M.; van den Hout, M.A.; Arntz, A. Posttraumatic Stress Disorder after Pregnancy Loss. Gen. Hosp. Psychiatry 2001, 23, 62–66. [Google Scholar] [CrossRef]
- Herbert, D.; Young, K.; Pietrusińska, M.; MacBeth, A. The Mental Health Impact of Perinatal Loss: A Systematic Review and Meta-Analysis. J. Affect. Disord. 2022, 297, 118–129. [Google Scholar] [CrossRef]
- Fernández Ordóñez, E.; Rengel Díaz, C.; Morales Gil, I.M.; Labajos Manzanares, M.T.; Fernández Ordóñez, E.; Rengel Díaz, C.; Morales Gil, I.M.; Labajos Manzanares, M.T. Post-Traumatic Stress Disorder after Subsequent Birth to a Gestational Loss: An Observational Study. Salud Ment. 2020, 43, 129–136. [Google Scholar] [CrossRef]
- Berry, S.N. The Trauma of Perinatal Loss: A Scoping Review. Trauma Care 2022, 2, 392–407. [Google Scholar] [CrossRef]
- Hodnett, E.D.; Gates, S.; Hofmeyr, G.J.; Sakala, C. Continuous Support for Women during Childbirth. Cochrane Database Syst. Rev. 2013, 7, CD003766. [Google Scholar] [CrossRef]
- Taheri, M.; Takian, A.; Taghizadeh, Z.; Jafari, N.; Sarafraz, N. Creating a Positive Perception of Childbirth Experience: Systematic Review and Meta-Analysis of Prenatal and Intrapartum Interventions. Reprod. Health 2018, 15, 73. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Schepper, S.; Vercauteren, T.; Tersago, J.; Jacquemyn, Y.; Raes, F.; Franck, E. Post-Traumatic Stress Disorder after Childbirth and the Influence of Maternity Team Care during Labour and Birth: A Cohort Study. Midwifery 2016, 32, 87–92. [Google Scholar] [CrossRef] [PubMed]
- Orovou, E.; Dagla, M.; Iatrakis, G.; Lykeridou, A.; Tzavara, C.; Antoniou, E. Correlation between Kind of Cesarean Section and Posttraumatic Stress Disorder in Greek Women. Int. J. Environ. Res. Public Health 2020, 17, 1592. [Google Scholar] [CrossRef] [Green Version]
- Handelzalts, J.E.; Levy, S.; Ayers, S.; Krissi, H.; Peled, Y. Two Are Better Than One? The Impact of Lay Birth Companions on Childbirth Experiences and PTSD. Arch. Womens Ment. Health 2022, 25, 797–805. [Google Scholar] [CrossRef]
- Suarez, A.; Yakupova, V. The Impacts of the COVID-19 Pandemic on Birth Satisfaction and Birth Experiences in Russian Women. Front. Glob. Womens Health 2022, 3, 1040879. [Google Scholar] [CrossRef]
- World Health Organization. Regional Office for Europe. Survey on the Prevalence of Adverse Childhood Experiences among Young People in the Russian Federation: Report; World Health Organization. Regional Office for Europe: Geneva, Switzerland, 2014. [Google Scholar]
- Julia, R. #Нетабу. Академия Безoпаснoсти Ольги Бoчкoвoй. Available online: https://bochkova.academy/netabu/ (accessed on 5 February 2023).
- Light in Hands. Специалистам|БФ «Свет в Руках». Available online: https://lightinhands.ru/specialistam/ (accessed on 5 February 2023).
- Yakupova, V.A. The Impact of Psychological and Physiological Conditions of Motherhood on Postnatal Depression. Russ. J. Psychol. 2018, 15, 8–23. (In Russia) [Google Scholar] [CrossRef] [Green Version]
- Cox, J.L.; Holden, J.M.; Sagovsky, R. Detection of Postnatal Depression. Development of the 10-Item Edinburgh Postnatal Depression Scale. Br. J. Psychiatry J. Ment. Sci. 1987, 150, 782–786. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ayers, S.; Wright, D.B.; Thornton, A. Development of a Measure of Postpartum PTSD: The City Birth Trauma Scale. Front. Psychiatry 2018, 9, 409. [Google Scholar] [CrossRef] [Green Version]
- Weigl, T.; Beck-Hiestermann, F.M.L.; Stenzel, N.; Benson, S.; Schedlowski, M.; Garthus-Niegel, S. Assessment of Childbirth-Related PTSD: Psychometric Properties of the German Version of the City Birth Trauma Scale. Front. Psychiatry 2021, 12, 731537. [Google Scholar] [CrossRef]
- Osório, F.D.L.; Rossini Darwin, A.C.; Bombonetti, E.A.; Ayers, S. Posttraumatic Stress Following Childbirth: Psychometric Properties of the Brazilian Version of the City Birth Trauma Scale. J. Psychosom. Obstet. Gynaecol. 2022, 43, 374–383. [Google Scholar] [CrossRef]
- Nagle, U.; Naughton, S.; Ayers, S.; Cooley, S.; Duffy, R.M.; Dikmen-Yildiz, P. A Survey of Perceived Traumatic Birth Experiences in an Irish Maternity Sample—Prevalence, Risk Factors and Follow Up. Midwifery 2022, 113, 103419. [Google Scholar] [CrossRef]
- Fisher, J.; de Mello, M.C.; Patel, V.; Rahman, A.; Tran, T.; Holton, S.; Holmes, W. Prevalence and Determinants of Common Perinatal Mental Disorders in Women in Low- and Lower-Middle-Income Countries: A Systematic Review. Bull. World Health Organ. 2012, 90, 139–149H. [Google Scholar] [CrossRef] [PubMed]
- IBM Corp. IBM SPSS Statistics for Macintosh; IBM Corp.: Armonk, NY, USA, 2020. [Google Scholar]
- Dekel, S.; Ein-Dor, T.; Dishy, G.A.; Mayopoulos, P.A. Beyond Postpartum Depression: Posttraumatic Stress-Depressive Response Following Childbirth. Arch. Womens Ment. Health 2020, 23, 557–564. [Google Scholar] [CrossRef] [PubMed]
- Dikmen-Yildiz, P.; Ayers, S.; Phillips, L. Longitudinal Trajectories of Post-Traumatic Stress Disorder (PTSD) after Birth and Associated Risk Factors. J. Affect. Disord. 2018, 229, 377–385. [Google Scholar] [CrossRef] [PubMed]
- McGowan, P.O.; Sasaki, A.; D’Alessio, A.C.; Dymov, S.; Labonté, B.; Szyf, M.; Turecki, G.; Meaney, M.J. Epigenetic Regulation of the Glucocorticoid Receptor in Human Brain Associates with Childhood Abuse. Nat. Neurosci. 2009, 12, 342–348. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Blanco, L.; Nydegger, L.A.; Camarillo, G.; Trinidad, D.R.; Schramm, E.; Ames, S.L. Neurological Changes in Brain Structure and Functions among Individuals with a History of Childhood Sexual Abuse: A Review. Neurosci. Biobehav. Rev. 2015, 57, 63–69. [Google Scholar] [CrossRef] [PubMed]
- Teicher, M.H.; Samson, J.A.; Anderson, C.M.; Ohashi, K. The Effects of Childhood Maltreatment on Brain Structure, Function and Connectivity. Nat. Rev. Neurosci. 2016, 17, 652–666. [Google Scholar] [CrossRef] [PubMed]
- Buss, C.; Entringer, S.; Reyes, J.F.; Chicz-DeMet, A.; Sandman, C.A.; Waffarn, F.; Wadhwa, P.D. The Maternal Cortisol Awakening Response in Human Pregnancy Is Associated with the Length of Gestation. Am. J. Obstet. Gynecol. 2009, 201, 398.e1–398.e8. [Google Scholar] [CrossRef] [Green Version]
- Zhang, G.; Srivastava, A.; Bacelis, J.; Juodakis, J.; Jacobsson, B.; Muglia, L.J. Genetic Studies of Gestational Duration and Preterm Birth. Best Pract. Res. Clin. Obstet. Gynaecol. 2018, 52, 33–47. [Google Scholar] [CrossRef]
- Stevens, N.R.; Tirone, V.; Lillis, T.A.; Holmgreen, L.; Chen-McCracken, A.; Hobfoll, S.E. Posttraumatic Stress and Depression May Undermine Abuse Survivors’ Self-Efficacy in the Obstetric Care Setting. J. Psychosom. Obstet. Gynecol. 2017, 38, 103–110. [Google Scholar] [CrossRef]
- Ertan, D.; Hingray, C.; Burlacu, E.; Sterlé, A.; El-Hage, W. Post-Traumatic Stress Disorder Following Childbirth. BMC Psychiatry 2021, 21, 155. [Google Scholar] [CrossRef]
- Cohen, M.M.; Ansara, D.; Schei, B.; Stuckless, N.; Stewart, D.E. Posttraumatic Stress Disorder after Pregnancy, Labor, and Delivery. J. Womens Health 2004, 13, 315–324. [Google Scholar] [CrossRef] [PubMed]
- Hauff, N.J.; Fry-McComish, J.; Chiodo, L.M. Cumulative Trauma and Partner Conflict Predict Post-Traumatic Stress Disorder in Postpartum African-American Women. J. Clin. Nurs. 2017, 26, 2372–2383. [Google Scholar] [CrossRef] [PubMed]
- Dobernecker, J.; Spyridou, A.; Elbert, T.; Schauer, M.; Garthus-Niegel, S.; Ruf-Leuschner, M.; Schalinski, I. Cumulative Trauma Predicts Hair Cortisol Concentrations and Symptoms of Depression and Anxiety in Pregnant Women-an Investigation of Community Samples from Greece, Spain and Perú. Sci. Rep. 2023, 13, 1434. [Google Scholar] [CrossRef]
- Turton, P.; Hughes, P.; Evans, C.D.; Fainman, D. Incidence, Correlates and Predictors of Post-Traumatic Stress Disorder in the Pregnancy after Stillbirth. Br. J. Psychiatry J. Ment. Sci. 2001, 178, 556–560. [Google Scholar] [CrossRef] [Green Version]
- Çapik, A.; Durmaz, H. Fear of Childbirth, Postpartum Depression, and Birth-Related Variables as Predictors of Posttraumatic Stress Disorder After Childbirth. Worldviews Evid. Based Nurs. 2018, 15, 455–463. [Google Scholar] [CrossRef]
- Nakić Radoš, S.; Martinić, L.; Matijaš, M.; Brekalo, M.; Martin, C. The Relationship between Birth Satisfaction, Posttraumatic Stress Disorder and Postnatal Depression Symptoms in Croatian Women. Stress Health 2021, 38, 500–508. [Google Scholar] [CrossRef]
- Harrison, S.E.; Ayers, S.; Quigley, M.A.; Stein, A.; Alderdice, F. Prevalence and Factors Associated with Postpartum Posttraumatic Stress in a Population-Based Maternity Survey in England. J. Affect. Disord. 2021, 279, 749–756. [Google Scholar] [CrossRef]
- Ayers, S. Birth Trauma and Post-Traumatic Stress Disorder: The Importance of Risk and Resilience. J. Reprod. Infant Psychol. 2017, 35, 427–430. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Beck, C.T.; Watson, S. Subsequent Childbirth after a Previous Traumatic Birth. Nurs. Res. 2010, 59, 241–249. [Google Scholar] [CrossRef]
- Bohren, M.A.; Hofmeyr, G.J.; Sakala, C.; Fukuzawa, R.K.; Cuthbert, A. Continuous Support for Women during Childbirth. Cochrane Database Syst. Rev. 2017, 2017, CD003766. [Google Scholar] [CrossRef] [PubMed]
- Ford, E.; Ayers, S. Support during Birth Interacts with Prior Trauma and Birth Intervention to Predict Postnatal Post-Traumatic Stress Symptoms. Psychol. Health 2011, 26, 1553–1570. [Google Scholar] [CrossRef] [Green Version]
- Halvorsen, L.; Nerum, H.; Oian, P.; Sørlie, T. Giving Birth with Rape in One’s Past: A Qualitative Study. Birth 2013, 40, 182–191. [Google Scholar] [CrossRef]
- Companion of Choice during Labour and Childbirth for Improved Quality of Care. Available online: https://www.who.int/publications-detail-redirect/WHO-SRH-20.13 (accessed on 14 March 2023).
- Borozdina, E.; Novkunskaya, A. Patient-Centered Care in Russian Maternity Hospitals: Introducing a New Approach through Professionals’ Agency. Health 2022, 26, 200–220. [Google Scholar] [CrossRef] [PubMed]
- Ozhiganova, A.A. Active mistrust of doctors: A case study of legal support during childbirth. Sib. Hist. Res. 2020, 4, 195–216. [Google Scholar] [CrossRef]
- WHO Recommendations: Intrapartum Care for a Positive Childbirth Experience. Available online: https://www.who.int/publications-detail-redirect/9789241550215 (accessed on 13 March 2023).
- Образoвание в Цифрах: 2019. Available online: https://issek.hse.ru/news/326742876.html (accessed on 13 March 2023).




{kind=link}
{kind=link}
{kind=link}
| Characteristic | Mean | SD | Range | |
|---|---|---|---|---|
| Age | 31.03 | 4.30 | 18–46 | |
| Time since childbirth | 5.49 | 3.52 | 0–12 | |
| Gestational age at birth | 39.57 | 1.65 | 25.0–43.0 | |
| EPDS | 9.09 | 6.16 | 0–30 | |
| How traumatic did you find your birth? | 3.84 | 2.56 | 1–10 | |
| CBiTS total score (Q3–Q22) | 15.79 | 10.08 | 0–53 | |
| Cumulative traumatic experiences | 0.87 | 1.05 | 0–7 | |
| N | % | |||
| Education | Primary | 44 | 1.7% | |
| Secondary | 185 | 7.2% | ||
| Tertiary | 2350 | 91.1% | ||
| Family status | Married | 2366 | 91.7% | |
| In relationship | 151 | 5.9% | ||
| Single | 51 | 2.0% | ||
| SES 1 | Low-income | 263 | 10.2% | |
| Middle-income | 1707 | 66.2% | ||
| High-income | 609 | 23.6% | ||
| Mode of birth | Vaginal | 1882 | 73% | |
| Assisted vaginal | 64 | 2.5% | ||
| Emergency cesarean | 406 | 15.7% | ||
| Planned cesarean | 227 | 8.8% | ||
| Region of childbirth facility | Moscow | 589 | 22.8% | |
| St. Petersburg | 289 | 11.2% | ||
| Another region in Russia | 1701 | 66% | ||
| Parity | 1 | 1628 | 63.1% | |
| 2 | 700 | 27.1% | ||
| 3+ | 251 | 9.7% | ||
| Support during labor (yes) | 1083 | 42% | ||
| Mode of support | No support | 1496 | 58% | |
| Partner | 649 | 25.2% | ||
| Doula or Private midwife | 227 | 8.8% | ||
| Partner + Doula or Private midwife | 207 | 8% | ||
| Previously diagnosed mental disorders | Yes | 247 | 9.6% | |
| Unsure | 277 | 10.8% | ||
| No | 2050 | 79.6% | ||
| Clinically significant symptoms of PPD (EPDS > 10) | 967 | 37.5% | ||
| Clinically significant symptoms of PP-PTSD (according to DSM-5) | 528 | 20.5% | ||
| Traumatic experience of previous childbirth (yes) | 515 | 20% | ||
| Perinatal loss experience (yes) | 596 | 23.1% | ||
| Physical Assault (yes) | 205 | 7.9% | ||
| Sexual Assault (yes) | 281 | 10.9% | ||
| Child abuse (yes) | 426 | 16.5% | ||
| No previous trauma | 1191 | 46.2% | ||
| Predictor | Cumulative Traumatic Experiences (0–7) | Support during Labor (Yes/No) | ||||||
|---|---|---|---|---|---|---|---|---|
| Outcome | B/OR * | SE | 95% CI | p-Value | B/OR | SE | 95% CI | p-Value |
| PTSD symptoms according to CBiTS continuous scale (0–53) | 1.88 | 0.18 | 1.52–2.24 | <0.001 | −0.89 | 0.40 | −1.67; −0.10 | 0.027 |
| Clinically significant PTSD according to DSM-5 (yes/no) | 1.26 | 0.05 | 1.15–1.38 | <0.001 | 0.73 | 0.11 | 0.58; 0.90 | 0.004 |
| Subjective rates of traumatic birth experience (0–10) | 0.18 | 0.05 | 0.09–0.27 | <0.001 | −0.074 | 0.10 | −0.93; −0.54 | <0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Suarez, A.; Yakupova, V. Past Traumatic Life Events, Postpartum PTSD, and the Role of Labor Support. Int. J. Environ. Res. Public Health 2023, 20, 6048. https://doi.org/10.3390/ijerph20116048
Suarez A, Yakupova V. Past Traumatic Life Events, Postpartum PTSD, and the Role of Labor Support. International Journal of Environmental Research and Public Health. 2023; 20(11):6048. https://doi.org/10.3390/ijerph20116048
Chicago/Turabian StyleSuarez, Anna, and Vera Yakupova. 2023. "Past Traumatic Life Events, Postpartum PTSD, and the Role of Labor Support" International Journal of Environmental Research and Public Health 20, no. 11: 6048. https://doi.org/10.3390/ijerph20116048